

The Role of the Olfactory System in Obesity and Metabolism in Humans: A Systematic Review and Meta-Analysis


Abstract
1. Introduction
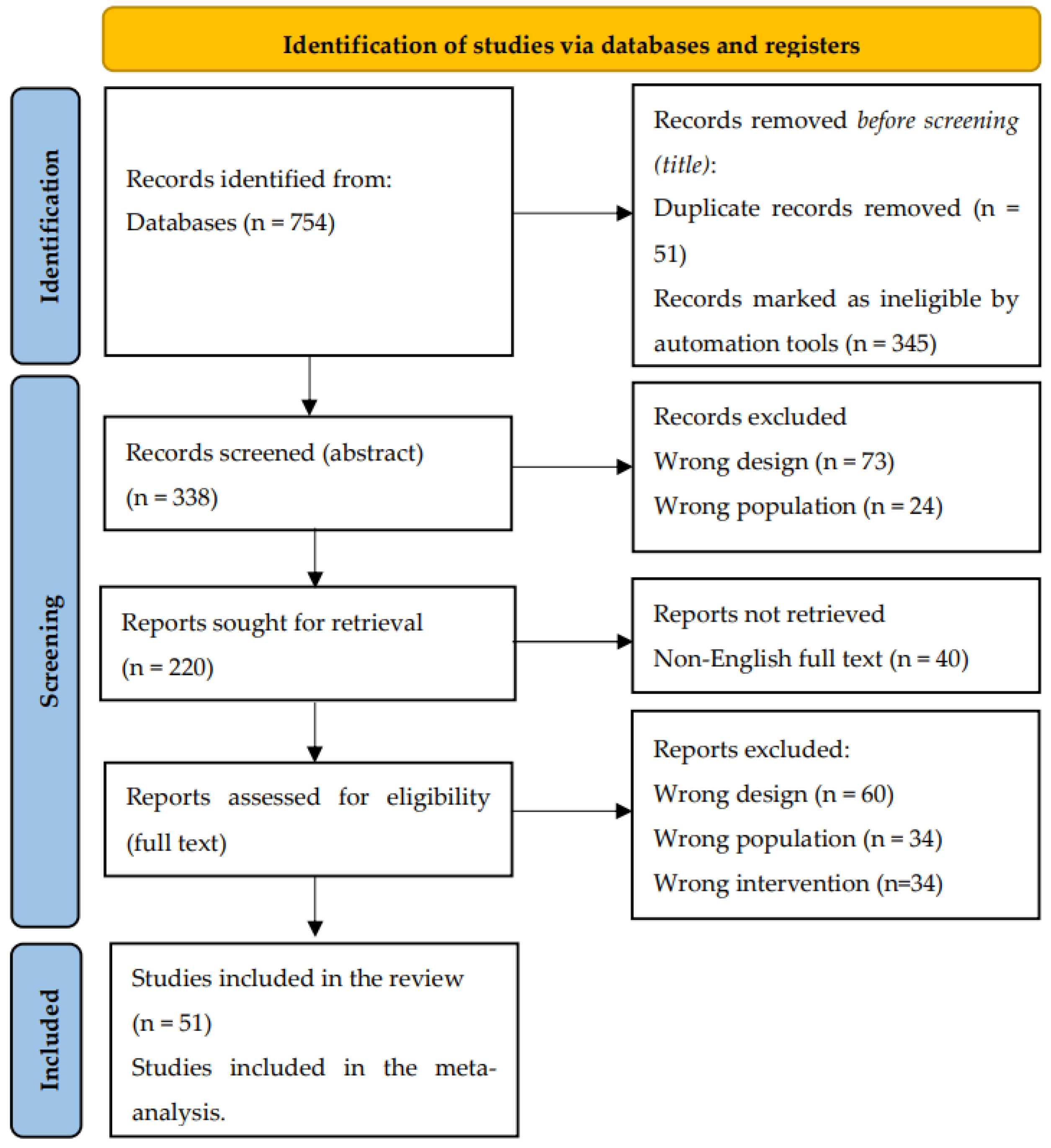
2. Materials and Methods
2.1. Source and Methods of Data Retrieval
2.2. Data Extraction
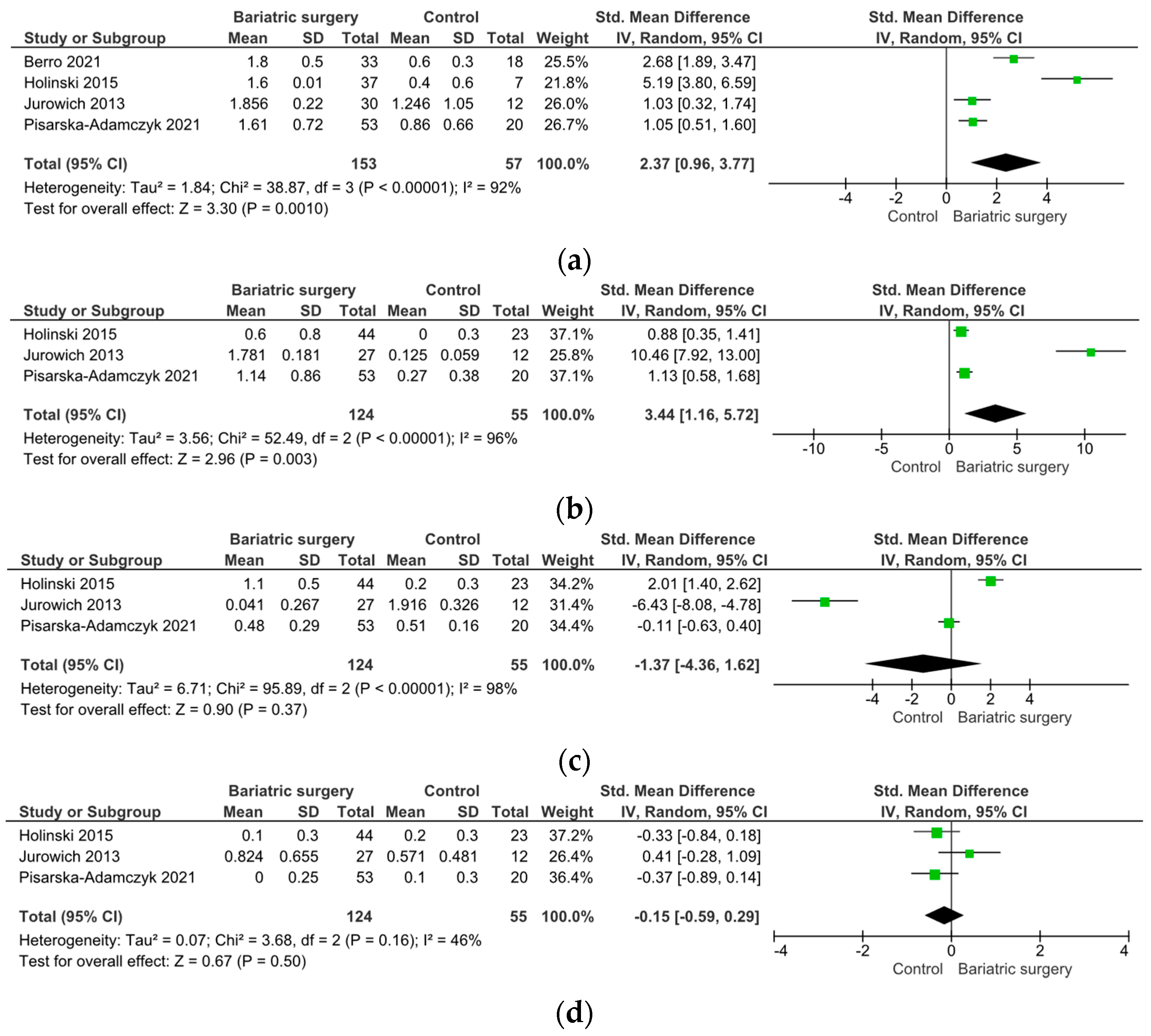
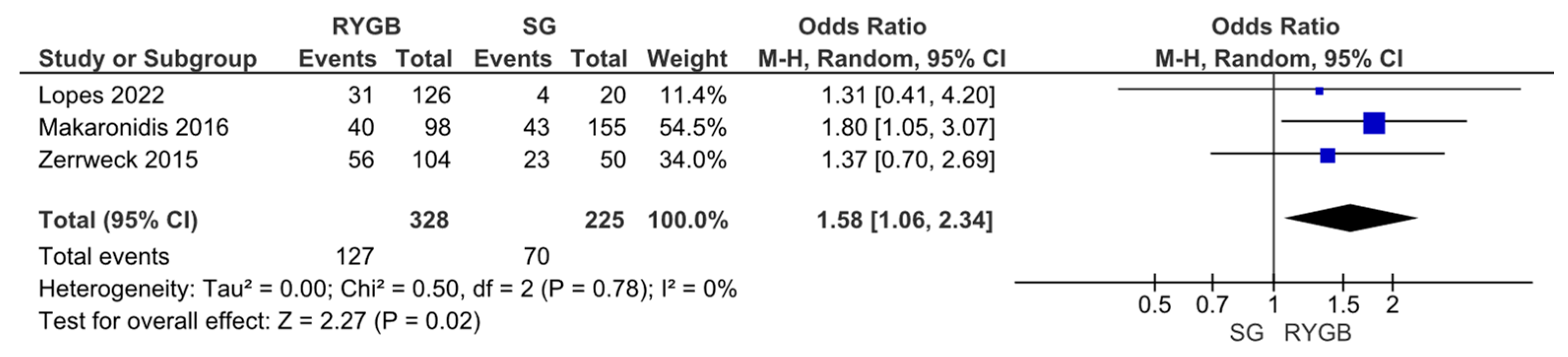
2.3. Meta-Analysis
3. Results
3.1. Variations in Olfactory Receptor Genes and Metabolism

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study and Number of Participants (N) Age y.o. BMI kg/m2 | Method | Chromosome Gene Variations SNPs | Positive Association | Negative Association |
|---|---|---|---|---|
| Choquette [68] 2012 N = 890 Age = 43.7 ± 16.8 y.o. BMI = 27.9 ± 7.6 kg/m2 | Direct sequencing in the Quebec Family Study | 19p13 OR7D4 c.-466 | No association | |
| 19p13 OR7D4 rs56139543 | VAT | |||
| 19p13 OR7D4 rs1235784 | TAT, SAT | |||
| 19p13 OR7D4 rs10421711 | Hunger | |||
| 19p13 OR7D4 rs2878329 | BMI, WC, BF, hunger, restraint | |||
| 19p13 OR7D4 rs61729907 | VAT | |||
| 19p13 OR7D4 rs5020278 | ||||
| 19p13 OR7D4 rs8109935 | Restraint, hunger, BMI, BF | |||
| 19p13 OR7D4 rs61732676 | No association | |||
| 19p13 OR7G1 rs7246980 | VAT | |||
| 19p13 OR7G3 rs10414255 | Hunger, BMI, BF | Restraint, | ||
| 19p13 OR7E24 rs2240927 | Disinhibition | |||
| Jarick [70] 2010 N = 453 N = 435 control | Genotyping by the Affymetrix Genome-Wide Human SNP Array 6.0 (PCR) | 11q11 OR4P4 rs9804659 | Obesity | |
| 11q11 OR4S2 | ||||
| 11q11 OR4C6 | ||||
| Ortega [76] 2016 N = 210 women BMI = 34 ± 12 kg/m2 N 52 = 16.5 ± 1.3 y.o., N 86 = 21.5 ± 2.8 y.o., N 72 = 41.1 ± 7.7 y.o. | Genotyped by means of allelic discrimination assays, using a LightCyclerR | TAS2R38 AVI/AVI haplotypes arraying | Non-smoker women showed decreased smelling sensitivity. No connection to BMI | |
| Ramos-Lopez [69] 2019 N = 474 Age = 47.2 ± 14.1 y.o. BMI = 30.1 ± 5.6 kg/m2 | Nutriepigenomic analysis from Methyl Epigenome Network Association | OR4D2 cg02874396 | BMI, WC, daily intakes of total energy, carbohydrates, protein, fat | |
| OR51A7 cg00467296 | BMI, WC | |||
| OR2T34 cg13441213 | ||||
| OR2Y1 cg18482656 | BMI, WC, daily intakes of total energy, carbohydrates, protein, fat | |||
| SLC8A1 cg19302979 | BMI, WC | |||
| SLC8A1 cg12498094 | ||||
| ANO2 cg10610428 | ||||
| PDE2A cg07736155 | ||||
| CALML3 cg17283169 | ||||
| GNG7 cg02849894 | ||||
| CALML6 cg15102821 | ||||
| CALML6 cg15819352 | ||||
| PRKG1 cg16401207 | ||||
| PRKG1 cg24609819 | ||||
| CAMK2D cg13801347 | ||||
| Sun [78] 2022 N= 301 N = 307 control Age = 53.51 ± 11.1 y.o. Age = 51.20 ± 14.5 y.o. control | Bio Miao Biological Technology (PCR) | 17 OR4D1 rs8071251 rs7218964 rs9908511 rs1075009 | Obesity, smoking | |
| 11 OR52K1 rs96489 rs331508 rs331510 rs4468345 | Obesity | |||
| 1 OR2L8 rs4925583 rs4925792 | Obesity | |||
| 10 CALML3 rs1131482 rs2231413 rs1142825 rs4072071 rs4072070 rs4589188 rs4589189 | Smoking | Obesity |
