

Therapeutic Physical Exercise Programs in the Context of NASH Cirrhosis and Liver Transplantation: A Systematic Review

 , , ,
, , , 
Abstract
1. Introduction
1.1. Sedentary Lifestyles and Physical Inactivity
1.2. Physical Activity in People with Type 2 Diabetes
1.3. “Personalized Physical Exercise Programs”: Definitions and Principles
1.4. The General Benefits of Personalized Physical Exercise Programs
1.4.1. Benefits for Overall Health
1.4.2. Benefits for the Liver
1.5. Patients with NASH Cirrhosis: Sarcopenia and a Sedentary Lifestyle
1.5.1. Physical Activity in the Setting of Liver Cirrhosis
1.5.2. Frailty before Liver Transplantation
1.5.3. Malnutrition and Sarcopenia
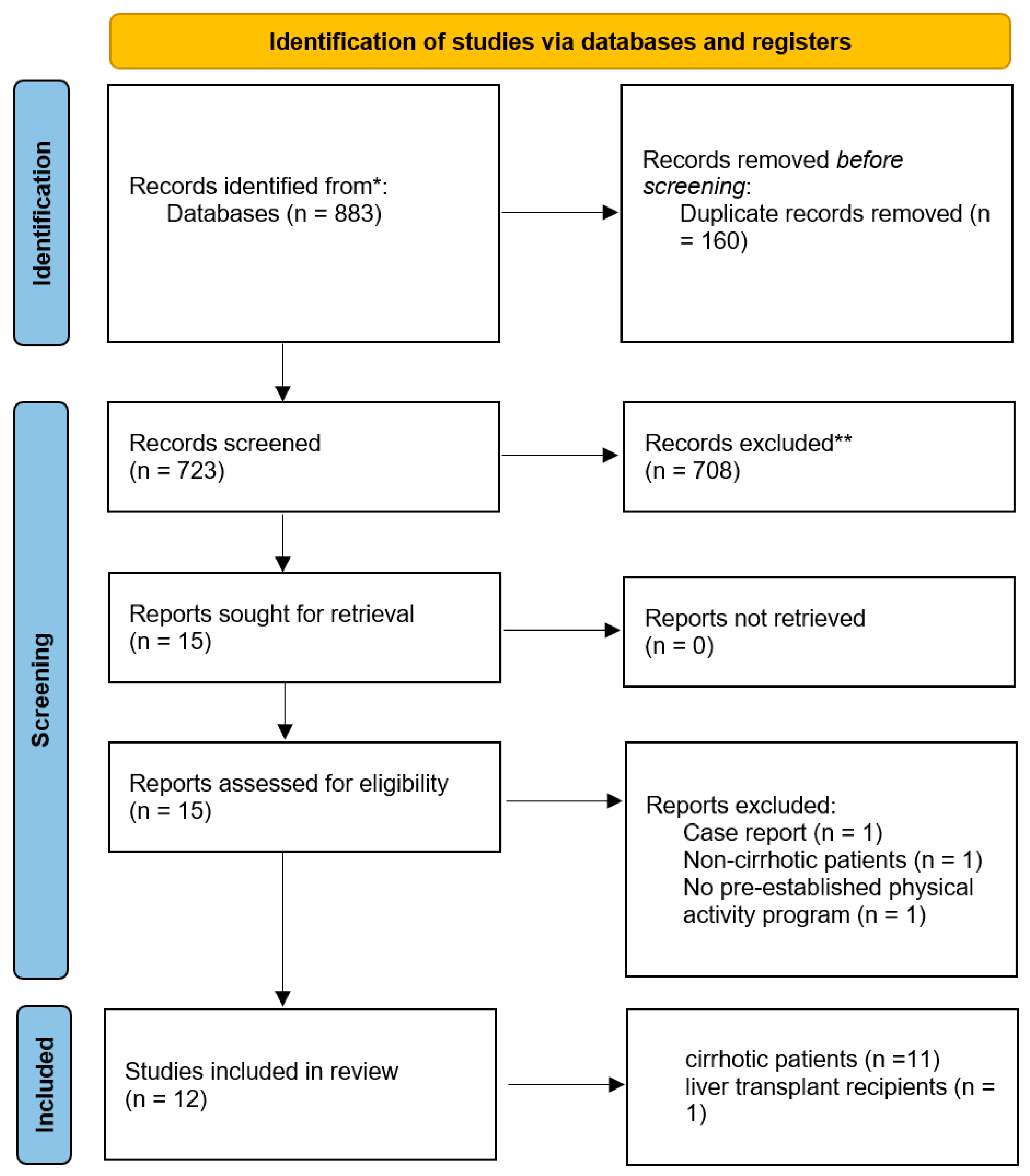
2. Materials and Methods
3. Results and Discussion
3.1. Personalized Physical Exercise Programs in Cirrhotic Patients
3.2. Personalized Physical Exercise Programs in Liver Transplant Recipients
3.2.1. Liver Transplantation and Cardiovascular Risks
3.2.2. Personalized Physical Exercise Programs in Liver Transplant Recipients: A New Promising Approach
4. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Tressou, J.; Moulin, P.; Vergès, B.; Guillou, C.L.; Simon, N.; Pasteau, S. Fatty acid dietary intake in the general French population: Are the French Agency for Food, Environmental and Occupational Health & Safety (ANSES) national recommendations met? Br. J. Nutr. 2016, 116, 1966–1973. [Google Scholar] [CrossRef]
- Katzmarzyk, P.T.; Friedenreich, C.; Shiroma, E.J.; Lee, I.-M. Physical inactivity and non-communicable disease burden in low-income, middle-income and high-income countries. Br. J. Sport. Med. 2022, 56, 101–106. [Google Scholar] [CrossRef]
- World Health Organization. Global Recommendations on Physical Activity for Health; World Health Organization: Geneva, Switzerland, 2010. [Google Scholar]
- Ekelund, U.; Steene-Johannessen, J.; Brown, W.J.; Fagerland, M.W.; Owen, N.; Powell, K.E.; Bauman, A.; Lee, I.M. Does physical activity attenuate, or even eliminate, the detrimental association of sitting time with mortality? A harmonised meta-analysis of data from more than 1 million men and women. Lancet 2016, 388, 1302–1310. [Google Scholar] [CrossRef]
- Knowier, W.C.; Barrett-Connor, E.; Fowler, S.E. Reduction in the Incidence of Type 2 Diabetes with Lifestyle Intervention or Metformin. N. Engl. J. Med. 2002, 346, 393–403. [Google Scholar] [CrossRef]
- Heiskanen, M.A.; Motiani, K.K.; Mari, A.; Saunavaara, V.; Eskelinen, J.-J.; Virtanen, K.A.; Koivumãki, M.; Löyttyniemi, E.; Nuutila, N.; Kalliokoski, K.K.; et al. Exercise training decreases pancreatic fat content and improves beta cell function regardless of baseline glucose tolerance: A randomised controlled trial. Diabetologia 2018, 61, 1817–1828. [Google Scholar] [CrossRef] [PubMed]
- Kirwan, J.P.; Solomon, T.P.J.; Wojta, D.M.; Staten, M.A.; Holloszy, J.O. Effects of 7 days of exercise training on insulin sensitivity and responsiveness in type 2 diabetes mellitus. Am. J. Physiol. Endocrinol. Metab. 2009, 297, E151–E156. [Google Scholar] [CrossRef] [PubMed]
- Magalhães, J.P.; Melo, X.; Correia, I.R.; Ribeiro, R.T.; Raposo, J.; Dores, H.; Bicho, M.; Sardinha, L.B. Effects of combined training with different intensities on vascular health in patients with type 2 diabetes: A 1-year randomized controlled trial. Cardiovasc. Diabetol. 2019, 18, 34. [Google Scholar] [CrossRef] [PubMed]
- ACSM’s Exercise Management for Persons with Chronic Diseases and Disabilities-4th. Human Kinetics n.d. Available online: https://us.humankinetics.com/products/acsms-exercise-management-for-persons-with-chronic-diseases-and-disabilities-4th (accessed on 26 September 2022).
