Perturbed Point-to-Point Reaching Tasks in a 3D Environment Using a Portable Haptic Device

 , ,
, ,  and
and 
Abstract
1. Introduction
2. Materials and Methods
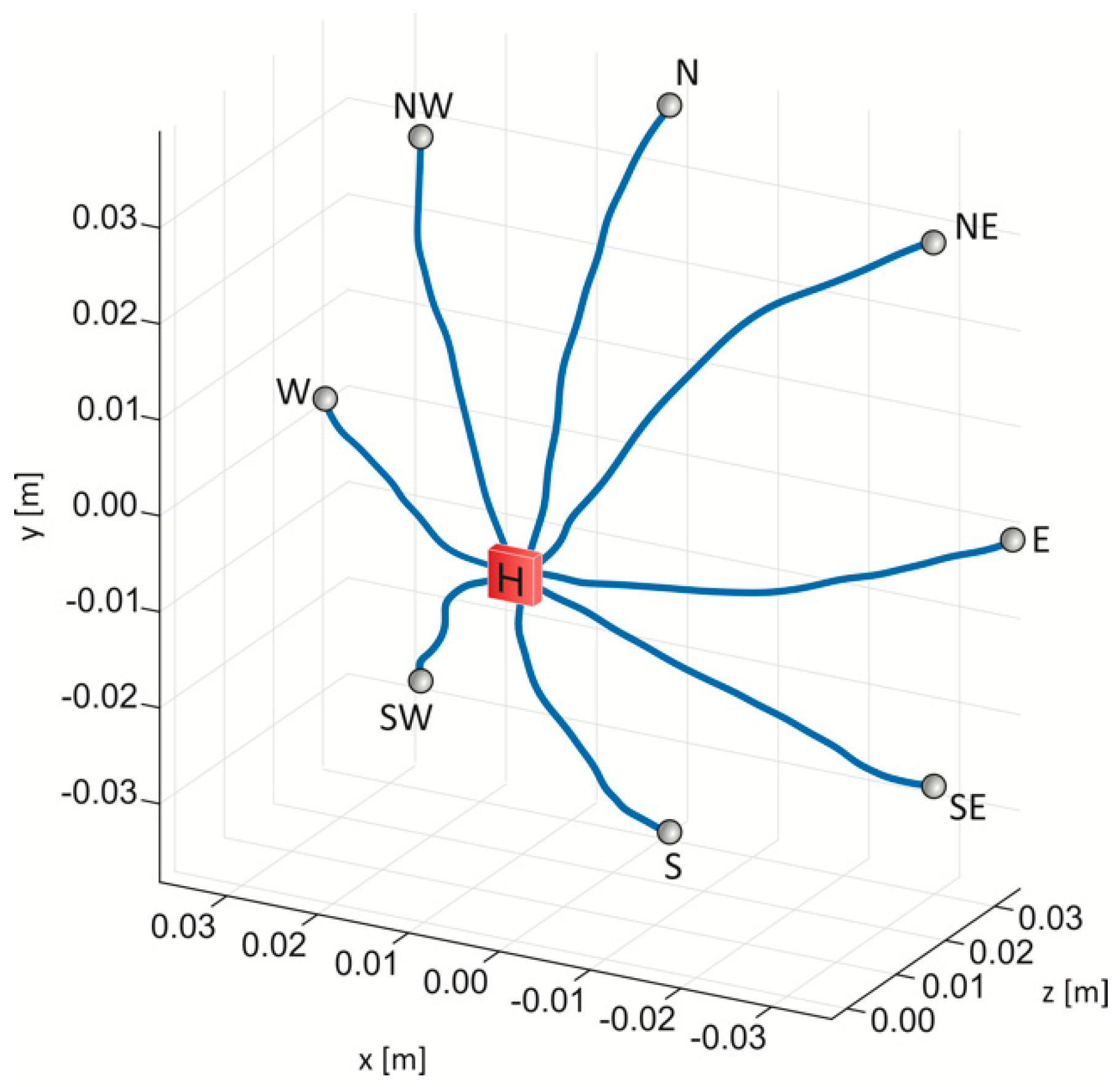
2.1. Experimental Setup and Game Design
2.2. Experimental Protocol
2.3. Data Analysis
- The Length Ratio (LR) is the ratio between the path actually travelled by the subject and the ideal one (Lt), i.e., the minimum distance between the centers of the home-base and the target-base [35]:where dR is the distance between two consecutive points of the trajectory. Zollo et al. [35] proposed this index to evaluate the gradual performance in a chronic stroke cohort.
