
Cognitive Cardiac Assessment Using Low-Cost Electrocardiogram Acquisition System


Abstract
1. Introduction
- -
- An ECG acquisition system for cognitive load analysis is developed based on a low-cost device and graphical interface, in order to control and store the recorded data on cloud storage.
- -
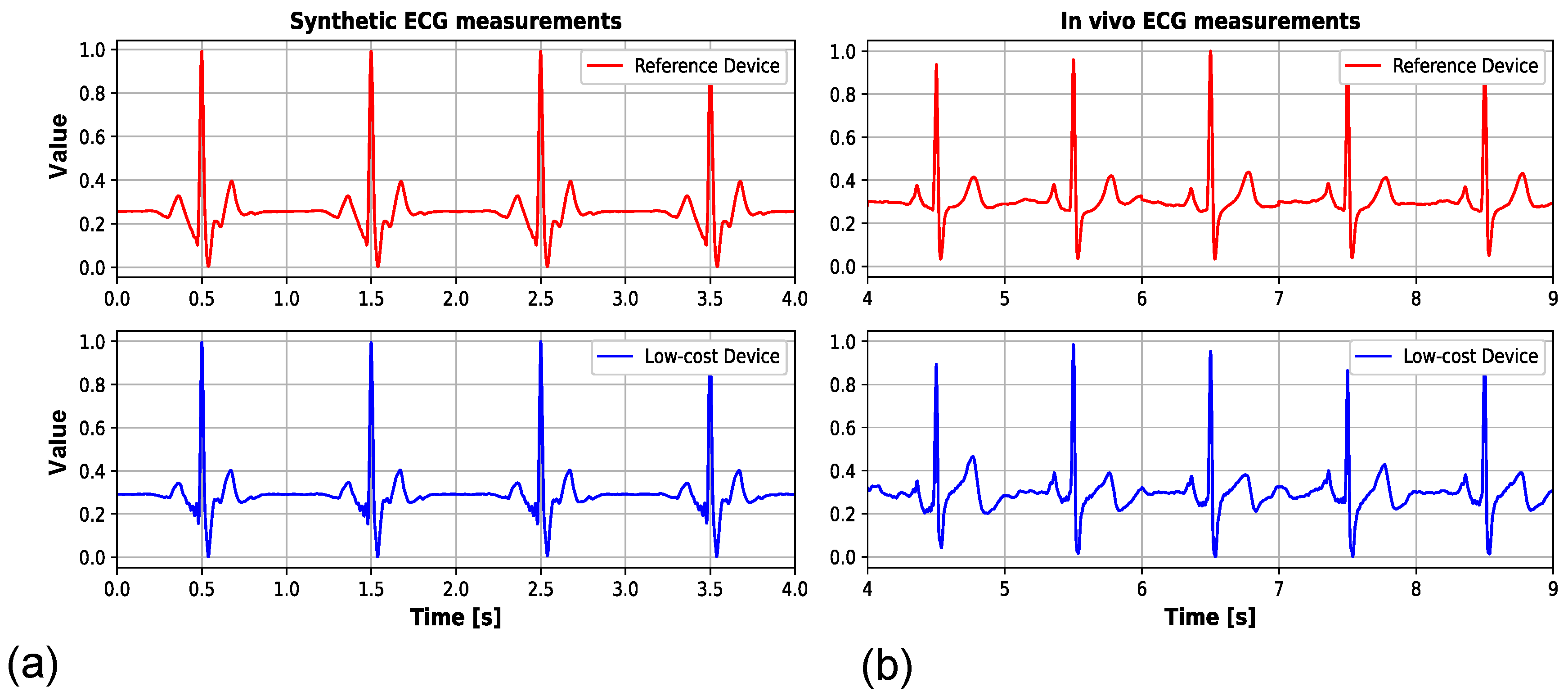
- The signal acquisition is analyzed using the low-budget device synchronously with the reference professional acquisition medical device, where signals originate from both the ECG signal generator and healthy volunteers.
- -
- The novel ECG-only cognitive load examination is performed using the device and the Stroop test.
- -
- The new classification method for the ECG-based cognitive load presence via Shannon entropy and multifractal total variation features is proposed.
- -
- The proposed classification model applies a relatively small number of features.
