

A Multimodal Approach in the Treatment of Persistent Post-COVID

Abstract
1. Introduction
1.1. Post-COVID
1.2. Complementary Medicine
1.3. Whole-Body Hyperthermia
2. Case
2.1. Physical Status at Admission
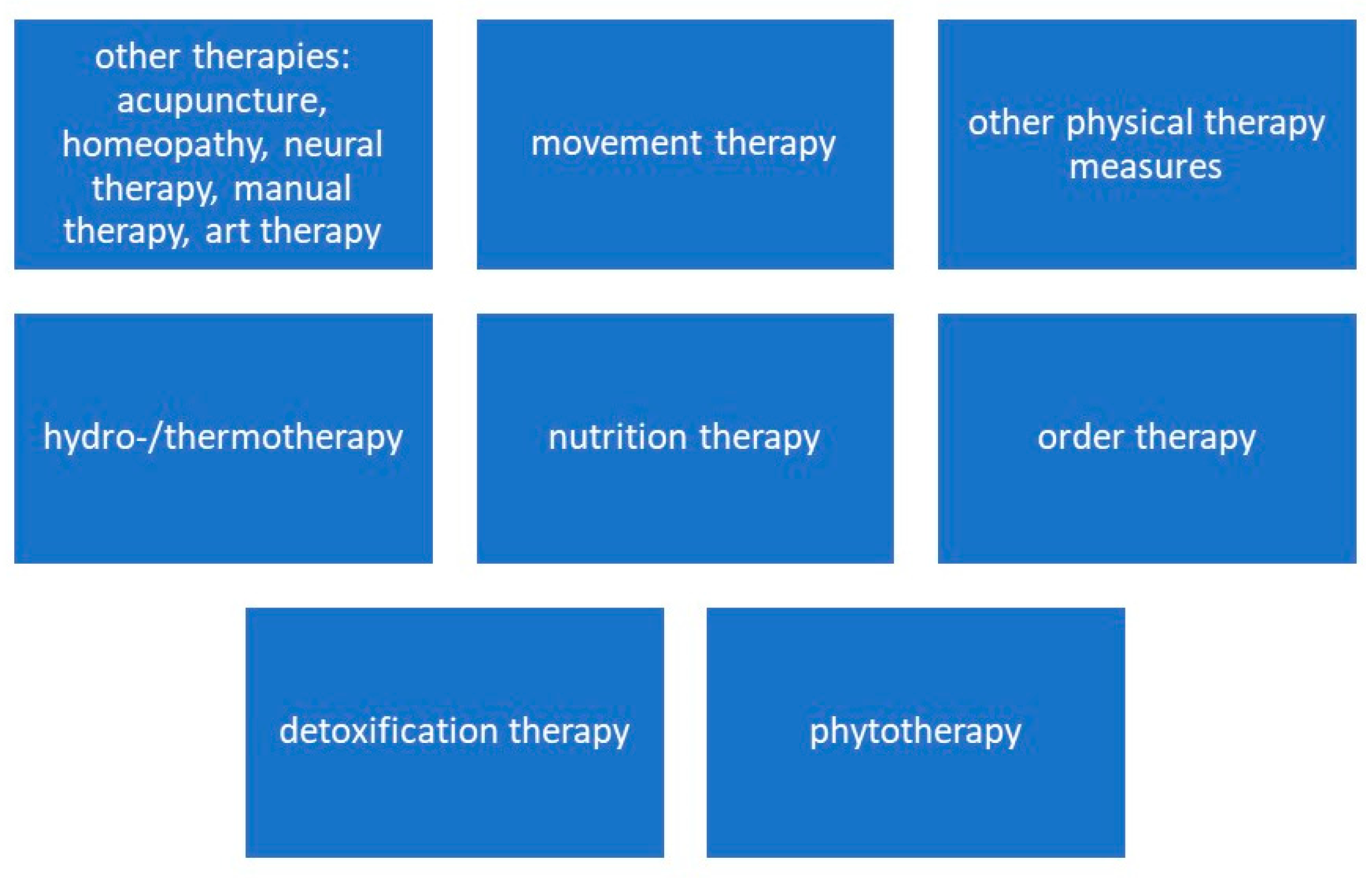
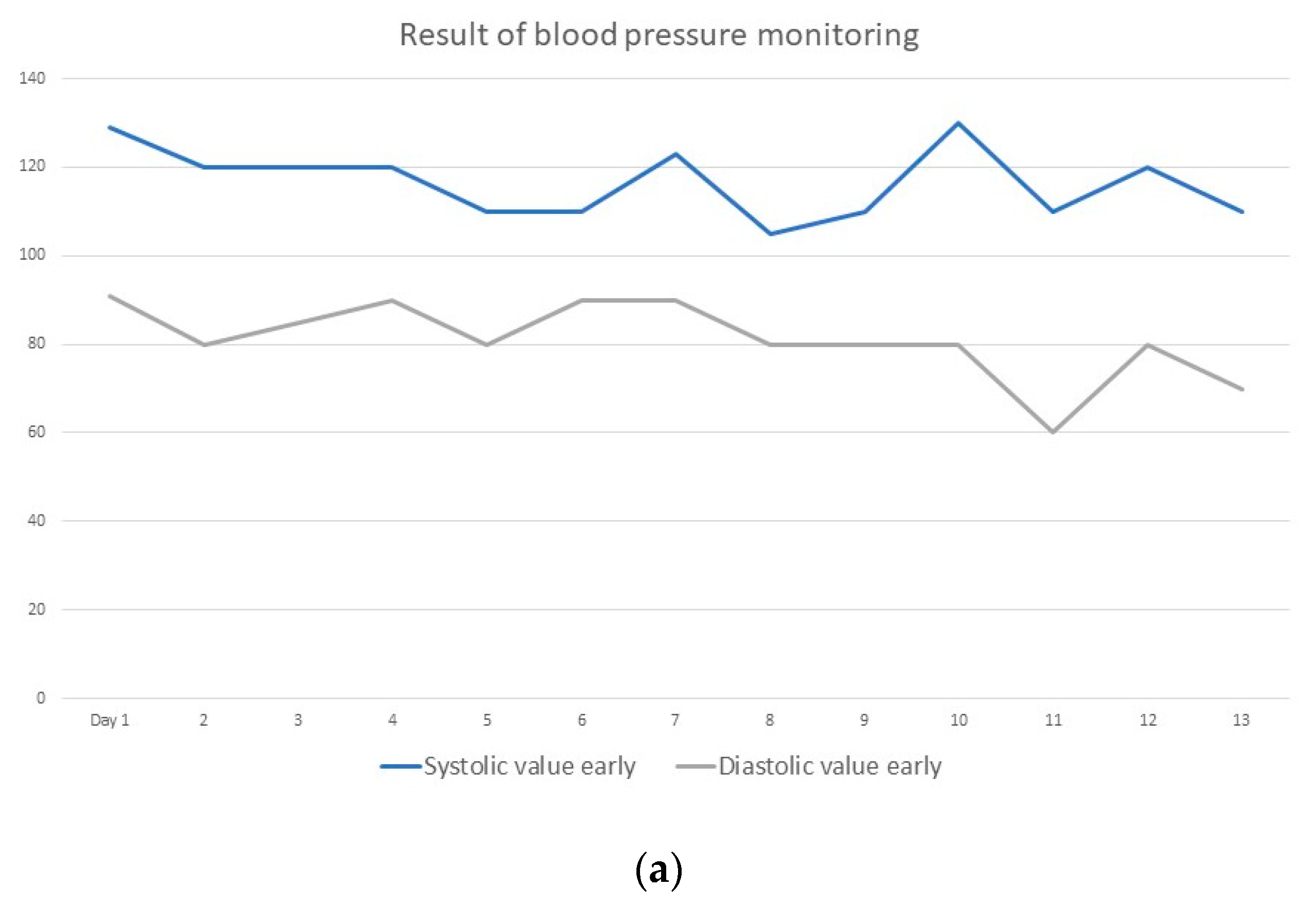
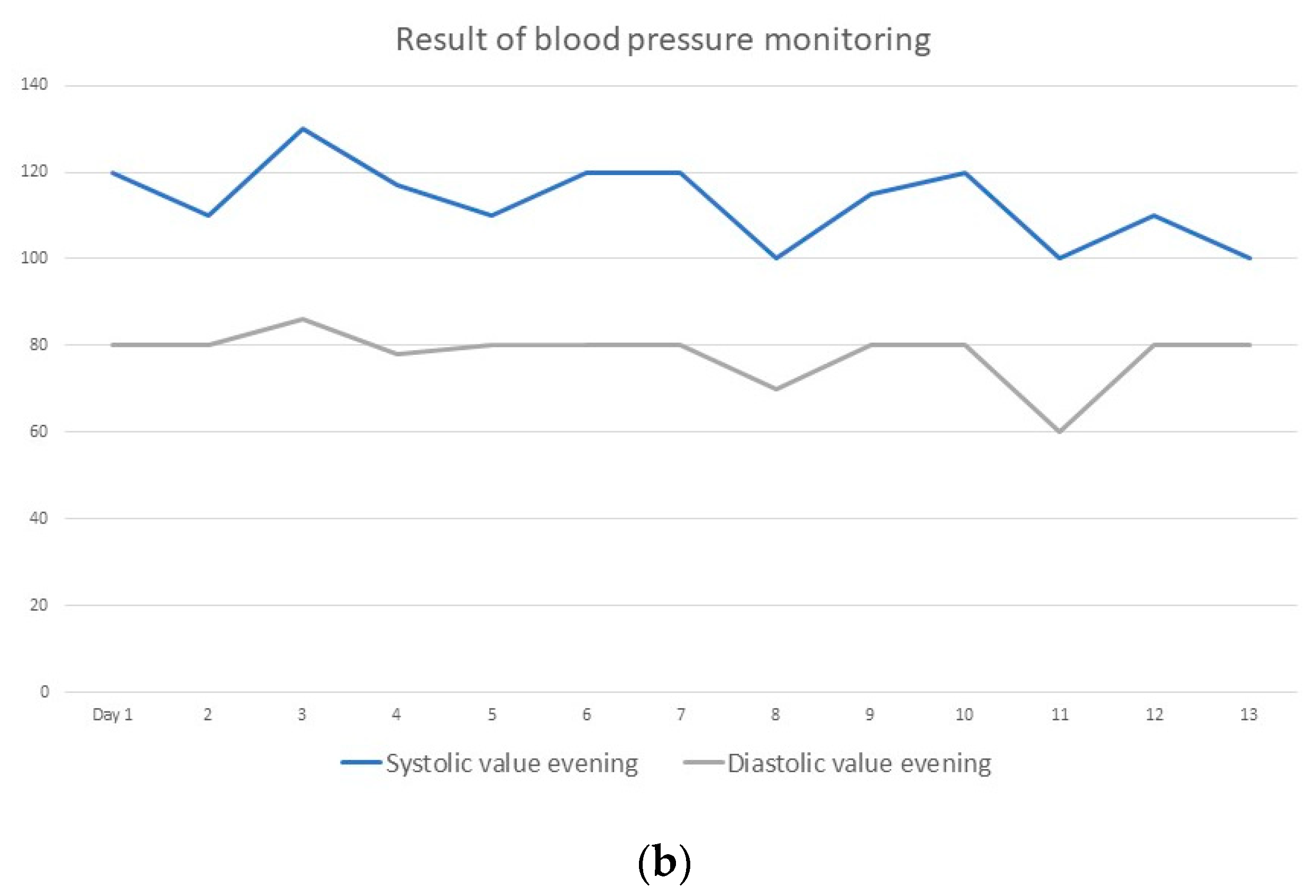
2.2. Implementation of a Naturopathic Complex Therapy with the Integration of Systemic Whole-Body Hyperthermia
- -
- “I was included in the therapy as a whole person”;
- -
- “The staff responded to my questions”;
- -
- “Especially the hyperthermia, the liniments, relaxation-leading procedures, and the physiotherapeutic measures helped”;
- -
- “My quality of life has improved significantly.”
3. Discussion
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- National Institute for Health and Care Excellence, Royal College of General Practitioners, Healthcare Improvement Scotland SIGN. COVID-19 Rapid Guideline: Managing the Long Term Effects of COVID-19. 2020. Available online: www.nice.org.uk/guidance/ng188 (accessed on 25 September 2022).
