
Investigation of Genetic Variants Associated with Tryptophan Metabolite Levels via Serotonin and Kynurenine Pathways in Patients with Bipolar Disorder

 ,
,  , ,
, ,  ,
,  ,
,  and
and  add
Show full author list
add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
2.1. Sample
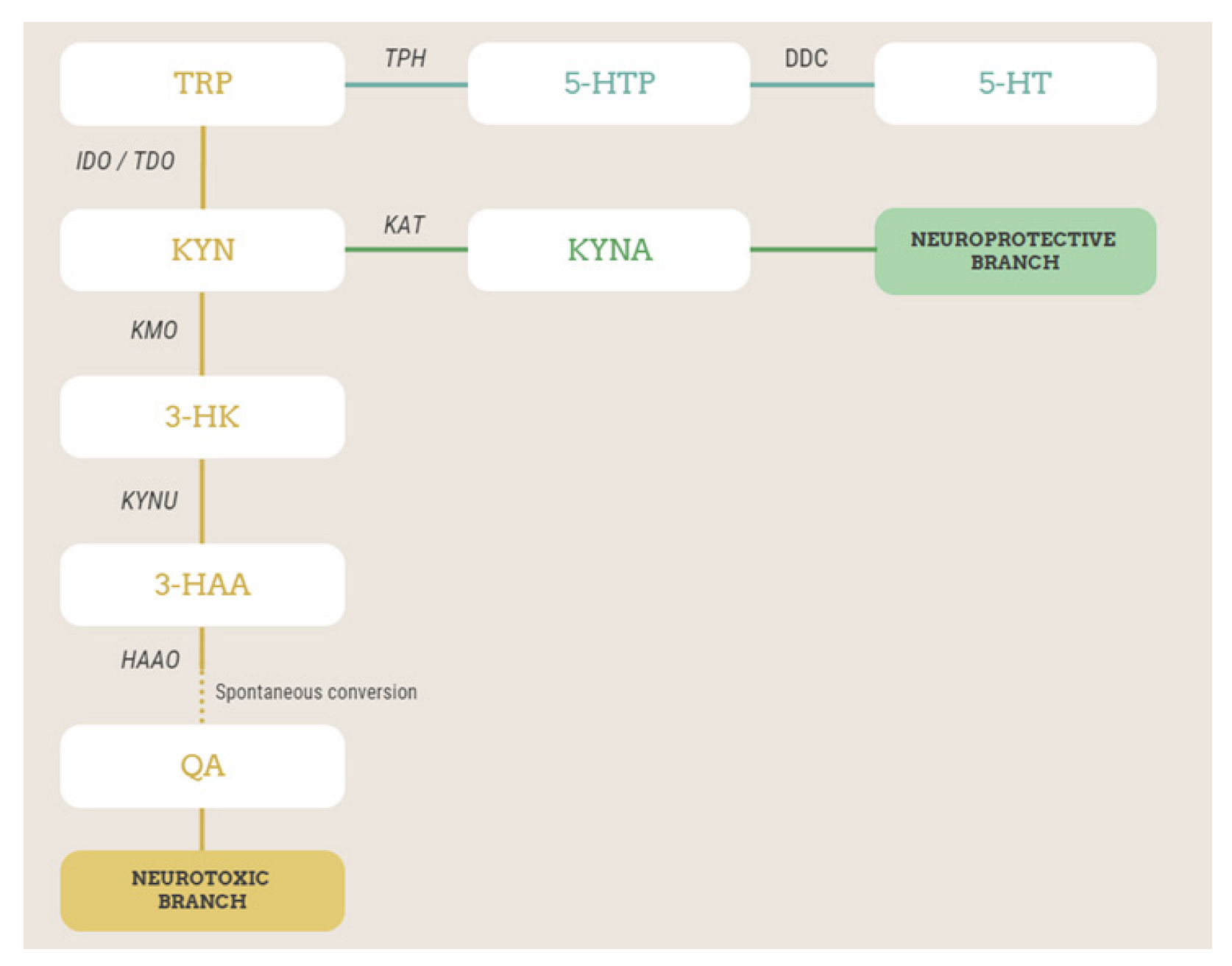
2.2. Measurement of Plasma Levels of TRP and Its Metabolites via 5-HT and KYN
2.3. Genotyping and Quality Control
2.4. Statistical Analysis
3. Results
3.1. Association Analysis of Metabolite Levels with Genetic Variants
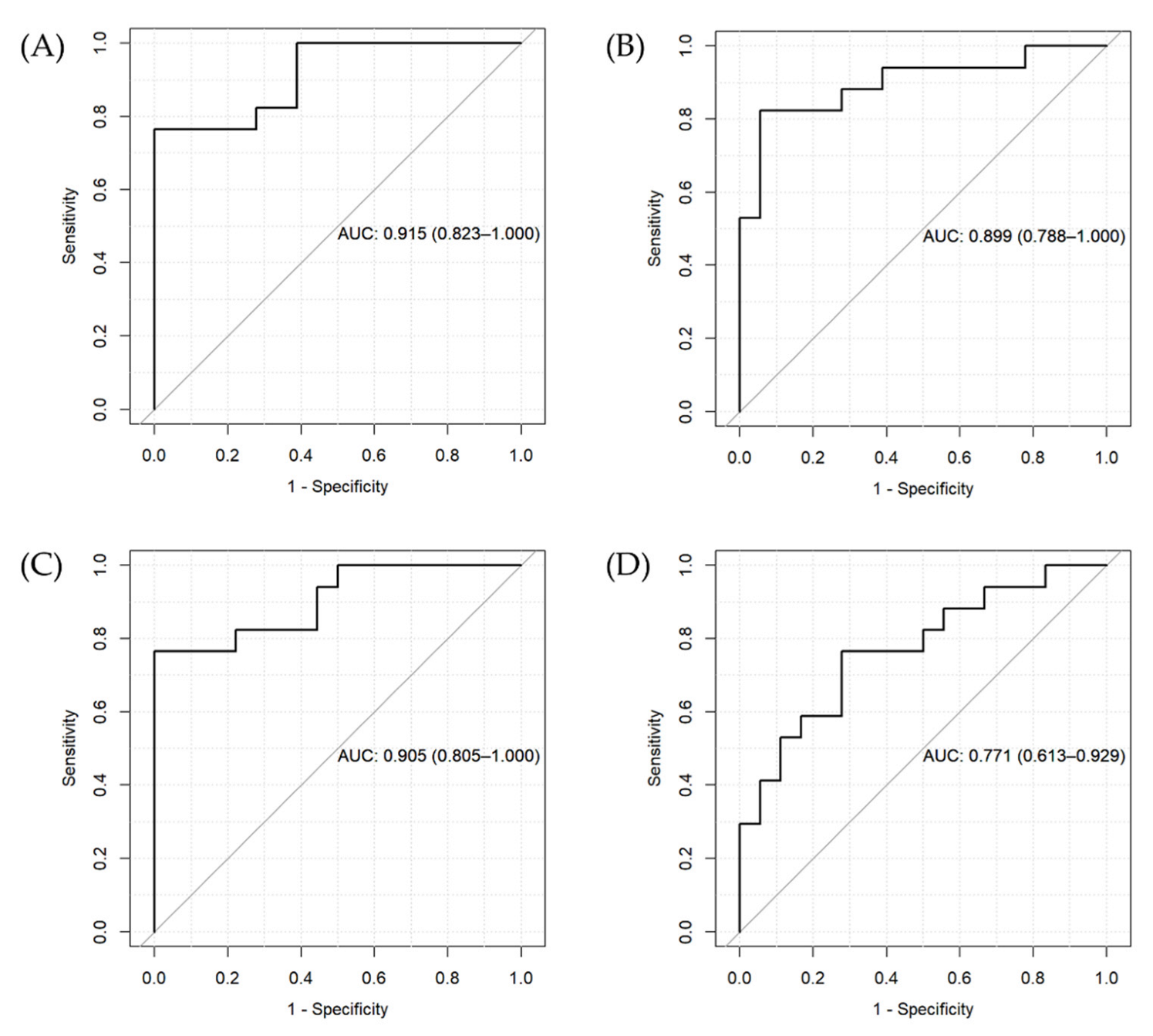
3.2. Penalized Regression with Diagnosis of BD as the Outcome
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Alda, M.; Manchia, M. Personalized management of bipolar disorder. Neurosci. Lett. 2018, 669, 3–9. [Google Scholar] [CrossRef] [PubMed]
- O’Donovan, C.; Garnham, J.S.; Hajek, T.; Alda, M. Antidepressant monotherapy in pre-bipolar depression; predictive value and inherent risk. J. Affect. Disord. 2008, 107, 293–298. [Google Scholar] [CrossRef] [PubMed]
- Bartoli, F.; Misiak, B.; Callovini, T.; Cavaleri, D.; Cioni, R.M.; Crocamo, C.; Savitz, J.B.; Carra, G. The kynurenine pathway in bipolar disorder: A meta-analysis on the peripheral blood levels of tryptophan and related metabolites. Mol. Psychiatry 2021, 26, 3419–3429. [Google Scholar] [CrossRef] [PubMed]
- Comai, S.; Bertazzo, A.; Brughera, M.; Crotti, S. Tryptophan in health and disease. Adv. Clin. Chem. 2020, 95, 165–218. [Google Scholar] [CrossRef]
