
Design and Joint Dynamics of Human Recumbent Rehabilitation Training Devices



Abstract
1. Introduction
2. Materials and Methods
2.1. Experiments on Motion Capture and Reaction Force Acquisition for Prone Limb Rehabilitation Exercises
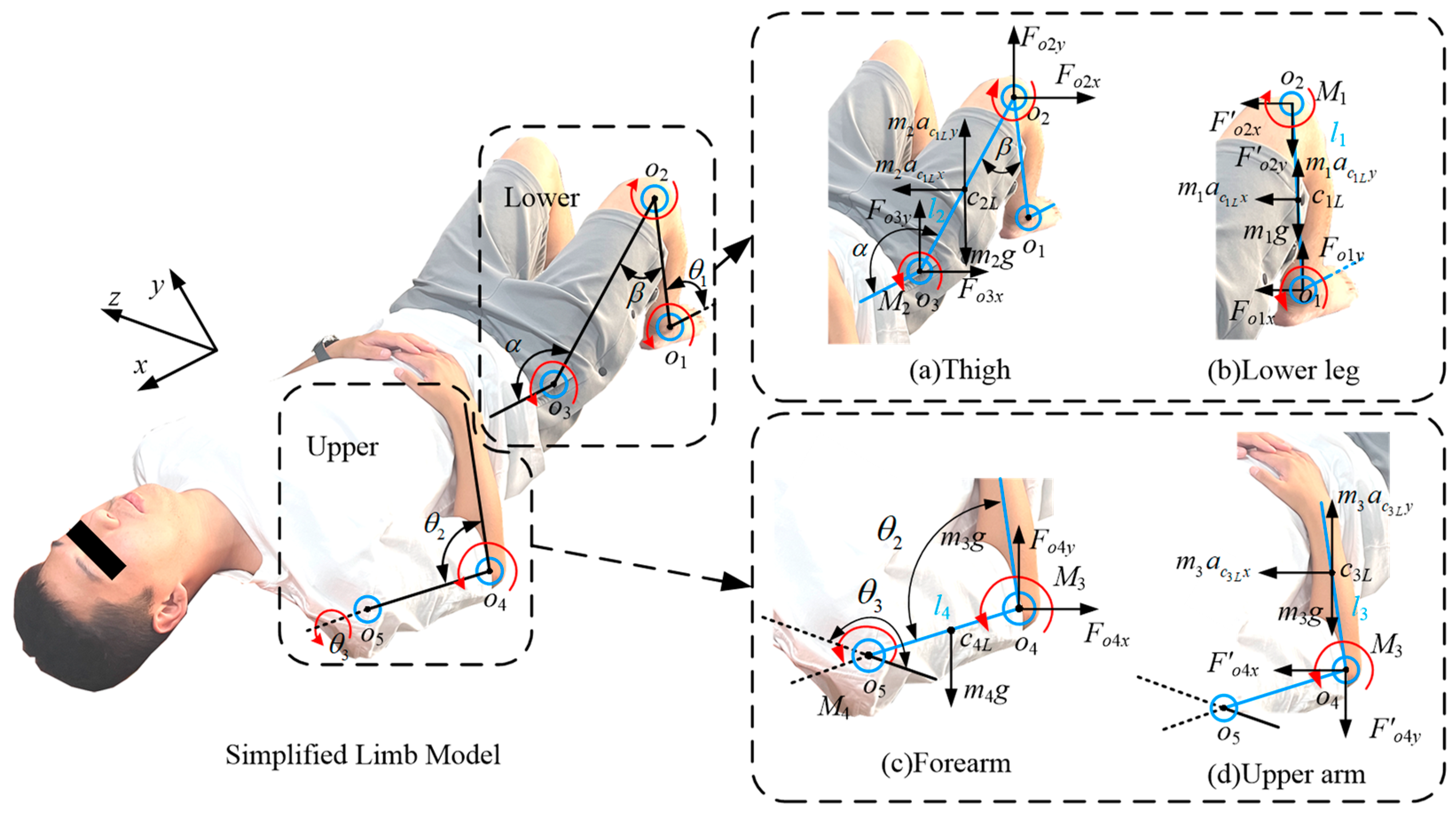
2.2. Modeling the Kinematics of Human Recumbent Limb Rehabilitation
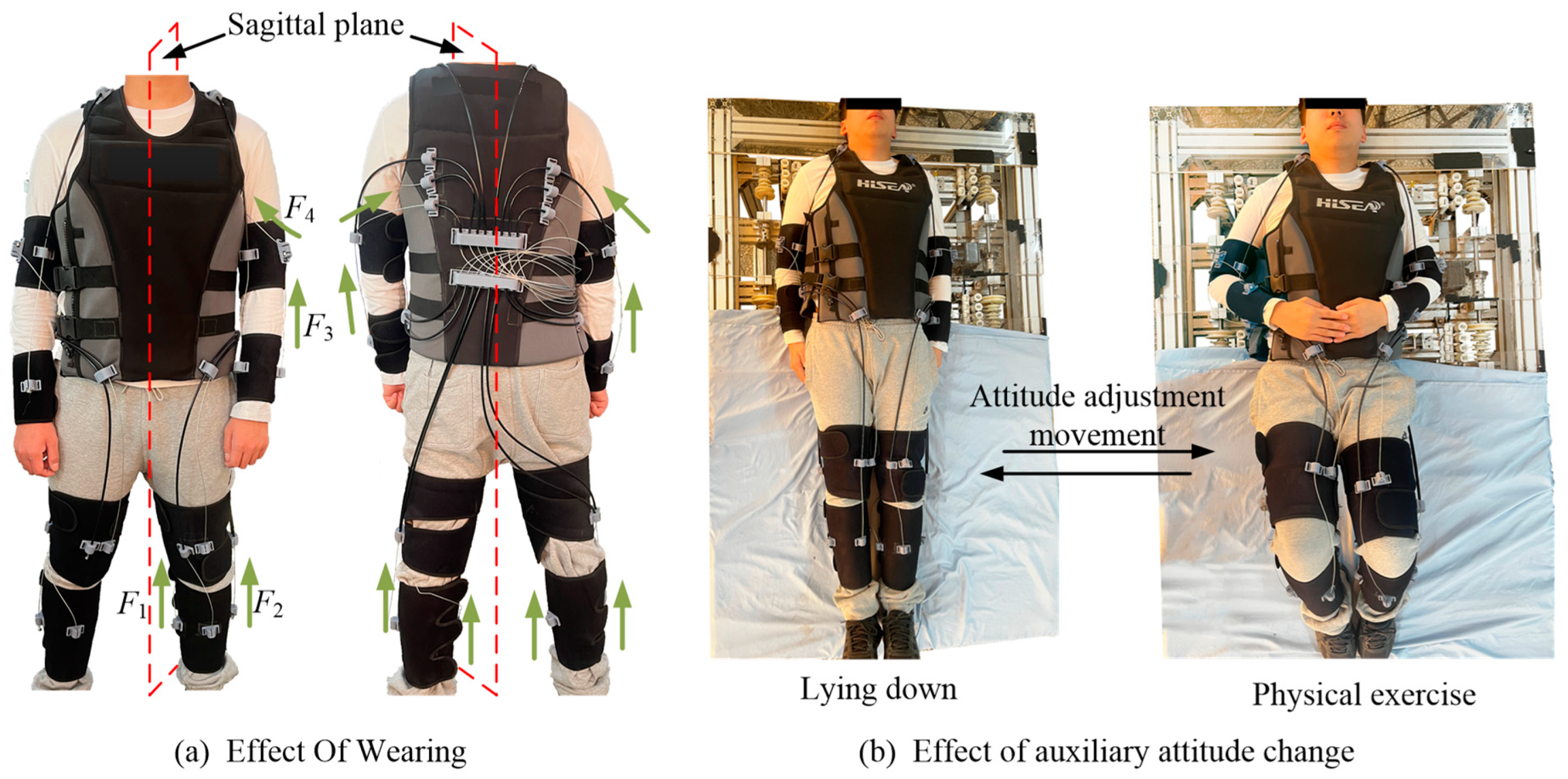
2.3. Design and Verification of a Wearable Multi-Posture Robot
3. Results
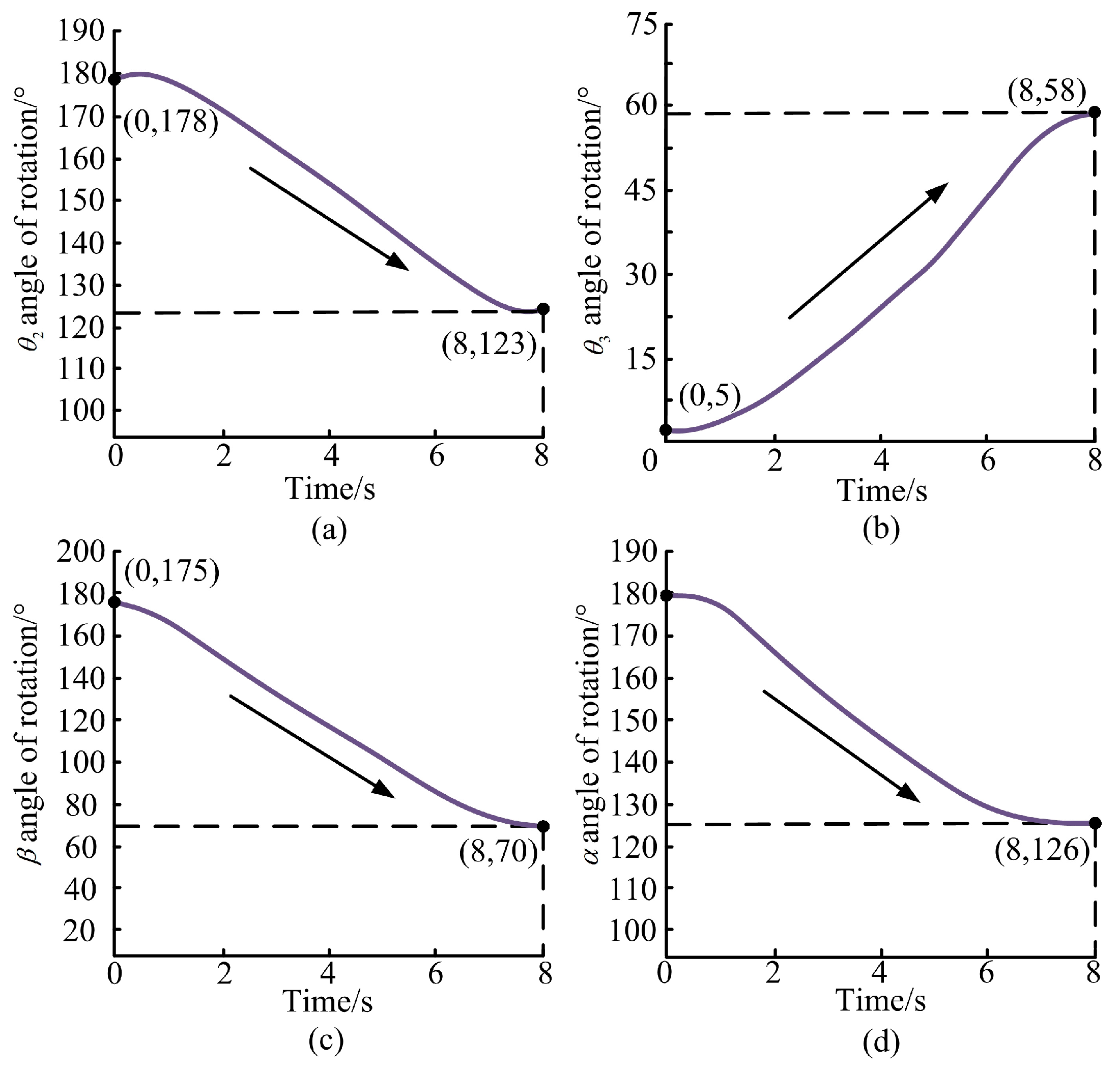
3.1. Theoretical Data Solution
3.2. Motion Capture and Force Sensing Experimental Analysis
3.3. Experimental Analysis of the Prototype of Recumbent Rehabilitation Training Device
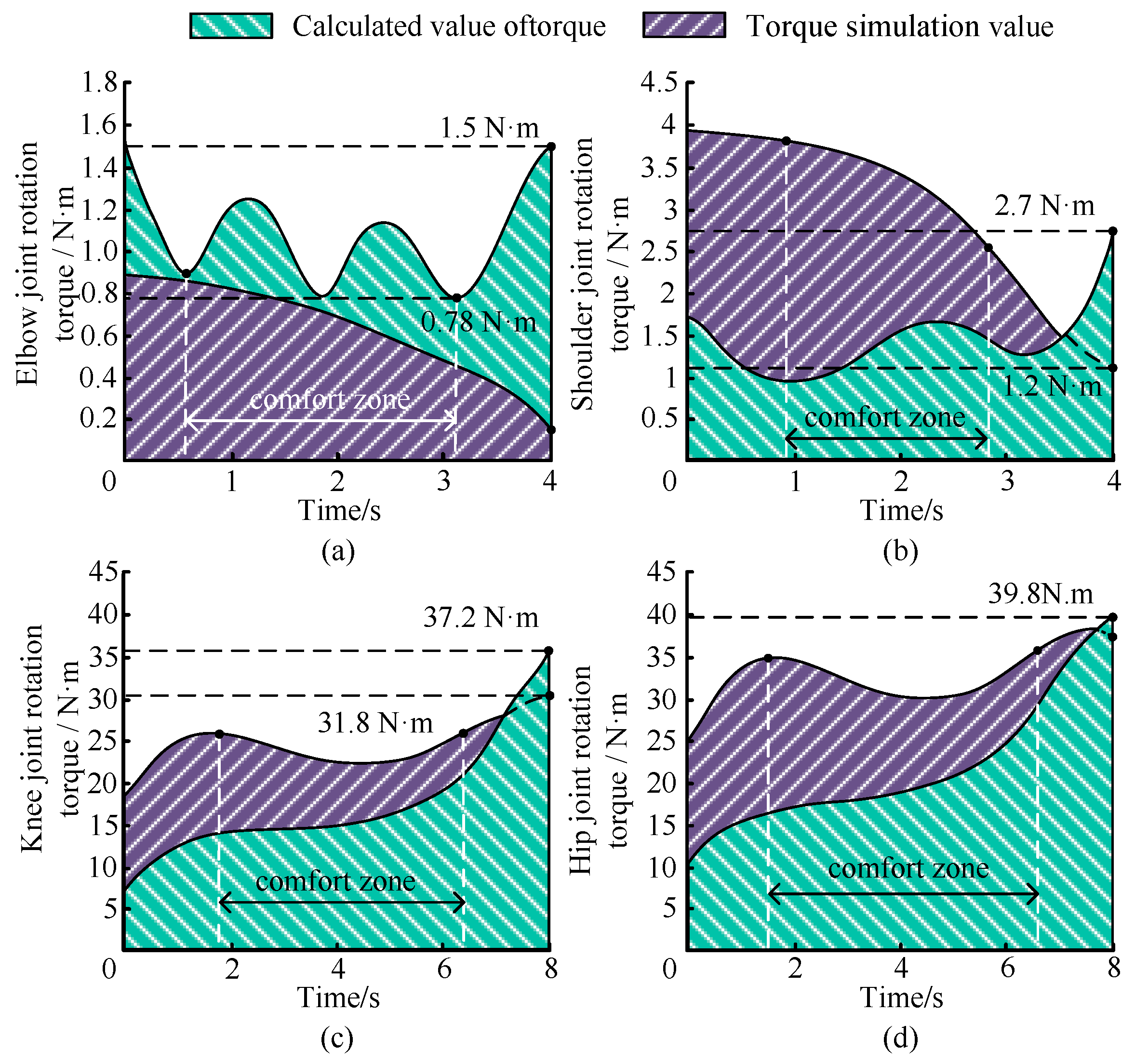
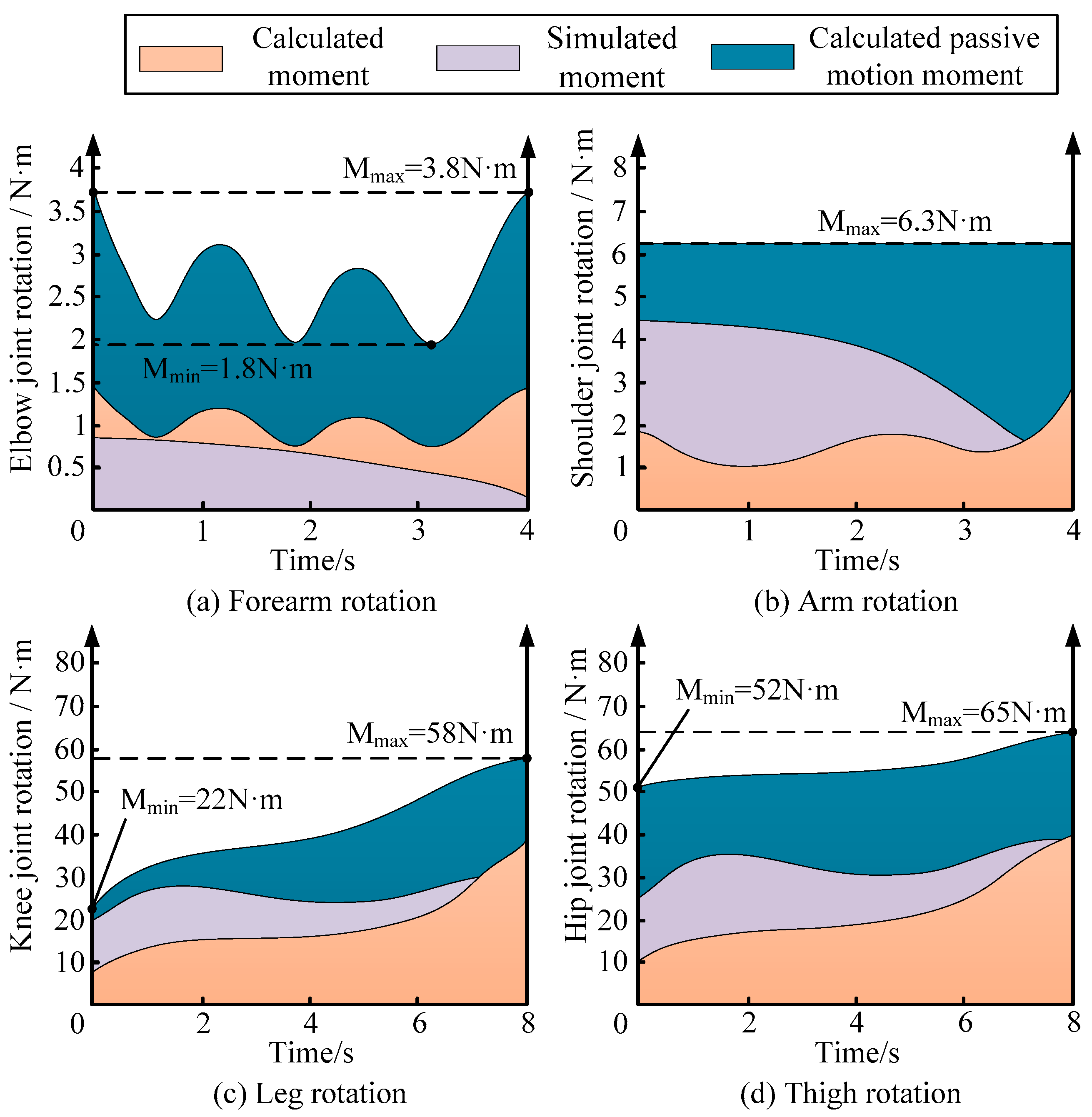
3.4. Verification
4. Discussion
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Trebbi, A.; Mukhina, E.; Rohan, P.-Y.; Connesson, N.; Bailet, M.; Perrier, A.; Payan, Y. MR-based quantitative measurement of human soft tissue internal strains for pressure ulcer prevention. Med. Eng. Phys. 2022, 108, 103888. [Google Scholar] [CrossRef]
