
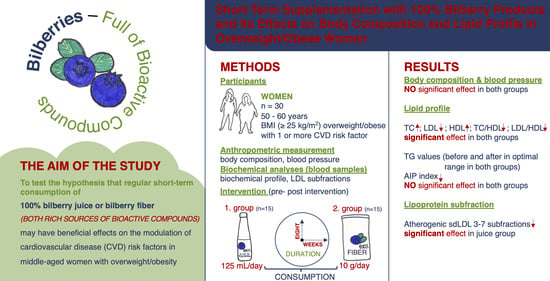
Short-Term Supplementation with 100% Bilberry Products and Its Effects on Body Composition and Lipid Profile in Overweight/Obese Women

 , , , , and
, , , , and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants and Study Design
2.2. Intervention
2.3. Anthropometric Measurements
2.4. Preparation of Blood Samples
2.5. Clinical Parameters
2.6. Statistical Analysis
3. Results
3.1. The Bioactive Compounds in 100% Bilberry Juice and Dietary Fibre of Bilberry
3.2. Characteristics of Study Participants
3.2.1. Anthropometric Parameters and Blood Pressure Measurements
3.2.2. Changes in Basic Lipid Profile Parameters and Lipoprotein Indexes
3.2.3. Changes in Lipoprotein Subfractions
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ANOVA | Analysis of variance |
| BFM | Body fat mass |
| BMI | Body mass index |
| CVD | Cardiovascular disease |
| DBP | Diastolic blood pressure |
| DPPH | 2,2-diphenyl-1-picrylhydrazyl |
| EDTA | Ethylenediaminetetraacetic acid |
| FFM | Fat-free mass |
| GAE | Gallic acid equivalent |
| HDL | High-density lipoprotein |
| HDL-C | High-density lipoprotein cholesterol–refers to the amount of cholesterol carried by low-density lipoproteins in the blood |
| IDL | Intermediate-density lipoprotein |
| LDL | Low-density lipoprotein |
| NFC | Not from concentrate |
| PBF | Body fat percentage |
| SBP | Systolic blood pressure |
| sdLDL | Small dense low-density cholesterol |
| SSM | Skeletal muscle mass |
| TC | Total cholesterol |
| TC/HDL | Ratio of total cholesterol to high-density lipoprotein |
| TG | Triglyceride |
| VFA | Visceral fat area |
| VLDL | Very-low-density lipoprotein |
| WC | Waist circumference |
| WHR | Waist-to-hip ratio |
References
- WHO. Obesity and Overweight. 2024. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 10 January 2025).
- Saxena, I.; Kaur, P.A.; Suman, S.; Abhilasha; Mitra, P.; Sharma, P.; Kumar, M. The Multiple Consequences of Obesity. In Weight Management—Challenges and Opportunities; IntechOpen: Anthem, AZ, USA, 2022; 250p, Available online: https://www.intechopen.com/books/11022 (accessed on 20 March 2025).
- Taylor, V.H.; Forhan, M.; Vigod, S.N.; McIntyre, R.S.; Morrison, K.M. The impact of obesity on quality of life. Best Practice & Research. Clin. Endocrinol. Metab. 2013, 27, 139–146. [Google Scholar] [CrossRef]
- Koskinas, K.C.; Van Craenenbroeck, E.M.; Antoniades, C.; Blüher, M.; Gorter, T.M.; Hanssen, H.; Marx, N.; McDonagh, T.A.; Mingrone, G.; Rosengren, A.; et al. Obesity and cardiovascular disease: An ESC clinical consensus statement. Eur. Heart J. 2024, 45, 4063–4098. [Google Scholar] [CrossRef]
- Minglan, J.; Xiao, R.; Longyang, H.; Xiaowei, Z. Associations between sarcopenic obesity and risk of cardiovascular disease: A population-based cohort study among middle-aged and older adults using the CHARLS. Clin. Nutr. 2024, 43, 796–802. [Google Scholar] [CrossRef]
- Perone, F.; Pingitore, A.; Conte, E.; Halasz, G.; Ambrosetti, M.; Peruzzi, M.; Cavarretta, E. Obesity and Cardiovascular Risk: Systematic Intervention Is the Key for Prevention. Healthcare 2023, 11, 902. [Google Scholar] [CrossRef]
