
Single Fetal Demise in Twin Pregnancy—A Great Concern but Still a Favorable Outcome

 ,
,
Abstract
1. Introduction
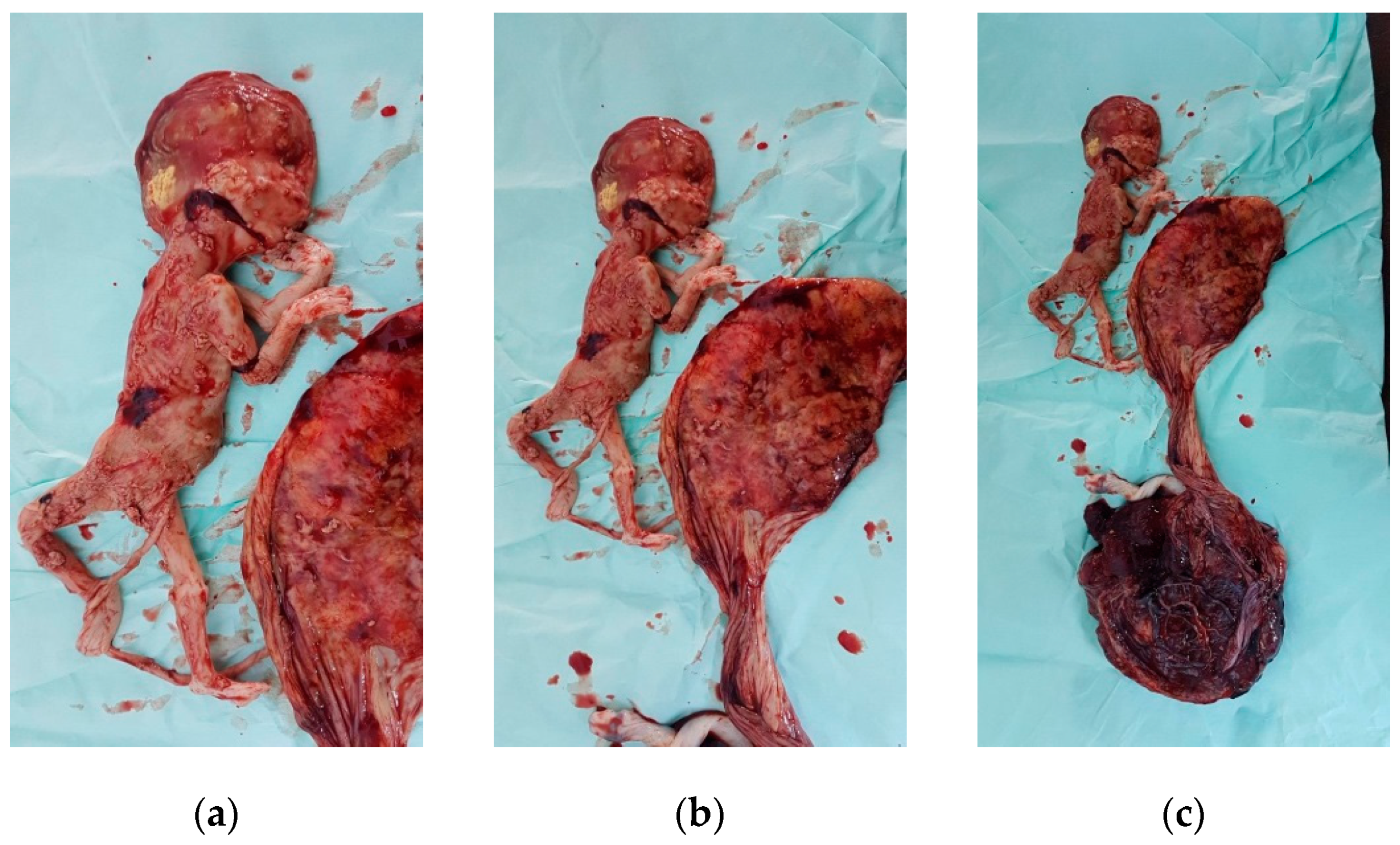
2. Case Report
3. Results and Discussions
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jain, D.; Purohit, R.C. Review of twin pregnancies with single fetal death: Management, maternal and fetal outcome. J. Obstet. Gynecol. India 2014, 64, 180–183. [Google Scholar] [CrossRef] [PubMed]
- Landy, H.J.; Weiner, S.; Corson, S.L.; Batzer, F.R.; Bolognese, R.J. The “vanishing twin”: Ultrasonographic assessment of fetal disappearance in the first trimester. Am. J. Obs. Gynecol. 1986, 155, 14–19. [Google Scholar] [CrossRef]
- Woo, H.H.; Sin, S.Y.; Tang, L.C. Single foetal death in twin pregnancies: Review of the maternal and neonatal outcomes and management. Hong Kong Med. J. 2000, 6, 293–300. [Google Scholar]
- Gaucherand, P.; Rudigoz, R.C.; Piacenza, J.M. Monofetal death in multiple pregnancies: Risks for the co-Twin, risk factors and obstetrical management. Eur. J. Obs. Gynecol. Reprod. Biol. 1994, 55, 111–115. [Google Scholar] [CrossRef]
- Mackie, F.L.; Rigby, A.; Morris, R.K.; Kilby, M.D. Prognosis of the co-twin following spontaneous single intrauterine fetal death in twin pregnancies: A systematic review and meta-analysis. BJOG Int. J. Obs. Gynaecol. 2019, 126, 569–578. [Google Scholar] [CrossRef] [PubMed]
- Enbom, J.A. Twin pregnancy with intrauterine death of one twin. Am. J. Obs. Gynecol. 1985, 152, 424–429. [Google Scholar] [CrossRef]
- Babah, O.A.; Olamijulo, A.; Ayanbode, O.S.; Sanusi, M.M. Conservative management of single fetal death in twin pregnancy at a tertiary health institution in southern Nigeria: A case report. IOSR J. Dent. Med. Sci. 2014, 13, 79–83. [Google Scholar]
- Sonneveld, S.W.; Correy, J.F. Antenatal loss of one of twins. Aust. N. Z. J. Obstet. Gynaecol. 1992, 32, 10–13. [Google Scholar] [CrossRef]
- Santema, J.G.; Swaak, A.M.; Wallenburg, H.C. Expectant management of twin pregnancy with single fetal death. BJOG Int. J. Obstet. Gynaecol. 1995, 102, 26–30. [Google Scholar] [CrossRef]
