
Effectiveness of mHealth Interventions in Medication Adherence among Patients with Cardiovascular Diseases: A Systematic Review
 , and
, and 
Abstract
1. Introduction
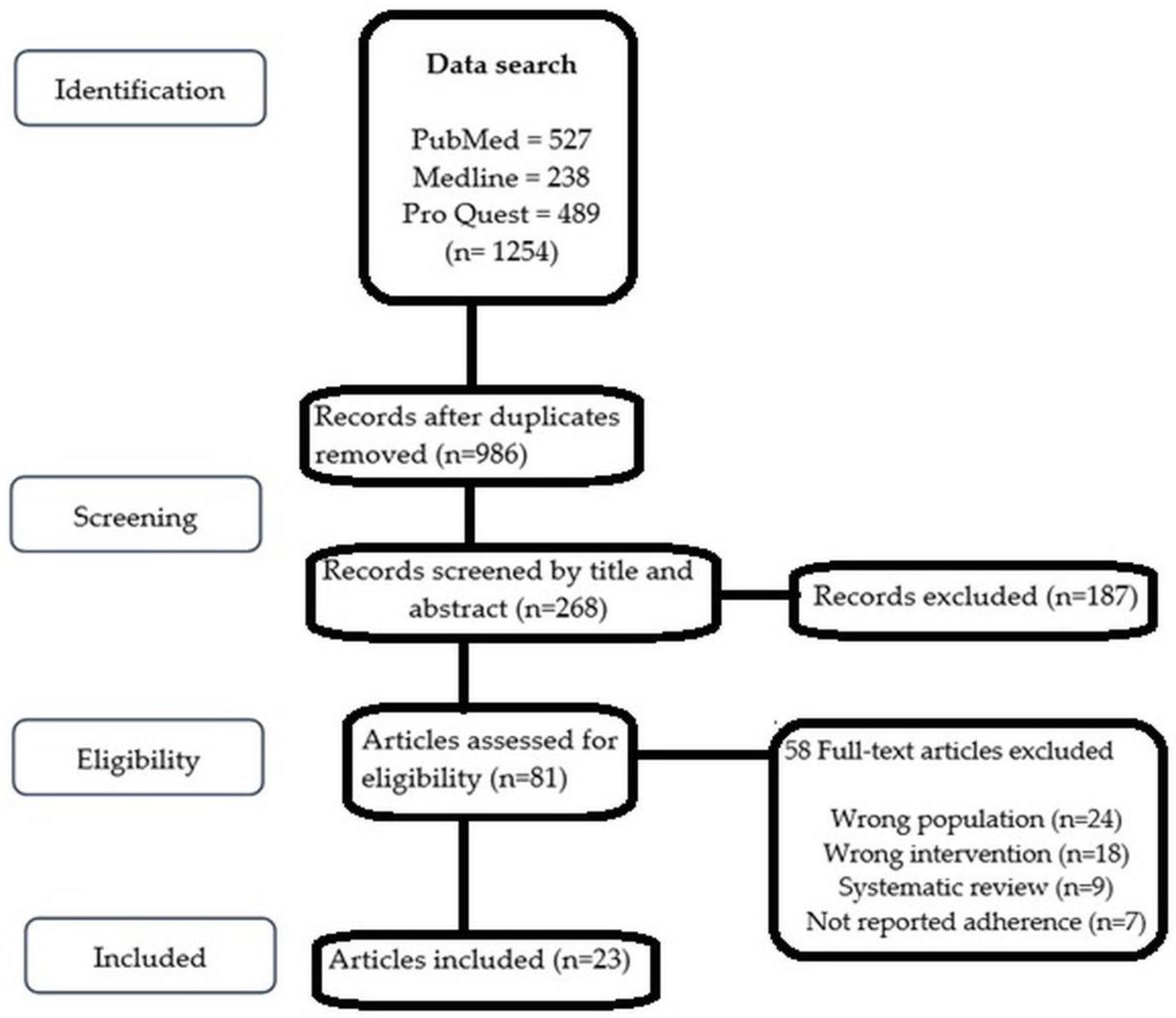
2. Materials and Methods
2.1. Search Criteria
2.2. Inclusion and Exclusion Criteria
2.3. Search Strategy
2.4. Quality Evaluation
3. Result
3.1. Characteristics of Trials
3.2. Types of Intervention
3.3. Outcome Measures
3.4. Medication Adherence
3.5. Hypertension
3.6. Ischemic Heart Disease
3.7. Heart Failure
3.8. Stroke
3.9. Diabetes Mellitus
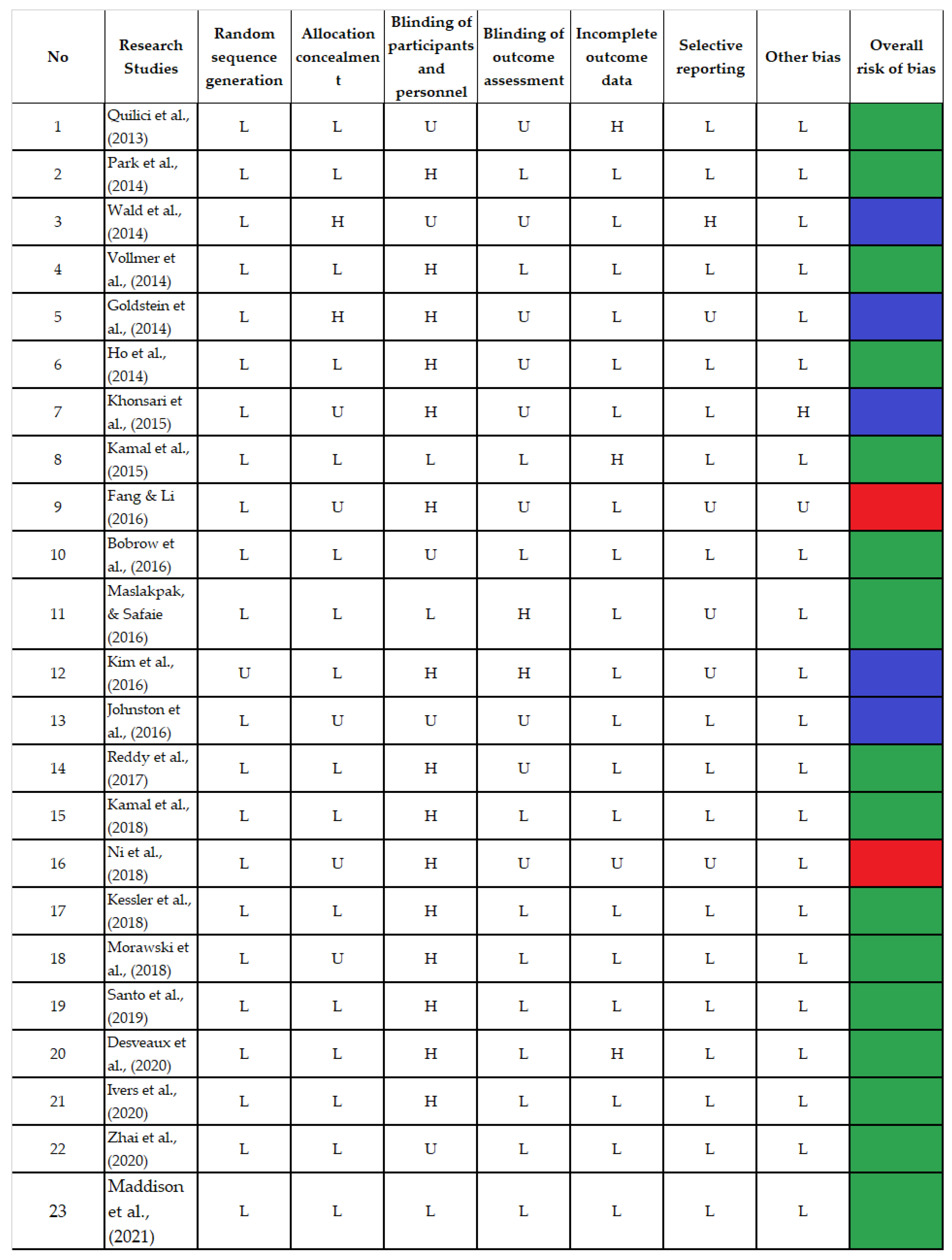
3.10. Risk of Bias and Methodological Quality Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Roth, G.A.; Johnson, C.; Abajobir, A.; Abd-Allah, F.; Abera, S.F.; Abyu, G.; Ahmed, M.; Aksut, B.; Alam, T.; Alam, K.; et al. Global, Regional, and National Burden of Cardiovascular Diseases for 10 Causes, 1990 to 2015. J. Am. Coll. Cardiol. 2017, 70, 1–25. [Google Scholar] [CrossRef]
- Abbafati, C.; Machado, D.B.; Cislaghi, B.; Salman, O.M.; Karanikolos, M.; McKee, M.; Abbas, K.M.; Brady, O.J.; Larson, H.J.; Trias-Llimós, S.; et al. Global burden of 369 diseases and injuries in 204 countries and territories, 1990-2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar]
- Mensah, G.A.; Roth, G.A.; Fuster, V. The Global Burden of Cardiovascular Diseases and Risk Factors: 2020 and Beyond. J. Am. Coll. Cardiol. 2019, 74, 2529–2532. [Google Scholar] [CrossRef]
- Zhu, Z.; Liu, Y.; Zhang, C.; Yuan, Z.; Zhang, Q.; Tang, F.; Lin, H.; Zhang, Y.; Liu, L.; Xue, F. Identification of Cardiovascular Risk Components in Urban Chinese with Metabolic Syndrome and Application to Coronary Heart Disease Prediction: A Longitudinal Study. Han W, editor. PLoS ONE 2013, 8, e84204. [Google Scholar] [CrossRef]
- Peters, S.; Wang, X.; Lam, T.H.; Kim, H.C.; Suzanne Asia Pacific Cohort Studies Collaboration; Ninomiya, T.; Knuiman, M.; Vaartjes, I.; Bots, M.L.; Woodward, M. Clustering of risk factors and the risk of incident cardiovascular disease in Asian and Caucasian populations: Results from the Asia Pacific Cohort Studies Collaboration. BMJ Open 2018, 8, e019335. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.; Murray, L.; Donnelly, M. Systematic review protocol of interventions to improve the psychological well-being of general practitioners. Syst. Rev. 2015, 4, 117. [Google Scholar] [CrossRef]
- Conn, V.S.; Ruppar, T.M. Medication adherence outcomes of 771 intervention trials: Systematic review and meta-analysis. Prev. Med. 2017, 99, 269–276. [Google Scholar] [CrossRef]
- Kini, V.; Ho, P.M. Interventions to Improve Medication Adherence: A Review. JAMA. 2018, 320, 2461–2473. [Google Scholar] [CrossRef] [PubMed]
- Sieben, A.; Bredie, S.J.H.B.; van Laarhoven, C.J.H.M.K.; Schoonhoven, L.; Burger, D.M.; van Onzenoort, H.A.W. e-Health interventions and improvement in treatment adherence. Ned. Tijdschr. Geneeskd. 2014, 158, A8460. [Google Scholar]
- Wilhelmsen, N.C.; Eriksson, T. Medication adherence interventions and outcomes: An overview of systematic reviews. Eur. J. Hosp. Pharm. Sci. Pract. 2019, 26, 187–192. [Google Scholar] [CrossRef] [PubMed]
- Kolandaivelu, K.; Leiden, B.B.; O’Gara, P.T.; Bhatt, D.L. Non-adherence to cardiovascular medications. Eur. Heart J. 2014, 35, 3267–3276. [Google Scholar] [CrossRef]
- Kumar, S.; Nilsen, W.J.; Abernethy, A.; Atienza, A.; Patrick, K.; Pavel, M.; Riley, W.T.; Shar, A.; Spring, B.; Spruijt-Metz, D.; et al. Mobile health technology evaluation: The mHealth evidence workshop. Am. J. Prev. Med. 2013, 45, 228–236. [Google Scholar] [CrossRef]
