Transformation of Business Models in Spa Enterprises for Medical Purposes in Situations of Epidemic Threats


Abstract
:1. Introduction
2. Literature Review
2.1. Business Models and Business Model of Spa Tourism Enterprise
2.1.1. Business Models
2.1.2. Spa Business Model
- Application of environmentally friendly practices to transport, accommodation, food, and attractions;
- Better positioning of tourism activities, taking into account the positive impact on sustainable development;
- Use of technology to better manage the flow of visitors, avoiding overtourism and undertourism.
- Facilitating a paradigm shift in the perception of tourism success, taking into account the impact of tourism on environmental and socio-cultural elements.
- Adopting an integrated approach to tourism activities by coordinating the strategic objectives of the city, region, and national economy in integration with industry and the local community.
- Integrating sustainable development practices into policy agendas at all levels of government by supporting the tourism economy in taking environmentally friendly actions and implementing programs to reduce emissions and climate change impacts.
- Implementing better methods of measuring the impact of tourism on tourist destinations, which are necessary in the management process.
- Developing sustainable business models in tourism enterprises.
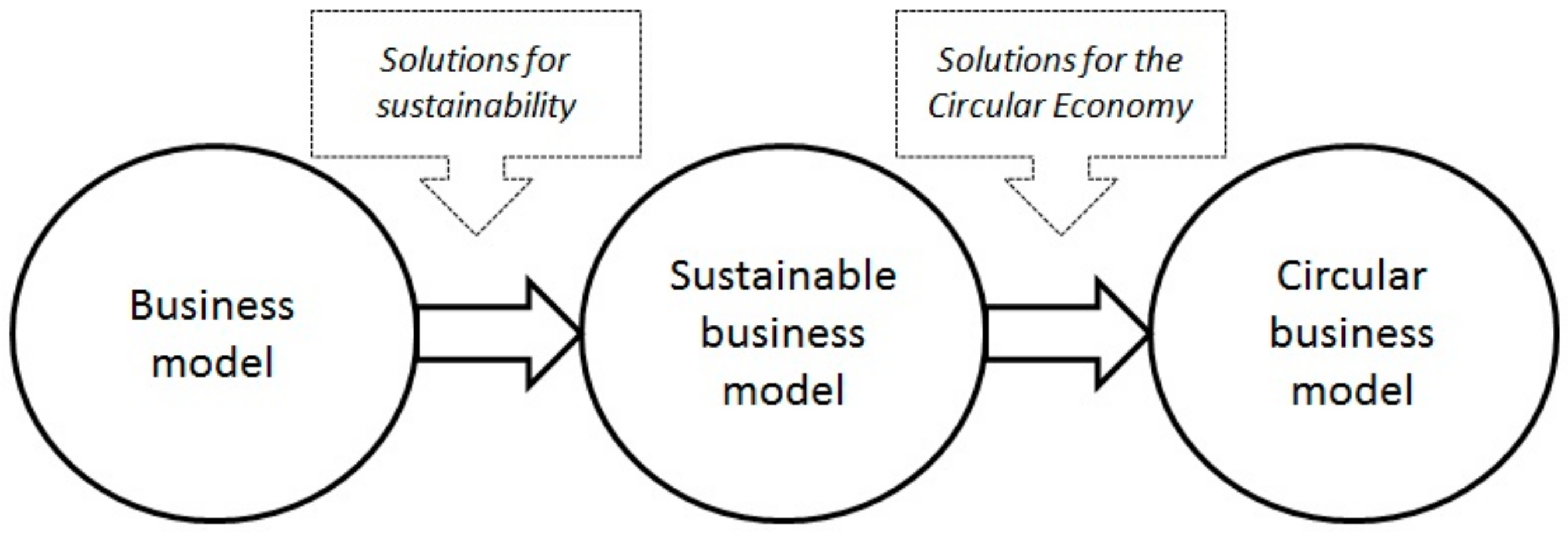
2.2. From Sustainable Business Models to Open Innovation
2.2.1. Sustainable Development Concept
2.2.2. Sustainable Business Models
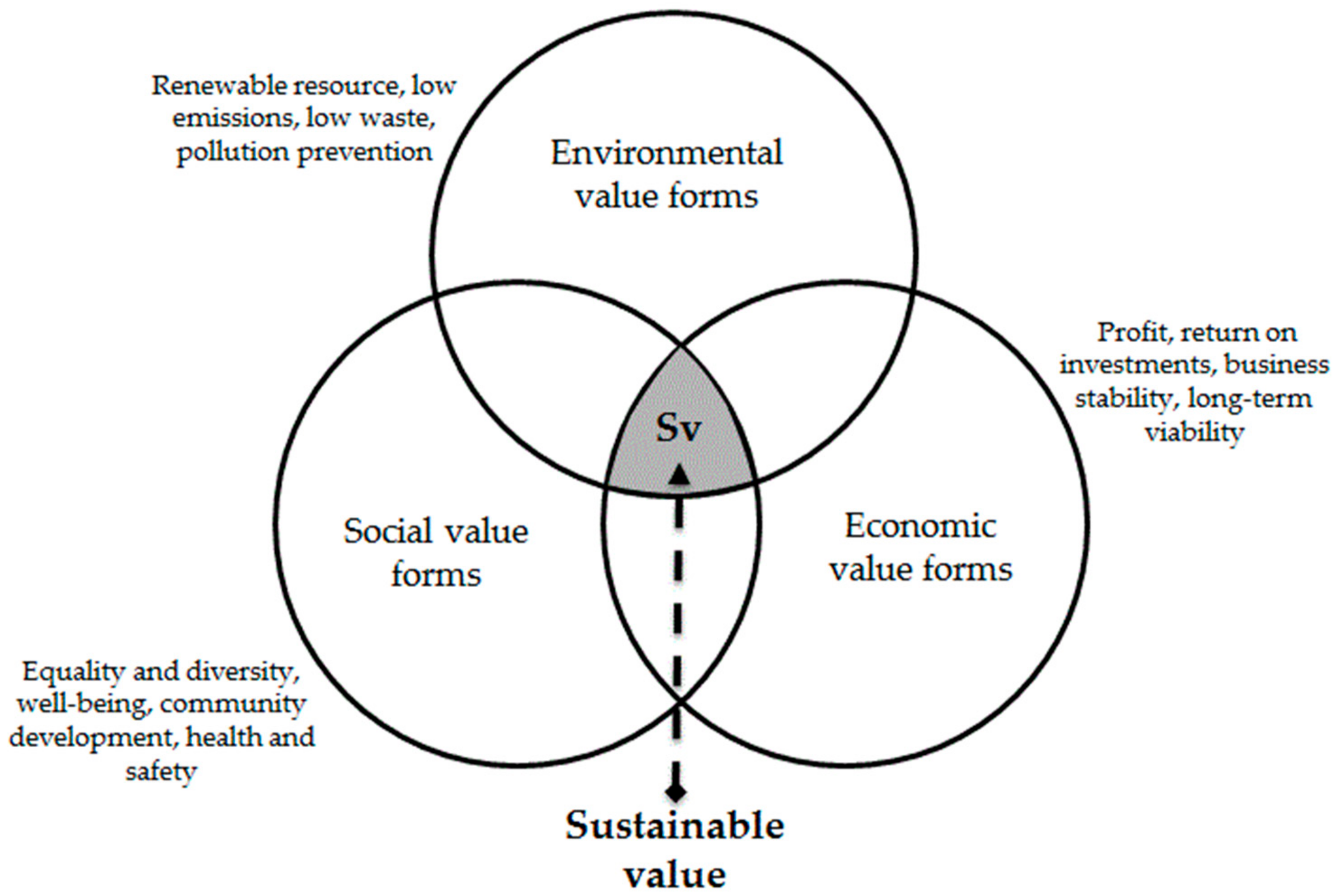
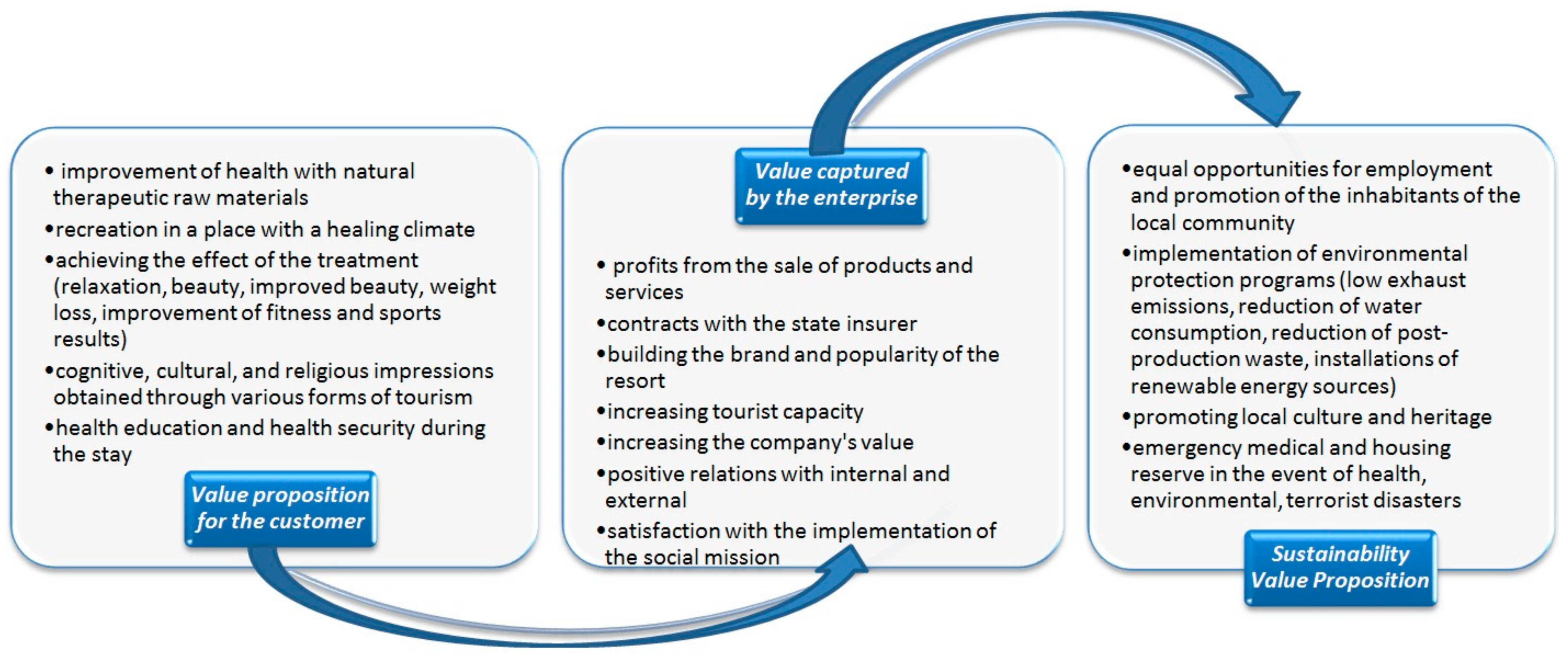
2.2.3. Sustainability Value Proposition
3. Materials and Methods
- The expert could only come from a spa company, placed by the state administration on the list of spa treatment facilities, conducting treatment and tourism activities in the spa [105].
