1. Introduction
Posterior capsule opacification (PCO) is a condition that develops in as many as 50% of cases following surgery for senile cataract, the most common cause of lens opacification [
1]. PCO develops from a process of epithelial-to-mesenchymal transition (EMT) of lens epithelial cells left behind after surgical removal of the cataractous lens, either through phacoemulsification or bulk removal of the lens mass mediated by hydrodissection. After going through EMT, lens epithelial cells deposit extracellular matrix components that cause contraction, wrinkling of the lens capsule, and interruption of the light path that would otherwise focus on the retina to stimulate photoreceptors. Restoration of a clear light path can be achieved by creating a capsulotomy with use of a Nd:YAG laser. While the YAG procedure is usually successful and uneventful, eyes with such capsulotomies are at higher risk for retinal detachment, cystoid macular edema, and increased ocular pressures [
2]. Therefore, academic and industry teams are actively working to develop therapeutic agents to reduce the need for YAG therapy.
Many studies have shown that growth factors such as TGF-β play an important role in regulating the development of PCO [
3]. Studies have demonstrated in cell culture and preclinical animal models that inhibitors of TGF-β signaling can suppress EMT and changes in lens epithelial cells involved in PCO [
4,
5,
6]. In the ideal case, such inhibitors would be deposited into the lens capsular bag at the time of surgery and inhibit TGF-β signaling either acutely or in an extended time-dependent fashion through slow release from a drug depot fabricated from nanogel materials.
In the current study, we created a nanogel-based drug delivery matrix to slowly release a small molecule PCO inhibitor into the capsular bag in a mouse cataract model. Profiling of the post-surgical mouse eye showed that the drug delivery device was capable of delivering amounts of the PCO inhibitor sufficient to suppress markers of PCO over a 5-day period. These results suggest that nanogel-facilitated delivery of therapeutic agents into the postsurgical lens capsule may provide an effective means to delay or prevent development of PCO.
2. Materials and Methods
2.1. Materials
2-Hydroxethyl acrylate (HEA) 96%, 2,2′-azobis(2-methylpropionitrile) (AIBN) 98%, and 2-hydroxyethyl methacrylate (HEMA) were all obtained from Sigma-Aldrich (St. Louis, MO, USA). Tetraethylene glycol dimethacrylate (TTEGDMA-pure grade with MEHQ) and urethane dimethacrylate (UDMA) were both purchased from Esstech Inc. (Essington, PA, USA), whereas acrylic acid (AA) > 99.0% was purchased from Tokyo Chemical Industry Co., Ltd. (Tokyo, Japan). 2-mercaptoethanol (ME) 99% was purchased from Acros Organics (Fair Lawn, NJ, USA). Ebecryl 270™ (EB270) and Genocure* LTM were kindly donated by Allnex (Alpharetta, GA, USA) and RAHN USA Corp. (Aurora, IL, USA), respectively, and all solvents used were obtained from Fisher.