- Burke, L.E.; Ma, J.; Azar, K.M.; Bennett, G.G.; Peterson, E.D.; Zheng, Y.; Riley, W.; Stephens, J.; Shah, S.H.; Suffoletto, B.; et al. Current science on consumer use of mobile health for cardiovascular disease prevention: A scientific statement from the American Heart Association. Circulation 2015, 132, 1157–1213. [Google Scholar] [CrossRef]
- Adler, A.J.; Martin, N.; Mariani, J.; Tajer, C.D.; Owolabi, O.O.; Free, C.; Serrano, N.C.; Casas, J.P.; Perel, P. Mobile phone text messaging to improve medication adherence in secondary prevention of cardiovascular disease. Cochrane Database Syst. Rev. 2017, 4, CD011851. [Google Scholar] [CrossRef] [PubMed]
- Marcolino, M.S.; Oliveira, J.A.Q.; D’Agostino, M.; Ribeiro, A.L.; Alkmim, M.B.M.; Novillo-Ortiz, D. The Impact of mHealth Interventions: Systematic Review of Systematic Reviews. JMIR mHealth uHealth 2018, 6, e8873. [Google Scholar] [CrossRef] [PubMed]
- Quilici, J.; Fugon, L.; Beguin, S.; Morange, P.E.; Bonnet, J.-L.; Alessi, M.-C.; Carrieri, P.; Cuisset, T. Effect of motivational mobile phone short message service on aspirin adherence after coronary stenting for acute coronary syndrome. Int. J. Cardiol. 2013, 168, 568–569. [Google Scholar] [CrossRef]
- Park, L.G.; Howie-Esquivel, J.; Chung, M.L.; Dracup, K. A text messaging intervention to promote medication adherence for patients with coronary heart disease: A randomized controlled trial. Patient Educ. Couns. 2014, 94, 261–268. [Google Scholar] [CrossRef] [PubMed]
- Wald, D.S.; Bestwick, J.P.; Raiman, L.; Brendell, R.; Wald, N.J. Randomised Trial of Text Messaging on Adherence to Cardiovascular Preventive Treatment (INTERACT Trial). PLoS ONE 2014, 9, e114268. [Google Scholar] [CrossRef]
- Vollmer, W.M.; Owen-Smith, A.A.; O Tom, J.; Laws, R.; Ditmer, D.G.; Smith, D.H.; Waterbury, A.C.; Schneider, J.L.; Yonehara, C.H.; Williams, A.; et al. Improving adherence to cardiovascular disease medications with information technology. Am. J. Manag. Care 2014, 20, SP502. [Google Scholar]
- Goldstein, C.M.; Gathright, E.C.; Dolansky, A.M.; Gunstad, J.; Sterns, A.; Redle, J.D.; Josephson, R.; Hughes, J.W. Randomized controlled feasibility trial of two telemedicine medication reminder systems for older adults with heart failure. J. Telemed. Telecare. 2014, 20, 293–299. [Google Scholar] [CrossRef]
- Ho, P.M.; Lambert-Kerzner, A.; Carey, E.P.; Fahdi, I.E.; Bryson, C.L.; Melnyk, S.D.; Bosworth, H.B.; Radcliff, T.; Davis, R.; Mun, H.; et al. Multifaceted intervention to improve medication adherence and secondary prevention measures after acute coronary syndrome hospital discharge: A randomized clinical trial. JAMA Intern. Med. 2014, 174, 186–193. [Google Scholar] [CrossRef]
- Khonsari, S.; Subramanian, P.; Chinna, K.; Latif, L.A.; Ling, L.W.; Gholami, O. Effect of a reminder system using an automated short message service on medication adherence following acute coronary syndrome. Eur. J. Cardiovasc. Nurs. 2015, 14, 170–179. [Google Scholar] [CrossRef] [PubMed]
- Kamal, A.K.; Shaikh, Q.; Pasha, O.; Azam, I.; Islam, M.; Memon, A.A.; Rehman, H.; Akram, M.A.; Affan, M.; Nazir, S.; et al. A randomized controlled behavioral intervention trial to improve medication adherence in adult stroke patients with prescription tailored Short Messaging Service (SMS)-SMS4Stroke study. BMC Neurol. 2015, 15, 212. [Google Scholar] [CrossRef] [PubMed]
- Fang, R.; Li, X. Electronic messaging support service programs improve adherence to lipid-lowering therapy among outpatients with coronary artery disease: An exploratory randomised control study. J. Clin. Nurs. 2016, 25, 664–671. [Google Scholar] [CrossRef] [PubMed]
