
Urinary Metabolome Analyses of Patients with Acute Kidney Injury Using Capillary Electrophoresis-Mass Spectrometry

 ,
,  , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Results
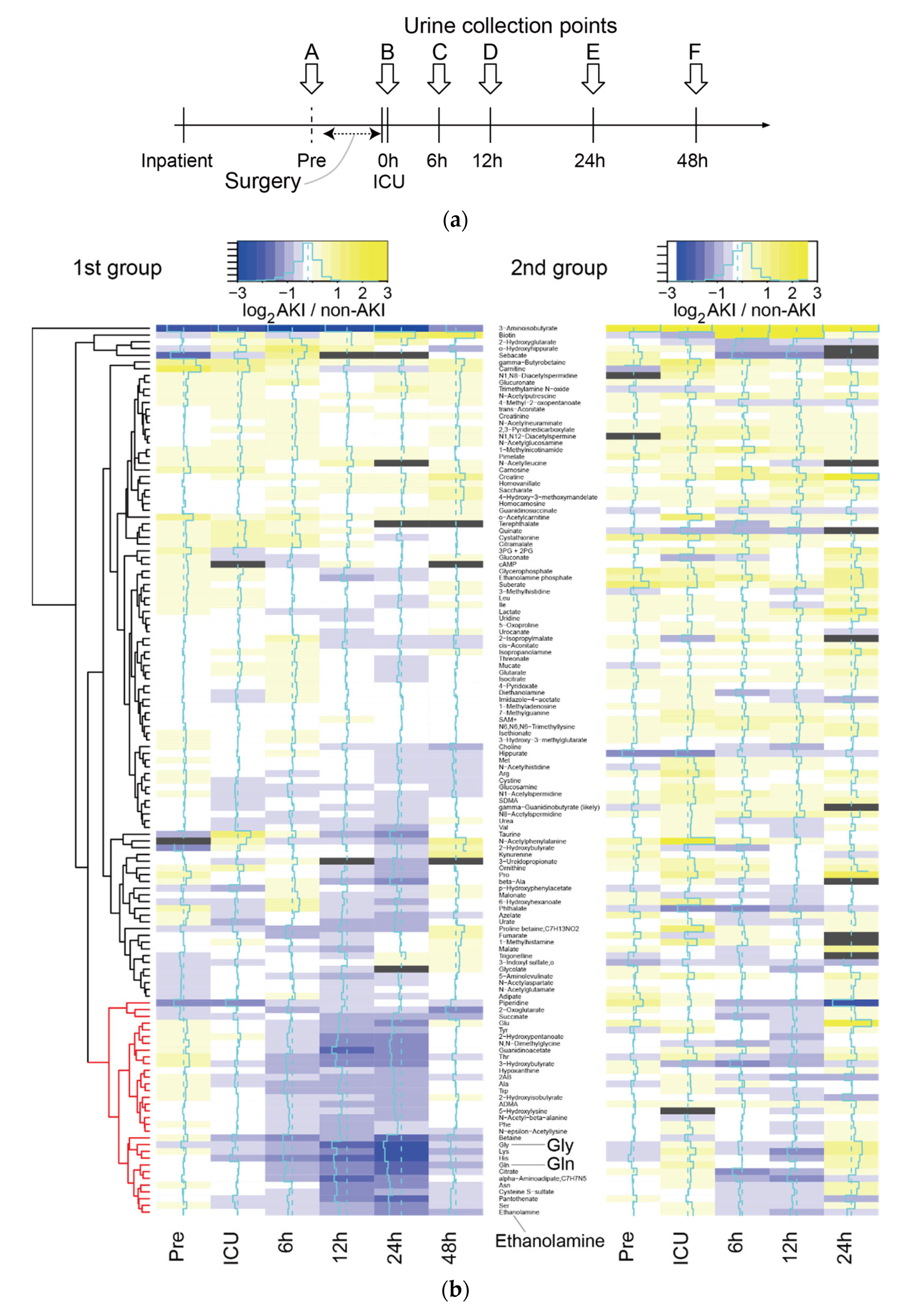
2.1. Comprehensive Differential Analysis of Metabolites among AKI and Non-AKI Subjects
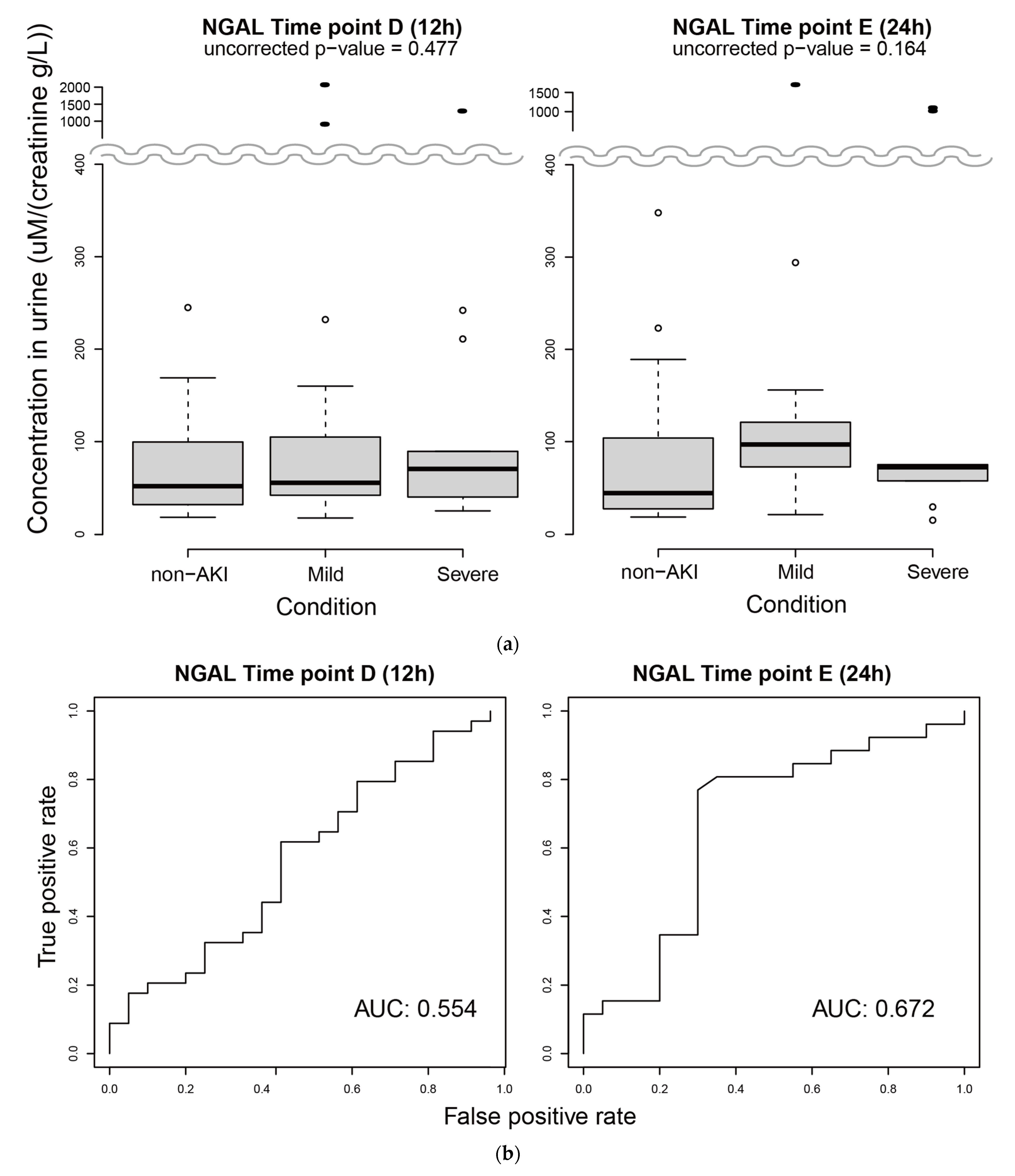
2.2. Measurement of uNGAL
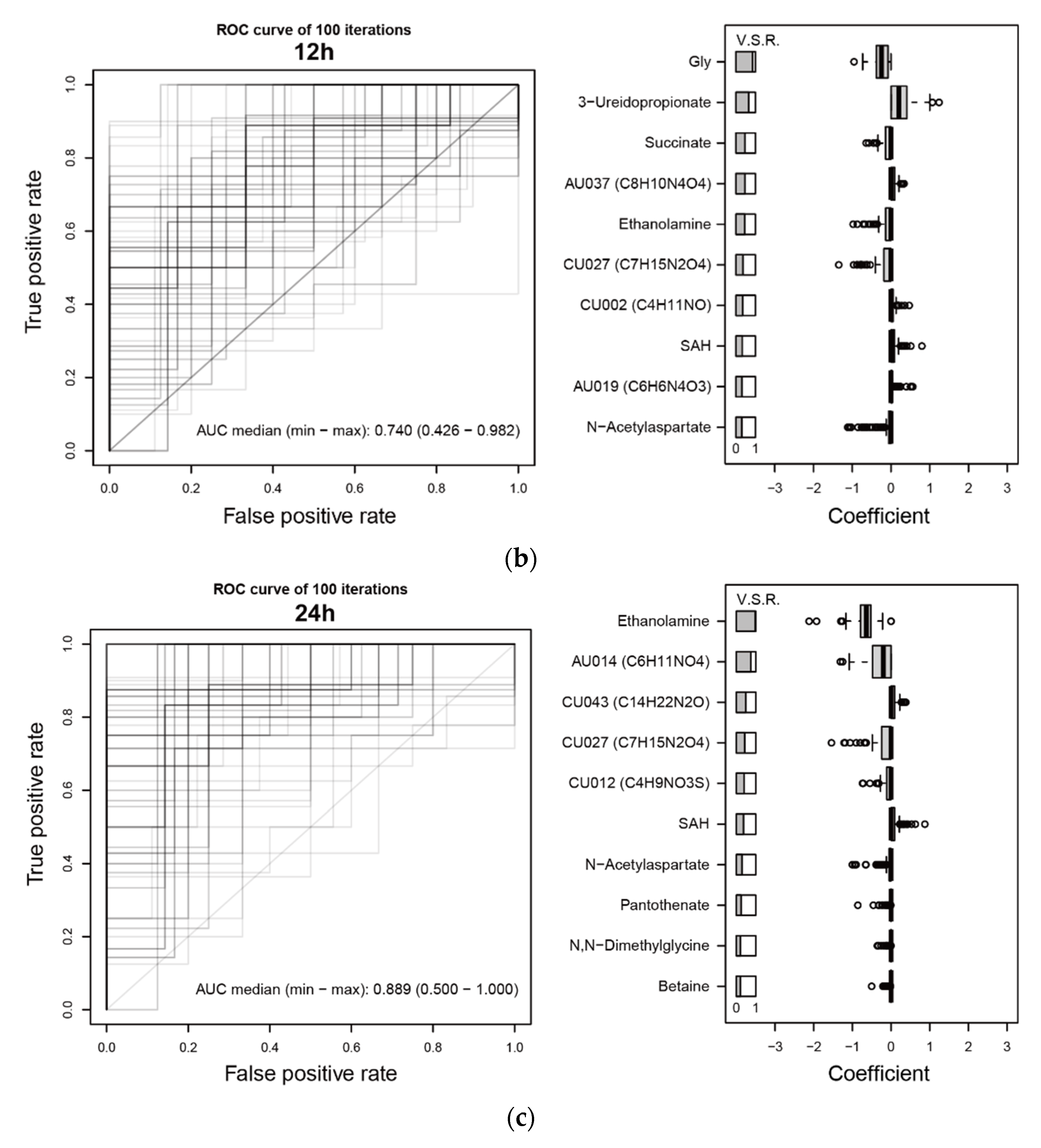
2.3. Prediction of AKI Based on Metabolome Profiles and Clinical Variables Using LASSO
3. Discussion
4. Materials and Methods
4.1. Collection of Medical Information and Specimens from Patients
4.2. Urine Creatinine (Cr) Measurements by an Enzyme Method
4.3. Preprocessing of Urine Samples
4.4. Chemicals
4.5. Instruments and Analytical Conditions
4.6. Data Processing of CE-MS
= (metabolite level × dilution factor)/(Cr × 10/113.118)
4.7. Urinary NGAL Measurement
4.8. Statistical Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Khwaja, A. KDIGO clinical practice guidelines for acute kidney injury. Nephron. Clin. Pract. 2012, 120, c179–c184. [Google Scholar] [CrossRef]
- Bolignano, D.; Donato, V.; Coppolino, G.; Campo, S.; Buemi, A.; Lacquaniti, A.; Buemi, M. Neutrophil gelatinase-associated lipocalin (NGAL) as a marker of kidney damage. Am. J. Kidney Dis. 2008, 52, 595–605. [Google Scholar] [CrossRef]
- Oh, D.J. A long journey for acute kidney injury biomarkers. Ren Fail. 2020, 42, 154–165. [Google Scholar] [CrossRef]
- Husi, H.; Sanchez-Nino, M.D.; Delles, C.; Mullen, W.; Vlahou, A.; Ortiz, A.; Mischak, H. A combinatorial approach of Proteomics and Systems Biology in unravelling the mechanisms of acute kidney injury (AKI): Involvement of NMDA receptor GRIN1 in murine AKI. BMC Syst. Biol. 2013, 7, 110. [Google Scholar] [CrossRef] [Green Version]
- Malagrino, P.A.; Venturini, G.; Yogi, P.S.; Dariolli, R.; Padilha, K.; Kiers, B.; Gois, T.C.; Cardozo, K.H.; Carvalho, V.M.; Salgueiro, J.S.; et al. Proteome analysis of acute kidney injury-Discovery of new predominantly renal candidates for biomarker of kidney disease. J. Proteomics. 2017, 151, 66–73. [Google Scholar] [CrossRef]