- Kanaley, J.A.; Colberg, S.R.; Corcoran, M.H.; Malin, S.K.; Rodriguez, N.R.; Crespo, C.J.; John, P.K.; Zierath, J.R. Exercise/Physical Activity in Individuals with Type 2 Diabetes: A Consensus Statement from the American College of Sports Medicine. Med. Sci. Sport. Exerc. 2022, 54, 353–368. [Google Scholar] [CrossRef]
- Boulé, N.G.; Kenny, G.P.; Haddad, E.; Wells, G.A.; Sigal, R.J. Meta-analysis of the effect of structured exercise training on cardiorespiratory fitness in Type 2 diabetes mellitus. Diabetologia 2003, 46, 1071–1081. [Google Scholar] [CrossRef]
- Smith, A.D.; Crippa, A.; Woodcock, J.; Brage, S. Physical activity and incident type 2 diabetes mellitus: A systematic review and dose–response meta-analysis of prospective cohort studies. Diabetologia 2016, 59, 2527–2545. [Google Scholar] [CrossRef]
- Bouzakri, K.; Koistinen, H.A.; Zierath, J.R. Molecular Mechanisms of Skeletal Muscle Insulin Resistance in Type 2 Diabetes. Curr. Diabetes Rev. 2005, 1, 167–174. [Google Scholar] [CrossRef] [PubMed]
- Tunstall, R.J.; Mehan, K.A.; Wadley, G.D.; Collier, G.R.; Bonen, A.; Hargreaves, M.; Cameron-Smith, D. Exercise training increases lipid metabolism gene expression in human skeletal muscle. Am. J. Physiol. Endocrinol. Metab. 2002, 283, E66–E72. [Google Scholar] [CrossRef] [PubMed]
- Holloszy, J.O.; Coyle, E.F. Adaptations of skeletal muscle to endurance exercise and their metabolic consequences. J. Appl. Physiol. 1984, 56, 831–838. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.-X.; Zhang, C.-L.; Yu, R.T.; Cho, H.K.; Nelson, M.C.; Bayuga-Ocampo, C.R.; Ham, J.; Kang, H.; Evans, R.M. Regulation of Muscle Fiber Type and Running Endurance by PPARδ. PLoS Biol. 2004, 2, e294. [Google Scholar] [CrossRef]
- Short, K.R.; Bigelow, M.L.; Kahl, J.; Singh, R.; Coenen-Schimke, J.; Raghavakaimal, S.; Sreekumaran Nair, K. Decline in skeletal muscle mitochondrial function with aging in humans. Proc. Natl. Acad. Sci. USA 2005, 102, 5618–5623. [Google Scholar] [CrossRef]
- Gleeson, M.; Bishop, N.C.; Stensel, D.J.; Lindley, M.R.; Mastana, S.S.; Nimmo, M.A. The anti-inflammatory effects of exercise: Mechanisms and implications for the prevention and treatment of disease. Nat. Rev. Immunol. 2011, 11, 607–615. [Google Scholar] [CrossRef]
- Chow, L.S.; Gerszten, R.E.; Taylor, J.M.; Pedersen, B.K.; van Praag, H.; Trappe, S.; Febbraio, M.A.; Galis, Z.S.; Gao, Y.; Haus, J.M.; et al. Exerkines in health, resilience and disease. Nat. Rev. Endocrinol. 2022, 18, 273–289. [Google Scholar] [CrossRef]
- Pedersen, B.K. Anti-inflammatory effects of exercise: Role in diabetes and cardiovascular disease. Eur. J. Clin. Investig. 2017, 47, 600–611. [Google Scholar] [CrossRef]
- Rice, S.M.; Purcell, R.; De Silva, S.; Mawren, D.; McGorry, P.D.; Parker, A.G. The Mental Health of Elite Athletes: A Narrative Systematic Review. Sport. Med. 2016, 46, 1333–1353. [Google Scholar] [CrossRef]
- Benedetti, M.G.; Furlini, G.; Zati, A.; Letizia Mauro, G. The Effectiveness of Physical Exercise on Bone Density in Osteoporotic Patients. Biomed. Res. Int. 2018, 2018, 4840531. [Google Scholar] [CrossRef]
- El-Sayed, M.S.; Ali, N.; Ali, Z.E.-S. Haemorheology in Exercise and Training. Sport. Med. 2005, 35, 649–670. [Google Scholar] [CrossRef]
- Van der Windt, D.J.; Sud, V.; Zhang, H.; Tsung, A.; Huang, H. The Effects of Physical Exercise on Fatty Liver Disease. Gene Expr. 2018, 18, 89–101. [Google Scholar] [CrossRef]
- De Sousa, C.V.; Sales, M.M.; Rosa, T.S.; Lewis, J.E.; de Andrade, R.V.; Simões, H.G. The Antioxidant Effect of Exercise: A Systematic Review and Meta-Analysis. Sport. Med. 2017, 47, 277–293. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, S.; Kirk, E.P.; Mittendorfer, B.; Patterson, B.W.; Klein, S. Randomized trial of exercise effect on intrahepatic triglyceride content and lipid kinetics in nonalcoholic fatty liver disease. Hepatology 2012, 55, 1738–1745. [Google Scholar] [CrossRef] [PubMed]
- Hashida, R.; Kawaguchi, T.; Bekki, M.; Omoto, M.; Matsuse, H.; Nago, T.; Takano, Y.; Ueno, T.; Koga, H.; George, J.; et al. Aerobic vs. resistance exercise in non-alcoholic fatty liver disease: A systematic review. J. Hepatol. 2017, 66, 142–152. [Google Scholar] [CrossRef]
- Flamm, S.L. Hot Topics in Primary Care: Diagnosis of Cirrhosis and Evaluation of Hepatic Encephalopathy: Common Errors and Their Significance for the PCP. J. Fam. Pract. 2017, 66, S34–S39. [Google Scholar] [PubMed]
- Asrani, S.K.; Devarbhavi, H.; Eaton, J.; Kamath, P.S. Burden of liver diseases in the world. J. Hepatol. 2019, 70, 151–171. [Google Scholar] [CrossRef]
- Blachier, M.; Leleu, H.; Peck-Radosavljevic, M.; Valla, D.-C.; Roudot-Thoraval, F. The burden of liver disease in Europe: A review of available epidemiological data. J. Hepatol. 2013, 58, 593–608. [Google Scholar] [CrossRef]
- De Siqueira, M.R.; de Pace, F.H.L.; Limongi, T.M.; Henrique, D.M.N.; de Mira, P.A.C.; de Oliveira, T.M.D.; Oliveira, C.C.; de Aguiar, A.S.; Malaguti, C. Factors associated with the perceived benefits and barriers to physical activity in liver cirrhosis. Rev. Assoc. Med. Bras. 2021, 67, 271–276. [Google Scholar] [CrossRef]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [CrossRef]
- Galiè, N.; Humbert, M.; Vachiery, J.-L.; Gibbs, S.; Lang, I.; Torbicki, A.; Simonneau, G.; Peacock, A.; Vonk Noordegraaf, A.; Beghetti, M.; et al. 2015 ESC/ERS Guidelines for the diagnosis and treatment of pulmonary hypertension: The Joint Task Force for the Diagnosis and Treatment of Pulmonary Hypertension of the European Society of Cardiology (ESC) and the European Respiratory Society (ERS)Endorsed by: Association for European Paediatric and Congenital Cardiology (AEPC), International Society for Heart and Lung Transplantation (ISHLT). Eur. Respir. J. 2015, 46, 903–975. [Google Scholar] [CrossRef] [PubMed]