- Bobrow, K.; Farmer, A.J.; Springer, D.; Shanyinde, M.; Yu, L.M.; Brennan, T.; Rayner, B.; Namane, M.; Steyn, K.; Tarassenko, L.; et al. Mobile Phone Text Messages to Support Treatment Adherence in Adults with High Blood Pressure (SMS-Text Adherence Support [StAR]): A Single-Blind, Randomized Trial. Circulation 2016, 133, 592–600. [Google Scholar] [CrossRef]
- Maslakpak, M.H.; Safaie, M. A Comparison between The Effectiveness of Short Message Service and Reminder Cards Regarding Medication Adherence in Patients with Hypertension: A Randomized Controlled Clinical Trial. Int. J. Community Based Nurs. Midwifery 2016, 4, 209. [Google Scholar]
- Kim, J.Y.; Wineinger, N.E.; Steinhubl, S.R. The Influence of Wireless Self-Monitoring Program on the Relationship Between Patient Activation and Health Behaviors, Medication Adherence, and Blood Pressure Levels in Hypertensive Patients: A Substudy of a Randomized Controlled Trial. J. Med. Internet Res. 2016, 18, e116. [Google Scholar] [CrossRef]
- Johnston, N.; Bodegard, J.; Jerström, S.; Åkesson, J.; Brorsson, H.; Alfredsson, J.; Albertsson, P.A.; Karlsson, J.-E.; Varenhorst, C. Effects of interactive patient smartphone support app on drug adherence and lifestyle changes in myocardial infarction patients: A randomized study. Am. Heart J. 2016, 178, 85–94. [Google Scholar] [CrossRef]
- Reddy, A.; Huseman, T.L.; Canamucio, A.; Marcus, S.C.; Asch, D.A.; Volpp, K.; Long, J.A. Patient and Partner Feedback Reports to Improve Statin Medication Adherence: A Randomized Control Trial. J. Gen. Intern. Med. 2017, 32, 256–261. [Google Scholar] [CrossRef]
- Kamal, A.K.; Khalid, W.; Muqeet, A.; Jamil, A.; Farhat, K.; Gillani, S.R.A.; Zulfiqar, M.; Saif, M.; Muhammad, A.A.; Zaidi, F.; et al. Making prescriptions “talk” to stroke and heart attack survivors to improve adherence: Results of a randomized clinical trial (The Talking Rx Study). PLoS ONE 2018, 13, e0197671. [Google Scholar] [CrossRef]
- Ni, Z.; Liu, C.; Wu, B.; Yang, Q.; Douglas, C.; Shaw, R.J. An mHealth intervention to improve medication adherence among patients with coronary heart disease in China: Development of an intervention. Int. J. Nurs. Sci. 2018, 5, 322–330. [Google Scholar] [CrossRef]
- Kessler, J.B.; Troxel, A.B.; Asch, D.A.; Mehta, S.J.; Marcus, N.; Lim, R.; Zhu, J.; Shrank, W.; Brennan, T.; Volpp, K.G. Partners and Alerts in Medication Adherence: A Randomized Clinical Trial. J. Gen. Intern. Med. 2018, 33, 1536–1542. [Google Scholar] [CrossRef] [PubMed]
- Morawski, K.; Ghazinouri, R.; Krumme, A.; Lauffenburger, J.C.; Lu, Z.; Durfee, E.; Oley, L.; Lee, J.; Mohta, N.; Haff, N.; et al. Association of a Smartphone Application With Medication Adherence and Blood Pressure Control: The MedISAFE-BP Randomized Clinical Trial. JAMA Intern. Med. 2018, 178, 802–809. [Google Scholar] [CrossRef] [PubMed]
- Santo, K.; Singleton, A.; Chow, C.K.; Redfern, J. Evaluating Reach, Acceptability, Utility, and Engagement with An App-Based Intervention to Improve Medication Adherence in Patients with Coronary Heart Disease in the MedApp-CHD Study: A Mixed-Methods Evaluation. Med. Sci. 2019, 7, 68. [Google Scholar] [CrossRef]
- Desveaux, L.; Saragosa, M.; Russell, K.; McCleary, N.; Presseau, J.; Witteman, H.O.; Schwalm, J.D.; Ivers, N.M. How and why a multifaceted intervention to improve adherence post-MI worked for some (and could work better for others): An outcome-driven qualitative process evaluation. BMJ Open 2020, 10, e036750. [Google Scholar] [CrossRef] [PubMed]
- Ivers, N.M.; Schwalm, J.D.; Bouck, Z.; McCready, T.; Taljaard, M.; Grace, S.L.; Cunningham, J.; Bosiak, B.; Presseau, J.; Witteman, H.O.; et al. Interventions supporting long term adherence and decreasing cardiovascular events after myocardial infarction (ISLAND): Pragmatic randomised controlled trial. BMJ 2020, 369, m1731. [Google Scholar] [CrossRef]
