
Thromboembolic Complications of SARS-CoV-2 and Metabolic Derangements: Suggestions from Clinical Practice Evidence to Causative Agents


Abstract

1. SARS-CoV-2 Pathogenesis, Hemostatic Alterations and Metabolism Interference of Therapeutical Agents
1.1. SARS-CoV-2 Infection Strategy and Host Immune Response
1.2. Alteration of Hematological Parameters from Clinical Experience of Thromboembolic Events
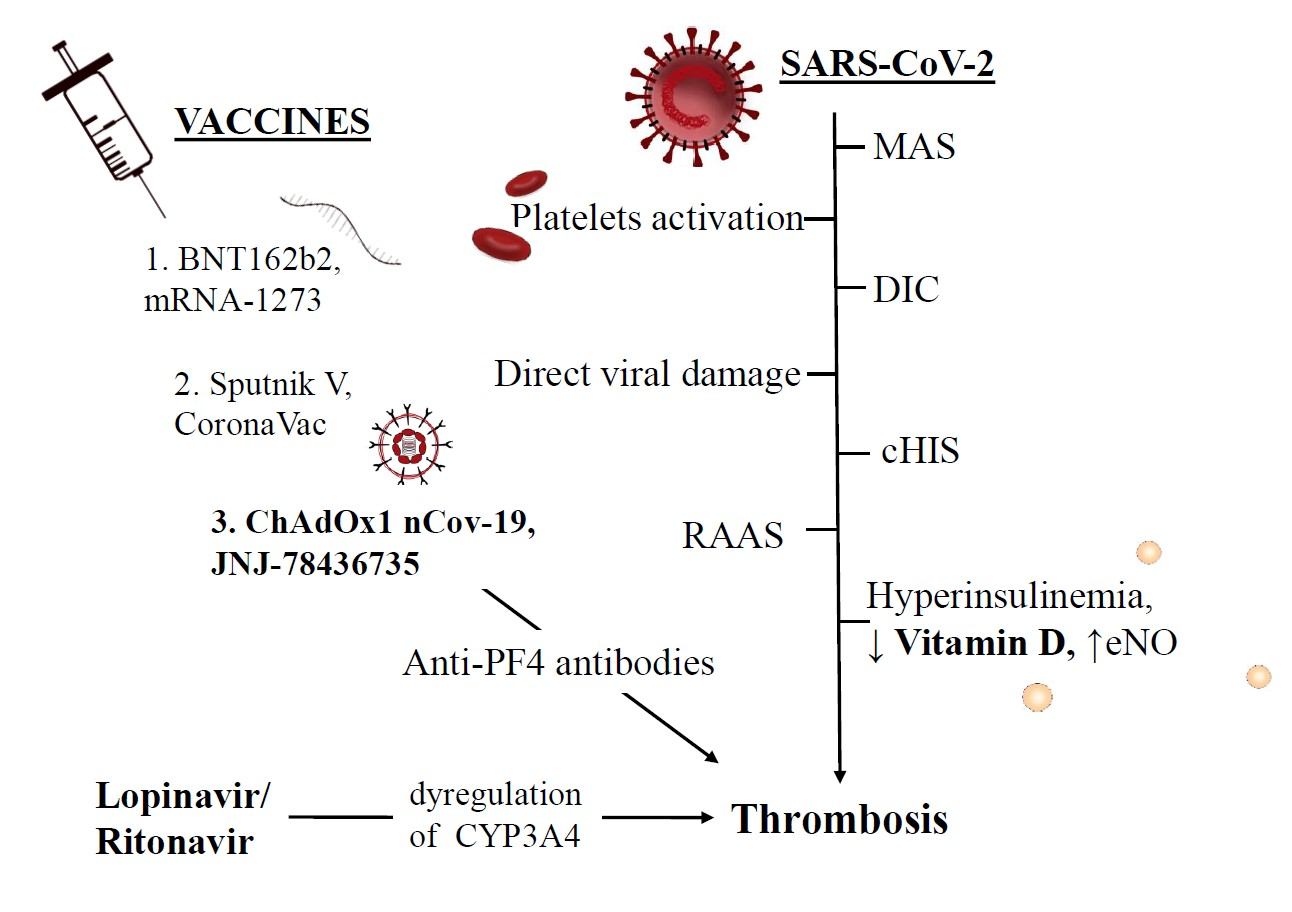
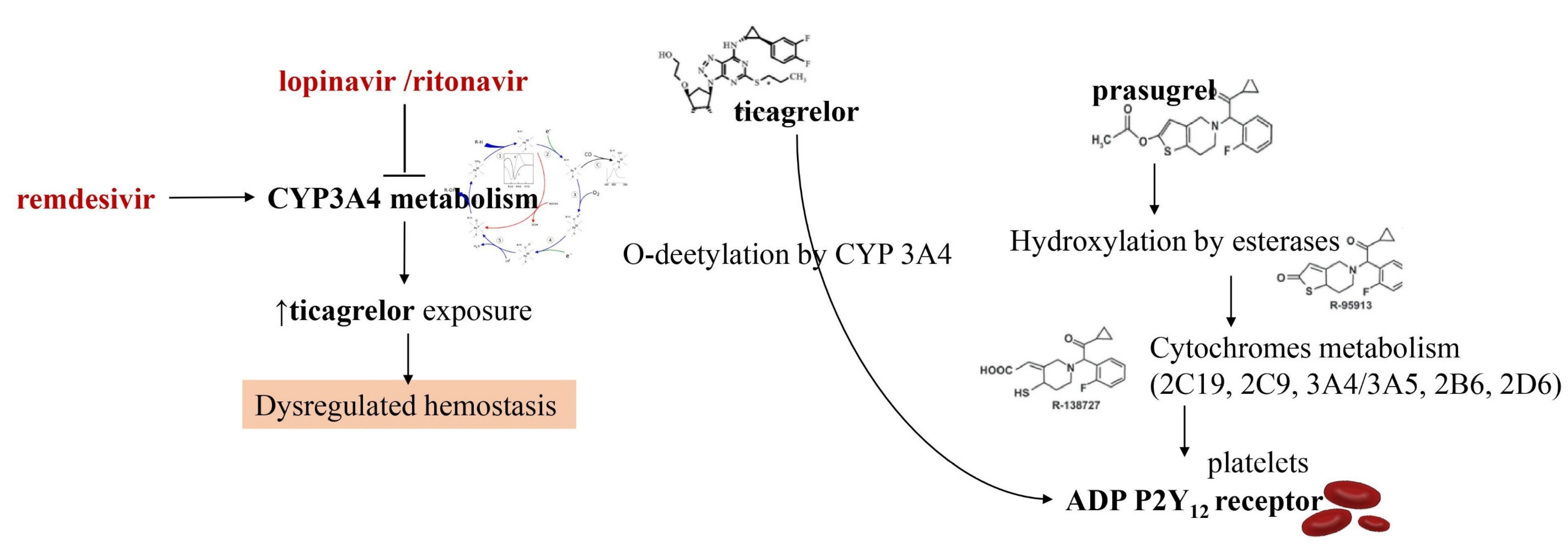
1.3. Interference of Antiviral Drugs with Antiplatelet and Anticoagulant Medications
2. Venous Thromboembolism Diagnosed in Covid-19 Patients and Management
2.1. Clinical Diagnoses of Venous Thromboembolism
2.2. Medical Treatment in the Acute Setting and on Discharge
2.3. Pulmonary Embolism in Covid-19 Patients: Stratification and Choice of Therapy
2.4. Management of Antithrombotic Drugs in Patients with SARS-CoV-2 Infection and Critical Illness
2.5. Risk Stratification Scores to Drive Pharmacological Prophylactic Treatment
3. Hypotheses of Thrombosis Generation and Pathophysiological Mechanisms
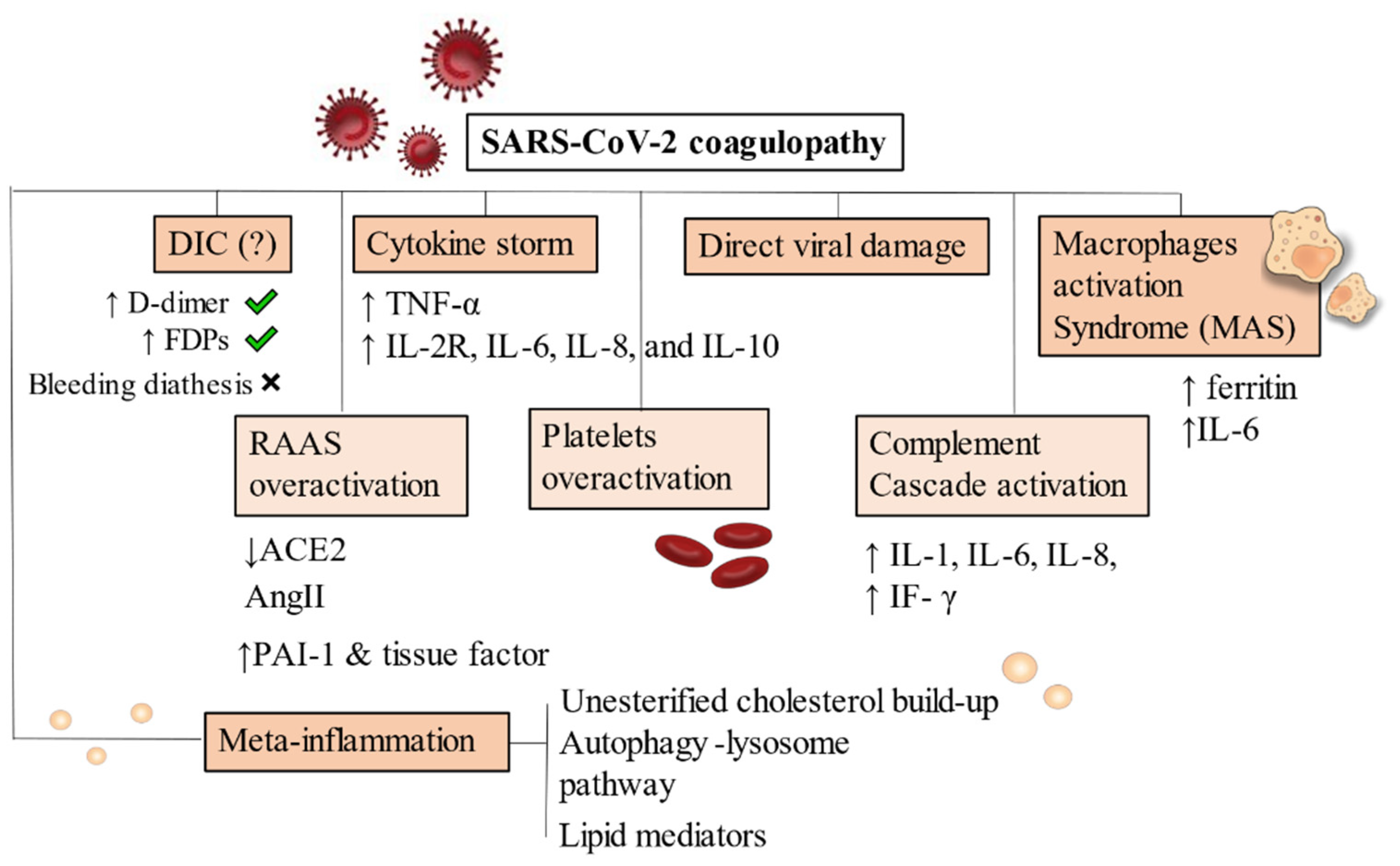
3.1. Covid-19 and Disseminated Intravascular Coagulation
3.2. Direct Viral Damage and Endothelitis-Driven Inflammatory Reaction
3.3. Covid-19-Associated Hyperinflammatory Syndrome (cHIS)
4. Inflammatory Cascade: The Bridge between Metabolic Derangements and Thrombogenesis
The Immunologic Dialogue of Cytokines, T Cells, and Checkpoint Proteins Accelerating Thrombosis in Atherosclerotic Lesions
5. Meta-Inflammation: Alterations of Metabolism Leading to Thrombus Generation
5.1. Obesity, Metabolic Syndrome and Dysregulated Lipid Metabolism
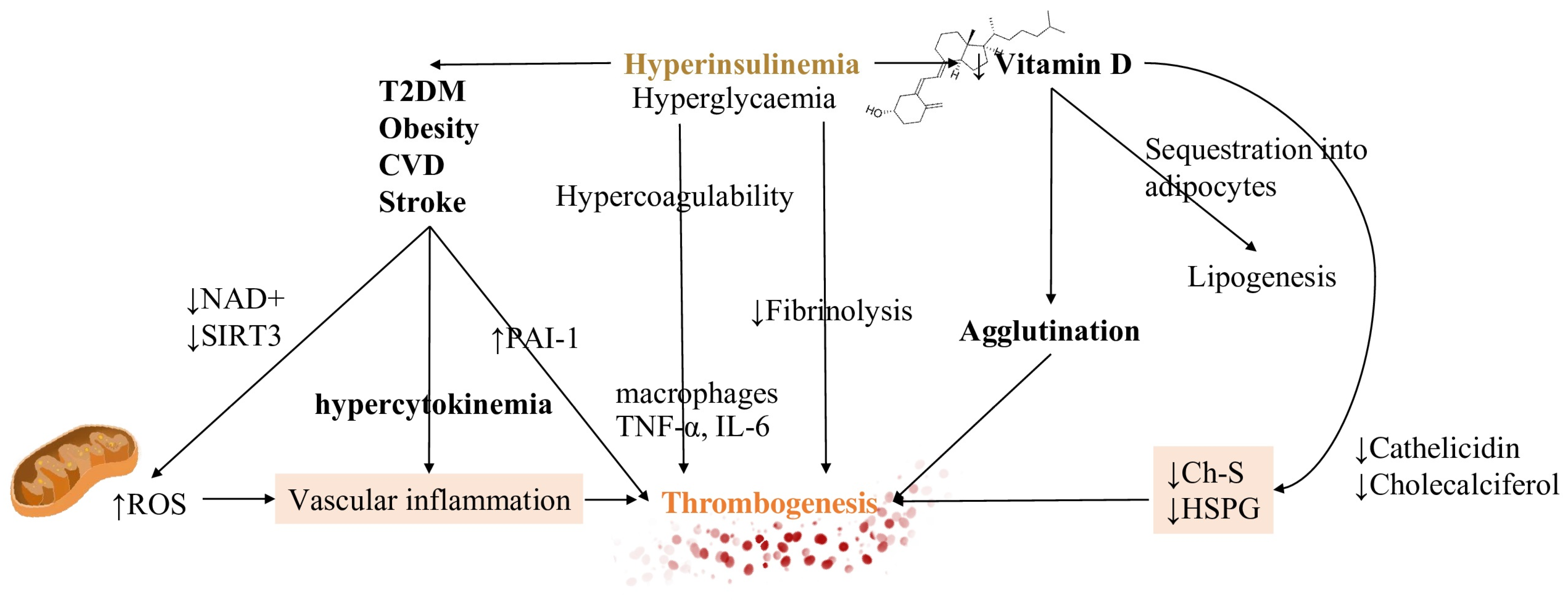
5.2. Hyperinsulinemia Contributes to Both Impaired Fibrinolysis and Hypercoagulable States
5.3. Vitamin D Metabolism and Its Interference in the Inflammatory Pathway
5.4. Extrahepatic Vitamin K Insufficiency and Dependency of Coagulation Factors
5.5. Hormonal Factors Contributing to Covid-19 Thrombotic Complications
6. Disorders of Haemostasis and ChAdOx1 nCoV-19 Adenoviral Vector Vaccine
7. Future Directions and Perspectives
8. Conclusions
Funding
Conflicts of Interest
Abbreviations
References
- Walls, A.C.; Park, Y.J.; Tortorici, M.A.; Wall, A.; McGuire, A.T.; Veesler, D. Structure, function, and antigenicity of the SARS-CoV-2 spike glycoprotein. Cell 2020, 181, 281–292. [Google Scholar] [CrossRef]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef]
- Zhang, H.; Penninger, J.M.; Li, Y.; Zhong, N.; Slutsky, A.S. Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 re-ceptor: Molecular mechanisms and potential therapeutic target. Intensive Care Med. 2020, 46, 586–590. [Google Scholar] [CrossRef]
- Van Doremalen, N.; Bushmaker, T.; Morris, D.H.; Holbrook, M.G.; Gamble, A.; Williamson, B.N.; Tamin, A.; Harcourt, J.L.; Thornburg, N.J.; Gerber, S.I.; et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N. Engl. J. Med. 2020, 382, 1564–1567. [Google Scholar] [CrossRef]
- Zhou, P.; Yang, X.L.; Wang, X.G.; Hu, B.; Zhang, L.; Zhang, W.; Si, H.R.; Zhu, Y.; Li, B.; Huang, C.L.; et al. A pneumonia outbreak associated with a new coronavirus of probable bat origin. Nature 2020, 579, 270–273. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneu-monia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef]
- Wu, Z.; McGoogan, J.M. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: Summary of a report of 72 314 cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated With Acute Respiratory Distress Syndrome and Death in Patients With Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934–943. [Google Scholar] [CrossRef]
- Volz, E.; Mishra, S.; Chand, M.; Barrett, J.C.; Johnson, R.; Geidelberg, L.; Hinsley, W.R.; Laydon, D.J.; Dabrera, G.; O’Toole, Á.; et al. Transmission of SARS-CoV-2 lineage B.1.1.7 in England: Insights from linking epidemio-logical and genetic data. medRxiv 2021. [Google Scholar] [CrossRef]
- Faria, N.R.; Claro, I.M.; Candido, D.; Franco, L.A.M.; Andrade, P.S.; Coletti, T.M.; Silva, C.A.M.; Sales, F.C.; Manuli, E.R.; Aguiar, R.S.; et al. Genomic characterization of an emergent SARS-CoV-2 lineage in Manaus: Prelimi-nary findings. Virological 2021. [Google Scholar] [CrossRef]
- Tegally, H.; Wilkinson, E.; Giovanetti, M.; Iranzadeh, A.; Fonseca, V.; Giandhari, J.; Doolabh, D.; Pillay, S.; San, E.J.; Msomi, N.; et al. Emergence and rapid spread of a new severe acute respiratory syn-drome-related coronavirus 2 (SARS-CoV-2) lineage with multiple spike mutations in South Africa. MedRxiv 2020. [Google Scholar] [CrossRef]
- Yang, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult in patients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar]
