
Serum Osteopontin and Procollagen Type 1 N-Terminal Propeptide Concentrations: Links to Liver Function, Muscle Mass, and Bone Mineral Density in MASLD and Hypertension

 , and
, and
Abstract
1. Introduction
2. Materials and Methods
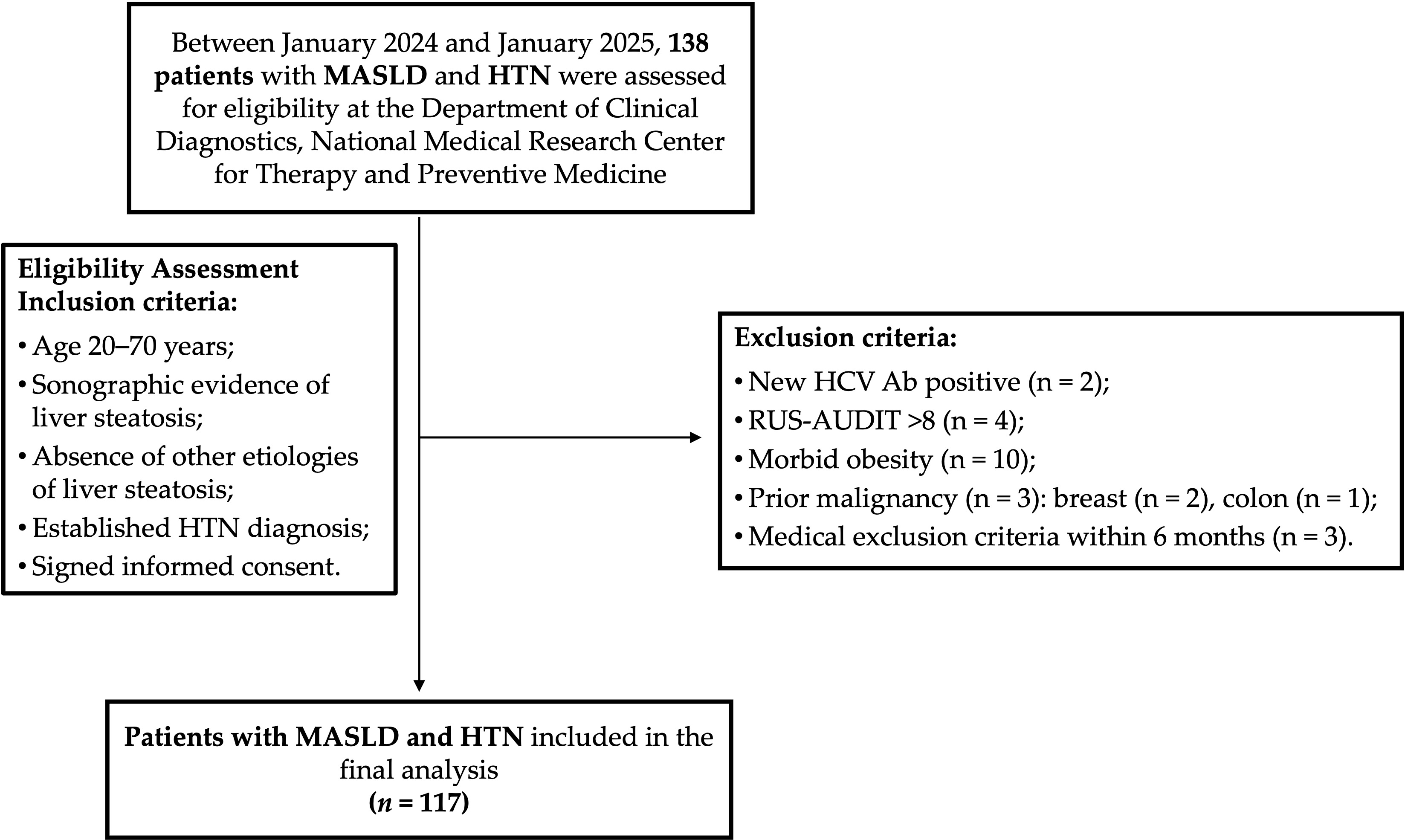
2.1. Patients
- •
- Inclusion criteria:
- ○
- Age 20–70 years.
- ○
- Sonographic evidence of liver steatosis.
- ○
- Absence of other causes of liver steatosis.
- ○
- Established diagnosis of HTN.
- ○
- Signed informed consent.
