
Anticancer Dose Adjustment for Patients with Renal and Hepatic Dysfunction: From Scientific Evidence to Clinical Application

Abstract
:1. Introduction
2. Materials and Methods
2.1. Literature Search
2.2. Algorithm Development
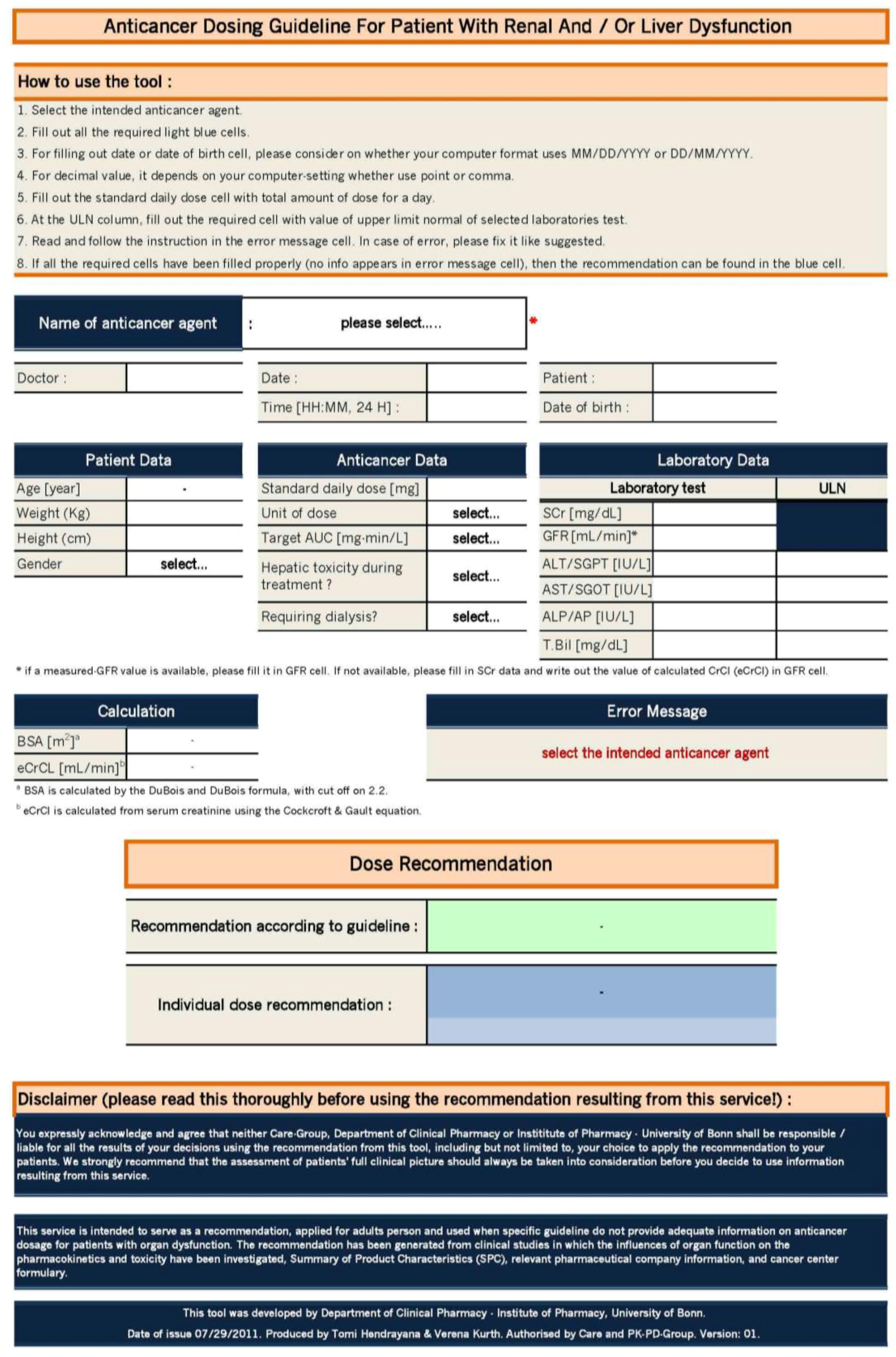
2.3. Excel Tool
2.4. Guideline Application
3. Results
3.1. Development of the Dose Adaption Guideline
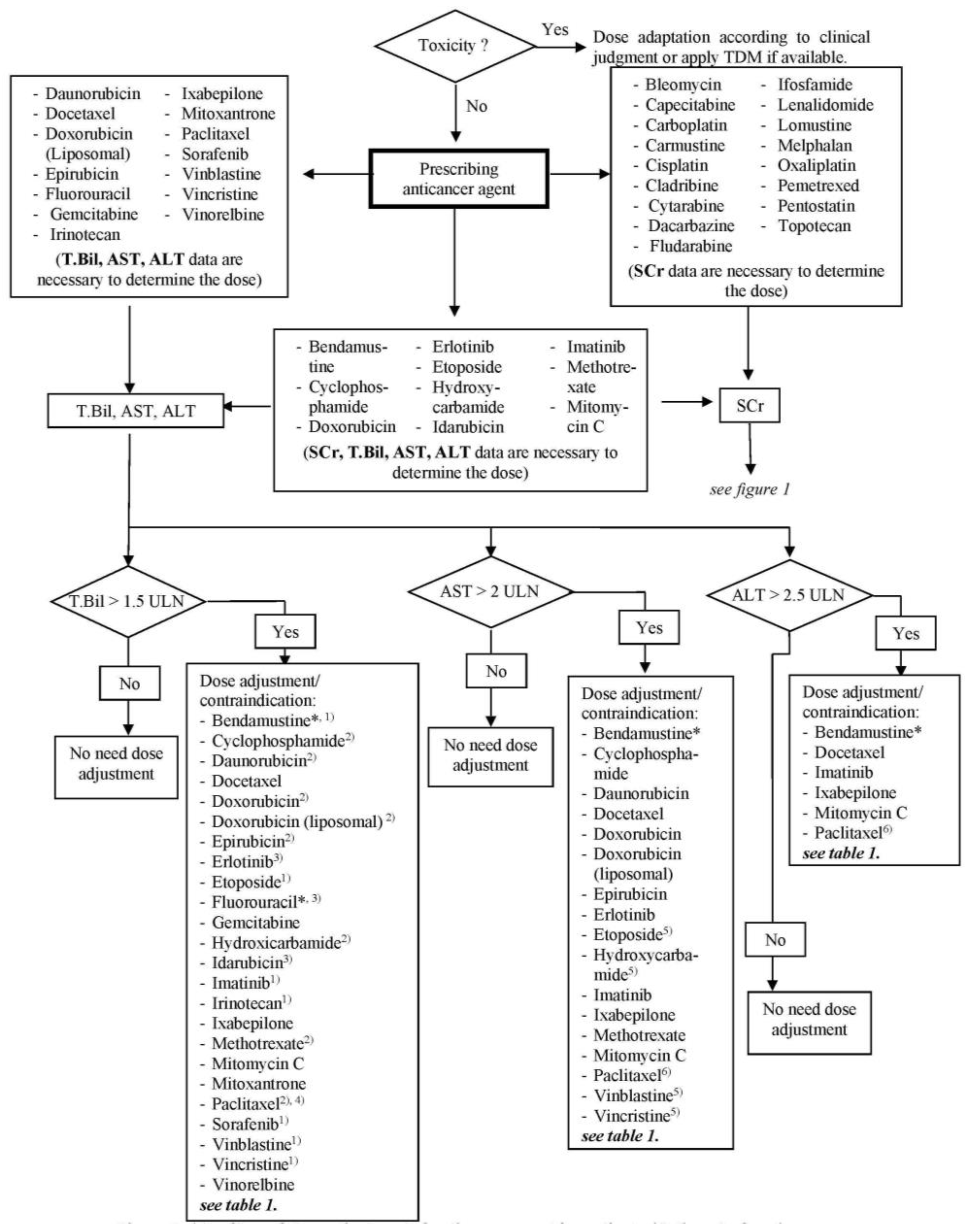
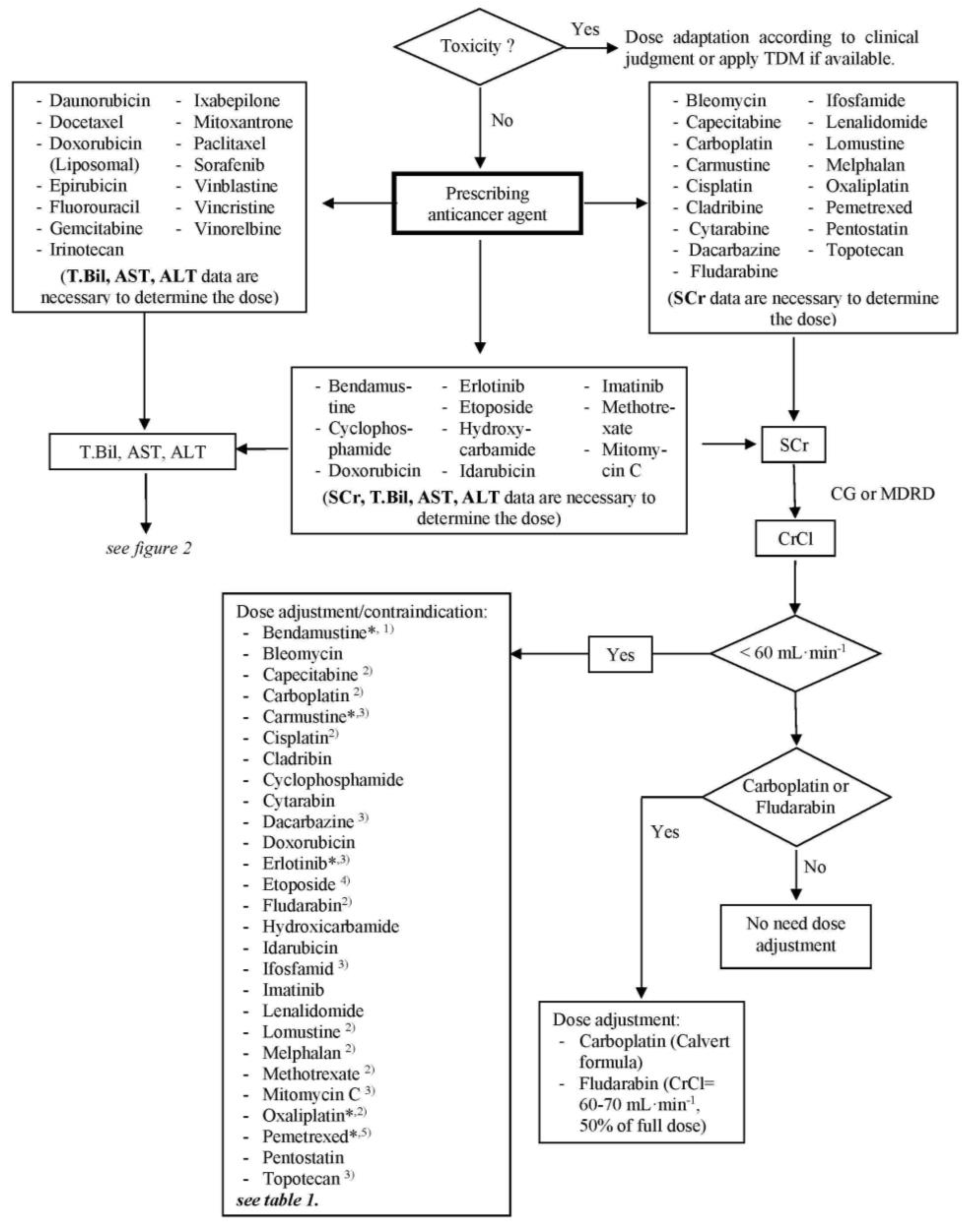
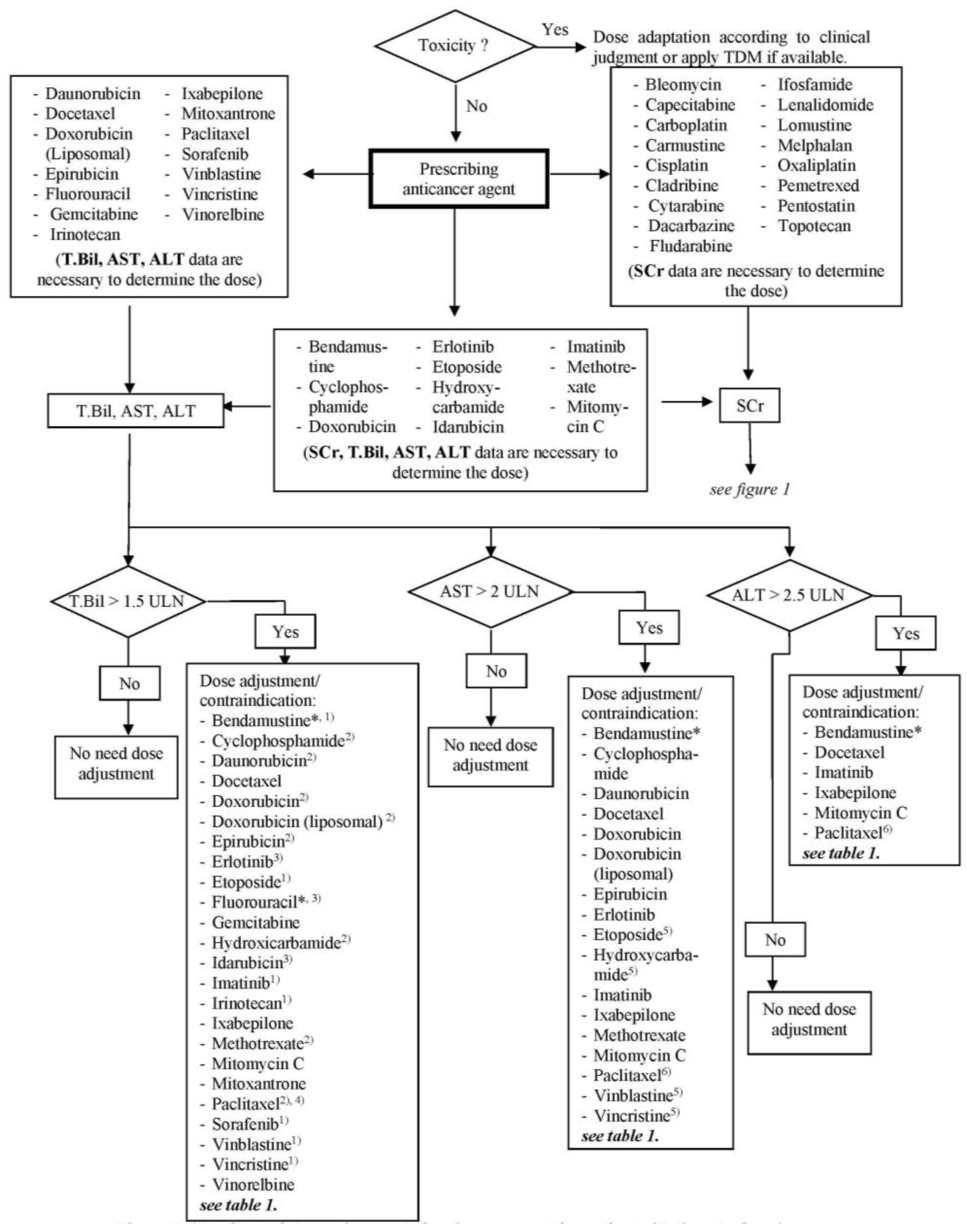
3.2. Algorithm Development
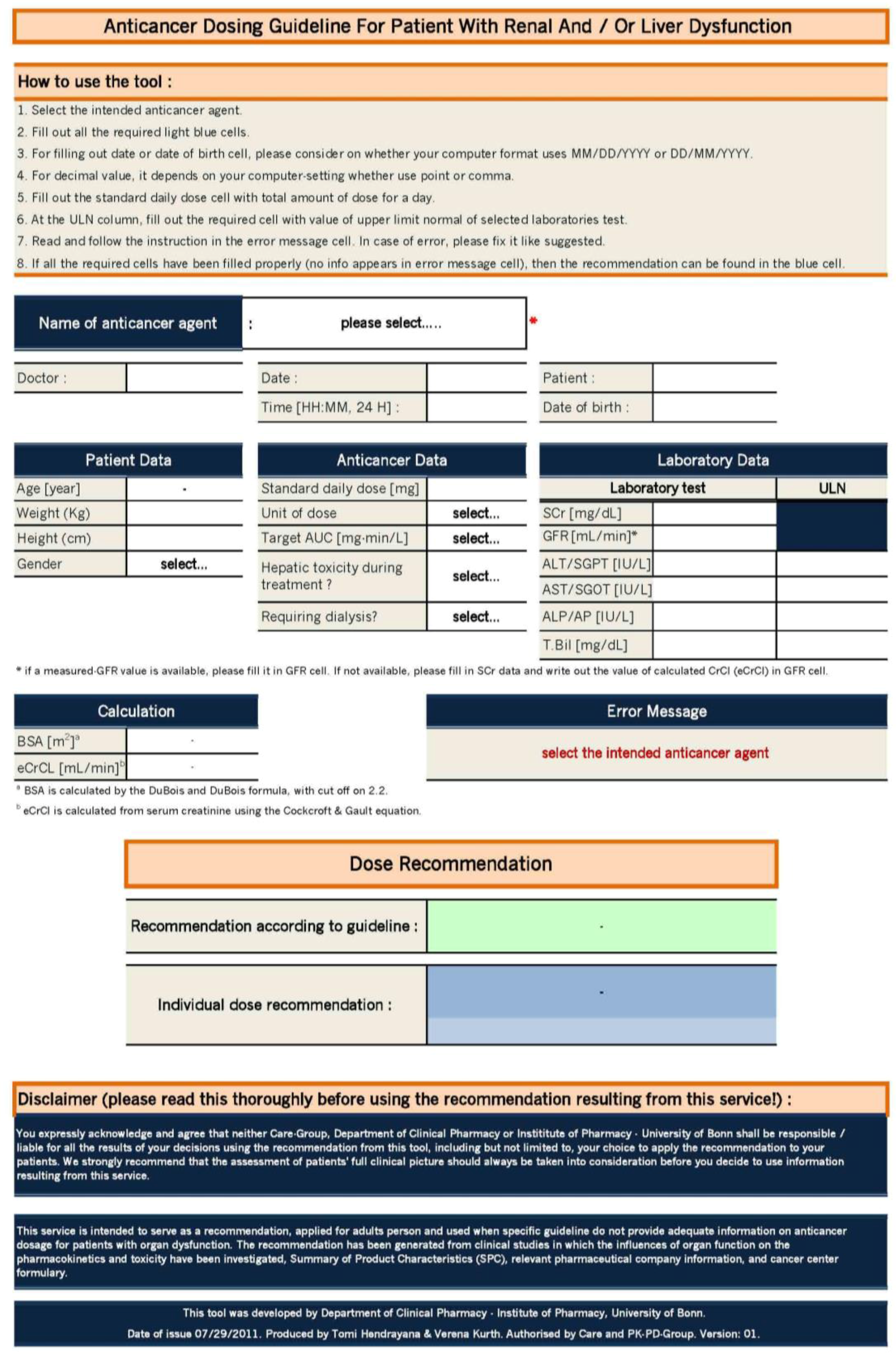
3.3. Excel Tool
3.4. Guideline Application and Acceptance
4. Discussion
5. Conclusions
Acknowledgments
Author Contributions
Conflicts of Interest
References
- Masson, E.; Zamboni, W.C. Pharmacokinetic optimisation of cancer chemotherapy. Effect on outcomes. Clin. Pharmacokinet. 1997, 32, 324–343. [Google Scholar] [CrossRef] [PubMed]