- Comai, S.; Melloni, E.; Lorenzi, C.; Bollettini, I.; Vai, B.; Zanardi, R.; Colombo, C.; Valtorta, F.; Benedetti, F.; Poletti, S. Selective association of cytokine levels and kynurenine/tryptophan ratio with alterations in white matter microstructure in bipolar but not in unipolar depression. Eur. Neuropsychopharmacol. 2022, 55, 96–109. [Google Scholar] [CrossRef]
- Fellendorf, F.T.; Manchia, M.; Squassina, A.; Pisanu, C.; Dall’Acqua, S.; Sut, S.; Nasini, S.; Congiu, D.; Reininghaus, E.Z.; Garzilli, M.; et al. Is poor lithium response in individuals with bipolar disorder associated with increased degradation of tryptophan along the kynurenine pathway? Results of an exploratory study. J. Clin. Med. 2022, 11, 2517. [Google Scholar] [CrossRef]
- Poletti, S.; Melloni, E.; Aggio, V.; Colombo, C.; Valtorta, F.; Benedetti, F.; Comai, S. Grey and white matter structure associates with the activation of the tryptophan to kynurenine pathway in bipolar disorder. J. Affect. Disord. 2019, 259, 404–412. [Google Scholar] [CrossRef]
- Sellgren, C.M.; Gracias, J.; Jungholm, O.; Perlis, R.H.; Engberg, G.; Schwieler, L.; Landen, M.; Erhardt, S. Peripheral and central levels of kynurenic acid in bipolar disorder subjects and healthy controls. Transl. Psychiatry 2019, 9, 37. [Google Scholar] [CrossRef]
- Messaoud, A.; Rym, M.; Wahiba, D.; Neffati, F.; Najjar, M.F.; Gobbi, G.; Manchia, M.; Valtorta, F.; Lotfi, G.; Comai, S. Investigation of the relationship among cortisol, pro-inflammatory cytokines, and the degradation of tryptophan into kynurenine in patients with major depression and suicidal behavior. Curr. Top. Med. Chem. 2021; Online ahead of print. [Google Scholar] [CrossRef]
- Myint, A.M. Kynurenines: From the perspective of major psychiatric disorders. FEBS J. 2012, 279, 1375–1385. [Google Scholar] [CrossRef]
