Systemic Effects of Radiotherapy and Concurrent Chemo-Radiotherapy in Head and Neck Cancer Patients—Comparison of Serum Metabolome Profiles

 ,
,  , ,
, , 
Abstract
1. Introduction
2. Results
3. Discussion
4. Materials and Methods
4.1. Characteristics of the Patient Group
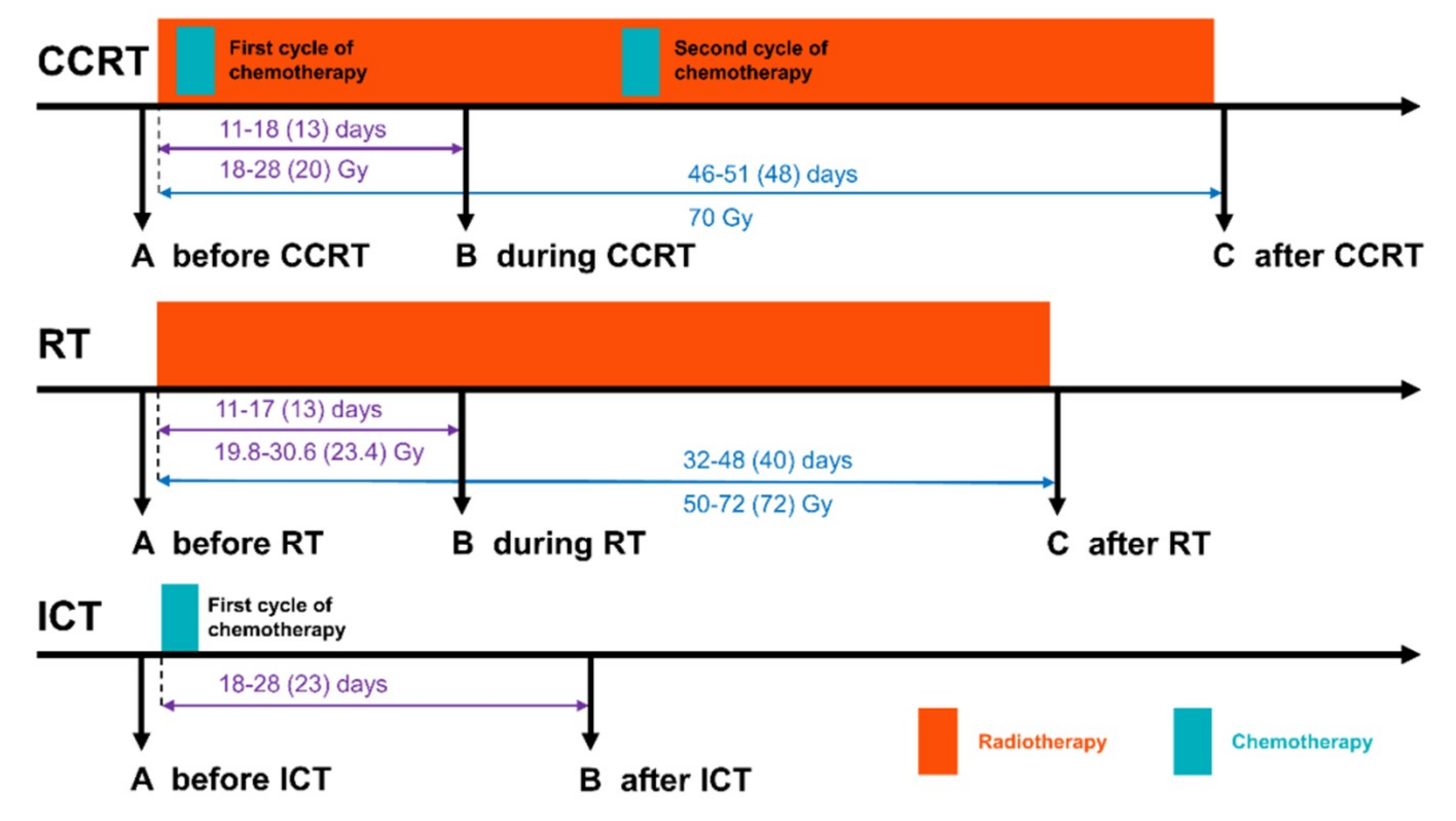
4.2. Material Collection
4.3. LC-MS Targeted Metabolomics
4.4. Analysis of Selected Amino Acids and Their Derivatives
4.5. Albumin and 3-Hydroxybutyrate Detection
4.6. Statistical and Bioinformatic Analyses
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Orth, M.; Lauber, K.; Niyazi, M.; Friedl, A.A.; Li, M.; Maihofer, C.; Schuttrumpf, L.; Ernst, A.; Niemoller, O.M.; Belka, C. Current concepts in clinical radiation oncology. Radiat. Environ. Biophys. 2014, 53, 1–29. [Google Scholar] [CrossRef] [PubMed]
- Marur, S.; Forastiere, A.A. Update on role of chemotherapy in head and neck squamous cell cancer. Indian J. Surg. Oncol. 2010, 1, 85–95. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Yeh, S.-A. Radiotherapy for head and neck cancer. Semin. Plast. Surg. 2010, 24, 127–136. [Google Scholar] [CrossRef] [PubMed]
- Nicholson, J.K.; Lindon, J.C. Systems biology: Metabonomics. Nature 2008, 455, 1054–1056. [Google Scholar] [CrossRef] [PubMed]
- Spratlin, J.L.; Serkova, N.J.; Eckhardt, S.G. Clinical applications of metabolomics in oncology: A review. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2009, 15, 431–440. [Google Scholar] [CrossRef]
- Laiakis, E.C.; Mak, T.D.; Anizan, S.; Amundson, S.A.; Barker, C.A.; Wolden, S.L.; Brenner, D.J.; Fornace, A.J., Jr. Development of a metabolomic radiation signature in urine from patients undergoing total body irradiation. Radiat. Res. 2014, 181, 350–361. [Google Scholar] [CrossRef]
- Patel, R.M.; Roback, J.D.; Uppal, K.; Yu, T.; Jones, D.P.; Josephson, C.D. Metabolomics profile comparisons of irradiated and nonirradiated stored donor red blood cells. Transfusion 2015, 55, 544–552. [Google Scholar] [CrossRef]
- Jelonek, K.; Pietrowska, M.; Ros, M.; Zagdanski, A.; Suchwalko, A.; Polanska, J.; Marczyk, M.; Rutkowski, T.; Skladowski, K.; Clench, M.R.; et al. Radiation-induced changes in serum lipidome of head and neck cancer patients. Int. J. Mol. Sci. 2014, 15, 6609–6624. [Google Scholar] [CrossRef]
