
Exploratory Evaluation of Pre-Treatment Inflammation Profiles in Patients with Colorectal Cancer




Abstract
1. Introduction
2. Materials and Methods
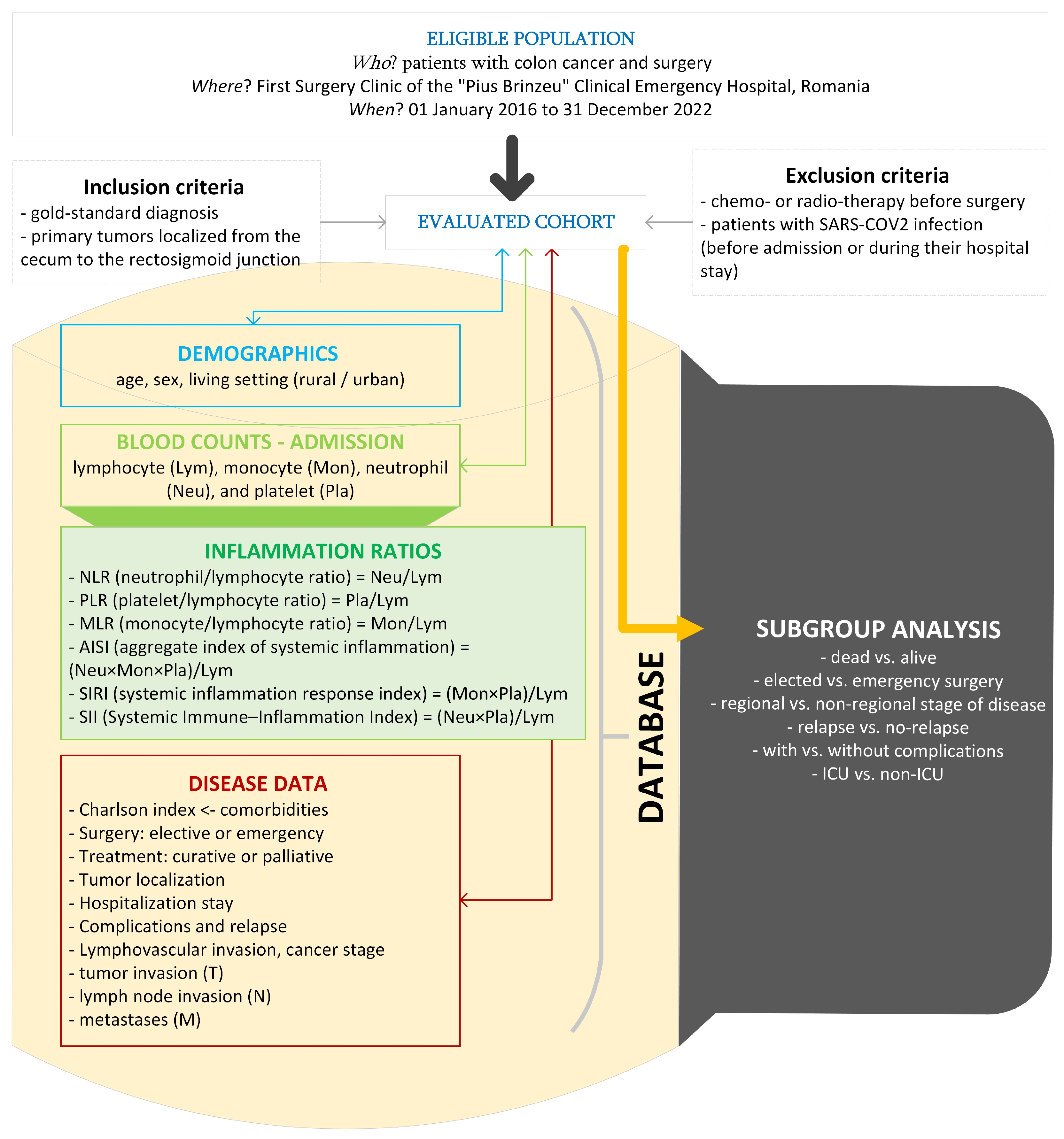
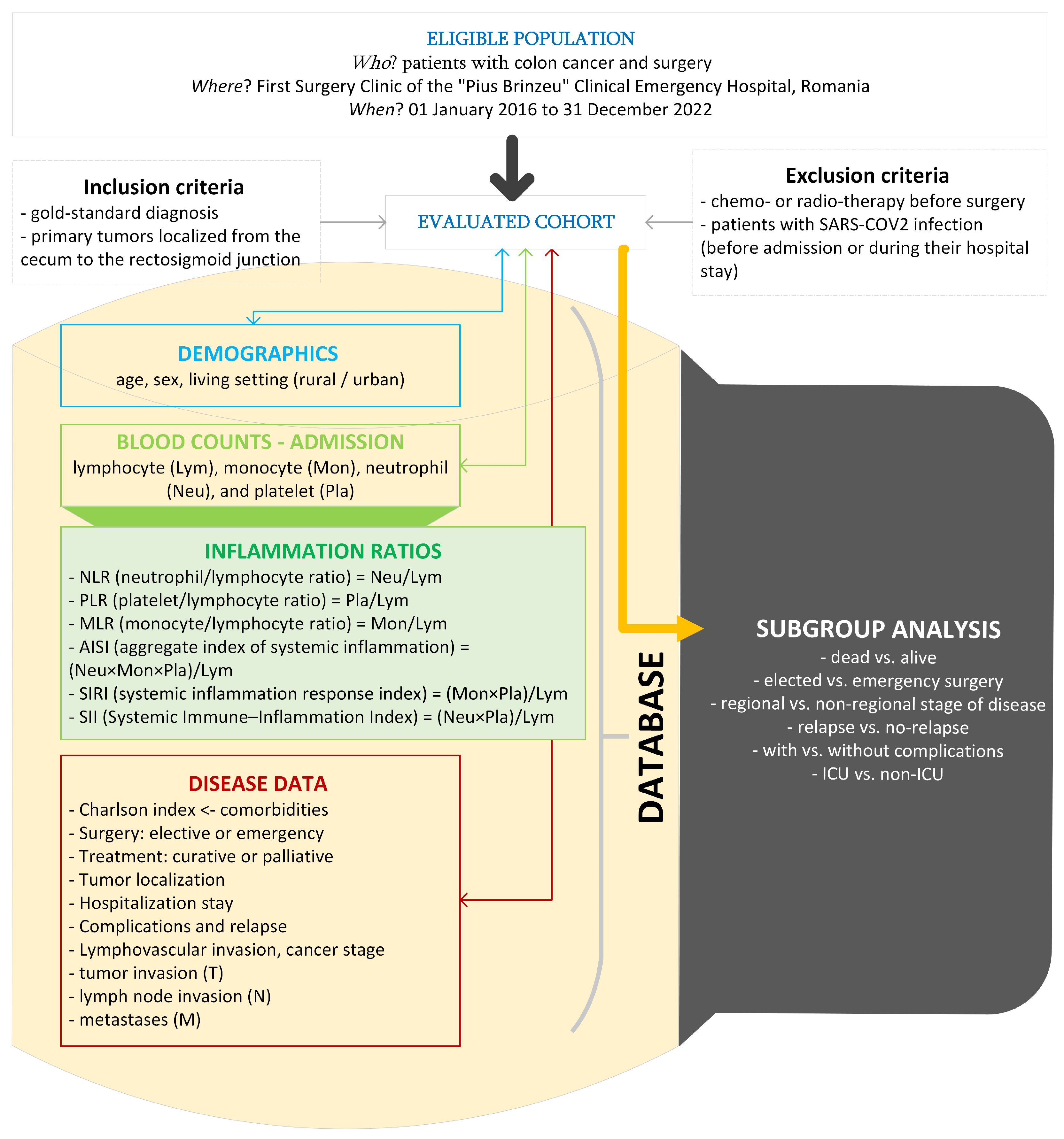
2.1. Design and Settings
2.2. Data Analysis
3. Results
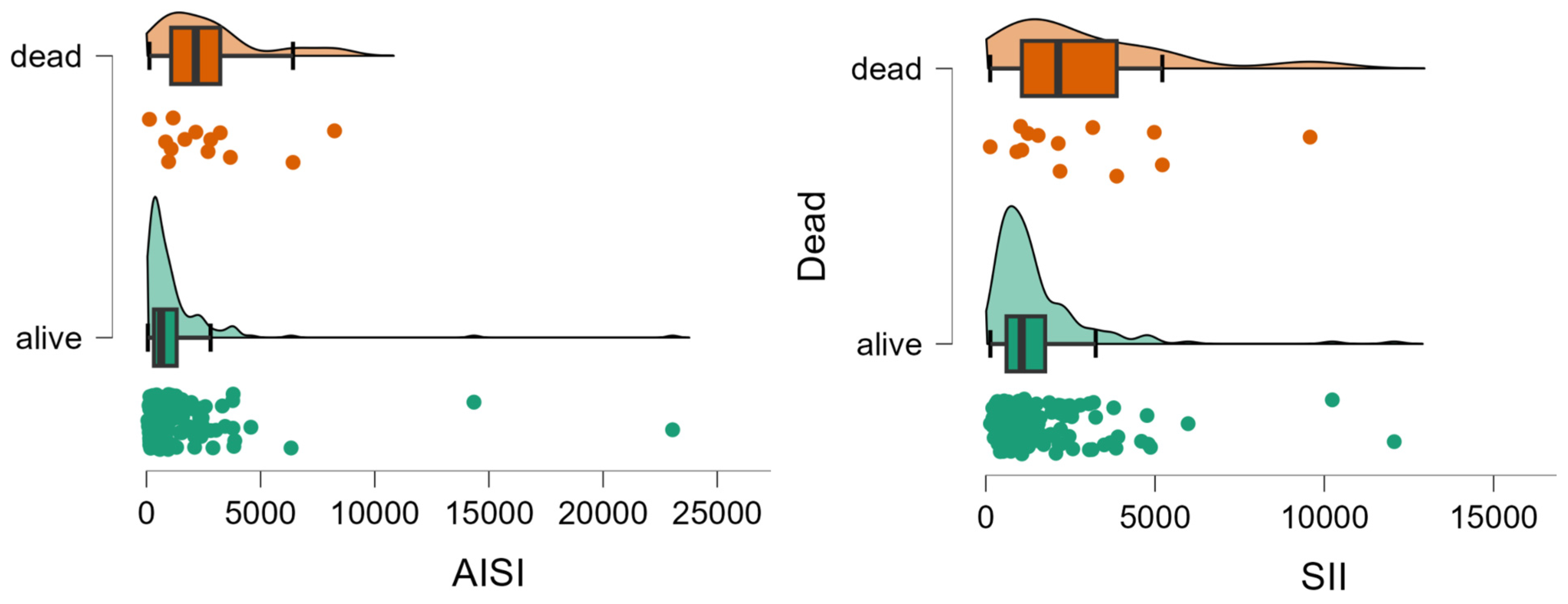
3.1. Deceased vs. Alive
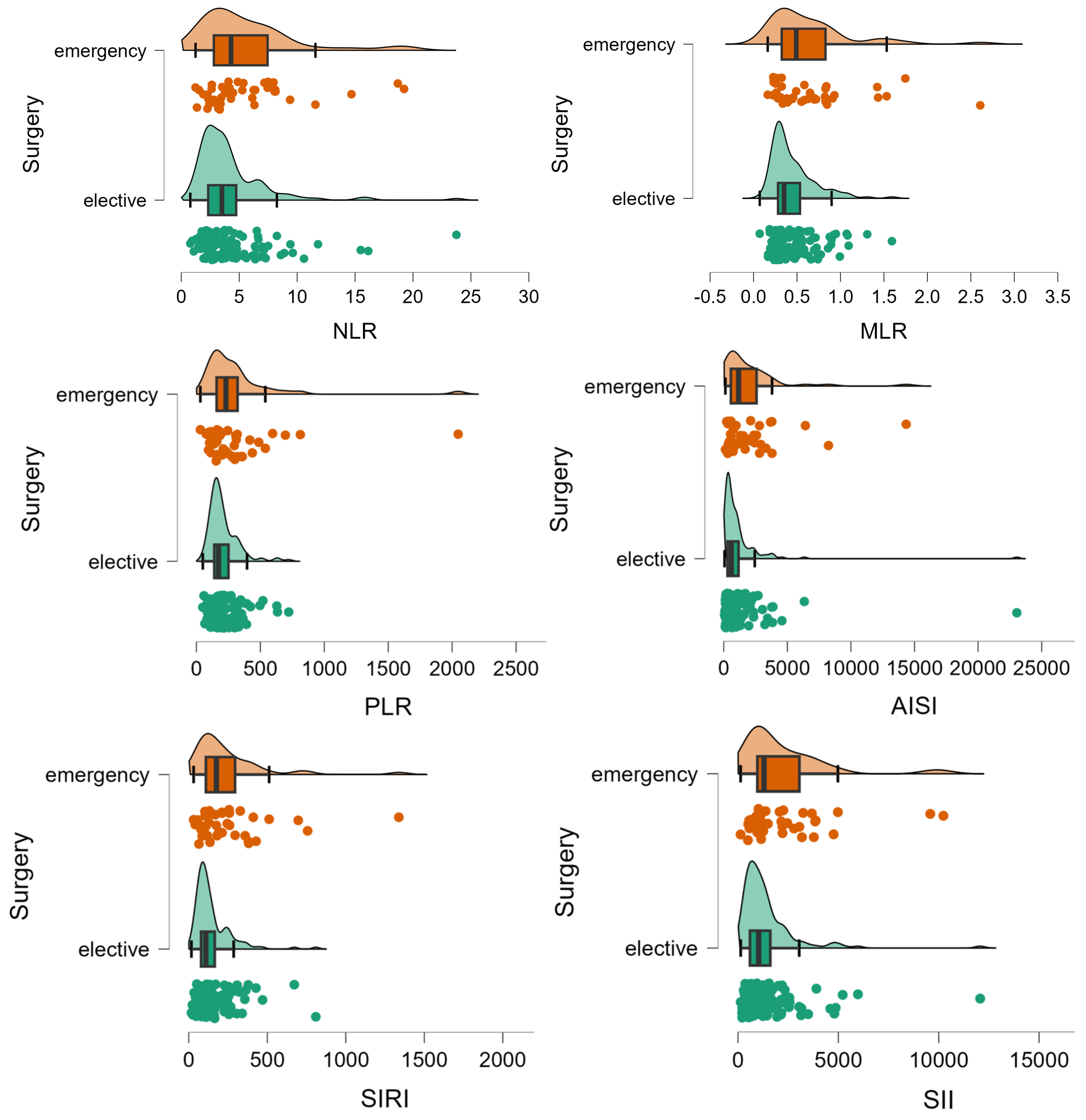
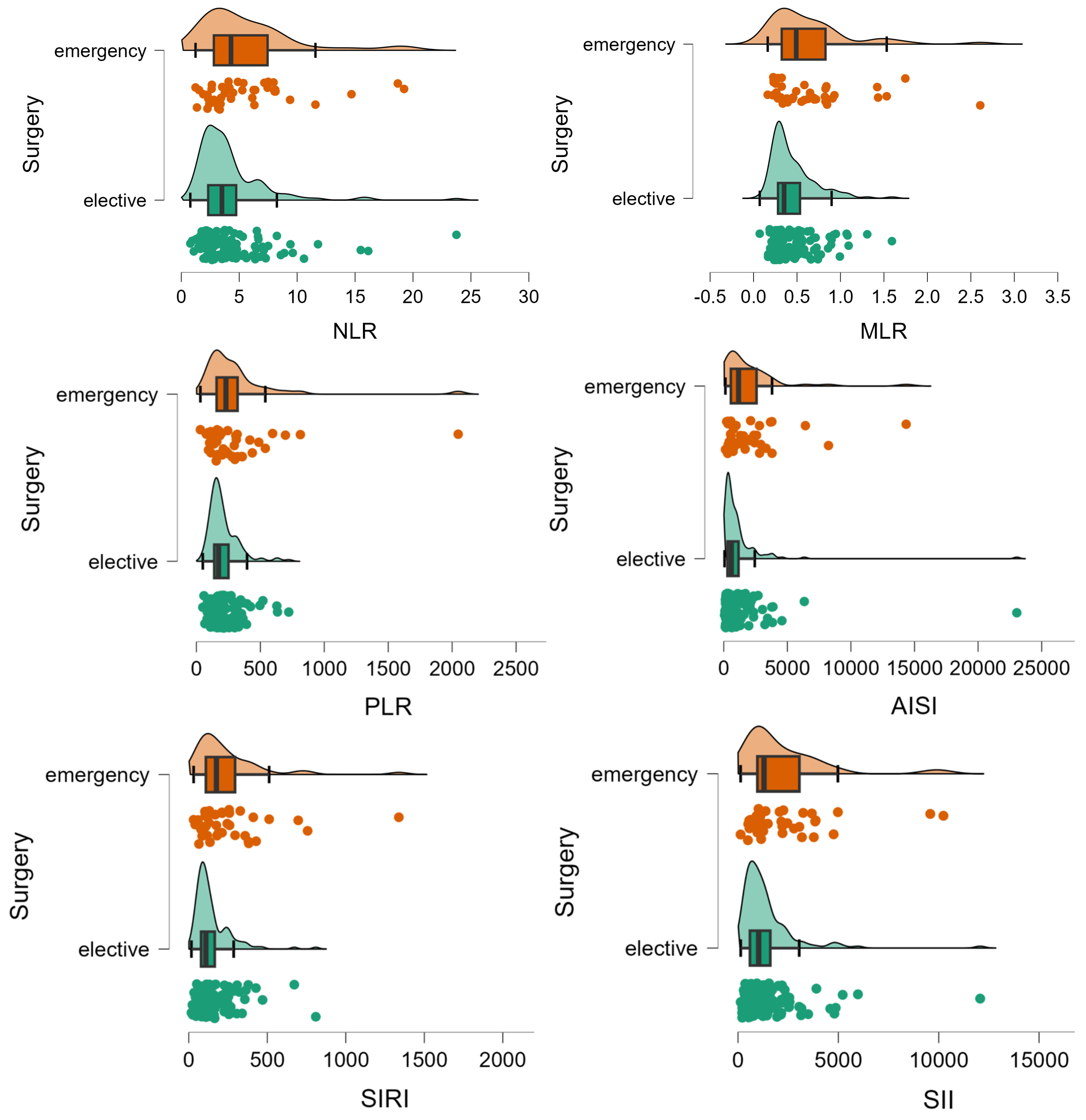
3.2. Elected vs. Emergency Surgery
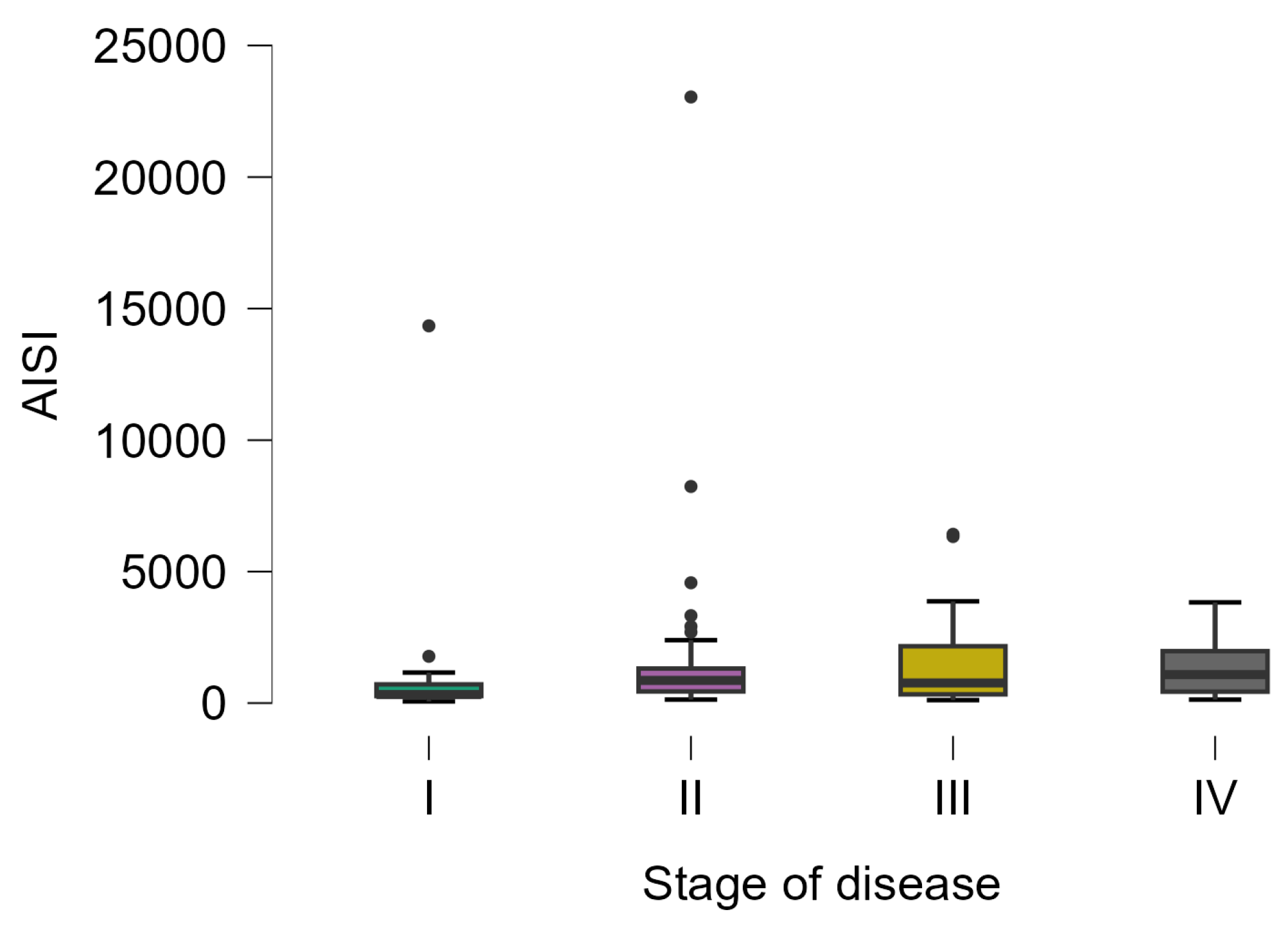
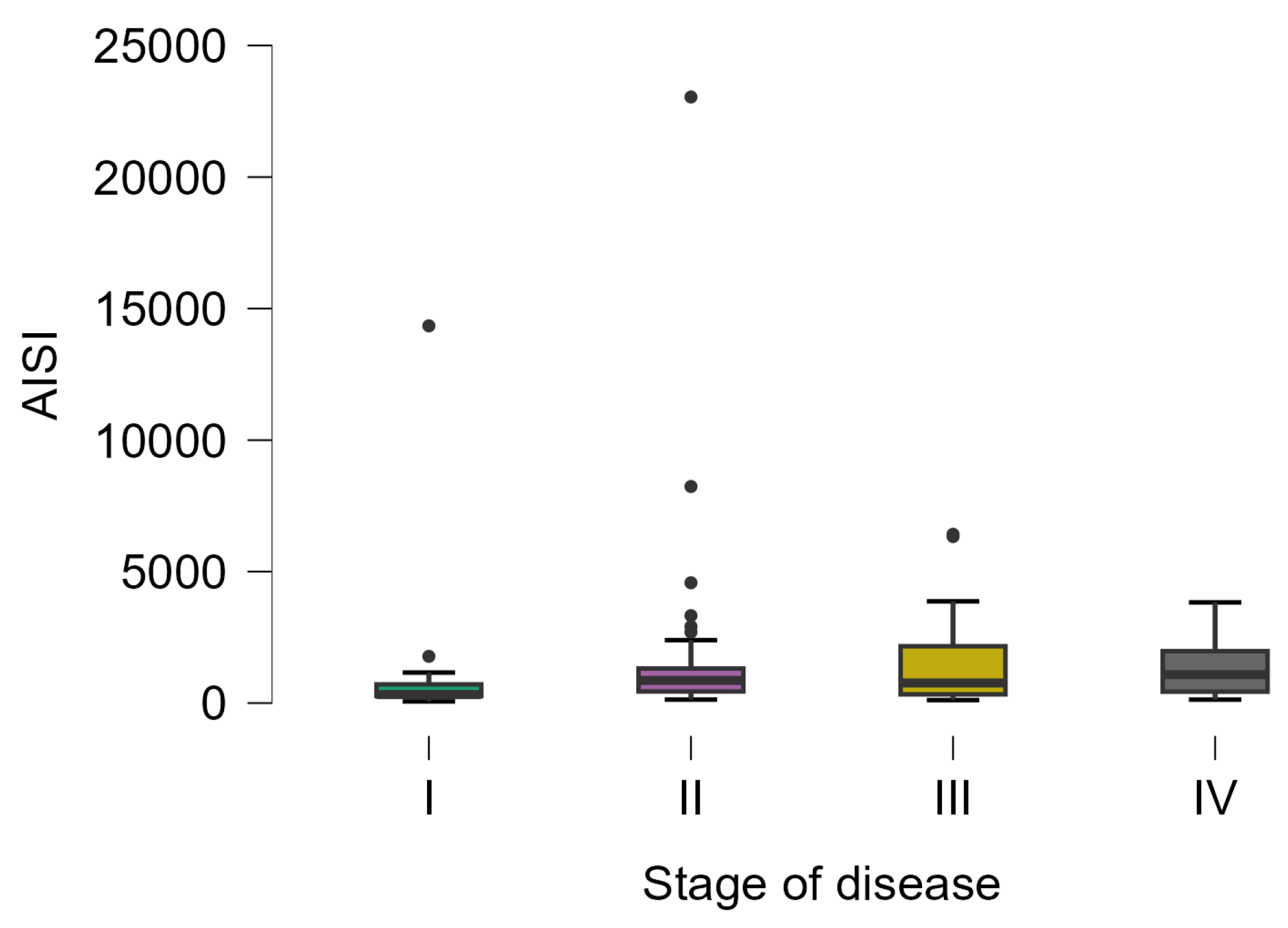
3.3. Stage of the Disease
3.4. Relapse, Early Complications and Post-Surgery Intensive Care Admission
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Altobelli, E.; Rapacchietta, L. Differences in colorectal cancer surveillance epidemiology and screening in the WHO European Region. Oncol. Lett. 2019, 17, 2531–2542. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- Powell, A.G.; Wallace, R.; McKee, R.F.; Anderson, J.H.; Going, J.J.; Edwards, J.; Horgan, P.G. The relationship between tumour site, clinicopathological characteristics and cancer-specific survival in patients undergoing surgery for colorectal cancer. Color. Dis. Off. J. Assoc. Coloproctol. Great Br. Irel. 2012, 14, 1493–1499. [Google Scholar] [CrossRef]
- Walsh, S.R.; Cook, E.J.; Goulder, F.; Justin, T.A.; Keeling, N.J. Neutrophil-lymphocyte ratio as a prognostic factor in colorectal cancer. J. Surg. Oncol. 2005, 91, 181–184. [Google Scholar] [CrossRef]
- Xia, L.J.; Li, W.; Zhai, J.C.; Yan, C.W.; Chen, J.B.; Yang, H. Significance of neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio, lymphocyte-to-monocyte ratio and prognostic nutritional index for predicting clinical outcomes in T1-2 rectal cancer. BMC Cancer 2020, 20, 208. [Google Scholar] [CrossRef] [PubMed]
- Nakamoto, S.; Ohtani, Y.; Sakamoto, I.; Hosoda, A.; Ihara, A.; Naitoh, T. Systemic Immune-Inflammation Index Predicts Tumor Recurrence after Radical Resection for Colorectal Cancer. Tohoku J. Exp. Med. 2023, 261, 229–238. [Google Scholar] [CrossRef]
- Dong, M.; Shi, Y.; Yang, J.; Zhou, Q.; Lian, Y.; Wang, D.; Ma, T.; Zhang, Y.; Mi, Y.; Gu, X.; et al. Prognostic and clinicopathological significance of systemic immune-inflammation index in colorectal cancer: A meta-analysis. Ther. Adv. Med. Oncol. 2020, 12, 1758835920937425. [Google Scholar] [CrossRef]