2.2. Synthesis of Nanogel
A previously published synthetic protocol was adapted for synthesis of the nanogel [
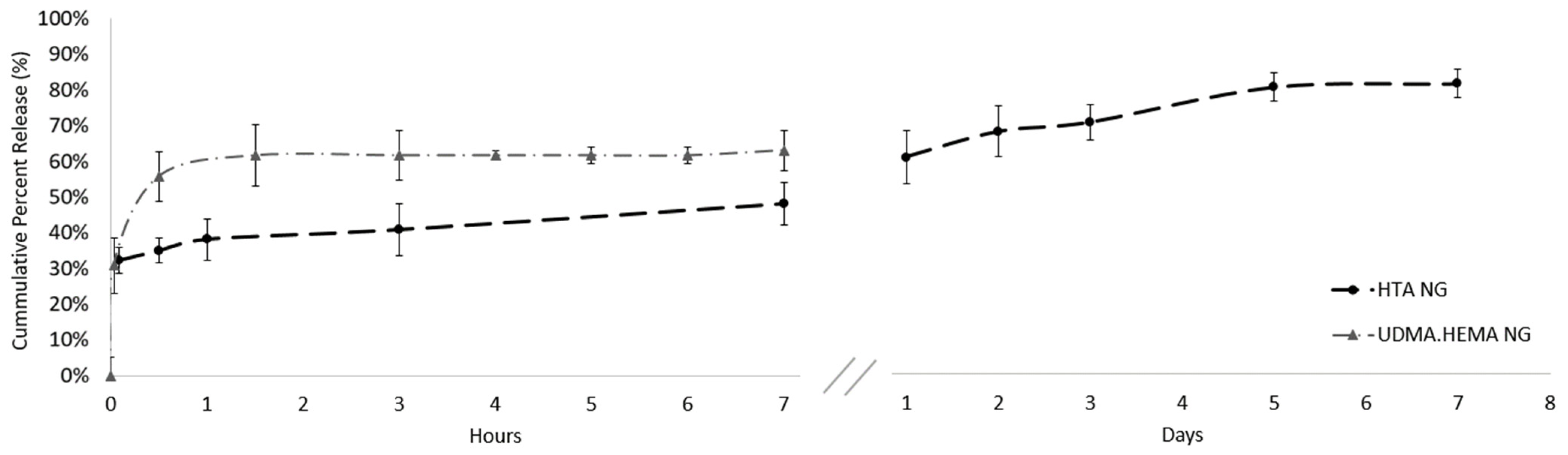
7]. Briefly, a 60:20:20 molar ratio of HEA:TTEGDMA:AA using 15 mol % of ME as a chain transfer agent was initially synthesized herein denoted as HTA NG. Next, 1 wt.% of the thermal initiator 2,2′-azobis(2-methylpropionitrile) (AIBN) was added and stirred at 200 RPM (80 °C) using 4× methyl ethyl ketone (MEK) as the solvent and stopped at 70% conversion. The double bond conversion of the acrylate groups was monitored via FTIR spectroscopy (mid-IR, 814 cm
−1). Once the 70% double-bond conversion was achieved the nanogel was terminated by precipitating in 10-fold excess hexanes. Subsequently, the nanogel was dispersed in dichloromethane and a stoichiometric quantity of ME was added to the nanogels such that 20% of the remaining double-bonds could undergo a thiol-Michael reaction. The reaction would provide the nanogels with OH functionality on the surface, thereby increasing their hydrophilicity while still retaining residual acrylates which could enable the nanogels to covalently link onto a substrate. Any residual solvent was then removed completely via a rotary evaporator until a gel-like NG was achieved.
The molecular weight and size of the NG was analyzed via the Viscoteck-270 gel permeation chromatograph (GPC) with tetrahydrofuran (THF) (0.35 μL/min) as the mobile phase.
2.3. Eb270/HEA Substrate Fabrication
For benchtop experiments, circular substrates of 6 mm in diameter and 1 mm in thickness were fabricated by casting a 2:1 weight ratio of Eb270:HEA into silicon molds and photopolymerizing them at room temperature. The samples were clamped between two glass slides that were cured with a broad spectra lamp (365–600 nm, 36 W/cm2) using 1 wt.% Genocure* LTM as the photo initiator. Substrates used for in vivo testing were fabricated with dimensions of 1 mm in diameter by 0.5 mm in thickness using the same method described above.
The modulus of elasticity of the IOL before and after the coating was placed was characterized on a Materials Testing System (MiniBionix II, MTS, Eden Prairie, MN, USA) by generating stress-strain graphs. Bar specimens (25 mm × 2 mm × 2 mm, n = 5) of the polymerized IOL with and without the coating were subject to flexural loading using a 100 N load cell at a rate of 1 mm/min and the modulus of elasticity was calculated.
2.4. Encapsulating Sorbinil in Nanogels
A 2 mg/mL Sorbinil solution was prepared by sonicating 10 mg of Sorbinil with 0.75 mL of 0.1 M NaOH until dissolved completely. Next, 4 mL of phosphate-buffered saline was added to solution and then separated into 1 mL aliquots. When ready to use, samples were thawed via sonication and 10 uL of 0.1 M HCL was added to the 1 mL aliquot.
