
Serum Brevican as a Biomarker of Cerebrovascular Disease in an Elderly Cognitively Impaired Cohort
 , , ,
, , ,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Population
2.2. Demographic and Risk Factor Assessments
2.3. Neuroimaging
2.3.1. Amyloid PET-MRI Acquisition and Quantification
2.3.2. Brain Atrophy and CeVD MRI Markers
2.4. Serum Brevican Measurements
2.5. Statistical Analyses
3. Results
3.1. Participant Characteristics
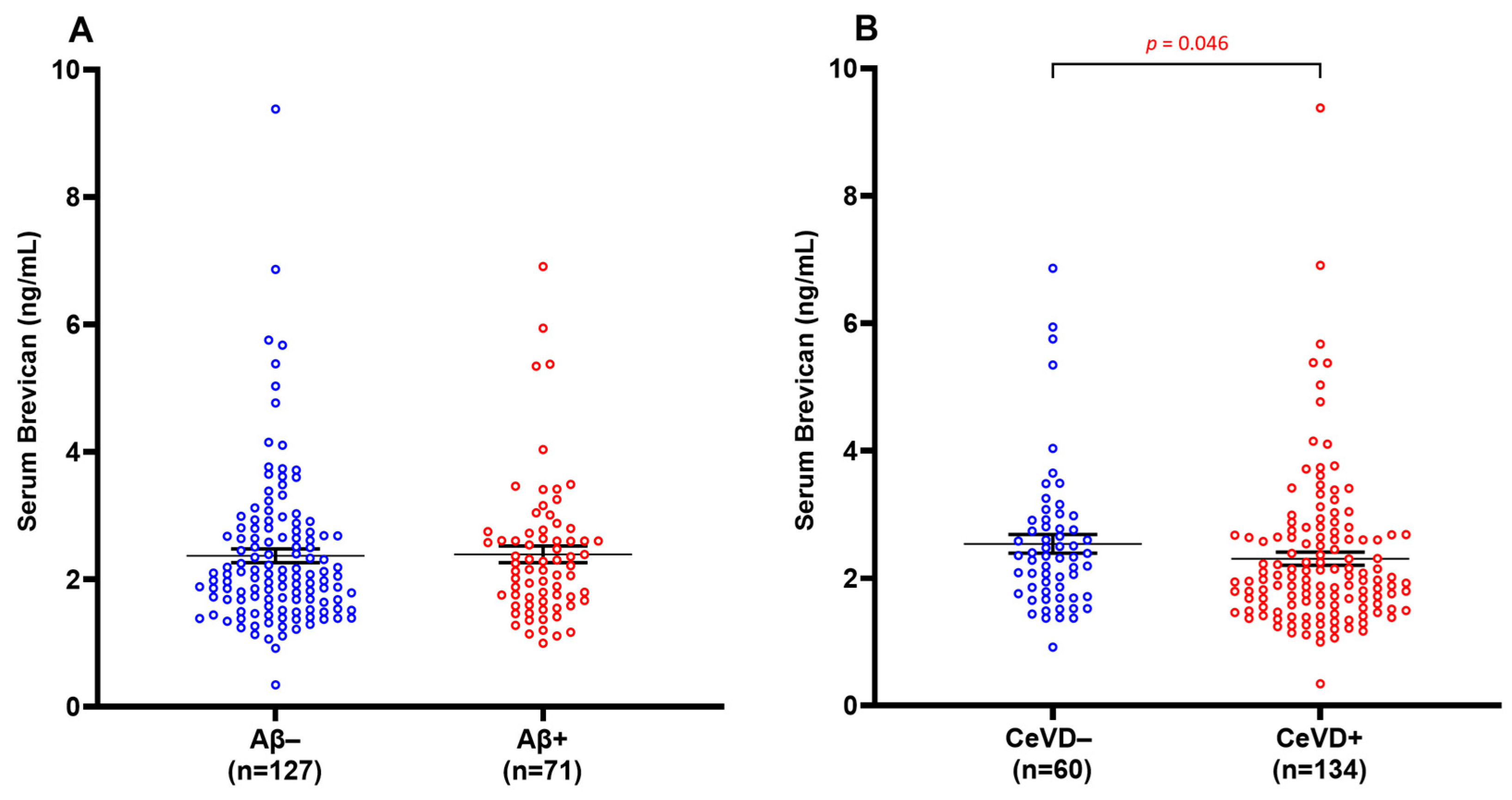
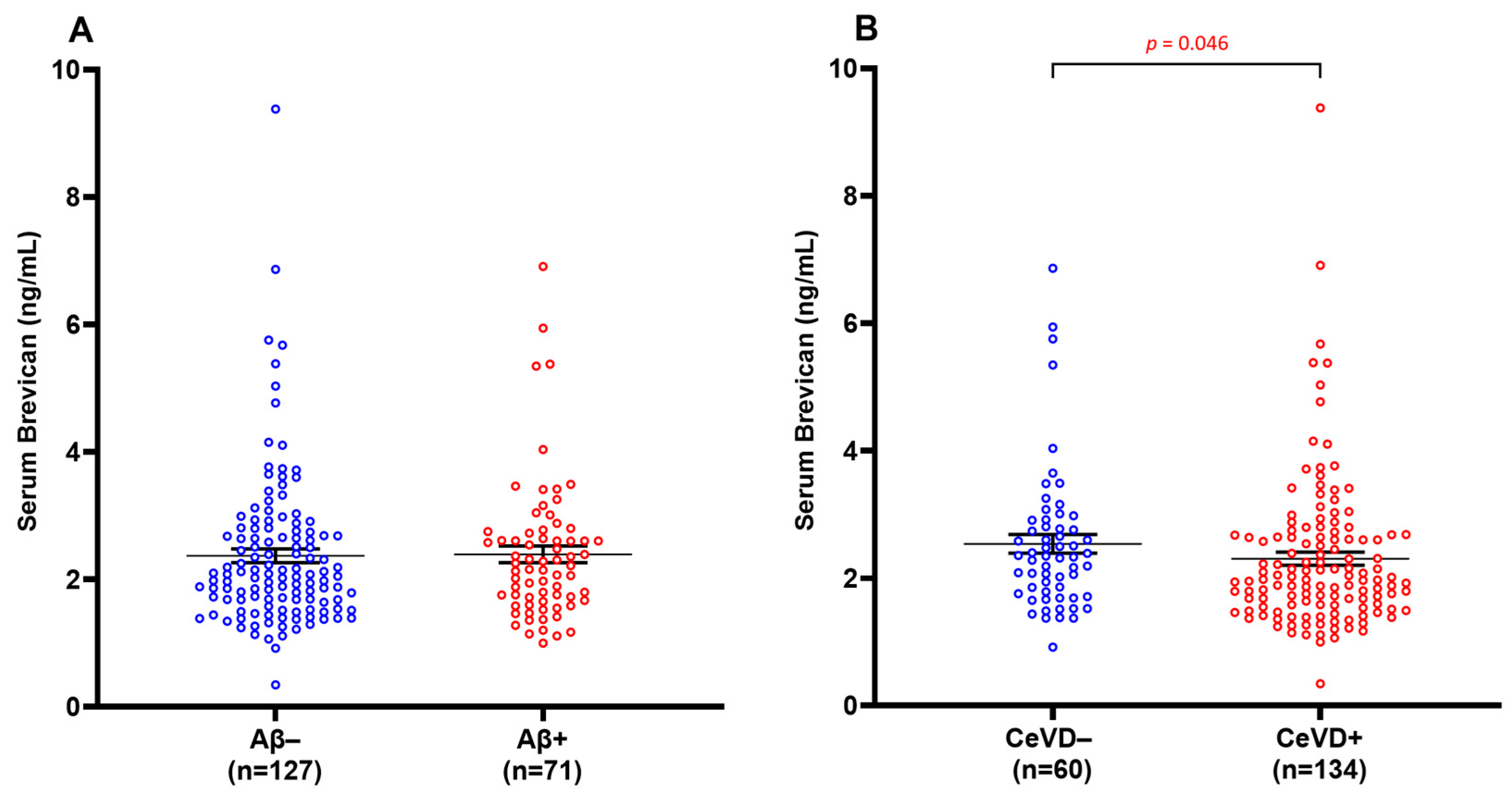
3.2. Serum Brevican Concentrations in a Clinical Cohort Stratified by Aβ and CeVD Burden
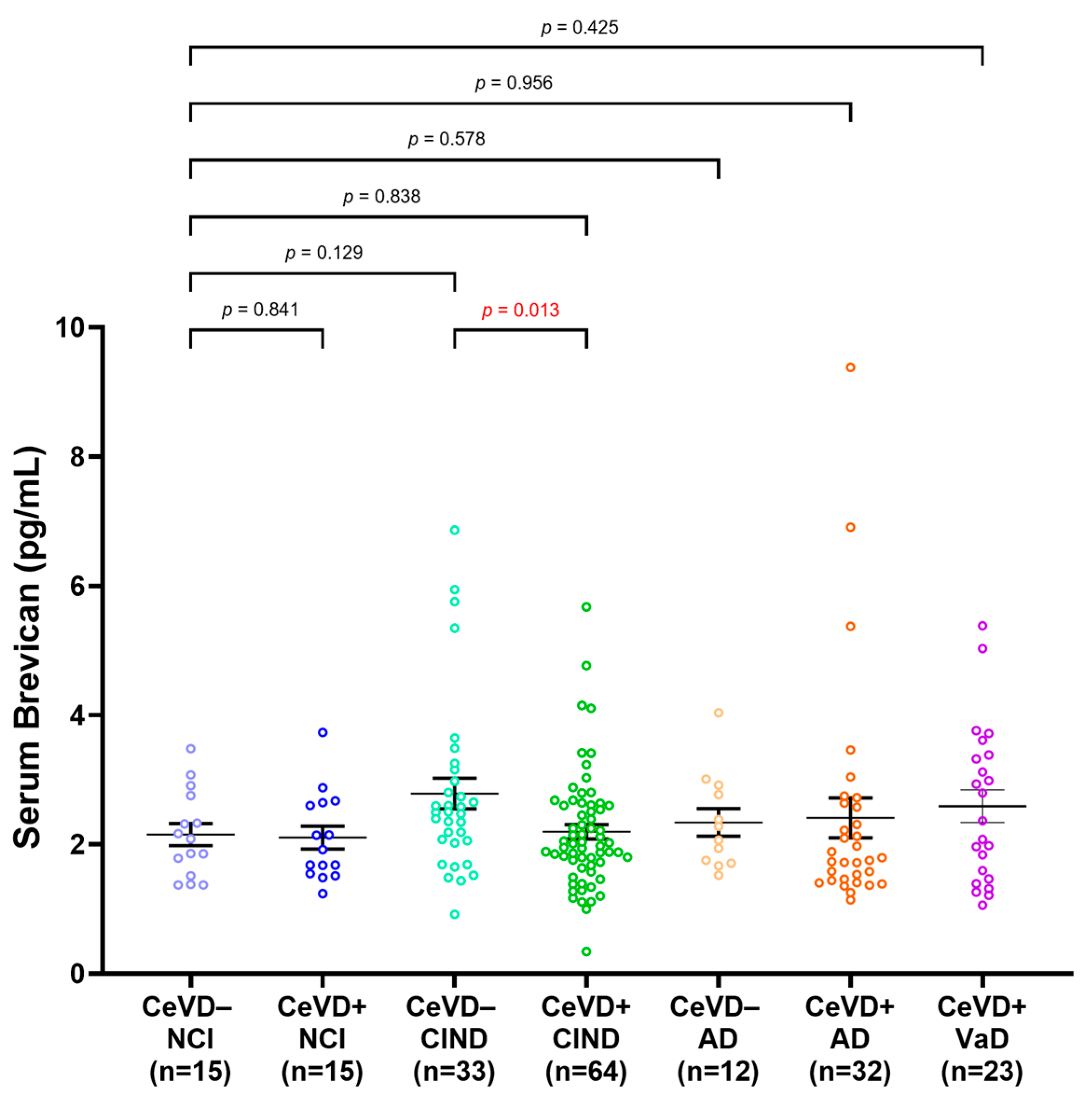
3.3. Serum Brevican Concentrations in a Clinical Cohort Stratified by Clinical Diagnosis and CeVD
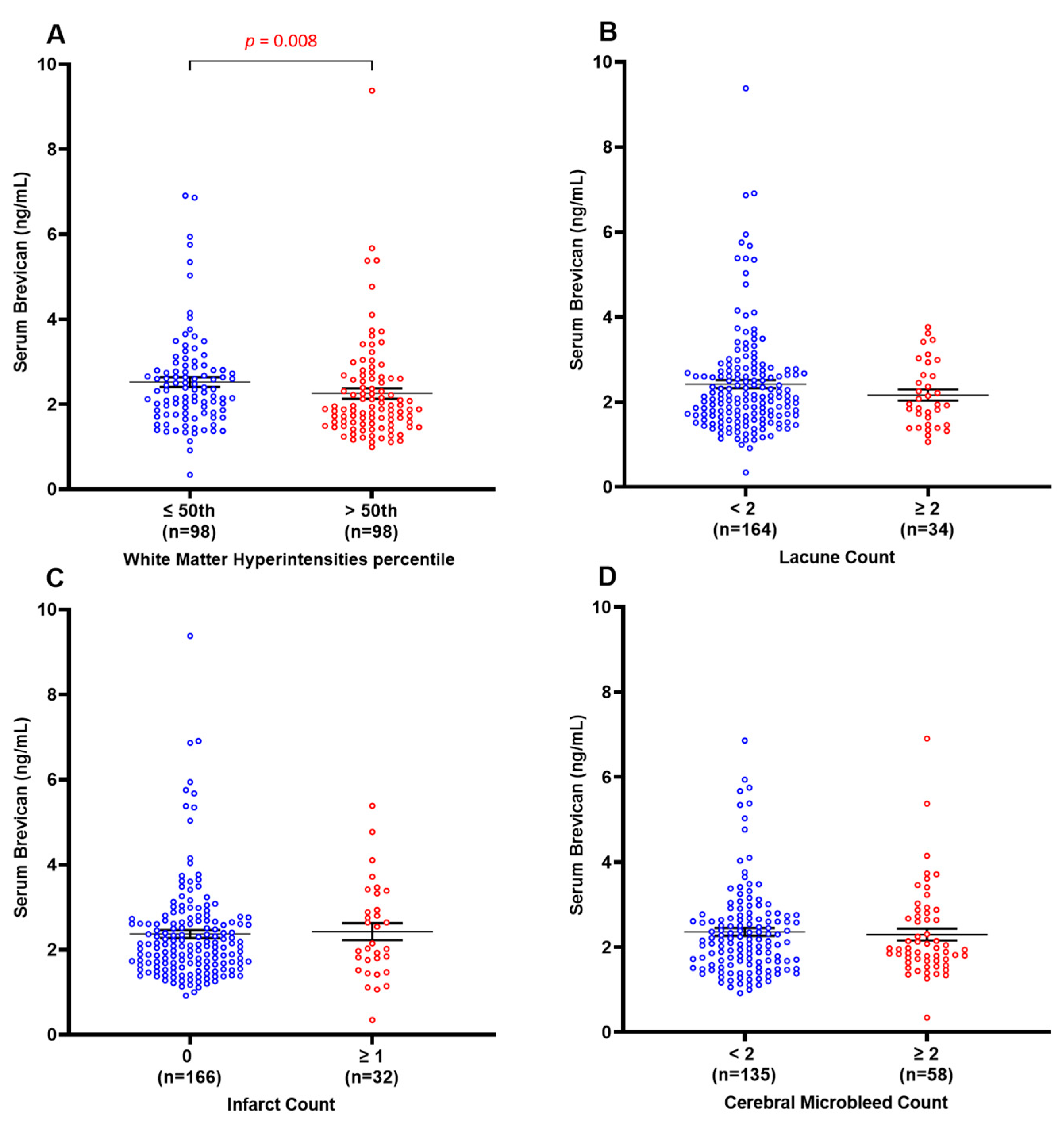
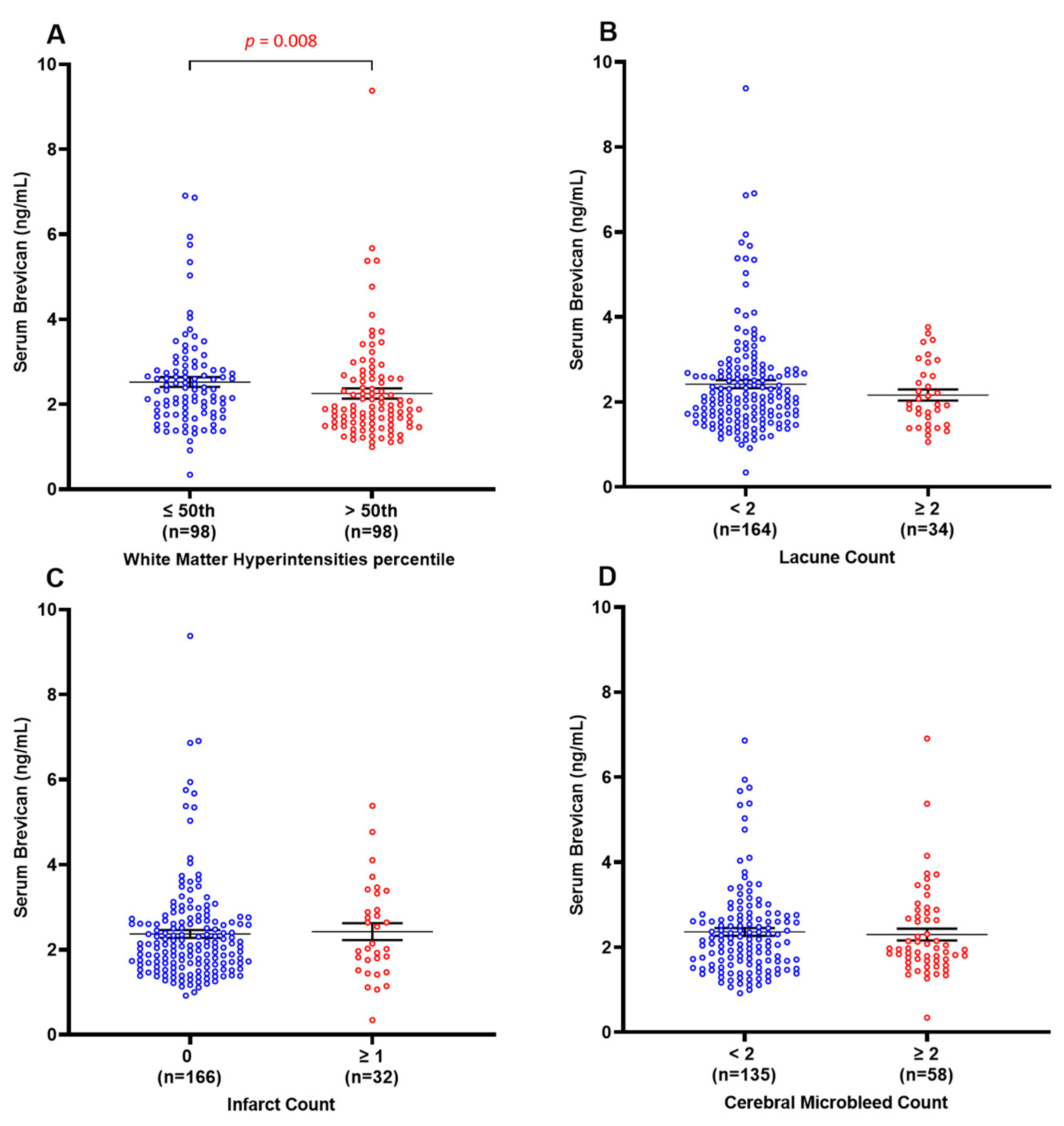
3.4. Decreased Serum Brevican Is Associated Specifically with Elevated White Matter Hyperintensities
3.5. ROC Analyses of Serum Brevican as a Possible Biomarker of Early Vascular Damage
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- McAleese, K.E.; Alafuzoff, I.; Charidimou, A.; De Reuck, J.; Grinberg, L.T.; Hainsworth, A.H.; Hortobagyi, T.; Ince, P.; Jellinger, K.; Gao, J.; et al. Post-mortem assessment in vascular dementia: Advances and aspirations. BMC Med. 2016, 14, 129. [Google Scholar] [CrossRef] [PubMed]
- Jellinger, K.A. Alzheimer disease and cerebrovascular pathology: An update. J. Neural Transm. 2002, 109, 813–836. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.E.; Kim, H.J.; Jang, H.; Weiner, M.W.; DeCarli, C.; Na, D.L.; Seo, S.W. Interaction between Alzheimer’s Disease and Cerebral Small Vessel Disease: A Review Focused on Neuroimaging Markers. Int. J. Mol. Sci. 2022, 23, 10490. [Google Scholar] [CrossRef] [PubMed]
- Chai, Y.L.; Lee, J.H.; Chong, J.R.; Ballard, C.; Francis, P.T.; Kennedy, B.K.; Arumugam, T.V.; Chen, C.P.; Aarsland, D.; Lai, M.K.P. Inflammatory panel cytokines are elevated in the neocortex of late-stage Alzheimer’s disease but not Lewy body dementias. J. Neuroinflamm. 2023, 20, 111. [Google Scholar] [CrossRef] [PubMed]
