

Papillary Thyroid Cancer Trends in the Wake of the COVID-19 Pandemic: Is There a Shift toward a More Aggressive Entity?

Abstract
1. Background
2. Materials and Methods
2.1. Surgical Technique
2.2. Data Acquisition
2.3. Study Groups
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Medas, F.; Ansaldo, G.L.; Avenia, N.; Basili, G.; Bononi, M.; Bove, A.; Carcoforo, P.; Casaril, A.; Cavallaro, G.; Conzo, G.; et al. Impact of the COVID-19 pandemic on surgery for thyroid cancer in Italy: Nationwide retrospective study. Br. J. Surg. 2021, 108, e166–e167. [Google Scholar] [CrossRef] [PubMed]
- Ito, Y.; Miyauchi, A.; Inoue, H.; Fukushima, M.; Kihara, M.; Higashiyama, T.; Tomoda, C.; Takamura, Y.; Kobayashi, K.; Miya, A. An observational trial for papillary thyroid microcarcinoma in Japanese patients. World J. Surg. 2010, 34, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Horn-Ross, P.L.; Lichtensztajn, D.Y.; Clarke, C.A.; Dosiou, C.; Oakley-Girvan, I.; Reynolds, P.; Gomez, S.L.; Nelson, D.O. Continued rapid increase in thyroid cancer incidence in california: Trends by patient, tumor, and neighborhood characteristics. Cancer Epidemiol. Biomark. Prev. 2014, 23, 1067–1079. [Google Scholar] [CrossRef]
- Pellegriti, G.; Frasca, F.; Regalbuto, C.; Squatrito, S.; Vigneri, R. Worldwide increasing incidence of thyroid cancer: Update on epidemiology and risk factors. J. Cancer Epidemiol. 2013, 2013, 965212. [Google Scholar] [CrossRef] [PubMed]
- Lim, H.; Devesa, S.S.; Sosa, J.A.; Check, D.; Kitahara, C.M. Trends in thyroid cancer incidence and mortality in the United States, 1974–2013. JAMA 2017, 317, 1338–1348. [Google Scholar] [CrossRef]
- Liu, W.; Jiang, B.; Xue, J.; Liu, R.; Wei, Y.; Li, P. Clinicopathological features of differentiated thyroid carcinoma as predictors of the effects of radioactive iodine therapy. Ann. Diagn. Pathol. 2023, 69, 152243. [Google Scholar] [CrossRef]
- Smulever, A.; Pitoia, F. Thirty years of active surveillance for low-risk thyroid cancer, lessons learned and future directions. Rev. Endocr. Metab. Disord. 2024, 25, 65–78. [Google Scholar] [CrossRef]
- Popa, O.; Barna, R.A.; Borlea, A.; Cornianu, M.; Dema, A.; Stoian, D. The impact of the COVID-19 pandemic on thyroid nodular disease: A retrospective study in a single center in the western part of Romania. Front. Endocrinol. 2023, 14, 1221795. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Yuan, I.J.; Mirshahidi, S.; Simental, A.; Lee, S.C.; Yuan, X. Thyroid Carcinoma: Phenotypic Features, Underlying Biology and Potential Relevance for Targeting Therapy. Int. J. Mol. Sci. 2021, 22, 1950. [Google Scholar] [CrossRef]