- Sakamoto, D.; Hamaguchi, T.; Murata, K.; Ito, H.; Nakayama, Y.; Abo, M. Upper Limb Function Recovery by Combined Repetitive Transcranial Magnetic Stimulation and Occupational Therapy in Patients with Chronic Stroke According to Paralysis Severity. Brain Sci. 2023, 13, 284. [Google Scholar] [CrossRef]
- Fabulas, F.; Paisant, P.; Dinomais, M.; Mucci, S.; Casa, C.; Le Naoures, P.; Hamel, J.F.; Perrot, J.; Venara, A. Pre-habilitation before colorectal cancer surgery could improve postoperative gastrointestinal function recovery: A case-matched study. Langenbeck’s Arch. Surg. 2022, 407, 1595–1603. [Google Scholar] [CrossRef] [PubMed]
- Qassim, H.M.; Wan Hasan, W.Z. A review on upper limb rehabilitation robots. Appl. Sci. 2020, 10, 6976. [Google Scholar] [CrossRef]
- Fareh, R.; Elsabe, A.; Baziyad, M.; Kawser, T.; Brahmi, B.; Rahman, M.H. Will Your Next Therapist Be A Robot?—A Review of the Advancements in Robotic Upper Extremity Rehabilitation. Sensors 2023, 23, 5054. [Google Scholar] [CrossRef] [PubMed]
- Gu, J.; Xu, C.; Liu, K.; Zhao, L.; He, T.; Sun, Z. Impedance Control of Upper Limb Rehabilitation Robot Based on Series Elastic Actuator. In Proceedings of the International Conference on Intelligent Robotics and Applications, Harbin, China, 1–3 August 2022; Springer International Publishing: Cham, Switzerland, 2022; pp. 138–149. [Google Scholar]