- Guo, F.; Garvey, W.T. Cardiometabolic Disease Risk in Metabolically Healthy and Unhealthy Obesity: Stability of Metabolic Health Status in Adults. Obesity 2016, 24, 516–525. [Google Scholar] [CrossRef]
- Halland, H.; Lønnebakken, M.T.; Pristaj, N.; Saeed, S.; Midtbø, H.; Einarsen, E.; Gerdts, E. Sex differences in subclinical cardiac disease in overweight and obesity (the FATCOR study). Nutr. Metab. Cardiovasc. Dis. 2018, 28, 1054–1060. [Google Scholar] [CrossRef]
- Bakhtiyari, M.; Kazemian, E.; Kabir, K.; Hadaegh, F.; Aghajanian, S.; Mardi, P.; Ghahfarokhi, N.T.; Ghanbari, A.; Mansournia, M.A.; Azizi, F. Contribution of obesity and cardiometabolic risk factors in developing cardiovascular disease: A population-based cohort study. Sci. Rep. 2022, 12, 1544. [Google Scholar] [CrossRef]
- Lopez-Jimenez, F.; Almahmeed, W.; Bays, H.; Cuevas, A.; Di Angelantonio, E.; le Roux, C.W.; Sattar, N.; Sun, M.C.; Wittert, G.; Pinto, F.J.; et al. Obesity and cardiovascular disease: Mechanistic insights and management strategies. A joint position paper by the World Heart Federation and World Obesity Federation. Eur. J. Prev. Cardiol. 2022, 29, 2218–2237. [Google Scholar] [CrossRef]
- Chan, D.C.; Pang, J.; Watts, G.F. Dyslipidemia in Obesity. In Metabolic Syndrome; Ahima, R.S., Ed.; Springer: Cham, Switzerland, 2016. [Google Scholar] [CrossRef]
- Libby, P.; Ridker, P.M.; Maseri, A. Inflammation and atherosclerosis. Circulation 2002, 105, 1135–1143. [Google Scholar] [CrossRef]
- Chary, A.; Tohidi, M.; Hedayati, M. Association of LDL-cholesterol subfractions with cardiovascular disorders: A systematic review. BMC Cardiovasc. Disord. 2023, 23, 533. [Google Scholar] [CrossRef]
- Oravec, S.; Mikl, J.; Gruber, K.; Dostal, E. A Non-Atherogenic and Atherogenic Lipoprotein Profile in Individuals with Dyslipoproteinemia [Internet]. In Lipoproteins—Role in Health and Diseases; InTech: Hyogo, Japan, 2012. [Google Scholar] [CrossRef]
- Deza, S.; Colina, I.; Beloqui, O.; Monreal, J.I.; Martínez-Chávez, E.; Maroto-García, J.; Mugueta, C.; González, A.; Varo, N. Evaluation of measured and calculated small dense low-density lipoprotein in capillary blood and association with the metabolic syndrome. Clin. Chim. Acta 2024, 557, 117897. [Google Scholar] [CrossRef]
- Sikand, G.; Severson, T. Top 10 dietary strategies for atherosclerotic cardiovascular risk reduction. Am. J. Prev. Cardiol. 2020, 4, 100106. [Google Scholar] [CrossRef]
- Iqbal, I.; Wilairatana, P.; Saqib, F.; Nasir, B.; Wahid, M.; Latif, M.F.; Iqbal, A.; Naz, R.; Mubarak, M.S. Plant Polyphenols and Their Potential Benefits on Cardiovascular Health: A Review. Molecules 2023, 28, 6403. [Google Scholar] [CrossRef]
- Murray, M.; Dordevic, A.L.; Ryan, L.; Bonham, M.P. An emerging trend in functional foods for the prevention of cardiovascular disease and diabetes: Marine algal polyphenols. Crit. Rev. Food Sci. Nutr. 2018, 58, 1342–1358. [Google Scholar] [CrossRef]
- Yang, B.; Kortesniemi, M. Clinical evidence on potential health benefits of berries. Curr. Opin. Food Sci. 2015, 2, 36–42. [Google Scholar] [CrossRef]