2.2. Diagnosis of Metabolic Dysfunction-Associated Steatotic Liver Disease and Hypertension
2.3. Anthropometric Measurements
2.4. Skeletal Muscle Mass and Bone Mineral Density Assessment
2.5. Muscle Strength Assessment
2.6. Quantification of Serum Osteopontin and Procollagen Type 1 N-Terminal Propeptide
2.7. Statistical Analysis
3. Results
3.1. Patient Characteristics

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Antihypertensive Drug Class | Number of Patients with MASLD and HTN, n (%) |
|---|---|
| Calcium channel blockers | 3.0 (2.6) |
| Beta blockers | 9.0 (7.7) |
| Angiotensin receptor blockers | 11.0 (9.4) |
| ACE inhibitors | 8.0 (6.8) |
| Combination antihypertensive therapy | 48 (41) |
3.2. Assessment of Serum Osteopontin and Procollagen Type 1 N-Terminal Propeptide Concentrations in Patients with Metabolic Dysfunction-Associated Steatotic Liver Disease and Hypertension
3.2.1. Correlation Analysis
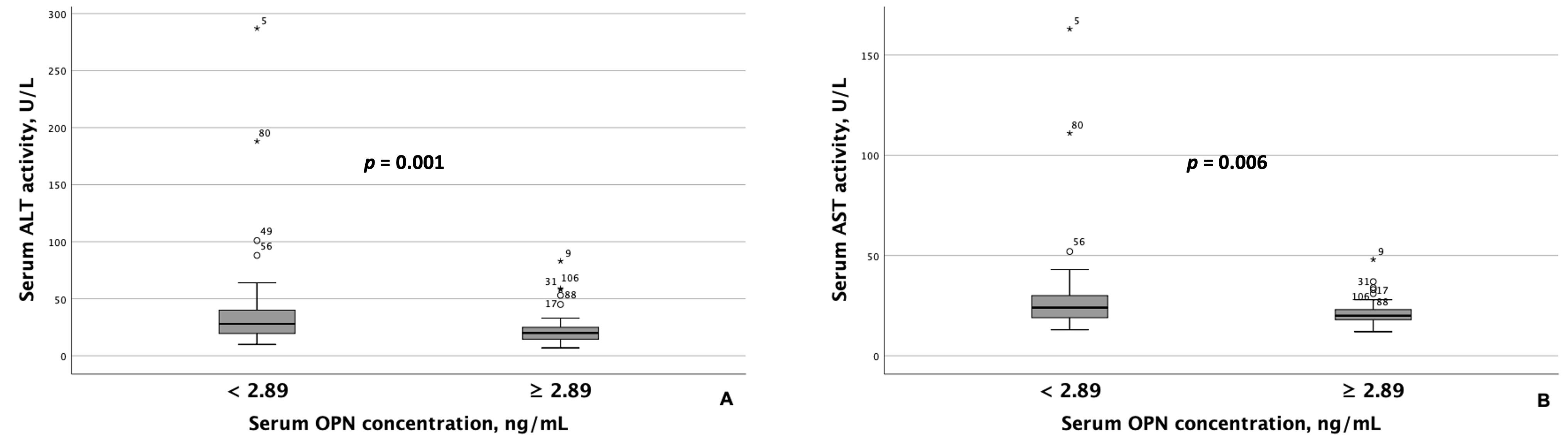
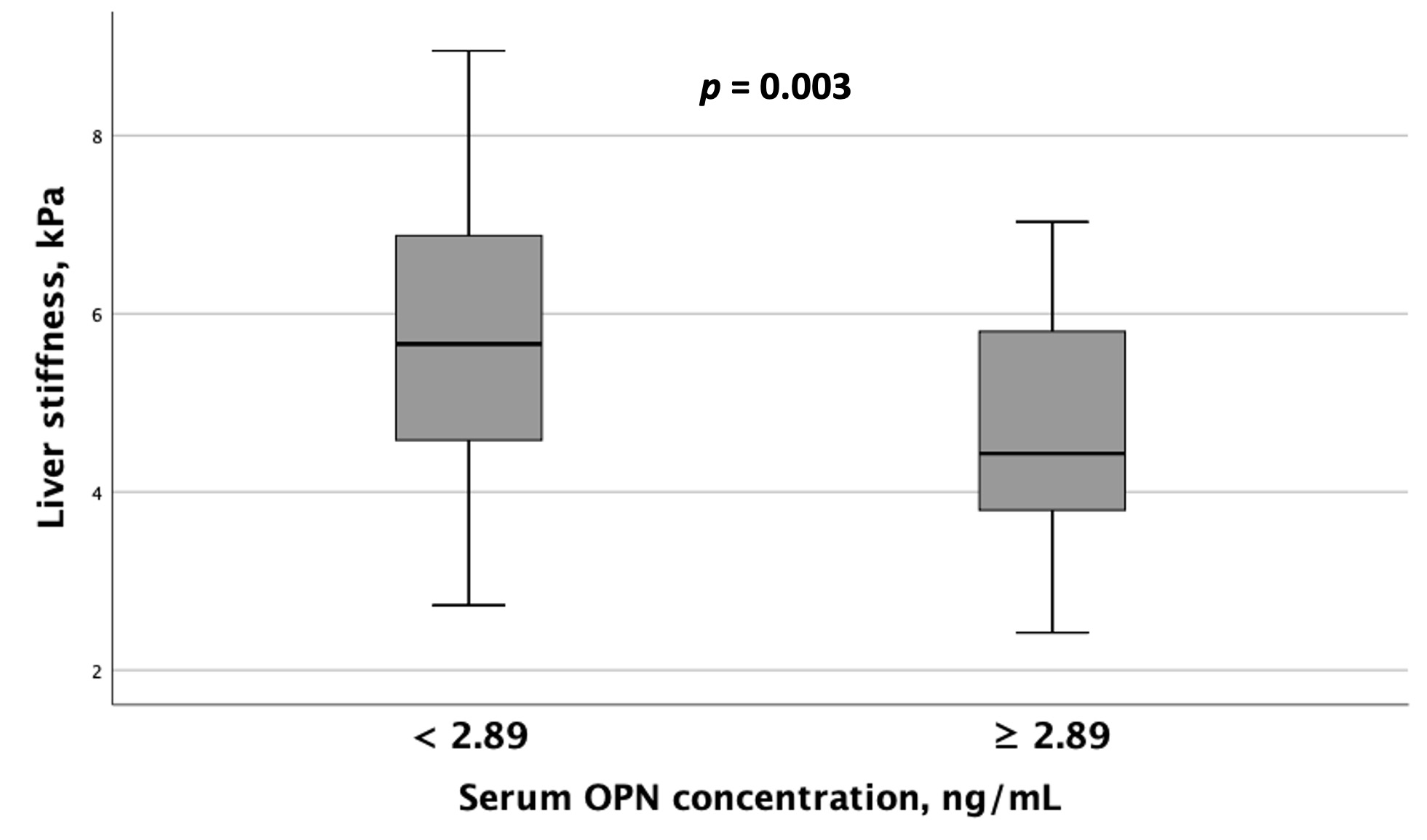
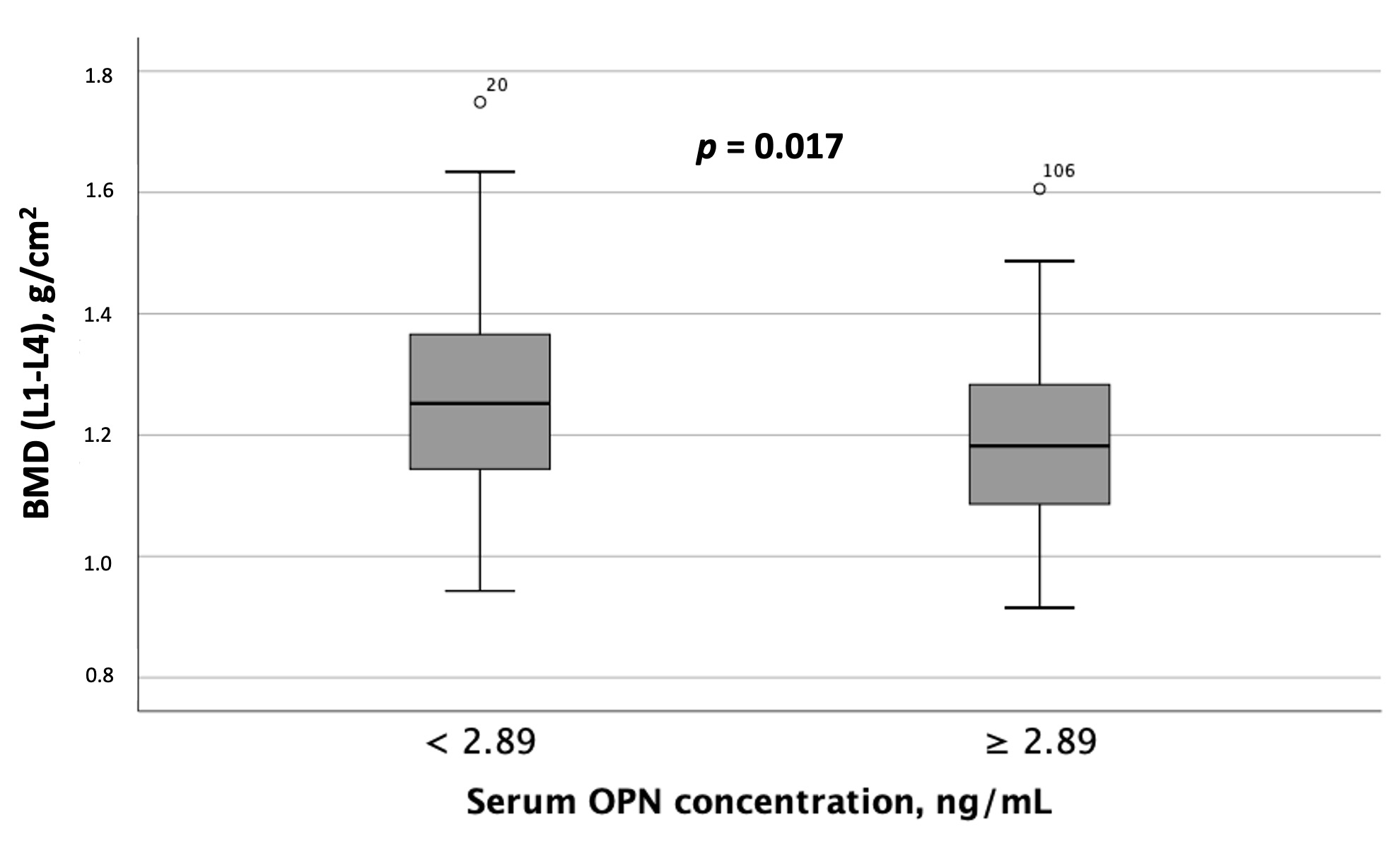
3.2.2. Subgroup Analysis Depending on the OPN and P1NP Serum Concentrations
4. Discussion
5. Limitations of the Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Younossi, Z.M.; Golabi, P.; Paik, J.M.; Henry, A.; Van Dongen, C.; Henry, L. The Global Epidemiology of Nonalcoholic Fatty Liver Disease (NAFLD) and Nonalcoholic Steatohepatitis (NASH): A Systematic Review. Hepatology 2023, 77, 1335–1347. [Google Scholar] [CrossRef] [PubMed]
- Younossi, Z.M.; Henry, L. Epidemiology of Non-Alcoholic Fatty Liver Disease and Hepatocellular Carcinoma. JHEP Rep. 2021, 3, 100305. [Google Scholar] [CrossRef] [PubMed]
- Huang, Q.; Yu, H.; Zhong, X.; Tian, Y.; Cui, Z.; Quan, Z. Association between Hypertension and Nonalcoholic Fatty Liver Disease: A Cross-Sectional and Meta-Analysis Study. J. Hum. Hypertens. 2023, 37, 313–320. [Google Scholar] [CrossRef] [PubMed]
- Cao, L.; An, Y.; Liu, H.; Jiang, J.; Liu, W.; Zhou, Y.; Shi, M.; Dai, W.; Lv, Y.; Zhao, Y.; et al. Global Epidemiology of Type 2 Diabetes in Patients with NAFLD or MAFLD: A Systematic Review and Meta-Analysis. BMC Med. 2024, 22, 101. [Google Scholar] [CrossRef] [PubMed]
- Ding, Y.; Deng, Q.; Yang, M.; Niu, H.; Wang, Z.; Xia, S. Clinical Classification of Obesity and Implications for Metabolic Dysfunction-Associated Fatty Liver Disease and Treatment. Diabetes Metab. Syndr. Obes. 2023, 16, 3303–3329. [Google Scholar] [CrossRef] [PubMed]
- Houghton, D.; Thoma, C.; Hallsworth, K.; Cassidy, S.; Hardy, T.; Burt, A.D.; Tiniakos, D.; Hollingsworth, K.G.; Taylor, R.; Day, C.P.; et al. Exercise Reduces Liver Lipids and Visceral Adiposity in Patients with Nonalcoholic Steatohepatitis in a Randomized Controlled Trial. Clin. Gastroenterol. Hepatol. 2017, 15, 96–102.e3. [Google Scholar] [CrossRef]