- Chai, Y.L.; Rajeev, V.; Poh, L.; Selvaraji, S.; Hilal, S.; Chen, C.P.; Jo, D.G.; Koo, E.H.; Arumugam, T.V.; Lai, M.K. Chronic cerebral hypoperfusion alters the CypA-EMMPRIN-gelatinase pathway: Implications for vascular dementia. J. Cereb. Blood Flow. Metab. 2023, 43, 722–735. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Homma, A.; Mok, V.C.; Krishnamoorthy, E.; Alladi, S.; Meguro, K.; Abe, K.; Dominguez, J.; Marasigan, S.; Kandiah, N.; et al. Alzheimer’s disease with cerebrovascular disease: Current status in the Asia-Pacific region. J. Intern. Med. 2016, 280, 359–374. [Google Scholar] [CrossRef] [PubMed]
- Chong, J.R.; Ashton, N.J.; Karikari, T.K.; Tanaka, T.; Saridin, F.N.; Reilhac, A.; Robins, E.G.; Nai, Y.H.; Vrooman, H.; Hilal, S.; et al. Plasma P-tau181 to Aβ42 ratio is associated with brain amyloid burden and hippocampal atrophy in an Asian cohort of Alzheimer’s disease patients with concomitant cerebrovascular disease. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2021, 17, 1649–1662. [Google Scholar] [CrossRef]
- Chong, J.R.; Hilal, S.; Ashton, N.J.; Karikari, T.K.; Reilhac, A.; Vrooman, H.; Schöll, M.; Zetterberg, H.; Blennow, K.; Chen, C.P.; et al. Brain atrophy and white matter hyperintensities are independently associated with plasma neurofilament light chain in an Asian cohort of cognitively impaired patients with concomitant cerebral small vessel disease. Alzheimer’s Dement. 2023, 15, e12396. [Google Scholar] [CrossRef]
- Iadecola, C. The overlap between neurodegenerative and vascular factors in the pathogenesis of dementia. Acta Neuropathol. 2010, 120, 287–296. [Google Scholar] [CrossRef]
- Sun, Y.; Xu, S.; Jiang, M.; Liu, X.; Yang, L.; Bai, Z.; Yang, Q. Role of the Extracellular Matrix in Alzheimer’s Disease. Front. Aging Neurosci. 2021, 13, 707466. [Google Scholar] [CrossRef]
- Schneider, J.A.; Arvanitakis, Z.; Bang, W.; Bennett, D.A. Mixed brain pathologies account for most dementia cases in community-dwelling older persons. Neurology 2007, 69, 2197–2204. [Google Scholar] [CrossRef]
- Agrawal, S.; Schneider, J.A. Vascular pathology and pathogenesis of cognitive impairment and dementia in older adults. Cereb. Circ. Cogn. Behav. 2022, 3, 100148. [Google Scholar] [CrossRef] [PubMed]
- Lam, B.Y.K.; Yiu, B.; Ampil, E.; Chen, C.L.; Dikot, Y.; Dominguez, J.C.; Ganeshbhai, P.V.; Hilal, S.; Kandiah, N.; Kim, S.; et al. High burden of cerebral white matter lesion in 9 Asian cities. Sci. Rep. 2021, 11, 11587. [Google Scholar] [CrossRef] [PubMed]
