
Plasma Brain-Derived Neurotrophic Factor Levels in First-Episode and Recurrent Major Depression and before and after Bright Light Therapy in Treatment-Resistant Depression

 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Study Design
2.3. Bright Light Therapy
2.4. Blood Sampling and Plasma BDNF Measurement
2.5. Statistics
3. Results
3.1. Subject Characteristics
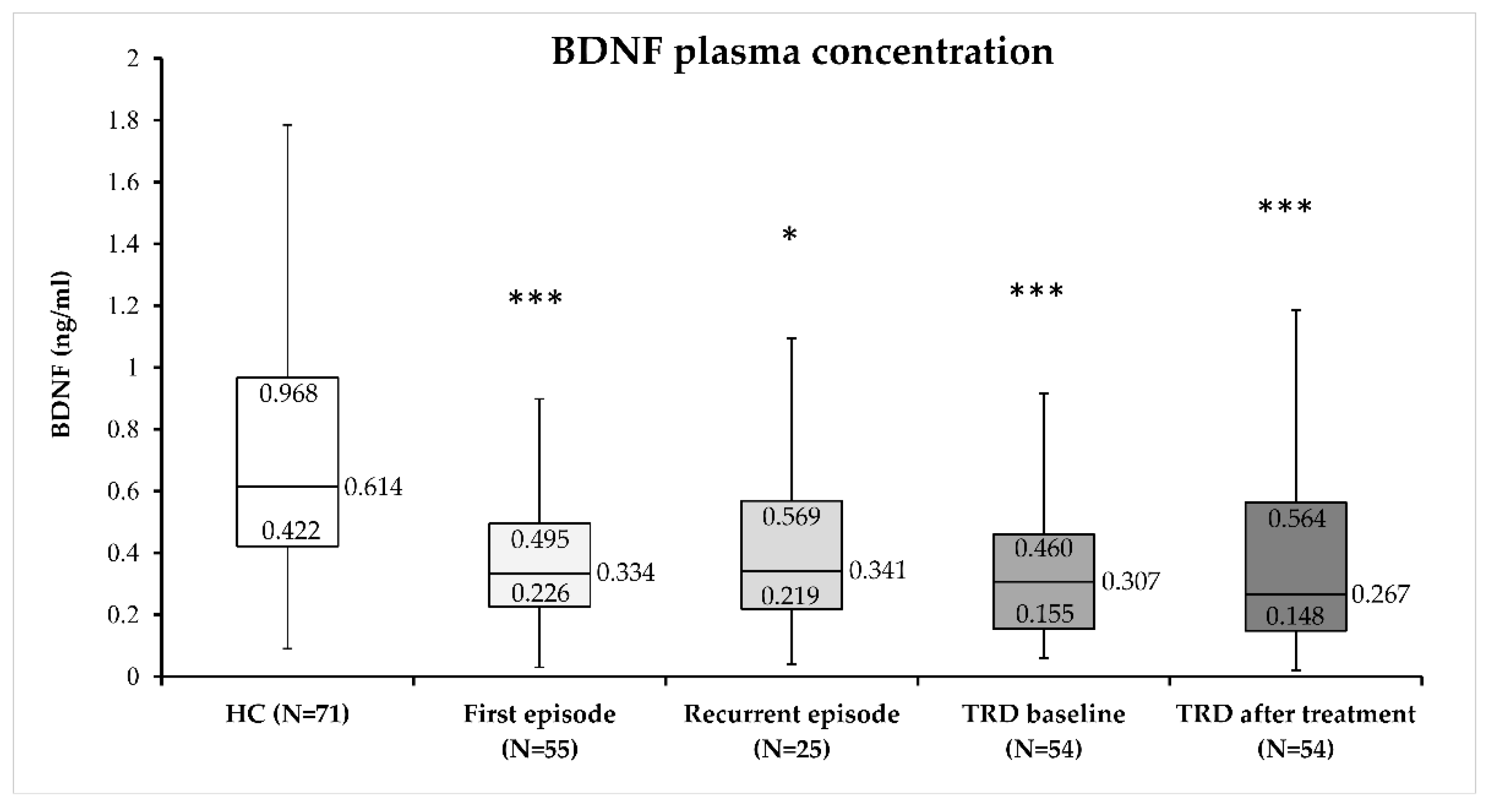
3.2. Plasma BDNF Concentration in MDD Subjects
3.3. Plasma BDNF Concentration in TRD Patients before BLT
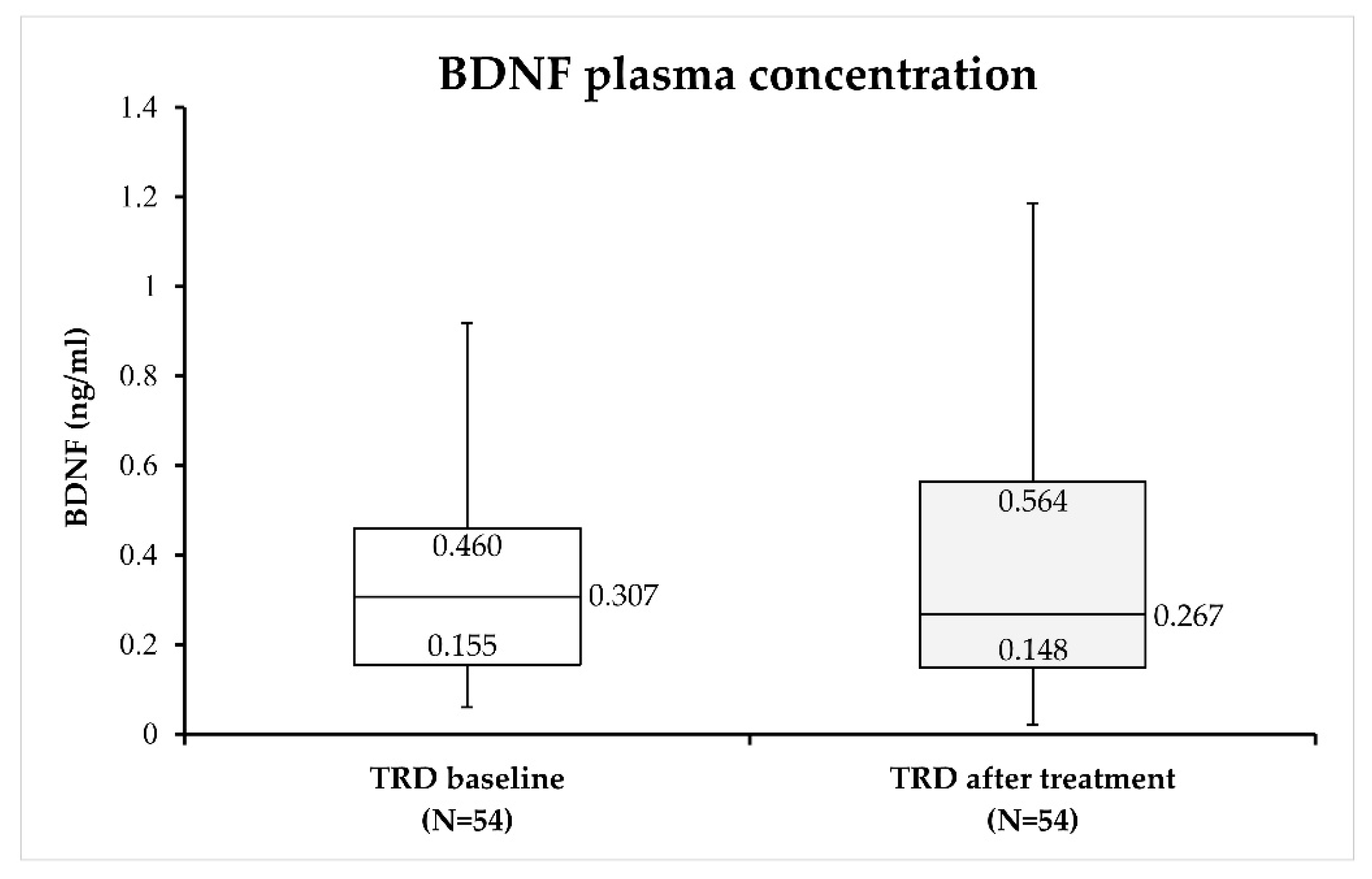
3.4. BLT and Plasma BDNF Concentration in TRD Patients
4. Discussion
4.1. Plasma BDNF Concentration in MDD Patients
4.2. Plasma BDNF Concentration after BLT
4.3. Limitations and Strengths of the Study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sagud, M.; Mihaljevic-Peles, A.; Uzun, S.; Vuksan Cusa, B.; Kozumplik, O.; Kudlek-Mikulic, S.; Mustapic, M.; Barisic, I.; Muck-Seler, D.; Pivac, N. The lack of association between components of metabolic syndrome and treatment resistance in depression. Psychopharmacology 2013, 230, 15–21. [Google Scholar] [CrossRef][Green Version]
- Zhdanava, M.; Pilon, D.; Ghelerter, I.; Chow, W.; Joshi, K.; Lefebvre, P.; Sheehan, J.J. The Prevalence and National Burden of Treatment-Resistant Depression and Major Depressive Disorder in the United States. J. Clin. Psychiatry 2021, 82, 20m13699. [Google Scholar] [CrossRef]
- García Bonetto, G.; Corral, R.M.; Lupo, C.; Vilapriño Duprat, M.; Alessandria, H.; Kanevsky, G.; Cabrera, P. Trastorno depresivo mayor y depresión resistente al tratamiento: Un análisis epidemiológico en Argentina del estudio de Depresión resistente al tratamiento en América Latina [Major depressive disorder and treatment-resistant depression: An epidemiological analysis in Argentina of the Study of Treatment-Resistant Depression in Latin America]. Vertex 2022, XXXIII, 36–49. [Google Scholar] [CrossRef]
- Soares, B.; Kanevsky, G.; Teng, C.T.; Pérez-Esparza, R.; Bonetto, G.G.; Lacerda, A.L.T.; Uribe, E.S.; Cordoba, R.; Lupo, C.; Samora, A.M.; et al. Prevalence and Impact of Treatment-Resistant Depression in Latin America: A Prospective, Observational Study. Psychiatr. Q. 2021, 92, 1797–1815. [Google Scholar] [CrossRef]
- Kern, D.M.; Canuso, C.M.; Daly, E.; Johnson, J.C.; Fu, D.J.; Doherty, T.; Blauer-Peterson, C.; Cepeda, M.S. Suicide-specific mortality among patients with treatment-resistant major depressive disorder, major depressive disorder with prior suicidal ideation or suicide attempts, or major depressive disorder alone. Brain Behav. 2023, 21, e3171. [Google Scholar] [CrossRef] [PubMed]
- Li, C.T. Overview of treatment-resistant depression. Prog. Brain Res. 2023, 278, 1–23. [Google Scholar] [CrossRef] [PubMed]
- Nuñez, N.A.; Joseph, B.; Pahwa, M.; Kumar, R.; Resendez, M.G.; Prokop, L.J.; Veldic, M.; Seshadri, A.; Biernacka, J.M.; Frye, M.A.; et al. Augmentation strategies for treatment resistant major depression: A systematic review and network meta-analysis. J. Affect. Disord. 2022, 302, 385–400. [Google Scholar] [CrossRef]