- Schaue, D.; Micewicz, E.D.; Ratikan, J.A.; Xie, M.W.; Cheng, G.; McBride, W.H. Radiation and inflammation. Semin. Radiat. Oncol. 2015, 25, 4–10. [Google Scholar] [CrossRef]
- Zou, Z.Y.; Liu, H.L.; Ning, N.; Li, S.Y.; Du, X.H.; Li, R. Clinical significance of pre-operative neutrophil lymphocyte ratio and platelet lymphocyte ratio as prognostic factors for patients with colorectal cancer. Oncol. Lett. 2016, 11, 2241–2248. [Google Scholar] [CrossRef]
- Salazar-Onfray, F.; López, M.N.; Mendoza-Naranjo, A. Paradoxical effects of cytokines in tumor immune surveillance and tumor immune escape. Cytokine Growth Factor Rev. 2007, 18, 171–182. [Google Scholar] [CrossRef]
- Porosnicu, T.M.; Sirbu, I.O.; Oancea, C.; Sandesc, D.; Bratosin, F.; Rosca, O.; Jipa, D.; Boeriu, E.; Bandi, S.S.S.; Pricop, M. The Impact of Therapeutic Plasma Exchange on Inflammatory Markers and Acute Phase Reactants in Patients with Severe SARS-CoV-2 Infection. Medicina 2023, 59, 867. [Google Scholar] [CrossRef] [PubMed]
- Tang, G.; Pi, F.; Tao, J.; Wei, Z. Impact of the COVID-19 pandemic on surgical outcomes in patients undergoing colorectal cancer surgery: A retrospective study and meta-analysis of data from 11,082 participants. Front. Public Health 2022, 10, 907571. [Google Scholar] [CrossRef] [PubMed]
- Giuliani, G.; Guerra, F.; Messinese, S.; Santelli, F.; Salvischiani, L.; Esposito, S.; Ferraro, L.; Esposito, A.; De Pastena, M.; Rega, D.; et al. The COVID-AGICT Collaborative group. The COVID-AGICT study: COVID-19 and advanced gastro-intestinal cancer surgical treatment. A multicentric Italian study on the SARS-CoV-2 pandemic impact on gastro-intestinal cancers surgical treatment during the 2020. Analysis of perioperative and short-term oncological outcomes. Surg. Oncol. 2023, 47, 101907. [Google Scholar] [CrossRef] [PubMed]
- Uyan, M.; Özdemir, A.; Kalcan, S.; Tomas, K.; Demiral, G.; Pergel, A.; Tarım, İ.A. Effects of COVID-19 pandemic on colorectal cancer surgery. Sao Paulo Med. J. 2022, 140, 244–249. [Google Scholar] [CrossRef] [PubMed]
- Fericean, R.M.; Rosca, O.; Citu, C.; Manolescu, D.; Bloanca, V.; Toma, A.O.; Boeriu, E.; Dumitru, C.; Ravulapalli, M.; Barbos, V.; et al. COVID-19 Clinical Features and Outcomes in Elderly Patients during Six Pandemic Waves. J. Clin. Med. 2022, 11, 6803. [Google Scholar] [CrossRef]
