Multi-Sensor Validation Approach of an End-Effector-Based Robot for the Rehabilitation of the Upper and Lower Limb

 ,
,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
2.1. Methods
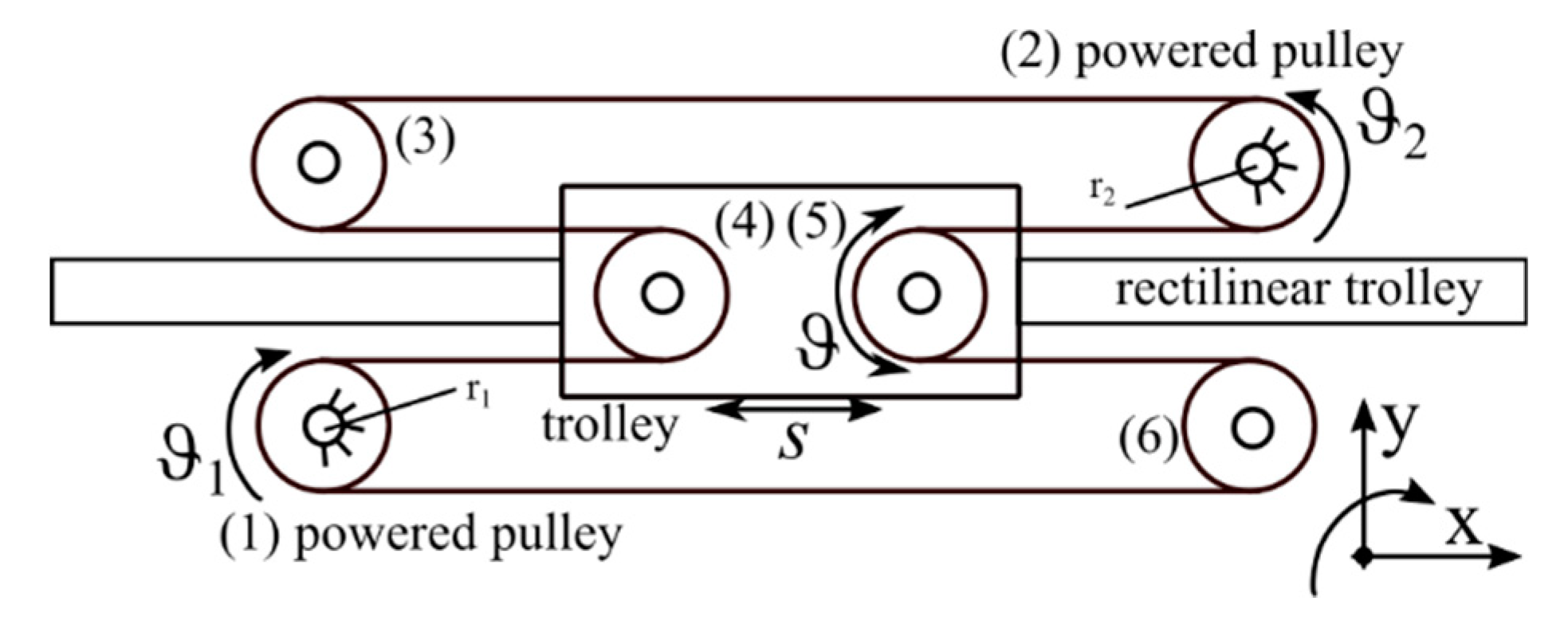
2.1.1. The Rehabilitation Device
2.1.2. Acquisition Protocol
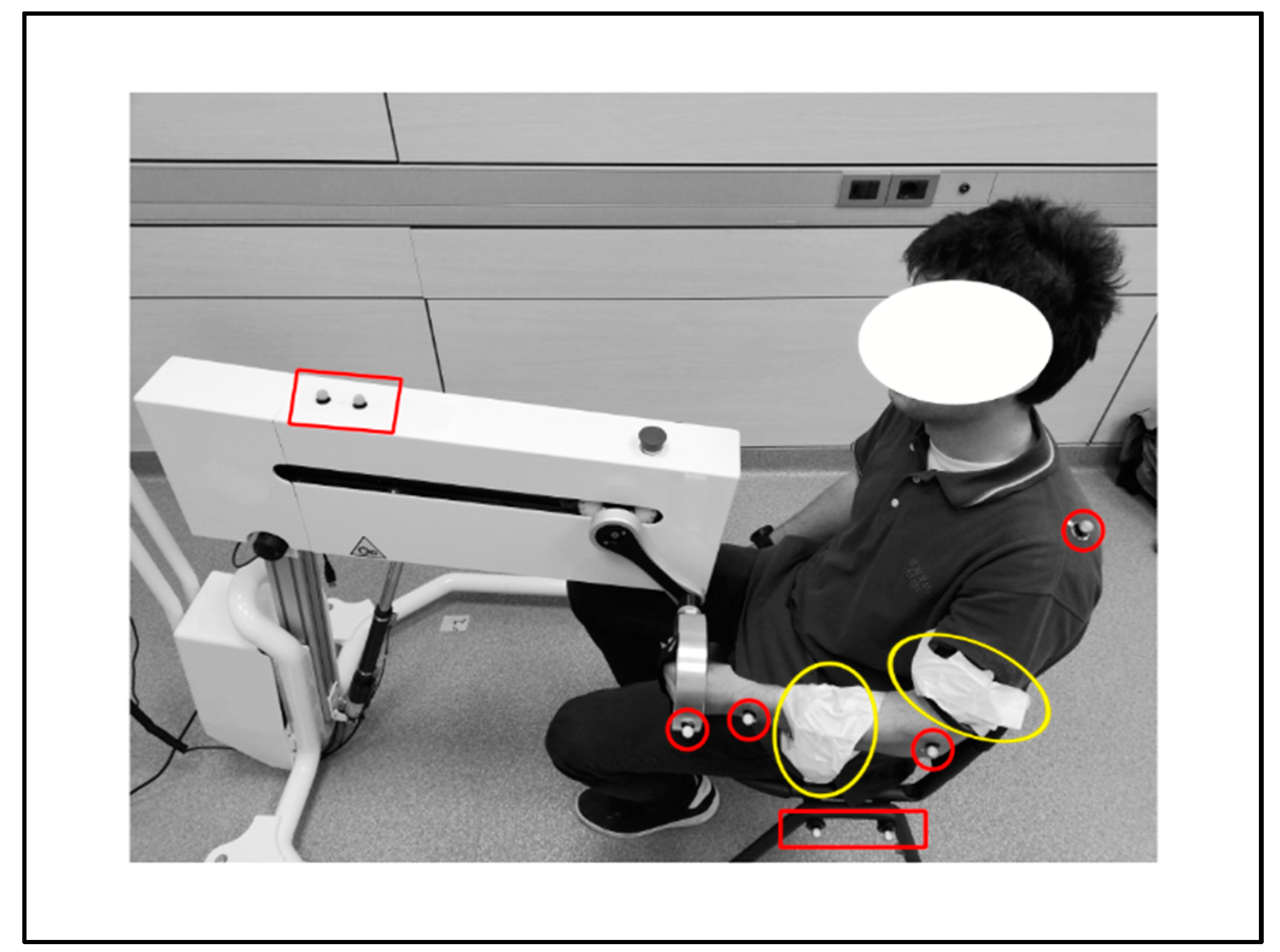
2.1.3. Experimental Settings
2.1.4. Kinematic Models
2.2. Data Analysis