- The expert could only be the highest-level manager (president) or his/her designee (lower-level manager, division director or legal advisor).
4. Results of Own Research in Enterprises of Health Tourism and Treatment
5. Discussion
6. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Kapczyński, A.; Szromek, A.R. Hypotheses concerning the development of Polish spas in the years 1949–2006. Tour. Manag. 2008, 29, 1035–1037. [Google Scholar] [CrossRef]
- Smith, M.; Puczkó, L. Historical overview. In Health and Wellness Tourism; Smith, M., Puczkó, L., Eds.; Routledge: New York, NY, USA, 2009. [Google Scholar]
- Rodríguez-Antón, J.M.; Alonso-Almeida, M.d.M. COVID-19 Impacts and Recovery Strategies: The Case of the Hospitality Industry in Spain. Sustainability 2020, 12, 8599. [Google Scholar] [CrossRef]
- Gössling, S.; Scott, D.; Hall, C.M. Pandemics, tourism and global change: A rapid assessment of COVID-19. J. Sustain. Tour. 2020, 29, 1–20. [Google Scholar] [CrossRef]
- Nosratabadi, S.; Mosavi, A.; Shamshirband, S.; Zavadskas, E.K.; Rakotonirainy, A.; Wing Chau, K. Sustainable Business Models: A Review. Sustainability 2019, 11, 1663. [Google Scholar] [CrossRef] [Green Version]
- Delft, S.; Zhao, Y. Business models in process industries: Emerging trends and future research. Technovation 2020, 7, 102195. [Google Scholar] [CrossRef]
- Diaconu, M.; Dutu, A. Business model in the hospitality industry, from traditional to open innovation. Sci. Bull. Econ. Sci. 2017, 16, 3–10. [Google Scholar]
- Langviniene, N.; Daunoraviþinjtơ, I. Factors influencing the success of business model in the hospitality service industry. Procedia Soc. Behav. Sci. 2015, 213, 902–910. [Google Scholar] [CrossRef] [Green Version]
- Falencikowski, T. Model biznesu dla Polski współczesnym wyzwaniem gospodarczym. Studia I Pr. Kol. Zarządzania I Finans.Szkoła Główna Handlowa 2012, 115, 38–54. [Google Scholar]
- Osterwalder, A.; Pigneur, Y. Business Model Generation: A Handbook for Visionaries, Game Changers, and Challengers; John Wiley & Sons: Hoboken, NJ, USA, 2010; p. 59. [Google Scholar]
- Chesbrough, H.W. Open Business Models: How to Thrive in the New Innovation Landscape; Harvard Business Press: Boston, MA, USA, 2006; pp. 1–272. [Google Scholar]
- Westa, J.; Salterb, A.; Vanhaverbekecef, W.; Chesbrough, H. Open Innovation: The Next Decade. Res. Policy 2014, 43, 805–811. [Google Scholar] [CrossRef]
- Seidenstricker, S.; Scheuerle, S.; Linder, C. Business Model Prototyping—Using the Morphological Analysis to Develop New Business Models. Procedia Soc. Behav. Sci. 2014, 148, 102–109. [Google Scholar] [CrossRef]
- Al-Debei, M.; El-Haddadeh, R.; Avison, D. Defining the Business Model in the New World of Digital Business. In Proceedings of the Fourteenth Americas Conference on Information Systems, Toronto, ON, Canada, 14–17 August 2008. [Google Scholar]
- Costa Climent, R.; Haftor, D.M. Value creation through the evolution of business model themes. J. Bus. Res. 2021, 122, 353–361. [Google Scholar] [CrossRef]
- Bellman, R.; Clark, C.E.; Malcolm, D.G.; Craft, C.J.; Ricciardi, F.M. On the Construction of a Multi-Stage, Multi-Person Business Game. Oper. Res. 1957, 5, 457–608. [Google Scholar] [CrossRef]
- Lang, F. Insurance research. J. Mark. 1947, 12, 66–71. [Google Scholar] [CrossRef]
- Chesbrough, H.; Rosenbloom, R. The role of the business model in capturing value from innovation: Evidence from Xerox Corporation’s technology spin-off companies. For. Ind. 2002, 11, 529–555. [Google Scholar] [CrossRef] [Green Version]
- Wit, B. Ekologistyka w Systemie Zarządzania Odpadami Niebezpiecznymi; Towarzystwo Naukowe Organizacji i Kierowania: Toruń, Poland; Stowarzyszenie Wyższej Użyteczności Dom Organizatora: Toruń, Poland, 2016; p. 138. [Google Scholar]
- Obłój, K. Tworzywo Skutecznych Strategii; PWE: Warsaw, Poland, 2002; p. 97. [Google Scholar]
- Teece, D. Business models and dynamic capabilities. Long Range Plan. 2018, 51, 40–49. [Google Scholar] [CrossRef]
- Prendeville, S.; Bocken, N. Sustainable Business Models through Service Design. Procedia Manuf. 2017, 8, 292–299. [Google Scholar] [CrossRef] [Green Version]