- Ros-Mazurczyk, M.; Wojakowska, A.; Marczak, L.; Polanski, K.; Pietrowska, M.; Jelonek, K.; Dominczyk, I.; Hajduk, A.; Rutkowski, T.; Skladowski, K.; et al. Ionizing radiation affects profile of serum metabolites: Increased level of 3-hydroxybutyric acid in serum of cancer patients treated with radiotherapy. Acta Biochim. Pol. 2017, 64, 189–193. [Google Scholar]
- Jelonek, K.; Pietrowska, M.; Widlak, P. Systemic effects of ionizing radiation at the proteome and metabolome levels in the blood of cancer patients treated with radiotherapy: The influence of inflammation and radiation toxicity. Int. J. Radiat. Biol. 2017, 93, 683–696. [Google Scholar] [CrossRef]
- Jobard, E.; Blanc, E.; Negrier, S.; Escudier, B.; Gravis, G.; Chevreau, C.; Elena-Herrmann, B.; Tredan, O. A serum metabolomic fingerprint of bevacizumab and temsirolimus combination as first-line treatment of metastatic renal cell carcinoma. Br. J. Cancer 2015, 113, 1148–1157. [Google Scholar] [CrossRef] [PubMed]
- Boeckman, H.J.; Trego, K.S.; Turchi, J.J. Cisplatin sensitizes cancer cells to ionizing radiation via inhibition of nonhomologous end joining. Mol. Cancer Res. Mcr 2005, 3, 277–285. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Sathawane, R.; Mody, R. Correlation of radiotherapy with serum total and lipid-bound sialic acid in oscc patients. J. Indian Acad. Oral Med. Radiol. 2014, 26, 2–7. [Google Scholar] [CrossRef]
- Shaikh, S.; Channa, N.A.; Talpur, F.N.; Younis, M.; Tabassum, N. Radiotherapy improves serum fatty acids and lipid profile in breast cancer. Lipids Health Dis. 2017, 16, 92. [Google Scholar] [CrossRef] [PubMed]
- Widlak, P.; Jelonek, K.; Wojakowska, A.; Pietrowska, M.; Polanska, J.; Marczak, L.; Miszczyk, L.; Skladowski, K. Serum proteome signature of radiation response: Upregulation of inflammation-related factors and downregulation of apolipoproteins and coagulation factors in cancer patients treated with radiation therapy—A pilot study. Int. J. Radiat. Oncol. Biol. Phys. 2015, 92, 1108–1115. [Google Scholar] [CrossRef]