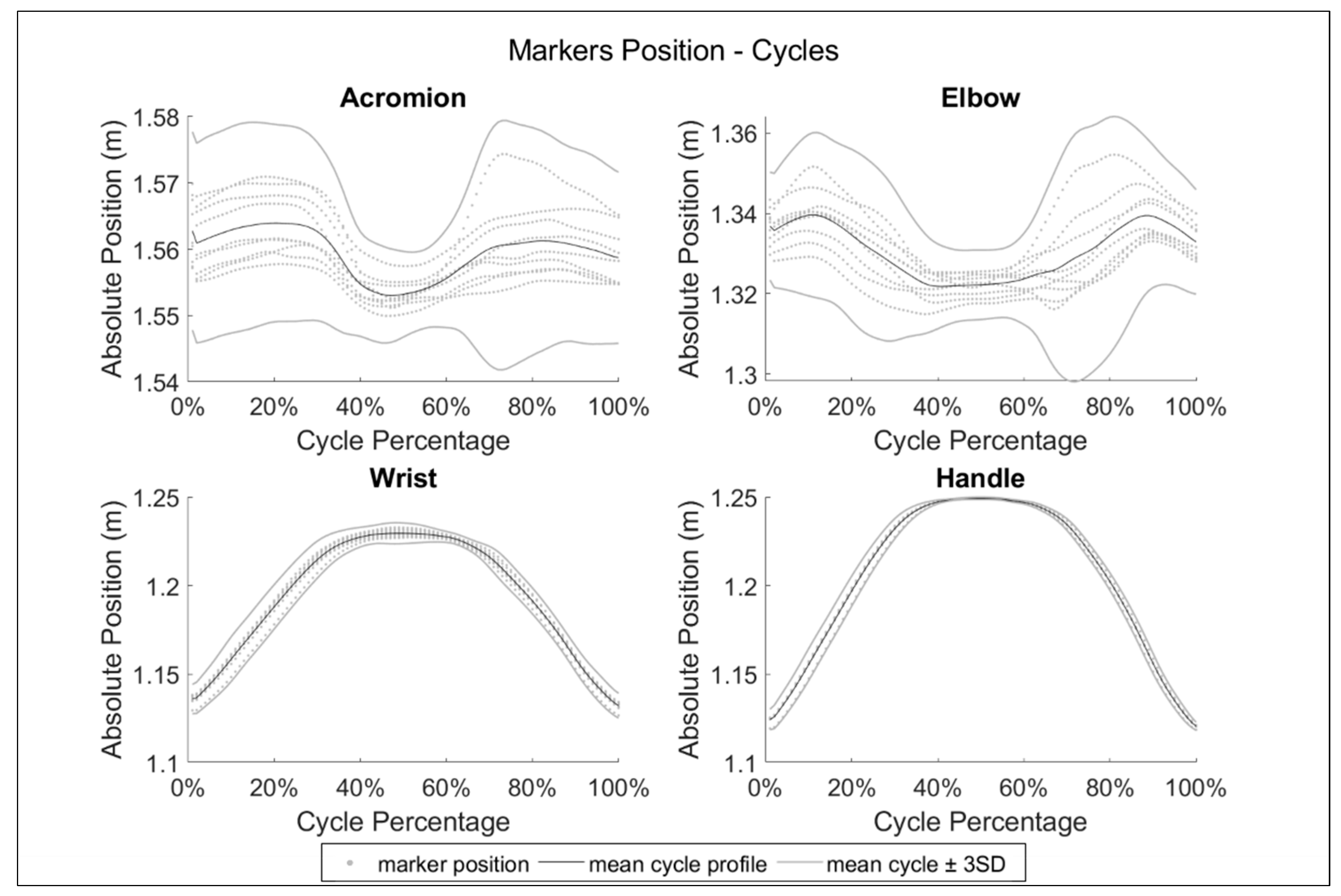
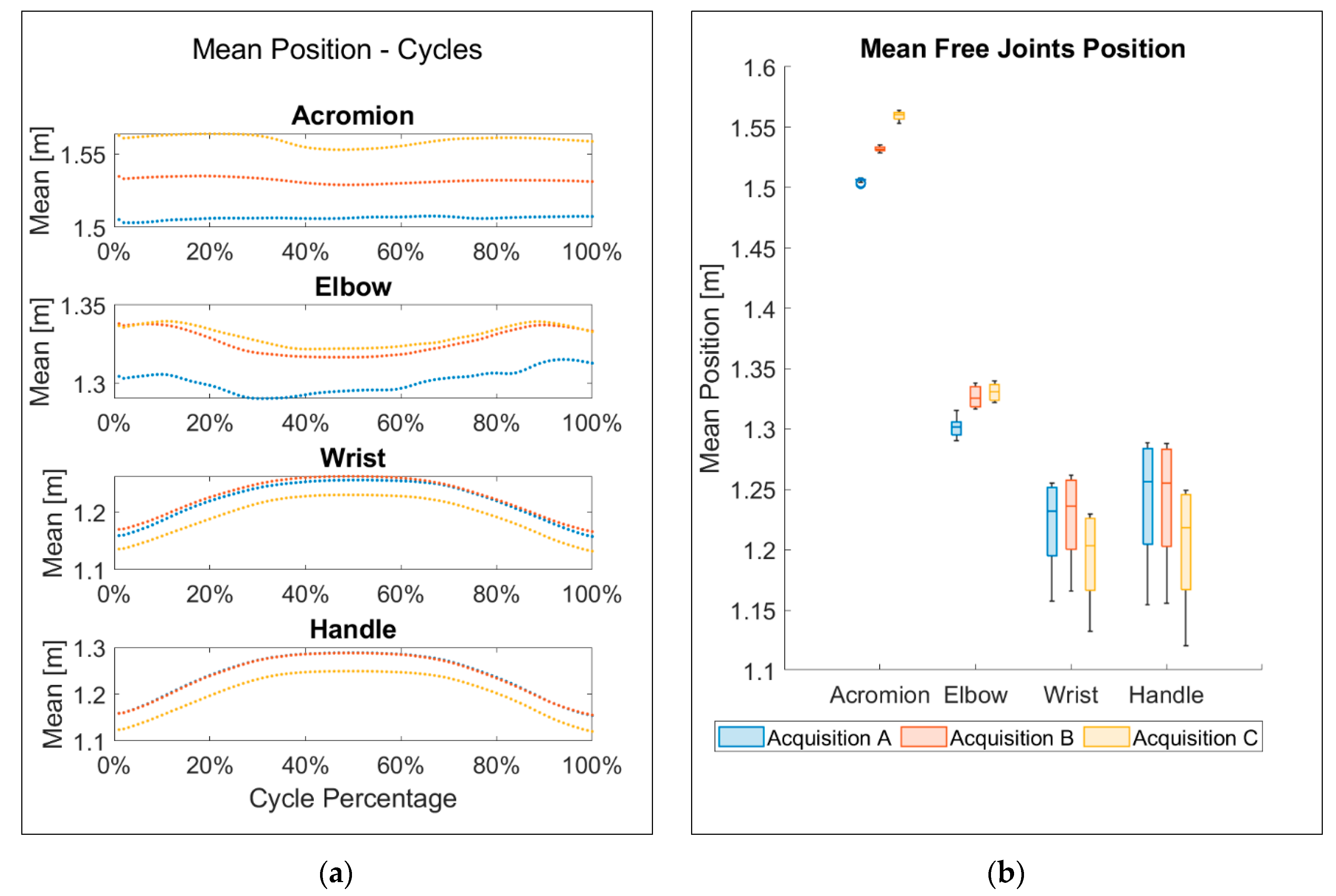
2.2.1. Optoelectronic Data
- •
- In signal processing, peaks can be detected easier than local minima. The filtered signal was therefore changed in sign, converting the analysis into a problem of local maxima evaluation;
- •
- Actual start/stop events are close to the maximum value. To be accepted as start/stop events, candidates must be above the 95% of the average value of the signal;
- •
- The operator imposed the repetition of the same motion profile 9 times, so cycles time is expected to be reasonably constant. Thus, only peaks at a certain distance from the previous and the following candidate can be chosen: this acceptability distance was defined as the range within the mean expected duration of the cycles, ±5%.