- Antonucci, F.; Di Carlo, D.; Falcone, M. Evaluation of a potential prognostic parameter for the inflammatory status in COVID-19 patients: The inflammatory protein ratio. Electrophoresis 2022, 43, 1647–1654. [Google Scholar] [CrossRef] [PubMed]
- Grigoras, M.L.; Citu, I.M.; Citu, C.; Chiriac, V.D.; Gorun, F.; Levai, M.C.; Manolescu, D.; Rosca, O.; Bratosin, F.; Gurumurthy, S.; et al. Evaluation of FIB-4, NFS, APRI and Liver Function Tests as Predictors for SARS-CoV-2 Infection in the Elderly Population: A Matched Case-Control Analysis. J. Clin. Med. 2022, 11, 5149. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Colorectal Cancer Mortality Rates in Adults Aged 20 to 54 Years in the United States, 1970-2014. JAMA 2017, 318, 572–574. [Google Scholar] [CrossRef]
- Center, M.M.; Jemal, A.; Smith, R.A.; Ward, E. Worldwide variations in colorectal cancer. CA A Cancer J. Clin. 2009, 59, 366–378. [Google Scholar] [CrossRef] [PubMed]
- Brenner, D.R.; Heer, E.; Sutherland, R.L.; Ruan, Y.; Tinmouth, J.; Heitman, S.J.; Hilsden, R.J. National Trends in Colorectal Cancer Incidence among Older and Younger Adults in Canada. JAMA 2019, 2, e198090. [Google Scholar] [CrossRef] [PubMed]
- Ciocan, A.; Ciocan, R.A.; Al Hajjar, N.; Gherman, C.D.; Bolboacă, S.D. Abilities of Pre-Treatment Inflammation Ratios as Classification or Prediction Models for Patients with Colorectal Cancer. Diagnostics 2021, 11, 566. [Google Scholar] [CrossRef] [PubMed]
- Tonini, V.; Zanni, M. Impact of anastomotic leakage on long-term prognosis after colorectal cancer surgery. World J. Gastrointest. Surg. 2023, 15, 745–756. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Q.L.; Feng, B.; Lu, A.G.; Wang, M.L.; Hu, W.G.; Li, J.W.; Mao, Z.H.; Zheng, M.H. Laparoscopic low anterior resection for rectal carcinoma: Complications and management in 132 consecutive patients. World J. Gastroenterol. 2010, 16, 4605–4610. [Google Scholar] [CrossRef] [PubMed]
- Roxburgh, C.S.; Salmond, J.M.; Horgan, P.G.; Oien, K.A.; McMillan, D.C. Comparison of the prognostic value of inflammation-based pathologic and biochemical criteria in patients undergoing potentially curative resection for colorectal cancer. Ann. Surg. 2009, 249, 788–793. [Google Scholar] [CrossRef] [PubMed]
- Kuper, H.; Adami, H.O.; Trichopoulos, D. Infections as a major preventable cause of human cancer. J. Intern. Med. 2000, 248, 171–183. [Google Scholar] [CrossRef]