A 1:2 w/v of the nanogel was dispersed in the Sorbinil solution described above and incubated overnight at ambient temperature. The mixture was centrifuged with a centrifugal concentrator (MWCO 10 kDa, polyether sulfone membrane) at 4300 RPM followed by a Milli-Q wash. The filtrate was collected and diluted from this sample where the encapsulation efficiency of the nanogel was then calculated given the following equation:
The optical clarity of the Sorbinil-encapsulated nanogel was studied via UV-Visible spectroscopy on a 96-well plate using Biotek Synergy 4 microplate reader (BioTek Instruments, Inc., Winooski, VT, USA), in which 3 µL of the Sorbinil-encapsulated nanogel was added in each well plate well (n = 3) to confirm Sorbinil was encapsulated and no absorbace was detected in the visible region (400–700 nm).
2.5. Drug Elution from NG Devices
To measure Sorbinil release from the HTA NG, 3 µL of the Sorbinil-loaded NG was spin coated on top of the benchtop substrates then cured with a broad spectra lamp (365–600 nm, 36 W/cm2) using 0.1 wt.% Genocure *LTM as the photo initiator. To monitor drug release, coated substrates were submerged in a 10 mL 1×-PBS reservoir at 24 °C. For each reading, 1 mL samples were collected from the reservoir at 30 min, 1 h, 3 h, 7 h, and 1, 2, 3, 5, and 7 days. This benchtop study was designed to baseline the maximum amount of Sorbinil that could be removed from the nanogels into the reservoir via diffusion, therefore the reservoir (10 mL) was replaced at the 7 h mark and subsequently at days 1, 2, 3, 5, and 7. Additionally, the reservoir was stirred at 100 RPM to expedite the removal of Sorbinil from the nanogels. Sorbinil was detected by measuring absorbance of 280 nm light. The readings were then normalized relative to the theoretical maximum concentration of Sorbinil released given by that encapsulation efficiency calculated earlier.
2.6. Sterile Sample Preparation
Substrates were sterilized in an autoclave (Tuttnauer, 2540 M-B/L Heiddolph, Alexander, AK, USA) at 265 °F for one hour followed by a dry cycle at the same temperature and duration. Then, 1 µL of the Sorbinil loaded NGs, filter sterilized using a Celltreat 0.22 µm filter (Pepperell, MA, USA), was pipetted on top of the substrate and cured with a broad spectra lamp (365–600 nm, 36 W/cm2) using 0.1 wt.% Genocure *LTM as the photo initiator. Samples were prepared 24 h before surgery.
2.7. Mouse PCO Model
For animal studies of PCO, we utilized our previously published mouse model wherein a transgene encoding human aldose reductase (AKR1B1) accelerates the onset and progression of PCO following lens extraction [
6,
8]. Animals were anesthetized using 90 mg/kg ketamine (VetOne, Cambridge, ON, Canada) and 10 mg/Kg xylazine (VetOne, Cambridge, ON, Canada), and given 1 mg/kg buprenorphine SR (ZooPharm, Laramie, WY, USA). The pupils were then dilated with one eye drop of 0.2% tropicamide (Akron, Lake Forest, IL, USA), 0.5% phenylephrine (Akron, Lake Forest, IL, USA), and the cornea anesthetized with one drop of ophthalmic proparacaine (Alcon, Geneva, Switzerland) and 5% ophthalmic betadine (Alcon, Geneva, Switzerland). Extra capsular lens extraction (ECLE) was performed by making an incision through the cornea and the lens capsule using a 1 mm slit scalpel (Alcon, Geneva, Switzerland) followed by hydrodissection of the lens fiber mass using saline in a 5 mL syringe with a bent cannula (Alcon, Geneva, Switzerland). For animals that received EB270:HEA substrates, nanogel loaded with or without Sorbinil combinations was placed through the anterior chamber into the lens capsule. The anterior chamber volume was restored using viscoat (Alcon, Geneva, Switzerland) if needed and the cornea opening was sealed using Resure™ (Ocular Therapeutix, Bedford, MA, USA). A drop of dexamethasone, polymyxin B, and neomycin ophthalmic gel (Bausch and Lomb, Bridgewater, NJ, USA) was placed over the corneal incision. The animals recovered for 5 days before imaging, then the lens capsule was recovered for RNA analysis or the whole eye fixed for immunohistochemistry studies.