- Gurney, H. How to calculate the dose of chemotherapy. Br. J. Cancer 2002, 86, 1297–1302. [Google Scholar] [CrossRef] [PubMed]
- Launay-Vacher, V.; Spano, J.-P.; Janus, N.; Gligorov, J.; Ray-Coquardd, I.; Oudard, S.; Pourrat, X.; Morereg, J.-F.; Beuzeboch, P.; Deray, G.; et al. Renal insufficiency and anticancer drugs in elderly cancer patients: A subgroup analysis of the irma study. Crit. Rev. Oncol. Hematol. 2009, 70, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Launay-Vacher, V.; Izzedine, H.; Rey, J.-B.; Rixe, O.; Chapalain, S.; Nourdine, S.; Bourget, P.; Deray, G. Incidence of renal insufficiency in cancer patients and evaluation of information available on the use of anticancer drugs in renally impaired patients. Med. Sci. Monit. 2004, 10, CR209–CR212. [Google Scholar] [PubMed]
- Rahman, A.; White, R.M. Cytotoxic anticancer agents and renal impairment study: The challenge remains. J. Clin. Oncol. 2006, 24, 533–536. [Google Scholar] [CrossRef] [PubMed]
- Eklund, J.W.; Trifilio, S.; Mulcahy, M.F. Chemotherapy dosing in the setting of liver dysfunction. Oncology 2005, 19, 1057–1069. [Google Scholar] [PubMed]
- Lam, M.S.; Ignoffo, R.J. A guide to clinically relevant drug interactions in oncology. J. Oncol. Pharm. Pract. 2003, 9, 45–85. [Google Scholar] [CrossRef]
- Network, D.-B.L.C. Dose Modification for Renal and Hepatic Impairment. Available online: http://www.derbyhospitals.nhs.uk/EasysiteWeb/getresource.axd?AssetID=6287&type=Full&servicetype=Attachment (accessed on 20 September 2011).
- Superfin, D.; Iannucci, A.A.; Davies, A.M. Commentary: Oncologic drugs in patients with organ dysfunction: A summary. Oncologist 2007, 12, 1070–1083. [Google Scholar] [CrossRef] [PubMed]
- Ontario, C.C. Cancer Center Ontario Drug Formulary for Health Professionals. Available online: https://www.cancercare.on.ca/cms/one.aspx?objectld=1076O&contextId=1377 (accessed on 20 September 2011).