| Study and Number of Participants (N) | Method | Odorant Receptor Name | Pseudogene Allele Percentage | Resulting Odor to Be Detected | Natural Agonist |
|---|---|---|---|---|---|
| Mainland [75] 2013 N = 511 | For sequencing, human genomic DNA was amplified with HotStar Taq (Qiagen) | OR2B11 | 43% | 8-amino-acid protein | Cinnamaldehyde |
| OR4E2 | 30% | MAYDRY domain | Amyl acetate | ||
| OR8K3 | 24% | MAYDRY domain | (+)-menthol | ||
| OR10A6 | 22% | PMLNPLIY domain | 3-phenyl propyl propionate | ||
| OR2C1 | 4% | 272 amino acid protein | Octanethiol | ||
| OR4Q3 | 1.5% | 159 amino acid protein | Eugenol | ||
| OR10G7 | 1.4% | 191 amino acid protein | Eugenol | ||
| OR10G4 | guaiacol, vanillin and ethyl vanillin |
| Study and Number of Participants (N) | Method | Chromosome Odorant Receptor Variants (SNPs) | Related Odors to Be Detected |
|---|---|---|---|
| Eriksson [79] 2009 N = 22 studies | Genotyped on the Illumina HumanHap550+ BeadChip platform | 1 OR2M7 rs4481887 rs4309013 rs4244187 | Smell of asparagus metabolites in urine |
| Eriksson [80] 2012 N = 26691 | Genotyping by Beagle and Minimac | 11 OR6A2 rs72921001 | Aldehydes (cilantro) |
| Jaegaer [81] 2009 N = 48 | Microarray probe genotyping | 6 OR2W1 | Alcohols including 1-hexanol |
| 6 OR2J2 | |||
| 6 OR2J3 rs28757581 | Cis-3-hexen-1-ol (fruits, vegetables, white wine and processed foods) | ||
| 6 OR2J3 rs3749977 | |||
| Lunde [74] 2012 N = 23 | For sequencing, human genomic DNA was amplified with HotStar Taq (Qiagen) | OR7D4 rs61729907 | Androstenone (cooked pork) |
| OR7D4 rs5020278 | |||
| Menashe [82] 2007 N = 377 | Matrix-assisted laser desorption/ionization–time of flight (MALDI-TOF | OR11H7 | Isovaleric acid (sweaty odor) |
3.2. Olfactory Sensory Perception and Metabolism
3.3. Olfactory Function and Obesity
3.4. Olfactory Function and Bariatric Surgery
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Timper, K.; Brüning, J.C. Hypothalamic Circuits Regulating Appetite and Energy Homeostasis: Pathways to Obesity. Dis. Model. Mech. 2017, 10, 679–689. [Google Scholar] [CrossRef] [PubMed]
- Blüher, M. Obesity: Global Epidemiology and Pathogenesis. Nat. Rev. Endocrinol. 2019, 15, 288–298. [Google Scholar] [CrossRef] [PubMed]
- NCD Risk Factor Collaboration (NCD-RisC). Trends in Adult Body-Mass Index in 200 Countries from 1975 to 2014: A Pooled Analysis of 1698 Population-Based Measurement Studies with 19·2 Million Participants. Lancet 2016, 387, 1377–1396. [Google Scholar] [CrossRef] [PubMed]
- Abarca-Gómez, L.; Abdeen, Z.A.; Hamid, Z.A.; Abu-Rmeileh, N.M.; Acosta-Cazares, B.; Acuin, C.; Adams, R.J.; Aekplakorn, W.; Afsana, K.; Aguilar-Salinas, C.A.; et al. Worldwide Trends in Body-Mass Index, Underweight, Overweight, and Obesity from 1975 to 2016: A Pooled Analysis of 2416 Population-Based Measurement Studies in 128·9 Million Children, Adolescents, and Adults. Lancet 2017, 390, 2627–2642. [Google Scholar] [CrossRef] [PubMed]
- Noncommunicable Diseases. Available online: https://www.who.int/news-room/fact-sheets/detail/noncommunicable-diseases (accessed on 8 June 2022).