- The Lateral Deviation (LD) is defined as the highest deviation from a straight line connecting the starting and the ending points of the movement trajectory [14]. Masia et al. [14] found that the LD values for a group of children with cerebral palsy, were higher compared to a group of typically developed children.
- The Aiming Angle (AA) is the angle between the line connecting the starting and ending target, and the line at the starting point to the trajectory point, which is characterized by the maximum peak of velocity. Germanotta et al. [31] found higher values for AA in patients with Friedreich’s Ataxia compare to a healthy control group. Higher values of LR, LD and AA represent a reaching task performed with a lower accuracy [34].
- The Normalized Jerk (NJ), as proposed by Teulings et al. [37]:where j is the jerk, i.e., the derivative of acceleration and T is the duration of the movement. Lower values of NJ indicate smoother movements. Teulings et al. [37] evaluated the motor performance for a group of patients suffering from Parkinson’s disease using the NJ.
2.4. Statistical Analysis
3. Results
3.1. Repeatability and Reliability of the Protocol
3.2. Evaluation of Motor Performance
4. Discussion
4.1. Repeatability and Reliability of the Protocol
4.2. Is the Movement Performance Influenced by an Increase in Force Field Magnitude?
4.3. Do Movement Directions Influence Motor Performance?
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Mang, C.S.; Campbell, K.L.; Ross, C.J.D.; Boyd, L.A. Promoting Neuroplasticity for Motor Rehabilitation After Stroke: Considering the Effects of Aerobic Exercise and Genetic Variation on Brain-Derived Neurotrophic Factor. Phys. Ther. 2018, 93, 1707–1716. [Google Scholar] [CrossRef] [PubMed]
- You, S.; Jang, S.; Kim, H.Y.; Hallett, M.; Ahn, S.; Kwon, Y.; Kim, H.J.; Lee, M. Virtual Reality–Induced Cortical Reorganization and Associated Locomotor Recovery in Chronic Stroke. Stroke 2005, 36, 1166–1171. [Google Scholar] [CrossRef] [PubMed]
- Pacilli, A.; Germanotta, M.; Rossi, S.; Cappa, P. Quantification of age-related differences in reaching and circle-drawing using a robotic rehabilitation device. Appl. Bionics Biomech. 2014, 11, 91–104. [Google Scholar] [CrossRef]
- Cappa, P.; Clerico, A.; Nov, O.; Porfiri, M. Can Force Feedback and Science Learning Enhance the Effectiveness of Neuro-Rehabilitation? An Experimental Study on Using a Low-Cost 3D Joystick and a Virtual Visit to a Zoo. PLoS ONE 2013, 8, e83945. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.; Kaber, D.B.; Tupler, L.; Lee, Y.-S. Haptic-based Virtual Environment Design and Modeling of Motor Skill Assessment for Brain Injury PatientsRehabilitation. Comput. Aided Des. Appl. 2011, 8, 149–162. [Google Scholar] [CrossRef]
- Muhanna, M.A. Virtual reality and the CAVE: Taxonomy, interaction challenges and research directions. J. King Saud Univ. Comput. Inf. Sci. 2015, 27, 344–361. [Google Scholar] [CrossRef]
- Scalona, E.; Hayes, D.; Palermo, E.; Del Prete, Z.; Rossi, S. Performance Evaluation of 3D Reaching Tasks Using a Low-cost Haptic Device and Virtual Reality. In Proceedings of the 2017 IEEE International Symposium on Haptic, Audio and Visual Environments and Games (HAVE), Abu Dhabi, UAE, 22–23 October 2017. [Google Scholar]