- Myint, A.M.; Kim, Y.K.; Verkerk, R.; Scharpe, S.; Steinbusch, H.; Leonard, B. Kynurenine pathway in major depression: Evidence of impaired neuroprotection. J. Affect. Disord. 2007, 98, 143–151. [Google Scholar] [CrossRef] [PubMed]
- Serafini, G.; Adavastro, G.; Canepa, G.; Capobianco, L.; Conigliaro, C.; Pittaluga, F.; Murri, M.B.; Valchera, A.; De Berardis, D.; Pompili, M.; et al. Abnormalities in Kynurenine Pathway Metabolism in Treatment-Resistant Depression and Suicidality: A Systematic Review. CNS Neurol. Disord. Drug Targets 2017, 16, 440–453. [Google Scholar] [CrossRef] [PubMed]
- Lavebratt, C.; Olsson, S.; Backlund, L.; Frisen, L.; Sellgren, C.; Priebe, L.; Nikamo, P.; Traskman-Bendz, L.; Cichon, S.; Vawter, M.P.; et al. The KMO allele encoding Arg452 is associated with psychotic features in bipolar disorder type 1, and with increased CSF KYNA level and reduced KMO expression. Mol. Psychiatry 2014, 19, 334–341. [Google Scholar] [CrossRef] [PubMed]
- Claes, S.; Myint, A.M.; Domschke, K.; Del-Favero, J.; Entrich, K.; Engelborghs, S.; De Deyn, P.; Mueller, N.; Baune, B.; Rothermundt, M. The kynurenine pathway in major depression: Haplotype analysis of three related functional candidate genes. Psychiatry Res. 2011, 188, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Ottenhof, K.W.; Sild, M.; Levesque, M.L.; Ruhe, H.G.; Booij, L. TPH2 polymorphisms across the spectrum of psychiatric morbidity: A systematic review and meta-analysis. Neurosci. Biobehav. Rev. 2018, 92, 29–42. [Google Scholar] [CrossRef]