- Flegal, K.M.; Kit, B.K.; Orpana, H.; Graubard, B.I. Association of All-Cause Mortality with Overweight and Obesity Using Standard Body Mass Index Categories. JAMA 2013, 309, 71–82. [Google Scholar] [CrossRef] [PubMed]
- Farr, O.M.; Li, C.S.R.; Mantzoros, C.S. Central Nervous System Regulation of Eating: Insights from Human Brain Imaging. Metabolism 2016, 65, 699–713. [Google Scholar] [CrossRef] [PubMed]
- Val-Laillet, D.; Aarts, E.; Weber, B.; Ferrari, M.; Quaresima, V.; Stoeckel, L.E.; Alonso-Alonso, M.; Audette, M.; Malbert, C.H.; Stice, E. Neuroimaging and Neuromodulation Approaches to Study Eating Behavior and Prevent and Treat Eating Disorders and Obesity. Neuroimage Clin. 2015, 8, 1–31. [Google Scholar] [CrossRef]
- Weingarten, H.P. Conditioned Cues Elicit Feeding in Sated Rats: A Role for Learning in Meal Initiation. Science 1983, 220, 431–433. [Google Scholar] [CrossRef]
- Su, Z.; Alhadeff, A.L.; Betley, J.N. Nutritive, Post-Ingestive Signals Are the Primary Regulators of AgRP Neuron Activity. Cell Rep. 2017, 21, 2724–2736. [Google Scholar] [CrossRef]
- Petrovich, G.D.; Setlow, B.; Holland, P.C.; Gallagher, M. Amygdalo-Hypothalamic Circuit Allows Learned Cues to Override Satiety and Promote Eating. J. Neurosci. 2002, 22, 8748–8753. [Google Scholar] [CrossRef]
- Jovanovic, P.; Riera, C.E. Olfactory System and Energy Metabolism: A Two-Way Street. Trends Endocrinol. Metab. 2022, 33, 281–291. [Google Scholar] [CrossRef]
- Quarta, C.; Claret, M.; Zeltser, L.M.; Williams, K.W.; Yeo, G.S.H.; Tschöp, M.H.; Diano, S.; Brüning, J.C.; Cota, D. POMC Neuronal Heterogeneity in Energy Balance and beyond: An Integrated View. Nat. Metab. 2021, 3, 299–308. [Google Scholar] [CrossRef]
- Pager, J. Ascending Olfactory Information and Centrifugal Influxes Contributing to a Nutritional Modulation of the Rat Mitral Cell Responses. Brain Res. 1978, 140, 251–269. [Google Scholar] [CrossRef] [PubMed]
- Kelley, A.E.; Baldo, B.A.; Pratt, W.E.; Will, M.J. Corticostriatal-Hypothalamic Circuitry and Food Motivation: Integration of Energy, Action and Reward. Physiol. Behav. 2005, 86, 773–795. [Google Scholar] [CrossRef] [PubMed]
- Barrientos-Riosalido, A.; Bertran, L.; Vilaró-Blay, M.; Aguilar, C.; Martínez, S.; Paris, M.; Sabench, F.; Riesco, D.; Binetti, J.; Del Castillo, D.; et al. The Role of Olfactomedin 2 in the Adipose Tissue–Liver Axis and Its Implication in Obesity-Associated Nonalcoholic Fatty Liver Disease. Int. J. Mol. Sci. 2023, 24, 5221. [Google Scholar] [CrossRef] [PubMed]
- Sultana, A.; Nakaya, N.; Dong, L.; Abu-Asab, M.; Qian, H.; Tomarev, S.I. Deletion of Olfactomedin 2 Induces Changes in the AMPA Receptor Complex and Impairs Visual, Olfactory, and Motor Functions in Mice. Exp. Neurol. 2014, 261, 802–811. [Google Scholar] [CrossRef] [PubMed]
- González-García, I.; Freire-Agulleiro, Ó.; Nakaya, N.; Ortega, F.J.; Garrido-Gil, P.; Liñares-Pose, L.; Fernø, J.; Labandeira-Garcia, J.L.; Diéguez, C.; Sultana, A.; et al. Olfactomedin 2 Deficiency Protects against Diet-Induced Obesity. Metabolism 2022, 129, 155122. [Google Scholar] [CrossRef] [PubMed]
- López, M.; Fernández-Real, J.M.; Tomarev, S.I. Obesity Wars: May the Smell Be with You. Am. J. Physiol. Metab. 2023, 324, E569–E576. [Google Scholar] [CrossRef] [PubMed]
- Buck, L.; Axel, R. A Novel Multigene Family May Encode Odorant Receptors: A Molecular Basis for Odor Recognition. Cell 1991, 65, 175–187. [Google Scholar] [CrossRef]
- Olender, T.; Lancet, D.; Nebert, D.W. Update on the Olfactory Receptor (OR) Gene Superfamily. Hum. Genom. 2008, 3, 87–97. [Google Scholar] [CrossRef]
- Conrad, D.F.; Andrews, T.D.; Carter, N.P.; Hurles, M.E.; Pritchard, J.K. A High-Resolution Survey of Deletion Polymorphism in the Human Genome. Nat. Genet. 2006, 38, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Sollai, G.; Melis, M.; Tomassini Barbarossa, I.; Crnjar, R. A Polymorphism in the Human Gene Encoding OBPIIa Affects the Perceived Intensity of Smelled Odors. Behav. Brain Res. 2022, 427, 113860. [Google Scholar] [CrossRef] [PubMed]
- Richardson, B.E.; vander Woude, E.A.; Sudan, R.; Thompson, J.S.; Leopold, D.A. Altered Olfactory Acuity in the Morbidly Obese. Obes. Surg. 2004, 14, 967–969. [Google Scholar] [CrossRef] [PubMed]
- Peng, M.; Coutts, D.; Wang, T.; Cakmak, Y.O. Systematic Review of Olfactory Shifts Related to Obesity. Obes. Rev. 2019, 20, 325–338. [Google Scholar] [CrossRef] [PubMed]
- Fernández-Aranda, F.; Agüera, Z.; Fernández-García, J.C.; Garrido-Sanchez, L.; Alcaide-Torres, J.; Tinahones, F.J.; Giner-Bartolomé, C.; Baños, R.M.; Botella, C.; Cebolla, A.; et al. Smell–Taste Dysfunctions in Extreme Weight/Eating Conditions: Analysis of Hormonal and Psychological Interactions. Endocrine 2016, 51, 256–267. [Google Scholar] [CrossRef] [PubMed]
- Obrebowski, A.; Obrebowska-Karsznia, Z.; Gawliński, M. Smell and Taste in Children with Simple Obesity. Int. J. Pediatr. Otorhinolaryngol. 2000, 55, 191–196. [Google Scholar] [CrossRef] [PubMed]
- Simchen, U.; Koebnick, C.; Hoyer, S.; Issanchou, S.; Zunft, H.J.F. Odour and Taste Sensitivity Is Associated with Body Weight and Extent of Misreporting of Body Weight. Eur. J. Clin. Nutr. 2006, 60, 698–705. [Google Scholar] [CrossRef]
- Guild, A.A. Olfactory Acuity in Normal and Obese Human Subjects: Diurnal Variations and the Effect of D-Amphetamine Sulphate. J. Laryngol. Otol. 1956, 70, 408–414. [Google Scholar] [CrossRef]
- Thompson, D.A.; Moskowitz, H.R.; Campbell, R.G. Taste and Olfaction in Human Obesity. Physiol. Behav. 1977, 19, 335–337. [Google Scholar] [CrossRef]
