1. Introduction
Gastroscopy and colonoscopy are the two basic and most commonly performed endoscopic examinations of the digestive tract. Gastroscopy is used to evaluate the oesophagus, stomach, and duodenum. It is a basic examination in the diagnosis of cancers of these organs or ulcer diseases. A colonoscopy is an endoscopic examination of the large intestine, just like gastroscopy, used in the diagnosis of cancer and other intestinal diseases. These diagnostics can also be performed with the use of wireless endoscopes fabricated in the form of a small capsule equipped with a camera and a transmitter used to transmit the recorded image. This type of device helps to detect pathological changes along the entire length of the digestive system in a comfortable and non-invasive way for the patient. The duration of such an examination is approximately 8 hours. Very often, the use of this type of device in medical diagnostics requires that the image recorded by the camera be supplemented with information about its exact location. This is very important, especially when further treatment of the patient requires surgery or precise application of pharmacological agents. It is important not only to know where the capsule is along the digestive tract, but also where is located in three dimensions to corelate the images captured by camera with results of other medical diagnostics techniques (e.g., magnetic resonance imaging (MRI)) [
1].
Many methods of locating capsule endoscopes have been developed so far. We can distinguish methods based on the analysis of the electromagnetic field [
2,
3,
4,
5], image processing [
6], or tracking methods based on information from inertial sensors [
7].
The localization methods of capsule endoscopes can be also classified according to the position of the object in relation to the body. There are methods that allow to determine the position of the endoscope along the digestive tract and those that identify the position in a three-dimensional coordinate system. The first group of methods is based on tracking displacements and orientation of the capsule. In the case of the second group, methods based on the analysis of the electromagnetic field are most often used. For example, solutions using information on the distribution of magnetic field strength provide results with an error not exceeding 20 mm [
2,
4], which is comparable to the size of an endoscope. Other methods (including the one described in this article) use algorithms based on parameters of the received signal, such as received power level, signal propagation time, or received signal phase difference. Due to the complexity of wireless propagation channel inside the human body, it is necessary to use a model that takes into account the electrical parameters of individual tissues.
All these methods have certain limitations that significantly affect the accuracy of the positioning. In the case of algorithms based on the analysis of the electromagnetic field, the parameters of the received signal are affected by multipath propagation inside the human body. As a result, it is not possible to unambiguously map the measured values of received power or phase shift to the distance of the transmitter from the individual receiving nodes located on the patient’s body. The use of accurate body models made, for example, with the use of an Nuclear Magnetic Resonance (NMR) scanner allows to significantly improve the accuracy of localization; however, it is a costly and time-consuming solution. In the case of methods based on image analysis or movement tracking with the use of inertial sensors, the obtained results may be subject to error resulting from the patient’s movement or the variable velocity of the capsule’s displacement in individual sections of the digestive system.
Methods that are based on the analysis of the signal phase shift are sensitive to the location of the receivers on the patient’s body. The algorithm proposed by the authors in the previous paper can use information about the signal phase from any number of external receivers [
8]. However, as the research has shown, a large number of receivers (in practice more than 5) causes an increase in the positioning error and extends the estimation time of a single capsule position. Therefore, a method was developed in which the algorithm automatically selects only five receivers from a set of nine receivers placed on the patient’s body based on the received power level.
Many methods of capsule endoscope localization proposed so far use information on the parameters of the wireless signal emitted the by endoscope by its antenna [
3,
5,
8]. Moreover, wireless capsules have limited power budget which is mainly determined by limited space which can be used by capsule battery. For this reason, there is a need to reduce transmitter power as much as possible. Data transmission performance may be improved by introducing optimal channel coding [
9] as well as improving antenna parameters. The latter can be obtained by minimizing return loss which may be caused by antenna detuning effect in different body tissues. For this reason, next to the camera and algorithms for the automatic detection of lesions, the capsule antenna is a key element of endoscopic capsules. There are two basic limitations that must be considered when designing a capsule antenna. The first is the size of the capsule which varies depending on the manufacturer. The shape is similar to a cylinder with a height varying from 24.5 to 31 mm and a diameter from 10.8 to 11.4 mm [
10]. The second limitation is the frequency of the signal that can be used in implantable medical devices. In the case of endoscope capsules, it is Medical Implant Communication System (MICS) band with a frequency range from 401 MHz to 406 MHz [
11]. A human body is a heterogenous environment that affects antenna impedance matching and received power level in the wireless link. During the medical examination, the capsule goes through entire digestive tract and is exposed to the environment with variable electrical properties. Therefore, the antenna should have wide bandwidth so that the detuning effect in tissues with different electric properties does not deteriorate the transmission at the particular frequency.
Due to the limited size, relatively low operating frequency (the wavelength is greater than the capsule size) and dynamic electrical environment, designing small antenna that can be built into the capsules is a challenging task. Designing antenna for lower band (MICS) is more complex as it must match to relatively long wave. The wavelength
λd in dielectric of relative permittivity
εr is shorter than in the wavelength in free space
λc, according to Equation (1).