- Zhai, P.; Hayat, K.; Ji, W.; Li, Q.; Shi, L.; Atif, N.; Xu, S.; Li, P.; Du, Q.; Fang, Y. Efficacy of text messaging and personal consultation by pharmacy students among adults with hypertension: Randomized controlled trial. J. Med. Internet Res. 2020, 22, e16019. [Google Scholar] [CrossRef]
- Maddison, R.; Jiang, Y.; Stewart, R.; Scott, T.; Kerr, A.; Whittaker, R.; Benatar, J.; Rolleston, A.; Estabrooks, P.; Dale, L. An intervention to improve medication adherence in people with heart disease (text4heartii): Randomized controlled trial. JMIR mHealth uHealth. 2021, 9, e24952. [Google Scholar] [CrossRef]
- Klimis, H.; Thakkar, J.; Chow, C.K. Breaking Barriers: Mobile Health Interventions for Cardiovascular Disease. Can. J. Cardiol. 2018, 34, 905–913. [Google Scholar] [CrossRef]
- Andre, N.; Wibawanti, R.; Siswanto, B.B. Mobile Phone-Based Intervention in Hypertension Management. Int. J. Hypertens. 2019, 2019, 9021017. [Google Scholar] [CrossRef]
- Gandapur, Y.; Kianoush, S.; Kelli, H.M.; Misra, S.; Urrea, B.; Blaha, M.J.; Graham, G.; Marvel, F.A.; Martin, S.S. The role of mHealth for improving medication adherence in patients with cardiovascular disease: A systematic review. Eur. Hear. J. Qual. Care Clin. Outcomes 2016, 2, 237–244. [Google Scholar] [CrossRef] [PubMed]
- Bond, Z.; Scanlon, T.; Judah, G. Systematic Review of RCTs Assessing the Effectiveness of mHealth Interventions to Improve Statin Medication Adherence: Using the Behaviour-Change Technique Taxonomy to Identify the Techniques That Improve Adherence. Healthcare 2021, 9, 1282. [Google Scholar] [CrossRef]
- Gandhi, S.; Chen, S.; Hong, L.; Sun, K.; Gong, E.; Li, C.; Yan, L.L.; Schwalm, J.-D. Effect of Mobile Health Interventions on the Secondary Prevention of Cardiovascular Disease: Systematic Review and Meta-analysis. Can. J. Cardiol. 2017, 33, 219–231. [Google Scholar] [CrossRef] [PubMed]
- Thakkar, J.; Kurup, R.; Laba, T.L.; Santo, K.; Thiagalingam, A.; Rodgers, A.; Woodward, M.; Redfern, J.; Chow, C.K. Mobile Telephone Text Messaging for Medication Adherence in Chronic Disease: A Meta-analysis. JAMA Intern Med. 2016, 176, 340–349. [Google Scholar] [CrossRef]
- Al-Arkee, S.; Mason, J.; A Lane, D.; Fabritz, L.; Chua, W.; Haque, M.S.; Jalal, Z. Mobile Apps to Improve Medication Adherence in Cardiovascular Disease: Systematic Review and Meta-analysis. J. Med. Internet Res. 2021, 23, e24190. [Google Scholar] [CrossRef]
- Kassavou, A.; Sutton, S. Automated telecommunication interventions to promote adherence to cardio-metabolic medications: Meta-analysis of effectiveness and meta-regression of behaviour change techniques. Health Psychol. Rev. 2018, 12, 25–42. [Google Scholar] [CrossRef]
- Pfaeffli Dale, L.; Dobson, R.; Whittaker, R.; Maddison, R. The effectiveness of mobile-health behaviour change interventions for cardiovascular disease self-management: A systematic review. Eur. J. Prev. Cardiol. 2016, 23, 801–817. [Google Scholar] [CrossRef]
- van Driel, M.L.; Morledge, M.D.; Ulep, R.; Shaffer, J.P.; Davies, P.; Deichmann, R. Interventions to improve adherence to lipid-lowering medication. Cochrane Database Syst. Rev. 2016, 12, CD004371. [Google Scholar]
- Thirumurthy, H.; Jakubowski, A.; Camlin, C.; Kabami, J.; Ssemmondo, E.; Elly, A.; Mwai, D.; Clark, T.; Cohen, C.; Bukusi, E.; et al. Expectations about future health and longevity in Kenyan and Ugandan communities receiving a universal test-and-treat intervention in the SEARCH trial. AIDS Care 2016, 28 (Suppl. S3), 90–98. [Google Scholar] [CrossRef] [PubMed]