- Bester, J.; Pretorius, E. Effects of IL-1β, IL-6 and IL-8 on erythrocytes, platelets and clot viscoelasticity. Sci. Rep. 2016, 6, 32188. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Plebani, M.; Henry, B.M. Thrombocytopenia is associated with severe coronavirus disease 2019 (COVID-19) infec-tions: A meta-analysis. Clin. Chim. Acta 2020, 506, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Favaloro, E.J. D-dimer is associated with severity of coronavirus disease 2019: A pooled analysis. Thromb. Haemost. 2020, 120, 876–878. [Google Scholar] [CrossRef] [PubMed]
- Chen, G.; Wu, D.; Guo, W.; Cao, Y.; Huang, D.; Wang, H.; Wang, T.; Zhang, X.; Chen, H.; Yu, H.; et al. Clinical and immunological fea-tures of severe and moderate coronavirus disease 2019. J. Clin. Investig. 2020, 130, 2620–2629. [Google Scholar] [CrossRef]
- Chen, T.; Wu, D.; Chen, H.; Yan, W.; Yang, D.; Chen, G.; Ma, K.; Xu, D.; Yu, H.; Wang, H.; et al. Clinical characteristics of 113 deceased patients with coronavirus disease 2019: Retrospective study. BMJ 2020, 368, m1091. [Google Scholar] [CrossRef]
- Tang, N.; Li, D.; Wang, X.; Sun, Z. Abnormal coagulation parameters are associated with poor prognosis in patients with novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 844–847. [Google Scholar] [CrossRef]
- Zhang, L.; Yan, X.; Fan, Q.; Liu, H.; Liu, X.; Liu, Z.; Zhang, Z. D-dimer levels on admission to predict in-hospital mortality in patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1324–1329. [Google Scholar] [CrossRef]
- Gris, J.C.; Quéré, I.; Pérez-Martin, A.; Lefrant, J.Y.; Sotto, A. Uncertainties on the prognostic value of D-dimers in COVID-19 patients. J. Thromb. Haemost. 2020, 18, 2066–2067. [Google Scholar] [CrossRef]
- Han, H.; Yang, L.; Liu, R.; Liu, F.; Wu, K.L.; Li, J.; Liu, X.H.; Zhu, C.L. Prominent changes in blood coagulation of patients with SARS-CoV-2 infection. Clin. Chem. Lab. Med. 2020, 58, 1116–1120. [Google Scholar] [CrossRef]
- Lippi, G.; Plebani, M. Laboratory abnormalities in patients with COVID-2019 infection. Clin. Chem. Lab. Med. 2020, 58, 1131–1134. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef]
- Gao, Y.; Li, T.; Han, M.; Li, X.; Wu, D.; Xu, Y.; Zhu, Y.; Liu, Y.; Wang, X.; Wang, L. Diagnostic utility of clinical laboratory data determinations for patients with the severe COVID-19. J. Med. Virol. 2020, 92, 791–796. [Google Scholar] [CrossRef]
- Stoneham, S.M.; Milne, K.M.; Nuttall, E.; Frew, G.H.; Sturrock, B.R.; Sivaloganathan, H.; Ladikou, E.E.; Drage, S.; Phillips, B.; Chevassut, T.J.; et al. Thrombotic risk in COVID-19: A case series and case-control study. Clin. Med. 2020, 20, e76–e81. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Y.; Zuo, M.; Yalavarthi, S.; Gockman, K.; Madison, J.A.; Shi, H.; Woodard, W.; Lezak, S.P.; Lugogo, N.L.; Knight, J.S.; et al. Neutrophil extracellular traps and thrombosis in COVID-19. J. Thromb. Thrombolysis 2021, 51, 446–453. [Google Scholar] [CrossRef]
- Zhang, L.; Feng, X.; Zhang, D.; Jiang, C.; Mei, H.; Wang, J.; Zhang, C.; Li, H.; Xia, X.; Kong, S.; et al. Deep Vein Thrombosis in Hospitalized Patients With COVID-19 in Wuhan, China: Prevalence, Risk Factors, and Outcome. Circulation 2020, 142, 114–128. [Google Scholar] [CrossRef]
- Planquette, B.; Le Berre, A.; Khider, L.; Yannoutsos, A.; Gendron, N.; de Torcy, M.; Mohamedi, N.; Jouveshomme, S.; Smadja, D.M.; Lazareth, I.; et al. Prevalence and characteristics of pulmonary embolism in 1042 COVID-19 patients with respiratory symptoms: A nested case-control study. Thromb. Res. 2021, 197, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Trimaille, A.; Curtiaud, A.; Marchandot, B.; Matsushita, K.; Sato, C.; Leonard-Lorant, I.; Sattler, L.; Grunebaum, L.; Ohana, M.; Von Hunolstein, J.J.; et al. Venous thromboembolism in non-critically ill patients with COVID-19 infection. Thromb. Res. 2020, 193, 166–169. [Google Scholar] [CrossRef]
- Shah, A.; Donovan, K.; McHugh, A.; Pandey, M.; Aaron, L.; Bradbury, C.A.; Stanworth, S.J.; Alikhan, R.; Von Kier, S.; Maher, K.; et al. Thrombotic and haemorrhagic complications in critically ill patients with COVID-19: A multicentre observational study. Crit Care 2020, 24, 561. [Google Scholar] [CrossRef]
- Koleilat, I.; Galen, B.; Choinski, K.; Hatch, A.N.; Jones, D.B.; Billett, H.; Indes, J.; Lipsitz, E. Clinical characteristics of acute lower extremity deep venous thrombosis diagnosed by duplex in patients hospitalized for coronavirus disease 2019. J. Vasc. Surg. Venous Lymphat. Disord. 2021, 9, 36–46. [Google Scholar] [CrossRef]
- Kampouri, E.; Filippidis, P.; Viala, B.; Méan, M.; Pantet, O.; Desgranges, F.; Tschopp, J.; Regina, J.; Karachalias, E.; Bianchi, C.; et al. Predicting Venous Thromboembolic Events in Patients with Coronavirus Disease 2019 Requiring Hospitalization: An Observational Retrospective Study by the COVIDIC Initiative in a Swiss University Hospital. Biomed. Res. Int. 2020, 2020, 9126148. [Google Scholar] [CrossRef]