2. Related Works
2.1. Related Works on ECG-Based Cardiac Monitoring Devices
2.2. Related Works on Cognitive Load Examination Using Cardiac Data
3. Materials and Methods
3.1. Description of Low-Cost Monitoring Device and Synthetic Data Acquisition
3.2. Reference Device-Based Performance Assessment
3.3. Cognitive Load
3.4. Cognitive Load Detection Using Multifractal Features and Machine Learning
4. Experimental Results
4.1. Initial Performance Assessment of Low-Cost Monitoring Device
4.2. Cognitive Load-Dependant Usage of the Low-Cost Device
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Alahi, M.E.E.; Sukkuea, A.; Tina, F.W.; Nag, A.; Kurdthongmee, W.; Suwannarat, K.; Mukhopadhyay, S.C. Integration of IoT-Enabled Technologies and Artificial Intelligence (AI) for Smart City Scenario: Recent Advancements and Future Trends. Sensors 2023, 23, 5206. [Google Scholar] [CrossRef] [PubMed]
- Gatouillat, A.; Badr, Y.; Massot, B.; Sejdic, E. Internet of Medical Things: A Review of Recent Contributions Dealing with Cyber-Physical Systems in Medicine. IEEE Internet Things J. 2018, 5, 3810–3822. [Google Scholar] [CrossRef]
- Yang, X.-L.; Liu, G.-Z.; Tong, Y.-H.; Yan, H.; Xu, Z.; Chen, Q.; Liu, X.; Zhang, H.-H.; Wang, H.-B.; Tan, S.-H. The History, Hotspots, and Trends of Electrocardiogram. PubMed 2015, 12, 448–456. [Google Scholar] [CrossRef]
- Jeon, B.; Lee, J.; Choi, J. Design and implementation of a wearable ECG system. Int. J. Smart Home 2013, 7, 61–70. [Google Scholar]
- Goldberger, A.L.; Amaral, L.A.N.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.-K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet. Circulation 2000, 101, E215–E220. [Google Scholar] [CrossRef]
- Sahoo, S.S.; Jayapandian, C.; Garg, G.; Kaffashi, F.; Chung, S.; Bozorgi, A.; Chen, C.-H.; Loparo, K.; Lhatoo, S.D.; Zhang, G.-Q. Heart Beats in the Cloud: Distributed Analysis of Electrophysiological ‘Big Data’ Using Cloud Computing for Epilepsy Clinical Research. J. Am. Med. Inform. Assoc. 2013, 21, 263–271. [Google Scholar] [CrossRef]
- Sun, J.-Y.; Shen, H.; Qu, Q.; Sun, W.; Kong, X.-Q. The Application of Deep Learning in Electrocardiogram: Where We Came from and Where We Should Go? Int. J. Cardiol. 2021, 337, 71–78. [Google Scholar] [CrossRef]
- Friedman, P.A. The Electrocardiogram at 100 Years: History and Future. Circulation 2024, 149, 411–413. [Google Scholar] [CrossRef]
- Anbalagan, T.; Nath, M.K.; Vijayalakshmi, D.; Anbalagan, A. Analysis of Various Techniques for ECG Signal in Healthcare, Past, Present, and Future. Biomed. Eng. Adv. 2023, 6, 100089. [Google Scholar] [CrossRef]
- Samartkit, P.; Pullteap, S. Non-Invasive Continuous Blood Pressure Sensors in Biomedical Engineering Research: A Review. Sens. Actuators A Phys. 2024, 367, 115084. [Google Scholar] [CrossRef]
- Rafie, N.; Kashou, A.H.; Noseworthy, P.A. ECG Interpretation: Clinical Relevance, Challenges, and Advances. Hearts 2021, 2, 505–513. [Google Scholar] [CrossRef]
- Fye, W.B. A History of the Origin, Evolution, and Impact of Electrocardiography. Am. J. Cardiol. 1994, 73, 937–949. [Google Scholar] [CrossRef] [PubMed]
- Kashou, A.H.; Ko, W.-Y.; Attia, Z.I.; Cohen, M.S.; Friedman, P.A.; Noseworthy, P.A. A Comprehensive Artificial Intelligence–Enabled Electrocardiogram Interpretation Program. Cardiovasc. Digit. Health J. 2020, 1, 62–70. [Google Scholar] [CrossRef] [PubMed]
- Brad, R.; Ilie, B.; Florea, A.; Berntzen, L.; Teodoru, M. IoT Device for Long-Term ECG Monitoring in Collaborative Environment. J. Artif. Intell. Auton. Intell. 2024, 1, 82–95. [Google Scholar] [CrossRef]
- Jiao, W.; Wang, J.; Gao, X.; Du, L.; Li, Y.; Zhao, L.; Fang, D.; Chen, X. ZEROECG: Zero-Sensation ECG Monitoring by Exploring RFID MOSFET. In Proceedings of the ACM MobiCom ’24: Proceedings of the 30th Annual International Conference on Mobile Computing and Networking, Washington, DC, USA, 18–22 November 2024; pp. 1237–1251. [Google Scholar] [CrossRef]