- Johnson, W.; Christensen, C.; Kagerman, H. Reinventing Your Business Model. Harv. Bus. Rev. 2008, 86, 57–68. [Google Scholar]
- Keen, P.; Quereshi, S. Organizational Transformation through Business Models: A Framework for Business Model Design. Inf. Syst. Quant. Anal. Fac. Proc. Present. 2006, 43, 1–10. [Google Scholar]
- Brzóska, J. Model biznesowy—współczesna forma modelu organizacyjnego zarządzania przedsiębiorstwem. Organ. I Zarządzanie Kwart. Nauk. 2009, 2, 5–23. [Google Scholar]
- Auer, C.; Follack, M. Using Action Research for Gaining Competitive Advantage out of the Internet’s Impact on Existing Business Models. In Proceedings of the 15th Bled Electronic Commerce Conference eReality: Constructing the eEconomy, Bled, Slovenia, 17–19 June 2002; pp. 767–784. [Google Scholar]
- Pateli, A.; Giaglis, G. Technology Innovation-induced Business Model Change: A Contingency Approach. J. Organ. Chang. Manag. 2005, 18, 167–183. [Google Scholar] [CrossRef]
- Senge, P.M.; Sterman, J.D. System Thinking and Organizational Learning; Acting Locally and Thinking Globally in the Organization of the Future. In Modeling for Learning Organizations; Morecroft, J.D., Sterman, J.D., Eds.; Productivity Press: Portland, OR, USA, 1994; pp. 195–216. [Google Scholar]
- Morris, M.; Schindehutte, M.; Allen, J. The entrepreneur’s business model: Toward a unified perspective. J. Bus. Res. 2005, 58, 726–735. [Google Scholar] [CrossRef]
- Amit, R.; Zott, C. Value creation in e-business. Strateg. Manag. J. 2001, 22, 493–520. [Google Scholar] [CrossRef]
- Amit, R.; Zott, C. Creating value through business model innovation. MIT Sloan Manag. Rev. 2012, 53, 41–49. [Google Scholar]
- Amit, R.; Zott, C. Crafting business architecture: The antecedents of business model design. Strateg. Entrep. J. 2015, 9, 331–350. [Google Scholar] [CrossRef]
- Souto, J. Business model innovation and business concept innovation as the context of incremental innovation and radical innovation. Tour. Manag. 2015, 51, 142–155. [Google Scholar] [CrossRef]
- Grabowska, S. Modelowanie Procesów Biznesowych w Działalności Przedsiębiorstw Turystycznych w Warunkach Konkurencyjności. Ph.D. Thesis, Silesian University of Technology, Gliwice, Poland, 2013. [Google Scholar]
- Herman, K.; Szromek, A.R. Przedsiębiorstwo Turystyczne w ujęciu Modelowym. Model Biznesu w Przedsiębiorstwie Turystyki Dziedzictwa Przemysłowego; Wydawnictwo Politechniki Śląskiej: Gliwice, Poland, 2018; p. 36. [Google Scholar]
- Szromek, A.R. Model of Business Relations in Spa Tourism Enterprises and Their Business Environment. Sustainability 2020, 12, 4941. [Google Scholar] [CrossRef]
- Strulak-Wójcikiewicz, R.; Wagner, N.; Łapko, A.; Hącia, E. Applying the Business Model Canvas to Design the E-platform for Sailing Tourism. Procedia Comput. Sci. 2020, 176, 1643–1651. [Google Scholar] [CrossRef]
- Perić, M.; Vitezić, V.; Đurkin Badurina, J. Business models for active outdoor sport event tourism experiences. Tour. Manag. Perspect. 2019, 32, 100561. [Google Scholar] [CrossRef]
- Miguéns, J.; Baggio, R.; Costa, C. Social media and Tourism Destinations: TripAdvisor Case Study. Adv. Tour. Res. 2008, 26, 1–6. [Google Scholar]
- Inversini, A.; Xiang, Z.; Fesenmaier, D.R. New meDia in Travel and Tourism Communication: Toward a New Paradigm. Available online: https://inversini.files.wordpress.com/2008/01/27_cont_9783110266535_inversini_xiang_fesenmaier1.pdf (accessed on 4 March 2021).
- Bodenau, A. Innovative Value of Sustainable Tourism Practices. Innovation and Value Creation in Experience Based Tourism. In Proceedings of the 22nd Nordic Symposium in Tourism and Hospitality Research, Bodø/Lofoten, Norway, 24–27 September 2013; pp. 23–25. [Google Scholar]
- Prebensen, N.; Dahl, J. Value co-creation significance of tourist resources. Ann. Tour. Res. 2013, 42, 240–261. [Google Scholar] [CrossRef]
- OECD. Managing tourism development for sustainable and inclusive recovery. In OECD Tourism Papers; OECD Publishing: Paris, France, 2021; pp. 1–61. [Google Scholar]
- Global Sustainable Tourism Council. GSTC Criteria for Hotels. GSTC Criteria for Tour Operators. GSTC Criteria for Destinations. 2019. Available online: http://www.gstcouncil.org/gstc-criteria/ (accessed on 1 August 2019).