- Metzger, J.; Kirsch, T.; Schiffer, E.; Ulger, P.; Mentes, E.; Brand, K.; Weissinger, E.M.; Haubitz, M.; Mischak, H.; Herget-Rosenthal, S. Urinary excretion of twenty peptides forms an early and accurate diagnostic pattern of acute kidney injury. Kidney Int. 2010, 78, 1252–1262. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Metzger, J.; Mullen, W.; Husi, H.; Stalmach, A.; Herget-Rosenthal, S.; Groesdonk, H.V.; Mischak, H.; Klingele, M. Acute kidney injury prediction in cardiac surgery patients by a urinary peptide pattern: A case-control validation study. Crit. Care 2016, 20, 157. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Izquierdo-Garcia, J.L.; Nin, N.; Cardinal-Fernandez, P.; Rojas, Y.; de Paula, M.; Granados, R.; Martinez-Caro, L.; Ruiz-Cabello, J.; Lorente, J.A. Identification of novel metabolomic biomarkers in an experimental model of septic acute kidney injury. Am. J. Physiol. Renal Physiol. 2019, 316, F54–F62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jouret, F.; Leenders, J.; Poma, L.; Defraigne, J.O.; Krzesinski, J.M.; de Tullio, P. Nuclear Magnetic Resonance Metabolomic Profiling of Mouse Kidney, Urine and Serum Following Renal Ischemia/Reperfusion Injury. PLoS ONE 2016, 11, e0163021. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zacharias, H.U.; Schley, G.; Hochrein, J.; Klein, M.S.; Köberle, C.; Eckardt, K.-U.; Willam, C.; Oefner, P.J.; Gronwald, W. Analysis of human urine reveals metabolic changes related to the development of acute kidney injury following cardiac surgery. Metabolomics 2013, 9, 697–707. [Google Scholar] [CrossRef]
- Elmariah, S.; Farrell, L.A.; Daher, M.; Shi, X.; Keyes, M.J.; Cain, C.H.; Pomerantsev, E.; Vlahakes, G.J.; Inglessis, I.; Passeri, J.J.; et al. Metabolite Profiles Predict Acute Kidney Injury and Mortality in Patients Undergoing Transcatheter Aortic Valve Replacement. J. Am. Heart Assoc. 2016, 5, e002712. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Li, H.-H.; Pan, J.-L.; Hui, S.; Ma, X.-W.; Wang, Z.-L.; Yao, H.-X.; Wang, J.-F.; Li, H. Retracted Article: High-throughput metabolomics identifies serum metabolic signatures in acute kidney injury using LC-MS combined with pattern recognition approach. RSC Adv. 2018, 8, 14838–14847. [Google Scholar] [CrossRef] [Green Version]