- Koupenova, M.; Corkrey, H.A.; Vitseva, O.; Manni, G.; Pang, C.J.; Clancy, L.; Yao, C.; Rade, J.; Levy, D.; Wang, J.P.; et al. The role of platelets in mediating a response to human influenza infection. Nat. Commun. 2019, 10, 1–18. [Google Scholar] [CrossRef]
- Koupenova, M.; Clancy, L.; Corkrey, H.A.; Freedman, J.E. Circulating Platelets as Mediators of Immunity, Inflammation, and Thrombosis. Circ. Res. 2018, 122, 337–351. [Google Scholar] [CrossRef] [PubMed]
- Koupenova, M. Potential role of platelets in COVID-19: Implications for thrombosis. Res. Pr. Thromb. Haemost. 2020, 4, 737–740. [Google Scholar] [CrossRef]
- Yang, X.; Yang, Q.; Wang, Y.; Wu, Y.; Xu, J.; Yu, Y.; Shang, Y. Thrombocytopenia and its association with mortality in patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1469–1472. [Google Scholar] [CrossRef]
- Pang, J.; Xu, F.; Aondio, G.; Li, Y.; Fumagalli, A.; Lu, M.; Valmadre, G.; Wei, J.; Bian, Y.; Canesi, M.; et al. Efficacy and tolerability of bevacizumab in patients with severe Covid-19. Nat. Commun. 2021, 12, 1–10. [Google Scholar] [CrossRef]
- Totzeck, M.; Mincu, R.I.; Rassaf, T. Cardiovascular adverse events in patients with cancer treated with bevacizumab: A meta-analysis of more than 20,000 patients. J. Am. Heart Assoc. 2017, 6, e006278. [Google Scholar] [CrossRef] [PubMed]
- Tasat, D.R.; Yakisich, J.S. Rationale for the use of sphingosine analogues in COVID-19 patients. Clin. Med. 2021, 21, e84–e87. [Google Scholar] [CrossRef] [PubMed]
- Schmidt-Tanguy, A.; Voswinkel, J.; Henrion, D.; Subra, J.F.; Loufrani, L.; Rohmer, V.; Ifrah, N.; Belizna, C. Antithrombotic effects of hydroxychloroquine in primary antiphospholipid syndrome patients. J. Thromb. Haemost. 2013, 11, 1927–1929. [Google Scholar] [CrossRef] [PubMed]
- Prescribing Information. Brilinta (Ticagrelor); AstraZeneca LP: Wilmington, DE, USA, 2011. [Google Scholar]
- Product Monograph. Brilinta (Ticagrelor); AstraZeneca Canada: Mississauga, ON, Canada, 2011. [Google Scholar]
- Itkonen, M.K.; Tornio, A.; Lapatto-Reiniluoto, O.; Neuvonen, M.; Neuvonen, P.J.; Niemi, M.; Backman, J.T. Clopidogrel Increases Dasabuvir Exposure With or Without Ritonavir, and Ritonavir Inhibits the Bioactivation of Clopidogrel. Clin. Pharm. Ther. 2019, 105, 219–228. [Google Scholar] [CrossRef]
- Marsousi, N.; Daali, Y.; Fontana, P.; Reny, J.-L.; Ancrenaz-Sirot, V.; Calmy, A.; Rudaz, S.; Desmeules, J.A.; Samer, C.F. Impact of Boosted Antiretroviral Therapy on the Pharmacokinetics and Efficacy of Clopidogrel and Prasugrel Active Metabolites. Clin. Pharmacokinet. 2018, 57, 1347–1354. [Google Scholar] [CrossRef] [PubMed]
- Cao, B.; Wang, Y.; Wen, D.; Liu, W.; Wang, J.; Fan, G.; Ruan, L.; Song, B.; Cai, Y.; Wei, M.; et al. A Trial of Lopinavir–Ritonavir in Adults Hospitalized with Severe Covid-19. N. Engl. J. Med. 2020, 382, 1787–1799. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Wang, X.; Yang, P.; Zhang, S. COVID-19 Complicated by Acute Pulmonary Embolism. Radiol. Cardiothorac. Imaging 2020, 2, e200067. [Google Scholar] [CrossRef] [PubMed]
- Danzi, G.B.; Loffi, M.; Galeazzi, G.; Gherbesi, E. Acute pulmonary embolism and COVID-19 pneumonia: A random association? Eur. Hear. J. 2020, 41, 1858. [Google Scholar] [CrossRef]
- Cui, S.; Chen, S.; Li, X.; Liu, S.; Wang, F. Prevalence of venous thromboembolism in patients with severe novel coronavirus pneumonia. J. Thromb. Haemost. 2020, 18, 1421–1424. [Google Scholar] [CrossRef] [PubMed]
- Klok, F.A.; Kruip, M.J.; Van der Meer, N.J.; Arbous, M.S.; Gommers, D.A.; Kant, K.M.; Kaptein, F.H.; van Paassen, J.; Stals, M.A.; Huisman, M.V.; et al. Incidence of thrombotic complications in critically ill ICU patients with COVID-19. Thromb. Res. 2020, 191, 145–1457. [Google Scholar] [CrossRef]
- Vedantham, S.; Goldhaber, S.Z.; Julian, J.A.; Kahn, S.R.; Jaff, M.R.; Cohen, D.J.; Magnuson, E.; Razavi, M.K.; Comerota, A.J.; Gornik, H.L.; et al. ATTRACT Trial Investigators. Pharmacomechanical catheter-directed thrombolysis for deep-vein throm-bosis. N. Engl. J. Med. 2017, 377, 2240–2252. [Google Scholar] [CrossRef]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. ESC Scientific Document Group. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef]
- Chodakowski, J.D.; Courtney, D.M. Pulmonary embolism critical care update: Prognosis, treatment, and research gaps. Curr. Opin. Crit. Care 2018, 24, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Barnes, G.D.; Kabrhel, C.; Courtney, D.M.; Naydenov, S.; Wood, T.; Rosovsky, R.; Rosenfield, K.; Giri, J.; National PERT Consortium Research Committee. Diversity in the pulmonary embolism response team model: An organizational survey of the National PERT Consortium Members. Chest 2016, 150, 1414–1417. [Google Scholar] [CrossRef]