- Alamri, A.; Eid, M.; Iglesias, R.; Shirmohammadi, S.; Saddik, A. El Haptic Virtual Rehabilitation Exercises for Post- stroke Diagnosis. IEEE Trans. Instrum. Meas. 2007, 57, 1–10. [Google Scholar]
- Ramaprabha, T.; Sathik, M. The Efficiency Enhancement in Non Immersive Virtual Reality System by Haptic Devices. Int. J. Adv. Res. Comput. Sci. 2012, 2, 1–5. [Google Scholar]
- Leonardis, D.; Solazzi, M.; Bortone, I.; Frisoli, A. A 3-RSR Haptic Wearable Device for Rendering Fingertip Contact Forces. IEEE Trans. Haptics 2017, 10, 305–316. [Google Scholar] [CrossRef]
- Frisoli, A.; Solazzi, M.; Salsedo, F.; Bergamasco, M. A Fingertip Haptic Display for Improving Curvature Discrimination. Presence Teleoperators Virtual Environ. 2008, 17, 550–561. [Google Scholar] [CrossRef]
- Igo Krebs, H.; Hogan, N.; Aisen, M.L.; Volpe, B.T. Robot-aided neurorehabilitation. IEEE Trans. Rehabil. Eng. 1998, 6, 75–87. [Google Scholar] [CrossRef]
- Lo, A.C.; Guarino, P.D.; Richards, L.G.; Haselkorn, J.K.; Wittenberg, G.F.; Federman, D.G.; Ringer, R.J.; Wagner, T.H.; Krebs, H.I.; Volpe, B.T.; et al. Robot-assisted therapy for long-term upper-limb impairment after stroke. N. Engl. J. Med. 2010, 362, 1772–1783. [Google Scholar] [CrossRef]
- Masia, L.; Frascarelli, F.; Morasso, P.; Di Rosa, G.; Petrarca, M.; Castelli, E.; Cappa, P. Reduced short term adaptation to robot generated dynamic enviroment in children affected by Cerebral Palsy. J. Neuroeng. Rehabil. 2011, 8, 28. [Google Scholar] [CrossRef] [PubMed]
- Lum, P.S.; Burgar, C.G.; Van der Loos, M.; Shor, P.C.; Majmundar, M.; Yap, R. MIME robotic device for upper-limb neurorehabilitation in subacute stroke subjects: A follow-up study. J. Rehabil. Res. Dev. 2006, 43, 631–642. [Google Scholar] [CrossRef] [PubMed]
- Amirabdollahian, F.; Loureiro, R.; Gradwell, E.; Collin, C.; Harwin, W.; Johnson, G. Multivariate analysis of the Fugl-Meyer outcome measures assessing the effectiveness of GENTLE/S robot-mediated stroke therapy. J. Neuroeng. Rehabil. 2007, 4, 4. [Google Scholar] [CrossRef] [PubMed]
- Bovolenta, F.; Goldoni, M.; Clerici, P.; Agosti, M.; Franceschini, M. Robot therapy for functional recovery of the upper limbs: A pilot study on patients after stroke. J. Rehabil. Med. 2009, 41, 971–975. [Google Scholar] [CrossRef]
- Basteris, A.; Nijenhuis, S.M.; Stienen, A.H.A.; Buurke, J.H.; Prange, G.B.; Amirabdollahian, F. Training modalities in robot-mediated upper limb rehabilitation in stroke: A framework for classification based on a systematic review. J. Neuroeng. Rehabil. 2014, 11, 111. [Google Scholar] [CrossRef] [PubMed]
- Viau, A.; Feldman, A.G.; McFadyen, B.J.; Levin, M.F. Reaching in reality and virtual reality: A comparison of movement kinematics in healthy subjects and in adults with hemiparesis. J. Neuroeng. Rehabil. 2004, 1, 11. [Google Scholar] [CrossRef]
- Gouveia, D.; Lopes, D.; De Carvalho, C.V. Serious Gaming for Experiential Learning. In Proceedings of the 41st ASEE/IEEE Frontiers in Education Conference, Rapid City, SD, USA, 12–15 October 2011; pp. 1–6. [Google Scholar]