- Leitch, E.F.; Chakrabarti, M.; Crozier, J.E.; McKee, R.F.; Anderson, J.H.; Horgan, P.G.; McMillan, D.C. Comparison of the prognostic value of selected markers of the systemic inflammatory response in patients with colorectal cancer. Br. J. Cancer 2007, 97, 1266–1270. [Google Scholar] [CrossRef]
- Kishi, Y.; Kopetz, S.; Chun, Y.S.; Palavecino, M.; Abdalla, E.K.; Vauthey, J.N. Blood neutrophil-to-lymphocyte ratio predicts survival in patients with colorectal liver metastases treated with systemic chemotherapy. Ann. Surg. Oncol. 2009, 16, 614–622. [Google Scholar] [CrossRef]
- Halazun, K.J.; Aldoori, A.; Malik, H.Z.; Al-Mukhtar, A.; Prasad, K.R.; Toogood, G.J.; Lodge, J.P. Elevated preoperative neutrophil to lymphocyte ratio predicts survival following hepatic resection for colorectal liver metastases. Eur. J. Surg. Oncol. 2008, 34, 55–60. [Google Scholar] [CrossRef]
- Absenger, G.; Szkandera, J.; Stotz, M.; Postlmayr, U.; Pichler, M.; Ress, A.L.; Schaberl-Moser, R.; Loibner, H.; Samonigg, H.; Gerger, A. Preoperative neutrophil-to-lymphocyte ratio predicts clinical outcome in patients with stage II and III colon cancer. Anticancer Res. 2013, 33, 4591–4594. [Google Scholar]
- Absenger, G.; Szkandera, J.; Pichler, M.; Stotz, M.; Arminger, F.; Weissmueller, M.; Schaberl-Moser, R.; Samonigg, H.; Stojakovic, T.; Gerger, A. A derived neutrophil to lymphocyte ratio predicts clinical outcome in stage II and III colon cancer patients. Br. J. Cancer 2013, 109, 395–400. [Google Scholar] [CrossRef] [PubMed]
- Kozak, M.M.; von Eyben, R.; Pai, J.S.; Anderson, E.M.; Welton, M.L.; Shelton, A.A.; Kin, C.; Koong, A.C.; Chang, D.T. The Prognostic Significance of Pretreatment Hematologic Parameters in Patients Undergoing Resection for Colorectal Cancer. Am. J. Clin. Oncol. 2017, 40, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Ding, P.R.; An, X.; Zhang, R.X.; Fang, Y.J.; Li, L.R.; Chen, G.; Wu, X.J.; Lu, Z.H.; Lin, J.Z.; Kong, L.H.; et al. Elevated preoperative neutrophil to lymphocyte ratio predicts risk of recurrence following curative resection for stage IIA colon cancer. Int. J. Color. Dis. 2010, 25, 1427–1433. [Google Scholar] [CrossRef] [PubMed]
- Shibutani, M.; Maeda, K.; Nagahara, H.; Noda, E.; Ohtani, H.; Nishiguchi, Y.; Hirakawa, K. A high preoperative neutrophil-to-lymphocyte ratio is associated with poor survival in patients with colorectal cancer. Anticancer Res. 2013, 33, 3291–3294. [Google Scholar]