- Cockcroft, D.W.; Gault, M.H. Prediction of creatinine clearance from serum creatinine. Nephron 1976, 16, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Bendamustin. In Drugdex. Available online: http://www.micromedexsolutions.com/home/dispatch (accessed on 16 May 2011).
- Bleomycin Injection, Blenoxane®—Summary of Product Characteristics (spc). Available online: http://www.rxlist.com/blenoxane-drug.htm (accessed on 16 May 2011).
- Bleomycin. In Drug Formulary Monograph. Available online: https://www.cancercare.on.ca/cms/One.aspx?portalId=1377&pageId=10760 (accessed on 16 May 2011).
- Hurria, A.; Lichtman, S. Clinical pharmacology of cancer therapies in older adults. Br. J. Cancer 2008, 98, 517–522. [Google Scholar] [CrossRef] [PubMed]
- Shellens, J.H.M. Capecitabine. Oncologist 2007, 12, 152–155. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.F.; Fu, S.; Hu, W.; Liu, J.H.; Finkel, K.W.; Gershenson, D.M.; Kavanagh, J.J. Systemic anticancer therapy in gynecological cancer patients with renal dysfunction. Int. J. Gynecol. Cancer 2007, 17, 739–763. [Google Scholar] [CrossRef] [PubMed]
- Carboplatin. In Drug Monograph. Available online: http://www.fachinfo.de/suche/carboplatin (accessed on 16 May 2011).
- Carboplatin. In Drug Formulary Monograph. Available online: http://www.cancercare.on.ca/cms/One.aspx?portalId=1377&pageId=10760 (accessed on 16 May 2011).
- Carmustine. In Drugdex. Available online: http://www.micromedexsolutions.com/home/dispatch (accessed on 16 May 2011).
- Lichtman, S.M.; Wildiers, H.; Launay-Vacher, V.; Steer, C.; Chatelut, E.; Aapro, M. International society of geriatric oncology (siog) recommendations for the adjustment of dosing in elderly cancer patients with renal insufficiency. Eur. J. Cancer 2007, 43, 14–34. [Google Scholar] [CrossRef] [PubMed]
- Cisplatin. In Drug Formulary Monograph. Available online: https://www.cancercare.on.ca/cms/One.aspx?portalId=1377&pageId=10760 (accessed on 16 May 2011).