- Silva, A.J.; Ramirez, O.A.D.; Vega, V.P.; Oliver, J.P.O. PHANToM OMNI Haptic Device: Kinematic and Manipulability. In Proceedings of the 2009 Electronics, Robotics and Automotive Mechanics Conference (CERMA), Cuernavaca, Mexico, 22–25 September 2009; pp. 193–198. [Google Scholar]
- Rodet, X.; Lambert, J.; Gaudy, T.; Gosselin, F. Study of haptic and visual interaction for sound and music control in the Phase project. In Proceedings of the 2005 Conference on New Interfaces for Musical Expression, Vancouver, BC, Canada, 26–28 May 2005; pp. 109–114. [Google Scholar]
- Ferreira, A.; Mavroidis, C. Virtual reality and haptics for nanorobotics. IEEE Robot. Autom. Mag. 2006, 13, 78–92. [Google Scholar] [CrossRef]
- Martin, S.; Hillier, N. Characterisation of the Novint Falcon Haptic Device for Application as a Robot Manipulator. In Proceedings of the Australasian Conference on Robotics and Automation (ACRA), Sydney, Australia, 2–4 December 2009. [Google Scholar]
- Chortis, A.; Standen, P.J.; Walker, M. Virtual reality system for upper extremity rehabilitation of chronic stroke patients living in the community. In Proceedings of the 7th ICDVRAT with ArtAbilitation, Maia, Portugal, 8–11 September 2008; pp. 221–228. [Google Scholar]
- Palsbo, S.E.; Marr, D.; Streng, T.; Bay, B.K.; Norblad, A.W. Towards a modified consumer haptic device for robotic-assisted fine-motor repetitive motion training. Disabil. Rehabil. Assist. Technol. 2011, 6, 546–551. [Google Scholar] [CrossRef]
- Loureiro, R.C.V.; Harwin, W.S. Reach & Grasp Therapy: Design and Control of a 9-DOF Robotic Neuro-rehabilitation System. In Proceedings of the 2007 IEEE 10th International Conference on Rehabilitation Robotics, Noordwijk, The Netherlands, 13–15 June 2007; IEEE: Piscataway, NJ, USA, 2007; pp. 757–763. [Google Scholar]
- Prange, G.B.; Jannik, M.J.; Groothuis-Oudshoorn, C.G.; Hermens, H.J.; Ijzerman, M.J. Systematic review of the effect of robot-aided therapy on recovery of the hemiparetic arm after stroke. J. Rehabil. Res. Dev. 2006, 43, 171–184. [Google Scholar] [CrossRef] [PubMed]
- Scalona, E.; Martelli, F.; Del Prete, Z.; Palermo, E.; Rossi, S. A novel protocol for the evaluation of motor learning in 3D reching tasks using novint falcon. In Proceedings of the 7th IEEE RAS/EMBS International Conference on Biomedical Robotics and Biomechatronics, Enschede, The Netherlands, 27–29 August 2018; pp. 268–272. [Google Scholar]
- Scheidt, R.A.; Stoeckmann, T. Reach adaptation and final position control amid environmental uncertainty after stroke. J. Neurophysiol. 2007, 97, 2824–2836. [Google Scholar] [CrossRef] [PubMed]
- Germanotta, M.; Vasco, G.; Petrarca, M.; Rossi, S.; Carniel, S.; Bertini, E.; Cappa, P.; Castelli, E. Robotic and clinical evaluation of upper limb motor performance in patients with Friedreich’s Ataxia: An observational study. J. Neuroeng. Rehabil. 2015, 12, 41. [Google Scholar] [CrossRef] [PubMed]
- Harwin, B.W.S.; Patton, J.L.; Edgerton, V.R. Challenges and Opportunities for Robot-Mediated Neurorehabilitation. Proc. IEEE 2006, 94, 1717–1726. [Google Scholar] [CrossRef]
- Celik, O.; O’Malley, M.K.; Boake, C.; Levin, H.S.; Yozbatiran, N.; Reistetter, T.A. Normalized Movement Quality Measures for Therapeutic Robots Strongly Correlate with Clinical Motor Impairment Measures. IEEE Trans. Neural Syst. Rehabil. Eng. 2010, 18, 433–444. [Google Scholar] [CrossRef] [PubMed]