- Mathur, S.; Janaudis-Ferreira, T.; Wickerson, L.; Singer, L.G.; Patcai, J.; Rozenberg, D.; Blydt-Hansen, T.; Hartmann, E.L.; Haykowsky, M.; Helm, D.; et al. Meeting Report: Consensus Recommendations for a Research Agenda in Exercise in Solid Organ Transplantation. Am. J. Transplant. 2014, 14, 2235–2245. [Google Scholar] [CrossRef]
- Sirisunhirun, P.; Bandidniyamanon, W.; Jrerattakon, Y.; Muangsomboon, K.; Pramyothin, P.; Nimanong, S.; Tanwandee, T.; Charatcharoenwitthata, P.; Chainuvati, S.; Chotiyaputta, W. Effect of a 12-week home-based exercise training program on aerobic capacity, muscle mass, liver and spleen stiffness, and quality of life in cirrhotic patients: A randomized controlled clinical trial. BMC Gastroenterol. 2022, 22, 66. [Google Scholar] [CrossRef] [PubMed]
- Berzigotti, A.; Saran, U.; Dufour, J.-F. Physical activity and liver diseases. Hepatology 2016, 63, 1026–1040. [Google Scholar] [CrossRef] [PubMed]
- Powell, E.E.; Wong, V.W.-S.; Rinella, M. Non-alcoholic fatty liver disease. Lancet 2021, 397, 2212–2224. [Google Scholar] [CrossRef]
- Villeret, F.; Dharancy, S.; Erard, D.; Abergel, A.; Barbier, L.; Besch, C.; Boillot, O.; Boudjema, K.; Coilly, A.; Conti, F.; et al. Liver transplantation for NAFLD cirrhosis: Age and recent coronary angioplasty are major determinants of survival. Liver Int. 2022, 42, 2428–2441. [Google Scholar] [CrossRef]
- Church, T.S.; Kuk, J.L.; Ross, R.; Priest, E.L.; Biltoff, E.; Blair, S.N. Association of Cardiorespiratory Fitness, Body Mass Index, and Waist Circumference to Nonalcoholic Fatty Liver Disease. Gastroenterology 2006, 130, 2023–2030. [Google Scholar] [CrossRef]
- EASL–EASD–EASO Clinical Practice Guidelines for the management of non-alcoholic fatty liver disease. J. Hepatol. 2016, 64, 1388–1402. [CrossRef]
- Chalasani, N.; Younossi, Z.; Lavine, J.E.; Charlton, M.; Cusi, K.; Rinella, M.; Harrison, S.A.; Brunt, E.M.; Sanyal, A.J. The diagnosis and management of nonalcoholic fatty liver disease: Practice guidance from the American Association for the Study of Liver Diseases. Hepatology 2018, 67, 328–357. [Google Scholar] [CrossRef]
- Alexander, M.; Loomis, A.K.; van der Lei, J.; Duarte-Salles, T.; Prieto-Alhambra, D.; Ansell, D.; Pasqua, A.; Lapi, F.; Rijnbeek, P.; Mosseveld, M.; et al. Non-alcoholic fatty liver disease and risk of incident acute myocardial infarction and stroke: Findings from matched cohort study of 18 million European adults. BMJ 2019, 367, l5367. [Google Scholar] [CrossRef]
- Kasper, P.; Martin, A.; Lang, S.; Kütting, F.; Goeser, T.; Demir, M.; Steffen, H.M. NAFLD and cardiovascular diseases: A clinical review. Clin. Res. Cardiol. 2021, 110, 921–937. [Google Scholar] [CrossRef] [PubMed]
- Targher, G.; Byrne, C.D.; Tilg, H. NAFLD and increased risk of cardiovascular disease: Clinical associations, pathophysiological mechanisms and pharmacological implications. Gut 2020, 69, 1691–1705. [Google Scholar] [CrossRef] [PubMed]
- Simon, T.G.; Roelstraete, B.; Hagström, H.; Sundström, J.; Ludvigsson, J.F. Non-alcoholic fatty liver disease and incident major adverse cardiovascular events: Results from a nationwide histology cohort. Gut 2022, 71, 1867–1875. [Google Scholar] [CrossRef] [PubMed]
- Ratziu, V.; Ghabril, M.; Romero-Gomez, M.; Svegliati-Baroni, G. Recommendations for Management and Treatment of Nonalcoholic Steatohepatitis. Transplantation 2019, 103, 28–38. [Google Scholar] [CrossRef] [PubMed]
- Vilar-Gomez, E.; Martinez-Perez, Y.; Calzadilla-Bertot, L.; Torres-Gonzalez, A.; Gra-Oramas, B.; Gonzalez-Fabian, L.; Friedman, S.L.; Diago, M.; Romero-Gomez, M. Weight Loss Through Lifestyle Modification Significantly Reduces Features of Nonalcoholic Steatohepatitis. Gastroenterology 2015, 149, 367–378.e5. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, G.G.; Klein, S. Exercise and NAFLD: Is It Worth the Effort? Hepatology 2017, 66, 1691–1694. [Google Scholar] [CrossRef] [PubMed]
- EASL Clinical Practice Guidelines on nutrition in chronic liver disease. J. Hepatol. 2019, 70, 172–193. [CrossRef]
- Kraus, W.E.; Powell, K.E.; Haskell, W.L.; Janz, K.F.; Campbell, W.W.; Jakicic, J.M.; Troiano, R.P.; Sprow, K.; Torres, A.; Piercy, K.L. Physical Activity, All-Cause and Cardiovascular Mortality, and Cardiovascular Disease. Med. Sci. Sports Exerc. 2019, 51, 1270–1281. [Google Scholar] [CrossRef]
- Powell, K.E.; King, A.C.; Buchner, D.M.; Campbell, W.W.; DiPietro, L.; Erickson, K.I.; Hillman, C.H.; Jakicic, J.M.; Janz, K.F.; Katzmarzyk, P.T.; et al. The Scientific Foundation for the Physical Activity Guidelines for Americans, 2nd Edition. J. Phys. Act. Health 2018, 16, 1–11. [Google Scholar] [CrossRef]
- Sattelmair, J.; Pertman, J.; Ding, E.L.; Kohl, H.W.; Haskell, W.; Lee, I.-M. Dose-Response Between Physical Activity and Risk of Coronary Heart Disease: A Meta-Analysis. Circulation 2011, 124, 789–795. [Google Scholar] [CrossRef]
- Visseren, F.L.J.; Mach, F.; Smulders, Y.M.; Carballo, D.; Koskinas, K.C.; Bäck, M.; Benetos, A.; Biffi, A.; Boavida, J.M.; Capodanno, D.; et al. 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice: Developed by the Task Force for cardiovascular disease prevention in clinical practice with representatives of the European Society of Cardiology and 12 medical societies With the special contribution of the European Association of Preventive Cardiology (EAPC). Eur. Heart J. 2021, 42, 3227–3337. [Google Scholar] [CrossRef] [PubMed]
- Wahid, A.; Manek, N.; Nichols, M.; Kelly, P.; Foster, C.; Webster, P.; Kaur, A.; Friedemann Smith, C.; Wilkins, E.; Rayner, M.; et al. Quantifying the Association Between Physical Activity and Cardiovascular Disease and Diabetes: A Systematic Review and Meta-Analysis. J. Am. Heart Assoc. 2016, 5, e002495. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.C.; Dodge, J.L.; Kappus, M.R.; Wong, R.; Mohamad, Y.; Segev, D.L.; McAdams-DeMarco, M. A Multi-Center Pilot Randomized Clinical Trial of a Home-Based Exercise Program for Patients with Cirrhosis: The Strength Training Intervention (STRIVE). Am. J. Gastroenterol. 2021, 116, 717–722. [Google Scholar] [CrossRef] [PubMed]