- Habanova, M.; Saraiva, J.A.; Haban, M.; Schwarzova, M.; Chlebo, P.; Predna, L.; Gažo, J.; Wyka, J. Intake of bilberries (Vaccinium myrtillus L.) reduced risk factors for cardiovascular disease by inducing favorable changes in lipoprotein profiles. Nutr. Res. 2016, 36, 1415–1422. [Google Scholar] [CrossRef]
- Habanova, M.; Holovicova, M.; Scepankova, H.; Lorkova, M.; Gazo, J.; Gazarova, M.; Pinto, C.A.; Saraiva, J.A.; Estevinho, L.M. Modulation of Lipid Profile and Lipoprotein Subfractions in Overweight/Obese Women at Risk of Cardiovascular Diseases through the Consumption of Apple/Berry Juice. Antioxidants 2022, 11, 2239. [Google Scholar] [CrossRef]
- Zhang, L.; Muscat, J.E.; Kris-Etherton, P.M.; Chinchilli, V.M.; Al-Shaar, L.; Richie, J.P. The Epidemiology of Berry Consumption and Association of Berry Consumption with Diet Quality and Cardiometabolic Risk Factors in United States Adults: The National Health and Nutrition Examination Survey, 2003–2018. J. Nutr. 2024, 154, 1014–1026. [Google Scholar] [CrossRef]
- Donno, D.; Neirotti, G.; Fioccardi, A.; Razafindrakoto, Z.R.; Tombozara, N.; Mellano, M.G.; Beccaro, G.L.; Gamba, G. Freeze-Drying for the Reduction of Fruit and Vegetable Chain Losses: A Sustainable Solution to Produce Potential Health-Promoting Food Applications. Plants 2025, 14, 168. [Google Scholar] [CrossRef] [PubMed]
- Yousdefizadeh, S.; Farkhondeh, T.; Almzadeh, E.; Samarghandian, S. A Systematic Study on the Impact of Blueberry Supplementation on Metabolic Syndrome Components. Curr. Nutr. Food Sci. 2025, 21, 333–340. [Google Scholar] [CrossRef]
- Pires, T.C.S.P.; Caleja, C.; Santos-Buelga, C.; Barros, L.; Ferreira, I.C.F.R. Vaccinium myrtillus L. Fruits as a Novel Source of Phenolic Compounds with Health Benefits and Industrial Applications—A Review. Curr. Pharm. Des. 2020, 26, 1917–1928. [Google Scholar] [CrossRef] [PubMed]
- Thiese, M.S. Observational and interventional study design types; an overview. Lessons Biostat. 2014, 24, 199–210. [Google Scholar] [CrossRef]
- Lachman, J.; Hamouz, K.; Čepl, J.; Pivec, V.; Šulc, M.; Dvořák, P. The Effect of Selected Factors on Polyphenol Content and Antioxidant Activity in Potato Tubers. Chem. Listy 2006, 100, 522–527. [Google Scholar]
- Lapornik, B.; Prošek, M.; Golc Wondraet, A. Comparison of extracts prepared from plant by-products using different solvents and extraction time. J. Food Eng. 2005, 71, 214–222. [Google Scholar] [CrossRef]
- Gabriele, M.; Pucci, L.; Árvay, J.; Longo, V. Anti-inflammatory and antioxidant effect of fermented whole wheat on TNFα-stimulated HT-29 and NF-κB signalling pathway activation. J. Funct. Foods 2018, 48, 392–400. [Google Scholar] [CrossRef]
- Brand-Williams, W.; Cuvelier, M.E.; Berset, C. Use of a Free Radical Method to Evaluate Antioxidant Activity. LWT-Food Sci. Technol. 1995, 28, 25–30. [Google Scholar] [CrossRef]
- Hernández, Y.; Lobo, M.G.; Gonzálezet, M. Determination of vitamin C in tropical fruits: A comparative evaluation of methods. Food Chem. 2006, 96, 654–664. [Google Scholar] [CrossRef]