- Cladribine. In Drugdex. Available online: http://www.micromedexsolutions.com/home/dispatch (accessed on 16 May 2011).
- Docetaxel. In Drug Formulary Monograph. Available online: https://www.cancercare.on.ca/cms/One.aspx?portalId=1377&pageId=10760 (accessed on 16 May 2011).
- Docetaxel Trihydrate, Taxotere®—Summary of Product Characteristics (spc)—(emc). Available online: https://www.medicines.org.uk/emc/search (accessed on 16 May 2011).
- Liposomal Doxorubicin. In Drug Formulary Monograph. Available online: https://www.cancercare.on.ca/cms/One.aspx?portalId=1377&pageId=10760 (accessed on 16 May 2011).
- Field, K.M.; Michael, M. Part ii: Liver function in oncology: Towards safer chemotherapy use. Lancet Oncol. 2008, 9, 1181–1190. [Google Scholar] [CrossRef]
- Erlotinib. In Drug Monograph. Available online: http://www.fachinfo.de/suche/erlotinib (accessed on 16 May 2011).
- Etoposid. In Drug Monograph. Available online: http://www.fachinfo.de/suche/etoposid (accessed on 16 May 2011).
- Fludarabine, Fludara®—Summary of Product Characteristics (spc)—(emc). Available online: https://www.medicines.org.uk/emc/search (accessed on 16 May 2011).
- Fluorouracil. In Drug Formulary Monograph. Available online: https://www.cancercare.on.ca/cms/One.aspx?portalId=1377&pageId=10760 (accessed on 16 May 2011).
- Gemcitabine—Summary of Product Characteristics (spc)—(emc). Available online: https://www.medicines.org.uk/emc/search (accessed on 16 May 2011).
- Idarubicin. In Drugdex. Available online: http://www.micromedexsolutions.com/home/dispatch (accessed on 16 May 2011).
- Imatinib. In Drugdex. Available online: http://www.micromedexsolutions.com/home/dispatch (accessed on 16 May 2011).
- Irinotecan. In Drug Formulary Monograph. Available online: https://www.cancercare.on.ca/cms/One.aspx?portalId=1377&pageId=10760 (accessed on 16 May 2011).
- Irinotecan. In Drug Monograph. Available online: http://www.fachinfo.de/suche/irinotecan (accessed on 16 May 2011).
- Ixabepilone. In Drugdex. Available online: http://www.micromedexsolutions.com/home/dispatch (accessed on 16 May 2011).
- Lenalidomide. In Drugdex. Available online: http://www.micromedexsolutions.com/home/dispatch (accessed on 16 May 2011).
- Lenalidomide. In Drug Formulary Monograph. Available online: https://www.cancercare.on.ca/cms/One.aspx?portalId=1377&pageId=10760 (accessed on 16 May 2011).
- Kintzel, P.E.; Dorr, R.T. Anticancer drug renal toxicity and elimination: Dosing guidelines for altered renal function. Cancer Treat. Rev. 1995, 21, 33–64. [Google Scholar] [CrossRef]
- Melphalan. In Drug Formulary Monograph. Available online: https://www.cancercare.on.ca/cms/One.aspx?portalId=1377&pageId=10760 (accessed on 16 May 2011).
- Mitoxantrone. In Drug Formulary Monograph. Available online: https://www.cancercare.on.ca/cms/One.aspx?portalId=1377&pageId=10760 (accessed on 16 May 2011).
- Oxaliplatin. In Drug Monograph. Available online: http://www.fachinfo.de/suche/oxaliplatin (accessed on 16 May 2011).
- Paclitaxel. In Drugdex. Available online: http://www.micromedexsolutions.com/home/dispatch (accessed on 16 May 2011).
- Paclitaxel. In Drug Formulary Monograph. Available online: https://www.cancercare.on.ca/cms/One.aspx?portalId=1377&pageId=10760 (accessed on 16 May 2011).
- Pemetrexed. In Drugdex. Available online: http://www.micromedexsolutions.com/home/dispatch (accessed on 16 May 2011).
- Sorafenib, Nexavar®—Summary of Product Characteristics (spc)—(emc)”. Available online: https://www.medicines.org.uk/emc/search (accessed on 16 May 2011).
- Vinblastine. In Drug Formulary Monograph. Available online: https://www.cancercare.on.ca/cms/One.aspx?portalId=1377&pageId=10760 (accessed on 16 May 2011).
- Vincristine. In Drug Formulary Monograph. Available online: https://www.cancercare.on.ca/cms/One.aspx?portalId=1377&pageId=10760 (accessed on 16 May 2011).
- Vinorelbine—Summary of Product Characteristics (spc)—(emc). Available online: https://www.medicines.org.uk/emc/search (accessed on 16 May 2011).
- Vinorelbine. In Drug Formulary Monograph. Available online: https://www.cancercare.on.ca/cms/One.aspx?portalId=1377&pageId=10760 (accessed on 16 May 2011).