- Chong, J.R.; Ashton, N.J.; Karikari, T.K.; Tanaka, T.; Schöll, M.; Zetterberg, H.; Blennow, K.; Chen, C.P.; Lai, M.K.P. Blood-based high sensitivity measurements of beta-amyloid and phosphorylated tau as biomarkers of Alzheimer’s disease: A focused review on recent advances. J. Neurol. Neurosurg. Psychiatry 2021, 92, 1231–1241. [Google Scholar] [CrossRef] [PubMed]
- Hosoki, S.; Hansra, G.K.; Jayasena, T.; Poljak, A.; Mather, K.A.; Catts, V.S.; Rust, R.; Sagare, A.; Kovacic, J.C.; Brodtmann, A.; et al. Molecular biomarkers for vascular cognitive impairment and dementia. Nat. Rev. Neurol. 2023, 19, 737–753. [Google Scholar] [CrossRef] [PubMed]
- Teunissen, C.E.; Verberk, I.M.W.; Thijssen, E.H.; Vermunt, L.; Hansson, O.; Zetterberg, H.; van der Flier, W.M.; Mielke, M.M.; Del Campo, M. Blood-based biomarkers for Alzheimer’s disease: Towards clinical implementation. Lancet Neurol. 2022, 21, 66–77. [Google Scholar] [CrossRef] [PubMed]
- Dzyubenko, E.; Gottschling, C.; Faissner, A. Neuron-Glia Interactions in Neural Plasticity: Contributions of Neural Extracellular Matrix and Perineuronal Nets. Neural Plast. 2016, 2016, 5214961. [Google Scholar] [CrossRef] [PubMed]
- Brakebusch, C.; Seidenbecher, C.I.; Asztely, F.; Rauch, U.; Matthies, H.; Meyer, H.; Krug, M.; Bockers, T.M.; Zhou, X.; Kreutz, M.R.; et al. Brevican-deficient mice display impaired hippocampal CA1 long-term potentiation but show no obvious deficits in learning and memory. Mol. Cell. Biol. 2002, 22, 7417–7427. [Google Scholar] [CrossRef]
- Cox, T.R.; Erler, J.T. Remodeling and homeostasis of the extracellular matrix: Implications for fibrotic diseases and cancer. Dis. Model. Mech. 2011, 4, 165–178. [Google Scholar] [CrossRef]
- Morawski, M.; Bruckner, M.K.; Riederer, P.; Bruckner, G.; Arendt, T. Perineuronal nets potentially protect against oxidative stress. Exp. Neurol. 2004, 188, 309–315. [Google Scholar] [CrossRef]
- Martin-de-Saavedra, M.D.; del Barrio, L.; Canas, N.; Egea, J.; Lorrio, S.; Montell, E.; Verges, J.; Garcia, A.G.; Lopez, M.G. Chondroitin sulfate reduces cell death of rat hippocampal slices subjected to oxygen and glucose deprivation by inhibiting p38, NFkappaB and iNOS. Neurochem. Int. 2011, 58, 676–683. [Google Scholar] [CrossRef] [PubMed]
- Soles, A.; Selimovic, A.; Sbrocco, K.; Ghannoum, F.; Hamel, K.; Moncada, E.L.; Gilliat, S.; Cvetanovic, M. Extracellular Matrix Regulation in Physiology and in Brain Disease. Int. J. Mol. Sci. 2023, 24, 7049. [Google Scholar] [CrossRef] [PubMed]