- Boguszewicz, L.; Bielen, A.; Mrochem-Kwarciak, J.; Skorupa, A.; Ciszek, M.; Heyda, A.; Wygoda, A.; Kotylak, A.; Skladowski, K.; Sokol, M. Nmr-based metabolomics in real-time monitoring of treatment induced toxicity and cachexia in head and neck cancer: A method for early detection of high risk patients. Metabolomics 2019, 15, 110. [Google Scholar] [CrossRef] [PubMed]
- Couch, M.E.; Dittus, K.; Toth, M.J.; Willis, M.S.; Guttridge, D.C.; George, J.R.; Barnes, C.A.; Gourin, C.G.; Der-Torossian, H. Cancer cachexia update in head and neck cancer: Definitions and diagnostic features. Head Neck 2015, 37, 594–604. [Google Scholar] [CrossRef]
- Ritchie, R.F.; Palomaki, G.E.; Neveux, L.M.; Navolotskaia, O.; Ledue, T.B.; Craig, W.Y. Reference distributions for the negative acute-phase serum proteins, albumin, transferrin and transthyretin: A practical, simple and clinically relevant approach in a large cohort. J. Clin. Lab. Anal. 1999, 13, 273–279. [Google Scholar] [CrossRef]
- Zhang, W.; Sun, G.; Aitken, D.; Likhodii, S.; Liu, M.; Martin, G.; Furey, A.; Randell, E.; Rahman, P.; Jones, G.; et al. Lysophosphatidylcholines to phosphatidylcholines ratio predicts advanced knee osteoarthritis. Rheumatology (Oxf. Engl.) 2016, 55, 1566–1574. [Google Scholar] [CrossRef]
- Laiakis, E.C.; Canadell, M.P.; Grilj, V.; Harken, A.D.; Garty, G.Y.; Astarita, G.; Brenner, D.J.; Smilenov, L.; Fornace, A.J., Jr. Serum lipidomic analysis from mixed neutron/x-ray radiation fields reveals a hyperlipidemic and pro-inflammatory phenotype. Sci. Rep. 2019, 9, 4539. [Google Scholar] [CrossRef]
- Wallace, T.C.; Blusztajn, J.K.; Caudill, M.A.; Klatt, K.C.; Natker, E.; Zeisel, S.H.; Zelman, K.M. Choline: The underconsumed and underappreciated essential nutrient. Nutr. Today 2018, 53, 240–253. [Google Scholar] [CrossRef] [PubMed]
- Fagone, P.; Jackowski, S. Phosphatidylcholine and the cdp-choline cycle. Biochim. Biophys. Acta 2013, 1831, 523–532. [Google Scholar] [CrossRef] [PubMed]
- Lalla, R.V.; Sonis, S.T.; Peterson, D.E. Management of oral mucositis in patients who have cancer. Dent. Clin. N. Am. 2008, 52, 61–77. [Google Scholar] [CrossRef] [PubMed]