- Janus, N.; Launay-Vacher, V.; Byloos, E.; Machiels, J.-P.; Duck, L.; Kerger, J.; Wynendaele, W.; Canon, J.-L.; Lybaert, W.; Nortier, J.; et al. Cancer and renal insufficiency results of the birma study. Br. J. Cancer 2010, 103, 1815–1821. [Google Scholar] [CrossRef] [PubMed]
- Bostom, A.G.; Kronenberg, F.; Ritz, E. Predictive performance of renal function equations for patients with chronic kidney disease and normal serum creatinine levels. J. Am. Soc. Nephrol. 2002, 13, 2140–2144. [Google Scholar] [CrossRef] [PubMed]
- Kaestner, S. Chemotherapy dose modifications according to organ function or pharmacokinetics. Eur. J. Hosp. Pharm. Pract. 2008, 14, 24–25. [Google Scholar]
- Levey, A.S.; Bosch, J.P.; Lewis, J.B.; Greene, T.; Rogers, N.; Roth, D. A more accurate method to estimate glomerular filtration rate from serum creatinine: A new prediction equation. Modification of diet in renal disease study group. Ann. Intern. Med. 1999, 130, 461–470. [Google Scholar] [CrossRef] [PubMed]
- Goerdt, P.J.; Heim-Duthoy, L.K.; Macres, M.; Swan, S.K. Predictive performance of renal function estimate equations in renal allografts. Br. J. Clin. Pharmacol. 1997, 44, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Launay-Vacher, V.; Etessami, R.; Janus, N.; Spano, J.-P.; Ray-Coquard, I.; Oudard, S.P.; Gligorov, J.; Pourrat, X.; Beuzeboc, P.; Deray, G.; et al. Lung cancer and renal insufficiency: Prevalence and anticancer drug issues. Lung 2009, 187, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Field, K.M.; Dow, C.; Michael, M. Part I: Liver function in oncology: Biochemistry and beyond. Lancet Oncol. 2008, 9, 1092–1101. [Google Scholar] [CrossRef]
- Kaestner, S.A.; Sewell, G.J. Chemotherapy dosing part II: Alternative approaches and future prospects. Clin. Oncol. 2007, 19, 99–107. [Google Scholar] [CrossRef]
- Ng, T.; Chan, A. Dosing modifications of targeted cancer therapies in patients with special needs: Evidence and controversies. Crit. Rev. Oncol. Hematol. 2012, 81, 58–74. [Google Scholar] [CrossRef] [PubMed]
- Patel, H.; Egorin, M.J.; Remick, S.C.; Mulkerin, D.; Takimoto, C.H.M.; Doroshow, J.H.; Potter, D.; Ivy, S.P.; Murgo, A.J.; Ramanathan, R.K. Comparison of child-pugh (cp) criteria and nci organ dysfunction working group (nci-odwg) criteria for hepatic dysfunction (hd): Implications for chemotherapy dosing. J. Clin. Oncol. 2004, 22, 6051. [Google Scholar]
- Hon, Y.Y.; Evans, W.E. Making tdm work to optimize cancer chemotherapy: A multidisciplinary team approach. Clin. Chem. 1998, 44, 388–400. [Google Scholar] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| No. | Agent | Dose Adjustment in | Ref. | |
|---|---|---|---|---|
| Renal Dysfunction | Hepatic Dysfunction | |||
| 1. | Bendamustine |
| Moderate (transaminase 2.5–10 × ULN and T.Bil 1.5–3 × ULN) or severe (T.Bil > 3 × ULN), omit | [12] |
| 2. | Bleomycin |
| No adjustment is required | [9,13,14] |
| 3. | Capecitabine |
| No adjustment is required | [7,9,15,16] |
| 4. | Carboplatin | Dose based on GFR, using Calvert formula: Dose (mg) = target AUC × (GFR + 25). AUC = 5–7 For ESRD patient,
| No adjustment is required | [8,17,18,19] |
| 5. | Carmustine |
| Dosage adjustment maybe necessary; no specific recommendations found | [20,21] |
| 6. | Cisplatin |
| No adjustment is required | [7,8,22] |
| 7. | Cladribine |
| No specific recommendations found | [8,23] |
| 8. | Cyclophosphamide |
|
| [7] |
| 9. | Cytarabine |
| No specific recommendations found. Patient with liver dysfunction receiving cytarabine should be carefully monitored and adjust the dose based on clinical judgment. | [7] |
| 10. | Dacarbazine |
| No specific recommendations found. Patient with liver dysfunction receiving dacarbazine should be carefully monitored and adjust the dose based on clinical judgment. | [7] |
| 11. | Daunorubicin | Serum creatinine > 3 mg/dL, 50% of full dose |
| [7] |
| 12. | Docetaxel | No adjustment is required |
| [8,9,24,25] |
| 13. | Doxorubicin |
|
| [7,9] |
| 14. | Doxorubicin (Liposomal) | No adjustment is required |