- Fried, L.P.; Ferrucci, L.; Darer, J.; Williamson, J.D.; Anderson, G. Untangling the Concepts of Disability, Frailty, and Comorbidity: Implications for Improved Targeting and Care. J. Gerontol. Ser. A 2004, 59, M255–M263. [Google Scholar] [CrossRef]
- Ng, T.P.; Feng, L.; Nyunt, M.S.Z.; Feng, L.; Niti, M.; Tan, B.Y.; Chan, G.; Khoo, S.A.; Chan, S.M.; Yap, P.; et al. Nutritional, Physical, Cognitive, and Combination Interventions and Frailty Reversal Among Older Adults: A Randomized Controlled Trial. Am. J. Med. 2015, 128, 1225–1236.e1. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.C.; Feng, S.; Terrault, N.A.; Lizaola, B.; Hayssen, H.; Covinsky, K. Frailty Predicts Wait-List Mortality in Liver Transplant Candidates. Am. J. Transplant. 2014, 14, 1870–1879. [Google Scholar] [CrossRef]
- Duarte-Rojo, A.; Ruiz-Margáin, A.; Montaño-Loza, A.J.; Macías-Rodríguez, R.U.; Ferrando, A.; Kim, W.R. Exercise and physical activity for patients with end-stage liver disease: Improving functional status and sarcopenia while on the transplant waiting list. Liver Transplant. 2018, 24, 122–139. [Google Scholar] [CrossRef]
- Laube, R.; Wang, H.; Park, L.; Heyman, J.K.; Vidot, H.; Majumdar, A.; Strasser, S.I.; McCaughan, G.W.; Liu, K. Frailty in advanced liver disease. Liver Int. 2018, 38, 2117–2128. [Google Scholar] [CrossRef]
- Sinclair, M.; Poltavskiy, E.; Dodge, J.L.; Lai, J.C. Frailty is independently associated with increased hospitalisation days in patients on the liver transplant waitlist. World J. Gastroenterol. 2017, 23, 899–905. [Google Scholar] [CrossRef]
- Lai, J.C.; Covinsky, K.E.; Dodge, J.L.; Boscardin, W.J.; Segev, D.L.; Roberts, J.P.; Feng, S. Development of a Novel Frailty Index to Predict Mortality in Patients with End-Stage Liver Disease. Hepatology 2017, 66, 564–574. [Google Scholar] [CrossRef]
- Verna, E.; Chan, C.; Pisa, J.; Abdelmessih, R.; Lukose, T.; Krishnamoorthy, S.; Brown, R. Frailty, Physical Performance and Sarcopenia Measures in Patients Awaiting Liver Transplantation Predict Mortality and Post-Operative Complications: Abstract# C1938. Transplantation 2014, 98, 742. [Google Scholar]
- Moreno, R.; Berenguer, M. Post-liver transplantation medical complications. Ann. Hepatol. 2006, 5, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Crespo, G.; Hessheimer, A.J.; Armstrong, M.J.; Berzigotti, A.; Monbaliu, D.; Spiro, M.; Raptis, D.A.; Lai, J.C. Which preoperative assessment modalities best identify patients who are suitable for enhanced recovery after liver transplantation?–A systematic review of the literature and expert panel recommendations. Clin. Transplant. 2022, 36, e14644. [Google Scholar] [CrossRef] [PubMed]
- Alberino, F.; Gatta, A.; Amodio, P.; Merkel, C.; Di Pascoli, L.; Boffo, G.; Caregaro, L. Nutrition and survival in patients with liver cirrhosis. Nutrition 2001, 17, 445–450. [Google Scholar] [CrossRef] [PubMed]
- Montano–Loza, A.J.; Meza–Junco, J.; Prado, C.M.M.; Lieffers, J.R.; Baracos, V.E.; Bain, V.G.; Sawyer, M.B. Muscle Wasting Is Associated With Mortality in Patients With Cirrhosis. Clin. Gastroenterol. Hepatol. 2012, 10, 166–173.e1. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.C.; Coombes, J.S.; Macdonald, G.A. Exercise capacity and muscle strength in patients with cirrhosis. Liver Transplant. 2012, 18, 146–151. [Google Scholar] [CrossRef] [PubMed]
- Kachaamy, T.; Bajaj, J.S.; Heuman, D.M. Muscle and Mortality in Cirrhosis. Clin. Gastroenterol. Hepatol. 2012, 10, 100–102. [Google Scholar] [CrossRef] [PubMed]
- Dasarathy, S. Consilience in sarcopenia of cirrhosis. J. Cachexia Sarcopenia Muscle 2012, 3, 225–237. [Google Scholar] [CrossRef]
- Román, E.; Córdoba, J.; Torrens, M.; Guarner, C.; Soriano, G. Falls and cognitive dysfunction impair health-related quality of life in patients with cirrhosis. Eur. J. Gastroenterol. Hepatol. 2013, 25, 77–84. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [PubMed]
- Kim, G.; Kang, S.H.; Kim, M.Y.; Baik, S.K. Prognostic value of sarcopenia in patients with liver cirrhosis: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0186990. [Google Scholar] [CrossRef] [PubMed]
- Dunn, M.A.; Josbeno, D.A.; Schmotzer, A.R.; Tevar, A.D.; DiMartini, A.F.; Landsittel, D.P.; Delitto, A. The gap between clinically assessed physical performance and objective physical activity in liver transplant candidates. Liver Transplant. 2016, 22, 1324–1332. [Google Scholar] [CrossRef] [PubMed]
- Chen, H.W.; Ferrando, A.; White, M.G.; Dennis, R.A.; Xie, J.; Pauly, M.; Park, S.; Bartter, T.; Dunn, M.A.; Ruiz-Margain, A.; et al. Home-Based Physical Activity and Diet Intervention to Improve Physical Function in Advanced Liver Disease: A Randomized Pilot Trial. Dig. Dis. Sci. 2020, 65, 3350–3359. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.C.; Sonnenday, C.J.; Tapper, E.B.; Duarte-Rojo, A.; Dunn, M.A.; Bernal, W.; Carey, E.J.; Dasarathy, S.; Kamath, B.M.; Kappus, M.R.; et al. Frailty in liver transplantation: An expert opinion statement from the American Society of Transplantation Liver and Intestinal Community of Practice. Am. J. Transplant. 2019, 19, 1896–1906. [Google Scholar] [CrossRef]
- Debette-Gratien, M.; Tabouret, T.; Antonini, M.-T.; Dalmay, F.; Carrier, P.; Legros, R.; Jacques, J.; Vincent, F.; Sautereau, D.; Samuel, D.; et al. Personalized Adapted Physical Activity Before Liver Transplantation: Acceptability and Results. Transplantation 2015, 99, 145–150. [Google Scholar] [CrossRef]
- Boursier, J.; Anty, R.; Carette, C.; Cariou, B.; Castera, L.; Caussy, C.; Fontaine, H.; Garioud, A.; Gourdy, P.; Guerci, B.; et al. Management of diabetes mellitus in patients with cirrhosis: An overview and joint statement. Diabetes Metab. 2021, 47, 101272. [Google Scholar] [CrossRef]