- Schindler, A.; Denaro, N.; Russi, E.G.; Pizzorni, N.; Bossi, P.; Merlotti, A.; Spadola Bissetti, M.; Numico, G.; Gava, A.; Orlandi, E.; et al. Dysphagia in head and neck cancer patients treated with radiotherapy and systemic therapies: Literature review and consensus. Crit. Rev. Oncol. Hematol. 2015, 96, 372–384. [Google Scholar] [CrossRef] [PubMed]
- Hajduk, A.; Składowski, K.; Boguszewicz, Ł.; Mrochem-Kwarciak, J.; Hutnik, M.; Lukaszczyk-Wideł, B.; Rutkowski, T.; Wygoda, A.; Przeorek, W.; Golen, M.; et al. Acute Radiaton Sequel evaluaton in head and neck cancer patients. A new concept of comprehensive scoring system—multiparametric monitoring. Eur. Arch. Otorhinolaryngol. 2012, 269, 1311. [Google Scholar]
- Olkowicz, M.; Debski, J.; Jablonska, P.; Dadlez, M.; Smolenski, R.T. Application of a new procedure for liquid chromatography/mass spectrometry profiling of plasma amino acid-related metabolites and untargeted shotgun proteomics to identify mechanisms and biomarkers of calcific aortic stenosis. J. Chromatogr. A 2017, 1517, 66–78. [Google Scholar] [CrossRef] [PubMed]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patient Groups | CCRT | RT | Pattern of Changes | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Level (Mean Value) | Change (Mean Value ± S.D.) | Level (Mean Value) | Change (Mean Value ± S.D.) | |||||||||
| Metabolites | A | B | C | B-A | C-B | A | B | C | B-A | C-B | CCRT | RT |
| ac C0 | 47.36 | 42.61 | 41.17 | −4.75 ± 11.42 | −1.44 ± 13.61 | 43.04 | 43.44 | 36.34 | 0.4 ± 9.37 | −7.1 * ± 9.95 | A = B > C | |
| ac C16 | 0.11 | 0.08 | 0.10 | −0.03 * ± 0.04 | 0.02 ± 0.04 | 0.11 | 0.09 | 0.10 | −0.01 ± 0.05 | 0.01 ± 0.06 | A > B = C | |
| ac C18:1 | 0.19 | 0.14 | 0.17 | −0.05 * ± 0.08 | 0.03 ± 0.1 | 0.15 | 0.12 | 0.14 | −0.03 ± 0.05 | 0.02 ± 0.04 | A > B = C | |
| Cit | 36.99 | 27.89 | 26.86 | −9.1 * ± 8.48 | −1.03 ± 9.09 | 36.12 | 33.49 | 27.69 | −2.63 ± 8.29 | −5.8 ± 6.36 | A > B = C | |
| His | 102.29 | 80.43 | 75.00 | −21.86 * ± 11.88 | −5.43 ± 16.09 | 104.68 | 95.38 | 83.02 | −9.29 ± 11.91 | −12.37 ± 18.83 | A > B = C | |