2.8. Histology
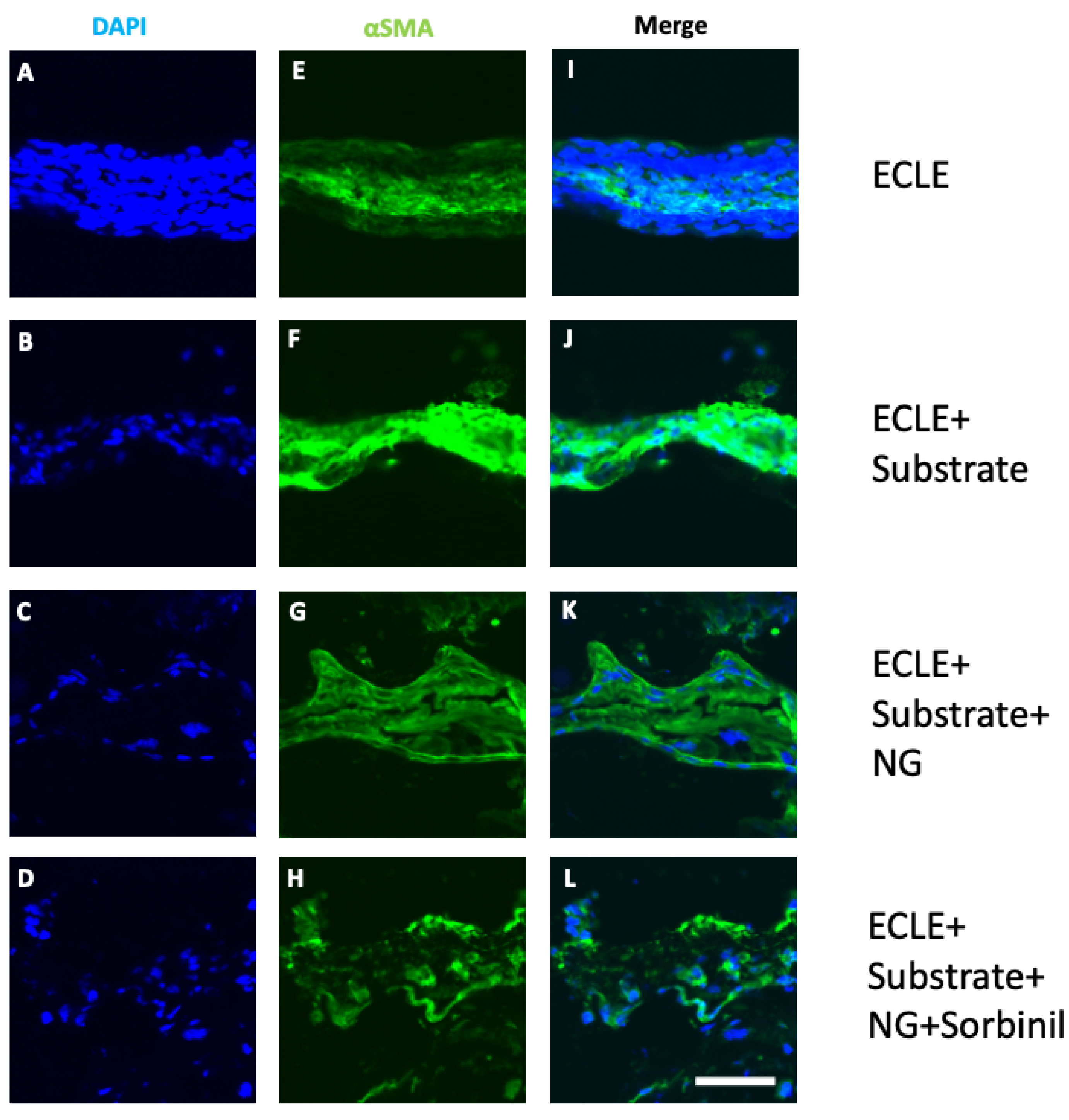
Whole eyes were fixed in 4% paraformaldehyde for 10 min at 4 °C followed by 4 h per each sucrose (Sigma, St. Louis, MO, USA) gradient 10%, 20%, 30%, and then frozen into optimal cutting temperature (OCT, Tissue Tek, Torrance, CA, USA). The sections were stained with 1:500-diluted αSMA A488 antiserum (Abcam, ab202295, Cambridge, MA, USA) in 1% BSA (Sigma, St. Louis, MO, USA) and 0.1% Tween 20 (Fisher, Waltham, MA, USA) in saline for 1 h at room temperature. The slides were then washed and counter-stained with fluoromount (Fisher, Waltham, MA, USA) containing DAPI. They were imaged on a Nikon Eclipse Ti confocal microscope (Nikon, Tokyo, Japan).