- Donini, L.M.; Busetto, L.; Bischoff, S.C.; Cederholm, T.; Ballesteros-Pomar, M.D.; Batsis, J.A.; Bauer, J.M.; Boirie, Y.; Cruz-Jentoft, A.J.; Dicker, D.; et al. Definition and Diagnostic Criteria for Sarcopenic Obesity: ESPEN and EASO Consensus Statement. Obes. Facts 2022, 15, 321–335. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Macías-Rodríguez, R.U.; Ilarraza-Lomelí, H.; Ruiz-Margáin, A.; Ponce-de-León-Rosales, S.; Vargas-Vorácková, F.; García-Flores, O.; Torre, A.; Duarte-Rojo, A. Changes in Hepatic Venous Pressure Gradient Induced by Physical Exercise in Cirrhosis: Results of a Pilot Randomized Open Clinical Trial. Clin. Transl. Gastroenterol. 2016, 7, e180. [Google Scholar] [CrossRef]
- Berzigotti, A.; Albillos, A.; Villanueva, C.; Genescá, J.; Ardevol, A.; Augustín, S.; Calleja, J.L.; Bañares, R.; García-Pagán, J.C.; Mesonero, F.; et al. Effects of an intensive lifestyle intervention program on portal hypertension in patients with cirrhosis and obesity: The sportdiet study. Hepatology 2017, 65, 1293–1305. [Google Scholar] [CrossRef]
- Román, E.; Torrades, M.T.; Nadal, M.J.; Cárdenas, G.; Nieto, J.C.; Vidal, S.; Bascuñana, H.; Juárez, C.; Guarner, C.; Córdoba, J.; et al. Randomized Pilot Study: Effects of an Exercise Programme and Leucine Supplementation in Patients with Cirrhosis. Dig. Dis. Sci. 2014, 59, 1966–1975. [Google Scholar] [CrossRef] [PubMed]
- Zenith, L.; Meena, N.; Ramadi, A.; Yavari, M.; Harvey, A.; Carbonneau, M.; Ma, M.; Abraldes, J.G.; Paterson, I.; Haykowsky, M.J.; et al. Eight Weeks of Exercise Training Increases Aerobic Capacity and Muscle Mass and Reduces Fatigue in Patients With Cirrhosis. Clin. Gastroenterol. Hepatol. 2014, 12, 1920–1926.e2. [Google Scholar] [CrossRef] [PubMed]
- Morkane, C.M.; Kearney, O.; Bruce, D.A.; Melikian, C.N.; Martin, D.S. An Outpatient Hospital-based Exercise Training Program for Patients With Cirrhotic Liver Disease Awaiting Transplantation: A Feasibility Trial. Transplantation 2020, 104, 97–103. [Google Scholar] [CrossRef]
- Román, E.; García-Galcerán, C.; Torrades, T.; Herrera, S.; Marín, A.; Doñate, M.; Alvarado-Tapias, E.; Malouf, J.; Nácher, L.; Serra-Grima, R.; et al. Effects of an Exercise Programme on Functional Capacity, Body Composition and Risk of Falls in Patients with Cirrhosis: A Randomized Clinical Trial. PLoS ONE 2016, 11, e0151652. [Google Scholar] [CrossRef] [PubMed]
- Kruger, C.; McNeely, M.L.; Bailey, R.J.; Yavari, M.; Abraldes, J.G.; Carbonneau, M.; Newnham, K.; DenHeyer, V.; Ma, M.; Thompson, R.; et al. Home Exercise Training Improves Exercise Capacity in Cirrhosis Patients: Role of Exercise Adherence. Sci. Rep. 2018, 8, 99. [Google Scholar] [CrossRef]
- Neviere, R.; Edme, J.L.; Montaigne, D.; Boleslawski, E.; Pruvot, F.R.; Dharancy, S. Prognostic Implications of Preoperative Aerobic Capacity and Exercise Oscillatory Ventilation After Liver Transplantation. Am. J. Transplant. 2014, 14, 88–95. [Google Scholar] [CrossRef]
- Bernal, W.; Martin-Mateos, R.; Lipcsey, M.; Tallis, C.; Woodsford, K.; Mcphail, M.J.; Willars, C.; Auzinger, G.; Sizer, E.; Heneghan, M.; et al. Aerobic capacity during cardiopulmonary exercise testing and survival with and without liver transplantation for patients with chronic liver disease. Liver Transplant. 2014, 20, 54–62. [Google Scholar] [CrossRef]
- Prentis, J.M.; Manas, D.M.D.; Trenell, M.I.; Hudson, M.; Jones, D.J.; Snowden, C.P. Submaximal cardiopulmonary exercise testing predicts 90-day survival after liver transplantation. Liver Transplant. 2012, 18, 152–159. [Google Scholar] [CrossRef]
- Brustia, R.; Savier, E.; Scatton, O. Physical exercise in cirrhotic patients: Towards prehabilitation on waiting list for liver transplantation. A systematic review and meta-analysis. Clin. Res. Hepatol. Gastroenterol. 2018, 42, 205–215. [Google Scholar] [CrossRef]
- Plauth, M.; Merli, M.; Kondrup, J.; Weimann, A.; Ferenci, P.; Müller, M.J. ESPEN guidelines for nutrition in liver disease and transplantation. Clin. Nutr. 1997, 16, 43–55. [Google Scholar] [CrossRef]
- Mohta, S.; Anand, A.; Sharma, S.; Qamar, S.; Agarwal, S.; Gunjan, D.; Singh, N.; Madhusudhan, K.S.; Pandey, R.M.; Saraya, A. Randomised clinical trial: Effect of adding branched chain amino acids to exercise and standard-of-care on muscle mass in cirrhotic patients with sarcopenia. Hepatol. Int. 2022, 16, 680–690. [Google Scholar] [CrossRef] [PubMed]
- Nishida, Y.; Ide, Y.; Okada, M.; Otsuka, T.; Eguchi, Y.; Ozaki, I.; Tanaka, K.; Mizuta, T. Effects of home-based exercise and branched-chain amino acid supplementation on aerobic capacity and glycemic control in patients with cirrhosis. Hepatol. Res. 2017, 47, E193–E200. [Google Scholar] [CrossRef] [PubMed]
- Charlton, M. Obesity, hyperlipidemia, and metabolic syndrome. Liver Transplant. 2009, 15, S83–S89. [Google Scholar] [CrossRef] [PubMed]
- Izzy, M.; VanWagner, L.B.; Lee, S.S.; Altieri, M.; Angirekula, M.; Watt, K.D. Understanding and managing cardiovascular outcomes in liver transplant recipients. Curr. Opin. Organ. Transplant. 2019, 24, 148–155. [Google Scholar] [CrossRef]
- Guckelberger, O. Long-term medical comorbidities and their management: Hypertension/cardiovascular disease. Liver Transplant. 2009, 15, S75–S78. [Google Scholar] [CrossRef] [PubMed]
- VanWagner, L.B.; Holl, J.L.; Montag, S.; Gregory, D.; Connolly, S.; Kosirog, M.; Campbell, P.; Pine, S.; Daud, A.; Finn, D.; et al. Blood Pressure Control According to Clinical Practice Guidelines is Associated with Decreased Mortality and Cardiovascular Events among Liver Transplant Recipients. Am. J. Transplant. 2020, 20, 797–807. [Google Scholar] [CrossRef]
- Obesity and Overweight, n.d. Available online: https://www.who.int/news-room/fact-sheets/detail/obesity-and-overweight (accessed on 16 October 2022).