- Singh, R.; Rajpal, N.; Soni, P.K.; Upadhyay, G.M. An AIOT Enabled Multi-Level Decision Support System for Remote Arrhythmia Analysis Using Efficient Wavelet Transform. SN Comput. Sci. 2024, 5, 1121. [Google Scholar] [CrossRef]
- Zovko, K.; Šerić, L.; Perković, T.; Belani, H.; Šolić, P. IoT and Health Monitoring Wearable Devices as Enabling Technologies for Sustainable Enhancement of Life Quality in Smart Environments. J. Clean. Prod. 2023, 413, 137506. [Google Scholar] [CrossRef]
- Yang, Z.; Zhou, Q.; Lei, L.; Zheng, K.; Xiang, W. An IoT-Cloud Based Wearable ECG Monitoring System for Smart Healthcare. J. Med. Syst. 2016, 40, 286. [Google Scholar] [CrossRef]
- Zhang, Y.; Liu, H.; Su, X.; Jiang, P.; Wei, D. Remote Mobile Health Monitoring System Based on Smart Phone and Browser/Server Structure. J. Healthc. Eng. 2015, 6, 717–738. [Google Scholar] [CrossRef]
- Assaad, R.H.; Mohammadi, M.; Poudel, O. Developing an Intelligent IoT-Enabled Wearable Multimodal Biosensing Device and Cloud-Based Digital Dashboard for Real-Time and Comprehensive Health, Physiological, Emotional, and Cognitive Monitoring Using Multi-Sensor Fusion Technologies. Sens. Actuators A Phys. 2024, 381, 116074. [Google Scholar] [CrossRef]
- Giordano, M.; Leitner, C.; Vogt, C.; Benini, L.; Magno, M. PULSE: Accurate and Robust Ultrasound-Based Continuous Heart-Rate Monitoring on a Wrist-Worn IoT Device. arXiv 2024, arXiv:2410.16219. [Google Scholar] [CrossRef]
- Zhu, G.; Wang, X.; Zhang, G.; Yue, Y.; Yuan, S.; Du, H.; Zhang, Z.; Ren, F.; Ren, P.; Sun, Q. Multifunctional Flexible Sensor with the Hybrid Staggered-Rib Conductive Network for Intelligent Recognition of Human Biomechanical and Electrophysiological Signals. ACS Appl. Nano Mater. 2024, 7, 24061–24070. [Google Scholar] [CrossRef]
- Alegre, L.M.; Pisarello, M.I. Ambulatory Electrocardiographic Monitoring Prototype. In Proceedings of the 2024 IEEE Biennial Congress of Argentina (ARGENCON), San Nicolás de los Arroyos, Argentina, 18–20 September 2024; pp. 1–6. [Google Scholar] [CrossRef]
- Wang, W.; Lu, L.; Ma, H.; Li, Z.; Lu, X.; Xie, Y. Self-Template Manufacturing of on-Skin Electrodes with 3D Multi-Channel Structure for Standard 3-Limb-Lead ECG Suit. Microsyst. Nanoeng. 2024, 10, 196. [Google Scholar] [CrossRef]
- Schramm, D.; Varini, R.; Gala, A.B.E.; Banerjee, A.; Betts, T. Comprehensive Cardiac Interval Analysis in the WEAR-TECH Study Cohort by Comparing the Apple Watch Series 6 against a Simultaneous 12-Lead ECG. Eur. Heart J. 2024, 45, ehae666.353. [Google Scholar] [CrossRef]
- Madavarapu, J.B.; Nachiyappan, S.; Rajarajeswari, S.; Anusha, N.; Venkatachalam, N.; Madavarapu, R.C.B.; Ahilan, A. Hot Watch: IOT Based Wearable Health Monitoring System. IEEE Sens. J. 2024, 24, 33252–33259. [Google Scholar] [CrossRef]
- Vizitiu, C.; Bîră, C.; Dinculescu, A.; Nistorescu, A.; Marin, M. Exhaustive Description of the System Architecture and Prototype Implementation of an IoT-Based eHealth Biometric Monitoring System for Elders in Independent Living. Sensors 2021, 21, 1837. [Google Scholar] [CrossRef]
- Scrugli, M.A.; Loi, D.; Raffo, L.; Meloni, P. An Adaptive Cognitive Sensor Node for ECG Monitoring in the Internet of Medical Things. IEEE Access 2021, 10, 1688–1705. [Google Scholar] [CrossRef]
- Dankovich, L.J.; Joyner, J.S.; He, W.; Sesay, A.; Vaughn-Cooke, M. CogWatch: An Open-Source Platform to Monitor Physiological Indicators for Cognitive Workload and Stress. HardwareX 2024, 19, e00538. [Google Scholar] [CrossRef]
- Pavlov, Y.G.; Kasanov, D.; Kosachenko, A.I.; Kotyusov, A.I.; Busch, N.A. Pupillometry and Electroencephalography in the Digit Span Task. Sci. Data 2022, 9, 325. [Google Scholar] [CrossRef]
- Parent, M.; Albuquerque, I.; Tiwari, A.; Cassani, R.; Gagnon, J.-F.; Lafond, D.; Tremblay, S.; Falk, T.H. PASS: A Multimodal Database of Physical Activity and Stress for Mobile Passive Body/Brain-Computer Interface Research. Front. Neurosci. 2020, 14, 542934. [Google Scholar] [CrossRef]