- Skrzypczak, M.; Szwed, A.; Pawli, R.; Skrzypulec, V. Assessment of the BMI, WHR and W/Ht in pre- and postmenopausal women. Anthropol. Rev. 2007, 70, 3–13. [Google Scholar] [CrossRef]
- Whelton, P.K.; Carey, R.M.; Aronow, W.S.; Casey, D.E.; Collins, K.J.; Dennison Himmelfarb, C.; DePalma, S.M.; Gidding, S.; Jamerson, K.A.; Jones, D.W.; et al. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/APhA/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension 2018, 71, 1269–1324. [Google Scholar] [CrossRef]
- NCEP ATP III. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol in Adults (Adult Treatment Panel III). JAMA 2001, 285, 2486–2497. [Google Scholar] [CrossRef]
- Millán, J.; Pintó, X.; Muñoz, A.; Zúñiga, M.; Rubiés-Prat, J.; Pallardo, L.F.; Masana, L.; Mangas, A.; Hernández-Mijares, A.; González-Santos, P.; et al. Lipoprotein ratios: Physiological significance and clinical usefulness in cardiovascular prevention. Vasc. Health Risk Manag. 2009, 5, 757–765. [Google Scholar] [PubMed]
- Dobiásová, M. AIP-atherogenic index of plasma as a significant predictor of cardiovascular risk: From research to practice. Vnitr. Lek. 2006, 52, 64–71. [Google Scholar] [PubMed]
- Zitnanova, I.; Oravec, S.; Janubova, M.; Konarikova, K.; Dvorakova, M.; Laubertova, L.; Kralova, M.; Simko, M.; Muchova, J. Gender differences in LDL and HDL subfractions in atherogenic and nonatherogenic phenotypes. Clin. Biochem. 2020, 79, 9–13. [Google Scholar] [CrossRef]
- Harris, A.D.; McGregor, J.C.; Perencevich, E.N.; Furuno, J.P.; Zhu, J.; Peterso, D.E.; Finkelstein, J. The Use and Interpretation of Quasi-Experimental Studies in Medical Informatics. J. Am. Med. Inform. Assoc. 2006, 13, 16–23. [Google Scholar] [CrossRef]
- Lavefve, L.; Howard, L.R.; Carboneroi, F. Berry polyphenols metabolism and impact on human gut microbiota and health. Food Funct. 2020, 11, 45–65. [Google Scholar] [CrossRef] [PubMed]
- Vaneková, Z.; Rollinger, J.M. Bilberries: Curative and Miraculous—A Review on Bioactive Constituents and Clinical Research. Front. Pharmacol. 2022, 13, 909914. [Google Scholar] [CrossRef]
- Brezoiu, A.M.; Deaconu, M.; Mitran, R.-A.; Sedky, N.K.; Schiets, F.; Marote, P.; Voicu, I.-S.; Matei, C.; Ziko, L.; Berger, D. The Antioxidant and Anti-Inflammatory Properties of Wild Bilberry Fruit Extracts Embedded in Mesoporous Silica-Type Supports: A Stability Study. Antioxidants 2024, 13, 250. [Google Scholar] [CrossRef]
- Kalt, W.; Cassidy, A.; Howard, L.R.; Krikorian, R.; Stull, A.J.; Tremblay, F.; Zamora-Ros, R. Recent Research on the Health Benefits of Blueberries and Their Anthocyanins. Adv. Nutr. 2020, 11, 224–236. [Google Scholar] [CrossRef]
- Wu, Y.; Han, T.; Yang, H.; Lyu, L.; Li, W.; Wu, W. Known and potential health benefits and mechanisms of blueberry anthocyanins: A review. Food Biosci. 2023, 55, 103050. [Google Scholar] [CrossRef]
- Negrușier, C.; Colișar, A.; Rózsa, S.; Chiș, M.S.; Sîngeorzan, S.-M.; Borsai, O.; Negrean, O.-R. Bilberries vs. Blueberries: A Comprehensive Review. Horticulturae 2024, 10, 1343. [Google Scholar] [CrossRef]