- Hu, B.; Yang, X.R.; Xu, Y.; Sun, Y.F.; Sun, C.; Guo, W.; Zhang, X.; Wang, W.M.; Qiu, S.J.; Zhou, J.; et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin. Cancer Res. Off. J. Am. Assoc. Cancer Res. 2014, 20, 6212–6222. [Google Scholar] [CrossRef]
- Crusz, S.M.; Balkwill, F.R. Inflammation and cancer: Advances and new agents. Nature reviews. Clin. Oncol. 2015, 12, 584–596. [Google Scholar] [CrossRef]
- Li, Y.; Jia, H.; Yu, W.; Xu, Y.; Li, X.; Li, Q.; Cai, S. Nomograms for predicting prognostic value of inflammatory biomarkers in colorectal cancer patients after radical resection. Int. J. Cancer 2016, 139, 220–231. [Google Scholar] [CrossRef] [PubMed]
- Turri, G.; Barresi, V.; Valdegamberi, A.; Gecchele, G.; Conti, C.; Ammendola, S.; Guglielmi, A.; Scarpa, A.; Pedrazzani, C. Clinical Significance of Preoperative Inflammatory Markers in Prediction of Prognosis in Node-Negative Colon Cancer: Correlation between Neutrophil-to-Lymphocyte Ratio and Poorly Differentiated Clusters. Biomedicines 2021, 9, 94. [Google Scholar] [CrossRef]
- Özgehan, G.; Kahramanca, Ş.; Kaya, İ.O.; Bilgen, K.; Bostanci, H.; Güzel, H.; Küçükpinar, T.; Kargici, H. Neutrophil-lymphocyte ratio as a predictive factor for tumor staging in colorectal cancer. Turk. J. Med. Sci. 2014, 44, 365–368. [Google Scholar] [CrossRef]
- Basile, D.; Garattini, S.K.; Corvaja, C.; Montico, M.; Cortiula, F.; Pelizzari, G.; Gerratana, L.; Audisio, M.; Lisanti, C.; Fanotto, V.; et al. The MIMIC Study: Prognostic Role and Cutoff Definition of Monocyte-to-Lymphocyte Ratio and Lactate Dehydrogenase Levels in Metastatic Colorectal Cancer. Oncologist 2020, 25, 661–668. [Google Scholar] [CrossRef]
- Josse, J.M.; Cleghorn, M.C.; Ramji, K.M.; Jiang, H.; Elnahas, A.; Jackson, T.D.; Okrainec, A.; Quereshy, F.A. The neutrophil-to-lymphocyte ratio predicts major perioperative complications in patients undergoing colorectal surgery. Color. Dis. Off. J. Assoc. Coloproctol. Great Br. Irel. 2016, 18, O236–O242. [Google Scholar] [CrossRef]
- Chen, X.Q.; Xue, C.R.; Hou, P.; Lin, B.Q.; Zhang, J.R. Lymphocyte-to-monocyte ratio effectively predicts survival outcome of patients with obstructive colorectal cancer. World J. Gastroenterol. 2019, 25, 4970–4984. [Google Scholar] [CrossRef]
- Palin, R.P.; Devine, A.T.; Hicks, G.; Burke, D. Association of pretreatment neutrophil-lymphocyte ratio and outcome in emergency colorectal cancer care. Ann. R. Coll. Surg. Engl. 2018, 100, 308–315. [Google Scholar] [CrossRef]