2.9. qRT-PCR
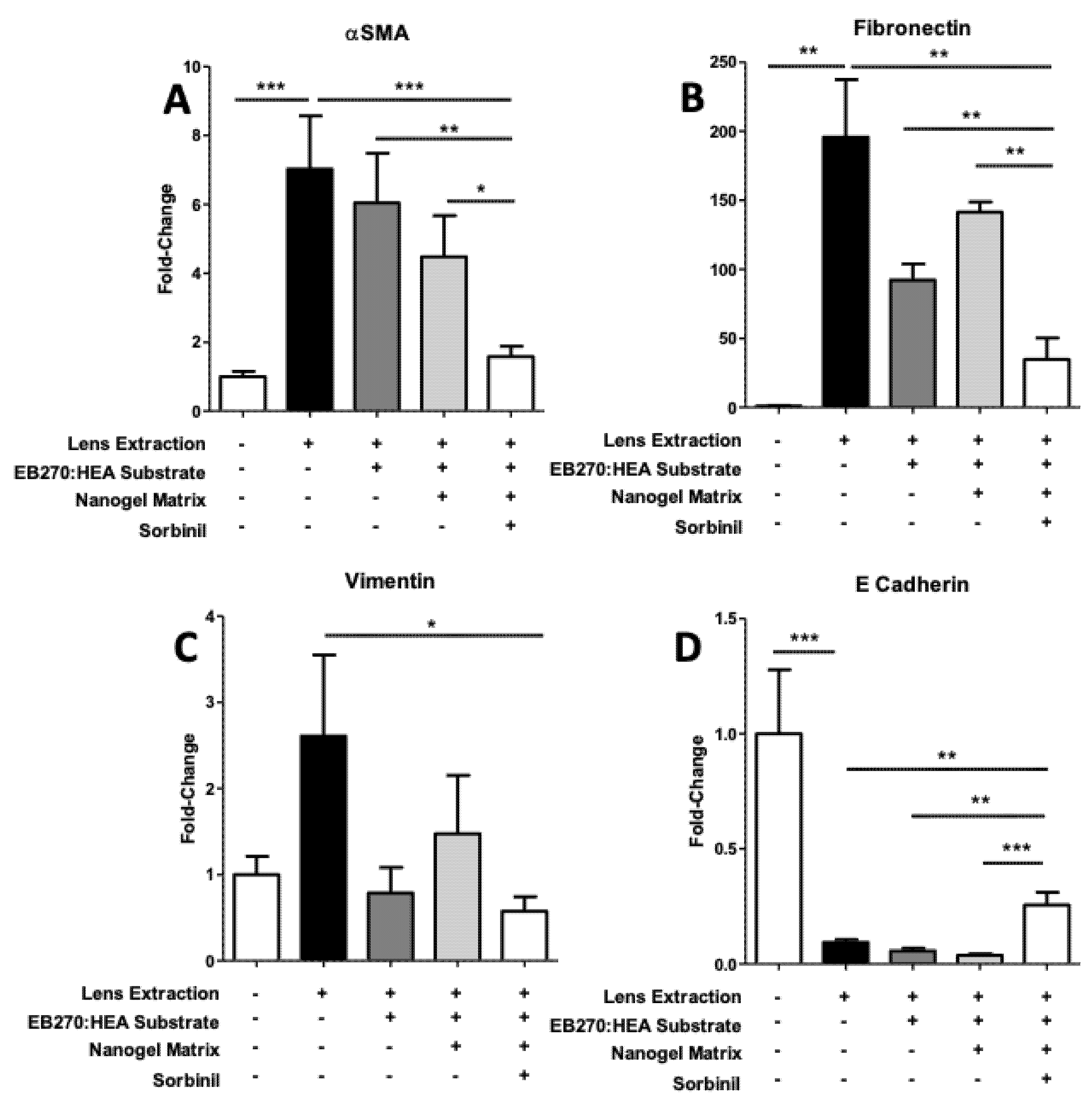
RNA was extracted from the lens capsule which was placed into 500 µL Qiazol (Qiagen, Austin, TX, USA):100 µL chloroform which was immediately frozen to −80 °C following extraction using RNeasy micro kit (Qiagen, Austin, TX, USA) according to the manufacturer’s instructions. Complimentary DNA was created using iScript reverse transcription supermix for qRT-PCR (Biorad, Hercules, CA, USA) and the qPCR was performed with iTaq Universal SYBR green supermix (Biorad, Hercules, CA, USA). We used four sets of primers (Integrated DNA Technologies, Coralville, IA, USA) for gene expression markers of EMT αSMA, fibronectin, vimentin, and E-cadherin, and GAPDH was used as the internal ubiquitous control. The primer sequences are listed in
Table 1. Reactions were performed in triplicate using the CFX (Biorad, Hercules, CA, USA).
2.10. Statistical Analysis
Statistical analysis was performed using GraphPad Prism software 5.03 (GraphPad Software, La Jolla, CA, USA). Power calculations to estimate sample sizes to achieve 95% confidence intervals carried a maximum error of 4.615.
4. Discussion
Cataracts are responsible for almost 11 million cases of blindness and 35 million cases of visual impairment worldwide [
10]. The surgical treatment of cataracts involves removal of the cloudy lens mass and usually replacement of the native lens with an artificial device called an intraocular lens (IOL). While this procedure is usually safe and uneventful, in up to 30% of cases, and even more depending on time, patients develop a secondary cataract called posterior capsule opacification (PCO), which causes visual impairment [
11]. Removal of the secondary cataract and restoration of the visual light path is most often accomplished with Nd:YAG laser capsulotomy. Because YAG laser adds expense and potential complications such as secondary glaucoma, macular edema, and retinal detachment [