- Esgalhado, F.; Batista, A.; Vassilenko, V.; Russo, S.; Ortigueira, M. Peak Detection and HRV Feature Evaluation on ECG and PPG Signals. Symmetry 2022, 14, 1139. [Google Scholar] [CrossRef]
- Hemakom, A.; Atiwiwat, D.; Israsena, P. ECG and EEG Based Detection and Multilevel Classification of Stress Using Machine Learning for Specified Genders: A Preliminary Study. PLoS ONE 2023, 18, e0291070. [Google Scholar] [CrossRef]
- Wu, N.M.; Cao, N.H.; Nguyen, N.H.-L.; Surmacz, K.; Hargrove, C. Modeling Perceived Stress via HRV and Accelerometer Sensor Streams. In Proceedings of the 37th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Milan, Italy, 25–29 August 2015; pp. 1625–1628. [Google Scholar] [CrossRef]
- Masrur, N.; Halder, N.; Rashid, S.; Setu, J.H.; Islam, A.; Ahmed, T. Performance Analysis of Ensemble and DNN Models for Decoding Mental Stress Utilizing ECG-Based Wearable Data Fusion. In Proceedings of the 2024 IEEE International Black Sea Conference on Communications and Networking, Tbilisi, Georgia, 24–27 June 2024; pp. 276–279. [Google Scholar] [CrossRef]
- Heyat, M.B.B.; Akhtar, F.; Abbas, S.J.; Al-Sarem, M.; Alqarafi, A.; Stalin, A.; Abbasi, R.; Muaad, A.Y.; Lai, D.; Wu, K. Wearable Flexible Electronics Based Cardiac Electrode for Researcher Mental Stress Detection System Using Machine Learning Models on Single Lead Electrocardiogram Signal. Biosensors 2022, 12, 427. [Google Scholar] [CrossRef]
- Hasnul, M.A.; Aziz, N.A.A.; Alelyani, S.; Mohana, M.; Aziz, A.A. Electrocardiogram-Based Emotion Recognition Systems And Their Applications in Healthcare—A Review. Sensors 2021, 21, 5015. [Google Scholar] [CrossRef] [PubMed]
- Butkevičiūtė, E.; Michalkovič, A.; Bikulčienė, L. ECG Signal Features Classification for the Mental Fatigue Recognition. Mathematics 2022, 10, 3395. [Google Scholar] [CrossRef]
- Tjolleng, A.; Pramudita, N.D. A Review of Driver Cognitive Load Detection Using ECG Signals. SHS Web Conf. 2024, 189, 01008. [Google Scholar] [CrossRef]
- Amin, M.; Ullah, K.; Asif, M.; Waheed, A.; Haq, S.U.; Zareei, M.; Biswal, R.R. ECG-Based Driver’s Stress Detection Using Deep Transfer Learning and Fuzzy Logic Approaches. IEEE Access 2022, 10, 29788–29809. [Google Scholar] [CrossRef]
- Amancharla, A.; Shanbhag, A.A.; Sunitha, R. Analysis of EEG and ECG Time Series in Response to Olfactory and Cognitive Tasks. Procedia Comput. Sci. 2024, 235, 745–756. [Google Scholar] [CrossRef]
- Milivojević, M.; Dujković, D.; Luković, A.; Gavrovska, A. Entropy Analysis of Electrocardiograms for Cognitive Performance Evaluation. In Proceedings of the 2024 32nd Telecommunications Forum (TELFOR), Belgrade, Serbia, 26–27 November 2024; pp. 1–4. [Google Scholar] [CrossRef]
- Grzeszczyk, M.K.; Blanco, R.; Adamczyk, P.; Kus, M.; Marek, S.; Pręcikowski, R.; Lisowska, A. CogWear: Can we detect cognitive effort with consumer-grade wearables? (version 1.0.0). PhysioNet 2023, RRID:SCR_007345. [Google Scholar] [CrossRef]
- Islam, M.R.; Kabir, M.M.; Mridha, M.F.; Alfarhood, S.; Safran, M.; Che, D. Deep Learning-Based IoT System for Remote Monitoring and Early Detection of Health Issues in Real-Time. Sensors 2023, 23, 5204. [Google Scholar] [CrossRef]
- Pash, A.; Nagaraja, S.R. An Efficient ECG Monitoring System using MQTT Protocol for Remote Patients in an IoT System. Int. J. Intell. Syst. Appl. Eng. 2023, 12, 146–153. [Google Scholar]
- Grassini, S. Electrochemical Impedance Spectroscopy (EIS) for the in-Situ Analysis of Metallic Heritage Artefacts. In Corrosion and Conservation of Cultural Heritage Metallic Artefacts; Elsevier: Amsterdam, The Netherlands, 2013; pp. 347–367. [Google Scholar]
- ECG Top D/BT—Medset. n.d. Available online: https://www.medset.com/en/products/resting-ecg/3148-2-2-2 (accessed on 11 May 2025).
- PADSY ECG-Management—Medset. n.d. Available online: https://www.medset.com/en/krankenhausmanagement (accessed on 11 May 2025).