- Rosato, V.; Masarone, M.; Dallio, M.; Federico, A.; Aglitti, A.; Persico, M. NAFLD and Extra-Hepatic Comorbidities: Current Evidence on a Multi-Organ Metabolic Syndrome. Int. J. Environ. Res. Public Health 2019, 16, 3415. [Google Scholar] [CrossRef]
- Rinella, M.E.; Lazarus, J.V.; Ratziu, V.; Francque, S.M.; Sanyal, A.J.; Kanwal, F.; Romero, D.; Abdelmalek, M.F.; Anstee, Q.M.; Arab, J.P.; et al. A Multisociety Delphi Consensus Statement on New Fatty Liver Disease Nomenclature. Hepatology 2023, 78, 1966–1986. [Google Scholar] [CrossRef]
- Pan, B.; Cai, J.; Zhao, P.; Liu, J.; Fu, S.; Jing, G.; Niu, Q.; Li, Q. Relationship between Prevalence and Risk of Osteoporosis or Osteoporotic Fracture with Non-Alcoholic Fatty Liver Disease: A Systematic Review and Meta-Analysis. Osteoporos. Int. 2022, 33, 2275–2286. [Google Scholar] [CrossRef]
- Gao, Z.; Deng, H.; Qin, B.; Bai, L.; Li, J.; Zhang, J. Impact of Hypertension on Liver Fibrosis in Patients with Metabolic Dysfunction-Associated Fatty Liver Disease. Front. Med. 2025, 12, 1539283. [Google Scholar] [CrossRef]
- Lu, K.; Shi, T.-S.; Shen, S.-Y.; Shi, Y.; Gao, H.-L.; Wu, J.; Lu, X.; Gao, X.; Ju, H.-X.; Wang, W.; et al. Defects in a Liver-Bone Axis Contribute to Hepatic Osteodystrophy Disease Progression. Cell Metab. 2022, 34, 441–457.e7. [Google Scholar] [CrossRef] [PubMed]
- Xia, S.; Qin, X.; Wang, J.; Ren, H. Advancements in the Pathogenesis of Hepatic Osteodystrophy and the Potential Therapeutic of Mesenchymal Stromal Cells. Stem Cell Res. Ther. 2023, 14, 359. [Google Scholar] [CrossRef]
- Guañabens, N.; Parés, A. Osteoporosis in Chronic Liver Disease. Liver Int. 2018, 38, 776–785. [Google Scholar] [CrossRef]
- Ye, Z.; Lu, H.; Liu, P. Association between Essential Hypertension and Bone Mineral Density: A Systematic Review and Meta-Analysis. Oncotarget 2017, 8, 68916–68927. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.J.; Kim, D.J. An Overview of the Molecular Mechanisms Contributing to Musculoskeletal Disorders in Chronic Liver Disease: Osteoporosis, Sarcopenia, and Osteoporotic Sarcopenia. Int. J. Mol. Sci. 2021, 22, 2604. [Google Scholar] [CrossRef]
- Li, C.; Zeng, Y.; Tao, L.; Liu, S.; Ni, Z.; Huang, Q.; Wang, Q. Meta-Analysis of Hypertension and Osteoporotic Fracture Risk in Women and Men. Osteoporos. Int. 2017, 28, 2309–2318. [Google Scholar] [CrossRef] [PubMed]
- Chai, H.; Ge, J.; Li, L.; Li, J.; Ye, Y. Hypertension Is Associated with Osteoporosis: A Case-Control Study in Chinese Postmenopausal Women. BMC Musculoskelet. Disord. 2021, 22, 253. [Google Scholar] [CrossRef]
- Fodor, D.; Bondor, C.; Albu, A.; Simon, S.; Craciun, A.; Muntean, L. The Value of Osteopontin in the Assessment of Bone Mineral Density Status in Postmenopausal Women. J. Investig. Med. 2013, 61, 15–21. [Google Scholar] [CrossRef]
- Graupera, I.; Isus, L.; Coll, M.; Pose, E.; Díaz, A.; Vallverdú, J.; Rubio-Tomás, T.; Martínez-Sánchez, C.; Huelin, P.; Llopis, M.; et al. Molecular Characterization of Chronic Liver Disease Dynamics: From Liver Fibrosis to Acute-on-Chronic Liver Failure. JHEP Rep. 2022, 4, 100482. [Google Scholar] [CrossRef]