- Sailer, F.; Pobiruchin, M.; Wiesner, M.; Meixner, G. An Approach to Improve Medication Adherence by Smart Watches. In Digital Healthcare Empowering Europeans; MIE; IOS Press: Amsterdam, The Netherlands, 2015. [Google Scholar]
- Keil, A.; Gegier, K.; Pobiruchin, M.; Wiesner, M. A Smartwatch-Driven Medication Management System Compliant to the German Medication Plan. Stud. Health Technol. Inform. 2016, 228, 185–189. [Google Scholar]
- Wang, H.; Naghavi, M.; Allen, C.; Barber, R.; Bhutta, Z.; Carter, A.; Casey, D.; Charlson, F.; Chen, A.Z.; Coates, M.; et al. Global, regional, and national life expectancy, all-cause mortality, and cause-specific mortality for 249 causes of death, 1980–2015: A systematic analysis for the Global Burden of Disease Study 2015. Lancet 2016, 388, 1459–1544. Available online: http://www.thelancet.com/journals/lancet/article/PIIS0140-6736(16)31012-1/abstract#.WtGaUq8NnO4.mendeley (accessed on 13 October 2022). [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| No. | Authors | Study Design | Country | Population | Adherence Measurement | Study Intervention | Outcomes | Findings | |
|---|---|---|---|---|---|---|---|---|---|
| Primary | Secondary | ||||||||
| 1 | Quilici et al. (2013) [16] | RCT (1 month) | France | n = 5546 ACS patients after PCI on aspirin medication | AA-Ag | Two-arm trial: Arm-1: daily SMS reminders for aspirin-adherence in intervention arm; Arm-2: control (no intervention) | Adherence | Not mentioned | Adherence to aspirin improved in the intervention arm with SMS reminders with an odds ratio of 0.37 to 0.02. |
| 2 | Park et al. (2014) [17] | RCT (1 month) | USA (Northern California) | n = 90 ACS patients | 1—MMAS-8 2—SEAMS 3—MEMS | Three-arm trial: Arm-1: reminder text messages for medication; Arm-2: rext messages for education; Arm-3: control (no intervention) | Adherence | Patient feasibility and satisfaction with the text messages | Text messaging intervention improved adherence. Patients with text message interventions showed a higher percentage of accurate doses (p = 0.02), percentage of doses taken (p = 0.01), and percentage of prescribed doses taken on time (p = 0.01). Antiplatelet response rates were higher than statin response rates (p = 0.005) as per the schedule. |
| 3 | Wald et al. (2014) [18] | RCT (6 months) | UK (London) | n = 301 Patients on AHT + lipid-lowering medication | 1—Personal inquiry for medication adherence 2—Electronic records for drug prescription | Two arm trial: Arm-1: text messaging intervention for reminders to take medication; Arm-2: control (no intervention) | Adherence | Blood pressure and serum cholesterol | Adherence significantly improved compared to the control group. Non-adherence to medication was lower among the text messaging group (14/150 (9%)) than in the control group (38/151 (25%)). No statistically significant differences in blood pressure were found. |
| 4 | Vollmer et al. (2014) [19] | RCT (12 months) | USA (Northwest, Hawaii, and Georgia) | n = 21,752 CAD patients with type 2 diabetes (suboptimal adherence to medication) | Modified version of the PDC | Three-arm trial: Arm-1: phone calls (interactive voice); Arm-2: interactive voice-recognition-enhanced phone calls; Arm-3: control (no intervention) | Adherence | Blood pressure and lipid levels | Adherence significantly improved in both intervention groups. Both intervention groups showed 2.2 percentage points higher than the control group with odds ratios of 1.16 and 1.14 higher in the first and second intervention groups than the control. |