2.2.2. Accelerometers Data
2.2.3. Data Statistics
2.2.4. Measurement Systems Comparison
3. Results and Discussion
4. Conclusions
- •
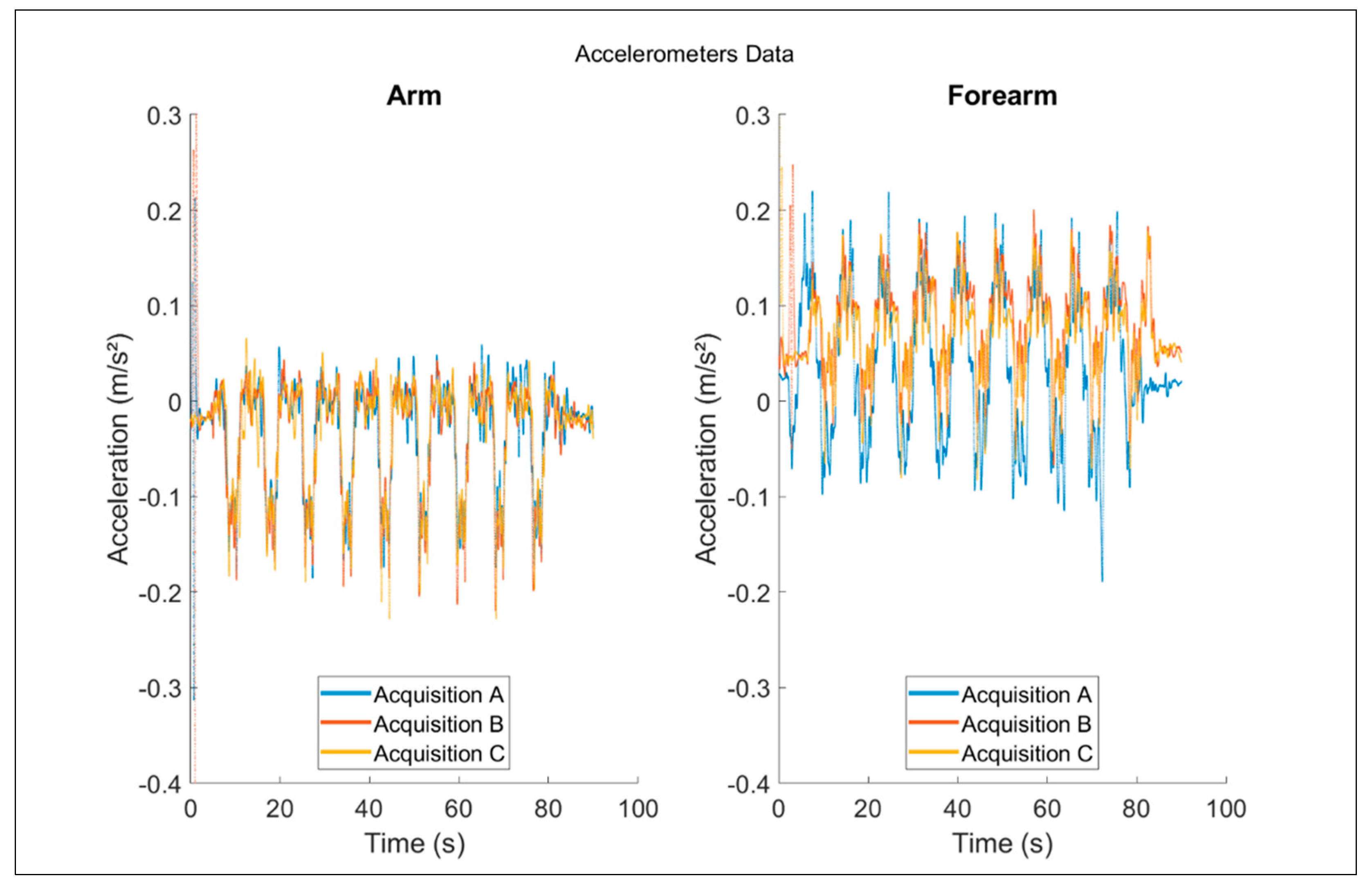
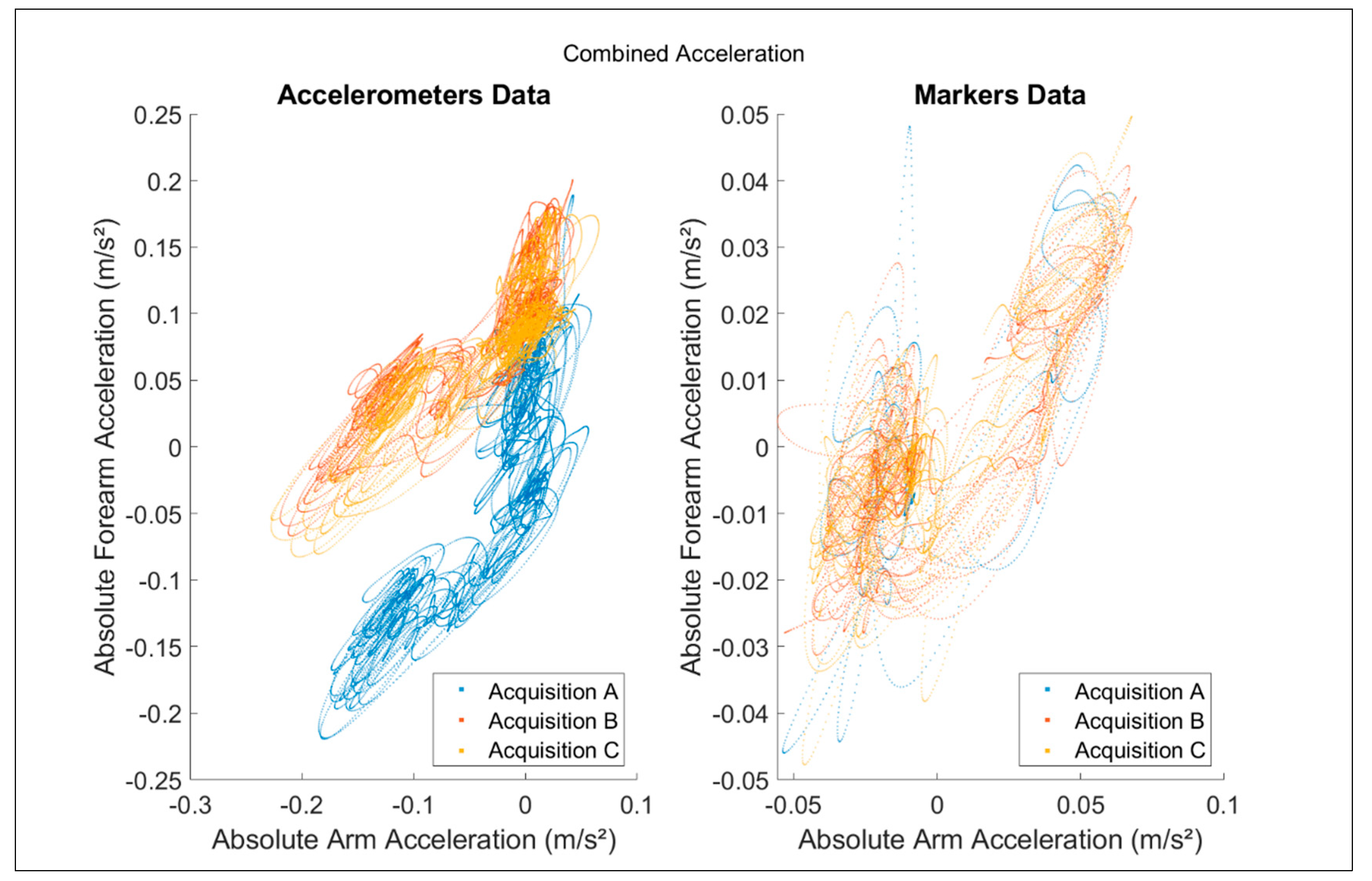
- Accelerometers provide more complex information, and optical markers are more suitable for evaluating the repeatability of the subject performance;
- •
- Both the systems can be used to evaluate the acceleration of the subject’s arm and forearm, but they provide different information;
- •
- Optical markers should be preferred when analyzing the kinematic system as a whole, e.g., for the definition of the functional design of a system;
- •
- Accelerometers should be used when detailed information is needed at punctual level, like in the optimization process of a device component.