12], there is considerable need to prevent PCO in the first place.
PCO develops as a result of epithelial-to-mesenchymal transition (EMT) of lens epithelial cells that remain adherent to the lens capsule following cataract extraction [
3]. TGF-β is thought to be a key regulator of PCO through its role in signaling downstream from its cell surface receptor to SMAD proteins [
13,
14,
15]. While strategies to prevent PCO have focused on signaling pathways as well as structural parameters of intraocular lenses, we still do not have sufficiently durable treatments to overcome the inexorable drive of lens epithelial cells to undergo EMT and cause visual impairment in the post-cataract patient [
16]. A major unanswered question is whether blockade of the EMT process that underlies PCO, if limited as in the present study to the acute period immediately following cataract removal, will be sufficient to prevent PCO at later times. This question will be addressed in animal studies to be carried out in the future.
Our previous studies identified aldose reductase (AR), an aldo-keto reductase thoroughly studied as a catalyst of sorbitol production in diabetes [
17], as a key player in regulating PCO [
5,
6,
8,
17]. Unlike in humans, mouse lenses contain very low levels of aldose reductase [
18]. To make a mouse model more relevant to human cataract, we cloned the human gene encoding aldose reductase into mice and demonstrated that such mice are at higher risk for cataracts [
19]. We hypothesize that elevation of AR using the transgenic approach resulted in a more human-like induction of EMT markers following the mock cataract procedure, and such changes represent measurable and meaningful indices for discovery of agents to prevent or delay PCO in humans.