- Sun, J.; Shannon, M.; Ando, Y.; Schnackenberg, L.K.; Khan, N.A.; Portilla, D.; Beger, R.D. Serum metabolomic profiles from patients with acute kidney injury: A pilot study. J. Chromatogr. B Analyt. Technol. Biomed. Life Sci. 2012, 893–894, 107–113. [Google Scholar] [CrossRef] [Green Version]
- Wei, Q.; Xiao, X.; Fogle, P.; Dong, Z. Changes in metabolic profiles during acute kidney injury and recovery following ischemia/reperfusion. PLoS ONE 2014, 9, e106647. [Google Scholar] [CrossRef] [Green Version]
- Martin-Lorenzo, M.; Gonzalez-Calero, L.; Ramos-Barron, A.; Sanchez-Nino, M.D.; Gomez-Alamillo, C.; Garcia-Segura, J.M.; Ortiz, A.; Arias, M.; Vivanco, F.; Alvarez-Llamas, G. Urine metabolomics insight into acute kidney injury point to oxidative stress disruptions in energy generation and H2S availability. J. Mol. Med. 2017, 95, 1399–1409. [Google Scholar] [CrossRef]
- Won, A.J.; Kim, S.; Kim, Y.G.; Kim, K.B.; Choi, W.S.; Kacew, S.; Kim, K.S.; Jung, J.H.; Lee, B.M.; Kim, S.; et al. Discovery of urinary metabolomic biomarkers for early detection of acute kidney injury. Mol. Biosyst. 2016, 12, 133–144. [Google Scholar] [CrossRef]
- Coca, S.G.; Yalavarthy, R.; Concato, J.; Parikh, C.R. Biomarkers for the diagnosis and risk stratification of acute kidney injury: A systematic review. Kidney Int. 2008, 73, 1008–1016. [Google Scholar] [CrossRef] [Green Version]
- Soga, T.; Ueno, Y.; Naraoka, H.; Ohashi, Y.; Tomita, M.; Nishioka, T. Simultaneous determination of anionic intermediates for Bacillus subtilis metabolic pathways by capillary electrophoresis electrospray ionization mass spectrometry. Anal. Chem. 2002, 74, 2233–2239. [Google Scholar] [CrossRef] [PubMed]
- Ta, H.Y.; Collin, F.; Perquis, L.; Poinsot, V.; Ong-Meang, V.; Couderc, F. Twenty years of amino acid determination using capillary electrophoresis: A review. Anal. Chim. Acta 2021, 1174, 338233. [Google Scholar] [CrossRef] [PubMed]