- Szromek, A.R. The Sustainable Business Model of Spa Tourism Enterprise—Results of Research Carried Out in Poland. J. Open Innov. Technol. Mark. Complex. 2021, 7, 73. [Google Scholar] [CrossRef]
- Kenig-Witkowska, M.M. Międzynarodowe Prawo Środowiska; Wolters Kluwer Polska Sp. z o.o.: Warszawa, Poland, 2011. [Google Scholar]
- United Nations. Proceedings of the United Nations Conference on Environment and Development, Rio de Janeiro, Brazil, 3–14 June 1992; pp. 1–492. Available online: https://undocs.org/en/A/CONF.151/26/Rev.1(vol.I) (accessed on 4 March 2021).
- United Nations. Proceedings of the AGENDA 21, United Nations Conference on Environment & Development, Rio de Janerio, Brazil, 3–14 June 1992; pp. 1–351. Available online: https://sustainabledevelopment.un.org/content/documents/Agenda21.pdf (accessed on 4 March 2021).
- Mensah, J. Sustainable development: Meaning, history, principles, pillars, and implications for human action: Literature review. Cogent Soc. Sci. 2019, 5, 1653531. [Google Scholar] [CrossRef]
- Ukaga, U.; Maser, C.; Reichenbach, M. Sustainable development: Principles, frameworks, and case studies. Int. J. Sustain. High. Educ. 2011, 12. [Google Scholar] [CrossRef]
- Hák, T.; Janoušková, S.; Moldan, B. Sustainable development goals: A need for relevant indicators. Ecol. Indic. 2016, 60, 565–573. [Google Scholar] [CrossRef]
- Brodhag, C.; Taliere, S. Sustainable development strategies: Tools for policy coherence. Nat. Resour. Forum 2006, 30, 136–145. [Google Scholar] [CrossRef]
- Diesendorf, M. Sustainability and sustainable development. In Sustainability: The Corporate Challenge of the 21st Century; Dunphy, D., Benveniste, J., Griffiths, A., Sutton, P., Eds.; Allen & Unwin: Sydney, Australia, 2000; Volume 2, pp. 19–37. [Google Scholar]
- Evers, B.A. Why Adopt the Sustainable Development Goals? The Case of Multinationals in the Colombian Coffee and Extractive Sector. Master’s Thesis, Erasmus University Rotterdam, Rotterdam, The Netherlands, 2018. [Google Scholar]
- Arefiev, N.; Garmanov, V.; Bogdanov, V.; Ryabov, Y.; Terleev, V.; Badenko, V. A Market Approach to the Evaluation of the Ecological-Economic Damage Dealt to the Urban Lands. Procedia Eng. 2015, 117, 26–31. [Google Scholar] [CrossRef] [Green Version]
- Saith, A. From universal values to millennium development goals: Lost in translation. Dev. Chang. 2006, 37, 1167–1199. [Google Scholar] [CrossRef]
- Geissdoerfer, M.; Bocken, N.M.; Hultink, E.J. Design thinking to enhance the sustainable business modelling process—A workshop based on a value mapping process. J. Clean. Prod. 2016, 135, 1218–1232. [Google Scholar] [CrossRef] [Green Version]
- Feng, J.; Liu, Z.; Feng, L. Identifying opportunities for sustainable business models in manufacturing: Application of patent analysis and generative topographic mapping. Sustain. Prod. Consum. 2021, 27, 509–522. [Google Scholar] [CrossRef]
- Boons, F.; Lüdeke-Freund, F. Business models for sustainable innovation: State of the art and steps towards a research agenda. J. Clean. Prod. 2013, 45, 9–19. [Google Scholar] [CrossRef]
- Lüdeke-Freund, F.; Carroux, S.; Joyce, A.; Massa, L.; Breuer, H. The sustainable business model pattern taxonomy—45 patterns to support sustainability-oriented business model innovation. Sustain. Prod. Consum. 2018, 15, 145–162. [Google Scholar] [CrossRef]
- Geissdoerfer, M.; Vladimirova, D.; Evans, S. Sustainable business model innovation: A review. J. Clean. Prod. 2018, 198, 401–416. [Google Scholar] [CrossRef]
- Nidumolu, R.; Prahalad, C.K.; Rangaswami, M.R. Why sustainability is now the key driver of innovation. Harv. Bus. Rev. 2009, 87, 56–64. [Google Scholar]
- Osterwalder, A. The Business Model Ontology. A Proposition in a Design Science Approach. Ph.D. Thesis, Université de Lausanne, Lausanne, Switzerland, 2004. Available online: http://www.hec.unil.ch/aosterwa/PhD/Osterwalder_PhD_BM_Ontology.pdf (accessed on 2 March 2021).