- Rosovsky, R.; Zhao, K.; Sista, A.; Rivera-Lebron, B.; Kabrhel, C. Pulmonary embolism response teams: Purpose, evidence for efficacy, and future research directions. Res. Pr. Thromb. Haemost. 2019, 3, 315–330. [Google Scholar] [CrossRef]
- Bikdeli, B.; Chatterjee, S.; Desai, N.R.; Kirtane, A.J.; Desai, M.M.; Bracken, M.B.; Spencer, F.A.; Monreal, M.; Goldhaber, S.Z.; Krumholz, H.M. Inferior vena cava filters to prevent pulmonary embolism: Systematic review and meta-analysis. J. Am. Coll. Cardiol. 2017, 70, 1587–1597. [Google Scholar] [CrossRef] [PubMed]
- Kearon, C.; Akl, E.A.; Ornelas, J.; Blaivas, A.; Jimenez, D.; Bounameaux, H.; Huisman, M.; King, C.S.; Morris, T.A.; Sood, N.; et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest 2016, 149, 315–352. [Google Scholar] [CrossRef]
- Piazza, G. Advanced Management of Intermediate- and High-Risk Pulmonary Embolism: JACC Focus Seminar. J. Am. Coll. Cardiol. 2020, 76, 2117–2127. [Google Scholar] [CrossRef]
- Giri, J.; Sista, A.K.; Weinberg, I.; Kearon, C.; Kumbhani, D.J.; Desai, N.D.; Piazza, G.; Gladwin, M.T.; Chatterjee, S.; Kobayashi, T.; et al. Interventional Therapies for Acute Pulmonary Embolism: Current Status and Principles for the Development of Novel Evidence: A Scientific Statement From the American Heart Association. Circulation 2019, 140, e774–e801. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, D.; Bikdeli, B.; Marshall, P.S.; Tapson, V. Aggressive Treatment of Intermediate-Risk Patients with Acute Symptomatic Pulmonary Embolism. Clin. Chest Med. 2018, 39, 569–581. [Google Scholar] [CrossRef] [PubMed]
- Pellegrini, J.A.S.; Rech, T.H.; Schwarz, P.; de Oliveira, A.C.T.; Vieceli, T.; Moraes, R.B.; Sekine, L.; Viana, M.V. Incidence of venous thromboembolism among patients with severe COVID-19 requiring mechanical ventilation compared to other causes of respiratory failure: A prospective cohort study. J. Thromb. Thrombolysis 2021, 1–11. [Google Scholar] [CrossRef]
- Moll, M.; Zon, R.L.; Sylvester, K.W.; Chen, E.C.; Cheng, V.; Connell, N.T.; Fredenburgh, L.E.; Baron, R.M.; Cho, M.H.; Woolley, A.E.; et al. VTE in ICU Patients With COVID-19. Chest 2020, 158, 2130–2135. [Google Scholar] [CrossRef]
- Di Minno, A.; Ambrosino, P.; Calcaterra, I.; Di Minno, M.N.D. COVID-19 and Venous Thromboembolism: A Meta-analysis of Literature Studies. Semin. Thromb. Hemost. 2020, 46, 763–771. [Google Scholar] [CrossRef]
- Mansfield, A.; Tafur, A.; Vulih, D.; Smith, G.; Harris, P.; Ivy, S. Severe hepatic dysfunction is associated with venous thromboembolic events in phase 1 clinical trials. Thromb. Res. 2015, 136, 1169–1173. [Google Scholar] [CrossRef] [PubMed]
- Smith, B.S.; Yogaratnam, D.; Levasseur-Franklin, K.E.; Forni, A.; Fong, J. Introduction to Drug Pharmacokinetics in the Critically III Patient. Chest 2012, 141, 1327–1336. [Google Scholar] [CrossRef]
- Aryal, M.R.; Gosain, R.; Donato, A.; Pathak, R.; Bhatt, V.R.; Katel, A.; Kouides, P. Venous Thromboembolism in COVID-19: Towards an Ideal Approach to Thrombo-prophylaxis, Screening, and Treatment. Curr. Cardiol. Rep. 2020, 22, 52. [Google Scholar] [CrossRef] [PubMed]
- Sklar, M.C.; Sy, E.; Lequier, L.; Fan, E.; Kanji, H.D. Anticoagulation practices during venovenous extracorporeal membrane oxy-genation for respiratory failure. A systematic review. Ann. Am. Thorac. Soc. 2016, 13, 2242–2250. [Google Scholar] [CrossRef]
- Extracorporeal Life Support Organization. ELSO Guidelines for Cardiopulmonary Extracorporeal Life Support. v1.4. 2017. Available online: https://onlinelibrary.wiley.com/doi/full/10.1111/jth.12155 (accessed on 1 April 2020).
- Dobesh, P.P.; Trujillo, T.C. Coagulopathy, Venous Thromboembolism, and Anticoagulation in Patients with COVID-19. Pharmacother. J. Hum. Pharmacol. Drug Ther. 2020, 40, 1130–1151. [Google Scholar] [CrossRef] [PubMed]
- Schunemann, H.J.; Cushman, M.; Burnett, A.E.; Kahn, S.R.; Beyer-Westendorf, J.; Spencer, F.A.; Rezende, S.M.; Zakai, N.A.; Bauer, K.A.; Dentali, F.; et al. American Society of Hematology 2018 guidelines for management of ve-nous thromboembolism: Prophylaxis for hospitalized and nonhospitalized medical patients. Blood Adv. 2018, 2, 3198–3225. [Google Scholar] [CrossRef] [PubMed]
- Lopes, R.D.; de Barros ESilva, P.G.M.; Furtado, R.H.M.; Macedo, A.V.S.; Ramacciotti, E.; Damini, L.P.; Bronhara, B.; Cavalcanti, A.B.; Rosa, R.G.; Azevedo, L.C.P.; et al. Randomized Clinical Trial to Evaluate a Routine Full Anticoagulation Strategy in Patients with Coronavirus Infection (SARS-CoV2) Admitted to Hospital: Rationale and Design of the ACTION (AntiCoagulaTlon cOroNavirus)-Coalition IV Trial. Am. Heart J. 2021. [Google Scholar] [CrossRef]
- National Institute for Health and Clinical Excellence. NICE Clinical Guideline 92: Venous Thromboembolism: Reducing the Risk. Available online: http://www.1000livesplus.wales.nhs.uk/sitesplus/documents/1011/CG92NICEGuidelinePDF.pdf (accessed on 30 March 2020).