- Stafford, L.D.; Welbeck, K. High Hunger State Increases Olfactory Sensitivity to Neutral but Not Food Odors. Chem. Senses 2011, 36, 189–198. [Google Scholar] [CrossRef]
- Stafford, L.D.; Whittle, A. Obese Individuals Have Higher Preference and Sensitivity to Odor of Chocolate. Chem. Senses 2015, 40, 279–284. [Google Scholar] [CrossRef] [PubMed]
- Skrandies, W.; Zschieschang, R. Olfactory and Gustatory Functions and Its Relation to Body Weight. Physiol. Behav. 2015, 142, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Llewellyn, C.; Wardle, J. Behavioral Susceptibility to Obesity: Gene-Environment Interplay in the Development of Weight. Physiol. Behav. 2015, 152, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Cecchetto, C.; Dal Bò, E.; Aiello, M.; Fischmeister, F.P.S.; Gentili, C.; Osimo, S.A. Alexithymia Modulates the Attitudes towards Odors but Not the Olfactory Abilities or the Affective Reactions to Odors. PLoS ONE 2023, 18, e0278496. [Google Scholar] [CrossRef] [PubMed]
- Zoon, H.F.A.; de Graaf, C.; Boesveldt, S. Food Odours Direct Specific Appetite. Foods 2016, 5, 12. [Google Scholar] [CrossRef] [PubMed]
- Fedoroff, I.; Polivy, J.; Peter Herman, C. The Specificity of Restrained versus Unrestrained Eaters’ Responses to Food Cues: General Desire to Eat, or Craving for the Cued Food? Appetite 2003, 41, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Ramaekers, M.G.; Boesveldt, S.; Gort, G.; Lakemond, C.M.M.; van Boekel, M.A.J.S.; Luning, P.A. Sensory-Specific Appetite Is Affected by Actively Smelled Food Odors and Remains Stable Over Time in Normal-Weight Women. J. Nutr. 2014, 144, 1314–1319. [Google Scholar] [CrossRef] [PubMed]
- Boesveldt, S.; de Graaf, K. The Differential Role of Smell and Taste for Eating Behavior. Perception 2017, 46, 307–319. [Google Scholar] [CrossRef]
- Yeomans, M.R. Olfactory Influences on Appetite and Satiety in Humans. Physiol. Behav. 2006, 87, 800–804. [Google Scholar] [CrossRef]
- Gaillet-Torrent, M.; Sulmont-Rossé, C.; Issanchou, S.; Chabanet, C.; Chambaron, S. Impact of a Non-Attentively Perceived Odour on Subsequent Food Choices. Appetite 2014, 76, 17–22. [Google Scholar] [CrossRef]
- Herrington, T.M.; Cheng, J.J.; Eskandar, E.N. Mechanisms of Deep Brain Stimulation. J. Neurophysiol. 2016, 115, 19–38. [Google Scholar] [CrossRef]
- Ramaekers, M.G.; Luning, P.A.; Ruijschop, R.M.A.J.; Lakemond, C.M.M.; Bult, J.H.F.; Gort, G.; Van Boekel, M.A.J.S. Aroma Exposure Time and Aroma Concentration in Relation to Satiation. Br. J. Nutr. 2014, 111, 554–562. [Google Scholar] [CrossRef] [PubMed]
- Ruijschop, R.M.A.J.; Boelrijk, A.E.M.; de Ru, J.A.; De Graaf, C.; Westerterp-Plantenga, M.S. Effects of Retro-Nasal Aroma Release on Satiation. Br. J. Nutr. 2008, 99, 1140–1148. [Google Scholar] [CrossRef] [PubMed]
- Betley, J.N.; Xu, S.; Cao, Z.F.H.; Gong, R.; Magnus, C.J.; Yu, Y.; Sternson, S.M. Neurons for Hunger and Thirst Transmit a Negative-Valence Teaching Signal. Nature 2015, 521, 180–185. [Google Scholar] [CrossRef] [PubMed]
- Brandt, C.; Nolte, H.; Henschke, S.; Engström Ruud, L.; Awazawa, M.; Morgan, D.A.; Gabel, P.; Sprenger, H.G.; Hess, M.E.; Günther, S.; et al. Food Perception Primes Hepatic ER Homeostasis via Melanocortin-Dependent Control of MTOR Activation. Cell 2018, 175, 1321–1335.e20. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.; Lin, Y.C.; Kuo, T.W.; Knight, Z.A. Sensory Detection of Food Rapidly Modulates Arcuate Feeding Circuits. Cell 2015, 160, 829–841. [Google Scholar] [CrossRef] [PubMed]
- Horio, N.; Liberles, S.D. Hunger Enhances Food-Odour Attraction through a Neuropeptide Y Spotlight. Nature 2021, 592, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Janet, R.; Fournel, A.; Fouillen, M.; Derrington, E.; Corgnet, B.; Bensafi, M.; Dreher, J.C. Cognitive and Hormonal Regulation of Appetite for Food Presented in the Olfactory and Visual Modalities. Neuroimage 2021, 230, 117811. [Google Scholar] [CrossRef] [PubMed]
- Rolls, E.T. Taste and Smell Processing in the Brain. In Handbook of Clinical Neurology; Elsevier: Amsterdam, The Netherlands, 2019; pp. 97–118. [Google Scholar]
- Kırgezen, T.; Yücetaş, U.; Server, E.A.; Övünç, O.; Yiğit, Ö. Possible Effects of Low Testosterone Levels on Olfactory Function in Males. Braz. J. Otorhinolaryngol. 2021, 87, 702–710. [Google Scholar] [CrossRef]
- Jung, H.J.; Shin, I.-S.; Lee, J.-E. Olfactory Function in Mild Cognitive Impairment and Alzheimer’s Disease: A Meta-Analysis. Laryngoscope 2019, 129, 362–369. [Google Scholar] [CrossRef]
- Rolls, E.T. Taste, Olfactory, and Food Reward Value Processing in the Brain. Prog. Neurobiol. 2015, 127–128, 64–90. [Google Scholar] [CrossRef] [PubMed]
- Ochner, C.N.; Kwok, Y.; Conceição, E.; Pantazatos, S.P.; Puma, L.M.; Carnell, S.; Teixeira, J.; Hirsch, J.; Geliebter, A. Selective Reduction in Neural Responses to High Calorie Foods Following Gastric Bypass Surgery. Ann. Surg. 2011, 253, 502–507. [Google Scholar] [CrossRef] [PubMed]
- Miras, A.D.; Jackson, R.N.; Jackson, S.N.; Goldstone, A.P.; Olbers, T.; Hackenberg, T.; Spector, A.C.; le Roux, C.W. Gastric Bypass Surgery for Obesity Decreases the Reward Value of a Sweet-Fat Stimulus as Assessed in a Progressive Ratio Task. Am. J. Clin. Nutr. 2012, 96, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.K. (Ed.) Essentials and Controversies in Bariatric Surgery; InTech: London, UK, 2014; ISBN 978-953-51-1726-1. [Google Scholar]
- Risk of Bias Tools—ROBINS-E Tool. Available online: https://www.riskofbias.info/welcome/robins-e-tool (accessed on 31 August 2023).