- Soga, T.; Baran, R.; Suematsu, M.; Ueno, Y.; Ikeda, S.; Sakurakawa, T.; Kakazu, Y.; Ishikawa, T.; Robert, M.; Nishioka, T.; et al. Differential metabolomics reveals ophthalmic acid as an oxidative stress biomarker indicating hepatic glutathione consumption. J. Biol. Chem. 2006, 281, 16768–16776. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Satoh, K.; Yachida, S.; Sugimoto, M.; Oshima, M.; Nakagawa, T.; Akamoto, S.; Tabata, S.; Saitoh, K.; Kato, K.; Sato, S.; et al. Global metabolic reprogramming of colorectal cancer occurs at adenoma stage and is induced by MYC. Proc. Natl. Acad. Sci. USA 2017, 114, E7697–E7706. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hirayama, A.; Nakashima, E.; Sugimoto, M.; Akiyama, S.; Sato, W.; Maruyama, S.; Matsuo, S.; Tomita, M.; Yuzawa, Y.; Soga, T. Metabolic profiling reveals new serum biomarkers for differentiating diabetic nephropathy. Anal. Bioanal. Chem. 2012, 404, 3101–3109. [Google Scholar] [CrossRef] [PubMed]
- Kawamura, N.; Shinoda, K.; Sato, H.; Sasaki, K.; Suzuki, M.; Yamaki, K.; Fujimori, T.; Yamamoto, H.; Osei-Hyiaman, D.; Ohashi, Y. Plasma metabolome analysis of patients with major depressive disorder. Psychiatry Clin. Neurosci. 2018, 72, 349–361. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beck, F.X.; Ohno, A.; Dorge, A.; Thurau, K. Ischemia-induced changes in cell element composition and osmolyte contents of outer medulla. Kidney Int. 1995, 48, 449–457. [Google Scholar] [CrossRef] [Green Version]
- Hu, Y.M.; Pai, M.H.; Yeh, C.L.; Hou, Y.C.; Yeh, S.L. Glutamine administration ameliorates sepsis-induced kidney injury by downregulating the high-mobility group box protein-1-mediated pathway in mice. Am. J. Physiol. Renal Physiol. 2012, 302, F150–F158. [Google Scholar] [CrossRef] [Green Version]
- Yin, M.; Zhong, Z.; Connor, H.D.; Bunzendahl, H.; Finn, W.F.; Rusyn, I.; Li, X.; Raleigh, J.A.; Mason, R.P.; Thurman, R.G. Protective effect of glycine on renal injury induced by ischemia-reperfusion in vivo. Am. J. Physiol. Renal. Physiol. 2002, 282, F417–F423. [Google Scholar] [CrossRef] [Green Version]