- Mautgreve, W.; Klunker, C.; Zywietz, C. HES EKG expert-an expert system for comprehensive ECG analysis and teaching. In Proceedings of the Computers in Cardiology, Jerusalem, Israel, 19–22 September 1989; pp. 77–80. [Google Scholar] [CrossRef]
- Kim, S.; Kim, H. A New Metric of Absolute Percentage Error for Intermittent Demand Forecasts. Int. J. Forecast. 2016, 32, 669–679. [Google Scholar] [CrossRef]
- Stroop, J.R. Studies of Interference in Serial Verbal Reactions. J. Exp. Psychol. 1935, 18, 643–662. [Google Scholar] [CrossRef]
- MacLeod, C.M. Half a Century of Research on the Stroop Effect: An Integrative Review. Psychol. Bull. 1991, 109, 163–203. [Google Scholar] [CrossRef] [PubMed]
- Koch, C. Self-Monitoring, Need for Cognition, and the Stroop Effect: A Preliminary Study. Percept. Mot. Ski. 2003, 96, 212–214. [Google Scholar] [CrossRef] [PubMed]
- Banich, M.T.; Milham, M.P.; Atchley, R.A.; Cohen, N.J.; Webb, A.; Wszalek, T.; Kramer, A.F.; Liang, Z.-P.; Barad, V.; Gullett, D.; et al. Prefrontal Regions Play a Predominant Role in Imposing an Attentional ‘Set’: Evidence from fMRI. Cogn. Brain Res. 2000, 10, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Peirce, J.; Gray, J.R.; Simpson, S.; MacAskill, M.; Höchenberger, R.; Sogo, H.; Kastman, E.; Lindeløv, J.K. PsychoPy2: Experiments in Behavior Made Easy. Behav. Res. Methods 2019, 51, 195–203. [Google Scholar] [CrossRef]
- Glenny, R.W.; Robertson, H.T.; Yamashiro, S.; Bassingthwaighte, J.B. Applications of Fractal Analysis to Physiology. J. Appl. Physiol. 1991, 70, 2351–2367. [Google Scholar] [CrossRef]
- Chen, Y. Fractal Modeling and Fractal Dimension Description of Urban Morphology. Entropy 2020, 22, 961. [Google Scholar] [CrossRef]
- Mandelbrot, B.B.; Wheeler, J.A. The Fractal Geometry of Nature. Am. J. Phys. 1983, 51, 286–287. [Google Scholar] [CrossRef]
- Dubrulle, B. Multi-Fractality, Universality and Singularity in Turbulence. Fractal Fract. 2022, 6, 613. [Google Scholar] [CrossRef]
- Vehel, J.L.; Rams, M. Large Deviation Multifractal Analysis of a Class of Additive Processes with Correlated Nonstationary Increments. IEEE/ACM Trans. Netw. 2013, 21, 1309–1321. [Google Scholar] [CrossRef]
- Christophe, C.; Véhel, J.L.; Tricot, C. Continuous Large Deviation Multifractal Spectrum: Definition and Estimation. In Proceedings of the Fractals 98, Valletta, Malta, 25–28 October 1998. [Google Scholar]
- Guével, R.L.; Véhel, J.L. Hausdorff, Large Deviation and Legendre Multifractal Spectra of Lévy Multistable Processes. Stoch. Process. Their Appl. 2019, 130, 2032–2057. [Google Scholar] [CrossRef]
- Ihlen, E.A.F. Multifractal Analyses of Response Time Series: A Comparative Study. Behav. Res. Methods 2013, 45, 928–945. [Google Scholar] [CrossRef] [PubMed]
- Gavrovska, A. Effects on Long-Range Dependence and Multifractality in Temporal Resolution Recovery of High Frame Rate HEVC Compressed Content. Appl. Sci. 2023, 13, 9851. [Google Scholar] [CrossRef]
- Karahanoglu, F.I.; Bayram, İ.; Van De Ville, D. A Signal Processing Approach to Generalized 1-D Total Variation. IEEE Trans. Signal Process. 2011, 59, 5265–5274. [Google Scholar] [CrossRef]
- Chethan, C. Prediction of Heart Disease Using Different KNN Classifier. In Proceedings of the 6th International Conference on Intelligent Computing and Control Systems (ICICCS), Madurai, India, 6–8 May 2021; pp. 1186–1194. [Google Scholar] [CrossRef]
- Cover, T.; Hart, P. Nearest Neighbor Pattern Classification. IEEE Trans. Inf. Theory 1967, 13, 21–27. [Google Scholar] [CrossRef]
- Shdefat, A.Y.; Mostafa, N.; Al-Arnaout, Z.; Kotb, Y.; Alabed, S. Optimizing HAR Systems: Comparative Analysis of Enhanced SVM and K-NN Classifiers. Int. J. Comput. Intell. Syst. 2024, 17, 150. [Google Scholar] [CrossRef]
- Vazan, R.; Filcikova, D.; Mravec, B. Effect of the Stroop Test Performed in Supine Position on the Heart Rate Variability in Both Genders. Auton. Neurosci. 2017, 208, 156–160. [Google Scholar] [CrossRef]
- Miller, K.M.; Price, C.C.; Okun, M.S.; Montijo, H.; Bowers , D. Is the N-Back Task a Valid Neuropsychological Measure for Assessing Working Memory? Arch. Clin. Neuropsychol. 2009, 24, 711–717. [Google Scholar] [CrossRef]
- Hoffmann, U.; Vesin, J.M.; Ebrahimi, T.; Diserens, K. An efficient P300-based brain-computer interface for disabled subjects. J. Neurosci. Methods 2008, 167, 115–125. [Google Scholar] [CrossRef]
- Olimex Shield EKG-EMG. Available online: https://www.olimex.com/Products/Duino/Shields/SHIELD-EKG-EMG/ (accessed on 5 June 2025).