- Hales, C.M.; Carroll, M.D.; Fryar, C.D.; Ogden, C.L. Prevalence of Obesity and Severe Obesity Among Adults: United States, 2017–2018; National Center for Health Statistics: Hyattsville, MD, USA, 2020; pp. 1–8.
- Targher, G.; Byrne, C.D.; Lonardo, A.; Zoppini, G.; Barbui, C. Non-alcoholic fatty liver disease and risk of incident cardiovascular disease: A meta-analysis. J. Hepatol. 2016, 65, 589–600. [Google Scholar] [CrossRef]
- Lucey, M.R.; Terrault, N.; Ojo, L.; Hay, J.E.; Neuberger, J.; Blumberg, E.; Teperman, L.W. Long-term management of the successful adult liver transplant: 2012 practice guideline by the American Association for the Study of Liver Diseases and the American Society of Transplantation. Liver Transplant. 2013, 19, 3–26. [Google Scholar] [CrossRef] [PubMed]
- Yoo, H.Y.; Thuluvath, P.J. The effect of insulin-dependent diabetes mellitus on outcome of liver transplantation. Transplantation 2002, 74, 1007–1012. [Google Scholar] [CrossRef] [PubMed]
- Chun, H.S.; Lee, M.; Lee, H.A.; Oh, S.Y.; Baek, H.J.; Moon, J.W.; Kim, Y.J.; Lee, J.; Kim, H.; Kim, H.Y.; et al. Association of Physical Activity With Risk of Liver Fibrosis, Sarcopenia, and Cardiovascular Disease in Nonalcoholic Fatty Liver Disease. Clin. Gastroenterol. Hepatol. 2023, 21, 358–369.e12. [Google Scholar] [CrossRef]
- Van Adrichem, E.J.; van de Zande, S.C.; Dekker, R.; Verschuuren, E.A.M.; Dijkstra, P.U.; van der Schans, C.P. Perceived Barriers to and Facilitators of Physical Activity in Recipients of Solid Organ Transplantation, a Qualitative Study. PLoS ONE 2016, 11, e0162725. [Google Scholar] [CrossRef]
- Roi, G.S.; Stefoni, S.; Mosconi, G.; Brugin, E.; Burra, P.; Ermolao, A.; Granito, M.; Macini, P.; Mastrosimone, S.; Nacchia, F.; et al. Physical Activity in Solid Organ Transplant Recipients: Organizational Aspects and Preliminary Results of the Italian Project. Transplant. Proc. 2014, 46, 2345–2349. [Google Scholar] [CrossRef] [PubMed]
- Berben, L.; Engberg, S.J.; Rossmeissl, A.; Gordon, E.J.; Kugler, C.; Schmidt-Trucksäss, A.; Klem, M.L.; Sereika, S.M.; De Simone, P.; Dobbels, F.; et al. Correlates and Outcomes of Low Physical Activity Posttransplant: A Systematic Review and Meta-Analysis. Transplantation 2019, 103, 679–688. [Google Scholar] [CrossRef] [PubMed]
- Van Adrichem, E.J.; Dekker, R.; Krijnen, W.P.; Verschuuren, E.A.M.; Dijkstra, P.U.; van der Schans, C.P. Physical Activity, Sedentary Time, and Associated Factors in Recipients of Solid-Organ Transplantation. Phys. Ther. 2018, 98, 646–657. [Google Scholar] [CrossRef] [PubMed]
- Stephenson, A.L.; Yoshida, E.M.; Abboud, R.T.; Fradet, G.; Levy, R.D. Impaired Exercice Performance after Successful Liver Transplantation. Transplantation 2001, 72, 1161–1164. [Google Scholar] [CrossRef]
- Krasnoff, J.B.; Vintro, A.Q.; Ascher, N.L.; Bass, N.M.; Paul, S.M.; Dodd, M.J.; Painter, P.L. A Randomized Trial of Exercise and Dietary Counseling After Liver Transplantation. Am. J. Transplant. 2006, 6, 1896–1905. [Google Scholar] [CrossRef]
- Didsbury, M.; McGee, R.G.; Tong, A.; Craig, J.C.; Chapman, J.R.; Chadban, S.; Wong, G. Exercise Training in Solid Organ Transplant Recipients: A Systematic Review and Meta-Analysis. Transplantation 2013, 95, 679–687. [Google Scholar] [CrossRef]
- Jetten, W.D.; Hogenbirk, R.N.M.; Van Meeteren, N.L.U.; Cuperus, F.J.C.; Klaase, J.M.; De Jong, R. Physical Effects, Safety and Feasibility of Prehabilitation in Patients Awaiting Orthotopic Liver Transplantation, a Systematic Review. Transpl. Int. 2022, 35, 10330. [Google Scholar] [CrossRef] [PubMed]
- Al-Judaibi, B.; Alqalami, I.; Sey, M.; Qumosani, K.; Howes, N.; Sinclair, L.; Chandok, N.; Eddin, A.H.; Hernandez-Alejandro, R.; Marotta, P.; et al. Exercise Training for Liver Transplant Candidates. Transplant. Proc. 2019, 51, 3330–3337. [Google Scholar] [CrossRef]
- Beyer, N.; Aadahl, M.; Strange, B.; Kirkegaard, P.; Hansen, B.A.; Mohr, T.; Kjaer, M. Improved physical performance after orthotopic liver transplantation. Liver Transplant. Surg. 1999, 5, 301–309. [Google Scholar] [CrossRef]
- Van den Berg-Emons, R.J.G.; van Ginneken, B.T.J.; Nooijen, C.F.J.; Metselaar, H.J.; Tilanus, H.W.; Kazemier, G.; Stam, H.J. Fatigue After Liver Transplantation: Effects of a Rehabilitation Program Including Exercise Training and Physical Activity Counseling. Phys. Ther. 2014, 94, 857–865. [Google Scholar] [CrossRef]
- Garcia, A.M.C.; Veneroso, C.E.; Soares, D.D.; Lima, A.S.; Correia, M.I.T.D. Effect of a Physical Exercise Program on the Functional Capacity of Liver Transplant Patients. Transplant. Proc. 2014, 46, 1807–1808. [Google Scholar] [CrossRef] [PubMed]
- Dunn, M.A.; Rogal, S.S.; Duarte-Rojo, A.; Lai, J.C. Physical Function, Physical Activity, and Quality of Life After Liver Transplantation. Liver Transpl. 2020, 26, 702–708. [Google Scholar] [CrossRef] [PubMed]
- Masala, D.; Mannocci, A.; Unim, B.; Del Cimmuto, A.; Turchetta, F.; Gatto, G.; Santoro, R.; Ettorre, G.M.; Boccia, A.; La Torre, G. Quality of Life and Physical Activity in Liver Transplantation Patients: Results of a Case-Control Study in Italy. Transplant. Proc. 2012, 44, 1346–1350. [Google Scholar] [CrossRef] [PubMed]