- Barron, E.; Bakhsh, M.; Gul, R. The impact of delays to surgery due to the COVID-19 pandemic on prognosis for patients with operable breast cancer. Eur. J. Surg. Oncol. 2020, 46, 1522–1527. [Google Scholar] [CrossRef]
- Giannoula, E.; Iakovou, I.; Giovanella, L.; Vrachimis, A. Updated clinical management guidance during the COVID-19 pandemic: Thyroid nodules and cancer. Eur. J. Endocrinol. 2022, 186, G1–G7. [Google Scholar] [CrossRef] [PubMed]
- Giusti, M.; Aragona, G.; Elefante, G.M.; Faggiano, A.; Grimaldi, F.; Leccisotti, L.; Ronga, G. Thyroid cancer management during COVID-19 pandemic: A multidisciplinary position statement. Cancer Treat. Res. Commun. 2021, 27, 100320. [Google Scholar] [CrossRef]
- Gorini, F.; Bianchi, F.; Giovannetti, L.; Del Rio, P.; Ferroli, P. COVID-19 and neurosurgical oncology: A review of the literature and future perspectives. Cancer Treat. Res. Commun. 2021, 27, 100352. [Google Scholar] [CrossRef]
- Johnson, B.A.; Waddimba, A.C.; Ogola, G.O.; Fleshman, J.W., Jr.; Preskitt, J.T. A systematic review and meta-analysis of surgery delays and survival in breast, lung and colon cancers: Implication for surgical triage during the COVID-19 pandemic. Am. J. Surg. 2021, 222, 311–318. [Google Scholar] [CrossRef] [PubMed]
- Qu, N.; Hui, Z.; Shen, Z.; Kan, C.; Hou, N.; Sun, X.; Han, F. Thyroid Cancer and COVID-19: Prospects for Therapeutic Approaches and Drug Development. Front. Endocrinol. 2022, 13, 873027. [Google Scholar] [CrossRef] [PubMed]
- Naguib, R. Potential relationships between COVID-19 and the thyroid gland: An update. J. Int. Med. Res. 2022, 50, 03000605221082898. [Google Scholar] [CrossRef] [PubMed]
- Sperlongano, P.; Parmeggiani, D.; Pisaniello, D.; De Falco, M.; Sordelli, I.; Accardo, M.; Cuccurullo, V.; Mansi, L.; Tartaro, G.P.; Barbarisi, A. Surgical treatment of differentiated thyroid carcinoma: A retrospective study. Front. Biosci.-Landmark 2006, 11, 2206–2212. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Cai, Z.; Lu, C.; He, J.; Liu, L.; Zou, Y.; Zhang, Z.; Zhu, Z.; Ge, X.; Wu, A.; Jiang, T.; et al. Identification and characterization of circRNAs encoded by MERS-CoV, SARS-CoV-1 and SARS-CoV-2. Brief. Bioinform. 2021, 22, 1297–1308. [Google Scholar] [CrossRef]
- Jahankhani, K.; Ahangari, F.; Adcock, I.M.; Mortaz, E. Possible cancer-causing capacity of COVID-19: Is COVID-19 an oncogenic agent? Biochimie 2023, 213, 130–138. [Google Scholar] [CrossRef]