- Karl, W.M. Intrauterine death in a twin: Implications for the survivor. In Multiple Pregnancy; Ward, R.H., Whittle, M., Eds.; RCOG Press: London, UK, 1995; pp. 218–230. [Google Scholar]
- Swarankar, M.L.; Shekhawat, U.; Choudhary, M.; Choudhary, V. Maternal and neonatal outcome of surviving twin after single fetal demise at 25 weeks: A rare case report. Fertil. Sci. Res. 2017, 4, 30. [Google Scholar]
- Haque, R.; Rahman, M.M.; Akhter, K. Intrauterine Single Fetal Demise in Twin Pregnancy. Delta Med Coll. J. 2018, 6, 53–57. [Google Scholar] [CrossRef]
- Arınkan, S.A.; Arısoy, R.; Api, M. Assesment of pregnancy outcomes among twin pregnancies with single fetal demise regarding chorionicity and fetal death time. J. Turk. Ger. Gynecol. Assoc. 2019, 20, 147. [Google Scholar] [CrossRef] [PubMed]
- D’Antonio, F.; Thilaganathan, B.; Dias, T.; Khalil, A. The influence of chorionicity and gestational age at single fetal loss on the risk of preterm birth in twin pregnancies: Analysis of the STORK multiple pregnancy cohort. Ultrasound Obstet. Gynecol. 2017, 50, 723–727. [Google Scholar] [CrossRef] [PubMed]
- Hillman, S.C.; Morris, R.K.; Kilby, M.D. Co-twin prognosis after single fetal death: A systematic review and meta-analysis. Obstet. Gynecol. 2011, 118, 928–940. [Google Scholar] [CrossRef] [PubMed]
- Livnat, E.J.; Burd, L.; Cadkin, A.; Keh, P.; Ward, A.B. Fetus papyraceus in twin pregnancy. Obstet. Gynecol. 1978, 51 (Suppl. 1), 41s–45s. [Google Scholar]
- Axt, R.; Mink, D.; Hendrik, J.; Ertan, K.; Von Blohn, M. Maternal and neonatal outcome of twin pregnancies 7 complicated by single fetal death. J. Perinat. Med. 1999, 27, 221–227. [Google Scholar] [CrossRef]
- Romero, R.; Duffy, T.P.; Berkowitz, R.L.; Chang, E.; Hobbins, J.C. Prolongation of a preterm pregnancy complicated by death of a single twin in utero and disseminated intravascular coagulation: Effects of treatment with heparin. N. Engl. J. Med. 1984, 310, 772–774. [Google Scholar] [CrossRef] [PubMed]
- Pritchard, J.A.; Ratnoff, O.D. Studies of fibrinogen and other haemostatic factors in women with intrauterine death and delayed delivery. Surg. Gynecol. Obs. 1955, 101, 467–477. [Google Scholar]