- Kokkoris, S.; Pipili, C.; Grapsa, E.; Kyprianou, T.; Nanas, S. Novel biomarkers of acute kidney injury in the general adult ICU: A review. Ren Fail. 2013, 35, 579–591. [Google Scholar] [CrossRef] [Green Version]
- Bennett, M.; Dent, C.L.; Ma, Q.; Dastrala, S.; Grenier, F.; Workman, R.; Syed, H.; Ali, S.; Barasch, J.; Devarajan, P. Urine NGAL predicts severity of acute kidney injury after cardiac surgery: A prospective study. Clin. J. Am. Soc. Nephrol. 2008, 3, 665–673. [Google Scholar] [CrossRef] [Green Version]
- Nisula, S.; Yang, R.; Kaukonen, K.M.; Vaara, S.T.; Kuitunen, A.; Tenhunen, J.; Pettila, V.; Korhonen, A.M.; Group, F.S. The urine protein NGAL predicts renal replacement therapy, but not acute kidney injury or 90-day mortality in critically ill adult patients. Anesth. Analg. 2014, 119, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Endre, Z.H.; Pickering, J.W.; Walker, R.J.; Devarajan, P.; Edelstein, C.L.; Bonventre, J.V.; Frampton, C.M.; Bennett, M.R.; Ma, Q.; Sabbisetti, V.S.; et al. Improved performance of urinary biomarkers of acute kidney injury in the critically ill by stratification for injury duration and baseline renal function. Kidney Int. 2011, 79, 1119–1130. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ho, J.; Tangri, N.; Komenda, P.; Kaushal, A.; Sood, M.; Brar, R.; Gill, K.; Walker, S.; MacDonald, K.; Hiebert, B.M.; et al. Urinary, Plasma, and Serum Biomarkers’ Utility for Predicting Acute Kidney Injury Associated With Cardiac Surgery in Adults: A Meta-analysis. Am. J. Kidney Dis. 2015, 66, 993–1005. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lameire, N.H.; Vanholder, R.C.; Van Biesen, W.A. How to use biomarkers efficiently in acute kidney injury. Kidney Int. 2011, 79, 1047–1050. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z. Machine learning method for the management of acute kidney injury: More than just treating biomarkers individually. Biomark Med. 2019, 13, 1251–1253. [Google Scholar] [CrossRef] [PubMed]