- Farolfi, A.; Petrone, M.; Scarpi, E.; Gallà, V.; Greco, F.; Casanova, C.; Longo, L.; Cormio, G.; Orditura, M.; Bologna, A.; et al. Inflammatory Indexes as Prognostic and Predictive Factors in Ovarian Cancer Treated with Chemotherapy Alone or Together with Bevacizumab. A Multicenter, Retrospective Analysis by the MITO Group (MITO 24). Target. Oncol. 2018, 13, 469–479. [Google Scholar] [CrossRef] [PubMed]
- Stotz, M.; Pichler, M.; Absenger, G.; Szkandera, J.; Arminger, F.; Schaberl-Moser, R.; Samonigg, H.; Stojakovic, T.; Gerger, A. The preoperative lymphocyte to monocyte ratio predicts clinical outcome in patients with stage III colon cancer. Br. J. Cancer 2014, 110, 435–440. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.Z.; Chen, W.J.; Zhang, X.; Wu, C.C.; Zhang, C.Y.; Sun, S.S.; Wu, J. An Elevated Platelet-to-Lymphocyte Ratio Predicts Poor Prognosis and Clinicopathological Characteristics in Patients with Colorectal Cancer: A Meta-Analysis. Dis. Markers 2017, 2017, 1053125. [Google Scholar] [CrossRef] [PubMed]
- Chen, J.H.; Zhai, E.T.; Yuan, Y.J.; Wu, K.M.; Xu, J.B.; Peng, J.J.; Chen, C.Q.; He, Y.L.; Cai, S.R. Systemic immune-inflammation index for predicting prognosis of colorectal cancer. World J. Gastroenterol. 2017, 23, 6261–6272. [Google Scholar] [CrossRef] [PubMed]
- Xie, Q.K.; Chen, P.; Hu, W.M.; Sun, P.; He, W.Z.; Jiang, C.; Kong, P.F.; Liu, S.S.; Chen, H.T.; Yang, Y.Z.; et al. The systemic immune-inflammation index is an independent predictor of survival for metastatic colorectal cancer and its association with the lymphocytic response to the tumor. J. Transl. Med. 2018, 16, 273. [Google Scholar] [CrossRef] [PubMed]
- Ferrone, C.; Dranoff, G. Dual roles for immunity in gastrointestinal cancers. J. Clin. Oncol. Off. J. Am. Soc. Clin. Oncol. 2010, 28, 4045–4051. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | All, n = 282 | Dead, n = 35 | Alive, n = 247 | Stat. (p-Value) |
|---|---|---|---|---|
| Age, years a | 68 [60 to 74], 282 | 73 [66 to 78], 35 | 67 [59 to 73], 247 | 2.86 (0.0042) |
| Sex, men b | 148 (52.5) | 23 (65.7) | 125 (50.6) | 2.81 (0.0939) |
| Rural b | 99 (35.2) | 11 (31.4) | 88 (35.8) | 0.25 (0.6147) |
| CHARLSON > 3 b | 111 (39.4) | 24 (68.6) | 87 (35.2) | 14.28 (0.0002) |
| Emergency b | 135 (47.9) | 30 (85.7) | 105 (42.5) | 22.93 (<0.0001) |
| Curative surgery b | 232 (82.3) | 24 (68.6) | 208 (84.2) | 5.14 (0.0234) |