- Miyata, S.; Kitagawa, H. Formation and remodeling of the brain extracellular matrix in neural plasticity: Roles of chondroitin sulfate and hyaluronan. Biochim. Biophys. Acta Gen. Subj. 2017, 1861, 2420–2434. [Google Scholar] [CrossRef] [PubMed]
- Haddock, G.; Cross, A.K.; Allan, S.; Sharrack, B.; Callaghan, J.; Bunning, R.A.; Buttle, D.J.; Woodroofe, M.N. Brevican and phosphacan expression and localization following transient middle cerebral artery occlusion in the rat. Biochem. Soc. Trans. 2007, 35, 692–694. [Google Scholar] [CrossRef] [PubMed]
- Hohn, L.; Hussler, W.; Richter, A.; Smalla, K.H.; Birkl-Toeglhofer, A.M.; Birkl, C.; Vielhaber, S.; Leber, S.L.; Gundelfinger, E.D.; Haybaeck, J.; et al. Extracellular Matrix Changes in Subcellular Brain Fractions and Cerebrospinal Fluid of Alzheimer’s Disease Patients. Int. J. Mol. Sci. 2023, 24, 5532. [Google Scholar] [CrossRef]
- Minta, K.; Brinkmalm, G.; Portelius, E.; Johansson, P.; Svensson, J.; Kettunen, P.; Wallin, A.; Zetterberg, H.; Blennow, K.; Andreasson, U. Brevican and Neurocan Peptides as Potential Cerebrospinal Fluid Biomarkers for Differentiation between Vascular Dementia and Alzheimer’s Disease. J. Alzheimer’s Dis. 2021, 79, 729–741. [Google Scholar] [CrossRef]
- Minta, K.; Portelius, E.; Janelidze, S.; Hansson, O.; Zetterberg, H.; Blennow, K.; Andreasson, U. Cerebrospinal Fluid Concentrations of Extracellular Matrix Proteins in Alzheimer’s Disease. J. Alzheimer’s Dis. 2019, 69, 1213–1220. [Google Scholar] [CrossRef]
- Jonesco, D.S.; Karsdal, M.A.; Henriksen, K. The CNS-specific proteoglycan, brevican, and its ADAMTS4-cleaved fragment show differential serological levels in Alzheimer’s disease, other types of dementia and non-demented controls: A cross-sectional study. PLoS ONE 2020, 15, e0234632. [Google Scholar] [CrossRef]
- Hilal, S.; Chai, Y.L.; Ikram, M.K.; Elangovan, S.; Yeow, T.B.; Xin, X.; Chong, J.Y.; Venketasubramanian, N.; Richards, A.M.; Chong, J.P.; et al. Markers of cardiac dysfunction in cognitive impairment and dementia. Medicine 2015, 94, e297. [Google Scholar] [CrossRef]
- Ng, S.; Villemagne, V.L.; Berlangieri, S.; Lee, S.T.; Cherk, M.; Gong, S.J.; Ackermann, U.; Saunder, T.; Tochon-Danguy, H.; Jones, G.; et al. Visual assessment versus quantitative assessment of 11C-PIB PET and 18F-FDG PET for detection of Alzheimer’s disease. J. Nucl. Med. Off. Publ. Soc. Nucl. Med. 2007, 48, 547–552. [Google Scholar] [CrossRef]