- Vas, C.; Jain, A.; Trivedi, M.; Jha, M.K.; Mathew, S.J. Pharmacotherapy for Treatment-Resistant Depression: Antidepressants and Atypical Antipsychotics. Psychiatr. Clin. N. Am. 2023, 46, 261–275. [Google Scholar] [CrossRef] [PubMed]
- Carter, B.; Strawbridge, R.; Husain, M.I.; Jones, B.D.M.; Short, R.; Cleare, A.J.; Tsapekos, D.; Patrick, F.; Marwood, L.; Taylor, R.W.; et al. Relative effectiveness of augmentation treatments for treatment-resistant depression: A systematic review and network meta-analysis. Int. Rev. Psychiatry 2020, 32, 477–490. [Google Scholar] [CrossRef]
- Liu, P.; Zhang, S.S.; Liang, Y.; Gao, Z.J.; Gao, W.; Dong, B.H. Efficacy and Safety of Esketamine Combined with Antidepressants for Treatment-Resistant Depression: A Meta-Analysis. Neuropsychiatr. Dis. Treat. 2022, 18, 2855–2865. [Google Scholar] [CrossRef]
- Li, J.; Cui, L.; Li, H. Optimal parameter determination of repetitive transcranial magnetic stimulation for treating treatment-resistant depression: A network meta-analysis of randomized controlled trials. Front. Psychiatry 2022, 13, 1038312. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Cui, L.; Li, J.; Liu, Y.; Chen, Y. Comparative efficacy and acceptability of neuromodulation procedures in the treatment of treatment-resistant depression: A network meta-analysis of randomized controlled trials. J. Affect. Disord. 2021, 287, 115–124. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Xi, Y.; Peng, Y.; Yang, Y.; Huang, X.; Fu, Y.; Tao, Q.; Xiao, J.; Yuan, T.; An, K.; et al. A Visual Circuit Related to Habenula Underlies the Antidepressive Effects of Light Therapy. Neuron 2019, 102, 128–142.e8. [Google Scholar] [CrossRef] [PubMed]
- Levitt, A.J.; Joffe, R.T.; Kennedy, S.H. Bright light augmentation in antidepressant nonresponders. J. Clin. Psychiatry 1991, 52, 336–337. [Google Scholar] [PubMed]
- Prasko, J.; Brunovsky, M.; Latalova, K.; Grambal, A.; Raszka, M.; Vyskocilova, J.; Zavesicka, L. Augmentation of antidepressants with bright light therapy in patients with comorbid depression and borderline personality disorder. Biomed. Pap. Med. Fac. Univ. Palacky Olomouc Czech. Repub. 2010, 154, 355–361. [Google Scholar] [CrossRef]
- Echizenya, M.; Suda, H.; Takeshima, M.; Inomata, Y.; Shimizu, T. Total sleep deprivation followed by sleep phase advance and bright light therapy in drug-resistant mood disorders. J. Affect. Disord. 2013, 144, 28–33. [Google Scholar] [CrossRef]
- Kragh, M.; Larsen, E.R.; Martiny, K.; Møller, D.N.; Wihlborg, C.S.; Lindhardt, T.; Videbech, P. Predictors of response to combined wake and light therapy in treatment-resistant inpatients with depression. Chronobiol. Int. 2018, 35, 1209–1220. [Google Scholar] [CrossRef]
- Sikkens, D.; Riemersma-Van der Lek, R.F.; Meesters, Y.; Schoevers, R.A.; Haarman, B.C.M. Combined sleep deprivation and light therapy: Clinical treatment outcomes in patients with complex unipolar and bipolar depression. J. Affect. Disord. 2019, 246, 727–730. [Google Scholar] [CrossRef]
- Mania, I.; Kaur, J. Bright Light Therapy and rTMS; novel combination approach for the treatment of depression. Brain Stimul. 2019, 12, 1338–1339. [Google Scholar] [CrossRef]