- •
- This preliminary analysis allowed assessing the effectiveness of the system as rehabilitation device;
- •
- Although the subject declared to experience a smooth actuation of his limb during the execution of the moment, the performed analyses revealed low frequencies vibrations of the device carter, suggesting future optimization margins for the transmission system;
- •
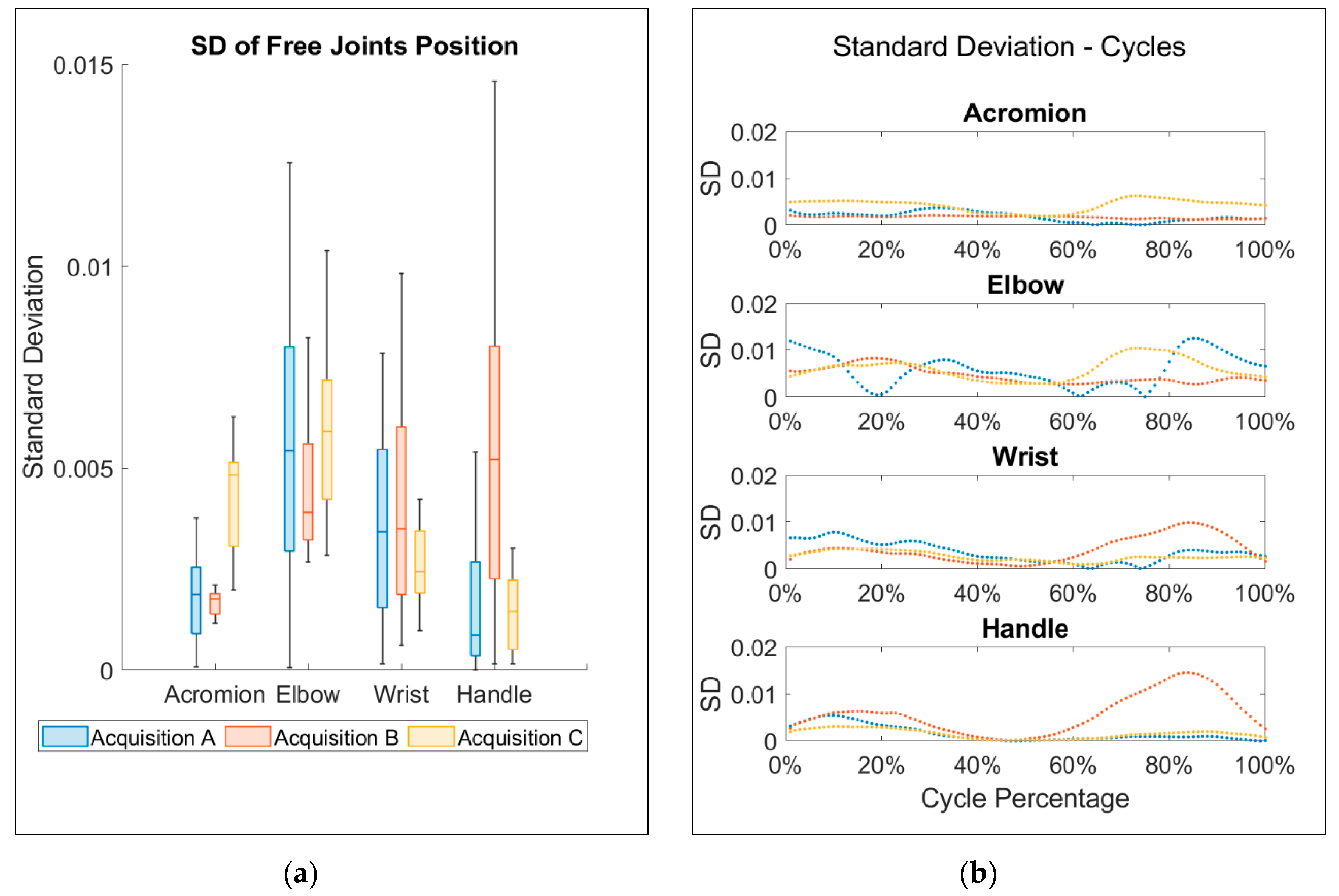
- The system demonstrated a remarkable repetition accuracy: during the simulated rehabilitation sessions, the free joints of the reduced kinematic model, corresponding to the subject wrist, elbow and shoulder, presented low values of SD among cycles.