- Manchia, M.; Squassina, A.; Pisanu, C.; Congiu, D.; Garzilli, M.; Guiso, B.; Suprani, F.; Paribello, P.; Pulcinelli, V.; Iaselli, M.N.; et al. Investigating the relationship between melatonin levels, melatonin system, microbiota composition and bipolar disorder psychopathology across the different phases of the disease. Int. J. Bipolar. Disord. 2019, 7, 27. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Arlington, VA, USA, 2013. [Google Scholar]
- Simonato, M.; Dall’Acqua, S.; Zilli, C.; Sut, S.; Tenconi, R.; Gallo, N.; Sfriso, P.; Sartori, L.; Cavallin, F.; Fiocco, U.; et al. Tryptophan metabolites, cytokines, and fatty acid binding protein 2 in myalgic encephalomyelitis/chronic fatigue syndrome. Biomedicines 2021, 9, 1724. [Google Scholar] [CrossRef]
- Purcell, S.; Neale, B.; Todd-Brown, K.; Thomas, L.; Ferreira, M.A.; Bender, D.; Maller, J.; Sklar, P.; de Bakker, P.I.; Daly, M.J.; et al. PLINK: A tool set for whole-genome association and population-based linkage analyses. Am. J. Hum. Genet. 2007, 81, 559–575. [Google Scholar] [CrossRef]
- Das, S.; Forer, L.; Schonherr, S.; Sidore, C.; Locke, A.E.; Kwong, A.; Vrieze, S.I.; Chew, E.Y.; Levy, S.; McGue, M.; et al. Next-generation genotype imputation service and methods. Nat. Genet. 2016, 48, 1284–1287. [Google Scholar] [CrossRef]
- Watanabe, K.; Taskesen, E.; van Bochoven, A.; Posthuma, D. Functional mapping and annotation of genetic associations with FUMA. Nat. Commun. 2017, 8, 1826. [Google Scholar] [CrossRef]
- Ranstam, J.; Cook, J.A. LASSO regression. Br. J. Surg. 2018, 105, 1348. [Google Scholar] [CrossRef]
- R Core Team. R: A Language and Environment for Statistical Computing. Available online: http://www.r-project.org/index.html (accessed on 11 October 2022).