- Akdoğan, E.; Adli, M.A. The design and control of a therapeutic exercise robot for lower limb rehabilitation: Physiotherabot. Mechatronics 2011, 21, 509–522. [Google Scholar] [CrossRef]
- Guzmán-Valdivia, C.; Blanco-Ortega, A.; Oliver-Salazar, M.; Gómez-Becerra, F.; Carrera-Escobedo, J. HipBot–The design, development, and control of a therapeutic robot for hip rehabilitation. Mechatronics 2015, 30, 55–64. [Google Scholar] [CrossRef]
- Yepes, J.C.; Rúa, S.; Osorio, M.; Pérez, V.Z.; Moreno, J.A.; Al-Jumaily, A.; Betancur, M.J. Human-Robot Interaction Torque Estimation Methods for a Lower Limb Rehabilitation Robotic System with Uncertainties. Appl. Sci. 2022, 12, 5529. [Google Scholar] [CrossRef]
- Pang, Z.; Wang, T.; Wang, Z.; Yu, J.; Sun, Z.; Liu, S. Design and analysis of a wearable upper limb rehabilitation robot with characteristics of tension mechanism. Appl. Sci. 2020, 10, 2101. [Google Scholar] [CrossRef]
- Jorge, D.R.; García, J.B.; Jayakumar, A.; Moreno, R.L.; Ortiz, R.A.; Sánchez, F.R. Force and torque characterization in the actuation of a walking-assistance, cable-driven exosuit. Sensors 2022, 22, 4309. [Google Scholar] [CrossRef]