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- French, B.; Thomas, L.H.; Coupe, J.; McMahon, N.E.; Connell, L.; Harrison, J.; Sutton, C.J.; Tishkovskaya, S.; Watkins, C.L. Repetitive task training for improving functional ability after stroke. Cochrane Database Syst. Rev. 2016, 11, CD006073. [Google Scholar] [CrossRef] [PubMed]
- Mehrholz, J.; Pohl, M.; Platz, T.; Kugler, J.; Elsner, B. Electromechanical and robot-assisted arm training for improving activities of daily living, arm function, and arm muscle strength after stroke. Cochrane Database Syst. Rev. 2012, 13, CD006876. [Google Scholar] [CrossRef]
- Legg, L.A.; Lewis, S.R.; Schofield-Robinson, O.J.; Drummond, A.; Langhorne, P. Occupational therapy for adults with problems in activities of daily living after stroke. Cochrane Database Syst. Rev. 2017, 7. [Google Scholar] [CrossRef]
- Wolf, S.L.; Winstein, C.J.; Miller, J.P.; Taub, E.; Uswatte, G.; Morris, D.; Giuliani, C.; Light, K.E.; Nichols-Larsen, D. Effect of Constraint-Induced Movement Therapy on Upper Extremity Function 3 to 9 Months After Stroke. JAMA 2006, 296, 2095–2104. [Google Scholar] [CrossRef]
- Díaz, I.; Gil, J.J.; Sánchez, E. Lower-Limb Robotic Rehabilitation: Literature Review and Challenges. J. Robot. 2011, 2011, 1–11. [Google Scholar] [CrossRef]
- Pedrocchi, A.; Ferrante, S.; Ambrosini, E.; Gandolla, M.; Casellato, C.; Schauer, T.; Klauer, C.; Pascual, J.; Vidaurre, C.; Gföhler, M.; et al. MUNDUS project: MUltimodal Neuroprosthesis for daily Upper limb Support. J. Neuroeng. Rehabil. 2013, 10, 66. [Google Scholar] [CrossRef]
- Schröder, J.; Truijen, S.; Criekinge, T.; Saeys, W. Feasibility and effectiveness of repetitive gait training early after stroke: A systematic review and meta-analysis. J. Rehabil. Med. 2019, 51, 78–88. [Google Scholar] [CrossRef] [PubMed]
- Rosenstein, L.; Ridgel, A.L.; Thota, A.K.; Samame, B.; Alberts, J.L. Effects of combined robotic therapy and repetitive-task practice on upper-extremity function in a patient with chronic stroke. Am. J. Occup. Ther. 2008, 62, 28–35. [Google Scholar] [CrossRef]
- Maciejasz, P.; Eschweiler, J.; Gerlach-Hahn, K.; Jansen-Troy, A.; Leonhardt, S. A survey on robotic devices for upper limb rehabilitation. J. Neuroeng. Rehabil. 2014, 11, 3. [Google Scholar] [CrossRef]
- Pinto-Fernandez, D.; Etorricelli, D.; Sanchez-Villamanan, M.D.C.; Aller, F.; Mombaur, K.; Conti, R.; Vitiello, N.; Moreno, J.; Pons, J.L. Performance Evaluation of Lower Limb Exoskeletons: A Systematic Review. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 1573–1583. [Google Scholar] [CrossRef] [PubMed]
- Ercolini, G.; Trigili, E.; Baldoni, A.; Crea, S.; Vitiello, N. A Novel Generation of Ergonomic Upper-Limb Wearable Robots: Design Challenges and Solutions. Robotica 2018, 37, 2056–2072. [Google Scholar] [CrossRef]
- Krebs, H.I.; Hogan, N.; Aisen, M.L.; Volpe, B.T. Robot-aided neurorehabilitation. IEEE Trans. Rehabil. Eng. 1998, 6, 75–87. [Google Scholar] [CrossRef] [PubMed]
- Schiele, A.; Van Der Helm, F.C.T. Kinematic Design to Improve Ergonomics in Human Machine Interaction. IEEE Trans. Neural Syst. Rehabil. Eng. 2006, 14, 456–469. [Google Scholar] [CrossRef] [PubMed]
- Xiong, C.-H.; Chen, W.-R.; Sun, B.-Y.; Liu, M.-J.; Yue, S. Design and Implementation of an Anthropomorphic Hand for Replicating Human Grasping Functions. IEEE Trans. Robot. 2016, 32, 652–671. [Google Scholar] [CrossRef]
- Welleweerd, M.K.; Siepel, F.J.; Groenhuis, V.; Veltman, J.; Stramigioli, S. Design of an end-effector for robot-assisted ultrasound-guided breast biopsies. Int. J. Comput. Assist. Radiol. Surg. 2020, 15, 681–690. [Google Scholar] [CrossRef]
- Gupta, A.; O’Malley, M.K.; Patoglu, V.; Burgar, C. Design, Control and Performance ofRiceWrist:A Force Feedback Wrist Exoskeleton for Rehabilitation and Training. Int. J. Robot. Res. 2008, 27, 233–251. [Google Scholar] [CrossRef]
- Lum, P.; Reinkensmeyer, D.; Mahoney, R.; Rymer, W.Z.; Burgar, C. Robotic Devices for Movement Therapy After Stroke: Current Status and Challenges to Clinical Acceptance. Top. Stroke Rehabil. 2002, 8, 40–53. [Google Scholar] [CrossRef]
- Rastegarpanah, A.; Saadat, M.; Borboni, A. Parallel Robot for Lower Limb Rehabilitation Exercises. Appl. Bionics Biomech. 2016, 2016, 1–10. [Google Scholar] [CrossRef]
- Takahashi, C.D.; Der-Yeghiaian, L.; Le, V.; Motiwala, R.R.; Cramer, S.C. Robot-based hand motor therapy after stroke. Brain 2008, 131, 425–437. [Google Scholar] [CrossRef]
- Nathan, D.E.; Johnson, M.J.; McGuire, J. Feasibility of integrating FES grasp assistance with a task-oriented robot-assisted therapy environment: A case study. In Proceedings of the 2008 2nd IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics, Scottsdale, AZ, USA, 19–22 October 2008; pp. 807–812. [Google Scholar]
- Oda, K.; Isozumi, S.; Ohyama, Y.; Tamida, K.; Kikuchi, T.; Furusho, J. Development of isokinetic and iso-contractile exercise machine “MEM-MRB” using MR brake. In Proceedings of the 2009 IEEE International Conference on Rehabilitation Robotics, Kyoto, Japan, 23–26 June 2009; pp. 6–11. [Google Scholar]