- Liu, H.; Ding, L.; Zhang, H.; Mellor, D.; Wu, H.; Zhao, D.; Wu, C.; Lin, Z.; Yuan, J.; Peng, D. The metabolic factor kynurenic acid of kynurenine pathway predicts major depressive disorder. Front. Psychiatry 2018, 9, 552. [Google Scholar] [CrossRef] [PubMed]
- van den Ameele, S.; van Nuijs, A.L.; Lai, F.Y.; Schuermans, J.; Verkerk, R.; van Diermen, L.; Coppens, V.; Fransen, E.; de Boer, P.; Timmers, M.; et al. A mood state-specific interaction between kynurenine metabolism and inflammation is present in bipolar disorder. Bipolar. Disord. 2020, 22, 59–69. [Google Scholar] [CrossRef] [PubMed]
- Gadelha, A.; Coleman, J.; Breen, G.; Mazzoti, D.R.; Yonamine, C.M.; Pellegrino, R.; Ota, V.K.; Belangero, S.I.; Glessner, J.; Sleiman, P.; et al. Genome-wide investigation of schizophrenia associated plasma Ndel1 enzyme activity. Schizophr. Res. 2016, 172, 60–67. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Krull, F.; Akkouh, I.; Hughes, T.; Bettella, F.; Athanasiu, L.; Smeland, O.B.; O’Connell, K.S.; Brattbakk, H.R.; Steen, V.M.; Steen, N.E.; et al. Dose-dependent transcriptional effects of lithium and adverse effect burden in a psychiatric cohort. Prog. Neuropsychopharmacol. Biol. Psychiatry 2022, 112, 110408. [Google Scholar] [CrossRef] [PubMed]
- Lu, S.; Hernan, R.; Marcogliese, P.C.; Huang, Y.; Gertler, T.S.; Akcaboy, M.; Liu, S.; Chung, H.L.; Pan, X.; Sun, X.; et al. Loss-of-function variants in TIAM1 are associated with developmental delay, intellectual disability, and seizures. Am. J. Hum. Genet. 2022, 109, 571–586. [Google Scholar] [CrossRef]
- Buoli, M.; Caldiroli, A.; Cumerlato Melter, C.; Serati, M.; de Nijs, J.; Altamura, A.C. Biological aspects and candidate biomarkers for psychotic bipolar disorder: A systematic review. Psychiatry Clin. Neurosci. 2016, 70, 227–244. [Google Scholar] [CrossRef]
- Le-Niculescu, H.; Roseberry, K.; Gill, S.S.; Levey, D.F.; Phalen, P.L.; Mullen, J.; Williams, A.; Bhairo, S.; Voegtline, T.; Davis, H.; et al. Precision medicine for mood disorders: Objective assessment, risk prediction, pharmacogenomics, and repurposed drugs. Mol. Psychiatry 2021, 26, 2776–2804. [Google Scholar] [CrossRef]
- Duan, J.; Wei, Y.; Womer, F.Y.; Zhang, X.; Chang, M.; Zhu, Y.; Liu, Z.; Li, C.; Yin, Z.; Zhang, R.; et al. Neurobiological substrates of major psychiatry disorders: Transdiagnostic associations between white matter abnormalities, neuregulin 1 and clinical manifestation. J. Psychiatry Neurosci. 2021, 46, E506–E515. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Patients with BD (n = 44) | HCs (n = 45) | Statistics | p | |