| 5 | Goldstein et al. (2014) [20] | RCT (28 days) | USA (Ohio) | n = 60 Patients with CF | Pillbox bin openings were used for the telehealth intervention group and electronic self-reporting for people with them—health intervention | Four-arm factorial feasibility trial: two arms with pillbox silent, pillbox reminding; and two arms with smartphone silent, smartphone reminding | Adherence | Acceptance of model | No improvement in adherence. The total adherence rate was 78% (SD 35), with the telehealth device adhering 80% of the time and people with a smartphone adhering 76% of the time; reminders adhered 79% of the time while reminding did not improve adherence. |
| 6 | Ho et al. (2014) [21] | RCT (12 months) | USA (Colorado, Washington, North Carolina, and Arkansas | n = 253 ACS/MI patients | PDC > 0.8 | Two-arm trial: Arm-1: multifaceted intervention, medication reconciliation and tailoring, patient education, collaborative care between a pharmacist and a patient’s primary care clinician, and voice messaging; Arm-2: control | Adherence | Blood pressure (BP) and low-density lipoprotein cholesterol (LDL-C) | Adherence improved. The intervention group showed 89.3% adherent patients vs. 73.9% in the usual care group (p = 0.003). In addition, the intervention arm had a greater mean proportion of days covered, with 0.94 vs. 0.87 (p = 0.001). No significant decrease in systolic blood pressure was found. |
| 7 | Khonsari et al. (2015) [22] | RCT (2 months) | Malaysia | n = 62 ACS patients | MMAS-8 | Two-arm trial: Arm-1: automated SMS reminders; Arm-2: control (no intervention) | Adherence | Heart functional status | Adherence was found to improve by (χ(2) (2) = 18.614, and heart functional status was also improved. |
| 8 | Kamal et al. (2015) [23] | RCT (3 months) | Pakistan | n = 200 Post-stroke patients treated for high blood pressure | MMAS-4 | Two-arm trial: Arm-I: SMS for reminders to take medication; Arm-2: control (no intervention) | Adherence | DBP | Adherence improved by 7.4 in the intervention group and 6.7 in the control group, while the mean diastolic blood pressure in the intervention group was 2.6 mmHg lower vs. the control group. |
| 9 | Fang and Li (2016) [24] | RCT (6 months) | China | n = 280 CAD patients post-angiography /CT | MMAS-8 | Three-arm trial: Arm-1: utilized SMS; Arm-2: utilized SMS + Micro Letter, Arm-3: control with the phone only | Adherence | Not mentioned | Improved adherence (improved score not mentioned). |
| 10 | Bobrow et al. (2016) [25] | RCT (12 months) | South Africa | n = 1372 Hypertensive patients | Proportion of days calculated + EuroQol Group 5-Dimension Self-Report Questionnaire | Three-arm trial: Arm-1: text message reminders for medication adherence; Arm-2: interactive text messages; Arm-3: control (usual care with no texts) | SBP Control | Adherence and quality of life | Improved adherence; odds ratio for PDC was 1.86 (p < 0.001) for information-only messaging vs. usual care and 1.60 (p = 0.002) for interactive messaging vs. usual care. SBP was significantly reduced in both experimental groups; the mean change for the information-only message group vs. the usual care group was −2.2 mm Hg (p = 0.046) and for the interactive message group vs. usual care group was −1.6 mm Hg (p = 0.16). |
| 11 | Maslakpak and Safaie (2016) [26] | RCT (3 months) | Iran | n = 123 Hypertensive patients | Hill-Bone Medication Adherence Scale | Three-arm trial: Arm 1: SMS; Arm 2: reminder card; Arm 3: control (no intervention) | Adherence | Not mentioned | Improved adherence; SMS (57.70 ± 2.75), reminder cards (57.51 ± 2.69), vs. control (46.63 ± 2.99) (p < 0.001). |