- Artífice, A.; Ferreira, F.; Marcelino-Jesus, E.; Sarraipa, J.; Jardim-Gonçalves, R. Student’s Attention Improvement Supported by Physiological Measurements Analysis. In Technological Innovation for Smart Systems; IFIP Advances in Information and Communication Technology; Springer: Cham, Switzerland, 2017; pp. 93–102. [Google Scholar]
- Ehrmann, G.; Blachowicz, T.; Homburg, S.V.; Ehrmann, A. Measuring Biosignals with Single Circuit Boards. Bioengineering 2022, 9, 84. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| No. | Solutions | Technology/Hardware | Cost | Advantages | Challenges |
|---|---|---|---|---|---|
| 1 | Arduino-based prototype/DIY solutions | ARM Cortex-M4 + AD8232 Module [18,26,41] * | Low-cost components included | Front-end for analog circuit design | Complex initial setup |
| Olimex ECG/EMG Shield + Arduino Uno [42] | Low-cost components included | Open-source hardware for simple initial setup | Plug-and-play experience with possible lower performance | ||
| ADS1293 Module + Arduino/MCU [24] | Low-cost components included | Powerful and cost-effective solution | Advanced component-level integration | ||
| 2 | Consumer- and professional-grade solutions | Zephyr BioHarness sensor and multimodal approach [19,29,31], Polar H10 [21], Apple Watch Series 6 [25,35], Empatica E4 wristband, Samsung Galaxy Watch4 and Muse S EEG headband [43] ** | Mid-cost components included | Accessibility of commercial solutions and plug-and-play experience | Not intended for diagnostics with possible limited data access |