- McCullough, M.L.; Peterson, J.J.; Patel, R.; Jacques, P.F.; Shah, R.; Dwyer, J.T. Flavonoid intake and cardiovascular disease mortality in a prospective cohort of US adults. Am. J. Clin. Nutr. 2012, 95, 454–464. [Google Scholar] [CrossRef] [PubMed]
- Habauzit, V.; Verny, M.A.; Milenkovic, D.; Barber-Chamoux, N.; Mazur, A.; Dubray, C.; Morand, C. Flavanones protect from arterial stiffness in postmenopausal women consuming grapefruit juice for 6 mo: A randomized, controlled, crossover trial. Am. J. Clin. Nutr. 2015, 102, 66–74. [Google Scholar] [CrossRef] [PubMed]
- Michalska, A.; Łysiak, G. Bioactive Compounds of Blueberries: Post-Harvest Factors Influencing the Nutritional Value of Products. Int. J. Mol. Sci. 2015, 16, 18642–18663. [Google Scholar] [CrossRef]
- Kuntz, S.; Kunz, C.; Rudloff, S. Inhibition of pancreatic cancer cell migration by plasma anthocyanins isolated from healthy volunteers receiving an anthocyanin-rich berry juice. Eur. J. Nutr. 2017, 56, 203–214. [Google Scholar] [CrossRef] [PubMed]
- Mendelová, A.; Mendel, Ľ.; Fikselová, M.; Czako, P. Evaluation of anthocynin changes in blueberries and in blueberry jam after the processing and storage. Potravin. Slovak J. Food Sci. 2013, 7, 130–135. [Google Scholar] [CrossRef]
- Wu, X.; Beecher, G.R.; Holden, J.M.; Haytowitz, D.B.; Gebhardt, S.E.; Prior, R.L. Concentrations of anthocyanins in common foods in the United States and estimation of normal consumption. J. Agric. Food Chem. 2006, 54, 4069–4975. [Google Scholar] [CrossRef]
- Skrovankova, S.; Sumczynski, D.; Mlcek, J.; Jurikova, T.; Sochor, J. Bioactive Compounds and Antioxidant Activity in Different Types of Berries. Int. J. Mol. Sci. 2015, 16, 24673–24706. [Google Scholar] [CrossRef]
- Casas-Forero, N.; Orellana-Palma, P.; Petzold, G. Comparative Study of the Structural Properties, Color, Bioactive Compounds Content and Antioxidant Capacity of Aerated Gelatin Gels Enriched with Cryoconcentrated Blueberry Juice during Storage. Polymers 2020, 12, 2769. [Google Scholar] [CrossRef]
- Zorzi, M.; Gai, F.; Medana, C.; Aigotti, R.; Morello, S.; Peiretti, P.G. Bioactive Compounds and Antioxidant Capacity of Small Berries. Foods 2020, 9, 623. [Google Scholar] [CrossRef]
- Huang, W.Y.; Zhang, H.C.; Liu, W.X.; Li, C.Y. Survey of antioxidant capacity and phenolic composition of blueberry, blackberry, and strawberry in Nanjing. J. Zhejiang Univ. Sci. B 2012, 13, 94–102. [Google Scholar] [CrossRef]
- Wood, E.; Hein, S.; Heiss, C.; Williams, C.; Rodriguez-Mateos, A. Blueberries and cardiovascular disease prevention. Food Funct. 2019, 10, 7621–7633. [Google Scholar] [CrossRef] [PubMed]
- Azari, H.; Morovati, A.; Pourghassem Gargari, B.; Sarbakhsh, P. Beneficial effects of blueberry supplementation on the components of metabolic syndrome: A systematic review and meta-analysis. Food Funct. 2022, 13, 4875–4900. [Google Scholar] [CrossRef]
- Kolehmainen, M.; Mykkänen, O.; Kirjavainen, P.V.; Leppänen, T.; Moilanen, E.; Adriaens, M.; Laaksonen, D.E.; Hallikainen, M.; Puupponen-Pimiä, R.; Pulkkinen, L.; et al. Bilberries reduce low-grade inflammation in individuals with features of metabolic syndrome. Mol. Nutr. Food Res. 2012, 56, 1501–1510. [Google Scholar] [CrossRef] [PubMed]