Small, orally active AR inhibitors such as Sorbinil substantially prevent EMT of lens epithelial cells following cataract surgery in mice [
6]. In addition, intraocular deposition of a protein biologic derived from the inhibitory SMAD7 also shows promise against PCO [
20]. In both cases, little is known yet about the width of the therapeutic window necessary to achieve efficacy against PCO pathogenesis. Assuming lens epithelial cells may develop a fibrotic response long after exposure to the inducing effects of TGF-β [
21], it seems reasonable to assume that blockade of PCO development in human patients may require delivery of therapeutic agents over an extended period of time. Our previous studies demonstrated that systemic delivery of Sorbinil suppressed expression of EMT markers associated with fibrotic PCO but did not affect the expression of proteins typical of lens fiber cells thought to be responsible for pearl-type PCO [
6]. Future studies will be needed to address the impact of nanogel-delivered inhibitors on the expression of markers for both fibrotic and pearl-type PCO at longer times following lens extraction in our mouse model.
While topical drug delivery accounts for approximately 90% of aqueous ophthalmic formulations, the biggest disadvantages include limited drug concentration and the barrier function of the cornea [
22,
23]. For these reasons, it would be beneficial to develop an effective system that can deliver therapeutic doses of a PCO-inhibiting molecule to the lens, which occupies space within the center of the eye and is separated from the ocular surface by several tissue and aqueous compartments. Many investigators have proposed using an IOL as a substrate to coat with drug-eluting materials. However, coating the nonrefractive IOL surfaces with drug formulations could alter the inherent properties of the IOL and introduce unacceptably complex manufacturing bottlenecks. Some early IOL-eluting prototypes have shown limited drug delivery windows of approximately 12 h [
24]. Other methods, such as the addition of drug releasing capsular tension rings, have proven to be problematic, as the membrane-controlled system has risk of ruptures leading to acute toxicity when large quantities of drugs possibly burst into the eye [
25]. For our studies, we considered it desirable to derive a mouse eye-sized piece of clinical IOL for coating rather than the IOL-mimic substrate used in our studies. Unfortunately, it was not possible to produce IOL fragments of a consistent size and shape which would be needed for coating and implantation in the mouse eye. Our workaround was to design a mouse-sized IOL-like substrate for our in vivo studies. Briefly, circular IOL substrates of 1 mm in diameter and 0.5 mm in thickness were generated. Subsequently, nanogel-coated IOLs were obtained when 1 uL of the Sorbinil-eluting nanogel was polymerized on the surface of the IOL substrates for the in vivo mouse studies. It is important to point out that the IOL mimic formulated for this proof-of-concept study was designed to demonstrate the feasibility of this approach to deliver an inhibitor and not to design an IOL with the intended refractive power. While drug-eluting contact lenses and intraocular lenses have been gaining significance over the past decade, to the best of our knowledge, the current study is unique in focusing on drug-eluting IOLs in which the drug-delivery carrier is a sub 10 nm pre-loaded nanogel that is covalently linked to the surface of IOL. The presence of Sorbinil within nanogel-based coatings in IOLs is also novel and has not been previously studied.
In terms of flexibility and hydrophilic nature, the EB270/HEA substrate utilized in our animal studies was designed to be similar to a typical IOL on the market but scaled to be suitable for implantation in the mouse lens capsular bag (approximately 1 mm diameter). Furthermore, since the substrate was not designed with a refractive function as would be expected for a device providing long term correction of visual acuity, we did not assess whether the materials have significant ocular toxicity. The water contact angle of the EB270/HEA substrate was measured to be 59.1 ± 3.9 degrees, showing that this substrate is clearly hydrophilic. While hydrophilic IOLs and hydrophobic IOLs perform the same, hydrophobic substrates have a higher tendency to adsorb extracellular matrix proteins and inflammatory cells which may lead to other complications. For these reasons, we chose to focus on hydrophilic substrates for our model system [
26]. Our nanoscale surface coating has been shown to not affect the inherent properties of the substrate and simply provide one week of sustained release. Further studies will be required to determine the duration and boundaries of the therapeutic window for PCO prevention and thus the requirements for delivery of PCO inhibitors. Ultimately, our goal is to develop a means to effect sustained release of inhibitor so as to remove the need for multiple surgeries. As the burden of cataracts will continue to increase in parallel with increases in the aged population worldwide, so will the need for effective measures to prevent vision loss due to PCO. Further studies underway will hopefully help to bridge the gap between intraocular drug delivery technology and this unmet clinical need.








{kind=link}
{kind=link}
{kind=link}
{kind=link}