| Pro | 212.13 | 157.87 | 162.69 | −54.26 * ± 38.47 | 4.82 ± 47.2 | 221.00 | 211.28 | 189.72 | −9.72 ± 46.7 | −21.56 ± 49.33 | A > B = C | |
| kynurenine | 3.01 | 2.51 | 2.14 | −0.5 * ± 0.79 | −0.36 ± 0.75 | 3.20 | 3.13 | 2.38 | −0.07 ± 0.83 | −0.75 * ± 0.61 | A > B = C | A = B > C |
| lysoPC a C16:0 | 103.65 | 83.23 | 88.67 | −20.42 * ± 21.36 | 5.44 ± 16.54 | 99.78 | 92.29 | 89.77 | −7.49 ± 20.07 | −2.52 ± 21.64 | A > B = C | |
| lysoPC a C16:1 | 2.77 | 1.86 | 1.85 | −0.9 * ± 0.87 | −0.01 ± 0.42 | 2.75 | 2.43 | 2.15 | −0.32 ± 0.89 | −0.28 ± 0.82 | A > B = C | |
| lysoPC a C18:0 | 28.62 | 21.61 | 20.34 | −7.01 * ± 7.93 | −1.28 ± 7.32 | 28.64 | 26.73 | 22.12 | −1.92 ± 6.27 | −4.61 ± 7.18 | A > B = C | |
| lysoPC a C18:1 | 18.95 | 13.84 | 17.20 | −5.11 * ± 4.75 | 3.36 ± 5.9 | 17.77 | 16.30 | 16.22 | −1.47 ± 4.02 | −0.08 ± 5.29 | A > B = C | |
| lysoPC a C18:2 | 17.48 | 11.63 | 14.20 | −5.85 * ± 5.11 | 2.57 ± 4.63 | 16.22 | 15.22 | 14.44 | −1 ± 4.33 | −0.78 ± 6.49 | A > B = C | |
| lysoPC a C20:3 | 1.66 | 1.09 | 1.04 | −0.57 * ± 0.33 | −0.05 ± 0.36 | 1.79 | 1.66 | 1.33 | −0.13 ± 0.42 | −0.33 ± 0.56 | A > B = C | |
| lysoPC a C20:4 | 5.05 | 4.08 | 4.97 | −0.97 ± 1.33 | 0.89 * ± 1.37 | 5.90 | 5.58 | 5.86 | −0.32 ± 1.03 | 0.29 ± 2.01 | A = B<C | |
| PC aa C32:0 | 14.90 | 13.68 | 17.64 | −1.23 ± 4.54 | 3.97 * ± 4.35 | 12.96 | 12.11 | 13.89 | −0.85 ± 2.66 | 1.78 ± 2.85 | A = B<C | |
| PC aa C32:1 | 22.08 | 15.32 | 15.70 | −6.76 ± 10.39 | 0.38 ± 6.35 | 16.55 | 13.13 | 12.94 | −3.43 * ± 4.82 | −0.19 ± 7.21 | A > B = C | |
| PC aa C32:2 | 2.21 | 1.66 | 2.07 | −0.55 ± 0.64 | 0.42 ± 0.72 | 2.34 | 2.33 | 0.99 | −0.01 ± 1.55 | −1.34 * ± 1.71 | A = B > C | |
| PC aa C32:3 | 0.36 | 0.29 | 0.36 | −0.07 * ± 0.08 | 0.07 * ± 0.09 | 0.37 | 0.36 | 0.36 | −0.01 ± 0.08 | −0.01 ± 0.1 | A > B<C | |
| PC aa C34:2 | 332.25 | 247.81 | 308.13 | −66.75 * ± 100.8 | 46.19 * ± 73.68 | 295.44 | 245.61 | 265.72 | −41 * ± 49.04 | 28.33 ± 59.29 | A > B<C | A > B = C |
| PC aa C34:4 | 1.20 | 0.82 | 0.81 | −0.38 ± 0.49 | −0.01 ± 0.43 | 1.14 | 1.03 | 0.71 | −0.11 ± 0.25 | −0.32 * ± 0.45 | A = B > C | |
| PC aa C36:2 | 188.38 | 137.85 | 148.95 | −50.53 * ± 52.78 | 11.1 ± 49.89 | 181.61 | 155.31 | 136.73 | −26.31 ± 23.73 | −18.57 ± 36.15 | A > B = C | |