|---|---|---|---|---|
| Age (years) | 51.94 (±11.01) | 50.99 (±8.06) | t = −0.47 | 0.64 |
| Sex (% F) | 63.6 | 64.4 | X2 = 0.00 | 1.00 |
| BMI | 25.77 (±5.23) | 23.66 (±3.52) | t = 2.24 | 0.028 |
| TRP [μg/mL] | 9.41 (±1.64) | 11.15 (±1.7) | F = 24.74 | 3.4 × 10−6 |
| KYN [μg/mL] | 0.35 (±0.10) | 0.39 (±0.14) | F = 2.87 | 0.09 |
| KYNA [ng/mL] | 9.28 (±4.66) | 10.53 (±8.27) | F = 0.77 | 0.38 |
| 3-HK [ng/mL] | 42.55 (±2.94) | 44.16 (±13.36) | F = 0.66 | 0.42 |
| QA [ng/mL] | 143.49 (±15.09) | 159.37 (±46.51) | F = 4.65 | 0.034 |
| 5-HTP [ng/mL] | 87.36 (±30.38) | 69.78 (±35.26) | F = 6.33 | 0.014 |
| 5-HT [ng/mL] | 324.02 (±175.24) | 245.18 (±147.00) | F = 5.23 | 0.025 |
| MLT [pg/mL] | 10.97 (±5.90) | 11.95 (±5.90) | F = 0.61 | 0.44 |
| KYN/TRP × 1000 ratio | 38.77 (±14.93) | 35.75 (±11.76) | F = 1.10 | 0.30 |
| 3-HK/KYN ratio | 131.82 (±39.93) | 128.1 (±66.29) | F = 0.10 | 0.75 |
| KYNA/KYN ratio | 28.8 (±16.72) | 29.48 (±25.85) | F = 0.02 | 0.89 |
| QA/KYNA ratio | 22.57 (±19.00) | 22.34 (±14.44) | F = 0.00 | 0.95 |
| 5-HTP/TRP ratio | 9.44 (±3.35) | 6.34 (±3.25) | F = 19.86 | 2.6 × 10−5 |
| All | BD Patients | Controls | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CHR | SNP | Gene | EA | OA | BETA | p | EAF | BETA | p | EAF | BETA | p |
| 5-HT | ||||||||||||
| 3 | rs73153916 | RP11-23D24.2 | T | C | 275.6 | 1.2 × 10−9 | 0.08 | 259.8 | 6.1 × 10−6 | 0.03 | 322.9 | 1.0 × 10−4 |
| 5-HTP | ||||||||||||
| 3 | rs11130047 | Intergenic | A | G | 62.96 | 2.5 × 10−8 | 0.05 | 32.26 | 0.08 | 0.06 | 84.04 | 8.4 × 10−9 |
| 10 | rs7902231 | Intergenic | A | C | 58.09 | 1.9 × 10−9 | 0.06 | 39.15 | 0.008 | 0.08 | 73.25 | 2.5 × 10−8 |
| TRP | ||||||||||||
| 5 | rs292212 | Intergenic | A | G | 2.70 | 4.1 × 10−8 | 0.07 | 2.37 | 0.001 | 0.06 | 3.06 | 2.5 × 10−5 |
| 5-HTP/TRP | ||||||||||||
| 2 | rs10209883 | Intergenic | A | G | 3.07 | 4.0 × 10−8 | 0.26 | 3.02 | 6.8 × 10−5 | 0.21 | 3.28 | 2.0 × 10−4 |
| 10 | rs7902231 | Intergenic | A | C | 6.11 | 1.2 × 10−10 | 0.06 | 5.74 | 3.0 × 10−4 | 0.08 | 6.48 | 7.7 × 10−8 |
| KYN/TRP | ||||||||||||
| 3 | rs13063065 | ZNF385D | G | T | 19.61 | 3.6 × 10−8 | 0.07 | 26.3 | 1.9 × 10−4 | 0.13 | 17.17 | 3.3 × 10−5 |
| QA | ||||||||||||