| 12 | Kim et al. (2016) [27] | RCT (6 months) | Republic of Korea | n = 95 Hypertensive patients | MMAS-8 | Two-arm trial: Arm 1: wireless self-monitoring app; Arm-2: control (no intervention) | Adherence, PAM, SBP, and DBP | Not mentioned | No improvement in adherence. Improved SBP (beta = −0.27, p = 0.02) and DBP (beta = −0.34, p = 0.007) with patient activation. |
| 13 | Johnston et al. (2016) [28] | RCT (6 months) | Sweden | n = 174 Post-MI patients | 2 missed doses throughout a maximum 7-day observation cycle | Two-arm trial: Arm-1: interactive patient assistance tool (web-based software); Arm-2: control | Non-adherence score | Change in cardiovascular risk factors and quality of life | Adherence improved. Score for non-adherence: intervention vs. control (16.6 vs. 22.8) (p = 0.025). In the intervention group, patient satisfaction was also higher. |
| 14 | Reddy et al. (2017) [29] | RCT (3 months) | USA (Philadelphia) | n = 126 30–75 years old, 65 years old, 96% male patients with CAD with poor adherence | GlowCap (electronic pill bottle) | Three-arm trial: Arm-1: feedback from a participant who received a daily alarm and a weekly report on their medication adherence; Arm-2: feedback from a partner who also received an alarm and a weekly report that was shared with a friend, family member, or peer; Arm-3: control | Adherence | Adherence (post-intervention) change in LDL and patient activation | Adherence improved in both intervention arms compared to control. Individual feedback arm: 89%; partner feedback arm: 86%; control arm: 67%; (p < 0.001). |
| 15 | Kamal et al. (2018) [30] | RCT (3 months) | Pakistan | n = 201 CAD + CVA patients | MMAS-8 | Two-arm trial: Arm-1: daily interactive voice call, daily medication reminder, and weekly lifestyle modification messages; Arm-2: control (no intervention) | Adherence | Not mentioned | Adherence improved insignificantly: 7.41 in the intervention group vs. 7.38 in the control group. However, it was not statistically significant (p = 0.40). |
| 16 | Ni et al. (2018) [31] | RCT (1 month) | China | n = 50 CHD patients | 1—Number of dosages taken by a patient 2—Voils Medication Non-Adherence Extent Scale 3—Likert scale of 5 points | Two-phase, two-arm trial: We Chat, BB reminder app vs. controls (no intervention) | Adherence | SBP and DBP | Adherence improved insignificantly; non-adherence reduced to −1.35 in the experimental group vs. −0.69 in the control group. However, it was not statistically significant (p = 0.33). The SBP was reduced by 3.76 in controls vs. an increase of 0.93 in the experimental arm but this was statistically insignificant (p = 0.51). DBP was decreased significantly. |
| 17 | Kessler et al. (2018) [32] | RCT (6 months) | USA (Philadelphia) | n = 179 Age: 18, 52 y; 65% male CVS Health employees or their dependents with active CVS Caremark prescription coverage | Wireless pill bottle opening | Four-arm trial: Arm-1: medication adherence partner (friend/family); Arm-2: alert reminder (wireless pill bottle) + automated message (email, text, or automated phone calls); Arm-3: alert and partner; Arm-4: control | Adherence | Not mentioned | Adherence improved. Alert arm: 52.9% vs. controls: 17.0% (p = 0.002); partner + alert arm: 54.5% vs. control: 18.6%, 95% (p = 0.003). |
| 18 | Morawski et al. (2018) [33] | RCT (3 months) | USA (California) | n = 413 Self-reported hypertension | MMAS-8 | Two-arm trial: Arm-1: given a mobile app intervention; Arm-2: control (no intervention) | Adherence | SBP | Improved adherence; statistically significant change in mean medication adherence between the smartphone app and control group (difference: 0.4; p = 0.01); while no significant change in blood pressure was noted (difference: −0.5; p = 0.78). |