- Vallin, M.; Guillaud, O.; Boillot, O.; Hervieu, V.; Scoazec, J.-Y.; Dumortier, J. Recurrent or de novo nonalcoholic fatty liver disease after liver transplantation: Natural history based on liver biopsy analysis. Liver Transplant. 2014, 20, 1064–1071. [Google Scholar] [CrossRef]
- Kallwitz, E.R.; Loy, V.; Mettu, P.; Von Roenn, N.; Berkes, J.; Cotler, S.J. Physical activity and metabolic syndrome in liver transplant recipients. Liver Transplant. 2013, 19, 1125–1131. [Google Scholar] [CrossRef]
- Perna, S. Is Vitamin D Supplementation Useful for Weight Loss Programs? A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Medicina 2019, 55, 368. [Google Scholar] [CrossRef]
- Bonner, K.; Heimbach, J.K. Obesity management in the liver transplant recipient: The role of bariatric surgery. Curr. Opin. Organ. Transplant. 2018, 23, 244–249. [Google Scholar] [CrossRef]
- Dayyeh, B.K.A.; Bazerbachi, F.; Vargas, E.J.; Sharaiha, R.Z.; Thompson, C.C.; Thaemert, B.C.; Teixeira, A.F.; Chapman, C.G.; Kumbhari, V.; Ujiki, M.B.; et al. Endoscopic sleeve gastroplasty for treatment of class 1 and 2 obesity (MERIT): A prospective, multicentre, randomised trial. Lancet 2022, 400, 441–451. [Google Scholar] [CrossRef]
- McCarty, T.R.; Thompson, C.C. The current state of bariatric endoscopy. Dig. Endosc. 2021, 33, 321–334. [Google Scholar] [CrossRef]
- De Block, C.E.M.; Dirinck, E.; Verhaegen, A.; Van Gaal, L.F. Efficacy and safety of high-dose glucagon-like peptide-1, glucagon-like peptide-1/glucose-dependent insulinotropic peptide, and glucagon-like Pept. -1/glucagon receptor agonists in type 2 diabetes. Diabetes Obes. Metab. 2022, 24, 788–805. [Google Scholar] [CrossRef] [PubMed]
- Coskun, T.; Urva, S.; Roell, W.C.; Qu, H.; Loghin, C.; Moyers, J.S.; O’Farrell, L.S.; Briere, D.A.; Sloop, K.W.; Thomas, M.K.; et al. LY3437943, a novel triple glucagon, GIP, and GLP-1 receptor agonist for glycemic control and weight loss: From discovery to clinical proof of concept. Cell Metab. 2022, 34, 1234–1247.e9. [Google Scholar] [CrossRef] [PubMed]
- Rondanelli, M.; Perna, S.; Astrone, P.; Grugnetti, A.; Solerte, S.B.; Guido, D. Twenty-four-week effects of liraglutide on body composition, adherence to appetite, and lipid profile in overweight and obese patients with type 2 diabetes mellitus. Patient Prefer. Adherence 2016, 10, 407–413. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Study | Age (Years) | Males (%) | NASH or NAFLD (%) | Child–Pugh Score | MELD | BMI (kg/m2) | Diabetes Mellitus | Study Design and Duration | Main Result | |
|---|---|---|---|---|---|---|---|---|---|---|
| Sirisunhirun et al. [35] | HoBET | 55.6 (mean) | 75% | 5% | 5 (median) | 7.95 (mean) | 25.3 (mean) | ND | Randomized controlled trial (12 weeks) | A 12-week home-based exercise training program significantly improved the quality of life for fatigue. However, no significant differences were observed regarding a 6MWT, thigh muscle mass, or hepatic venous pressure gradient. |
| Control | 57.1 (mean) | 55% | 0% | 5 (median) | 7.95 (mean) | 25.2 (mean) | ND | |||
| Lai et al. [55] | STRIVE | 62 (median) | ND | 10% | ND | 12 (median) | 28 (median) | 36% | Multicenter randomized clinical trial (12 weeks) | A structured home strength-training intervention for patients with cirrhosis was associated with a nonsignificant improvement in the LFI and a significant improvement in quality of life. |
| Control | 61 (median) | ND | 16% | ND | 13 (median) | 28 (median) | 24% | |||
| Chen et al. [75] | Exercise | 55 (median) | 56% | 11% | 9 (median) | ND | 31 (median) | 45% | Randomized clinical trial (12 weeks) | A home-based PA program maintained physical performance and improved aerobic fitness according to the 6MWT but not cardiopulmonary exercise testing. |
| Control | 54 (median) | 75% | 50% | 10 (median) | ND | 29 (median) | 13% | |||
| Debette-Gratien et al. [77] | Physical activity | 51 (mean) | 75% | 0 | 7.1 (mean) | 12.87 (mean) | ND | ND | Cohort (12 weeks) | A personalized, standardized physical exercise program was acceptable, effective, and safe in patients awaiting liver transplantation. It positively influenced the index of fitness and quality of life. |
| Román et al. [83] | Exercise | 65.5 (mean) | 62% | ND | ND | 9.5 (mean) | 26.7 (mean) | ND | Randomized clinical trial (12 weeks) | A program of moderate physical exercise with leucine supplements for patients with cirrhosis was safe, improved exercise capacity and health-related quality of life, and increased leg muscle mass. |
| Control | 61.0 (mean) | 78% | ND | ND | 9.0 (mean) | 27.6 (mean) | ND | |||
| Zenith et al. [84] | Exercise | 56.4 (mean) | 78% | ND | 6.2 (mean) | 9.7 (mean) | 27.7 (mean) | ND | Randomized clinical trial (8 weeks) | Eight weeks of supervised aerobic exercise training increased peak oxygen consumption (VO2max) and muscle mass and reduced fatigue in patients with cirrhosis. |
| Control | 58.6 (mean) | 80% | ND | 6.3 (mean) | 10.2 (mean) | 28.9 (mean) | ND | |||
| Morkane et al. [85] | Exercise | 55.6 (mean) | 87.5% | 12.5% | ND | 13.7 (mean) | ND | ND | Feasibility study with nonrandomized control cohort (6 and 12 weeks) | Engaging patients with cirrhotic liver disease awaiting liver transplant surgery in an intense, supervised exercise program was safe and feasible. |