| Localization b | n.a. (0.15406) | |||
| Right | 83 (29.4) | 13 (37.1) | 70 (28.3) | |
| Left | 162 (57.4) | 17 (48.6) | 145 (58.7) | |
| Transverse | 26 (9.2) | 1 (2.9) | 25 (10.1) | |
| Relapse b | 27 (9.6) | 2 (5.7) | 25 (10.1) | n.a. (0.3188) |
| Complications b | 16 (5.7) | 9 (25.7) | 7 (2.8) | 29.99 (<0.0001) |
| Postop ICU b | 35 (12.4) | 22 (62.9) | 13 (5.3) | 93.54 (<0.0001) |
| Stage | n.a. (0.0571) | |||
| I | 23 (8.2) | 0 (0) | 23 (9.3) | |
| II | 87 (30.9) | 8 (22.9) | 79 (32) | |
| III | 110 (39) | 13 (37.1) | 97 (39.3) | |
| IV | 42 (14.9) | 9 (25.7) | 33 (13.4) | |
| Lymphatic invasion b | 128 (49) | 18 (60) | 110 (47.6) | 1.63 (0.2019) |
| pT b | n.a. (0.2893) | |||
| 1 | 8 (3.1) | 0 (0) | 8 (3.5) | |
| 2 | 18 (7) | 1 (3.4) | 17 (7.5) | |
| 3 | 123 (48) | 11 (37.9) | 112 (49.3) | |
| 4 | 107 (41.8) | 17 (58.6) | 90 (39.6) | |
| pN b | 1.62 (0.4443) | |||
| 0 | 117 (45.9) | 11 (37.9) | 106 (46.9) | |
| 1 | 74 (29) | 8 (27.6) | 66 (29.2) | |
| 2 | 64 (25.1) | 10 (34.5) | 54 (23.9) | |
| pM b | 40 (15.4) | 8 (26.7) | 32 (13.9) | 3.32 (0.0686) |
| Hospitalization, days a | 13 [10 to 17], 282 | 9 [3 to 19.5], 35 | 13 [10 to 17], 247 | −2.74 (0.0062) |
| Post-surgery, days a | 10 [8 to 14], 282 | 6 [2 to 18], 35 | 10 [8 to 13], 247 | −2.58 (0.0099) |
| Marker | All, n = 282 | Dead, n = 35 | Alive, n = 247 | Stat. (p-Value) |
|---|---|---|---|---|
| Lymphocytes | 1600 [1212.5 to 2100], 282 | 1420 [795 to 1930], 35 | 1600 [1290 to 2100], 247 | −1.99 (0.0461) |
| Monocytes | 425 [200 to 720], 282 | 300 [200 to 905], 35 | 450 [300 to 700], 247 | −1.32 (0.1883) |
| Platelets | 303,800 [242,000 to 384,000], 282 | 306,000 [202,000 to 407,000], 35 | 303,600 [245,000 to 383,000], 247 | −0.34 (0.7331) |
| Neutrophils | 5760 [4380 to 7830], 165 | 7180 [5720 to 10,500], 13 | 5605 [4100 to 7697.5], 152 | 2.32 (0.0202) |
| NLR | 3.63 [2.41 to 5.44], 165 | 4.47 [3.39 to 11.58], 13 | 3.57 [2.355 to 5.3225], 152 | 1.73 (0.0837) |
| MLR | 0.28 [0.15 to 0.47], 282 | 0.25 [0.129 to 0.5515], 35 | 0.281 [0.159 to 0.4495], 247 | −0.39 (0.6934) |
| PLR | 185.5 [137 to 279.25], 282 | 250 [134.5 to 332], 35 | 183 [137 to 257.5], 247 | 1.56 (0.1182) |
| AISI | 765 [332 to 1546], 165 | 2162 [1082 to 3233], 13 | 646.5 [329.75 to 1325.75], 152 | 3.19 (0.0014) |
| SIRI | 83 [44 to 139], 281 | 72 [32.75 to 205.75], 34 | 83 [46 to 132.5], 247 | −0.18 (0.8606) |