- Li, Y.; Zi, B.; Yang, Z.; Ge, J. Combined kinematic and static analysis of an articulated lower limb traction device for a rehabilitation robotic system. Sci. China Technol. Sci. 2021, 64, 1189–1202. [Google Scholar] [CrossRef]
- Zhang, L.; Jiao, Z.; He, Y.; Su, P. Ergonomic design and performance evaluation of H-suit for human walking. Micromachines 2022, 13, 825. [Google Scholar] [CrossRef]
- Wu, X.; Bai, S.; O’Sullivan, L. Editorial for the special issue on wearable robots and intelligent device. Biomim. Intell. Robot. 2023, 3, 100102. [Google Scholar] [CrossRef]
- Lu, H.; Wang, H.B.; Feng, Y.F. Human-machine Coupling Dynamics Modeling and Active Compliance Control of Lower Limb Rehabilitation Robot. J. Mech. Eng. 2022, 58, 32–43. [Google Scholar]
- Sun, H.Y.; Zhang, L.X.; Wang, L. Dynamics modeling and control of horizontal lower limbs rehabilitation robot. Chin. High Technol. Lett. 2010, 6. [Google Scholar]
- Li, Y.; Zi, B.; Zhou, B.; Zhao, P.; Ge, Q.J. Cable angle and minimum resultant force response analysis of lower limb traction device for rehabilitation robot with interval parameters. J. Comput. Inf. Sci. Eng. 2021, 21, 021002. [Google Scholar] [CrossRef]