- O’Brien, P.E.; Hindle, A.; Brennan, L.; Skinner, S.; Burton, P.; Smith, A.; Crosthwaite, G.; Brown, W. Long-Term Outcomes After Bariatric Surgery: A Systematic Review and Meta-Analysis of Weight Loss at 10 or More Years for All Bariatric Procedures and a Single-Centre Review of 20-Year Outcomes After Adjustable Gastric Banding. Obes. Surg. 2019, 29, 3–14. [Google Scholar] [CrossRef] [PubMed]
- Wiggins, T.; Guidozzi, N.; Welbourn, R.; Ahmed, A.R.; Markar, S.R. Association of Bariatric Surgery with All-Cause Mortality and Incidence of Obesity-Related Disease at a Population Level: A Systematic Review and Meta-Analysis. PLoS Med. 2020, 17, e1003206. [Google Scholar] [CrossRef] [PubMed]
- Mechanick, J.I.; Apovian, C.; Brethauer, S.; Garvey, W.T.; Joffe, A.M.; Kim, J.; Kushner, R.F.; Lindquist, R.; Pessah-Pollack, R.; Seger, J.; et al. Clinical Practice Guidelines for the Perioperative Nutrition, Metabolic, and Nonsurgical Support of Patients Undergoing Bariatric Procedures—2019 Update: Cosponsored by American Association of Clinical Endocrinologists/American College of Endocrinology, the Obesity Society, American Society for Metabolic & Bariatric Surgery, Obesity Medicine Association, and American Society of Anesthesiologists—Executive Summary. Endocr. Pract. 2019, 25, 1346–1359. [Google Scholar] [CrossRef] [PubMed]
- Althumiri, N.A.; Basyouni, M.H.; Al-Qahtani, F.S.; Zamakhshary, M.; Bindhim, N.F. Food Taste, Dietary Consumption, and Food Preference Perception of Changes Following Bariatric Surgery in the Saudi Population: A Cross-Sectional Study. Nutrients 2021, 13, 3401. [Google Scholar] [CrossRef]
- Jennifer Traub, R. Taste Changes after Bariatric Surgery: What to Do When Your Patients Cannot Stand the Taste of Their Food. Bariatr. Times 2012, 9, 14–15. [Google Scholar]
- Reges, O.; Greenland, P.; Dicker, D.; Leibowitz, M.; Hoshen, M.; Gofer, I.; Rasmussen-Torvik, L.J.; Balicer, R.D. Association of Bariatric Surgery Using Laparoscopic Banding, Roux-En-Y Gastric Bypass, or Laparoscopic Sleeve Gastrectomy vs Usual Care Obesity Management with All-Cause Mortality. JAMA 2018, 319, 279–290. [Google Scholar] [CrossRef]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A Web and Mobile App for Systematic Reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef]
- RevMan|Cochrane Training. Available online: https://training.cochrane.org/online-learning/core-software/revman (accessed on 31 August 2023).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. PLoS Med. 2021, 18, e1003583. [Google Scholar] [CrossRef] [PubMed]
- Hasin-Brumshtein, Y.; Lancet, D.; Olender, T. Human Olfaction: From Genomic Variation to Phenotypic Diversity. Trends Genet. 2009, 25, 178–184. [Google Scholar] [CrossRef] [PubMed]
- Choquette, A.C.; Bouchard, L.; Drapeau, V.; Lemieux, S.; Tremblay, A.; Bouchard, C.; Vohl, M.C.; Pérusse, L. Association between Olfactory Receptor Genes, Eating Behavior Traits and Adiposity: Results from the Quebec Family Study. Physiol. Behav. 2012, 105, 772–776. [Google Scholar] [CrossRef] [PubMed]
- Ramos-Lopez, O.; Riezu-Boj, J.I.; Milagro, F.I.; Zulet, M.A.; Santos, J.L.; Martinez, J.A.; MENA Project. Associations between Olfactory Pathway Gene Methylation Marks, Obesity Features and Dietary Intakes. Genes. Nutr. 2019, 14, 11. [Google Scholar] [CrossRef] [PubMed]
- Jarick, I.; Vogel, C.I.G.; Scherag, S.; Schäfer, H.; Hebebrand, J.; Hinney, A.; Scherag, A. Novel Common Copy Number Variation for Early Onset Extreme Obesity on Chromosome 11q11 Identified by a Genome-Wide Analysis. Hum. Mol. Genet. 2011, 20, 840–852. [Google Scholar] [CrossRef] [PubMed]
- Vink, R.G.; Roumans, N.J.; Fazelzadeh, P.; Tareen, S.H.K.; Boekschoten, M.V.; Van Baak, M.A.; Mariman, E.C. Adipose Tissue Gene Expression Is Differentially Regulated with Different Rates of Weight Loss in Overweight and Obese Humans. Int. J. Obes. 2017, 41, 309–316. [Google Scholar] [CrossRef] [PubMed]
- Van Bussel, I.P.G.; Backx, E.M.P.; De Groot, C.P.G.M.; Tieland, M.; Müller, M.; Afman, L.A. The Impact of Protein Quantity during Energy Restriction on Genome-Wide Gene Expression in Adipose Tissue of Obese Humans. Int. J. Obes. 2017, 41, 1114–1120. [Google Scholar] [CrossRef]
- Spinelli, S.; Monteleone, E. Food Preferences and Obesity. Endocrinol. Metab. 2021, 36, 209–219. [Google Scholar] [CrossRef]
- Lunde, K.; Egelandsdal, B.; Skuterud, E.; Mainland, J.D.; Lea, T.; Hersleth, M.; Matsunami, H. Genetic Variation of an Odorant Receptor OR7D4 and Sensory Perception of Cooked Meat Containing Androstenone. PLoS ONE 2012, 7, e35259. [Google Scholar] [CrossRef]
- Mainland, J.D.; Keller, A.; Li, Y.R.; Zhou, T.; Trimmer, C.; Snyder, L.L.; Moberly, A.H.; Adipietro, K.A.; Liu, W.L.L.; Zhuang, H.; et al. The Missense of Smell: Functional Variability in the Human Odorant Receptor Repertoire. Nat. Neurosci. 2013, 17, 114–120. [Google Scholar] [CrossRef]
- Ortega, F.J.; Agüera, Z.; Sabater, M.; Moreno-Navarrete, J.M.; Alonso-Ledesma, I.; Xifra, G.; Botas, P.; Delgado, E.; Jimenez-Murcia, S.; Fernández-García, J.C.; et al. Genetic Variations of the Bitter Taste Receptor TAS2R38 Are Associated with Obesity and Impact on Single Immune Traits. Mol. Nutr. Food Res. 2016, 60, 1673–1683. [Google Scholar] [CrossRef] [PubMed]
- Pastor, A.; Fernández-Aranda, F.; Fitó, M.; Jiménez-Murcia, S.; Botella, C.; Fernández-Real, J.M.; Frühbeck, G.; Tinahones, F.J.; Fagundo, A.B.; Rodriguez, J.; et al. A Lower Olfactory Capacity Is Related to Higher Circulating Concentrations of Endocannabinoid 2-Arachidonoylglycerol and Higher Body Mass Index in Women. PLoS ONE 2016, 11, e0148734. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.; Li, S.; Ning, F.; Zhang, L.; Wang, W.; Duan, H.; Wu, Y. Association between Olfactory Pathway Gene Variants and Obesity in Chinese Han Population: A Case-Control Study Based on Genetic Score. Gene 2022, 825, 146442. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, N.; Macpherson, J.M.; Tung, J.Y.; Hon, L.S.; Naughton, B.; Saxonov, S.; Avey, L.; Wojcicki, A.; Pe’er, I.; Mountain, J. Web-Based, Participant-Driven Studies Yield Novel Genetic Associations for Common Traits. PLoS Genet. 2010, 6, e1000993. [Google Scholar] [CrossRef] [PubMed]