- Lenchus, J.D.; Biehl, M.; Cabrera, J.; De Moraes, A.G.; Dezfulian, C. In-Hospital Management and Follow-Up Treatment of Venous Thromboembolism: Focus on New and Emerging Treatments. J. Intensiv. Care Med. 2017, 32, 299–311. [Google Scholar] [CrossRef] [PubMed]
- Encke, A.; Haas, S.; Kopp, I. The Prophylaxis of Venous Thromboembolism. Dtsch. Aerzteblatt Online 2016, 113, 532–538. [Google Scholar] [CrossRef]
- Spyropoulos, A.C.; Levy, J.H.; Ageno, W.; Connors, J.M.; Hunt, B.J.; Iba, T.; Levi, M.; Samama, C.M.; Thachil, J.; Giannis, D.; et al. Scientific and Stand-ardization Committee communication: Clinical guidance on the diagnosis, prevention, and treatment of venous throm-boembolism in hospitalized patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1859–1865. [Google Scholar] [CrossRef] [PubMed]
- Albertsen, I.E.; Nielsen, P.B. Searching for High-Risk Venous Thromboembolism Patients Using Risk Scores: Adding to the Heap or Closing a Gap? Thromb. Haemost. 2018, 118, 1686–1687. [Google Scholar] [CrossRef]
- Zhou, H.; Hu, Y.; Li, X.; Wang, L.; Wang, M.; Xiao, J.; Yi, Q. Assessment of the Risk of Venous Thromboembolism in Medical Inpatients using the Padua Prediction Score and Caprini Risk Assessment Model. J. Atheroscler. Thromb. 2018, 25, 1091–1104. [Google Scholar] [CrossRef]
- Stuck, A.; Spirk, D.; Schaudt, J.; Kucher, N. Risk Assessment Models for Venous Thromboembolism in Acutely Ill Medical Patients: A Systematic Review. Thromb. Haemost. 2017, 5, 769–770. [Google Scholar] [CrossRef]
- Liu, X.; Liu, C.; Chen, X.; Wu, W.; Lu, G. Comparison between Caprini and Padua risk assessment models for hospitalized medi-cal patients at risk for venous thromboembolism: A retrospective study. Interact. Cardiovasc. Thorac. Surg. 2016, 23, 538–543. [Google Scholar] [CrossRef]
- Moumneh, T.; Riou, J.; Douillet, D.; Henni, S.; Mottier, D.; Tritschler, T.; Le Gal, G.; Roy, P. Validation of risk assessment models predicting venous thromboembolism in acutely ill medical inpatients: A cohort study. J. Thromb. Haemost. 2020, 18, 1398–1407. [Google Scholar] [CrossRef]
- Mlaver, E.; Lynde, G.C.; Gallion, C.; Sweeney, J.F.; Sharma, J. Development of a Novel Preoperative Venous Thromboembolism Risk Assessment Model. Am. Surg. 2020, 86. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.; Chen, R.; Liu, C.; Liang, W.; Guan, W.; Tang, R.; Tang, C.; Zhang, N.; Zhong, N.; Li, S. Attention should be paid to venous thromboembolism prophylaxis in the management of COVID-19. Lancet Haematol. 2020, 7, e362–e363. [Google Scholar] [CrossRef]
- Hunt, B.J. Hemostasis at Extremes of Body Weight. Semin. Thromb. Hemost. 2018, 44, 632–639. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Clinical Management of Severe Acute Respiratory Infection When Novel Coronavirus (2019-nCoV) Infection Is Suspected. INTERIM Guidance 28 January 2020. Available online: https://www.who.int/docs/defaultsource/coronaviruse/clinical-management-ofnovel-cov.pdf (accessed on 7 April 2020).
- Liew, N.C.; Alemany, G.V.; Angchaisuksiri, P.; Bang, S.M.; Choi, G.; De Silva, D.; Hong, J.M.; Lee, L.; Li, Y.J.; Rajamoney, G.N.; et al. Asian venous thromboembolism guidelines: Updated recommendations for the prevention of venous thromboembolism. Int. Angiol. 2016, 36, 1–20. [Google Scholar] [PubMed]
- Popoola, V.O.; Tavakoli, F.; Lau, B.D.; Lankiewicz, M.; Ross, P.; Kraus, P.; Shaffer, D.; Hobson, D.B.; Aboagye, J.K.; Farrow, N.A.; et al. Exploring the impact of route of administration on medication acceptance in hospi-talized patients: Implications for venous thromboembolism prevention. Thromb. Res. 2017, 160, 109–113. [Google Scholar] [CrossRef]
- Bates, S.M.; Rajasekhar, A.; Middeldorp, S.; McLintock, C.; Rodger, M.A.; James, A.H.; Vazquez, S.R.; Greer, I.A.; Riva, J.J.; Bhatt, M.; et al. American Society of Hematology 2018 guidelines for management of venous thromboembolism: Venous thromboembolism in the context of pregnancy. Blood Adv. 2018, 2, 3317–3359. [Google Scholar] [CrossRef]
- Royal College of Obstetricians and Gynaecologists. Reducing the Risk of Venous Thromboembolism during Pregnancy and the Puerperium. Green-Top Guideline No. 37a. 2015. Available online: https://www.rcog.org.uk/globalassets/documents/guide-lines/gtg%5f37a.pdf (accessed on 1 April 2020).
- Rybstein, M.D.; DeSancho, M.T. Risk factors for and clinical management of venous thromboembolism during pregnancy. Clin. Adv. Hematol. Oncol. 2019, 17, 396–404. [Google Scholar]
- Akel, T.; Qaqa, F.; Abuarqoub, A.; Shamoon, F. Pulmonary embolism: A complication of COVID 19 infection. Thromb. Res. 2020, 193, 79–82. [Google Scholar] [CrossRef]
- Cohen, A.T.; Harrington, R.A.; Goldhaber, S.Z.; Hull, R.D.; Wiens, B.L.; Gold, A.; Hernandez, A.F.; Gibson, C.M.; APEX Investigators. Extended thromboprophylaxis with betrixaban in acutely ill medical pa-tients. N. Engl. J. Med. 2016, 375, 534–544. [Google Scholar] [CrossRef] [PubMed]
- Arigondam, A.K.; Hakeem, A.R.; Reddy, M.S.; Rela, M. An Evidence-based Protocol for Minimizing Thromboembolic Events in SARS-CoV-2 Infection. Arch. Med. Res. 2021, 52, 252–260. [Google Scholar] [CrossRef] [PubMed]
- Spyropoulos, A.C.; Ageno, W.; Albers, G.W.; Elliott, C.G.; Halperin, J.L.; Hiatt, W.R.; Maynard, G.A.; Steg, P.G.; Weitz, J.I.; Suh, E.; et al. Rivaroxaban for thromboprophylaxis after hospitalization for medical ill-ness. N. Engl. J. Med. 2018, 379, 1118–1127. [Google Scholar] [CrossRef] [PubMed]
- Spyropoulos, A.C.; Lipardi, C.; Xu, J.; Peluso, C.; Spiro, T.E.; De Sanctis, Y.; Barnathan, E.S.; Raskob, G.E. Modified IMPROVE VTE Risk Score and Elevated D-Dimer Identify a High Venous Thromboembolism Risk in Acutely Ill Medical Population for Extended Thromboprophylaxis. TH Open 2020, 4, e59–e65. [Google Scholar] [CrossRef] [PubMed]
- Dentali, F.; Mumoli, N.; Prisco, D.; Fontanella, A.; Di Minno, M.N. Efficacy and safety of extended thromboprophylaxis for medi-cally ill patients. A meta-analysis of randomised controlled trials. Thromb. Haemost. 2017, 117, 606–617. [Google Scholar] [CrossRef] [PubMed]
- Schindewolf, M.; Weitz, J.I. Broadening the Categories of Patients Eligible for Extended Venous Thromboembolism Treatment. Thromb. Haemost. 2019, 120, 14–26. [Google Scholar] [CrossRef] [PubMed]
- Spyropoulos, A.C.; Lipardi, C.; Xu, J.; Lu, W.; Suh, E.; Yuan, Z.; Levitan, B.; Sugarmann, C.; De Sanctis, Y.; Spiro, T.E.; et al. Improved Benefit Risk Profile of Rivaroxaban in a Subpopulation of the MAGELLAN Study. Clin. Appl. Thromb. Hemost. 2019, 25. [Google Scholar] [CrossRef]
- Chi, G.; Goldhaber, S.Z.; Kittelson, J.M.; Turpie, A.G.G.; Hernandez, A.F.; Hull, R.D.; Gold, A.; Curnutte, J.T.; Cohen, A.T.; Harrington, R.A.; et al. Effect of extended-duration thromboprophylaxis on venous thromboembolism and major bleeding among acutely ill hospitalized medical patients: A bivariate analysis. J. Thromb. Haemost. 2017, 15, 1913–1922. [Google Scholar] [CrossRef]
- Zhang, A.; Leng, Y.; Zhang, Y.; Wu, K.; Ji, Y.; Lei, S.; Xia, Z. Meta-analysis of coagulation parameters associated with disease severity and poor prognosis of COVID-19. Int. J. Infect. Dis. 2020, 100, 441–448. [Google Scholar] [CrossRef]
- Iba, T.; Levy, J.H.; Levi, M.; Thachil, J. Coagulopathy in COVID-19. J. Thromb. Haemost. 2020, 18, 2103–2109. [Google Scholar] [CrossRef]
- Gando, S.; Shiraishi, A.; Yamakawa, K.; Ogura, H.; Saitoh, D.; Fujishima, S.; Mayumi, T.; Kushimoto, S.; Abe, T.; Shiino, Y.; et al. Japanese Association for Acute Medicine (JAAM) Focused Outcomes Research in Emergency Care in Acute Respiratory Distress Syndrome, Sepsis and Trauma (FORECAST) Study Group. Role of disseminated intravascular coagulation in severe sepsis. Thromb Res. 2019, 178, 182–188. [Google Scholar]
- Jackson Chornenki, N.L.; Dwivedi, D.J.; Kwong, A.C.; Zamir, N.; Fox-Robichaud, A.E.; Liaw, P.C.; Canadian Critical Care Translational Biology Group. Canadian Critical Care Translational Biology Group. Identification of hemostatic markers that define the pre-DIC state: A multi-center observational study. J. Thromb. Haemost. 2020, 18, 2524–2531. [Google Scholar] [CrossRef]
- Tang, N.; Bai, H.; Chen, X.; Gong, J.; Li, D.; Sun, Z. Anticoagulant treatment is associated with decreased mortality in severe coro-navirus disease 2019 patients with coagulopathy. J. Thromb. Haemost. 2020. [Google Scholar] [CrossRef]
- Wada, H.; Thachil, J.; Di Nisio, M.; Mathew, P.; Kurosawa, S.; Gando, S.; Kim, H.K.; Nielsen, J.D.; Dempfle, C.E.; Levi, M.; et al. Guidance for diagnosis and treatment of DIC from harmonization of the recommenda-tions from 3 guidelines. J. Thromb. Haemost. 2013. [Google Scholar] [CrossRef] [PubMed]