| [7,26] |
| 15. | Epirubicin | Serum creatinine > 5 mg/dL, lower doses should be considered |
| [7,9] |
| 16. | Erlotinib | CrCl < 10 mL/min, omit |
| [27,28] |
| 17. | Etoposide |
|
| [7,8,9,29] |
| 18. | Fludarabine |
| No adjustment is required | [8,30] |
| 19. | Fluorouracil | No adjustment is required |
| [7,31] |
| 20. | Gemcitabine | No specific recommendations found |
| [9,27,32] |
| 21. | Hydroxyurea/Hydroxycarbamide |
|
| [7] |
| 22. | Idarubicin |
|
| [7,33] |
| 23. | Ifosfamide |
| No specific recommendations found | [7,9] |
| 24. | Imatinib |
|
| [34] |
| 25. | Irinotecan (Weekly, usual dose 125 mg/m2 for 4 of 6 weeks) | No adjustment anticipated to be required |
| [27,35] |
| 26. | Irinotecan (3 weekly, usual dose 350 mg/m2 every 3 weeks) | No adjustment anticipated to be required |
| [27,35,36] |
| 27. | Ixabepilone (monotherapy) | No specific recommendations found |
| [37] |
| 28. | Ixabepilone (in combination with capecitabine) | No specific recommendations found |
| [37] |
| 29. | Lenalidomide (use for myelodysplastic syndrome/MDS) |
| No specific recommendations found | [38,39] |
| 30. | Lenalidomide (use for Multiple Myeloma/MM) |
| No specific recommendations found | [38,39] |
| 31. | Lomustine |
| No specific recommendations found | [8,40] |
| 32. | Melphalan |
| No adjustment is required | [7,40,41] |
| 33. | Methotrexate | For low dose (<1 g/m2):
|
| [7,8] |
| 34. | Mitomycin C |
|
| [7] |
| 35. | Mitoxantrone | No adjustment is required |
| [7,42] |
| 36. | Oxaliplatin | CrCl < 30 mL/min, omit | No adjustment is required | [9,15,27,43] |
| 37. | Paclitaxel (3-h infusion and first course of therapy) | No adjustment is required |
| [44,45] |
| 38. | Paclitaxel (24-h infusion and first course of therapy) | No adjustment is required |
| [43,44] |
| 39. | Pemetrexed |
| No specific recommendations found | [21,46] |
| 40. | Pentostatin |
| Not applicable | [7] |
| 41. | Sorafenib | No adjustment is required |
| [27,47] |
| 42. | Topotecan |
| No adjustment is required | [7,9] |
| 43. | Vinblastine | No adjustment is required |
| [7,48] |
| 44. | Vincristine | No adjustment is required |
| [7,49] |
| 45. | Vinorelbine | No adjustment is required |
| [7,27,50,51] |
| Characteristics | No. of Patients | Percentage |
|---|---|---|
| Sex | ||
| Female | 37 | 35.2% |
| Male | 68 | 64.8% |
| Age, years | ||
| Mean Age | 61.5 | |
| Median Age | 66 | |
| Range | 22–90 | |
| Group of age | ||
| Adult | 48 | 45.7% |
| Elderly (≥65 years) | 57 | 54.3% |
| Site of cancer prevalence | ||
| Billiary tract | 7 | 6.7% |
| Breast | 4 | 3.8% |
| Colorectal | 23 | 21.9% |
| Esophageal | 6 | 5.7% |
| Gastric | 10 | 9.5% |
| Lymphoma | 16 | 15.2% |
| Myeloma | 4 | 3.8% |
| Pancreatic | 13 | 12.4% |
| Testicular | 6 | 5.7% |
| Urethra | 6 | 5.7% |
| Others * | 10 | 9.5% |
© 2017 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hendrayana, T.; Wilmer, A.; Kurth, V.; Schmidt-Wolf, I.G.; Jaehde, U. Anticancer Dose Adjustment for Patients with Renal and Hepatic Dysfunction: From Scientific Evidence to Clinical Application. Sci. Pharm. 2017, 85, 8. https://doi.org/10.3390/scipharm85010008
Hendrayana T, Wilmer A, Kurth V, Schmidt-Wolf IG, Jaehde U. Anticancer Dose Adjustment for Patients with Renal and Hepatic Dysfunction: From Scientific Evidence to Clinical Application. Scientia Pharmaceutica. 2017; 85(1):8. https://doi.org/10.3390/scipharm85010008
Chicago/Turabian StyleHendrayana, Tomi, André Wilmer, Verena Kurth, Ingo GH Schmidt-Wolf, and Ulrich Jaehde. 2017. "Anticancer Dose Adjustment for Patients with Renal and Hepatic Dysfunction: From Scientific Evidence to Clinical Application" Scientia Pharmaceutica 85, no. 1: 8. https://doi.org/10.3390/scipharm85010008
APA StyleHendrayana, T., Wilmer, A., Kurth, V., Schmidt-Wolf, I. G., & Jaehde, U. (2017). Anticancer Dose Adjustment for Patients with Renal and Hepatic Dysfunction: From Scientific Evidence to Clinical Application. Scientia Pharmaceutica, 85(1), 8. https://doi.org/10.3390/scipharm85010008