- Gómez-Santos, B.; Saenz de Urturi, D.; Nuñez-García, M.; Gonzalez-Romero, F.; Buque, X.; Aurrekoetxea, I.; Gutiérrez de Juan, V.; Gonzalez-Rellan, M.J.; García-Monzón, C.; González-Rodríguez, Á.; et al. Liver Osteopontin Is Required to Prevent the Progression of Age-Related Nonalcoholic Fatty Liver Disease. Aging Cell 2020, 19, e13183. [Google Scholar] [CrossRef]
- Bruha, R.; Vitek, L.; Smid, V. Osteopontin—A Potential Biomarker of Advanced Liver Disease. Ann. Hepatol. 2020, 19, 344–352. [Google Scholar] [CrossRef] [PubMed]
- Song, Z.; Chen, W.; Athavale, D.; Ge, X.; Desert, R.; Das, S.; Han, H.; Nieto, N. Osteopontin Takes Center Stage in Chronic Liver Disease. Hepatology 2021, 73, 1594–1608. [Google Scholar] [CrossRef]
- Miyoshi, K.; Kurata, M.; Okura, T.; Nagao, T.; Jotoku, M.; Enomoto, D.; Irita, J.; Higaki, J. Relationship between Plasma Osteopontin Concentration and Improvement of Augmentation Index with Antihypertensive the Treatment. Int. J. Cardiol. 2009, 137, S150–S151. [Google Scholar] [CrossRef]
- Caesar, C.; Lyle, A.N.; Joseph, G.; Weiss, D.; Alameddine, F.M.F.; Lassègue, B.; Griendling, K.K.; Taylor, W.R. Cyclic Strain and Hypertension Increase Osteopontin Expression in the Aorta. Cell Mol. Bioeng. 2016, 10, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Luger, M.; Kruschitz, R.; Kienbacher, C.; Traussnigg, S.; Langer, F.B.; Schindler, K.; Würger, T.; Wrba, F.; Trauner, M.; Prager, G.; et al. Prevalence of Liver Fibrosis and Its Association with Non-Invasive Fibrosis and Metabolic Markers in Morbidly Obese Patients with Vitamin D Deficiency. Obes. Surg. 2016, 26, 2425–2432. [Google Scholar] [CrossRef]
- Mao, Y.; Jiang, L.; Yan, X.; Ma, H. Effects of Antihypertensive Drugs on Bone Metabolism in Ovariectomized Spontaneously Hypertensive Rats. Int. J. Clin. Exp. Med. 2016, 9, 17628–17635. [Google Scholar]
- Younossi, Z.; Aggarwal, P.; Shrestha, I.; Fernandes, J.; Johansen, P.; Augusto, M.; Nair, S. The Burden of Non-Alcoholic Steatohepatitis: A Systematic Review of Health-Related Quality of Life and Patient-Reported Outcomes. JHEP Rep. 2022, 4, 100525. [Google Scholar] [CrossRef]
- Brooke-Wavell, K.; Skelton, D.A.; Barker, K.L.; Clark, E.M.; De Biase, S.; Arnold, S.; Paskins, Z.; Robinson, K.R.; Lewis, R.M.; Tobias, J.H.; et al. Strong, Steady and Straight: UK Consensus Statement on Physical Activity and Exercise for Osteoporosis. Br. J. Sports Med. 2022, 56, 837–846. [Google Scholar] [CrossRef]
- Shepherd, J.; Ng, B.; Sommer, M.; Heymsfield, S.B. Body Composition by DXA. Bone 2017, 104, 101–105. [Google Scholar] [CrossRef]
- Younossi, Z.M.; Rinella, M.E.; Sanyal, A.J.; Harrison, S.A.; Brunt, E.M.; Goodman, Z.; Cohen, D.E.; Loomba, R. From NAFLD to MAFLD: Implications of a Premature Change in Terminology. Hepatology 2021, 73, 1194–1198. [Google Scholar] [CrossRef]