- Varga, Z.; Flammer, A.J.; Steiger, P.; Haberecker, M.; Andermatt, R.; Zinkernagel, A.S.; Mehra, M.R.; Schuepbach, R.A.; Ruschitzka, F.; Moch, H. Endothelial cell infection and endotheliitis in COVID-19. Lancet 2020, 395, 1417–1418. [Google Scholar] [CrossRef]
- Perico, L.; Benigni, A.; Casiraghi, F.; Ng, L.F.P.; Renia, L.; Remuzzi, G. Immunity, endothelial injury and complement-induced coagulopathy in COVID-19. Nat. Rev. Nephrol. 2021, 17, 46–64. [Google Scholar] [CrossRef] [PubMed]
- Monteil, V.; Kwon, H.; Prado, P.; Hagelkrüys, A.; Wimmer, R.A.; Stahl, M.; Leopoldi, A.; Garreta, E.; Del Pozo, C.H.; Prosper, F.; et al. Inhibition of SARS-CoV-2 Infections in engineered human tissues using clinical-grade soluble human ACE2. Cell 2020, 181, 905–913.e7. [Google Scholar] [CrossRef]
- Mehta, P.; McAuley, D.F.; Brown, M.; Sanchez, E.; Tattersall, R.S.; Manson, J.J. COVID-19: Consider cytokine storm syndromes and immunosuppression. Lancet 2020, 395, 1033–1034. [Google Scholar] [CrossRef]
- Jackson, B.S.; Pretorius, E. Pathological Clotting and Deep Vein Thrombosis in Patients with HIV. Semin. Thromb. Hemost. 2019, 45, 132–140. [Google Scholar] [CrossRef] [PubMed]
- Ramacciotti, E.; Agati, L.B.; Aguiar, V.C.R.; Wolosker, N.; Guerra, J.C.; De Almeida, R.P.; Alves, J.C.; Lopes, R.D.; Wakefield, T.W.; Comerota, A.J.; et al. Zika and Chikungunya Virus and Risk for Venous Thromboembolism. Clin. Appl. Thromb. 2019, 25. [Google Scholar] [CrossRef]
- Smither, S.J.; O’Brien, L.M.; Eastaugh, L.; Woolley, T.; Lever, S.; Fletcher, T.; Parmar, K.; Hunt, B.J.; Watts, S.; Kirkman, E. Haemostatic Changes in Five Patients Infected with Ebola Virus. Viruses 2019, 11, 647. [Google Scholar] [CrossRef] [PubMed]
- Karakike, E.; Giamarellos-Bourboulis, E.J. Macrophage Activation-Like Syndrome: A Distinct Entity Leading to Early Death in Sepsis. Front. Immunol. 2019, 10, 55. [Google Scholar] [CrossRef] [PubMed]
- McGonagle, D.; Sharif, K.; O’Regan, A.; Bridgewood, C. The Role of Cytokines including Interleukin-6 in COVID-19 induced Pneumonia and Macrophage Activation Syndrome-Like Disease. Autoimmun. Rev. 2020, 19, 102537. [Google Scholar] [CrossRef]
- Webb, B.J.; Peltan, I.D.; Jensen, P.; Hoda, D.; Hunter, B.; Silver, A.; Starr, N.; Buckel, W.; Grisel, N.; Hummel, E.; et al. Clinical criteria for COVID-19-associated hyperinflammatory syndrome: A co-hort study. Lancet Rheumatol. 2020, 2, e754–e763. [Google Scholar] [CrossRef]
- Peng, Z.; Shu, B.; Zhang, Y.; Wang, M. Endothelial Response to Pathophysiological Stress. Arter. Thromb. Vasc. Biol. 2019, 39, e233–e243. [Google Scholar] [CrossRef] [PubMed]
- Gimbrone, M.A., Jr.; Garcia-Cardena, G. Endothelial cell dysfunction and the pathobiology of atherosclerosis. Circ Res. 2016, 118, 620–636. [Google Scholar] [CrossRef] [PubMed]
- Milenkovic, J.; Milojkovic, M.; Stoimenov, T.J.; Djindjic, B.; Miljkovic, E. Mechanisms of plasminogen activator inhibitor 1 action in stromal remodeling and related diseases. Biomed. Pap. Med. Fac. Palacky Univ. Olomouc 2017, 161, 339–347. [Google Scholar] [CrossRef]
- Poels, K.; van Leent, M.M.; Reiche, M.E.; Kusters, P.J.; Huveneers, S.; de Winther, M.P.; Mulder, W.J.; Lutgens, E.; Seijkens, T.T. Antibody-Mediated Inhibition of CTLA4 Aggravates Atherosclerotic Plaque In-flammation and Progression in Hyperlipidemic Mice. Cells 2020, 9, 1987. [Google Scholar] [CrossRef] [PubMed]
- Matsumoto, T.; Sasaki, N.; Yamashita, T.; Emoto, T.; Kasahara, K.; Mizoguchi, T.; Hayashi, T.; Yodoi, K.; Kitano, N.; Saito, T.; et al. Overexpression of Cytotoxic T-Lymphocyte-Associated Antigen-4 Prevents Ath-erosclerosis in Mice. Arter. Thromb. Vasc. Biol. 2016, 36, 1141–1151. [Google Scholar] [CrossRef] [PubMed]
- Foks, A.; Kuiper, J. Immune checkpoint proteins: Exploring their therapeutic potential to regulate atherosclerosis. Br. J. Pharmacol. 2017, 174, 3940–3955. [Google Scholar] [CrossRef] [PubMed]
- Zuo, Y.; Warnock, M.; Harbaugh, A.; Yalavarthi, S.; Gockman, K.; Zuo, M.; Madison, J.A.; Knight, J.S.; Kanthi, Y.; Lawrence, D.A. Plasma tissue plasminogen activator and plasminogen activator inhibitor-1 in hospitalized COVID-19 patients. Sci. Rep. 2021, 11, 1–9. [Google Scholar] [CrossRef]
- Engin, A. Endothelial Dysfunction in Obesity. Adv. Exp. Med. Biol. 2017, 960, 345–379. [Google Scholar] [CrossRef]
- Yang, J.; Hu, J.; Zhu, C. Obesity aggravates COVID-19: A systematic review and meta-analysis. J. Med. Virol. 2020, 93, 257–261. [Google Scholar] [CrossRef] [PubMed]
- Hariyanto, T.I.; Kurniawan, A. Dyslipidemia is associated with severe coronavirus disease 2019 (COVID-19) infection. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 1463–1465. [Google Scholar] [CrossRef] [PubMed]
- Picard, F.; Adjedj, J.; Varenne, O. Diabetes Mellitus, a prothrombotic disease. Ann. Cardiol. D’angeiologie 2017, 66, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Bryk, A.H.; Satała, D.; Natorska, J.; Rąpała-Kozik, M.; Undas, A. Interaction of glycated and acetylated human α2-antiplasmin with fibrin clots. Blood Coagul. Fibrinolysis 2020, 31, 393–396. [Google Scholar] [CrossRef]
- Yazıcı, D.; Sezer, H. Insulin Resistance, Obesity and Lipotoxicity. Adv. Exp. Med. Biol. 2017, 960, 277–304. [Google Scholar] [CrossRef] [PubMed]
- Cooper, I.D.; Crofts, C.A.P.; DiNicolantonio, J.J.; Malhotra, A.; Elliott, B.; Kyriakidou, Y.; Brookler, K.H. Relationships between hyperinsulinaemia, magnesium, vitamin D, thrombosis and COVID-19: Rationale for clinical management. Open Hear. 2020, 7, e001356. [Google Scholar] [CrossRef] [PubMed]
- Hansen, M.E.; Tippetts, T.S.; Anderson, M.C.; Holub, Z.E.; Moulton, E.R.; Swensen, A.C.; Prince, J.T.; Bikman, B.T. Insulin Increases Ceramide Synthesis in Skeletal Muscle. J. Diabetes Res. 2014, 2014, 1–9. [Google Scholar] [CrossRef]
- Dias, I.H.; Ferreira, R.; Gruber, F.; Vitorino, R.; Rivas-Urbina, A.; Sanchez-Quesada, J.L.; Silva, J.V.; Fardilha, M.; de Freitas, V.; Reis, A. Sulfate-based lipids: Analysis of healthy human fluids and cell extracts. Chem. Phys. Lipids 2019, 221, 53–64. [Google Scholar] [CrossRef] [PubMed]
- Janssen, R.; Visser, M.P.J.; Dofferhoff, A.S.M.; Vermeer, C.; Janssens, W.; Walk, J. Vitamin K metabolism as the potential missing link between lung damage and thromboembolism in Coronavirus disease 2019. Br. J. Nutr. 2020, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Iba, T.; Levy, J.H. Sepsis-induced Coagulopathy and Disseminated Intravascular Coagulation. Anesthesiology 2020, 132, 1238–1245. [Google Scholar] [CrossRef] [PubMed]
- Hayden, M.R. Endothelial activation and dysfunction in metabolic syndrome, type 2 diabetes and coronavirus disease 2019. J. Int. Med. Res. 2020, 48. [Google Scholar] [CrossRef]
- Hotta, Y.; Kataoka, T.; Kimura, K. Testosterone Deficiency and Endothelial Dysfunction: Nitric Oxide, Asymmetric Dimethylarginine, and Endothelial Progenitor Cells. Sex. Med. Rev. 2019, 7, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Giagulli, V.A.; Guastamacchia, E.; Magrone, T.; Jirillo, E.; Lisco, G.; De Pergola, G.; Triggiani, V. Worse progression of COVID-19 in men: Is testosterone a key factor? Andrology 2021, 9, 53–64. [Google Scholar] [CrossRef]
- Zhang, Y.; Xiao, M.; Zhang, S.; Xia, P.; Cao, W.; Jiang, W.; Chen, H.; Ding, X.; Zhao, H.; Zhang, H.; et al. Coagulopathy and Antiphospholipid Antibodies in Patients with Covid-19. N. Engl. J. Med. 2020, 382, e38. [Google Scholar] [CrossRef]
- Greinacher, A.; Thiele, T.; Warkentin, T.E.; Weisser, K.; Kyrle, P.A.; Eichinger, S. Thrombotic Thrombocytopenia after ChAdOx1 nCov-19 Vaccination. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef]
- Schultz, N.H.; Sørvoll, I.H.; Michelsen, A.E.; Munthe, L.A.; Lund-Johansen, F.; Ahlen, M.T.; Wiedmann, M.; Aamodt, A.H.; Skattør, T.H.; Tjønnfjord, G.E.; et al. Thrombosis and Thrombocytopenia after ChAdOx1 nCoV-19 Vaccination. N. Engl. J. Med. 2021. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. Covid-19: WHO says rollout of AstraZeneca vaccine should continue, as Europe divides over safety. BMJ 2021, 372, n728. [Google Scholar] [CrossRef] [PubMed]
- Mahase, E. Covid-19: AstraZeneca vaccine is not linked to increased risk of blood clots, finds European Medicine Agency. BMJ 2021, 372, n774. [Google Scholar] [CrossRef] [PubMed]
- European Medicines Agency. COVID-19 Vaccine AstraZeneca: Benefits Still Outweigh the Risks Despite Possible Link to Rare Blood Clots with Low Blood Platelets. Available online: https://www.ema.europa.eu/en/news/covid-19-vac-cine-astrazeneca-benefits-still-outweigh-risks-despite-possible-linkrare-blood-clots (accessed on 18 March 2021).