- Kung, P.-C.; Ju, M.-S.; Lin, C.-C.K. Design of a forearm rehabilitation robot. In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 12–15 June 2007; ICORR: Morgan, UT, USA, 2007; pp. 228–233. [Google Scholar]
- Tiboni, M.; Legnani, G.; Lancini, M.; Serpelloni, M.; Gobbo, M.; Fausti, D. ERRSE: Elbow Robotic Rehabilitation System with an EMG-Based Force Control. In New Advances in Mechanism and Machine Science; Springer International Publishing: Basel, Switzerland, 2017; pp. 892–900. [Google Scholar]
- Tiboni, M.; Borboni, A.; Faglia, R.; Pellegrini, N. Robotics rehabilitation of the elbow based on surface electromyography signals. Adv. Mech. Eng. 2018, 10, 2. [Google Scholar] [CrossRef]
- Reiman, M.P.; Lorenz, D.S. Integration of Strength and Conditioning Principles into a Rehabilitation Program. Int. J. Sports Phys. Ther. 2011, 6, 241–253. Available online: http://www.ncbi.nlm.nih.gov/pubmed/21904701 (accessed on 16 May 2019). [PubMed]
- Gao, S.; Wang, Y.; Fang, C.; Xu, L. A Smart Terrain Identification Technique Based on Electromyography, Ground Reaction Force, and Machine Learning for Lower Limb Rehabilitation. Appl. Sci. 2020, 10, 2638. [Google Scholar] [CrossRef]
- Mezzina, G.; Aprigliano, F.; Micera, S.; Monaco, V.; De Venuto, D. EEG/EMG based Architecture for the Early Detection of Slip-induced Lack of Balance. In Proceedings of the 2019 IEEE 8th International Workshop on Advances in Sensors and Interfaces (IWASI), Otranto, Italy, 13–14 June 2019. [Google Scholar]
- Sonenblum, S.E.; Sprigle, S.; Caspall, J.; Lopez, R. Validation of an accelerometer-based method to measure the use of manual wheelchairs. Med. Eng. Phys. 2012, 34, 781–786. [Google Scholar] [CrossRef] [PubMed]
- Laidig, D.; Seel, T. Deriving kinematic quantities from accelerometer readings for assessment of functional upper limb motions. Curr. Dir. Biomed. Eng. 2017, 3, 573–576. [Google Scholar] [CrossRef]
- Daponte, P.; De Vito, L.; Sementa, C. Validation of a home rehabilitation system for range of motion measurements of limb functions. In Proceedings of the 2013 IEEE International Symposium on Medical Measurements and Applications (MeMeA), Gatineau, QC, Canada, 4–5 May 2013; pp. 288–293. [Google Scholar]
- Buongiorno, D.; Barsotti, M.; Barone, F.; Bevilacqua, V.; Frisoli, A. A Linear Approach to Optimize an EMG-Driven Neuromusculoskeletal Model for Movement Intention Detection in Myo-Control: A Case Study on Shoulder and Elbow Joints. Front. Neurorobotics 2018, 12, 1–12. [Google Scholar] [CrossRef]
- Faglia, R.; Fausti, D.; Antonini, M.; Petrogalli, G.; Mor, M.; Vertuan, A. Physical Exercise Machine. EP2865363A1, 29 April 2015. [Google Scholar]
- Ceresoli, F.; Aggogeri, F.; Amici, C.; Borboni, A.; Faglia, R.; Pellegrini, N.; Tiboni, M.; Antonini, M.; Fausti, D.; Mor, M.; et al. Differential system for limb rehabilitation. In Proceedings of the 6th International Workshop on New Trends in Medical and Service Robotics (MESROB 2018), Cassino, Italy, 4–6 July 2018; pp. 1–8. [Google Scholar]
- Bussola, R.; Faglia, R.; Incerti, G.; Biazzi, P.; Locatelli, V. Innovative mechanical devices as servo-system components for automation. In Proceedings of the IASTED International Conference on Modelling Identification and Control, Innsbruck, Austria, 10–13 February 2003; pp. 370–377. [Google Scholar]
- Legnani, G.; Casolo, F.; Righettini, P.; Zappa, B. A homogeneous matrix approach to 3D kinematics and dynamics—I. Theory. Mech. Mach. Theory 1996, 31, 573–587. [Google Scholar] [CrossRef]
- Legnani, G.; Casalo, F.; Righettini, P.; Zappa, B. A homogeneous matrix approach to 3D kinematics and dynamics—II. Applications to chains of rigid bodies and serial manipulators. Mech. Mach. Theory 1996, 31, 589–605. [Google Scholar] [CrossRef]
- Mandelbrot, B.B.; Wheeler, J.A. The Fractal Geometry of Nature. Am. J. Phys. 1983, 51, 286–287. [Google Scholar] [CrossRef]
- Ganea, R.; Paraschiv-Ionescu, A.; Büla, C.; Rochat, S.; Aminian, K. Multi-parametric evaluation of sit-to-stand and stand-to-sit transitions in elderly people. Med. Eng. Phys. 2011, 33, 1086–1093. [Google Scholar] [CrossRef]
- Błaszczyk, J.W.; Klonowski, W. Postural stability and fractal dynamics. Acta Neurobiol. Exp. 2001, 61, 105–112. [Google Scholar]
- Sekine, M.; Akay, M.; Tamura, T.; Higashi, Y.; Fujimoto, T. Fractal dynamics of body motion in patients with Parkinson’s disease. J. Neural Eng. 2004, 1, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Akay, M.; Sekine, M.; Tamura, T.; Higashi, Y.; Fujimoto, T. Fractal dynamics of body motion in post-stroke hemiplegic patients during walking. J. Neural Eng. 2004, 1, 111–116. [Google Scholar] [CrossRef]
- Boshoff, H.F.V. A fast box counting algorithm for determining the fractal dimension of sampled continuous functions. In Proceedings of the 1992 South African Symposium on Communications and Signal Processing, Cape Town, South Africa, 11 September 1992; pp. 43–48. [Google Scholar]
- Nguyen, T.; Hausdorff (Box-Counting) Fractal Dimension with multi-resolution calculation. MATLAB Central File Exchange. Available online: https://www.mathworks.com/matlabcentral/fileexchange/58148-hausdorff-box-counting-fractal-dimension-with-multi-resolution-calculation (accessed on 16 May 2019).