- Stull, A.J.; Cash, K.C.; Johnson, W.D.; Champagne, C.M.; Cefalu, W.T. Bioactives in blueberries improve insulin sensitivity in obese, insulin-resistant men and women. J. Nutr. 2010, 140, 1764–1768. [Google Scholar] [CrossRef]
- Niroumand, S.; Khajedaluee, M.; Khadem-Rezaiyan, M.; Abrishami, M.; Juya, M.; Khodaee, G.; Dadgarmoghaddam, M. Atherogenic Index of Plasma (AIP): A marker of cardiovascular disease. Med. J. Islam. Repub. Iran. 2015, 29, 240. [Google Scholar] [PubMed]
- Huang, H.; Chen, G.; Liao, D.; Zhu, Y.; Xue, X. Effects of Berries Consumption on Cardiovascular Risk Factors: A Meta-analysis with Trial Sequential Analysis of Randomized Controlled Trials. Sci. Rep. 2016, 6, 23625. [Google Scholar] [CrossRef]
- Grohmann, T.; Litts, C.; Horgan, G.; Zhang, X.; Hoggard, N.; Russell, W.; de Roos, B. Efficacy of Bilberry and Grape Seed Extract Supplement Interventions to Improve Glucose and Cholesterol Metabolism and Blood Pressure in Different Populations—A Systematic Review of the Literature. Nutrient 2021, 13, 1692. [Google Scholar] [CrossRef]
- Ridker, P.M.; Rifai, N.; Rose, L.; Buring, J.E.; Cook, N.R. Comparison of C-reactive protein and low-density lipoprotein cholesterol levels in the prediction of first cardiovascular events. N. Engl. J. Med. 2002, 347, 1557–1565. [Google Scholar] [CrossRef]
- Cao, X.; Wang, D.; Zhou, J.; Chen, Z. Comparison of lipoprotein derived indices for evaluating cardio-metabolic risk factors and subclinical organ damage in middle-aged Chinese adults. Clin. Chim. Acta 2017, 475, 22–27. [Google Scholar] [CrossRef]
- Fernández-Aparicio, Á.; Perona, J.S.; Schmidt-RioValle, J.; Padez, C.; González-Jiménez, E. Assessment of Different Atherogenic Indices as Predictors of Metabolic Syndrome in Spanish Adolescents. Biol. Res. Nurs. 2022, 24, 163–171. [Google Scholar] [CrossRef]
- Calling, S.; Johansson, S.E.; Wolff, M.; Sundquist, J.; Sundquist, K. The ratio of total cholesterol to high density lipoprotein cholesterol and myocardial infarction in Women’s health in the Lund area (WHILA): A 17-year follow-up cohort study. BMC Cardiovasc. Disord. 2019, 19, 239. [Google Scholar] [CrossRef]
- Sun, T.; Chen, M.; Shen, H.; Yin, P.; Fan, L.; Chen, X.; Wu, J.; Xu, Z.; Zhang, J. Predictive value of LDL/HDL ratio in coronary atherosclerotic heart disease. BMC Cardiovasc. Disord. 2022, 22, 273. [Google Scholar] [CrossRef]
- Oravec, S.; Dukat, A.; Gavornik, P.; Kucera, M.; Gruber, K.; Gaspar, L.; Rizzo, M.; Toth, P.P.; Mikhailidis, D.P.; Banach, M. Atherogenic versus non-atherogenic lipoprotein profiles in healthy individuals. is there a need to change our approach to diagnosing dyslipidemia? Curr. Med. Chem. 2014, 21, 2892–2901. [Google Scholar] [CrossRef]
- Kasko, M.; Gaspar, L.; Dukát, A.; Gavorník, P.; Oravec, S. High-density lipoprotein profile in newly-diagnosed lower extremity artery disease in Slovak population without diabetes mellitus. Neuro Endocrinol. Lett. 2014, 35, 531–535. [Google Scholar]
- Zhang, X.; van der Vorst, E.P.C. High-Density Lipoprotein Modifications: Causes and Functional Consequences in Type 2 Diabetes Mellitus. Cells 2024, 13, 1113. [Google Scholar] [CrossRef]