- European Medicines Agency. Covid-19 Vaccine AstraZeneca: PRAC Investigating Cases of Thromboembolic Events—Vaccine’s Benefits Currently Still Outweigh Risks: Update. Mar. 2021. Available online: https://www.ema.europa.eu/en/news/covid-19-vaccine-astrazeneca-prac-investigating-casesthromboembolic-events-vaccines-benefits (accessed on 19 April 2021).
- WHO’s Advisory Committee on Vaccine Safety. Available online: https://www.who.int/news/item/19-03-2021-statement-of-the-who-global-advisory-committee-on-vaccine-safety-(gacvs)-covid-19-subcommittee-on-safety-signals-related-to-the-astrazeneca-covid-19-vaccine (accessed on 20 April 2021).
- AstraZeneca’s COVID-19 Vaccine: EMA Finds Possible Link to Very Rare Cases of Unusual Blood Clots with Low Blood Platelets Share. Available online: https://www.ema.europa.eu/en/news/astrazenecas-covid-19-vaccine-ema-finds-possible-link-very-rare-cases-unusual-blood-clots-low-blood (accessed on 20 April 2021).
- Polack, F.P.; Thomas, S.J.; Kitchin, N.; Absalon, J.; Gurtman, A.; Lockhart, S.; Perez, J.L.; Marc, G.P.; Moreira, E.D.; Zerbini, C.; et al. Safety and Efficacy of the BNT162b2 mRNA Covid-19 Vaccine. N. Engl. J. Med. 2020, 383, 2603–2615. [Google Scholar] [CrossRef]
- Baden, L.R.; El Sahly, H.M.; Essink, B.; Kotloff, K.; Frey, S.; Novak, R.; Diemert, D.; Spector, S.A.; Rouphael, N.; Creech, C.B.; et al. COVE Study Group. Efficacy and Safety of the mRNA-1273 SARS-CoV-2 Vaccine. N. Engl. J. Med. 2021, 384, 403–416. [Google Scholar] [CrossRef] [PubMed]
- Voysey, M.; Clemens, S.A.C.; Madhi, S.A.; Weckx, L.Y.; Folegatti, P.M.; Aley, P.K.; Angus, B.; Baillie, V.L.; Barnabas, S.L.; Bhorat, Q.E.; et al. Oxford COVID Vaccine Trial Group. Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: An interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 2021, 397, 99–111. [Google Scholar] [CrossRef]
- Ramasamy, M.N.; Minassian, A.M.; Ewer, K.J.; Flaxman, A.L.; Folegatti, P.M.; Owens, D.R.; Voysey, M.; Aley, P.K.; Angus, B.; Babbage, G.; et al. Oxford COVID Vaccine Trial Group. Safety and immunogenicity of ChA-dOx1 nCoV-19 vaccine administered in a prime-boost regimen in young and old adults (COV002): A single-blind, random-ised, controlled, phase 2/3 trial. Lancet 2021, 396, 1979–1993. [Google Scholar] [CrossRef]
- Sadoff, J.; Le Gars, M.; Shukarev, G.; Heerwegh, D.; Truyers, C.; de Groot, A.M.; Stoop, J.; Tete, S.; Van Damme, W.; Leroux-Roels, I.; et al. Interim Results of a Phase 1–2a Trial of Ad26.COV2.S Covid-19 Vaccine. N. Engl. J. Med. 2021, 384, 1824–1835. [Google Scholar] [CrossRef]
- Logunov, D.Y.; Dolzhikova, I.V.; Shcheblyakov, D.V.; Tukhvatulin, A.; Zubkova, O.V.; Dzharullaeva, A.S.; Kovyrshina, A.V.; Lubenets, N.L.; Grousova, D.M.; Erokhova, A.S.; et al. Safety and efficacy of an rAd26 and rAd5 vector-based heterologous prime-boost COVID-19 vaccine: An interim analysis of a randomised controlled phase 3 trial in Russia. Lancet 2021, 397, 671–681. [Google Scholar] [CrossRef]
- VID-19: Latest Updates Share. The Latest Updates on the COVID-19 Pandemic from the European Medicines Agency. Available online: https://www.ema.europa.eu/en/human-regulatory/overview/public-health-threats/coronavirus-disease-covid-19/covid-19-latest-updates (accessed on 15 April 2021).
- WHO Coronavirus (COVID-19) Dashboard. Geneva: World Health Organization. Available online: https://covid19.who.int/ (accessed on 5 April 2021).
- European Centre for Disease Prevention and Control COVID-19 Vaccine Tracker. Available online: https://qap.ecdc.europa.eu/public/extensions/COVID-19/vaccine-tracker.html#uptake-tab (accessed on 15 April 2021).
- van Doremalen, N.; Lambe, T.; Spencer, A.; Belij-Rammerstorfer, S.; Purushotham, J.N.; Port, J.R.; Avanzato, V.A.; Bushmaker, T.; Flaxman, A.; Ulaszewska, M.; et al. ChAdOx1 nCoV-19 vaccine prevents SARS-CoV-2 pneumonia in rhesus ma-caques. Nature 2020, 586, 578–582. [Google Scholar] [CrossRef]
- Zhang, Y.; Zeng, G.; Pan, H.; Li, C.; Hu, Y.; Chu, K.; Han, W.; Chen, Z.; Tang, R.; Yin, W.; et al. Safety, tolerability, and immunogenicity of an inactivated SARS-CoV-2 vaccine in healthy adults aged 18–59 years: A randomised, double-blind, placebo-controlled, phase 1/2 clinical trial. Lancet Infect. Dis. 2021, 21, 181–192. [Google Scholar] [CrossRef]
- Vasileiou, E.; Simpson, C.R.; Robertson, C.; Shi, T.; Kerr, S.; Agrawal, U.; Akbari, A.; Bedston, S.; Beggs, J.; Bradley, D.; et al. Effectiveness of First Dose of COVID-19 Vaccines Against Hospital Admissions in Scotland: National Prospective Cohort Study of 5.4 Million People. Lancet 2021. [Google Scholar] [CrossRef]
- López-Medina, E.; López, P.; Hurtado, I.C.; Dávalos, D.M.; Ramirez, O.; Martínez, E.; Díazgranados, J.A.; Oñate, J.M.; Chavarriaga, H.; Herrera, S.; et al. Effect of Ivermectin on Time to Resolution of Symptoms Among Adults With Mild COVID-19: A Randomized Clinical Trial. JAMA 2021, 325, 1426–1435. [Google Scholar] [CrossRef] [PubMed]
- Bikdeli, B. Effect of Intermediate-Dose vs. Standard-Dose Prophylactic Anticoagulation on Thrombotic Events, Extracorporeal Membrane Oxygenation Treatment, or Mortality Among Patients With COVID-19 Admitted to the Intensive Care Unit The INSPIRATION Randomized Clinical Trial. JAMA 2021, 325, 1620–1630. [Google Scholar]
- COVIDSurg Collaborative; GlobalSurg Collaborative. Timing of surgery following SARS-CoV-2 infection: An international prospective cohort study. Anaesthesia 2021, 76, 748–758. [Google Scholar] [CrossRef]
- Nappi, F.; Avatar Singh, S.S.; Santana, O.; Mihos, C.G. Functional mitral regurgitation: An overview for surgical management framework. J. Thorac. Dis. 2018, 10, 4540–4555. [Google Scholar] [CrossRef] [PubMed]
- Nappi, F.; Spadaccio, C.; Chello, M.; Acar, C. The Ross procedure: Underuse or under-comprehension? J. Thorac. Cardiovasc. Surg. 2015, 149, 1463–1464. [Google Scholar] [CrossRef][Green Version]
- COVIDSurg Collaborative; GlobalSurg Collaborative. SARS-CoV-2 vaccination modelling for safe surgery to save lives: Data from an international prospective cohort study. Br. J. Surg. 2021. [Google Scholar] [CrossRef]
- Rubin, R. COVID-19 Vaccines vs. Variants—Determining How Much Immunity Is Enough. JAMA 2021, 325, 1241. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Reference | Total SARS-CoV-2 + Hospitalized Patients | VTE and ATE Cases | Risk Factors More Present in Cases (p < 0.05) | Risk Factors Similar in Cases and Controls (p > 0.05) | Conclusions |
|---|---|---|---|---|---|
| Stoneham et al., 2020 [26] | 208 | 21 | High Wbcs, high D-dimer, high INR. | aPTT ratio, fibrinogen. | Comorbidities were not associated with a higher risk of thrombosis. Monitoring of D-dimer and anti-factor Xa levels may be relevant for management. |
| Zuo et al., 2020 [27] | 44 | 11 | High calprotectin, markers of NETs (myeloperoxidase-DNA complexes) high D-dimer, high platelets. | Troponins, Wbcs. | There was a significant difference between peak D-dimer, calprotectin and cell free DNA levels between the populations. |
| Zhang et al., 2020 [28] | 143 | 66 | High Wbcs, older age, low oxygenation index, high rate of cardiac injury, CURB-65 score 3 to 5, Padua score ≥ 4, high D-dimer. | Platelets count. | COVID-19 is suspected to cause an additional risk factor for DVT in hospitalized patients. |
| Planquette et al., 2020 [29] | 1042 | 59 | High CRP, fibrinogen, D-dimer. IMV. | Comorbidities: BMI, previous VTE, ATE, Cancer, hypertension, Cardiovascular diseases. | Similar prevalence of VTE risk factors in cases and controls was found. In both groups, altered coagulation parameters were found. |