- Lang, A.E.; Kim, S.Y.; Milosavljevic, S.; Dickerson, C.R. The utility of the acromion marker cluster (AMC) in a clinical population. J. Electromyogr. Kinesiol. 2022, 62, 102298. [Google Scholar] [CrossRef]
- Andrews, J.G. Biomechanical analysis of human motion. Kinesiology 1974, 4, 32–42. [Google Scholar]
- Muscolino, J.E. Kinesiology-E-Book: The Skeletal System and Muscle Function; Elsevier Health Sciences: Amsterdam, The Netherlands, 2010. [Google Scholar]
- Jiang, D.; Liu, Z.; Ling, X.; Dai, J.; Long, L.; Lu, Y.; Zhou, S. Investigating the impact of inter-limb asymmetry in hamstring strength on jump, sprint, and strength performance in young athletes: Comparing the role of gross force. Front. Physiol. 2023, 14, 855. [Google Scholar] [CrossRef]
- Jin, Y.; Zhou, Y.M.; McCann, C.M.; Proietti, T.; Rycroft, C.H.; Walsh, C.J. A Data-based Approach to Simultaneously Align Local and Global Frames between an Inertial Measurement Unit (IMU) and an Optical Motion Capture System. In Proceedings of the 2022 9th IEEE RAS/EMBS International Conference for Biomedical Robotics and Biomechatronics (BioRob), Seoul, Republic of Korea, 21–24 August 2022; IEEE: Piscataway, NJ, USA, 2022; pp. 1–8. [Google Scholar]