- Bussmann, J.B.J.; Martens, W.L.J.; Tulen, J.H.M.; Schasfoort, F.C.; Berg-Emons, H.J.G.V.D.; Stam, H.J. Measuring daily behavior using ambulatory accelerometry: The Activity Monitor. Behav. Res. Methods Instrum. Comput. 2001, 33, 349–356. [Google Scholar] [CrossRef] [PubMed]
- Amici, C.; Ghidoni, M.; Ceresoli, F.; Gaffurini, P.; Bissolotti, L.; Mor, M.; Fausti, D.; Antonini, M.; Ragni, F.; Tiboni, M. Preliminary Validation of a Device for the Upper and Lower Limb Robotic Rehabilitation. In Proceedings of the 2019 23rd International Conference on Mechatronics Technology (ICMT), SALERNO, Italy, 23–26 October 2019; pp. 1–6. [Google Scholar] [CrossRef]
- Ragni, F.; Amici, C.; Borboni, A.; Faglia, R.; Cappellini, V.; Pedersini, P.; Villafañe, J.H. Effects of Soft Tissue Artifact in the Measurement of Hand Kinematics. Int. Rev. Mech. Eng. (IREME) 2020, 14, 230. [Google Scholar] [CrossRef]
- Negrini, S.; Serpelloni, M.; Amici, C.; Gobbo, M.; Silvestro, C.; Buraschi, R.; Borboni, A.; Crovato, D.; Lopomo, N. Use of Wearable Inertial Sensor in the Assessment of Timed-Up-and-Go Test: Influence of Device Placement on Temporal Variable Estimation. In Proceedings of the International Conference on Wireless Mobile Communication and Healthcare, Milan, Italy, 14–15 November 2016; pp. 310–317. [Google Scholar]
- Piovanelli, B.; Amici, C.; Cappellini, V.; Borboni, A.; Negrini, S. P106: Functional assessment of the spine through an optoelectronic system in spinal disorders. Gait Posture 2017, 57, 349–350. [Google Scholar] [CrossRef]
- Pedersini, P.; Villafañe, J.; Piovanelli, B.; Cappellini, V.; Buraschi, R.; Pollet, J.; Negrini, S. P 106—Intra- and inter-operator reliability of a novel hand protocol during grip movement in healthy subjects. Gait Posture 2018, 65, 409–410. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sessions | ||||
|---|---|---|---|---|
| Session A (Medial Radius) | Session B (Medial Ulna) | Session C (Medial Ulna) | ||
| Device | SD (mm) | <0.300 | 0.518 | <0.300 |
| Maximum variation (mm) | <0.300 | <0.300 | <0.300 | |
| Arm Absolute Acceleration Vs Forearm Absolute Acceleration | Fractal Dimension | ||
|---|---|---|---|
| Session A (Medial Radius) | Session B (Medial Ulna) | Session C (Medial Ulna) | |
| Accelerometers | 1.4091 | 1.4113 | 1.4144 |
| Optical Markers | 1.1487 | 1.1961 | 1.2264 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Amici, C.; Ragni, F.; Ghidoni, M.; Fausti, D.; Bissolotti, L.; Tiboni, M. Multi-Sensor Validation Approach of an End-Effector-Based Robot for the Rehabilitation of the Upper and Lower Limb. Electronics 2020, 9, 1751. https://doi.org/10.3390/electronics9111751
Amici C, Ragni F, Ghidoni M, Fausti D, Bissolotti L, Tiboni M. Multi-Sensor Validation Approach of an End-Effector-Based Robot for the Rehabilitation of the Upper and Lower Limb. Electronics. 2020; 9(11):1751. https://doi.org/10.3390/electronics9111751
Chicago/Turabian StyleAmici, Cinzia, Federica Ragni, Manuela Ghidoni, Davide Fausti, Luciano Bissolotti, and Monica Tiboni. 2020. "Multi-Sensor Validation Approach of an End-Effector-Based Robot for the Rehabilitation of the Upper and Lower Limb" Electronics 9, no. 11: 1751. https://doi.org/10.3390/electronics9111751
APA StyleAmici, C., Ragni, F., Ghidoni, M., Fausti, D., Bissolotti, L., & Tiboni, M. (2020). Multi-Sensor Validation Approach of an End-Effector-Based Robot for the Rehabilitation of the Upper and Lower Limb. Electronics, 9(11), 1751. https://doi.org/10.3390/electronics9111751