- Chojnacka, M.; Antosik-Wójcińska, A.Z.; Dominiak, M.; Bzinkowska, D.; Borzym, A.; Sokół-Szawłowska, M.; Bodzak-Opolska, G.; Antoniak, D.; Święcicki, Ł. A sham-controlled randomized trial of adjunctive light therapy for non-seasonal depression. J. Affect. Disord. 2016, 203, 1–8. [Google Scholar] [CrossRef]
- Barbini, B.; Attanasio, F.; Manfredi, E.; Cavallini, M.C.; Zanardi, R.; Colombo, C. Bright light therapy accelerates the antidepressant effect of repetitive transcranial magnetic stimulation in treatment resistant depression: A pilot study. Int. J. Psychiatry Clin. Pract. 2021, 25, 375–377. [Google Scholar] [CrossRef]
- Nikolac Perkovic, M.; Gredicak, M.; Sagud, M.; Nedic Erjavec, G.; Uzun, S.; Pivac, N. The association of brain-derived neurotrophic factor with the diagnosis and treatment response in depression. Expert Rev. Mol. Diagn. 2023, 23, 283–296. [Google Scholar] [CrossRef] [PubMed]
- Polyakova, M.; Stuke, K.; Schuemberg, K.; Mueller, K.; Schoenknecht, P.; Schroeter, M.L. BDNF as a biomarker for successful treatment of mood disorders: A systematic & quantitative meta-analysis. J. Affect. Disord. 2015, 174, 432–440. [Google Scholar] [CrossRef]
- Tiwari, S.; Qi, L.; Wong, J.; Han, Z. Association of peripheral manifestation of brain-derived neurotrophic factor with depression: A meta-analysis. Brain Behav. 2022, 12, e32581. [Google Scholar] [CrossRef] [PubMed]
- Cavaleri, D.; Moretti, F.; Bartoccetti, A.; Mauro, S.; Crocamo, C.; Carrà, G.; Bartoli, F. The role of BDNF in major depressive disorder, related clinical features, and antidepressant treatment: Insight from meta-analyses. Neurosci. Biobehav. Rev. 2023, 149, 105159. [Google Scholar] [CrossRef]
- Kwon, S.J.; Park, J.; Park, S.Y.; Song, K.S.; Jung, S.T.; Jung, S.B.; Park, I.R.; Choi, W.S.; Kwon, S.O. Low-intensity treadmill exercise and/or bright light promote neurogenesis in adult rat brain. Neural Regen. Res. 2013, 8, 922–929. [Google Scholar] [CrossRef]
- Tirassa, P.; Iannitelli, A.; Sornelli, F.; Cirulli, F.; Mazza, M.; Calza, A.; Alleva, E.; Branchi, I.; Aloe, L.; Bersani, G.; et al. Daily serum and salivary BDNF levels correlate with morning-evening personality type in women and are affected by light therapy. Riv. Psichiatr. 2012, 47, 527–534. [Google Scholar] [CrossRef]
- Normann, A.J. The Effect of Light Therapy and Acute Aerobic Exercise on Serum Brain Derived Neurotrophic Factor in Older Adults. Master’s Thesis, California State University, Long Beach, CA, USA, 2020. [Google Scholar]
- Molendijk, M.L.; Haffmans, J.P.; Bus, B.A.; Spinhoven, P.; Penninx, B.W.; Prickaerts, J.; Oude Voshaar, R.C.; Elzinga, B.M. Serum BDNF concentrations show strong seasonal variation and correlations with the amount of ambient sunlight. PLoS ONE 2012, 7, e48046. [Google Scholar] [CrossRef]
- Meshkat, S.; Alnefeesi, Y.; Jawad, M.Y.; Di Vincenzo, J.D.; Rodrigues, B.N.; Ceban, F.; Mw Lui, L.; McIntyre, R.S.; Rosenblat, J.D. Brain-Derived Neurotrophic Factor (BDNF) as a biomarker of treatment response in patients with Treatment Resistant Depression (TRD): A systematic review & meta-analysis. Psychiatry Res. 2022, 317, 114857. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar] [CrossRef]