- Balasubramanian, S.; Colombo, R.; Sterpi, I.; Sanguineti, V.; Burdet, E. Robotic Assessment of Upper Limb Motor Function After Stroke. Am. J. Phys. Med. Rehabil. 2012, 91, S255–S269. [Google Scholar] [CrossRef] [PubMed]
- Zollo, L.; Gallotta, E.; Guglielmelli, E.; Sterzi, S. Robotic technologies and rehabilitation: New tools for upper-limb therapy and assessment in chronic stroke. Eur. J. Phys. Rehabil. Med. 2011, 47, 223–236. [Google Scholar]
- Rohrer, B.; Fasoli, S.; Krebs, H.I.; Hughes, R.; Volpe, B.; Frontera, W.R.; Stein, J.; Hogan, N. Movement smoothness changes during stroke recovery. J. Neurosci. Off. J. Soc. Neurosci. 2002, 22, 8297–8304. [Google Scholar] [CrossRef]
- Teulings, H.L.; Contreras-Vidal, J.L.; Stelmach, G.E.; Adler, C.H. Parkinsonism reduces coordination of fingers, wrist, and arm in fine motor control. Exp. Neurol. 1997, 146, 159–170. [Google Scholar] [CrossRef]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Lawrence Erlbaum Associates: Mahwah, NJ, USA, 1988; ISBN 0805802835. [Google Scholar]
- Bock, O. Load compensation in human goal-directed arm movements. Behav. Brain Res. 1990, 41, 167–177. [Google Scholar] [CrossRef]
- Hwang, E.J.; Donchin, O.; Smith, M.A.; Shadmehr, R. A gain-field encoding of limb position and velocity in the internal model of arm dynamics. PLoS Biol. 2003, 1, e25. [Google Scholar] [CrossRef] [PubMed]
- Gordon, J.; Ghilardi, M.F.; Cooper, S.E.; Ghez, C. Accuracy of planar reaching movements II. Systematic extent errors resulting from inertial anisotropy. Exp. Brain Res. 1994, 99, 112–130. [Google Scholar] [CrossRef] [PubMed]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| CV (%) | ICC | |||
|---|---|---|---|---|
| Rep1 | Rep2 | Rep3 | ||
| T | 18.5 (4.1) | 18.4 (2.6) | 17.1 (3.8) | 0.82 (0.03) |
| LR | 8.3 (3.3) | 6.6 (2.5) | 5.3 (2.3) | 0.86 (0.02) |
| LD | 27.6 (4.4) | 27.0 (4.7) | 25.7 (5.2) | 0.82 (0.02) |
| AA | 46.3 (13.7) | 46.0 (12.9) | 46.0 (12.9) | 0.80 (0.02) |
| SM | 14.5 (2.0) | 13.5 (2.9) | 12.0 (2.4) | 0.77 (0.05) |
| NJ | 42.4 (10.9) | 42.0 (5.2) | 38.8 (8.6) | 0.65 (0.07) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Scalona, E.; Hayes, D.; Del Prete, Z.; Palermo, E.; Rossi, S. Perturbed Point-to-Point Reaching Tasks in a 3D Environment Using a Portable Haptic Device. Electronics 2019, 8, 32. https://doi.org/10.3390/electronics8010032
Scalona E, Hayes D, Del Prete Z, Palermo E, Rossi S. Perturbed Point-to-Point Reaching Tasks in a 3D Environment Using a Portable Haptic Device. Electronics. 2019; 8(1):32. https://doi.org/10.3390/electronics8010032
Chicago/Turabian StyleScalona, Emilia, Darren Hayes, Zaccaria Del Prete, Eduardo Palermo, and Stefano Rossi. 2019. "Perturbed Point-to-Point Reaching Tasks in a 3D Environment Using a Portable Haptic Device" Electronics 8, no. 1: 32. https://doi.org/10.3390/electronics8010032
APA StyleScalona, E., Hayes, D., Del Prete, Z., Palermo, E., & Rossi, S. (2019). Perturbed Point-to-Point Reaching Tasks in a 3D Environment Using a Portable Haptic Device. Electronics, 8(1), 32. https://doi.org/10.3390/electronics8010032