- Wilson, F.P. Machine Learning to Predict Acute Kidney Injury. Am. J. Kidney Dis. 2020, 75, 965–967. [Google Scholar] [CrossRef] [Green Version]
- Tomasev, N.; Glorot, X.; Rae, J.W.; Zielinski, M.; Askham, H.; Saraiva, A.; Mottram, A.; Meyer, C.; Ravuri, S.; Protsyuk, I.; et al. A clinically applicable approach to continuous prediction of future acute kidney injury. Nature 2019, 572, 116–119. [Google Scholar] [CrossRef]
- Saito, R.; Sugimoto, M.; Hirayama, A.; Soga, T.; Tomita, M.; Takebayashi, T. Quality Assessment of Untargeted Analytical Data in a Large-Scale Metabolomic Study. J. Clin. Med. 2021, 10, 1826. [Google Scholar] [CrossRef] [PubMed]
- Shinjo, H.; Sato, W.; Imai, E.; Kosugi, T.; Hayashi, H.; Nishimura, K.; Nishiwaki, K.; Yuzawa, Y.; Matsuo, S.; Maruyama, S. Comparison of kidney disease: Improving global outcomes and acute kidney injury network criteria for assessing patients in intensive care units. Clin. Exp. Nephrol. 2014, 18, 737–745. [Google Scholar] [CrossRef]
- Soga, T.; Igarashi, K.; Ito, C.; Mizobuchi, K.; Zimmermann, H.P.; Tomita, M. Metabolomic profiling of anionic metabolites by capillary electrophoresis mass spectrometry. Anal. Chem. 2009, 81, 6165–6174. [Google Scholar] [CrossRef] [Green Version]
- Hirayama, A.; Kami, K.; Sugimoto, M.; Sugawara, M.; Toki, N.; Onozuka, H.; Kinoshita, T.; Saito, N.; Ochiai, A.; Tomita, M.; et al. Quantitative metabolome profiling of colon and stomach cancer microenvironment by capillary electrophoresis time-of-flight mass spectrometry. Cancer Res. 2009, 69, 4918–4925. [Google Scholar] [CrossRef] [Green Version]
- Sugimoto, M.; Wong, D.T.; Hirayama, A.; Soga, T.; Tomita, M. Capillary electrophoresis mass spectrometry-based saliva metabolomics identified oral, breast and pancreatic cancer-specific profiles. Metabolomics 2010, 6, 78–95. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Metabolite Name | Uncorrected p-Values | BH Corrected p-Values | BF Corrected p-Values |
|---|---|---|---|