- Hamilton, M. A rating scale for depression. J. Neurol. Neurosurg. Psychiatry 1960, 23, 56–62. [Google Scholar] [CrossRef]
- Voineskos, D.; Daskalakis, Z.J.; Blumberger, D.M. Management of Treatment-Resistant Depression: Challenges and Strategies. Neuropsychiatr Dis. Treat. 2020, 16, 221–234. [Google Scholar] [CrossRef] [PubMed]
- Montgomery, S.A.; Asberg, M. A new depression scale designed to be sensitive to change. Br. J. Psychiatry 1979, 134, 382–389. [Google Scholar] [CrossRef]
- Leucht, S.; Fennema, H.; Engel, R.; Kaspers-Janssen, M.; Lepping, P.; Szegedi, A. What does the HAMD mean? J. Affect. Disord. 2013, 148, 243–248. [Google Scholar] [CrossRef] [PubMed]
- Trivedi, M.H.; Corey-Lisle, P.K.; Guo, Z.; Lennox, R.D.; Pikalov, A.; Kim, E. Remission, response without remission, and nonresponse in major depressive disorder: Impact on functioning. Int. Clin. Psychopharmacol. 2009, 24, 133–138. [Google Scholar] [CrossRef] [PubMed]
- Nobuta, S.; Sato, K.; Nakagawa, T.; Hatori, M.; Itoi, E. Effects of wrist splinting for Carpal Tunnel syndrome and motor nerve conduction measurements. Ups. J. Med. Sci. 2008, 113, 181–192. [Google Scholar] [CrossRef]
- Reddy, M.; Gill, S.S.; Kalkar, S.R.; Wu, W.; Anderson, P.J.; Rochon, P.A. Treatment of pressure ulcers: A systematic review. JAMA 2008, 300, 2647–2662. [Google Scholar] [CrossRef]
- Möller, H.J. Outcomes in major depressive disorder: The evolving concept of remission and its implications for treatment. World J. Biol. Psychiatry 2008, 9, 102–114. [Google Scholar] [CrossRef]
- Hawley, C.J.; Gale, T.M.; Sivakumaran, T.; Hertfordshire Neuroscience Research group. Defining remission by cut off score on the MADRS: Selecting the optimal value. J. Affect. Disord. 2002, 72, 177–184. [Google Scholar] [CrossRef]
- Bürhan-Çavuşoğlu, P.; İscan, E.; Güneş, A.; Atabey, N.; Alkın, T. Increased telomerase activity in major depressive disorder with melancholic features: Possible role of pro-inflammatory cytokines and the brain-derived neurotrophic factor. Brain Behav. Immun. Health 2021, 14, 100259. [Google Scholar] [CrossRef]
- Li, Z.; Zhang, C.; Fan, J.; Yuan, C.; Huang, J.; Chen, J.; Yi, Z.; Wang, Z.; Hong, W.; Wang, Y.; et al. Brain-derived neurotrophic factor levels and bipolar disorder in patients in their first depressive episode: 3-year prospective longitudinal study. Br. J. Psychiatry 2014, 205, 29–35. [Google Scholar] [CrossRef]
- Liu, X.; Li, P.; Ma, X.; Zhang, J.; Sun, X.; Luo, X.; Zhang, Y. Association between plasma levels of BDNF and GDNF and the diagnosis, treatment response in first-episode MDD. J. Affect. Disord. 2022, 315, 190–197. [Google Scholar] [CrossRef]
- Fujii, R.; Watanabe, K.; Okamoto, N.; Natsuyama, T.; Tesen, H.; Igata, R.; Konishi, Y.; Ikenouchi, A.; Kakeda, S.; Yoshimura, R. Hippocampal Volume and Plasma Brain-Derived Neurotrophic Factor Levels in Patients With Depression and Healthy Controls. Front. Mol. Neurosci. 2022, 15, 857293. [Google Scholar] [CrossRef]
- Natsuyama, T.; Okamoto, N.; Watanabe, K.; Chibaatar, E.; Tesen, H.; Hayasaki, G.; Ikenouchi, A.; Kakeda, S.; Yoshimura, R. Gyrification patterns in first-episode, drug-naïve major depression: Associations with plasma levels of brain-derived neurotrophic factor and psychiatric symptoms. Front. Psychiatry 2023, 13, 1031386. [Google Scholar] [CrossRef] [PubMed]