- Doganova, L.; Eyquem-Renault, M. What do business models do? Innovation devices in technology entrepreneurship. Res. Policy 2009, 38, 1559–1570. [Google Scholar] [CrossRef] [Green Version]
- Stubbs, W.; Cocklin, C. Conceptualizing a sustainability business model. Organ. Environ. 2008, 21, 103–127. [Google Scholar] [CrossRef]
- Abdelkafi, N.; Tauscher, K. Business models for sustainability from a system dynamics perspective. Organ. Environ. 2016, 29, 74–96. [Google Scholar] [CrossRef]
- Thorisdottir, T.S.; Johannsdottir, L. Sustainability within Fashion Business Models: A Systematic Literature Review. Sustainability 2019, 11, 2233. [Google Scholar] [CrossRef] [Green Version]
- Jabłoński, A. Scalability of Sustainable Business Models in Hybrid Organizations. Sustainability 2016, 8, 194. [Google Scholar] [CrossRef] [Green Version]
- Giannoni, C.; Alarcón, L.F.; Vera, S. Diagnosis of Sustainable Business Strategies Implemented by Chilean Construction Companies. Sustainability 2018, 10, 82. [Google Scholar] [CrossRef] [Green Version]
- Lemus-Aguilar, I.; Morales-Alonso, G.; Ramirez-Portilla, A.; Hidalgo, A. Sustainable Business Models through the Lens of Organizational Design: A Systematic Literature Review. Sustainability 2019, 11, 5379. [Google Scholar] [CrossRef] [Green Version]
- Bocken, N.M.P.; Short, S.W.; Rana, P.; Evans, S. A literature and practice review to develop sustainable business model archetypes. J. Clean. Prod. 2014, 65, 42–56. [Google Scholar] [CrossRef] [Green Version]
- Ritala, P.; Huotari, P.; Bocken, N.; Albareda, L.; Puumalainen, K. Sustainable business model adoption among S&P 500 firms: A longitudinal content analysis study. J. Clean. Prod. 2018, 170, 216–226. [Google Scholar]
- Urbinati, A.; Franzò, S.; Chiaroni, D. Enablers and Barriers for Circular Business Models: An empirical analysis in the Italian automotive industry. Sustain. Prod. Consum. 2021, 27, 551–566. [Google Scholar] [CrossRef]
- Stahel, W.R. Policy for material efficiency—sustainable taxation as a departure from the throwaway society. Philos. Trans. R. Soc. A Math. Phys. Eng. Sci. 2013, 371, 20110567. [Google Scholar] [CrossRef]
- Chiaroni, D.; Urbinati, A. Circular Economy Business Models: Towards a new taxonomy of the degree of circularity. In Proceedings of the XXVII edition of the Annual Scientific Meeting of the Italian Association of Management Engineering (AiIG), Higher Education and Socio-Economic Development, Bergamo, Italy, 13–14 October 2016. [Google Scholar]
- Zucchella, A.; Previtali, P. Circular business models for sustainable development: A “waste is food”restorative ecosystem. Bus. Strategy Environ. 2019, 28, 274–285. [Google Scholar] [CrossRef]
- Mostaghel, R.; Chirumalla, K. Role of customers in circular business models. J. Bus. Res. 2021, 127, 35–44. [Google Scholar] [CrossRef]
- Evans, S.; Vladimirova, D.; Holgado, M.; Van Fossen, K.; Yang, M.; Silva, E.; Barlow, C. Business model innovation for sustainability: Towards a unified perspective for creation of sustainable business models. Bus. Strat. Env. 2017. [Google Scholar] [CrossRef]
- Yun, J.J. Business Model Design Compass. Open Innovation Funnel to Schumpeterian New Combination Business Model Developing Circle; Management for Professionals; Springer: Berlin/Heidelberg, Germany, 2017; pp. 1–248. [Google Scholar]
- Wannakrairoj, W.; Velu, C. Productivity growth and business model innovation. Econ. Lett. 2021, 199, 109679. [Google Scholar] [CrossRef]
- Bhatti, S.H.; Santoro, G.; Khan, J.; Rizzato, F. Antecedents and consequences of business model innovation in the IT industry. J. Bus. Res. 2021, 123, 389–400. [Google Scholar] [CrossRef]
- Aziz, E.; Mustapha, H.; Jamila, E.A. A bibliometric study of the recent advances in open innovation concept. Procedia Comput. Sci. 2020, 175, 683–688. [Google Scholar] [CrossRef]
- Chesbrough, H.W. Business model innovation: It’s not just about technology anymore. Strategy Lead. 2007, 35, 12–17. [Google Scholar] [CrossRef] [Green Version]
- Yun, J.J.; Zhao, X. Business model innovation through a rectangular compass: From the perspective of open innovation with mechanism design. J. Open Innov. Technol. Mark. Complex. 2020, 6, 131. [Google Scholar] [CrossRef]
- Yun, J.J.; Zhao, X.; Wu, J.; Yi, J.C.; Park, K.; Jung, W. Business model, open innovation, and sustainability in car sharing industry—Comparing three economies. Sustainability 2020, 12, 1883. [Google Scholar] [CrossRef] [Green Version]