| Control | 55.6 (mean) | 82.4% | 17.6% | ND | 13.2 (mean) | ND | ND | |||
| Román et al. [86] | Exercise | 62.0 (mean) | 71% | ND | 5.4 (mean) | 8.2 (mean) | 31.5 (mean) | ND | Randomized clinical trial (12 weeks) | A moderate exercise program for patients with cirrhosis led to greater functional capacity, greater muscle mass, and less body fat. |
| Relaxation | 63.1 (mean) | 78% | ND | 5.4 (mean) | 9.1 (mean) | 30.3 (mean) | ND | |||
| Macías-Rodríguez et al. [81] | Exercise | 53 (median) | 69% | 23% | 6 (median) | 9 (median) | 27.5 (mean) | ND | Randomized clinical trial (14 weeks) | A supervised physical exercise program for patients with cirrhosis decreased the HVPG and improved nutritional status, with no changes in the quality of life. |
| Control | 51 (median) | 83% | 33% | 6 (median) | 12 (median) | 27.4 (mean) | ND | |||
| Berzigotti et al. [82] | Lifestyle intervention (diet and exercise) | 56 (median) | 62% | 24% | Child A: 92% | 9 (median) | 33.3 (mean) | 42% | Prospective, multicenter, noncontrolled study (16 weeks) | Sixteen weeks of diet and moderate exercise were safe and reduced body weight and portal pressure in overweight/obese patients with cirrhosis and portal hypertension. |
| Kruger et al. [87] | HoBET | 53.0 (mean) | 50% | 25% | 6.35 (mean) | 9.05 (mean) | ND | ND | Randomized clinical trial (8 weeks) | Eight weeks of home-based exercise training was an effective therapy for improving peak aerobic power, submaximal aerobic endurance and thigh muscle mass in clinically stable Child—Pugh class A and B cirrhosis. |
| Control | 56.4 (mean) | 65% | 25% | 6.26 (mean) | 9.70 (mean) | ND | ND | |||
| Articles | BMI (kg/m2) | Liver Stiffness (kPa) | LFI | 6MWT (m) | Peak VO2 (mL/kg/min) | MAC (cm) | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | End of Study | p | Baseline | End of Study | p | Baseline | End of Study | Change from Baseline | Baseline | End of Study | p | Baseline | End of Study | p | Baseline | End of Study | p | |
| Sirisunhirun et al. [35] | 25.2 (mean) | 25.2 (mean) | 0.71 | 14.0 (mean) | 12.2 (mean) | 0.016 | ND | ND | 479.8 (mean) | 498.6 (mean) | 0.08 | ND | ND | ND | ND | |||
| Lai et al. [55] | ND | ND | ND | ND | 3.8 (median) | 3.6 (median) | −0.1 (−0.4–0.1) | ND | ND | ND | ND | ND | ND | |||||
| Chen et al. [75] | 29 (median) | 28 (median) | 0.98 | ND | ND | ND | ND | 423 (median) | 482 (median) | 0.05 | ND | ND | ND | ND | ||||
| Debette-Gratien et al. [77] | ND | ND | ND | ND | ND | ND | 480.6 (mean) | 520.6 (mean) | <0.02 | 21.5 (mean) | 23.2 (mean) | <0.008 | ND | ND | ||||
| Román et al. [83] | 26.7 (mean) | 27.0 (mean) | > 0.05 | ND | ND | ND | ND | 365 (median) | 445 (median) | 0.01 | ND | ND | 27.5 (mean) | 28.5 (mean) | >0.05 | |||
| Zenith et al. [84] | 27.7 (mean) | 28.0 (mean) | 0.17 | ND | ND | ND | ND | 529.1 (mean) | 570.5 (mean) | 0.02 | 23.3 (mean) | 27.3 (mean) | 0.01 | ND | ND | |||
| Morkane et al. [85] | 30.9 (mean) | 31.1 (mean) | 0.38 | ND | ND | ND | ND | ND | ND | 16.2 (mean) | 18.5 (mean) | 0.02 | 35.4 (mean) | 35.7 (mean) | 0.59 | |||
| Román et al. [86] | ND | ND | ND | ND | ND | ND | ND | ND | ND | ND | 34.1 (mean) | 33.5 (mean) | 0.02 | |||||
| Macías-Rodríguez et al. [81] | 27.9 (mean) | 28.2 (mean) | 0.889 | ND | ND | ND | ND | ND | ND | ND | ND | ND | ND | |||||
| Berzigotti et al. [82] | ND | ND | ND | ND | ND | ND | ND | ND | ND | ND | ND | ND | ||||||
| Kruger et al. [87] | 29.3 (mean) | 29.3 (mean) | 0.74 | ND | ND | ND | ND | 476.0 (mean) | 490.7 (mean) | 0.08 | 17.3 (mean) | 19.0 (mean) | 0.03 | ND | ND | |||
| Adverse Event | Corticosteroids | Calcineurin Inhibitors | mTor Inhibitors | Mycophenolate Mofetil |
|---|---|---|---|---|
| Kidney injury | - | +++ | + (proteinuria) | - |
| Hypercholesterolemia | + | + | +++ | - |
| Diabetes | ++ | + (tacrolimus) | - | - |
| Hypertension | + | ++ | + | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Farrugia, M.A.; Le Garf, S.; Chierici, A.; Piche, T.; Gual, P.; Iannelli, A.; Anty, R. Therapeutic Physical Exercise Programs in the Context of NASH Cirrhosis and Liver Transplantation: A Systematic Review. Metabolites 2023, 13, 330. https://doi.org/10.3390/metabo13030330
Farrugia MA, Le Garf S, Chierici A, Piche T, Gual P, Iannelli A, Anty R. Therapeutic Physical Exercise Programs in the Context of NASH Cirrhosis and Liver Transplantation: A Systematic Review. Metabolites. 2023; 13(3):330. https://doi.org/10.3390/metabo13030330
Chicago/Turabian StyleFarrugia, Marwin A., Sebastien Le Garf, Andrea Chierici, Thierry Piche, Philippe Gual, Antonio Iannelli, and Rodolphe Anty. 2023. "Therapeutic Physical Exercise Programs in the Context of NASH Cirrhosis and Liver Transplantation: A Systematic Review" Metabolites 13, no. 3: 330. https://doi.org/10.3390/metabo13030330
APA StyleFarrugia, M. A., Le Garf, S., Chierici, A., Piche, T., Gual, P., Iannelli, A., & Anty, R. (2023). Therapeutic Physical Exercise Programs in the Context of NASH Cirrhosis and Liver Transplantation: A Systematic Review. Metabolites, 13(3), 330. https://doi.org/10.3390/metabo13030330