- Lee, C.-K.; Liao, C.-W.; Meng, S.-W.; Wu, W.-K.; Chiang, J.-Y.; Wu, M.-S. Lipids and Lipoproteins in Health and Disease: Focus on Targeting Atherosclerosis. Biomedicines 2021, 9, 985. [Google Scholar] [CrossRef]
- Lorey, M.B.; Öörni, K.; Kovanen, P.T. Modified Lipoproteins Induce Arterial Wall Inflammation During Atherogenesis. Front. Cardiovasc. Med. 2022, 9, 841545. [Google Scholar] [CrossRef]
- Vekic, J.; Zeljkovic, A.; Cicero, A.F.G.; Janez, A.; Stoian, A.P.; Sonmez, A.; Rizzo, M. Atherosclerosis Development and Progression: The Role of Atherogenic Small, Dense LDL. Medicina 2022, 58, 299. [Google Scholar] [CrossRef]
- Basu, A.; Fu, D.X.; Wilkinson, M.; Simmons, B.; Wu, M.; Betts, N.M.; Du, M.; Lyons, T.J. Strawberries decrease atherosclerotic markers in subjects with metabolic syndrome. Nutr. Res. 2010, 30, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Habanova, M.; Saraiva, J.A.; Holovicova, M.; Moreira, S.A.; Fidalgo, L.G.; Haban, M.; Gazo, J.; Schwarzova, M.; Chlebo, P.; Bronkowska, M. Effect of berries/apple mixed juice consumption on the positive modulation of human lipid profile. J. Funct. Foods 2019, 60, 103417. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameters | Bilberry Juice | Dietary Fibre of Bilberry |
|---|---|---|
| Total phenolic content | 2.29 ± 0.01(mg GAE 1/mL) | 32.81 ± 0.15 (mg GAE 1/g) |
| Total anthocyanins | 1.48 ± 0.03 (mg/mL) | 6.82 ± 0.06 (mg/g) |
| Vitamin C | 126.40 ± 0.13 (µg/mL) | 1.44 ± 0.12 (µg/g) |
| Caffeic acid | 24.87 ± 0.41 (mg/L) | 85.47 ± 0.31 (mg/g) |
| Coumaric acid | 28.59 ± 1.57 (mg/L) | 125.35 ± 0.26 (mg/g) |
| Ferric acid | 123.11 ± 0.83 (mg/L) | 77.94 ± 0.21 (mg/g) |
| Rutin | 309.95 ± 1.27 (mg/L) | 24.21 ± 0.08 (mg/g) |
| Myricetin | 34.66 ± 1.73 (mg/L) | 52.79 ± 0.44 (mg/g) |
| Resveratrol | 9.50 ± 0.74 (mg/L) | 30.15 ± 0.39 (mg/g) |
| Quercetin | 5.44 ± 0.04 (mg/L) | 53.45 ± 1.05 (mg/g) |
| Antioxidant activity 2 | 49.30 ± 0.56 (%) | 67.20 ± 0.41 (%) |
| Parameter | 100% Bilberry Juice (n = 15) | Dietary Fibre of Bilberry (n = 15) | ||||
|---|---|---|---|---|---|---|
| Pre | Post | p | Pre | Post | p | |
| Body weight (kg) | 80.14 ± 11.86 | 80.17 ± 11.97 | 0.853 | 80.56 ± 8.68 | 81.09 ± 9.12 | 0.116 |
| BMI (kg/m2) | 29.89 ± 3.75 | 29.90 ± 3.81 | 0.842 | 29.52 ± 3.06 | 29.71 ± 3.13 | 0.125 |
| WC (cm) | 103.39 ± 10.49 | 104.21 ± 9.85 | 0.084 | 100.93 ± 7.11 | 101.66 ± 7.52 | 0.083 |
| WHR index | 1.00 ± 0.06 | 1.01 ± 0.05 | 0.073 | 0.97 ± 0.05 | 0.98 ± 0.05 | 0.086 |
| SMM (kg) | 24.99 ± 2.57 | 25.12 ± 2.51 | 0.151 | 26.76 ± 3.33 | 26.86 ± 3.30 | 0.388 |
| FFM (kg) | 45.78 ± 4.48 | 45.6 ± 4.41 | 0.334 | 48.59 ± 5.61 | 48.77 ± 5.54 | 0.313 |
| FFM (%) | 57.39 ± 4.10 | 57.66 ± 4.26 | 0.256 | 60.48 ± 4.83 | 60.33 ± 4.73 | 0.516 |
| BFM (kg) | 34.08 ± 8.40 | 33.98 ± 8.62 | 0.614 | 31.97 ± 5.92 | 32.32 ± 6.11 | 0.237 |
| PBF (%) | 42.44 ± 4.18 | 42.20 ± 4.39 | 0.274 | 39.53 ± 4.83 | 39.66 ± 4.74 | 0.561 |
| VFA (cm2) | 134.18 ± 26.46 | 134.56 ± 25.24 | 0.596 | 124.64 ± 18.99 | 126.59 ± 20.26 | 0.071 |