- Agarwal, R.; Mittal, N.; Patterson, E.; Giorcelli, M. Evolution of the Indian LPG industry: Exploring conditions for public sector business model innovation. Res. Policy 2021, 50, 104196. [Google Scholar] [CrossRef]
- Harries, J.E.; Brindley, H.E.; Sagoo, P.J.; Bantges, R.J. Increases in greenhouse forcing inferred from the outgoing longwave radiation spectra of the Earth in 1970 and 1997. Nature 2001, 410, 355–357. [Google Scholar] [CrossRef]
- Hiteva, R.; Foxon, T.J. Beware the value gap: Creating value for users and for the system through innovation in digital energy services business models. Technol. Forecast. Soc. Chang. 2021, 166, 120525. [Google Scholar] [CrossRef]
- Schaltegger, S.; Hansen, E.; Lüdeke-Freund, F. Business cases for sustainability and the role of business model innovation. Int. J. Innov. Sustain. Dev. 2012, 6, 95–119. [Google Scholar] [CrossRef]
- Szromek, A.R.; Naramski, M. A Business Model in Spa Tourism Enterprises: Case Study from Poland. Sustainability 2019, 11, 2880. [Google Scholar] [CrossRef] [Green Version]
- Joyce, A.; Paquin, R. The triple layered business model canvas: A tool to design more sustainable business models. J. Clean. Prod. 2016, 135, 1484. [Google Scholar] [CrossRef]
- Jang, Y.; Ahn, Y.; Park, M.; Lee, H.-S.; Kwon, N. Business Models and Performance of International Construction Companies. Sustainability 2019, 11, 2575. [Google Scholar] [CrossRef] [Green Version]
- Butler, R.W.; Szromek, A.R. Incorporating the Value Proposition for Society with Business Models of Health Tourism Enterprises. Sustainability 2019, 11, 6711. [Google Scholar] [CrossRef] [Green Version]
- Yang, M.; Evans, S.; Vladimirova, D.; Rana, P. Value uncaptured perspective for sustainable business model innovation. J. Clean. Prod. 2016, 140, 1794–1804. [Google Scholar] [CrossRef] [Green Version]
- Elkington, J. Cannibals with Forks: The Triple Bottom Line of 21st Century Business; Capstone: Oxford, UK, 1999; ISBN 9780865713925. [Google Scholar]
- Silvius, A.J.G.; Schipper, R. A conceptual model for exploring the relationship between sustainability and project success. Procedia Comput. Sci. 2015, 64, 334–342. [Google Scholar] [CrossRef] [Green Version]
- Homrich, A.S.; Theodoro, D.S.; Monteiro de Carvalho, M. PSS creating business for sustainability: The Brazilian Olive Oil case in Mantiqueira Community. Procedia CIRP 2017, 64, 405–410. [Google Scholar] [CrossRef]
- Krechovská, M.; Tausl Prochazkova, P. Sustainability and its Integration into Corporate Governance Focusing on Corporate Performance Management and Reporting. Procedia Eng. 2014, 69, 1144–1151. [Google Scholar] [CrossRef] [Green Version]
- Waite, M. SURF Framework for a Sustainable Economy. J. Manag. Sustain. 2013, 3, 25. [Google Scholar] [CrossRef]
- Ying, T.; Wang, K.; Liu, X.; Wen, J.; Goh, E. Rethinking game consumption in tourism: A case of the 2019 novel coronavirus pneumonia outbreak in China. Tour. Recreat. Res. 2020. [Google Scholar] [CrossRef] [Green Version]
- Yang, M.; Vladimirova, D.; Rana, P.; Evans, S. Sustainable value analysis tool for value creation. Asian J. Manag. Sci. Appl. 2014, 1, 312–332. [Google Scholar] [CrossRef] [Green Version]
- Yang, M.; Rana, P.; Evans, S. Product service system (PSS) life cycle value analysis for sustainability. In Proceedings of the 6th International Conference on Design and Manufacture for Sustainable Development (ICDMSD), New York, NY, USA, 6–7 September 2013. [Google Scholar]
- Jovane, F.; Yoshikawa, H.; Alting, L.; Boër, C.R.; Westkamper, E.; Williams, D.; Tseng, M. The incoming global technological and industrial revolution towards competitive sustainable manufacturing. CIRP Ann. Manuf. Technol. 2008, 57, 641–659. [Google Scholar] [CrossRef]
- Statistisc Poland. Działalność Lecznicza Zakładów Lecznictwa Uzdrowiskowego i Stacjonarnych Zakładów Rehabilitacji Leczniczej w 2018 r. Główny Urząd Statystyczny 2019. pp. 1–5. Available online: https://stat.gov.pl/download/gfx/portalinformacyjny/pl/defaultaktualnosci/5513/12/3/1/dzialalnosc_lecznicza_zakladow_lecznictwa_uzdrowiskowego_i_stacjonarnych_w_2018.pdf (accessed on 17 March 2021).
- Ministerstwo Zdrowia Rzeczypospolitej Polskiej. 2021. Available online: http://www2.mz.gov.pl/wwwmz/index?mr=m8&ms=698&mL=pl&mi=698&mx=0&ma=13915 (accessed on 24 February 2021).