| Trimaille et al., 2020 [30] | 289 | 49 | High Improve score, high WBCs, D-dimer, low haemoglobin at discharge. | Padua score of 4 or more, CRP | Lack of thromboprophylaxis is a major determinant of VTE in non-ICU COVID-19 patients. Comorbidities were not found to affect the event occurrence. |
| Shah et al., 2020 [31] | 187 | 81 | High troponins, ferritin, D-dimer. | Platelets count, Wbcs, thromboelastography parameters. | Elevated D-dimer, ferritin, troponin and white cell count at ICU admission may reflect undiagnosed altered coagulation and be used to identify patients for CTPA. |
| Kolielat et al., 2021 [32] | 117 | 18 | High D-dimer, fibrinogen, ferritin. | Wbcs, platelets, troponins, Il-6. | Elevated D-dimer and a less elevated fibrinogen are associated with DVT despite conventional thromboprophylactic treatment. |
| Kampouri et al., 2020 [33] | 443 | 41 | High D-dimer, positive Wells criteria, bilateral infiltrates on X-rays or CT scan, mechanical ventilation. | Wbcs, platelets, CRP, Padua score, Geneva score. | The combination of Wells ≥ 2 score and D—dimer ≥ 3000 ng/L is predictive of VTE at admission. Hospitalization in the ICU and especially mechanical ventilation were associated with VTE occurrence. The combination of Wells’ score and D-dimer value can be used for guiding empiric anticoagulation therapy. |
| Published Study | Vaccine Type | Patient (N) | Women (N) | Age | Time Span | Cases’ Etiology | Major Findings |
|---|---|---|---|---|---|---|---|
| Greinacher et al. [137] | ChAdOx1 nCov-19 | 11 | 9 | 36 yrs (median) | 5 to 16 days after 1st dose | 10 multiple thrombosis, 9 cerebral venous thrombosis. 3 splanchnic-vein thrombosis. 3 pulmonary embolisms, and 4 others. 5 disseminated intravascular coagulation | Immune thrombotic thrombocytopenia. High level of Platelet-activating antibodies against PF4 mimicking autoimmune heparin-induced thrombocytopenia. |
| Schultz et al. [138] | ChAdOx1 nCov-19 | 5 | 4/5 | 40.8 ys (mean) | 7 to 10 days after | 2 thromboses (sigmoid cerebral sinuses), 1 thrombosis (portal vein branches) 1 massive thrombosis plus right cerebellar hemorrhagic infarction 1 massive cerebral vein thrombosis with global edema. | High levels of antibodies to platelet factor (PF) 4-polyanion complexes. Authors propose the acronym VITT (vaccine-induced immune thrombotic thrombocytopenia) as causative mechanism. |
| Vaccine Type | Thrombosis Cases | Total Administrations | Associated Factors |
|---|---|---|---|
| ChAdOx1 nCov-19 | 169 CVST, 53 splanchnic vein thrombosis | 34 million people had been vaccinated in the EEA and UK | <60 years of age, symptoms onset within 3 weeks after vaccination, female gender, thrombocytopenia. |
| JNJ-78436735/Ad26. COV2. S | 6 CVST (1 death) | 8.09 million in US | Thrombocytopenia, women between 18 and 48 ys. symptoms onset between 6 to 13 days after vaccination |
| Published Study | Vaccine Type | Participant (n) | Women (n) | Age | Vaccine Components | Adverse Events | Efficacy |
|---|---|---|---|---|---|---|---|
| Voysey et al. (interim analysis of COV001, COV002, COV004, COV005) [147] | ChAdOx1 nCoV-19 | 11,636 5807-va 5829-ca | 3525/5807 | mostly 18–55 yrs | dsDNA encoding for the Spike protein protected in an adenoviral particle | 175 severe adverse events | 2 standard doses efficacy was 62.1%. Low boosted dose efficacy was 90.0%. |
| Ramasamy et al. (phase 2 of COV002) [148] | ChAdOx1 nCoV-19 | 560 420-va 140-ca | 104 low-d 101 standard-d | 100 (18–55 yrs) 120 (56–69 yrs) 200 > 70 yrs | dsDNA encoding for the Spike protein protected in an adenovirus. | Systemic reactions 86% (18–55 yrs) 77% (56–69 yrs) 65% >70 yrs | 14 days after the 2nd dose, 208 of 209 boosted participants had neutralising antibody responses. T-cell responses peaked at day 14 after a single dose. |
| Logunov et al. (phase 3) [150] | rAd26 and rAd5 vector-based vaccine (Sputnik V) | 21.977 | 5821 (38.9%) | mostly 18–60 yrs | dsDNA encoding for the Spike protein protected in Ad26 vector for the 1st dose, Ad5 for the 2nd one). | 4 deaths, none was related to the vaccine. | Vaccine efficacy was 91.6% (95% CI 85.6–95.2). |
| Zhang et al. (phase 1/2) [155] | CoronaVac (Sinovac Life Sciences, Beijing, China) | 743 | 397/743 | phase 1 42.6 yrs phase 2 42.1 yrs | Inactivated virus vaccine with beta-propiolactone | In the phase 2 trial adverse reactions was 19% with 3 μg 19% with 6 μg group, and 18% with placebo. | In the phase 2.97% seroconversion with 3 μg, 100% with 6 μg group, and 0% with placebo group. |
| Sadoff et al. (interim analysis of phase 1–2) [149] | Ad26.COV2. S/JNJ-78436735 (Johnson&Johnson) | 805 | 169 in cohort 1, 159 in cohort 3 | 35.4 ± 10.2 (cohort 1) 69.8 ± 4.0 (cohort 3) | dsDNA encoding for the Spike protein protected in an adenoviral particle (Ad26) | The most frequent systemic adverse event was fever. Systemic adverse events were less common in cohort 3 than in cohort 1. | Reactogenicity was lower after the second dose. Neutralizing-antibody titers were detected in 90% or more of all participants on day 29 after the first vaccine dose |
| Polack et al. [145] | BNT162b2 mRNA | 43.548 | 9221 (48.9) | 52.0 | mRNA vaccine encoding for Spike protein protected in a lipid nanoparticle | Serious adverse events incidence was low and similar between the vaccine and placebo groups. | BNT162b2 95% effective in preventing the disease. Similar efficacy for age, sex, race, ethnicity, baseline body-mass index, and the presence of coexisting conditions. |
| Baden et al. [146] | mRNA-1273 vaccine (Moderna) | 30.351 | 7108 (46.9) | 51.3 (18–95) | encapsulated mRNA vaccine encoding for Spike protein protected in a lipid nanoparticle | Transient local systemic reactions. No safety concerns were identified. | mRNA-1273 94.1% effective in preventing severe and mild disease development. |
| - | Adenoviral Vector | mRNA | ||||
|---|---|---|---|---|---|---|
| Country | ChAdOx1 nCov-19 (Astrazeneca) | Sputnik V/Gam-Covid-Vac | CoronaVac (SinoVac) | JNJ-78436735/Ad26.COV2.S (Johnson&Johnson) | BNT162b2 mRNA (Pfizer) | mRNA-1273 (Moderna) |
| France | 3.72 million | 0 | 0 | 2004 | 14.33 million | 1.59 million |
| Germany | 5.60 million | 0 | 0 | 0 | 18.81 million | 1.47 million |
| Italy | 3.97 million | 0 | 0 | 20700 | 12.83 million | 1.27 million |
| United States | 0 | 0 | 0 | 8.09 million | 116.19 million | 100.83 million |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nappi, F.; Iervolino, A.; Avtaar Singh, S.S. Thromboembolic Complications of SARS-CoV-2 and Metabolic Derangements: Suggestions from Clinical Practice Evidence to Causative Agents. Metabolites 2021, 11, 341. https://doi.org/10.3390/metabo11060341
Nappi F, Iervolino A, Avtaar Singh SS. Thromboembolic Complications of SARS-CoV-2 and Metabolic Derangements: Suggestions from Clinical Practice Evidence to Causative Agents. Metabolites. 2021; 11(6):341. https://doi.org/10.3390/metabo11060341
Chicago/Turabian StyleNappi, Francesco, Adelaide Iervolino, and Sanjeet Singh Avtaar Singh. 2021. "Thromboembolic Complications of SARS-CoV-2 and Metabolic Derangements: Suggestions from Clinical Practice Evidence to Causative Agents" Metabolites 11, no. 6: 341. https://doi.org/10.3390/metabo11060341
APA StyleNappi, F., Iervolino, A., & Avtaar Singh, S. S. (2021). Thromboembolic Complications of SARS-CoV-2 and Metabolic Derangements: Suggestions from Clinical Practice Evidence to Causative Agents. Metabolites, 11(6), 341. https://doi.org/10.3390/metabo11060341