| E_K: Ethanolamine | 5.04 × 10−6 | 0.00769 | 0.00769 |
| E_K: Gln | 6.88 × 10−5 | 0.0347 | 0.105 |
| D_K: Gly | 8.17 × 10−5 | 0.0347 | 0.125 |
| E_K: 2-Hydroxypentanoate | 0.000102 | 0.0347 | 0.155 |
| E_K: Gly | 0.000114 | 0.0347 | 0.173 |
| E_U: AU034 (C9H16N2O4) | 0.000178 | 0.0452 | 0.271 |
| D_K: Ethanolamine | 0.000239 | 0.0521 | 0.365 |
| E_U: AU014 (C6H11NO4) | 0.00041 | 0.0603 | 0.624 |
| E_K: Ser | 0.000431 | 0.0603 | 0.656 |
| D_K: Succinate | 0.000473 | 0.0603 | 0.721 |
| Metabolite Name | Uncorrected p-Values | BH Corrected p-Values | BF Corrected p-Values |
|---|---|---|---|
| Gly | 8.68 × 10−5 | 0.0181 | 0.0302 |
| NCGC003 | 0.000118 | 0.0181 | 0.0410 |
| NCGA012 | 0.000189 | 0.0181 | 0.0657 |
| Urea | 0.000256 | 0.0181 | 0.0889 |
| Urate | 0.000318 | 0.0181 | 0.111 |
| NCGA025 | 0.000327 | 0.0181 | 0.114 |
| Ethanolamine | 0.000364 | 0.0181 | 0.127 |
| NCGA003 | 0.000487 | 0.0212 | 0.170 |
| Gln | 0.000619 | 0.0222 | 0.216 |
| N,N-Dimethylglycine | 0.000697 | 0.0222 | 0.243 |
| Metabolite Name | Uncorrected p-Values | BH Corrected p-Values | BF Corrected p-Values |
|---|---|---|---|
| Piperidine | 2.54 × 10−6 | 0.000883 | 0.000883 |
| AU035 (C7H8O6S) | 1.04 × 10−5 | 0.00181 | 0.00363 |
| CU021 (C6H10N2O4) | 6.85 × 10−5 | 0.00794 | 0.0238 |
| CU001 (C4H9N) | 0.000110 | 0.00953 | 0.0381 |
| CU043 (C14H22N2O) | 0.000191 | 0.0133 | 0.0663 |
| NCGC008 | 0.000412 | 0.0239 | 0.143 |
| Taurine | 0.000635 | 0.0300 | 0.221 |
| Methanesulfonate | 0.000689 | 0.0300 | 0.240 |
| AU021 (C7H8O4S) | 0.00131 | 0.0507 | 0.456 |
| 3-Hydroxykynurenine | 0.00184 | 0.0583 | 0.639 |
| Characteristic | Non-AKI (n = 23) | Mild AKI (n = 24) | Severe AKI (n = 14) |
|---|---|---|---|
| Gender [Male (M), Female (F)] | M: 16 (70%) F: 7 (30%) | M: 19 (79%) F: 5 (21%) | M: 9 (64%) F: 5 (36%) |
| Age range (median) | 52–83 (68.0) | 47–84 (71.0) | 53–76 (67.0) |
| Department | |||
| Cardiology | 12 (52%) | 10 (41%) | 4 (28%) |
| Gastroenterology | 7 (30%) | 9 (37%) | 6 (42%) |
| Breast | 1 (4%) | 0 (0%) | 1 (7%) |
| Orthopedics | 1 (4%) | 1 (4%) | 0 (0%) |