| 4 | rs6827515 | Intergenic | A | G | 51.62 | 3.6 × 10−8 | 0.08 | 8.92 | 0.16 | 0.06 | 90.35 | 1.7 × 10−8 |
| 5 | rs715692 | COMMD10 | C | G | 59.27 | 6.5 × 10−9 | 0.06 | 11.39 | 0.12 | 0.04 | 98.90 | 4.0 × 10−9 |
| 7 | rs116926743 | Intergenic | C | G | 57.90 | 2.2 × 10−8 | 0.06 | 5.03 | 0.51 | 0.04 | 96.33 | 1.3 × 10−8 |
| 8 | rs425094 | NRG1 | C | T | 47.19 | 3.0 × 10−8 | 0.08 | 3.89 | 0.54 | 0.09 | 76.56 | 3.7 × 10−8 |
| 12 | rs10843992 | ETFBKMT | C | T | 59.01 | 6.3 × 10−9 | 0.05 | -5.73 | 0.50 | 0.06 | 95.82 | 1.7 × 10−9 |
| 14 | rs4645874 | Intergenic | T | C | 38.38 | 3.2 × 10−8 | 0.15 | 7.88 | 0.17 | 0.11 | 58.13 | 1.9 × 10−7 |
| 17 | rs117632415 | Intergenic | A | G | 64.48 | 3.9 × 10−10 | 0.05 | 3.05 | 0.73 | 0.06 | 97.57 | 1.4 × 10−9 |
| 18 | rs77048355 | RP11-25I11.1 | A | G | 59.06 | 1.0 × 10−8 | 0.08 | 3.60 | 0.63 | 0.03 | 119.6 | 3.1 × 10−13 |
| CHR | SNP | Gene | EA | OA | EAF | BETA | p |
|---|---|---|---|---|---|---|---|
| 5-HT | |||||||
| 1 | rs10913387 | Intergenic | T | G | 0.23 | 152.3 | 4.2 × 10−8 |
| 3-HK | |||||||
| 13 | rs9579535 | Intergenic | A | G | 0.06 | 15.27 | 3.2 × 10−8 |
| KYNA | |||||||
| 5 | rs115379324 | PLEKHG4B | A | G | 0.05 | 11.55 | 4.6 × 10−8 |
| 10 | rs74119224 | CAMK1D | A | G | 0.06 | 11.20 | 1.3 × 10−8 |
| 12 | rs112998010 | Intergenic | T | C | 0.06 | 10.61 | 4.2 × 10−9 |
| 15 | rs62030183 | C15orf27 (TMEM266) | T | C | 0.06 | 11.34 | 2.9 × 10−10 |
| QA | |||||||
| 1 | rs17466728 | RP5-884C9.2 | A | T | 0.06 | 57.01 | 5.8 × 10−9 |
| 3 | rs80184502 | CD96 | C | A | 0.05 | 60.55 | 4.2 × 10−9 |
| 7 | rs138032435 | Intergenic | A | G | 0.05 | 57.51 | 1.9 × 10−8 |
| 9 | rs111735019 | Intergenic | T | A | 0.06 | 55.53 | 1.5 × 10−8 |
| 12 | rs200629811 | Intergenic | T | C | 0.05 | 56.66 | 3.9 × 10−8 |
| 13 | rs9556820 | Intergenic | T | C | 0.08 | 49.65 | 4.0 × 10−10 |
| 16 | rs77023911 | Intergenic | T | C | 0.06 | 53.21 | 3.3 × 10−8 |
| 16 | rs62041963 | RP11-467I17.1 | T | C | 0.10 | 47.39 | 6.8 × 10−10 |
| 17 | rs72842909 | ALOX15B | T | C | 0.07 | 51.96 | 2.8 × 10−8 |
| 17 | rs184751267 | Intergenic | T | C | 0.05 | 63.07 | 6.6 × 10−10 |
| 19 | rs73041282 | YIF1B | A | G | 0.06 | 59.95 | 1.2 × 10−9 |
| 19 | rs113703374 | IFNL3 | A | G | 0.06 | 57.49 | 5.1 × 10−9 |
| KYNA/KYN | |||||||
| 1 | rs1888826 | ADCK3 | T | C | 0.10 | 24.77 | 4.0 × 10−8 |
| 2 | rs141988608 | Intergenic | T | C | 0.07 | 32.59 | 1.4 × 10−8 |