| 19 | Santo et al. (2019) [34] | RCT (3 months) | Australia | n = 165 CHD patients | MMAS-8 and PDC | Three-arm trial with the usual care arm, basic medication reminder app, and advanced medication app | Adherence | Adherence according to PDC, blood pressure, and cholesterol | Adherence improved concerning each medicine. The app received a response from 95% of the patients. |
| 20 | Desveaux et al. (2020) [35] | RCT (4 months) | Canada | n = 90 Post-MI patients | Adherence (positive and negative outcomes) | Three-arm trial: Arm-1: positive adherence as an endpoint; Arm-2: negative adherence as an outcome; Arm-3: did not involve, with negative adherence as an outcome. | Adherence | Not mentioned | The intervention facilitated adherence. |
| 21 | Ivers et al. (2020) [36] | RCT (12 months) | Ontario, Canada | n = 2632 Adults; 67 y; 70% male with CA after MI discharged from CRC | PDC | Three-arm trial: Arm-1: mail-outs; Arm-2: mail-outs plus automated phone calls; Arm-3: control (usual care) | Adherence + completion of cardiac rehabilitation | Not mentioned | No improvement in adherence. Medication adherence odds ratio: 1.02 (0.78–1.32) (p = 0.91); mail-outs: 0.95 (0.68–1.10) (p = 0.73); mail-outs/calls Statin adherence (PDC = 0.8): 0.89 (0.69–1.16) (p = 0.39); mail-outs: 1.04 (0.75–1.30). However, mail-and-phone interventions could boost cardiac rehabilitation completion after myocardial infarction. |
| 22 | Zhai et al. (2020) [37] | RCT (3 months) | China | n = 445 Hypertensive patients | MMAS-8 | Two-arm cluster RCT: Arm-1: SMS-based reminders on adherence to medication vs. control (no SMS) | SBP DBP | Adherence | Improved adherence. Mean medication adherence: 7.4 in the intervention group vs. 7.0 in the control group (p = 0.04); while SBP was reduced and showed a mean SBP of 134.5 mm Hg in the intervention group vs. 140.7 mm Hg in the control group (p = 0.001). |
| 23 | Maddison et al. (2021) [38] | RCT (12 months) | New Zealand | n = 306 Participants with ACS/MI/percutaneous coronary revascularization | Prescription records, MMAS-8, A modified behaviour score (European Prospective into Cancer–Norfolk prospective population research) | Two-arm trial: Arm-1: Text4HeartII intervention; Arm-2: control (no intervention) | Adherence to medication at 24 weeks | Adherence to medication ratio at 52 weeks | No improvement in adherence. Medication adherence in intervention group vs. usual care (87/153 (56.8%) vs. 105/153). |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Arshed, M.; Mahmud, A.B.; Minhat, H.S.; Ying, L.P.; Umer, M.F. Effectiveness of mHealth Interventions in Medication Adherence among Patients with Cardiovascular Diseases: A Systematic Review. Diseases 2023, 11, 41. https://doi.org/10.3390/diseases11010041
Arshed M, Mahmud AB, Minhat HS, Ying LP, Umer MF. Effectiveness of mHealth Interventions in Medication Adherence among Patients with Cardiovascular Diseases: A Systematic Review. Diseases. 2023; 11(1):41. https://doi.org/10.3390/diseases11010041
Chicago/Turabian StyleArshed, Muhammad, Aidalina Binti Mahmud, Halimatus Sakdiah Minhat, Lim Poh Ying, and Muhammad Farooq Umer. 2023. "Effectiveness of mHealth Interventions in Medication Adherence among Patients with Cardiovascular Diseases: A Systematic Review" Diseases 11, no. 1: 41. https://doi.org/10.3390/diseases11010041
APA StyleArshed, M., Mahmud, A. B., Minhat, H. S., Ying, L. P., & Umer, M. F. (2023). Effectiveness of mHealth Interventions in Medication Adherence among Patients with Cardiovascular Diseases: A Systematic Review. Diseases, 11(1), 41. https://doi.org/10.3390/diseases11010041