- Tunç, S.Y.; Ağaçayak, E.; Yaman, G.N.; İçen, M.S.; Fındık, F.M.; Evsen, M.S.; Turgut, A.; Başaranoğlu, S.; Yıldızbakan, A.; Gül, T. Single intrauterine demise in twin pregnancies: Analysis of 29 cases. Turk. J. Obstet. Gynecol 2015, 12, 226–229. [Google Scholar] [CrossRef]
- D’alton, M.E.; Newton, E.R.; Cetrulo, C.L. Intrauterine fetal demise in multiple gestation. Acta Genet. Med. Gemellol. Twin Res. 1984, 33, 43–49. [Google Scholar] [CrossRef] [PubMed]
- Tasmin, S.F.; Akhtar, M.J.; Mondal, R.N.; Yesmin, N. Single fetal demise in twin pregnancy—A case report. Dinajpur Med. Coll. J. 2016, 9, 118–123. [Google Scholar]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1. Counseling and support. |
| 2. Individualized management plan. |
| 3. Management in a tertiary center with competent neonatal support. |
| 4. Information on chorionicity. |
| 5. Evaluation of fetal anomalies and close fetal surveillance. |
| 6. Steroid prophylaxis for lung maturity in case of preterm delivery. |
| 7. Conservative management until 37 weeks. Earlier intervention in the presence of other obstetric indications. |
| 8. Vaginal delivery if possible. |
| 9. Post-mortem examination of the stillborn. Placenta for histological examination. |
| 10. Pediatric assessment and long-term follow-up. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stefanescu, B.I.; Adam, A.-M.; Constantin, G.B.; Trus, C. Single Fetal Demise in Twin Pregnancy—A Great Concern but Still a Favorable Outcome. Diseases 2021, 9, 33. https://doi.org/10.3390/diseases9020033
Stefanescu BI, Adam A-M, Constantin GB, Trus C. Single Fetal Demise in Twin Pregnancy—A Great Concern but Still a Favorable Outcome. Diseases. 2021; 9(2):33. https://doi.org/10.3390/diseases9020033
Chicago/Turabian StyleStefanescu, Bogdan Ioan, Ana-Maria Adam, Georgiana Bianca Constantin, and Constantin Trus. 2021. "Single Fetal Demise in Twin Pregnancy—A Great Concern but Still a Favorable Outcome" Diseases 9, no. 2: 33. https://doi.org/10.3390/diseases9020033
APA StyleStefanescu, B. I., Adam, A.-M., Constantin, G. B., & Trus, C. (2021). Single Fetal Demise in Twin Pregnancy—A Great Concern but Still a Favorable Outcome. Diseases, 9(2), 33. https://doi.org/10.3390/diseases9020033