| 9 | rs10810150 | Intergenic | T | C | 0.08 | 30.17 | 1.8 × 10−8 |
| 10 | rs12413445 | Intergenic | C | G | 0.06 | 33.67 | 4.7 × 10−8 |
| 13 | rs9580486 | Intergenic | T | C | 0.05 | 36.47 | 1.1 × 10−8 |
| 14 | rs2031065 | Intergenic | C | T | 0.05 | 39.93 | 3.6 × 10−8 |
| 15 | rs32030170 | C15orf27 (TMEM266) | T | C | 0.06 | 34.54 | 7.7 × 10−9 |
| QA/KYNA | |||||||
| 12 | rs73041300 | LINC00942 | A | G | 0.07 | 25.46 | 1.3 × 10−8 |
| 13 | rs9587565 | Intergenic | A | G | 0.06 | 28.11 | 3.4 × 10−9 |
| 15 | rs1967975516 | Intergenic | G | C | 0.06 | 29.56 | 1.1 × 10−10 |
| 21 | rs138622229 | TIAM1 | A | C | 0.05 | 35.14 | 2.1 × 10−13 |
| MLT | |||||||
| 5 | rs6862509 | AC011343.1 | C | G | 0.06 | 9.89 | 2.7 × 10−8 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pisanu, C.; Squassina, A.; Paribello, P.; Dall’Acqua, S.; Sut, S.; Nasini, S.; Bertazzo, A.; Congiu, D.; Meloni, A.; Garzilli, M.; et al. Investigation of Genetic Variants Associated with Tryptophan Metabolite Levels via Serotonin and Kynurenine Pathways in Patients with Bipolar Disorder. Metabolites 2022, 12, 1127. https://doi.org/10.3390/metabo12111127
Pisanu C, Squassina A, Paribello P, Dall’Acqua S, Sut S, Nasini S, Bertazzo A, Congiu D, Meloni A, Garzilli M, et al. Investigation of Genetic Variants Associated with Tryptophan Metabolite Levels via Serotonin and Kynurenine Pathways in Patients with Bipolar Disorder. Metabolites. 2022; 12(11):1127. https://doi.org/10.3390/metabo12111127
Chicago/Turabian StylePisanu, Claudia, Alessio Squassina, Pasquale Paribello, Stefano Dall’Acqua, Stefania Sut, Sofia Nasini, Antonella Bertazzo, Donatella Congiu, Anna Meloni, Mario Garzilli, and et al. 2022. "Investigation of Genetic Variants Associated with Tryptophan Metabolite Levels via Serotonin and Kynurenine Pathways in Patients with Bipolar Disorder" Metabolites 12, no. 11: 1127. https://doi.org/10.3390/metabo12111127
APA StylePisanu, C., Squassina, A., Paribello, P., Dall’Acqua, S., Sut, S., Nasini, S., Bertazzo, A., Congiu, D., Meloni, A., Garzilli, M., Guiso, B., Suprani, F., Pulcinelli, V., Iaselli, M. N., Pinna, I., Somaini, G., Arru, L., Corrias, C., Pinna, F., ... Manchia, M. (2022). Investigation of Genetic Variants Associated with Tryptophan Metabolite Levels via Serotonin and Kynurenine Pathways in Patients with Bipolar Disorder. Metabolites, 12(11), 1127. https://doi.org/10.3390/metabo12111127