- Zhang, L.; Song, G.; Zou, C.; Huang, R.; Cheng, H.; Hu, D. Modulation for Impact Reducing of Lower-Limb Exoskeletons. Micromachines 2022, 13, 816. [Google Scholar] [CrossRef]
- Liu, Y.; Su, P.; Lun, Q.; Zhang, Y.; Zhang, Q. Design and Simulation of a Flexible Mechanism for Wearable Assisted Posture Adjustment. In Proceedings of the 2023 IEEE 13th International Conference on CYBER Technology in Automation, Control, and Intelligent Systems (CYBER), Qinhuangdao, China, 11–14 July 2023; IEEE: Piscataway, NJ, USA, 2023; pp. 859–864. [Google Scholar]
- Li, Q.; Wang, S.; Wang, C.; Zhu, J. Editorial for the special issue on bio-inspired robotic dexterity intelligence. Biomim. Intell. Robot. 2024, 4, 100186. [Google Scholar] [CrossRef]
- Walsh, C. Human-in-the-loop development of soft wearable robots. Nat. Rev. Mater. 2018, 3, 78–80. [Google Scholar] [CrossRef]
- Chen, G.; Peng, W.; Wang, Z.; Tu, J.; Hu, H.; Wang, D.; Cheng, H.; Zhu, L. Modeling of swimming posture dynamics for a beaver-like robot. Ocean Eng. 2023, 279, 114550. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Body Part | Quantity/kg | Length/m |