- Yamane, T.; Ishii, K.; Sakata, M.; Ikari, Y.; Nishio, T.; Ishii, K.; Kato, T.; Ito, K.; Senda, M.; Group, J.A.S. Inter-rater variability of visual interpretation and comparison with quantitative evaluation of 11C-PiB PET amyloid images of the Japanese Alzheimer’s Disease Neuroimaging Initiative (J-ADNI) multicenter study. Eur. J. Nucl. Med. Mol. Imaging 2017, 44, 850–857. [Google Scholar] [CrossRef] [PubMed]
- Saridin, F.N.; Hilal, S.; Villaraza, S.G.; Reilhac, A.; Gyanwali, B.; Tanaka, T.; Stephenson, M.C.; Ng, S.L.; Vrooman, H.; van der Flier, W.M.; et al. Brain amyloid β, cerebral small vessel disease, and cognition. Neurology 2020, 95, e2845–e2853. [Google Scholar] [CrossRef] [PubMed]
- van Veluw, S.J.; Hilal, S.; Kuijf, H.J.; Ikram, M.K.; Xin, X.; Yeow, T.B.; Venketasubramanian, N.; Biessels, G.J.; Chen, C. Cortical microinfarcts on 3T MRI: Clinical correlates in memory-clinic patients. Alzheimer’s Dement. J. Alzheimer’s Assoc. 2015, 11, 1500–1509. [Google Scholar] [CrossRef] [PubMed]
- Vrooman, H.A.; Cocosco, C.A.; van der Lijn, F.; Stokking, R.; Ikram, M.A.; Vernooij, M.W.; Breteler, M.M.; Niessen, W.J. Multi-spectral brain tissue segmentation using automatically trained k-Nearest-Neighbor classification. Neuroimage 2007, 37, 71–81. [Google Scholar] [CrossRef] [PubMed]
- de Boer, R.; Vrooman, H.A.; Ikram, M.A.; Vernooij, M.W.; Breteler, M.M.; van der Lugt, A.; Niessen, W.J. Accuracy and reproducibility study of automatic MRI brain tissue segmentation methods. Neuroimage 2010, 51, 1047–1056. [Google Scholar] [CrossRef] [PubMed]
- Gyanwali, B.; Shaik, M.A.; Venketasubramanian, N.; Chen, C.; Hilal, S. Mixed-Location Cerebral Microbleeds: An Imaging Biomarker for Cerebrovascular Pathology in Cognitive Impairment and Dementia in a Memory Clinic Population. J. Alzheimer’s Dis. JAD 2019, 71, 1309–1320. [Google Scholar] [CrossRef] [PubMed]
- Morawski, M.; Bruckner, G.; Jager, C.; Seeger, G.; Matthews, R.T.; Arendt, T. Involvement of perineuronal and perisynaptic extracellular matrix in Alzheimer’s disease neuropathology. Brain Pathol. 2012, 22, 547–561. [Google Scholar] [CrossRef]
- Mayer, J.; Hamel, M.G.; Gottschall, P.E. Evidence for proteolytic cleavage of brevican by the ADAMTSs in the dentate gyrus after excitotoxic lesion of the mouse entorhinal cortex. BMC Neurosci. 2005, 6, 52. [Google Scholar] [CrossRef]