- Lee, B.H.; Kim, H.; Park, S.H.; Kim, Y.K. Decreased plasma BDNF level in depressive patients. J. Affect. Disord. 2007, 101, 239–244. [Google Scholar] [CrossRef] [PubMed]
- Pillai, A.; Kale, A.; Joshi, S.; Naphade, N.; Raju, M.S.; Nasrallah, H.; Mahadik, S.P. Decreased BDNF levels in CSF of drug-naive first-episode psychotic subjects: Correlation with plasma BDNF and psychopathology. Int. J. Neuropsychopharmacol. 2010, 13, 535–539. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.B.; Huang, X.; He, H.B.; Mei, F.; Sun, B.; Zhou, S.M.; Yan, S.; Zheng, W.; Ning, Y. BDNF and the Antidepressant Effects of Ketamine and Propofol in Electroconvulsive Therapy: A Preliminary Study. Neuropsychiatr. Dis. Treat. 2020, 16, 901–908. [Google Scholar] [CrossRef]
- Park, Y.M.; Lee, B.H. Alterations in Serum BDNF and GDNF Levels after 12 Weeks of Antidepressant Treatment in Female Outpatients with Major Depressive Disorder. Psychiatry Investig. 2018, 15, 818–823. [Google Scholar] [CrossRef]
- Falaschi, V.; Palego, L.; Marazziti, D.; Betti, L.; Musetti, L.; Maglio, A.; Dell’Oste, V.; Sagona, S.; Felicioli, A.; Carpita, B. Variation of Circulating Brain-Derived Neurotrophic Factor (BDNF) in Depression: Relationships with Inflammatory Indices, Metabolic Status and Patients’ Clinical Features. Life 2023, 13, 1555. [Google Scholar] [CrossRef]
- Fusar-Poli, L.; Aguglia, A.; Amerio, A.; Orsolini, L.; Salvi, V.; Serafini, G.; Volpe, U.; Amore, M.; Aguglia, E. Peripheral BDNF levels in psychiatric patients with and without a history of suicide attempt: A systematic review and meta-analysis. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 111, 110342. [Google Scholar] [CrossRef]
- Piccinni, A.; Del Debbio, A.; Medda, P.; Bianchi, C.; Roncaglia, I.; Veltri, A.; Zanello, S.; Massimetti, E.; Origlia, N.; Domenici, L.; et al. Plasma Brain-Derived Neurotrophic Factor in treatment-resistant depressed patients receiving electroconvulsive therapy. Eur. Neuropsychopharmacol. 2009, 19, 349–355. [Google Scholar] [CrossRef]
- Brunoni, A.R.; Lopes, M.; Fregni, F. A systematic review and meta-analysis of clinical studies on major depression and BDNF levels: Implications for the role of neuroplasticity in depression. Int. J. Neuropsychopharmacol. 2008, 11, 1169–1180. [Google Scholar] [CrossRef] [PubMed]
- Caliman-Fontes, A.T.; Leal, G.C.; Correia-Melo, F.S.; Paixão, C.S.; Carvalho, M.S.; Jesus-Nunes, A.P.; Vieira, F.; Magnavita, G.; Bandeira, I.D.; Mello, R.P.; et al. Brain-derived neurotrophic factor serum levels following ketamine and esketamine intervention for treatment-resistant depression: Secondary analysis from a randomized trial. Trends Psychiatry Psychother. 2023, 45, e20210298. [Google Scholar] [CrossRef] [PubMed]
- Dvojkovic, A.; Nikolac Perkovic, M.; Sagud, M.; Nedic Erjavec, G.; Mihaljevic Peles, A.; Svob Strac, D.; Vuksan Cusa, B.; Tudor, L.; Kusevic, Z.; Konjevod, M.; et al. Effect of vortioxetine vs. escitalopram on plasma BDNF and platelet serotonin in depressed patients. Prog. Neuropsychopharmacol. Biol. Psychiatry 2021, 105, 110016. [Google Scholar] [CrossRef] [PubMed]