- Shah, W.; Hillman, T.; Playford, E.D.; Hishmeh, L. Managing the long term effects of COVID-19: Summary of NICE, SIGN, and RCGP rapid guideline. BMJ 2021, 372, n136. [Google Scholar] [CrossRef] [PubMed]
- Sudre, C.H.; Murray, B.; Varsavsky, T.; Graham, M.S.; Penfold, R.S.; Bowyer, R.C.; Pujol, J.C.; Klaser, K.; Antonelli, M.; Canas, L.S.; et al. Attributes and predictors of long COVID. Nat. Med. 2021, 27, 626–631. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.W.; Shah, A.S.; Johnston, J.C.; Carlsten, C.; Ryerson, C. Patient-reported outcome measures after COVID-19: A prospective cohort study. Eur. Respir. J. 2020, 56, 2003276. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Bansal, R.; Gubbi, S.; Koch, C.A. COVID-19 and chronic fatigue syndrome: An endocrine perspective. J. Clin. Transl. Endocrinol. 2022, 27, 100284. [Google Scholar] [CrossRef]
- Rabady, S.; Altenberger, J.; Brose, M.; Denk-Linnert, D.M.; Fertl, E.; Götzinger, F.; Pellin, M.d.l.C.G.; Hofbaur, B.; MPH, K.H.; Hoffmann-Dorninger, R.; et al. Leitlinie S1: Long COVID: Differenzialdiagnostik und Behandlungsstrategien. Wien. Klin. Wochenschr. 2021, 133, 237–278. [Google Scholar] [CrossRef]
- Sivan, M.; Taylor, S. NICE guideline on long COVID. BMJ 2020, 371, m4938. [Google Scholar] [CrossRef]
- Youn, B.-Y.; Moon, S.; Mok, K.; Cheon, C.; Ko, Y.; Park, S.; Jang, B.-H.; Shin, Y.-C.; Ko, S.-G. Use of Traditional, Complementary and Alternative Medicine in Nine Countries: A Cross-Sectional Multinational Survey. Complement. Ther. Med. 2022, 71, 102889. [Google Scholar] [CrossRef]
- World Health Organization. WHO Global Report on Traditional and Complementary Medicine; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Badakhsh, M.; Dastras, M.; Sarchahi, Z.; Doostkami, M.; Mir, A.; Bouya, S. Complementary and alternative medicine therapies and COVID-19: A systematic review. Rev. Environ. Health 2021, 36, 443–450. [Google Scholar] [CrossRef]
- Kim, T.H.; Jeon, S.R.; Kang, J.W.; Kwon, S. Complementary and Alternative Medicine for Long COVID: Scoping Review and Bibliometric Analysis. Evid. Based Complement. Altern. Med. 2022, 2022, 7303393. [Google Scholar] [CrossRef]
- Li, L.; Gou, C.-Y.; Li, X.-M.; Song, W.-Y.; Wang, X.-J.; Li, H.-Y.; Li, X.-H. Effects of Chinese medicine on symptoms, syndrome evolution, and lung inflammation absorption in COVID-19 convalescent patients during 84-day follow-up after hospital discharge: A prospective cohort and nested case-control study. Chin. J. Integr. Med. 2021, 27, 245–251. [Google Scholar] [CrossRef] [PubMed]
- Zhi, N.; Mo, Q.; Yang, S.; Qin, Y.-X.; Chen, H.; Wu, Z.-G.; Lan, C.-H.; Zhang, J.; Li, Y.-L. Treatment of pulmonary fibrosis in one convalescent patient with corona virus disease 2019 by oral traditional Chinese medicine decoction: A case report. J. Integr. Med. 2021, 19, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Romeyke, T.; Stummer, H. Evidence-based complementary and alternative medicine in inpatient care: Take a look at Europe. J. Evid. Based Complement. Altern. Med. 2015, 20, 87–93. [Google Scholar] [CrossRef] [PubMed]
- Tomiyama-Miyaji, C.; Watanabe, M.; Ohishi, T.; Kanda, Y.; Kainuma, E.; Bakir, H.Y.; Shen, J.; Ren, H.; Inoue, M.; Tajima, K.; et al. Modulation of the endocrine and immune systems by well-controlled hyperthermia equipment. Biomed. Res. 2007, 28, 119–125. [Google Scholar] [CrossRef] [PubMed]
- Schmidt, K.L. Effects of Whole Body Hyperthermia on Inflammations and Immune Reactions: Experimental Aspects. Phys. Med. Rehabil. Kurortmed. 2004, 14, 227–235. [Google Scholar]
- Jimenez, C.; Melin, B.; Savourey, G.; Launay, J.C.; Alonso, A.; Mathieu, J. Effects of passive hyperthermia versus exercise-induced hyperthermia on immune responses: Hormonal implications. Eur. Cytokine Netw. 2007, 18, 37–44. [Google Scholar]
- Janssen, C.W.; Lowry, C.A.; Mehl, M.R.; Allen, J.J.; Kelly, K.L.; Gartner, D.E.; Medrano, A.; Begay, T.K.; Rentscher, K.; White, J.J.; et al. Whole-body hyperthermia for the treatment of major depressive disorder: A randomized clinical trial. JAMA Psychiatry 2016, 73, 789–795. [Google Scholar] [CrossRef]
- Zhao, C.; Dai, C.; Chen, X. Whole-body hyperthermia combined with hyperthermic intraperitoneal chemotherapy for the treatment of stage IV advanced gastric cancer. Int. J. Hyperth. 2012, 28, 735–741. [Google Scholar] [CrossRef]