- Alseddeeqi, E.; Altinoz, A.; Oulhaj, A.; Suliman, A.; Ahmed, L.A. Incidence of thyroid cancer in Abu Dhabi, UAE: A registry-based study. J. Cancer Res. Ther. 2023, 19, 321–326. [Google Scholar] [CrossRef]
- Hassan, I.; Hassan, L.; Gamal, I.; Ibrahim, M.; Omer, A.R. Abu Dhabi Neural mapping (ADNM) during minimally invasive thyroidectomy enables the early identification of non-recurrent laryngeal nerve and prevents voice dysfunction. J. Clin. Med. 2022, 11, 5677. [Google Scholar] [CrossRef]
- Kathuria-Prakash, N.; Mosaferi, T.; Xie, M.; Antrim, L.; Angell, T.E.; In, G.K.; Bajwa, J.; Ghazinian, R.; Livhits, M.J.; Zeltsman, M.; et al. COVID-19 outcomes of patients with differentiated thyroid cancer: A multicenter Los Angeles cohort study. Endocr. Pract. 2021, 27, 90–94. [Google Scholar] [CrossRef]
- Kim, S.H.; Min, E.; Hwang, Y.M.; Choi, Y.S.; Yi, J.W. Impact of COVID-19 pandemic on thyroid surgery in a university hospital in South Korea. Cancers 2022, 14, 4338. [Google Scholar] [CrossRef]
- Lai, A.G.; Pasea, L.; Banerjee, A.; Hall, G.; Denaxas, S.; Chang, W.H.; Katsoulis, M.; Williams, B.; Pillay, D.; Noursadeghi, M.; et al. Estimated impact of the COVID-19 pandemic on cancer services and excess 1-year mortality in people with cancer and multimorbidity: Near real-time data on cancer care, cancer deaths, and a population-based cohort study. BMJ Open 2020, 10, e043828. [Google Scholar] [CrossRef]
- Shaha, A.R. Thyroid surgery during COVID-19 pandemic: Principles and philosophies. Head Neck 2020, 42, 1322. [Google Scholar] [CrossRef]
- Tsang, V.H.; Gild, M.; Glover, A.; Clifton-Bligh, R.; Robinson, B.G. Thyroid cancer in the age of COVID-19. Endocr.-Relat. Cancer 2020, 27, R407–R416. [Google Scholar] [CrossRef]
- Sawka, A.M.; Ghai, S.; Ihekire, O.; Jones, J.M.; Gafni, A.; Baxter, N.N.; Goldstein, D.P.; on behalf of the Canadian Thyroid Cancer Active Surveillance Study Group. Decision-making in surgery or active surveillance for low risk papillary thyroid cancer during the COVID-19 pandemic. Cancers 2021, 13, 371. [Google Scholar] [CrossRef]
- Nickel, B.; Glover, A.; Miller, J.A. Delays to Low-risk Thyroid Cancer Treatment During COVID-19—Refocusing From What Has Been Lost to What May Be Learned and Gained. JAMA Otolaryngol.-Head Neck Surg. 2021, 147, 5–6. [Google Scholar] [CrossRef]
- Almansoori, A.; Hamoudi, R.; Busch, H.; Bendardaf, R. Thyroid cancer incidence in the United Arab Emirates: A retrospective study on association with age and gender. F1000Research 2022, 11, 338. [Google Scholar] [CrossRef]
- Morris, L.G.; Sikora, A.G.; Tosteson, T.D.; Davies, L. The increasing incidence of thyroid cancer: The influence of access to care. Thyroid 2013, 23, 885–891. [Google Scholar] [CrossRef]