- Eriksson, N.; Wu, S.; Do, C.B.; Kiefer, A.K.; Tung, J.Y.; Mountain, J.L.; Hinds, D.A.; Francke, U. A Genetic Variant near Olfactory Receptor Genes Influences Cilantro Preference. Flavour 2012, 1, 22. [Google Scholar] [CrossRef]
- Jaeger, S.R.; McRae, J.F.; Salzman, Y.; Williams, L.; Newcomb, R.D. A Preliminary Investigation into a Genetic Basis for Cis-3-Hexen-1-Ol Odour Perception: A Genome-Wide Association Approach. Food Qual. Prefer. 2010, 21, 121–131. [Google Scholar] [CrossRef]
- Menashe, I.; Abaffy, T.; Hasin, Y.; Goshen, S.; Yahalom, V.; Luetje, C.W.; Lancet, D. Genetic Elucidation of Human Hyperosmia to Isovaleric Acid. PLoS Biol. 2007, 5, e284. [Google Scholar] [CrossRef]
- Massolt, E.T.; van Haard, P.M.; Rehfeld, J.F.; Posthuma, E.F.; van der Veer, E.; Schweitzer, D.H. Appetite Suppression through Smelling of Dark Chocolate Correlates with Changes in Ghrelin in Young Women. Regul. Pept. 2010, 161, 81–86. [Google Scholar] [CrossRef]
- Ketterer, C.; Heni, M.; Thamer, C.; Herzberg-Schäfer, S.A.; Häring, H.-U.; Fritsche, A. Acute, Short-Term Hyperinsulinemia Increases Olfactory Threshold in Healthy Subjects. Int. J. Obes. 2011, 35, 1135–1138. [Google Scholar] [CrossRef]
- Poessel, M.; Morys, F.; Breuer, N.; Villringer, A.; Hummel, T.; Horstmann, A. Brain Response to Food Odors Is Not Associated with Body Mass Index and Obesity-Related Metabolic Health Measures. Appetite 2022, 168, 105774. [Google Scholar] [CrossRef]
- Schöpf, V.; Kollndorfer, K.; Pollak, M.; Mueller, C.A.; Freiherr, J. Intranasal Insulin Influences the Olfactory Performance of Patients with Smell Loss, Dependent on the Body Mass Index: A Pilot Study. Rhinology 2015, 53, 371–378. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Brindisi, M.C.; Brondel, L.; Meillon, S.; Barthet, S.; Grall, S.; Fenech, C.; Liénard, F.; Schlich, P.; Astruc, K.; Mouillot, T.; et al. Proof of Concept: Effect of GLP-1 Agonist on Food Hedonic Responses and Taste Sensitivity in Poor Controlled Type 2 Diabetic Patients. Diabetes Metab. Syndr. Clin. Res. Rev. 2019, 13, 2489–2494. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zhang, B.; Wang, X.; Zhang, X.; Yang, Q.X.; Qing, Z.; Zhang, W.; Zhu, D.; Bi, Y. Olfactory Dysfunction Mediates Adiposity in Cognitive Impairment of Type 2 Diabetes: Insights from Clinical and Functional Neuroimaging Studies. Diabetes Care 2019, 42, 1274–1283. [Google Scholar] [CrossRef] [PubMed]
- Dicker, D.; Beck, A.; Markel, A.; Marcovicu, D.; Mazzawi, S.; Sarid, M.; Greenberg, E.; Atkinson, R.L. Weight Loss, Dietary Preferences, and Reduction in the Sense of Smell with the Use of a Novel Nasal Device. Obes. Facts 2020, 13, 473–486. [Google Scholar] [CrossRef] [PubMed]
- Boyce, J.M.; Shone, G.R. Effects of Ageing on Smell and Taste. Postgrad. Med. J. 2006, 82, 239–241. [Google Scholar] [CrossRef] [PubMed]
- Velluzzi, F.; Deledda, A.; Onida, M.; Loviselli, A.; Crnjar, R.; Sollai, G. Relationship between Olfactory Function and BMI in Normal Weight Healthy Subjects and Patients with Overweight or Obesity. Nutrients 2022, 14, 1262. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Wang, Y.; Liu, K.; Liu, R.; Tang, S.; Zhang, Q.; Ekström, I.; Laukka, E.J.; Du, Y.; Qiu, C. Olfactory Impairment Among Rural-Dwelling Chinese Older Adults: Prevalence and Associations with Demographic, Lifestyle, and Clinical Factors. Front. Aging Neurosci. 2021, 13, 621619. [Google Scholar] [CrossRef] [PubMed]
- Campolo, J.; Corradi, E.; Rizzardi, A.; Parolini, M.; Dellanoce, C.; Di Guglielmo, M.L.; Tarlarini, P.; Cattaneo, M.; Trivella, M.G.; De Maria, R. Correlates of Olfactory Impairment in Middle-Aged Non-Diabetic Caucasian Subjects with Stage I-II Obesity. Eur. Arch. Otorhinolaryngol. 2021, 278, 2047–2054. [Google Scholar] [CrossRef]
- Besser, G.; Erlacher, B.; Aydinkoc-tuzcu, K.; Liu, D.T.; Pablik, E.; Niebauer, V.; Koenighofer, M.; Renner, B.; Mueller, C.A. Body-Mass-Index Associated Differences in Ortho- and Retronasal Olfactory Function and the Individual Significance of Olfaction in Health and Disease. J. Clin. Med. 2020, 9, 366. [Google Scholar] [CrossRef]
- Fernandez-Garcia, J.C.; Alcaide, J.; Santiago-Fernandez, C.; Roca-Rodriguez, M.M.; Aguera, Z.; Baños, R.; Botella, C.; de La Torre, R.; Fernandez-Real, J.M.; Fruhbeck, G.; et al. An Increase in Visceral Fat Is Associated with a Decrease in the Taste and Olfactory Capacity. PLoS ONE 2017, 12, e0171204. [Google Scholar] [CrossRef]
- Rawal, S.; Duffy, V.B.; Berube, L.; Hayes, J.E.; Kant, A.K.; Li, C.M.; Graubard, B.I.; Hoffman, H.J. Self-Reported Olfactory Dysfunction and Diet Quality: Findings from the 2011-2014 National Health and Nutrition Examination Survey (NHANES). Nutrients 2021, 13, 4561. [Google Scholar] [CrossRef] [PubMed]
- Patel, Z.M.; Delgaudio, J.M.; Wise, S.K. Higher Body Mass Index Is Associated with Subjective Olfactory Dysfunction. Behav. Neurol. 2015, 2015, 675635. [Google Scholar] [CrossRef] [PubMed]
- Marty, L.; Bentivegna, H.; Nicklaus, S.; Monnery-Patris, S.; Chambaron, S. Non-Conscious Effect of Food Odors on Children’s Food Choices Varies by Weight Status. Front. Nutr. 2017, 4, 16. [Google Scholar] [CrossRef] [PubMed]
- Berro, C.; Pendolino, A.L.; Foletto, M.; Facciolo, M.C.; Maculan, P.; Prevedello, L.; Giuntoli, D.G.; Scarpa, B.; Pavan, C.; Andrews, P.J.; et al. Olfactory and Gustatory Function before and after Laparoscopic Sleeve Gastrectomy. Medicina 2021, 57, 913. [Google Scholar] [CrossRef] [PubMed]