| SII | 1070 [645 to 2009], 165 | 2140 [1065 to 3868], 13 | 1061.5 [612.75 to 1754.5], 152 | 2.33 (0.0197) |
| Marker | Emergency Surgery, n = 135 | Elected Surgery, n = 147 | Stat. (p-Value) |
|---|---|---|---|
| Lymphocytes | 1570 [1055 to 2120], 135 | 1650 [1310 to 2055], 147 | −1.29 (0.1986) |
| Monocytes | 300 [200 to 595], 135 | 550 [400 to 790], 147 | −6.00 (<0.0001) |
| Platelets | 310,000 [239,500 to 381,500], 135 | 300,000 [247,000 to 384,000], 147 | 0.22 (0.8225) |
| Neutrophils | 6840 [5000 to 8680], 41 | 5525 [4087.5 to 7440], 124 | 2.25 (0.0243) |
| NLR | 4.29 [2.8 to 7.5], 41 | 3.51 [2.3 to 4.7], 124 | 2.26 (0.0237) |
| MLR | 0.182 [0.1 to 0.3], 135 | 0.319 [0.2 to 0.5], 147 | −5.16 (<0.0004) |
| PLR | 197 [135 to 298], 135 | 175 [138 to 248], 147 | 3.15 (0.0016) |
| AISI | 1165 [559 to 2580], 41 | 599.5 [293.5 to 1162.3], 124 | −4.05 (0.0001) |
| SIRI | 59.5 [34 to 118], 134 | 96 [61 to 155], 147 | −4.05 (0.0001) |
| SII | 1297 [966 to 3058], 41 | 1030 [594.8 to 1609.5], 124 | 2.72 (0.0064) |
| Ratio | Regional Stage of Disease | No-Regional Stage of Disease | Stat. (p-Value) |
|---|---|---|---|
| NLR | 3.83 [3.13 to 6.31], 53 | 3.19 [2.18 to 4.52], 99 | 2.98 (0.0029) |
| PLR | 215 [144.5 to 305], 107 | 170.5 [128 to 232], 150 | 2.64 (0.0084) |
| AISI | 1082 [506 to 2373], 53 | 570 [287 to 1082], 99 | 3.68 (0.0002) |
| SII | 1449.5 [990.25 to 2360.25], 52 | 966 [543.5 to 1492.5], 99 | 3.55 (0.0004) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Feier, C.V.I.; Muntean, C.; Bolboacă, S.D.; Olariu, S. Exploratory Evaluation of Pre-Treatment Inflammation Profiles in Patients with Colorectal Cancer. Diseases 2024, 12, 61. https://doi.org/10.3390/diseases12030061
Feier CVI, Muntean C, Bolboacă SD, Olariu S. Exploratory Evaluation of Pre-Treatment Inflammation Profiles in Patients with Colorectal Cancer. Diseases. 2024; 12(3):61. https://doi.org/10.3390/diseases12030061
Chicago/Turabian StyleFeier, Catalin Vladut Ionut, Calin Muntean, Sorana D. Bolboacă, and Sorin Olariu. 2024. "Exploratory Evaluation of Pre-Treatment Inflammation Profiles in Patients with Colorectal Cancer" Diseases 12, no. 3: 61. https://doi.org/10.3390/diseases12030061
APA StyleFeier, C. V. I., Muntean, C., Bolboacă, S. D., & Olariu, S. (2024). Exploratory Evaluation of Pre-Treatment Inflammation Profiles in Patients with Colorectal Cancer. Diseases, 12(3), 61. https://doi.org/10.3390/diseases12030061