- Bedogni, G.; Bellentani, S.; Miglioli, L.; Masutti, F.; Passalacqua, M.; Castiglione, A.; Tiribelli, C. The Fatty Liver Index: A Simple and Accurate Predictor of Hepatic Steatosis in the General Population. BMC Gastroenterol. 2006, 6, 33. [Google Scholar] [CrossRef]
- Boursier, J.; Zarski, J.-P.; de Ledinghen, V.; Rousselet, M.-C.; Sturm, N.; Lebail, B.; Fouchard-Hubert, I.; Gallois, Y.; Oberti, F.; Bertrais, S.; et al. Determination of Reliability Criteria for Liver Stiffness Evaluation by Transient Elastography. Hepatology 2013, 57, 1182–1191. [Google Scholar] [CrossRef]
- Fang, C.; Sidhu, P.S. Ultrasound-Based Liver Elastography: Current Results and Future Perspectives. Abdom. Radiol. 2020, 45, 3463–3472. [Google Scholar] [CrossRef] [PubMed]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- Donini, L.M.; Busetto, L.; Bischoff, S.C.; Cederholm, T.; Ballesteros-Pomar, M.D.; Batsis, J.A.; Bauer, J.M.; Boirie, Y.; Cruz-Jentoft, A.J.; Dicker, D.; et al. Definition and Diagnostic Criteria for Sarcopenic Obesity: ESPEN and EASO Consensus Statement. Obes. Facts 2022, 15, 321–335. [Google Scholar] [CrossRef] [PubMed]
- Camacho, P.M.; Petak, S.M.; Binkley, N.; Diab, D.L.; Eldeiry, L.S.; Farooki, A.; Harris, S.T.; Hurley, D.L.; Kelly, J.; Lewiecki, E.M.; et al. American association of clinical endocrinologists/american college of endocrinology clinical practice guidelines for the diagnosis and treatment of postmenopausal osteoporosis—2020 update executive summary. Endocr. Pract. 2020, 26, 564–570. [Google Scholar] [CrossRef] [PubMed]
- Pan, Y.; Xu, J. Association between Muscle Mass, Bone Mineral Density and Osteoporosis in Type 2 Diabetes. J. Diabetes Investig. 2022, 13, 351–358. [Google Scholar] [CrossRef]
- Han, H.; Chen, S.; Wang, X.; Jin, J.; Li, X.; Li, Z. Association between Muscle Strength and Mass and Bone Mineral Density in the US General Population: Data from NHANES 1999–2002. J. Orthop. Surg. Res. 2023, 18, 397. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European Consensus on Definition and Diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef]
- Albalwi, A.A.; Alharbi, A.A. Optimal Procedure and Characteristics in Using Five Times Sit to Stand Test among Older Adults: A Systematic Review. Medicine 2023, 102, e34160. [Google Scholar] [CrossRef]
- Bland, M. An Introduction to Medical Statistics; Oxford University Press: Oxford, UK, 2015; ISBN 978-0-19-958992-0. [Google Scholar]
- Shen, Z.; Cen, L.; Chen, X.; Pan, J.; Li, Y.; Chen, W.; Yu, C. Increased Risk of Low Bone Mineral Density in Patients with Non-Alcoholic Fatty Liver Disease: A Cohort Study. Eur. J. Endocrinol. 2020, 182, 157–164. [Google Scholar] [CrossRef]
- Mantovani, A.; Gatti, D.; Zoppini, G.; Lippi, G.; Bonora, E.; Byrne, C.D.; Nobili, V.; Targher, G. Association Between Nonalcoholic Fatty Liver Disease and Reduced Bone Mineral Density in Children: A Meta-Analysis. Hepatology 2019, 70, 812–823. [Google Scholar] [CrossRef]