| Respiratory Medicine | 2 (8%) | 1 (4%) | 0 (0%) |
| Transplantation | 0 (0%) | 0 (0%) | 1 (7%) |
| Vascular | 0 (0%) | 3 (12%) | 1 (7%) |
| Urology | 0 (0%) | 0 (0%) | 1 (7%) |
| Characteristic | Non-AKI (n = 40) | Mild AKI (n = 20) |
|---|---|---|
| Gender [Male (M), Female (F)] | M: 34 (85%) F: 6 (15%) | M: 19 (95%) F: 1 (5%) |
| Age range (median) | 40–83 (68.0) | 31–81 (72.5) |
| Department | ||
| Cardiology | 14 (35%) | 3 (15%) |
| Gastroenterology | 7 (17%) | 11 (55%) |
| Neurology | 6 (15%) | 1 (5%) |
| Orthopedics | 1 (2%) | 0 (0%) |
| Respiratory Medicine | 2 (5%) | 2 (10%) |
| Transplantation | 1 (2%) | 1 (5%) |
| Vascular | 4 (10%) | 2 (10%) |
| Oral | 2 (5%) | 0 (0%) |
| Otorhinolaryngology | 3 (7%) | 0 (0%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Saito, R.; Hirayama, A.; Akiba, A.; Kamei, Y.; Kato, Y.; Ikeda, S.; Kwan, B.; Pu, M.; Natarajan, L.; Shinjo, H.; et al. Urinary Metabolome Analyses of Patients with Acute Kidney Injury Using Capillary Electrophoresis-Mass Spectrometry. Metabolites 2021, 11, 671. https://doi.org/10.3390/metabo11100671
Saito R, Hirayama A, Akiba A, Kamei Y, Kato Y, Ikeda S, Kwan B, Pu M, Natarajan L, Shinjo H, et al. Urinary Metabolome Analyses of Patients with Acute Kidney Injury Using Capillary Electrophoresis-Mass Spectrometry. Metabolites. 2021; 11(10):671. https://doi.org/10.3390/metabo11100671
Chicago/Turabian StyleSaito, Rintaro, Akiyoshi Hirayama, Arisa Akiba, Yushi Kamei, Yuyu Kato, Satsuki Ikeda, Brian Kwan, Minya Pu, Loki Natarajan, Hibiki Shinjo, and et al. 2021. "Urinary Metabolome Analyses of Patients with Acute Kidney Injury Using Capillary Electrophoresis-Mass Spectrometry" Metabolites 11, no. 10: 671. https://doi.org/10.3390/metabo11100671
APA StyleSaito, R., Hirayama, A., Akiba, A., Kamei, Y., Kato, Y., Ikeda, S., Kwan, B., Pu, M., Natarajan, L., Shinjo, H., Akiyama, S., Tomita, M., Soga, T., & Maruyama, S. (2021). Urinary Metabolome Analyses of Patients with Acute Kidney Injury Using Capillary Electrophoresis-Mass Spectrometry. Metabolites, 11(10), 671. https://doi.org/10.3390/metabo11100671