- Enck, P.; Rieber, N.; Sauer, H.; Klosterhalfen, S.; Mack, I.; Zipfel, S.; Teufel, M. Almost Nothing—Not Even Bariatric Surgery for Obesity—Changes Olfactory Sensitivity. J. Res. Obes. 2014, 2014, 491890. [Google Scholar] [CrossRef][Green Version]
- Graham, L.; Murty, G.; Bowrey, D.J. Taste, Smell and Appetite Change After Roux-En-Y Gastric Bypass Surgery. Obes. Surg. 2014, 24, 1463–1468. [Google Scholar] [CrossRef] [PubMed]
- Guyot, E.; Dougkas, A.; Robert, M.; Nazare, J.-A.; Iceta, S.; Disse, E. Food Preferences and Their Perceived Changes Before and After Bariatric Surgery: A Cross-Sectional Study. Obes. Surg. 2021, 31, 3075–3082. [Google Scholar] [CrossRef]
- Hancı, D.; Altun, H.; Altun, H.; Batman, B.; Karip, A.B.; Serin, K.R. Laparoscopic Sleeve Gastrectomy Improves Olfaction Sensitivity in Morbidly Obese Patients. Obes. Surg. 2016, 26, 558–562. [Google Scholar] [CrossRef]
- Holinski, F.; Menenakos, C.; Haber, G.; Olze, H.; Ordemann, J. Olfactory and Gustatory Function After Bariatric Surgery. Obes. Surg. 2015, 25, 2314–2320. [Google Scholar] [CrossRef]
- Jurowich, C.F.; Seyfried, F.; Miras, A.D.; Bueter, M.; Deckelmann, J.; Fassnacht, M.; Germer, C.-T.; Thalheimer, A. Does Bariatric Surgery Change Olfactory Perception? Results of the Early Postoperative Course. Int. J. Color. Dis. 2014, 29, 253–260. [Google Scholar] [CrossRef]
- Lopes, K.G.; dos Santos, G.P.; Romagna, E.C.; Mattos, D.M.F.; Braga, T.G.; Cunha, C.B.; Maranhão, P.A.; Kraemer-Aguiar, L.G. Changes in Appetite, Taste, Smell, and Food Aversion in Post-Bariatric Patients and Their Relations with Surgery Time, Weight Loss and Regain. Eat. Weight Disord.-Stud. Anorex. Bulim. Obes. 2022, 27, 1679–1686. [Google Scholar] [CrossRef]
- Makaronidis, J.M.; Neilson, S.; Cheung, W.-H.; Tymoszuk, U.; Pucci, A.; Finer, N.; Doyle, J.; Hashemi, M.; Elkalaawy, M.; Adamo, M.; et al. Reported Appetite, Taste and Smell Changes Following Roux-En-Y Gastric Bypass and Sleeve Gastrectomy: Effect of Gender, Type 2 Diabetes and Relationship to Post-Operative Weight Loss. Appetite 2016, 107, 93–105. [Google Scholar] [CrossRef] [PubMed]
- Melis, M.; Pintus, S.; Mastinu, M.; Fantola, G.; Moroni, R.; Pepino, M.Y.; Tomassini Barbarossa, I. Changes of Taste, Smell and Eating Behavior in Patients Undergoing Bariatric Surgery: Associations with PROP Phenotypes and Polymorphisms in the Odorant-Binding Protein OBPIIa and CD36 Receptor Genes. Nutrients 2021, 13, 250. [Google Scholar] [CrossRef] [PubMed]
- Pisarska-Adamczyk, M.; Tylec, P.; Gajewska, N.; Wierzbicka, J.; Przęczek, K.; Małczak, P.; Wysocki, M.; Pędziwiatr, M.; Wierdak, M.; Major, P. Postoperative Olfaction Alteration following Laparoscopic Bariatric Surgery. J. Clin. Med. 2021, 10, 1704. [Google Scholar] [CrossRef] [PubMed]
- Richardson, B.E.; Vanderwoude, E.A.; Sudan, R.; Leopold, D.A.; Thompson, J.S. Gastric Bypass Does Not Influence Olfactory Function in Obese Patients. Obes. Surg. 2012, 22, 283–286. [Google Scholar] [CrossRef] [PubMed]
- Zerrweck, C.; Zurita, L.; Álvarez, G.; Maydón, H.G.; Sepúlveda, E.M.; Campos, F.; Caviedes, A.; Guilbert, L. Taste and Olfactory Changes Following Laparoscopic Gastric Bypass and Sleeve Gastrectomy. Obes. Surg. 2016, 26, 1296–1302. [Google Scholar] [CrossRef] [PubMed]
- Zerrweck, C.; Gallardo, V.C.; Calleja, C.; Sepúlveda, E.; Guilber, L. Gross Olfaction Before and After Laparoscopic Gastric Bypass. Obes. Surg. 2017, 27, 2988–2992. [Google Scholar] [CrossRef] [PubMed]
- Aschenbrenner, K.; Hummel, C.; Teszmer, K.; Krone, F.; Ishimaru, T.; Seo, H.S.; Hummel, T. The Influence of Olfactory Loss on Dietary Behaviors. Laryngoscope 2008, 118, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Bushdid, C.; Magnasco, M.O.; Vosshall, L.B.; Keller, A. Humans Can Discriminate More than 1 Trillion Olfactory Stimuli. Science 2014, 343, 1370–1372. [Google Scholar] [CrossRef]
- Gerkin, R.C.; Castro, J.B. The Number of Olfactory Stimuli That Humans Can Discriminate Is Still Unknown. eLife 2015, 4, e08127. [Google Scholar] [CrossRef]
- Niimura, Y. Olfactory Receptor Multigene Family in Vertebrates: From the Viewpoint of Evolutionary Genomics. Curr. Genom. 2012, 13, 103–114. [Google Scholar] [CrossRef]
- Niimura, Y.; Nei, M. Comparative Evolutionary Analysis of Olfactory Receptor Gene Clusters between Humans and Mice. Gene 2005, 346, 13–21. [Google Scholar] [CrossRef]
- Mariman, E.C.M.; Szklarczyk, R.; Bouwman, F.G.; Aller, E.E.J.G.; van Baak, M.A.; Wang, P. Olfactory Receptor Genes Cooperate with Protocadherin Genes in Human Extreme Obesity. Genes. Nutr. 2015, 10, 465. [Google Scholar] [CrossRef] [PubMed]
- Kang, N.N.; Koo, J.H. Olfactory Receptors in Non-Chemosensory Tissues. BMB Rep. 2012, 45, 612–622. [Google Scholar] [CrossRef] [PubMed]
- Allerton, T.D.; Primeaux, S.D. High-Fat Diet Differentially Regulates Metabolic Parameters in Obesity-Resistant S5B/Pl Rats and Obesity-Prone Osborne-Mendel Rats. Can. J. Physiol. Pharmacol. 2016, 94, 206–215. [Google Scholar] [CrossRef] [PubMed]
- Simola, M.; Malmberg, H. Sense of Smell in Allergic and Nonallergic Rhinitis. Allergy Eur. J. Allergy Clin. Immunol. 1998, 53, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Kutlug, S.; Gunbey, E.; Sogut, A.; Celiksoy, M.H.; Kardas, S.; Yildirim, U.; Karli, R.; Murat, N.; Sancak, R. Evaluation of Olfactory Function in Children with Allergic Rhinitis and Nonallergic Rhinitis. Int. J. Pediatr. Otorhinolaryngol. 2016, 86, 172–176. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.; Luo, F.; Han, Y.; Lou, H.; Tang, X.; Zhang, L. Obesity/Overweight and Risk of Allergic Rhinitis: A Meta-Analysis of Observational Studies. Allergy 2020, 75, 1272–1275. [Google Scholar] [CrossRef] [PubMed]
- Cain, W.S.; Gent, J.F. Olfactory Sensitivity: Reliability, Generality, and Association with Aging. J. Exp. Psychol. Hum. Percept. Perform. 1991, 17, 382–391. [Google Scholar] [CrossRef] [PubMed]