- Min, X.; Wang, G.; Cui, Y.; Meng, P.; Hu, X.; Liu, S.; Wang, Y. Association between inflammatory cytokines and symptoms of major depressive disorder in adults. Front. Immunol. 2023, 14, 1110775. [Google Scholar] [CrossRef] [PubMed]
- Nikolac Perkovic, M.; Sagud, M.; Tudor, L.; Konjevod, M.; Svob Strac, D.; Pivac, N. A Load to Find Clinically Useful Biomarkers for Depression. Adv. Exp. Med. Biol. 2021, 1305, 175–202. [Google Scholar] [CrossRef]
- Yoshimura, R.; Sugita-Ikenouchi, A.; Hori, H.; Umene-Nakano, W.; Hayashi, K.; Katsuki, A.; Ueda, N.; Nakamura, J. A close correlation between plasma and serum levels of brain-derived neurotrophic factor (BDNF) in healthy volunteers. Int. J. Psychiatry Clin. Pract. 2010, 14, 220–222. [Google Scholar] [CrossRef]
- Kudlek Mikulic, S.; Mihaljevic-Peles, A.; Sagud, M.; Bajs Janovic, M.; Ganoci, L.; Grubisin, J.; Kuzman Rojnic, M.; Vuksan Cusa, B.; Bradaš, Z.; Božina, N. Brain-derived neurotrophic factor serum and plasma levels in the treatment of acute schizophrenia with olanzapine or risperidone: 6-week prospective study. Nord. J. Psychiatry 2017, 71, 513–520. [Google Scholar] [CrossRef]
- Vanicek, T.; Kranz, G.S.; Vyssoki, B.; Fugger, G.; Komorowski, A.; Höflich, A.; Saumer, G.; Milovic, S.; Lanzenberger, R.; Eckert, A.; et al. Acute and subsequent continuation electroconvulsive therapy elevates serum BDNF levels in patients with major depression. Brain Stimul. 2019, 12, 1041–1050. [Google Scholar] [CrossRef]
- Haile, C.N.; Murrough, J.W.; Iosifescu, D.V.; Chang, L.C.; Al Jurdi, R.K.; Foulkes, A.; Iqbal, S.; Mahoney, J.J., 3rd; De La Garza, R., 2nd; Charney, D.S.; et al. Plasma brain derived neurotrophic factor (BDNF) and response to ketamine in treatment-resistant depression. Int. J. Neuropsychopharmacol. 2014, 17, 331–336. [Google Scholar] [CrossRef]
- Yoshimura, R.; Ikenouchi-Sugita, A.; Hori, H.; Umene-Nakano, W.; Katsuki, A.; Hayashi, K.; Ueda, N.; Nakamura, J. Adding a low dose atypical antipsychotic drug to an antidepressant induced a rapid increase of plasma brain-derived neurotrophic factor levels in patients with treatment-resistant depression. Prog. Neuropsychopharmacol. Biol. Psychiatry 2010, 34, 308–312. [Google Scholar] [CrossRef]
- Yukimasa, T.; Yoshimura, R.; Tamagawa, A.; Uozumi, T.; Shinkai, K.; Ueda, N.; Tsuji, S.; Nakamura, J. High-frequency repetitive transcranial magnetic stimulation improves refractory depression by influencing catecholamine and brain-derived neurotrophic factors. Pharmacopsychiatry 2006, 39, 52–59. [Google Scholar] [CrossRef]
- Carspecken, C.W.; Borisovskaya, A.; Lan, S.T.; Heller, K.; Buchholz, J.; Ruskin, D.; Rozet, I. Ketamine Anesthesia Does Not Improve Depression Scores in Electroconvulsive Therapy: A Randomized Clinical Trial. J. Neurosurg. Anesthesiol. 2018, 30, 305–313. [Google Scholar] [CrossRef] [PubMed]
- Jiang, H.; Veldman, E.R.; Tiger, M.; Ekman, C.J.; Lundberg, J.; Svenningsson, P. Plasma Levels of Brain-Derived Neurotrophic Factor and S100B in Relation to Antidepressant Response to Ketamine. Front. Neurosci. 2021, 15, 698633. [Google Scholar] [CrossRef]