- Liu, H.; Zhan, L.; Guo, L.; Yu, X.; Li, L.; Feng, H.; Yang, D.; Xu, Z.; Tu, Y.; Chen, C.; et al. More aggressive cancer behaviour in thyroid cancer patients in the post-COVID-19 pandemic era: A retrospective study. Int. J. Gen. Med. 2021, 14, 7197–7206. [Google Scholar] [CrossRef]
- Durante, C.; Haddy, N.; Baudin, E.; Leboulleux, S.; Hartl, D.; Travagli, J.P.; Caillou, B.; Ricard, M.; Lumbroso, J.D.; De Vathaire, F.; et al. Long-term outcome of 444 patients with distant metastases from papillary and follicular thyroid carcinoma: Benefits and limits of radioiodine therapy. J. Clin. Endocr. Metab. 2006, 91, 2892–2899. [Google Scholar] [CrossRef]
- Ling, Y.; Xiong, X.; Luo, J.; Zou, Q.; Chen, P.; Pan, L.; Long, M.; Feng, H.; Ouyang, W. The efficacy and safety in radioactive iodine refractory thyroid cancer patients treated with sorafenib. Front. Endocrinol. 2023, 14, 1200932. [Google Scholar] [CrossRef]
- Cho, S.W.; Choi, H.S.; Yeom, G.J.; Lim, J.A.; Moon, J.H.; Park, D.J.; Chung, J.-K.; Cho, B.Y.; Yi, K.H.; Park, Y.J. Long-term prognosis of differentiated thyroid cancer with lung metastasis in Korea and its prognostic factors. Thyroid 2014, 24, 277–286. [Google Scholar] [CrossRef]
- Graves, C.E.; Goyal, N.; Levin, A.; Nuño, M.A.; Kim, J.; Campbell, M.J.; Shen, W.T.; Gosnell, J.E.; Roman, S.A.; Sosa, J.A.; et al. Anxiety during the COVID-19 pandemic: A web-based survey of thyroid cancer survivors. Endocr. Pract. 2022, 28, 405–413. [Google Scholar] [CrossRef]
- Falcone, R.; Grani, G.; Ramundo, V.; Melcarne, R.; Giacomelli, L.; Filetti, S.; Durante, C. Cancer care during COVID-19 era: The quality of life of patients with thyroid malignancies. Front. Oncol. 2020, 10, 1128. [Google Scholar] [CrossRef]
- Alhamlan, F.S.; Alfageeh, M.B.; Al Mushait, M.A.; Al-Badawi, I.A.; Al-Ahdal, M.N. Human Papillomavirus-Associated Cancers. In Advances in Experimental Medicine and Biology; Springer: Cham, Switzerland, 2021; Volume 1313, pp. 1–14. [Google Scholar] [CrossRef]
- Klain, M.; Nappi, C.; Maurea, S.; De Risi, M.; Volpe, F.; Caiazzo, E.; Piscopo, L.; Manganelli, M.; Schlumberger, M.; Cuocolo, A. Management of differentiated thyroid cancer through nuclear medicine facilities during COVID-19 emergency: The telemedicine challenge. Eur. J. Nucl. Med. Mol. Imaging 2021, 48, 831–836. [Google Scholar] [CrossRef]
- Bueno, F.; Abelleira, E.; Von Stecher, F.; Paes de Lima, A.; Pitoia, F. Dramatic clinical response to dabrafenib plus trametinib in anaplastic thyroid carcinoma and the challenges faced during the COVID-19 pandemic. Arch. Endocrinol. Metab. 2021, 65, 242–247. [Google Scholar] [CrossRef]