- Yilmaz, Y.; Ozturk, O.; Alahdab, Y.O.; Senates, E.; Colak, Y.; Doganay, H.L.; Coskunpinar, E.; Oltulu, Y.M.; Eren, F.; Atug, O.; et al. Serum Osteopontin Levels as a Predictor of Portal Inflammation in Patients with Nonalcoholic Fatty Liver Disease. Dig. Liver Dis. 2013, 45, 58–62. [Google Scholar] [CrossRef]
- Nyström, T.; Dunér, P.; Hultgårdh-Nilsson, A. A Constitutive Endogenous Osteopontin Production Is Important for Macrophage Function and Differentiation. Exp. Cell Res. 2007, 313, 1149–1160. [Google Scholar] [CrossRef]
- Giachelli, C.M.; Steitz, S. Osteopontin: A Versatile Regulator of Inflammation and Biomineralization. Matrix Biol. 2000, 19, 615–622. [Google Scholar] [CrossRef]
- Burdo, T.H.; Wood, M.R.; Fox, H.S. Osteopontin Prevents Monocyte Recirculation and Apoptosis. J. Leukoc. Biol. 2007, 81, 1504–1511. [Google Scholar] [CrossRef]
- Mazzali, M.; Kipari, T.; Ophascharoensuk, V.; Wesson, J.A.; Johnson, R.; Hughes, J. Osteopontin—A Molecule for All Seasons. QJM 2002, 95, 3–13. [Google Scholar] [CrossRef]
- Deng, H.; Dai, Y.; Lu, H.; Li, S.-S.; Gao, L.; Zhu, D.-L. Analysis of the Correlation between Non-Alcoholic Fatty Liver Disease and Bone Metabolism Indicators in Healthy Middle-Aged Men. Eur. Rev. Med. Pharmacol. Sci. 2018, 22, 1457–1462. [Google Scholar] [CrossRef]
- Fang, D.; Yin, H.; Ji, X.; Sun, H.; Zhao, X.; Bi, Y.; Gu, T. Low Levels of Osteocalcin, but Not CTX or P1NP, Are Associated with Nonalcoholic Hepatic Steatosis and Steatohepatitis. Diabetes Metab. 2023, 49, 101397. [Google Scholar] [CrossRef]
- Xuan, Y.; He, F.; Liu, Q.; Dai, D.; Wu, D.; Shi, Y.; Yao, Q. Elevated GGT to HDL Ratio as a Marker for the Risk of NAFLD and Liver Fibrosis. Sci. Rep. 2025, 15, 10. [Google Scholar] [CrossRef]
- Fujii, H.; Doi, H.; Ko, T.; Fukuma, T.; Kadono, T.; Asaeda, K.; Kobayashi, R.; Nakano, T.; Doi, T.; Nakatsugawa, Y.; et al. Frequently Abnormal Serum Gamma-Glutamyl Transferase Activity Is Associated with Future Development of Fatty Liver: A Retrospective Cohort Study. BMC Gastroenterol. 2020, 20, 217. [Google Scholar] [CrossRef]
- Farup, P.G. Changes in Bone Turnover Markers 6-12 Months after Bariatric Surgery. Sci. Rep. 2024, 14, 14844. [Google Scholar] [CrossRef]
- Nuijten, M.A.H.; Eijsvogels, T.M.H.; Monpellier, V.M.; Janssen, I.M.C.; Hazebroek, E.J.; Hopman, M.T.E. The Magnitude and Progress of Lean Body Mass, Fat-free Mass, and Skeletal Muscle Mass Loss Following Bariatric Surgery: A Systematic Review and Meta-analysis. Obes. Rev. 2022, 23, e13370. [Google Scholar] [CrossRef]
- Anyiam, O.; Abdul Rashid, R.S.; Bhatti, A.; Khan-Madni, S.; Ogunyemi, O.; Ardavani, A.; Idris, I. A Systematic Review and Meta-Analysis of the Effect of Caloric Restriction on Skeletal Muscle Mass in Individuals with, and without, Type 2 Diabetes. Nutrients 2024, 16, 3328. [Google Scholar] [CrossRef]