|---|---|---|
| Calf | 2.6 | 0.37 |
| Thigh | 9.2 | 0.425 |
| Lower arm | 0.85 | 0.26 |
| Test Statistics | Shoulder | Elbow | Knee | Hip |
|---|---|---|---|---|
| t-test df | 45.2 | 47.8 | 52.3 | 55.6 |
| p-value | <0.0001 | <0.0001 | <0.0001 | <0.0001 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wu, Q.; Sun, C.; Liu, Y.; Wang, S.; Li, J.; Su, P. Design and Joint Dynamics of Human Recumbent Rehabilitation Training Devices. Electronics 2025, 14, 1724. https://doi.org/10.3390/electronics14091724
Wu Q, Sun C, Liu Y, Wang S, Li J, Su P. Design and Joint Dynamics of Human Recumbent Rehabilitation Training Devices. Electronics. 2025; 14(9):1724. https://doi.org/10.3390/electronics14091724
Chicago/Turabian StyleWu, Qiulong, Chaoyue Sun, Yi Liu, Sikai Wang, Jian Li, and Peng Su. 2025. "Design and Joint Dynamics of Human Recumbent Rehabilitation Training Devices" Electronics 14, no. 9: 1724. https://doi.org/10.3390/electronics14091724
APA StyleWu, Q., Sun, C., Liu, Y., Wang, S., Li, J., & Su, P. (2025). Design and Joint Dynamics of Human Recumbent Rehabilitation Training Devices. Electronics, 14(9), 1724. https://doi.org/10.3390/electronics14091724