| PC aa C36:3 | 111.54 | 75.59 | 76.28 | −35.94 * ± 34.14 | 0.68 ± 29.13 | 109.86 | 93.58 | 78.48 | −16.28 * ± 19.03 | −15.1 ± 25.9 | A > B = C | A > B = C |
| PC aa C36:6 | 0.76 | 0.54 | 0.51 | −0.22 ± 0.3 | −0.03 ± 0.27 | 0.72 | 0.73 | 0.50 | 0.01 ± 0.29 | −0.22 * ± 0.28 | A = B > C | |
| PC aa C38:3 | 45.04 | 34.30 | 32.19 | −0.5 * ± 0.58 | 0.19 ± 0.83 | 47.89 | 41.80 | 33.03 | −0.23 ± 0.79 | −0.14 * ± 0.93 | A > B = C | A = B > C |
| PC aa C40:4 | 3.49 | 2.66 | 2.63 | −0.83 ± 1.06 | −0.03 ± 0.86 | 3.40 | 2.89 | 2.49 | −0.5 * ± 0.67 | −0.41 ± 0.79 | A > B = C | |
| PC aa C40:5 | 10.28 | 7.57 | 6.91 | −2.71 * ± 3.4 | −0.65 ± 2.77 | 10.26 | 9.26 | 7.74 | −1 ± 2.69 | −1.52 * ± 2.99 | A > B = C | A = B > C |
| PC aa C42:1 | 0.28 | 0.22 | 0.21 | −0.06 * ± 0.08 | −0.01 ± 0.09 | 0.27 | 0.23 | 0.23 | −0.04 ± 0.12 | 0 ± 0.11 | A > B = C | |
| PC aa C42:6 | 0.38 | 0.28 | 0.30 | −0.1 ± 0.12 | 0.02 ± 0.11 | 0.44 | 0.42 | 0.32 | −0.03 ± 0.15 | −0.1 * ± 0.13 | A = B > C | |
| PC ae C34:3 | 5.59 | 4.05 | 6.53 | −2.48 * ± 2.23 | 1.67 * ± 2.68 | 5.67 | 5.02 | 5.44 | −1.44 ± 2.08 | −0.29 ± 2.74 | A > B<C | |
| PC ae C36:2 | 9.24 | 7.08 | 8.77 | −2.15 * ± 1.71 | 1.69 ± 3.1 | 10.54 | 9.65 | 9.24 | −0.89 ± 2.23 | −0.41 ± 2.63 | A > B = C | |
| PC ae C36:3 | 5.62 | 3.54 | 4.15 | −2.08 * ± 1.36 | 0.61 ± 1.69 | 6.61 | 5.57 | 5.07 | −1.04 * ± 1.54 | −0.51 ± 1.77 | A > B = C | A > B = C |
| PC ae C36:4 | 15.63 | 11.42 | 12.08 | −4.21 * ± 3.5 | 0.66 ± 3.82 | 16.73 | 14.19 | 13.17 | −2.54 ± 4.14 | −1.02 ± 4 | A > B = C | |
| PC ae C38:2 | 1.57 | 1.13 | 1.10 | −0.44 * ± 0.45 | −0.02 ± 0.54 | 1.43 | 1.25 | 1.16 | −0.18 ± 0.26 | −0.08 ± 0.44 | A > B = C | |
| PC ae C38:3 | 3.33 | 2.39 | 2.70 | −0.94 * ± 0.8 | 0.31 ± 0.77 | 3.54 | 3.28 | 2.85 | −0.26 ± 0.69 | −0.44 ± 0.93 | A > B = C | |
| PC ae C38:4 | 11.26 | 8.77 | 9.64 | −2.5 * ± 2.28 | 0.87 ± 3.17 | 12.62 | 10.97 | 10.33 | −1.65 * ± 2.13 | −0.64 ± 2.06 | A > B = C | A > B = C |
| PC ae C38:5 | 16.56 | 12.74 | 14.99 | −3.81 * ± 3.23 | 2.25 ± 4.54 | 18.93 | 16.33 | 16.13 | −2.6 * ± 3.67 | −0.2 ± 3.84 | A > B = C | A > B = C |