| 3 | Medical- and clinical-grade solutions | eego™ 8 ANT neuro [33], ActiCHamp 64-channels EEG system with active electrodes [30] | High-cost components included | Medical certification and specialized ecosystem | High-cost and less portable |
| No. | Characteristics | Brief Explanation |
|---|---|---|
| 1 | HRV temporal measures | Mean RR interval, standard deviation of RR intervals, Root Mean Square of Successive Differences (RMSSD), pNN50 (percentage of NN intervals > 50 ms) |
| 2 | Shannon entropy | Entropy provides a measure of the complexity or irregularity of a signal (ShEn) |
| 3 | MF spectrum extrema | Analysis of extreme values in a multifractal spectrum, local and global minima and maxima |
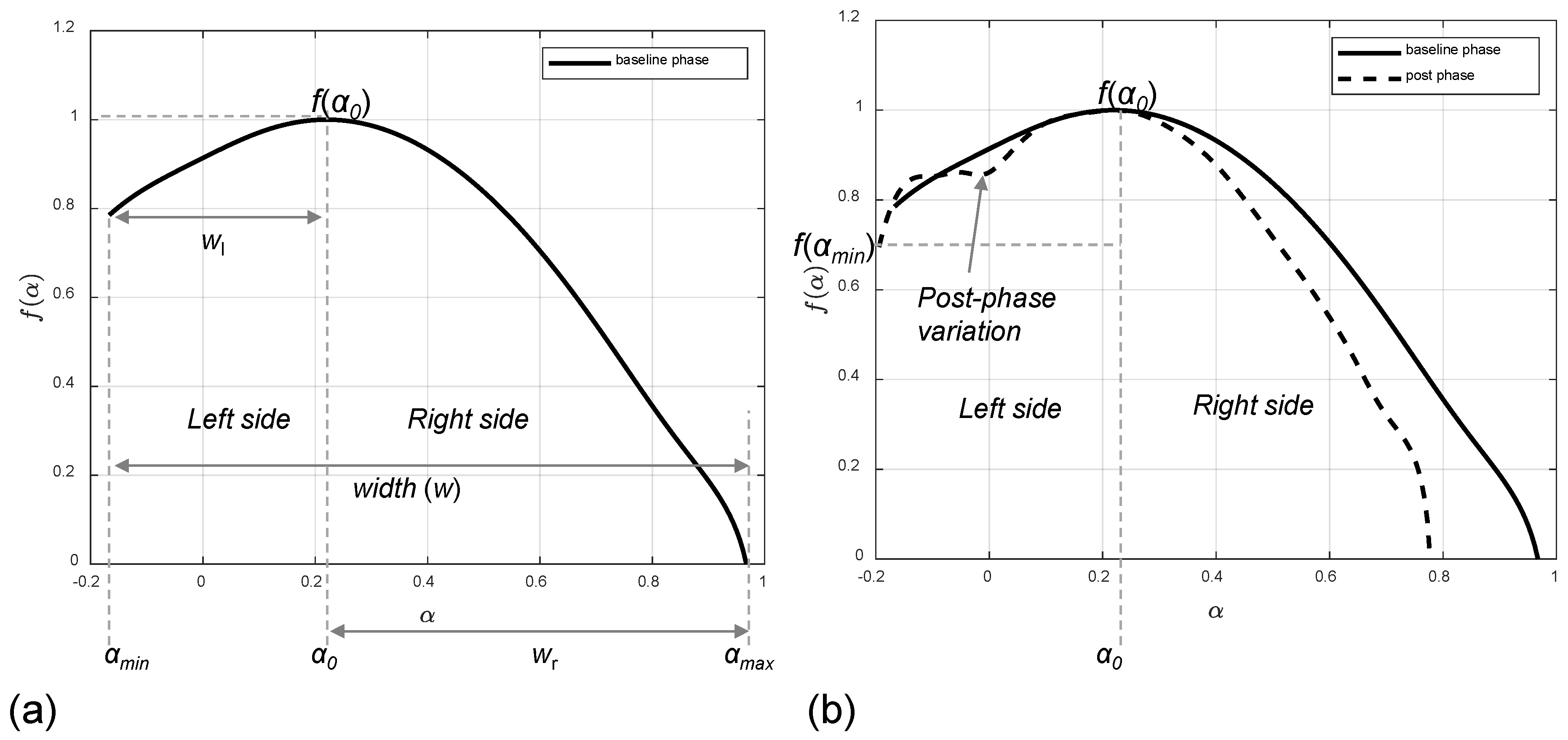
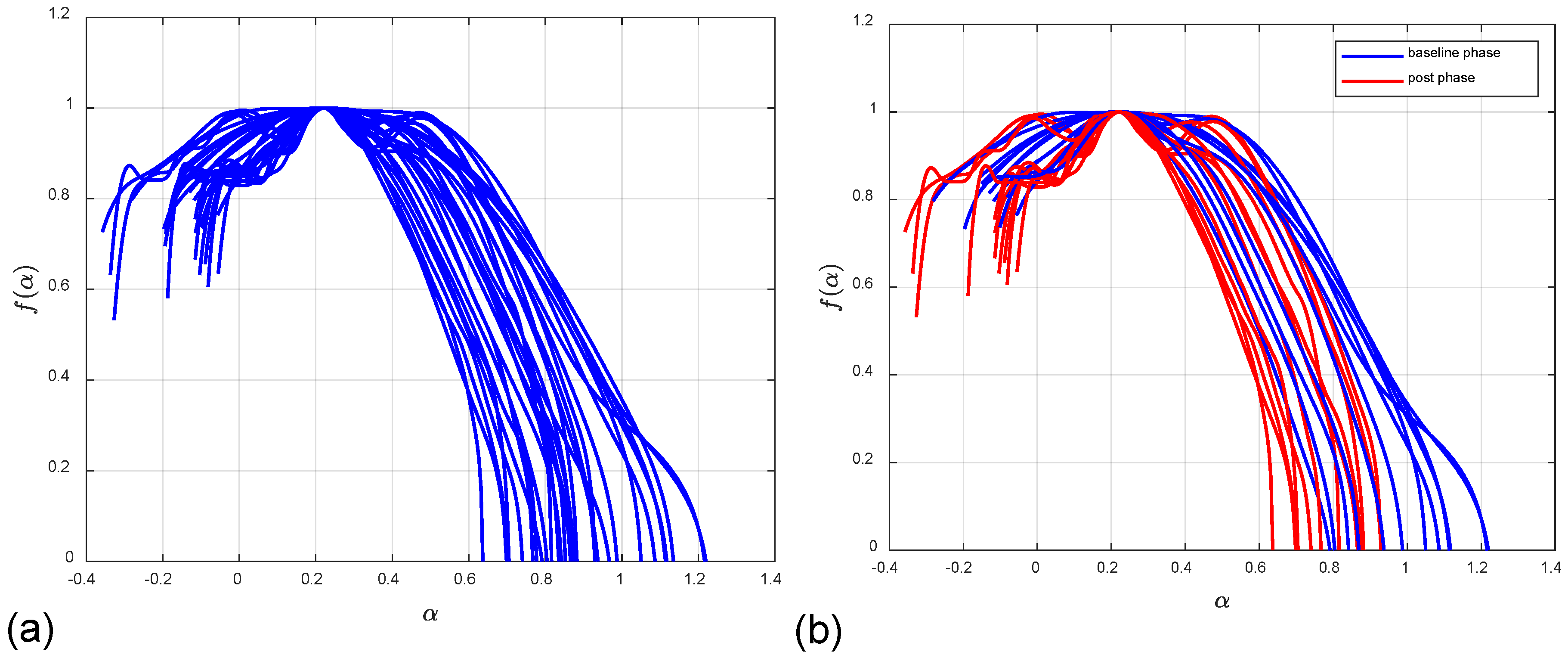
| 4 | Widths | Analysis of the multifractal spectrum’s width, examining both the total width and the widths of its left and right sides individually |
| 5 | Slopes | Analysis of the slope of the left and right sides of a multifractal spectrum |
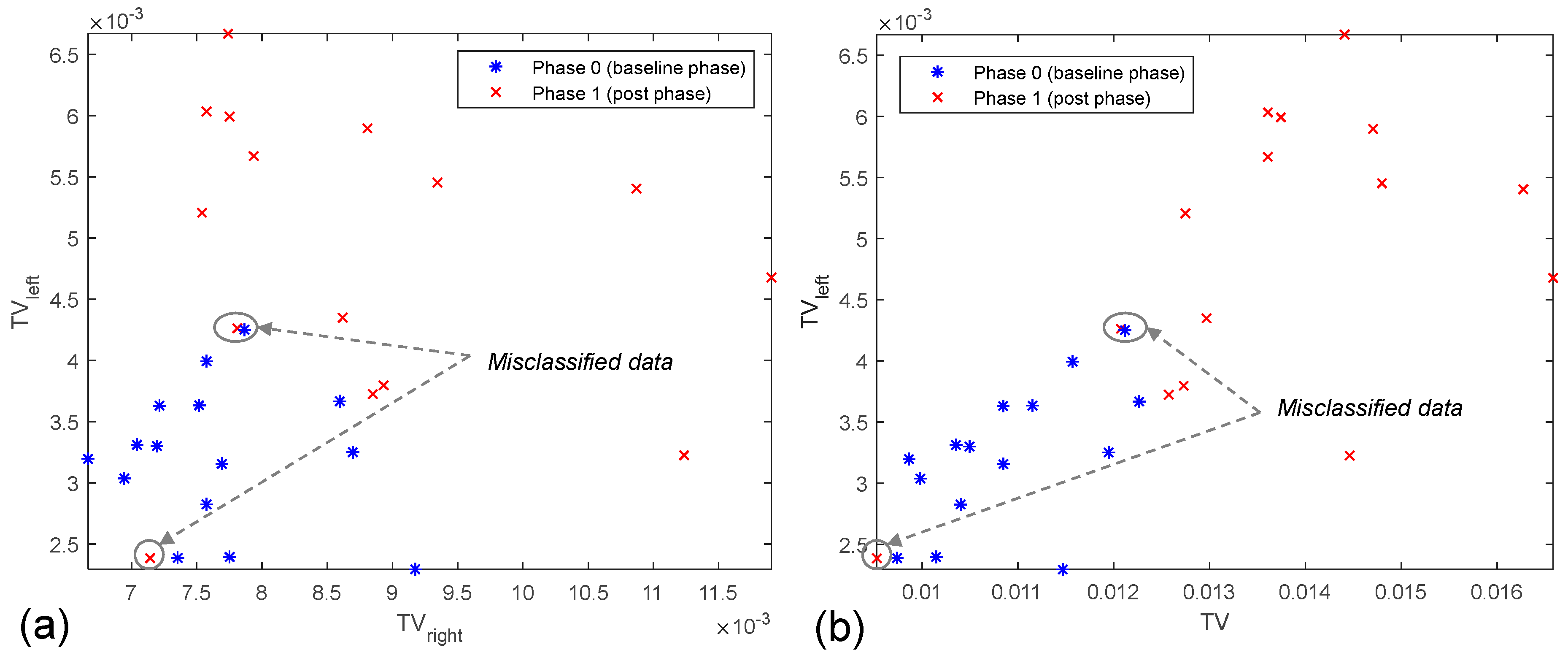
| 6 | Total variations | Calculation of the total variation for the left (TVleft) and right (TVright) sides of a spectrum, as well as the total variation (TV) for an entire spectrum |
| Feature Group ID | Feature Group Explanation |
|---|---|
| 1 | HRV temporal measures, entropy and MF spectrum-based features |
| 2 | Shannon entropy and MF spectrum-based features |
| 3 | MF spectrum-based features, including total variations |
| 4 * | MF-based total variations (TV, TVleft, TVright) |
| Classifier No. | Classifier Type | False Positive Rate (FPR) | True Positive Rate (TPR) | Accuracy [%] |
|---|---|---|---|---|