- Wang, X.; Khalil, R.A. Matrix Metalloproteinases, Vascular Remodeling, and Vascular Disease. Adv. Pharmacol. 2018, 81, 241–330. [Google Scholar] [CrossRef]
- Raffetto, J.D.; Khalil, R.A. Matrix metalloproteinases and their inhibitors in vascular remodeling and vascular disease. Biochem. Pharmacol. 2008, 75, 346–359. [Google Scholar] [CrossRef]
- Hobeika, M.J.; Thompson, R.W.; Muhs, B.E.; Brooks, P.C.; Gagne, P.J. Matrix metalloproteinases in peripheral vascular disease. J. Vasc. Surg. 2007, 45, 849–857. [Google Scholar] [CrossRef] [PubMed]
- Toledo, J.B.; Arnold, S.E.; Raible, K.; Brettschneider, J.; Xie, S.X.; Grossman, M.; Monsell, S.E.; Kukull, W.A.; Trojanowski, J.Q. Contribution of cerebrovascular disease in autopsy confirmed neurodegenerative disease cases in the National Alzheimer’s Coordinating Centre. Brain 2013, 136, 2697–2706. [Google Scholar] [CrossRef] [PubMed]
- Lendahl, U.; Nilsson, P.; Betsholtz, C. Emerging links between cerebrovascular and neurodegenerative diseases—A special role for pericytes. EMBO Rep. 2019, 20, e48070. [Google Scholar] [CrossRef] [PubMed]
- Dityatev, A.; Schachner, M.; Sonderegger, P. The dual role of the extracellular matrix in synaptic plasticity and homeostasis. Nat. Rev. Neurosci. 2010, 11, 735–746. [Google Scholar] [CrossRef]
- Favuzzi, E.; Marques-Smith, A.; Deogracias, R.; Winterflood, C.M.; Sanchez-Aguilera, A.; Mantoan, L.; Maeso, P.; Fernandes, C.; Ewers, H.; Rico, B. Activity-Dependent Gating of Parvalbumin Interneuron Function by the Perineuronal Net Protein Brevican. Neuron 2017, 95, 639–655.e610. [Google Scholar] [CrossRef] [PubMed]
- Morellini, F.; Sivukhina, E.; Stoenica, L.; Oulianova, E.; Bukalo, O.; Jakovcevski, I.; Dityatev, A.; Irintchev, A.; Schachner, M. Improved reversal learning and working memory and enhanced reactivity to novelty in mice with enhanced GABAergic innervation in the dentate gyrus. Cereb. Cortex 2010, 20, 2712–2727. [Google Scholar] [CrossRef] [PubMed]
- Ueno, H.; Takahashi, Y.; Murakami, S.; Wani, K.; Miyazaki, T.; Matsumoto, Y.; Okamoto, M.; Ishihara, T. Component-specific reduction in perineuronal nets in senescence-accelerated mouse strains. IBRO Neurosci. Rep. 2023, 14, 111–121. [Google Scholar] [CrossRef] [PubMed]
- Chutinet, A.; Rost, N.S. White matter disease as a biomarker for long-term cerebrovascular disease and dementia. Curr. Treat. Options Cardiovasc. Med. 2014, 16, 292. [Google Scholar] [CrossRef]