| PC ae C40:3 | 0.94 | 0.71 | 0.79 | −0.24 * ± 0.27 | 0.09 ± 0.29 | 0.90 | 0.90 | 0.85 | 0 ± 0.14 | −0.05 ± 0.22 | A > B = C | |
| PC ae C42:2 | 0.57 | 0.43 | 0.40 | −0.14 * ± 0.15 | −0.03 ± 0.17 | 0.59 | 0.55 | 0.49 | −0.05 ± 0.15 | −0.06 ± 0.17 | A > B = C | |
| SM (OH) C14:1 | 6.23 | 5.64 | 7.14 | −0.59 ± 1.72 | 1.5 * ± 1.89 | 5.28 | 5.23 | 5.94 | −0.05 ± 1.01 | 0.72 ± 1 | A = B<C | |
| SM (OH) C16:1 | 3.20 | 3.17 | 4.15 | −0.03 ± 0.67 | 0.98 * ± 1.2 | 3.17 | 3.22 | 3.87 | 0.04 ± 0.89 | 0.66 * ± 0.8 | A = B<C | A = B<C |
| SM (OH) C22:1 | 10.50 | 8.13 | 8.73 | −2.38 * ± 2.18 | 0.6 ± 3.3 | 9.72 | 8.94 | 8.64 | −0.77 ± 2.3 | −0.31 ± 2.57 | A > B = C | |
| SM C16:1 | 16.58 | 14.85 | 19.13 | −1.73 ± 4.34 | 4.27 * ± 4.83 | 15.71 | 14.42 | 16.54 | −1.28 ± 3.06 | 2.12 ± 2.83 | A = B<C | |
| SM C18:0 | 29.49 | 29.20 | 39.38 | −0.29 ± 9.17 | 10.18 * ± 11.71 | 26.62 | 25.94 | 32.77 | −0.68 ± 7.49 | 6.82 * ± 5.69 | A = B<C | A = B<C |
| SM C24:0 | 21.65 | 15.79 | 16.06 | −5.86 * ± 4.96 | 0.27 ± 5.79 | 18.77 | 16.57 | 15.49 | −2.21 ± 3.86 | −1.08 ± 3.59 | A > B = C | |
| SM C24:1 | 63.66 | 56.36 | 67.73 | −7.31 ± 14.77 | 11.37 ± 16.82 | 58.63 | 55.34 | 65.98 | −3.29 ± 14.52 | 10.64 * ± 9.45 | A = B<C | |
| Metabolites | RT | CCRT |
| Ratio B/A | ||
| PC aa C34:2 | 0.847 | 0.809 |
| PC aa C36:3 | 0.854 | 0.713 |
| PC ae C36:3 | 0.854 | 0.652 |
| PC ae C38:4 | 0.876 | 0.779 |
| PC ae C38:5 | 0.873 | 0.776 |
| Ratio C/B | ||
| SM (OH) C16:1 | 1.245 | 1.387 |
| SM C18:0 | 1.301 | 1.421 |
| Ratio C/A | ||
| C0 | 0.869 | 0.895 |
| His | 0.797 | 0.742 |
| Pro | 0.868 | 0.792 |
| Kynurenine | 0.775 | 0.756 |
| lysoPC a C20:3 | 0.787 | 0.668 |
| PC aa C36:3 | 0.714 | 0.719 |
| PC aa C38:3 | 0.687 | 0.733 |
| PC aa C40:5 | 0.774 | 0.720 |
| PC ae C36:3 | 0.783 | 0.780 |
| PC ae C38:3 | 0.815 | 0.843 |
| PC ae C38:4 | 0.835 | 0.872 |
| SM (OH) C16:1 | 1.270 | 1.322 |
| SM C18:0 | 1.289 | 1.347 |
| SM C24:0 | 0.825 | 0.756 |
| Characteristics | CCRT | RT | ICT |
|---|---|---|---|
| Number of patients | 16 | 18 | 13 |
| Age [years] (median) | 49–75 (58) | 55–77 (63) | 46–80 (63) |
| Gender: male/female | 13/3 | 12/6 | 11/2 |
| Tumor localization | |||