| 1 | Fine tree | 0.13 | 0.87 | 86.7 |
| 2 | Linear discriminant | 0.33 | 0.87 | 76.7 |
| 3 | Logistic regression | 0.20 | 0.93 | 86.7 |
| 4 | Linear SVM | 0.27 | 0.87 | 80.0 |
| 5 | Cubic SVM | 0.20 | 0.93 | 86.7 |
| 6 | Fine kNN | 0.13 | 0.80 | 83.3 |
| 7 | Cosine kNN | 0.20 | 1.00 | 90.0 |
| 8 | Cubic kNN | 0.33 | 1.00 | 83.3 |
| 9 | Weighted kNN | 0.13 | 0.80 | 83.3 |
| 10 | Ensemble bagged tree | 0.13 | 0.93 | 90.0 |
| No. | Classifier Type | Accuracy [%] | AUC | F1 Score | |||
|---|---|---|---|---|---|---|---|
| Without Entropy | With Entropy | Without Entropy | With Entropy | Without Entropy | With Entropy | ||
| 1 | Ensemble bagged tree | 90.0 | 86.7 | 0.92 | 0.89 | 0.9032 | 0.8750 |
| 2 | Cosine kNN (proposed approach) | 90.0 | 93.3 | 0.92 | 0.93 | 0.9091 | 0.9375 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milivojević, M.; Gavrovska, A. Cognitive Cardiac Assessment Using Low-Cost Electrocardiogram Acquisition System. Electronics 2025, 14, 2468. https://doi.org/10.3390/electronics14122468
Milivojević M, Gavrovska A. Cognitive Cardiac Assessment Using Low-Cost Electrocardiogram Acquisition System. Electronics. 2025; 14(12):2468. https://doi.org/10.3390/electronics14122468
Chicago/Turabian StyleMilivojević, Milan, and Ana Gavrovska. 2025. "Cognitive Cardiac Assessment Using Low-Cost Electrocardiogram Acquisition System" Electronics 14, no. 12: 2468. https://doi.org/10.3390/electronics14122468
APA StyleMilivojević, M., & Gavrovska, A. (2025). Cognitive Cardiac Assessment Using Low-Cost Electrocardiogram Acquisition System. Electronics, 14(12), 2468. https://doi.org/10.3390/electronics14122468