- Bjerke, M.; Zetterberg, H.; Edman, A.; Blennow, K.; Wallin, A.; Andreasson, U. Cerebrospinal fluid matrix metalloproteinases and tissue inhibitor of metalloproteinases in combination with subcortical and cortical biomarkers in vascular dementia and Alzheimer’s disease. J. Alzheimer’s Dis. JAD 2011, 27, 665–676. [Google Scholar] [CrossRef]
- Lorenzl, S.; Buerger, K.; Hampel, H.; Beal, M.F. Profiles of matrix metalloproteinases and their inhibitors in plasma of patients with dementia. Int. Psychogeriatr. IPA 2008, 20, 67–76. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| NCI | CIND | AD | VaD | p-Value | |
|---|---|---|---|---|---|
| Demographics | |||||
| Maximum n | 32 | 97 | 46 | 23 | |
| Age, y, mean (SD) | 76 (4) | 76 (6) | 77 (8) | 75 (9) | 0.767 |
| Female, n (%) | 21 (66) | 49 (51) | 36 (78) g | 8 (35) h | 0.001 |
| Education, y, mean (SD) | 11 (5) | 8 (5) | 5 (5) a,b | 4 (4) a | <0.001 |
| APOE ε4 carrier, n (%) | 3 (9) | 25 (26) | 20 (44) f | 7 (30) | 0.01 |
| Hypertension, n (%) | 23 (72) | 73 (75) | 35 (76) | 21 (91) | 0.349 |
| Diabetes, n (%) | 5 (16) | 32 (33) | 10 (22) | 9 (39) | 0.126 |
| Hyperlipidaemia, n (%) | 26 (81) | 70 (72) | 29 (63) | 19 (83) | 0.213 |
| Cardiovascular diseases, n (%) | 1 (3) | 10 (11) | 1 (2) | 3 (14) | 0.162 |
| Neuroimaging | |||||
| Presence of ≥2 lacunes, n (%) | 2 (6) | 16 (17) | 3 (7) g | 13 (57) f,g,h | <0.001 |
| Presence of cortical infarct, n (%) | 2 (6) | 15 (16) | 6 (13) | 9 (39) f | 0.009 |
| Presence of ≥2 CMBs, n (%) | 10 (33) | 24 (25) | 17 (40) | 7 (30) | 0.348 |
| Higher 50th WMH, n (%) | 8 (25) | 49 (51) | 26 (58) f | 15 (68) f | 0.007 |
| WMH volume, median (IQR), mL | 1.4 (3.9) | 3.7 (11.0) c | 5.3 (10.7) c | 14.6 (21.6) c | 0.001 |
| Hippocampal volume, median (IQR), mL | 7.1 (0.9) | 6.3 (1.8) | 5.0 (1.0) c,d | 6.0 (1.1) c,e | <0.001 |
| Global cortical thickness, median (IQR), mm | 2.4 (0.2) | 2.3 (0.1) | 2.2 (0.2) c,d | 2.3 (0.2) | <0.001 |
| Positive Aβ PET read, n (%) | 4 (13) | 32 (33) | 31 (67) f,g | 4 (17) h | <0.001 |
| PiB-PET SUVR, median (IQR) | 1.1 (0.1) | 1.2 (0.4) | 1.9 (0.7) | 1.2 (0.3) | <0.001 |
| Elevated CeVD, n (%) | 15 (50) | 64 (66) | 32 (73) | 23 (100) f,g | 0.001 |
| Serum brevican, median (IQR), ng/mL | 2.0 (1.1) | 2.2 (0.9) | 2.0 (1.2) | 2.4 (1.9) | 0.476 |
| CeVD Binary Outcome Variables Using Binary Logistic Regression | ||||||||
|---|---|---|---|---|---|---|---|---|