- Haeri, N.S.; Perera, S.; Greenspan, S.L. The Association of Bone Turnover Markers with Muscle Function, Falls, and Frailty in Older Women in Long-Term Care. J. Frailty Aging 2023, 12, 284–290. [Google Scholar] [CrossRef]
- Berzigotti, A.; Tsochatzis, E.; Boursier, J.; Castera, L.; Cazzagon, N.; Friedrich-Rust, M.; Petta, S.; Thiele, M. EASL Clinical Practice Guidelines on Non-Invasive Tests for Evaluation of Liver Disease Severity and Prognosis—2021 Update. J. Hepatol. 2021, 75, 659–689. [Google Scholar] [CrossRef]
- Wen, Y.; Jeong, S.; Xia, Q.; Kong, X. Role of Osteopontin in Liver Diseases. Int. J. Biol. Sci. 2016, 12, 1121–1128. [Google Scholar] [CrossRef]
- Glass, O.; Henao, R.; Patel, K.; Guy, C.D.; Gruss, H.J.; Syn, W.-K.; Moylan, C.A.; Streilein, R.; Hall, R.; Mae Diehl, A.; et al. Serum Interleukin-8, Osteopontin, and Monocyte Chemoattractant Protein 1 Are Associated with Hepatic Fibrosis in Patients with Nonalcoholic Fatty Liver Disease. Hepatol. Commun. 2018, 2, 1344–1355. [Google Scholar] [CrossRef]

| Parameter | Patients with MASLD and HTN (n = 117) |
|---|---|
| Female gender, n (%) | 67 (57.3) |
| Age, years | 57 (49–64) |
| BMI, kg/m2 | 32.9 (29.6–36.2) |
| Normal weight (BMI 18.5–24.9 kg/m2), n (%) | 2 (1.7) |
| Overweight (BMI 25.0–29.9 kg/m2), n (%) | 30 (25.6) |
| Obesity (BMI ≥ 30 kg/m2), n (%) | 85 (72.6) |
| Waist circumference (all subjects), cm | 108 (102–115) |
| Waist circumference (male), cm | 111.5 (106–117) |
| Normal Range | ≤94 cm |
| Patients Outside the Normal Range, n (%) | 50 (100) |
| Waist circumference (female), cm | 105 (98–111) |
| Normal Range | ≤80 cm |
| Patients Outside the Normal Range, n (%) | 66 (98.5) |
| Hip circumference, cm | 113 (108–118.75) |
| Parameter | Patients with MASLD and HTN (n = 117) | Normal Range | Patients Outside the Normal Range, n (%) |
|---|---|---|---|
| Erythrocytes, 1012/L | 4.80 (4.51–5.00) | ||
| Erythrocytes, 1012/L (male) | 4.98 (4.76–5.28) | 4.0–5.9 | 0 (0) |
| Erythrocytes, 1012/L (female) | 4.6 (4.3–4.8) | 3.8–5.2 | 0 (0) |
| Hemoglobin, g/L | 146 (133–152) | ||
| Hemoglobin, g/L (male) | 152 (147–156.5) | 140–175 | 0 (0) |
| Hemoglobin, g/L (female) | 137 (129–145.5) | 123–153 | 0 (0) |
| ESR, mm/h | 9 (4–14) | <20 | 0 (0) |
| Platelets, 109/L | 253.0 (211.8–290.0) | 150–450 | 0 (0) |
| Leukocytes, 109/L | 6.4 (5.3–7.5) | 5–10 | 0 (0) |
| ALT, IU/L | 23.0 (16.0–37.3) | 0–34 | 34 (29.1) |
| AST, IU/L | 22.0 (18.0–26.3) | 0–34 | 10 (8.5) |
| GGT, IU/L | 31.0 (21.0–45.5) | 0–38 | 42 (35.9) |
| Albumin, g/dL | 4.5 (4.3–4.6) | 3.5–5.2 | 0 (0) |
| Total bilirubin, μmol/L | 11.7 (9.0–14.5) | 3.4-20.5 | 6 (5.1) |
| Uric acid, μmol/L | 357 (327.3–416.5) | 154.7–356.9 | 57 (48.7) |
| CRP, mg/L | 2.2 (1.4–5.0) | 0–5 | 29 (24.8) |
| Total cholesterol, mmol/L | 5.8 (4.9–6.2) | 0–5 | 82 (70.1) |