| Oral cavity | 0 | 2 | 3 |
| Tonsil | 2 | 3 | 3 |
| Pharynx | 7 | 1 | 7 |
| Larynx | 7 | 12 | 0 |
| TNM staging | |||
| T1 | 0 | 1 | 0 |
| T2 | 4 | 11 | 1 |
| T3 | 7 | 6 | 6 |
| T4 | 5 | 0 | 6 |
| N0 | 6 | 16 | 1 |
| N1 | 2 | 1 | 1 |
| N2 | 8 | 1 | 7 |
| N3 | 0 | 0 | 4 |
| Radiotherapy | |||
| Total dose [Gy] (median) | 70 | 50-72 (72) | - |
| 7x1,8Gy/week | 0 | 10 | - |
| 5x2Gy/week | 16 | 2 | - |
| 5x2,2Gy/week | 0 | 4 | - |
| 5x2,5Gy/week | 0 | 2 | - |
| Chemotherapy | |||
| Cisplatin (100 mg/m2) | 16 | - | 5 |
| Cisplatin (100 mg/m2) + 5-fluorouracil (800 mg/m2) | 0 | - | 8 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jelonek, K.; Krzywon, A.; Jablonska, P.; Slominska, E.M.; Smolenski, R.T.; Polanska, J.; Rutkowski, T.; Mrochem-Kwarciak, J.; Skladowski, K.; Widlak, P. Systemic Effects of Radiotherapy and Concurrent Chemo-Radiotherapy in Head and Neck Cancer Patients—Comparison of Serum Metabolome Profiles. Metabolites 2020, 10, 60. https://doi.org/10.3390/metabo10020060
Jelonek K, Krzywon A, Jablonska P, Slominska EM, Smolenski RT, Polanska J, Rutkowski T, Mrochem-Kwarciak J, Skladowski K, Widlak P. Systemic Effects of Radiotherapy and Concurrent Chemo-Radiotherapy in Head and Neck Cancer Patients—Comparison of Serum Metabolome Profiles. Metabolites. 2020; 10(2):60. https://doi.org/10.3390/metabo10020060
Chicago/Turabian StyleJelonek, Karol, Aleksandra Krzywon, Patrycja Jablonska, Ewa M. Slominska, Ryszard T. Smolenski, Joanna Polanska, Tomasz Rutkowski, Jolanta Mrochem-Kwarciak, Krzysztof Skladowski, and Piotr Widlak. 2020. "Systemic Effects of Radiotherapy and Concurrent Chemo-Radiotherapy in Head and Neck Cancer Patients—Comparison of Serum Metabolome Profiles" Metabolites 10, no. 2: 60. https://doi.org/10.3390/metabo10020060
APA StyleJelonek, K., Krzywon, A., Jablonska, P., Slominska, E. M., Smolenski, R. T., Polanska, J., Rutkowski, T., Mrochem-Kwarciak, J., Skladowski, K., & Widlak, P. (2020). Systemic Effects of Radiotherapy and Concurrent Chemo-Radiotherapy in Head and Neck Cancer Patients—Comparison of Serum Metabolome Profiles. Metabolites, 10(2), 60. https://doi.org/10.3390/metabo10020060