| Serum Brevican (Tertiles) | WMH (>50th Percentile) (n = 196) | Presence of ≥2 Lacunes (n = 198) | Presence of Cortical Infarcts (n = 198) | Presence of ≥2 CMBs (n = 194) | ||||
| OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | OR (95% CI) | p | |
| Model 1 | ||||||||
| Lowest | 2.8 (1.4–5.8) | 0.005 | 1.3 (0.5–3.3) | 0.626 | 0.5 (0.2–1.3) | 0.164 | 1.0 (0.4–2.1) | 0.907 |
| Middle | 1.5 (0.8–3.1) | 0.235 | 1.3 (0.5–3.4) | 0.550 | 0.6 (0.2–1.4) | 0.207 | 1.0 (0.5–2.2) | 0.926 |
| Highest | 1 | 1 | 1 | 1 | ||||
| Model 2 | ||||||||
| Lowest | 2.8 (1.4–5.8) | 0.006 | 1.4 (0.5–3.7) | 0.522 | 0.5 (0.2–1.4) | 0.192 | 1.0 (0.4–2.1) | 0.958 |
| Middle | 1.5 (0.8–3.1) | 0.223 | 1.4 (0.5–3.7) | 0.479 | 0.6 (0.2–1.5) | 0.248 | 1.0 (0.5–2.2) | 0.909 |
| Highest | 1 | 1 | 1 | 1 | ||||
| Model 3 | ||||||||
| Lowest | 3.0 (1.4–6.4) | 0.005 | 1.1 (0.4–3.2) | 0.853 | 0.4 (0.1–1.2) | 0.099 | 0.8 (0.3–1.8) | 0.522 |
| Middle | 1.6 (0.8–3.5) | 0.197 | 1.4 (0.5–4.1) | 0.518 | 0.3 (0.1–1.0) | 0.050 | 0.9 (0.4–2.1) | 0.743 |
| Highest | 1 | 1 | 1 | 1 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chia, R.S.L.; Minta, K.; Wu, L.-Y.; Salai, K.H.T.; Chai, Y.L.; Hilal, S.; Venketasubramanian, N.; Chen, C.P.; Chong, J.R.; Lai, M.K.P. Serum Brevican as a Biomarker of Cerebrovascular Disease in an Elderly Cognitively Impaired Cohort. Biomolecules 2024, 14, 75. https://doi.org/10.3390/biom14010075
Chia RSL, Minta K, Wu L-Y, Salai KHT, Chai YL, Hilal S, Venketasubramanian N, Chen CP, Chong JR, Lai MKP. Serum Brevican as a Biomarker of Cerebrovascular Disease in an Elderly Cognitively Impaired Cohort. Biomolecules. 2024; 14(1):75. https://doi.org/10.3390/biom14010075
Chicago/Turabian StyleChia, Rachel S. L., Karolina Minta, Liu-Yun Wu, Kaung H. T. Salai, Yuek Ling Chai, Saima Hilal, Narayanaswamy Venketasubramanian, Christopher P. Chen, Joyce R. Chong, and Mitchell K. P. Lai. 2024. "Serum Brevican as a Biomarker of Cerebrovascular Disease in an Elderly Cognitively Impaired Cohort" Biomolecules 14, no. 1: 75. https://doi.org/10.3390/biom14010075
APA StyleChia, R. S. L., Minta, K., Wu, L.-Y., Salai, K. H. T., Chai, Y. L., Hilal, S., Venketasubramanian, N., Chen, C. P., Chong, J. R., & Lai, M. K. P. (2024). Serum Brevican as a Biomarker of Cerebrovascular Disease in an Elderly Cognitively Impaired Cohort. Biomolecules, 14(1), 75. https://doi.org/10.3390/biom14010075