| SBP (mm Hg) | 126.93 ± 13.83 | 124.67 ± 11.73 | 0.271 | 129.80 ± 12.23 | 128.07 ± 11.93 | 0.508 |
| DBP (mm Hg) | 83.80 ± 6.93 | 82.20 ± 4.65 | 0.244 | 87.53 ± 6.52 | 86.87 ± 6.51 | 0.692 |
| Parameter | 100% Bilberry Juice (n = 15) | Dietary Fibre of Bilberry (n = 15) | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post | p | Pre | Post | p | RV | |
| TC (mmol/L) | 6.41 ± 1.23 | 6.94 ± 1.30 | <0.001 | 6.06 ± 1.39 | 6.43 ± 1.05 | 0.046 | 3–5.2 |
| TG (mmol/L) | 1.34 ± 0.50 | 1.38 ± 0.47 | 0.721 | 1.41 ± 0.65 | 1.39 ± 0.68 | 0.880 | <1.7 |
| LDL-C (mmol/L) | 3.70 ± 0.94 | 3.42 ± 1.00 | 0.010 | 3.56 ± 0.81 | 3.08 ± 0.62 | 0.001 | <2.6 |
| HDL-C (mmol/L) | 1.78 ± 0.32 | 2.11 ± 0.38 | <0.001 | 1.60 ± 0.43 | 1.92 ± 0.52 | <0.001 | >1.3 |
| TC/HDL | 3.69 ± 0.92 | 3.33 ± 0.63 | 0.006 | 3.92 ± 0.90 | 3.48 ± 0.72 | <0.001 | <4 |
| LDL/HDL | 2.15 ± 0.71 | 1.65 ± 0.49 | <0.001 | 2.34 ± 0.71 | 1.69 ± 0.49 | <0.001 | <2.5 |
| AIP | −0.14 ± 0.21 | −0.20 ± 0.18 | 0.152 | −0.08 ± 0.25 | −0.17 ± 0.26 | 0.061 | −0.3–0.1 |
| Parameter | 100% Bilberry Juice (n = 12) | Dietary Fibre of Bilberry (n = 9) | ||||
|---|---|---|---|---|---|---|
| Pre | Post | p | Pre | Post | p | |
| LDL Subfractions | ||||||
| VLDL (mmol/L) | 1.04 ± 0.20 | 1.19 ± 0.25 | 0.011 | 1.12 ± 0.30 | 1.25 ± 0.41 | 0.098 |
| IDL A (mmol/L) | 0.47 ± 0.22 | 0.75 ± 0.18 | <0.001 | 0.49 ± 0.27 | 0.60 ± 0.23 | 0.168 |
| IDL B (mmol/L) | 0.40 ± 0.16 | 0.51 ± 0.12 | 0.008 | 0.41 ± 5.15 | 0.51 ± 0.09 | 0.084 |
| IDL C (mmol/L) | 0.85 ± 0.24 | 0.63 ± 0.45 | 0.041 | 0.81 ± 0.23 | 0.70 ± 0.15 | 0.246 |
| LDL 1 (mmol/L) | 1.07 ± 0.32 | 1.35 ± 0.35 | 0.009 | 1.04 ± 0.36 | 1.13 ± 0.18 | 0.430 |
| LDL 2 (mmol/L) | 0.87 ± 0.35 | 0.75 ± 0.42 | 0.088 | 0.90 ± 0.28 | 0.84 ± 0.43 | 0.937 |
| LDL 3-7 (mmol/L) | 0.26 ± 0.23 | 0.11 ± 0.16 | 0.016 | 0.31 ± 0.32 | 0.24 ± 0.31 | 0.261 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Habanova, M.; Bihari, M.; Latal, R.; Gažarova, M.; Lenártová, P.; Pastrnakova, J.; Hamulka, J. Short-Term Supplementation with 100% Bilberry Products and Its Effects on Body Composition and Lipid Profile in Overweight/Obese Women. Metabolites 2025, 15, 218. https://doi.org/10.3390/metabo15040218
Habanova M, Bihari M, Latal R, Gažarova M, Lenártová P, Pastrnakova J, Hamulka J. Short-Term Supplementation with 100% Bilberry Products and Its Effects on Body Composition and Lipid Profile in Overweight/Obese Women. Metabolites. 2025; 15(4):218. https://doi.org/10.3390/metabo15040218
Chicago/Turabian StyleHabanova, Marta, Maros Bihari, Radek Latal, Martina Gažarova, Petra Lenártová, Jana Pastrnakova, and Jadwiga Hamulka. 2025. "Short-Term Supplementation with 100% Bilberry Products and Its Effects on Body Composition and Lipid Profile in Overweight/Obese Women" Metabolites 15, no. 4: 218. https://doi.org/10.3390/metabo15040218
APA StyleHabanova, M., Bihari, M., Latal, R., Gažarova, M., Lenártová, P., Pastrnakova, J., & Hamulka, J. (2025). Short-Term Supplementation with 100% Bilberry Products and Its Effects on Body Composition and Lipid Profile in Overweight/Obese Women. Metabolites, 15(4), 218. https://doi.org/10.3390/metabo15040218