- Vlad, M.; Corlan, A.; Balas, M.; Golu, I.; Amzar, D.; Bistrian, E.; Cornianu, M. Collision tumor of the thyroid—A challenge during the COVID-19 pandemic. Arch. Clin. Cases 2021, 8, 64. [Google Scholar] [CrossRef]
- Grani, G.; Ciotti, L.; Del Gatto, V.; Montesano, T.; Biffoni, M.; Giacomelli, L.; Sponziello, M.; Pecce, V.; Verrienti, A.; Filetti, S.; et al. The legacy of the COVID-19 pandemics for thyroid cancer patients: Towards the application of clinical practice recommendations. Endocrine 2023, 79, 45–48. [Google Scholar] [CrossRef]
- Deligiorgi, M.V.; Siasos, G.; Vakkas, L.; Trafalis, D.T. Charting the unknown association of COVID-19 with thyroid cancer, focusing on differentiated thyroid cancer: A call for caution. Cancers 2021, 13, 5785. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Pre-Pandemic | Post-Pandemic | Total | p-Value | |
|---|---|---|---|---|
| Gender, female/male (n) | 90/21 | 142/40 | 232/61 | 0.532 |
| Age in years | 39.1 | 40.1 | 0.669 | |
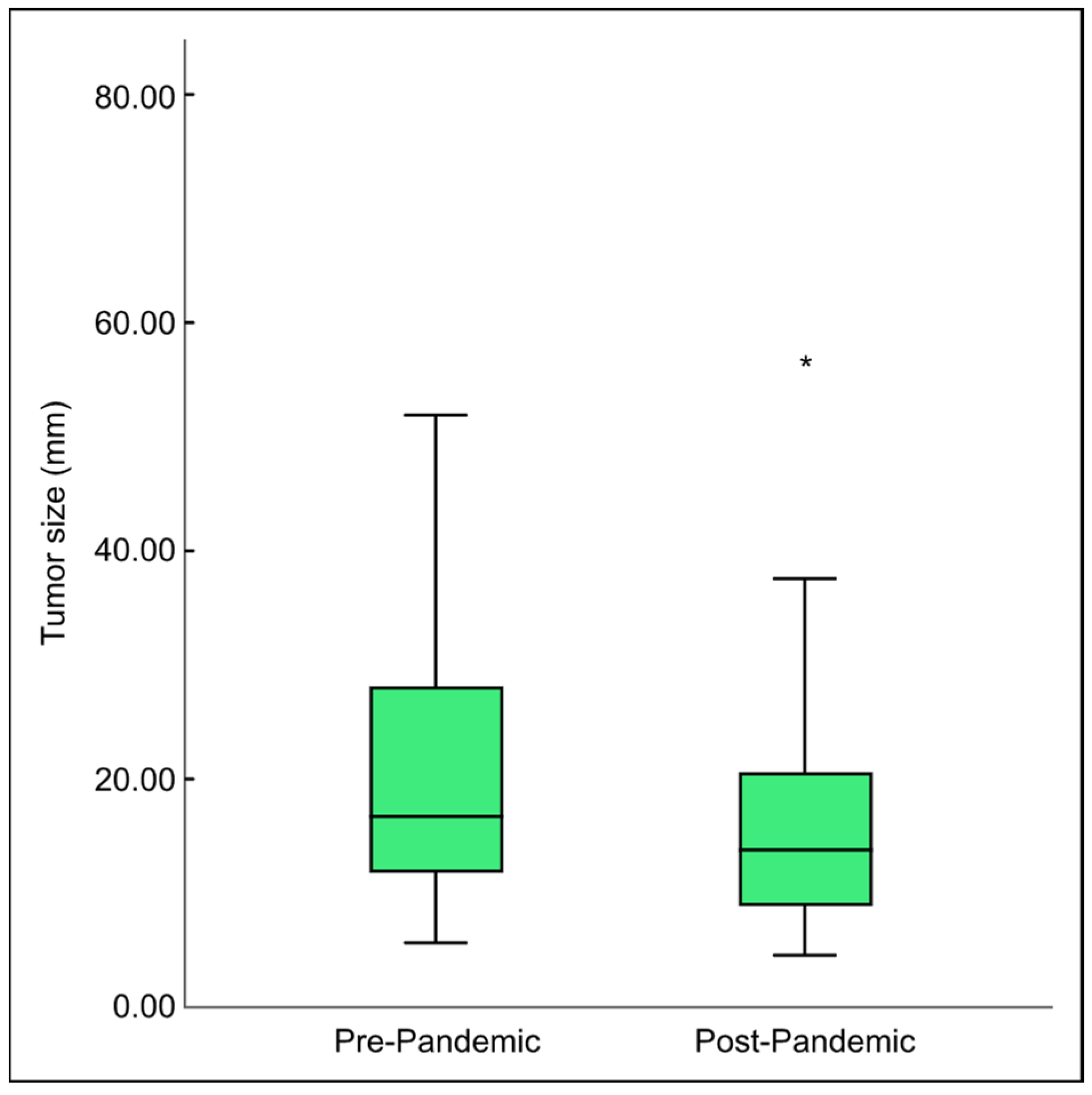
| Median tumor size in mm | 18.1 ▪ | 13.1 | 0.001 | |
| Multifocality unilateral/bilateral (n) | 99/12 | 123/59 † | 222/71 | 0.001 |
| Noninvasive (n) | 89 | 133 | 222 | 0.232 |
| Capsule–vascular invasion (n) | 22 | 49 † | 71 | 0.001 |
| Lobectomy/total thyroidectomy | 20/91 | 39/143 * | 59/234 | 0.001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hassan, I.; Hassan, L.; Bacha, F.; Al Salameh, M.; Gatee, O.; Hassan, W. Papillary Thyroid Cancer Trends in the Wake of the COVID-19 Pandemic: Is There a Shift toward a More Aggressive Entity? Diseases 2024, 12, 62. https://doi.org/10.3390/diseases12030062
Hassan I, Hassan L, Bacha F, Al Salameh M, Gatee O, Hassan W. Papillary Thyroid Cancer Trends in the Wake of the COVID-19 Pandemic: Is There a Shift toward a More Aggressive Entity? Diseases. 2024; 12(3):62. https://doi.org/10.3390/diseases12030062
Chicago/Turabian StyleHassan, Iyad, Lina Hassan, Farooq Bacha, Mohammad Al Salameh, Omran Gatee, and Wiam Hassan. 2024. "Papillary Thyroid Cancer Trends in the Wake of the COVID-19 Pandemic: Is There a Shift toward a More Aggressive Entity?" Diseases 12, no. 3: 62. https://doi.org/10.3390/diseases12030062
APA StyleHassan, I., Hassan, L., Bacha, F., Al Salameh, M., Gatee, O., & Hassan, W. (2024). Papillary Thyroid Cancer Trends in the Wake of the COVID-19 Pandemic: Is There a Shift toward a More Aggressive Entity? Diseases, 12(3), 62. https://doi.org/10.3390/diseases12030062