- Romeyke, T.; Scheuer, H.C.; Stummer, H. Fibromyalgia with severe forms of progression in a multidisciplinary therapy setting with emphasis on hyperthermia therapy—A prospective controlled study. Clin. Interv. Aging 2015, 10, 69. [Google Scholar] [CrossRef]
- Maltezou, H.C.; Pavli, A.; Tsakris, A. Post-COVID syndrome: An insight on its pathogenesis. Vaccines 2021, 9, 497. [Google Scholar] [CrossRef]
- Komaroff, A.L.; Lipkin, W.I. Insights from myalgic encephalomyelitis/chronic fatigue syndrome may help unravel the pathogenesis of postacute COVID-19 syndrome. Trends Mol. Med. 2021, 27, 895–906. [Google Scholar] [CrossRef] [PubMed]
- Augustin, M.; Schommers, P.; Stecher, M.; Dewald, F.; Gieselmann, L.; Gruell, H.; Horn, C.; Vanshylla, K.; Di Cristanziano, V.; Osebold, L.; et al. Post-COVID syndrome in non-hospitalised patients with COVID-19: A longitudinal prospective cohort study. Lancet Reg. Health Eur. 2021, 6, 100122. [Google Scholar] [CrossRef] [PubMed]
- Taquet, M.; Luciano, S.; Geddes, J.R.; Harrison, P.J. Bidirectional associations between COVID-19 and psychiatric disorder: Retrospective cohort studies of 62 354 COVID-19 cases in the USA. Lancet Psychiatry 2021, 8, 130–140. [Google Scholar] [CrossRef]
- Menges, D.; Ballouz, T.; Anagnostopoulos, A.; Aschmann, H.E.; Domenghino, A.; Fehr, J.S.; Puhan, M.A. Burden of post-COVID-19 syndrome and implications for healthcare service planning: A population-based cohort study. PLoS ONE 2021, 16, e0254523. [Google Scholar] [CrossRef]
- Woesner, M. What is old is new again: The use of whole-body hyperthermia for depression recalls the medicinal uses of hyperthermia, fever therapy, and hydrotherapy. Curr. Neurbiol. 2019, 10, 56–66. [Google Scholar]
- Al-Aly, Z.; Xie, Y.; Bowe, B. High-dimensional characterization of post-acute sequelae of COVID-19. Nature 2021, 594, 259–264. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Over the Past 2 Weeks, How Often Have You Felt Affected by the Following Complaints? | |
|---|---|
| - Little interest or pleasure in your work | Not at all |
| - Depression, sadness, or hopelessness | Not at all |
| - Difficulty falling asleep or staying asleep, or increased sleep | Almost every day |
| - Feeling tired or lacking in energy | Almost every day |
| - Decreased appetite or excessive need to eat | On some days |
| - Bad opinion of yourself; feeling a failure to be or to have disappointed the family | Not at all |
| - Difficulty concentrating on something, e.g., reading the newspaper or watching TV | Almost every day |
| - Were your movements or speech slowed down enough for others to notice? Or, on the contrary, were you “fidgety” or restless? Does this mean you have a stronger urge to move than usual? | On single days |
| - Thoughts that you would rather be dead or want to hurt yourself? | Not at all |
| In the last 4 weeks, have you had an anxiety attack (sudden feeling of fear or panic)? | No |
| Please indicate how much the problems described above made it difficult for you to do your job, take care of your household, or with other people to cope. | Very strong |
| Over the past 4 weeks, how often have you felt bothered by the following symptoms? | |
| Feeling nervous, anxious, tense, or overly concerned | Not at all |
| Feeling restless, making it difficult to sit still | Not at all |
| Easily fatigable | More than half the days |
| Muscle tightness, muscle pain | Not at all |
| Difficulty falling or staying asleep | More than half the days |
| Difficulty concentrating on something, such as reading or watching TV | More than half the days |
| Slight irritability, hypersensitivity | More than half the days |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Romeyke, T. A Multimodal Approach in the Treatment of Persistent Post-COVID. Diseases 2022, 10, 97. https://doi.org/10.3390/diseases10040097
Romeyke T. A Multimodal Approach in the Treatment of Persistent Post-COVID. Diseases. 2022; 10(4):97. https://doi.org/10.3390/diseases10040097
Chicago/Turabian StyleRomeyke, Tobias. 2022. "A Multimodal Approach in the Treatment of Persistent Post-COVID" Diseases 10, no. 4: 97. https://doi.org/10.3390/diseases10040097
APA StyleRomeyke, T. (2022). A Multimodal Approach in the Treatment of Persistent Post-COVID. Diseases, 10(4), 97. https://doi.org/10.3390/diseases10040097