- Lin, C.H.; Chen, M.C.; Lee, W.K.; Chen, C.C.; Huang, C.H.; Lane, H.Y. Electroconvulsive therapy improves clinical manifestation with plasma BDNF levels unchanged in treatment-resistant depression patients. Neuropsychobiology 2013, 68, 110–115. [Google Scholar] [CrossRef] [PubMed]
- Psomiades, M.; Mondino, M.; Galvão, F.; Mandairon, N.; Nourredine, M.; Suaud-Chagny, M.F.; Brunelin, J. Serum Mature BDNF Level Is Associated with Remission Following ECT in Treatment-Resistant Depression. Brain Sci. 2022, 12, 126. [Google Scholar] [CrossRef] [PubMed]
- Zhou, B.; Wang, Z.; Zhu, L.; Huang, G.; Li, B.; Chen, C.; Huang, J.; Ma, F.; Liu, T.C. Effects of different physical activities on brain-derived neurotrophic factor: A systematic review and bayesian network meta-analysis. Front. Aging Neurosci. 2022, 14, 981002. [Google Scholar] [CrossRef]
- Soler, J.E.; Robison, A.J.; Núñez, A.A.; Yan, L. Light modulates hippocampal function and spatial learning in a diurnal rodent species: A study using male nile grass rat (Arvicanthis niloticus). Hippocampus 2018, 28, 189–200. [Google Scholar] [CrossRef]
- Shang, M.; Zhang, J.; Shen, M.; Sun, Z.; Gao, P.; Li, J.; Xing, J.; Guo, G. Bright light exposure induces dynamic changes of spatial memory in nocturnal rodents. Brain Res. Bull. 2021, 174, 389–399. [Google Scholar] [CrossRef]
- Gadad, B.S.; Vargas-Medrano, J.; Ramos, E.I.; Najera, K.; Fagan, M.; Forero, A.; Thompson, P.M. Altered levels of interleukins and neurotrophic growth factors in mood disorders and suicidality: An analysis from periphery to central nervous system. Transl. Psychiatry 2021, 11, 341. [Google Scholar] [CrossRef]
- Iu, E.C.Y.; Chan, C.B. Is Brain-Derived Neurotrophic Factor a Metabolic Hormone in Peripheral Tissues? Biology 2022, 11, 1063. [Google Scholar] [CrossRef]
- Jones, B.D.M.; Razza, L.B.; Weissman, C.R.; Karbi, J.; Vine, T.; Mulsant, L.S.; Brunoni, A.R.; Husain, M.I.; Mulsant, B.H.; Blumberger, D.M.; et al. Magnitude of the Placebo Response Across Treatment Modalities Used for Treatment-Resistant Depression in Adults: A Systematic Review and Meta-analysis. JAMA Netw. Open 2021, 4, e2125531. [Google Scholar] [CrossRef]
- Pillai, A.; Bruno, D.; Sarreal, A.S.; Hernando, R.T.; Saint-Louis, L.A.; Nierenberg, J.; Ginsberg, S.D.; Pomara, N.; Mehta, P.D.; Zetterberg, H.; et al. Plasma BDNF levels vary in relation to body weight in females. PLoS ONE 2012, 7, e39358. [Google Scholar] [CrossRef]
- Chen, L.; Li, X.S.; Zheng, G.E.; Xie, G.J.; Cheng, Y. Peripheral blood BDNF-TrkB signaling in first-episode, drug-free patients with major depressive disorder and schizophrenia. Neurosci. Lett. 2020, 714, 134618. [Google Scholar] [CrossRef] [PubMed]
- Piccinni, A.; Marazziti, D.; Del Debbio, A.; Bianchi, C.; Roncaglia, I.; Mannari, C.; Origlia, N.; Catena Dell’Osso, M.; Massimetti, G.; Domenici, L.; et al. Diurnal variation of plasma brain-derived neurotrophic factor (BDNF) in humans: An analysis of sex differences. Chronobiol. Int. 2008, 25, 819–826. [Google Scholar] [CrossRef] [PubMed]