- Velluzzi, F.; Deledda, A.; Lombardo, M.; Fosci, M.; Crnjar, R.; Grossi, E.; Sollai, G. Application of Artificial Neural Networks (ANN) to Elucidate the Connections among Smell, Obesity with Related Metabolic Alterations, and Eating Habit in Patients with Weight Excess. Metabolites 2023, 13, 206. [Google Scholar] [CrossRef]
- Trellakis, S.; Tagay, S.; Fischer, C.; Rydleuskaya, A.; Scherag, A.; Bruderek, K.; Schlegl, S.; Greve, J.; Canbay, A.E.; Lang, S.; et al. Ghrelin, Leptin and Adiponectin as Possible Predictors of the Hedonic Value of Odors. Regul. Pept. 2011, 167, 112–117. [Google Scholar] [CrossRef] [PubMed]
- Hummel, T.; Sekinger, B.; Wolf, S.R.; Pauli, E.; Kobal, G. ‘Sniffin’ Sticks’: Olfactory Performance Assessed by the Combined Testing of Odour Identification, Odor Discrimination and Olfactory Threshold. Chem. Senses 1997, 22, 39–52. [Google Scholar] [CrossRef] [PubMed]
- Doty, R.L.; Shaman, P.; Kimmelman, C.P.; Dann, M.S. University of Pennsylvania Smell Identification Test: A Rapid Quantitative Olfactory Function Test for the Clinic. Laryngoscope 1984, 94, 176–178. [Google Scholar] [CrossRef] [PubMed]
- Duff, K.; McCaffrey, R.J.; Solomon, G.S. The Pocket Smell Test. J. Neuropsychiatry Clin. Neurosci. 2002, 14, 197–201. [Google Scholar] [CrossRef] [PubMed]
- Doty, R.L.; Marcus, A.; William Lee, W. Development of the 12-Item Cross-Cultural Smell Identification Test(CC-SIT). Laryngoscope 1996, 106, 353–356. [Google Scholar] [CrossRef] [PubMed]
- Qi, W.; Feng, L.; Yang, F.; Ma, W. Effects of Age on Recovery of Olfactory Function After Endoscopic Sinus Surgery and Related Risk Factors. Ear Nose Throat J. 2021, 102, 530–537. [Google Scholar] [CrossRef] [PubMed]
- Chiarotto, A.; Maxwell, L.J.; Ostelo, R.W.; Boers, M.; Tugwell, P.; Terwee, C.B. Measurement Properties of Visual Analogue Scale, Numeric Rating Scale, and Pain Severity Subscale of the Brief Pain Inventory in Patients with Low Back Pain: A Systematic Review. J. Pain 2019, 20, 245–263. [Google Scholar] [CrossRef] [PubMed]
- Facco, E.; Stellini, E.; Bacci, C.; Manani, G.; Pavan, C.; Cavallin, F.; Zanette, G. Validation of Visual Analogue Scale for Anxiety (VAS-A) in Preanesthesia Evaluation. Minerva Anestesiol. 2013, 79, 1389–1395. [Google Scholar]







| Study, Year Number of Participants (N) Age (Mean) BMI (kg/m2) | Design | Type of Surgery | Type of Olfactory Function Assessment | Follow-Up (Months) | Bariatric Surgery Group (N, BMI) | Control Group (N, BMI) |
|---|---|---|---|---|---|---|
| Berro, 2021 [99] N = 34 Age = 46.4 y.o. | Prospective longitudinal study | LSG | TDI | 6 | N = 18 BMI = 42.6 kg/m2 | N = 16 BMI = 43.1 kg/m2 |
| Enck, 2014 [100] N = 8 Age = 47.6 y.o. | Repeated measures design | SG | TDI | 12 | N = 8 Age = 47.6 y.o. | - |
| Graham, 2014 [101] N = 103 Age = 45 y.o. | Retrospective cohort study | RYGB | VAS | 12 & ≥36 | N = 103 BMI = 51 [36–97] kg/m2 | - |
| Guyot, 2021 [102] N = 220 Age = 41.0 y.o. BMI = 42.3 kg/m2 | Cross-sectional Study | RYGB, 56% had an SG, and 12% had other procedures Omega-loop gastric bypass N = 16 Gastric band N = 6 Fundoplication N = 2 Banded gastric bypass N = 1 Biliopancreatic derivation with duodenal Switch N = 1 Single anastomosis duodenum–ileal bypass (N = 1) | VAS | 24 | N = 220 BMI = 42.3 [30.4–64.6] kg/m2 | |
| Hanci, 2015 [103] N = 54 Age = 37.1 y.o. BMI 44.8 kg/m2 | Prospective cohort design | SG | TDI | 6 | N = 54 BMI 44.8 kg/m2 [30.5–63.0] kg/m2 | - |
| Holinski, 2015 [104] N = 67 Age = 47.1 y.o. | Prospective cohort study | AGB, SG, RYGB | TDI | 6 | N = 44 BMI = 48.6 kg/m2 | N = 23 BMI = 23.4 kg/m2 |
| Jurowich, 2013 [105] N = 42 Age = 43.4 y.o. BMI = 51.70 ± 7.36 kg/m2 | Prospective case–control observational study | RYGB, SG | TDI | 6 | RYGB N = 15 BMI = 48.7 ± 5.3 kg/m2 SG = 15 BMI = 56.0 ± 6.2 kg/m2 | N = 12 BMI = 49.49 ± 4.73 kg/m2 |
| Lopes, 2022 [106] N = 151 Age = 42 y.o. BMI = 32.6 km/m2 | Prospective observational study | RYGB, SG | VAS | 12 | RYGB N = 126 BMI = 32.7 kg/m2 SG N = 20 BMI = 32.0 kg/m2 | |
| Makaronidis, 2016 [107] N = 253 Age = 45.4 y.o. | Prospective observational study | RYGB, SG | VAS | 6–60 | RYGB N = 98 BMI = 44.7 kg/m2 SG N = 155 BMI = 46.1 kg/m2 | - |
| Melis, 2021 [108] N = 51 Age = 44.6 y.o. BMI = 43.0 kg/m2 | Prospective cohort study. | RYGB, SG, mGB | TDI | 6 | N = 51 BMI = 43.0 kg/m2 | - |
| Pisarska-Adamczyk, 2011 [109] N = 88 Age = 46.6 y.o. | Prospective study | RYGB, SG | TDI | 6 | N = 53 BMI = 45.4 kg/m2 | N = 35 BMI = 24.9 kg/m2 |
| Richardson, 2011 [110] N = 95 Age = 40.5 y.o. | Prospective study | RYGB + prophylactic cholecystectomy | CC-SIT | 6–12 | N = 55 | N = 40 (cholecystectomy) |
| Zerrweck, 2015 [111] N = 154 Age = 41.2 y.o. | Cohort study | RYGB, SG | VAS | 10 | LGBP N = 104 BMI = 43.3 kg/m2 LSG N = 50 BMI = 45.8 kg/m2 | - |
| Zerrweck2017 [112] N = 59 Age = 47.1 y.o. BMI = 46.9 km/m2 | Prospective cohort study | RYGB | PCT | 6 | N = 30 | N = 29 (nasofibroscopy) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matiashova, L.; Hoogkamer, A.L.; Timper, K. The Role of the Olfactory System in Obesity and Metabolism in Humans: A Systematic Review and Meta-Analysis. Metabolites 2024, 14, 16. https://doi.org/10.3390/metabo14010016
Matiashova L, Hoogkamer AL, Timper K. The Role of the Olfactory System in Obesity and Metabolism in Humans: A Systematic Review and Meta-Analysis. Metabolites. 2024; 14(1):16. https://doi.org/10.3390/metabo14010016
Chicago/Turabian StyleMatiashova, Lolita, Anouk Lisa Hoogkamer, and Katharina Timper. 2024. "The Role of the Olfactory System in Obesity and Metabolism in Humans: A Systematic Review and Meta-Analysis" Metabolites 14, no. 1: 16. https://doi.org/10.3390/metabo14010016
APA StyleMatiashova, L., Hoogkamer, A. L., & Timper, K. (2024). The Role of the Olfactory System in Obesity and Metabolism in Humans: A Systematic Review and Meta-Analysis. Metabolites, 14(1), 16. https://doi.org/10.3390/metabo14010016