| Triglycerides, mmol/L | 1.43 (1.10–2.10) | <1.7 | 46 (39.3) |
| Creatinine, μmol/L | 75.7 (67.6–90.0) | 51–98 | 10 (8.5) |
| Glucose, mmol/L | 5.7 (5.4–6.0) | 3.9-5.5 | 72 (61.5) |
| Calcium, mmol/L | 2.4 (2.3–2.5) | 2.1–2.55 | 4 (3.5) |
| Phosphorus, mmol/L | 1.1 (0.9–1.2) | 0.81-1.45 | 0 (0) |
| HOMA-IR > 2.7, n (%) | 61.0 (52.1) | 0.5–1.4 | - |
| pSWE, kPa | 5.4 (4.1–6.3) | <7 | 11 (9.4) |
| Parameter | Serum OPN Concentration in Patients with MASLD and HTN, ng/mL | Serum P1NP Concentration in Patients with MASLD and HTN, pg/mL | ||||
|---|---|---|---|---|---|---|
| <2.89 (n = 72) | ≥2.89 (n = 45) | p | <47.5 (n = 70) | ≥47.5 (n = 47) | p | |
| Age, years | 55.5 (47.3–62.8) | 58.0 (51.0–64.5) | n/s | 57.0 (49.0–65.0) | 56.0 (48.0–63.0) | n/s |
| Gender: female, n (%) | 38.0 (52.8) | 29.0 (64.4) | n/s | 38.0 (54.3) | 29.0 (61.7) | n/s |
| BMI, kg/m2 | 33.2 (30.6–36.1) | 32.1 (28.9–36.9) | n/s | 32.9 (30.1–36.1) | 32.8 (29.5–36.8) | n/s |
| HTN, n (%): | n/s | n/s | ||||
| Grade 1 | 24.0 (33.3) | 15.0 (33.3) | 23.0 (32.9) | 16.0 (34.0) | ||
| Grade 2 | 21.0 (29.2) | 13.0 (28.9) | 22.0 (31.4) | 12.0 (25.5) | ||
| Grade 3 | 27.0 (37.5) | 17.0 (37.8) | 25.0 (35.7) | 19.0 (40.5) | ||
| Antihyperten-sive therapy, n (%) | 47.0 (65.3) | 31.0 (68.8) | n/s | 43.0 (61.4) | 35 (74.5) | n/s |
| T2D, n (%) | 8.0 (11.1) | 4.0 (8.8) | n/s | 9.0 (12.9) | 3.0 (6.4) | n/s |
| IFG, n (%) | 13.0 (18.1) | 9.0 (20) | n/s | 12.0 (17.1) | 10.0 (21.3) | n/s |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sheptulina, A.F.; Elkina, A.Y.; Mamutova, E.M.; Timofeev, Y.S.; Metelskaya, V.A.; Drapkina, O.M. Serum Osteopontin and Procollagen Type 1 N-Terminal Propeptide Concentrations: Links to Liver Function, Muscle Mass, and Bone Mineral Density in MASLD and Hypertension. Metabolites 2025, 15, 459. https://doi.org/10.3390/metabo15070459
Sheptulina AF, Elkina AY, Mamutova EM, Timofeev YS, Metelskaya VA, Drapkina OM. Serum Osteopontin and Procollagen Type 1 N-Terminal Propeptide Concentrations: Links to Liver Function, Muscle Mass, and Bone Mineral Density in MASLD and Hypertension. Metabolites. 2025; 15(7):459. https://doi.org/10.3390/metabo15070459
Chicago/Turabian StyleSheptulina, Anna F., Anastasia Yu. Elkina, Elvira M. Mamutova, Yuriy S. Timofeev, Victoria A. Metelskaya, and Oxana M. Drapkina. 2025. "Serum Osteopontin and Procollagen Type 1 N-Terminal Propeptide Concentrations: Links to Liver Function, Muscle Mass, and Bone Mineral Density in MASLD and Hypertension" Metabolites 15, no. 7: 459. https://doi.org/10.3390/metabo15070459
APA StyleSheptulina, A. F., Elkina, A. Y., Mamutova, E. M., Timofeev, Y. S., Metelskaya, V. A., & Drapkina, O. M. (2025). Serum Osteopontin and Procollagen Type 1 N-Terminal Propeptide Concentrations: Links to Liver Function, Muscle Mass, and Bone Mineral Density in MASLD and Hypertension. Metabolites, 15(7), 459. https://doi.org/10.3390/metabo15070459