- Hashimoto, K. Ethnic differences in the serum levels of proBDNF, a precursor of brain-derived neurotrophic factor (BDNF), in mood disorders. Eur. Arch. Psychiatry Clin. Neurosci. 2016, 266, 285–287. [Google Scholar] [CrossRef] [PubMed]
- Moeller, S.B.; Gbyl, K.; Hjorthøj, C.; Andreasen, M.; Austin, S.F.; Buchholtz, P.E.; Fønss, L.; Hjerrild, S.; Hogervorst, L.; Jørgensen, M.B.; et al. Treatment of difficult-to-treat depression—Clinical guideline for selected interventions. Nord. J. Psychiatry 2022, 76, 177–188. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Assessments | HC at Baseline | First Episode at Baseline | Recurrent Episode at Baseline | TRD at Baseline | TRD after 4 Weeks of BLT |
|---|---|---|---|---|---|
| Structured clinical interview | x | ||||
| HAMD-17, MADRS | x | x | |||
| Plasma BDNF concentration | x | x | x | x | x |
| HC (N = 71) | First Episode (N = 55) | Recurrent Episode (N = 25) | TRD (N = 54) | Statistics | |
|---|---|---|---|---|---|
| Smokers (%) | 33.3 | 29.1 | 28.0 | 38.9 | χ2 = 13.18; p = 0.001 |
| Positive family history (%) | NA | 33.3 | 24.0 | 38.9 | χ2 = 1.70; p = 0.427 |
| The presence of life-time suicide attempts (%) | NA | 3.6 | 8.0 | 9.3 | χ2 = 1.46; p = 0.483 |
| Age (years, median, min–max) | 58 (37–68) | 45 (19–67) | 54 (19–78) | 53 (21–69) | H = 21.61; p < 0.001 |
| HAMD-17 scores (median, min–max) | NA | 22 (17–37) | 23 (17–32) | 21 (16–27) | H = 2.80; p = 0.246 |
| MADRS scores (median, min–max) | NA | 25 (17–42) | 27 (20–51) | 27 (19–36) | H = 1.97; p = 0.373 |
| TRD | Wilcoxon Test | |||
|---|---|---|---|---|
| Before Phototherapy | After 4 Weeks of Phototherapy | Z | p | |
| HAMD-17 scores | 21 (16–27) | 10 (3–17) | 6.41 | <0.001 |
| MADRS scores | 27 (19–36) | 13 (4–21) | 6.40 | <0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kosanovic Rajacic, B.; Sagud, M.; Begic, D.; Nikolac Perkovic, M.; Dvojkovic, A.; Ganoci, L.; Pivac, N. Plasma Brain-Derived Neurotrophic Factor Levels in First-Episode and Recurrent Major Depression and before and after Bright Light Therapy in Treatment-Resistant Depression. Biomolecules 2023, 13, 1425. https://doi.org/10.3390/biom13091425
Kosanovic Rajacic B, Sagud M, Begic D, Nikolac Perkovic M, Dvojkovic A, Ganoci L, Pivac N. Plasma Brain-Derived Neurotrophic Factor Levels in First-Episode and Recurrent Major Depression and before and after Bright Light Therapy in Treatment-Resistant Depression. Biomolecules. 2023; 13(9):1425. https://doi.org/10.3390/biom13091425
Chicago/Turabian StyleKosanovic Rajacic, Biljana, Marina Sagud, Drazen Begic, Matea Nikolac Perkovic, Anja Dvojkovic, Lana Ganoci, and Nela Pivac. 2023. "Plasma Brain-Derived Neurotrophic Factor Levels in First-Episode and Recurrent Major Depression and before and after Bright Light Therapy in Treatment-Resistant Depression" Biomolecules 13, no. 9: 1425. https://doi.org/10.3390/biom13091425
APA StyleKosanovic Rajacic, B., Sagud, M., Begic, D., Nikolac Perkovic, M., Dvojkovic, A., Ganoci, L., & Pivac, N. (2023). Plasma Brain-Derived Neurotrophic Factor Levels in First-Episode and Recurrent Major Depression and before and after Bright Light Therapy in Treatment-Resistant Depression. Biomolecules, 13(9), 1425. https://doi.org/10.3390/biom13091425