- Skare, M.; Soriano, D.R.; Porada-Rochoń, M. Impact of COVID-19 on the travel and tourism industry. Technol. Forecast. Soc. Chang. 2021, 163, 120469. [Google Scholar] [CrossRef]
- Bertella, G. Re-thinking sustainability and food in tourism. Ann. Tour. Res. 2020, 84, 103005. [Google Scholar] [CrossRef] [PubMed]
- Tew, P.J.; Lu, Z.; Tolomiczenko, G.; Gellatly, J. SARS: Lessons in strategic planning for hoteliers and destination marketers. Int. J. Contemp. Hosp. Manag. 2008, 20, 332–346. [Google Scholar]
- Silesian University of Technology. The Silesian University of Technology is Developing a Decontamination Gate for Medical Personnel. Available online: https://www.polsl.pl/Lists/AktualnosciUczelniane/PokazWiadomosc.aspx?WebPartTitle=ListaWiadomosci&Page=1&WebPartTitle2=Wiadomosc&Filter1Field2=Identyfikator&Filter1Value2=3228 (accessed on 17 March 2021).
- Butler, R.W. The concept of a Tourism Area Life Cycle of Evolution. Can. Geographer. 1980, 24, 5–12. [Google Scholar]
- Plog, S.C. Why Destination Areas Rise and Fall in Popularity. Cornell Hotel Restaur. Adm. Q. 1974, 14, 55–58. [Google Scholar] [CrossRef]
- Plog, S.C. Why Destination Areas Rise and Fall in Popularity. Cornell Hotel Restaur. Adm. Q. 2001, 42, 13–24. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| The CANVAS Business Model | |||||
|---|---|---|---|---|---|
| Key Partners | Key Activities | Value Proposition | Relations with the Customers | Customer Segments | |
| Network of suppliers and co-workers, whose activity is crucial for the effective company functioning | This element usually contains a list of key activities that make it possible to create value for the customer and functioning of particular components | It is a set of products and services that generate value for a particular customer segment. It is the reason why customers prefer a particular company’s offerings over those of competitors, as well as solving customers’ problems or satisfying their needs. | It is an element that describes the characteristics of the relationship between a company and representatives of a specific customer segment | These are groups of people and organizations that the enterprise tries to reach and service. | |
| Key Resources | Channels | ||||
| It is a company’s most essential resource that influences its performance | An element that indicates how a company communicates with its various customer segments and how it offers them its customer value proposition. | ||||
| Cost Structure | Revenue Streams | ||||
| These are all expenses incurred in using a particular business model (financial outlays of key activities, resource costs, sources of major costs) | It is a wide element of the model encompassing such issues as the size of specific revenues streams in total revenues and payment methods | ||||
| Key Partners | Key Activities | Value Proposition | Relations with the Customers | Customer Segments | |
|---|---|---|---|---|---|
|
|
|
|
| |
| Key resources | Channels | ||||
|
| ||||
| Cost Structure | Revenue Streams | ||||
|
| ||||
| Focus | Archetypes |
|---|---|
| Environment |
|
| Social |
|
| Economic |
|
| Actions Implemented by Spa Businesses during the COVID-19 Pandemic | Percentage of Establishments | Time (Days) |
|---|---|---|
| Spa therapy (stationary and outpatient) | 55.6% | 177 |
| Post-COVID therapy | 50.0% | 153 |
| Isolation section for people in quarantine | 27.8% | 107 |
| COVID vaccinations | 44.4% | 60 |
| Tourist services | 11.1% | 270 |
| Renting rooms to medical services | 11.1% | 90 |
| COVID-19 patient therapy | 16.7% | 60 |
| Specialist therapy | 5.6% | 120 |
| The Health Tourism Business Model (SusHT-CANVAS) | ||||||
|---|---|---|---|---|---|---|
| Key Partners | Key Activities | Extended Value Proposition | Relations with the Clients | Customer Segments | ||
|
| Value Proposition for the Customer (the Core) | Sustainability Value Proposition | Value Captured by the Enterprise |
| Segmentation criterion:
|
| Health effect, relax, improved beauty and sports results, weight loss, positive emotions, and memories | Employment of the local community, promoting local culture and heritage, limiting the company’s impact on the natural environment and community, emergency medical and housing reserve | Profits, increasing the company’s assets, developing relationships with clients and contractors, satisfaction with the social mission | ||||
| Key Resources |  | Channels | ||||
|
| |||||
| Cost Structure | Crisis Management and Critical Activities | Revenue Streams | ||||
|
| Breakdown criterion: market segments
| ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Szromek, A.R. Transformation of Business Models in Spa Enterprises for Medical Purposes in Situations of Epidemic Threats. J. Open Innov. Technol. Mark. Complex. 2021, 7, 143. https://doi.org/10.3390/joitmc7020143
Szromek AR. Transformation of Business Models in Spa Enterprises for Medical Purposes in Situations of Epidemic Threats. Journal of Open Innovation: Technology, Market, and Complexity. 2021; 7(2):143. https://doi.org/10.3390/joitmc7020143
Chicago/Turabian StyleSzromek, Adam R. 2021. "Transformation of Business Models in Spa Enterprises for Medical Purposes in Situations of Epidemic Threats" Journal of Open Innovation: Technology, Market, and Complexity 7, no. 2: 143. https://doi.org/10.3390/joitmc7020143
APA StyleSzromek, A. R. (2021). Transformation of Business Models in Spa Enterprises for Medical Purposes in Situations of Epidemic Threats. Journal of Open Innovation: Technology, Market, and Complexity, 7(2), 143. https://doi.org/10.3390/joitmc7020143