The values of relative permittivity
εr within the body differ in the range from 40 to 60 [
12]. For frequency of 405 MHz and the average permittivity of human tissues that equals 50, the wavelength
λd is approximately 105 mm. Assuming that the largest dimension of capsule is 26 mm, the entire antenna cannot be larger than ¼ of wavelength. Many types of endoscopic antennas have been presented in the literature [
13,
14,
15,
16,
17,
18,
19,
20,
21,
22,
23]. From the construction point of view and possible location of the antenna in the capsule, they can be divided into those that have a spatial structure that occupies significant volume of the capsule [
13,
14,
15], and those that can be placed on the surface of the capsule [
16,
17,
18,
19,
20,
21,
22,
23]. The first type has a limited applicability due to the fact that they take up space needed for other electronic capsule components such as camera battery, processor, transceiver parts, or LED. The second type is more popular due to its conformal structure. In such antennas, a conductive element is usually fabricated of copper placed on a flexible dielectric substrate, due to which it can be adapted to the size and shape of the capsule.
Capsule antennas can be also classified by their operation frequency band. Typical endoscopes antennas operate in one MICS band [
13]. There are also some antennas designed for industrial, scientific, and medical bands ((ISM) 433 MHz, 915 MHz, and 2.45 MHz, respectively) [
18,
20] or medical telemetry service (608–614 MHz) [
23]. Such an approach is usually determined by the evolution of endoscopes which must perform many tasks simultaneously providing a high data rate which requires higher bands. Even if the capsule antenna supports higher bands, in many cases it should be compatible with MICS.
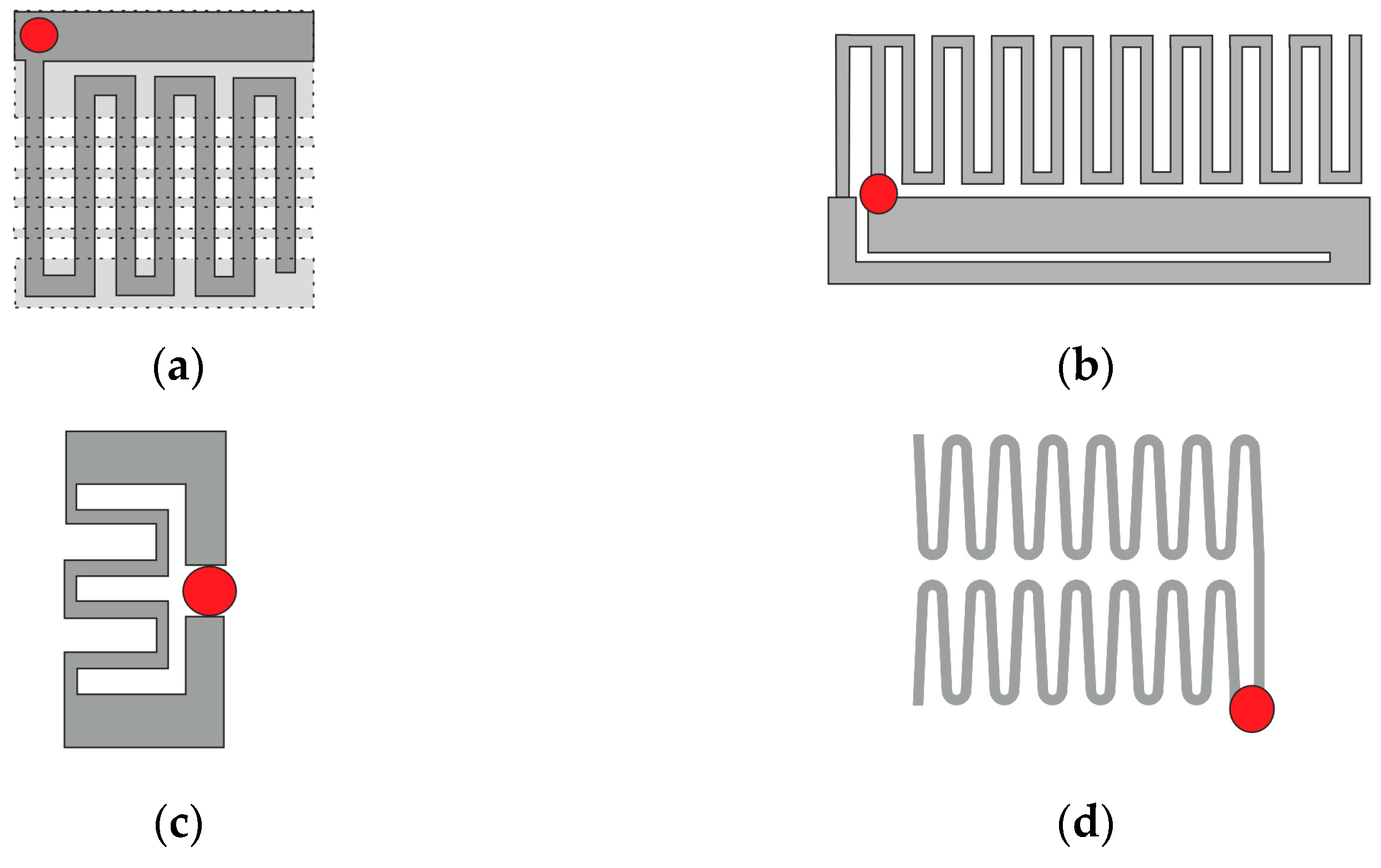
Among many modifications of the helical geometry of an antenna radiator, meander shape was often adapted for the antennas that operate inside human body.
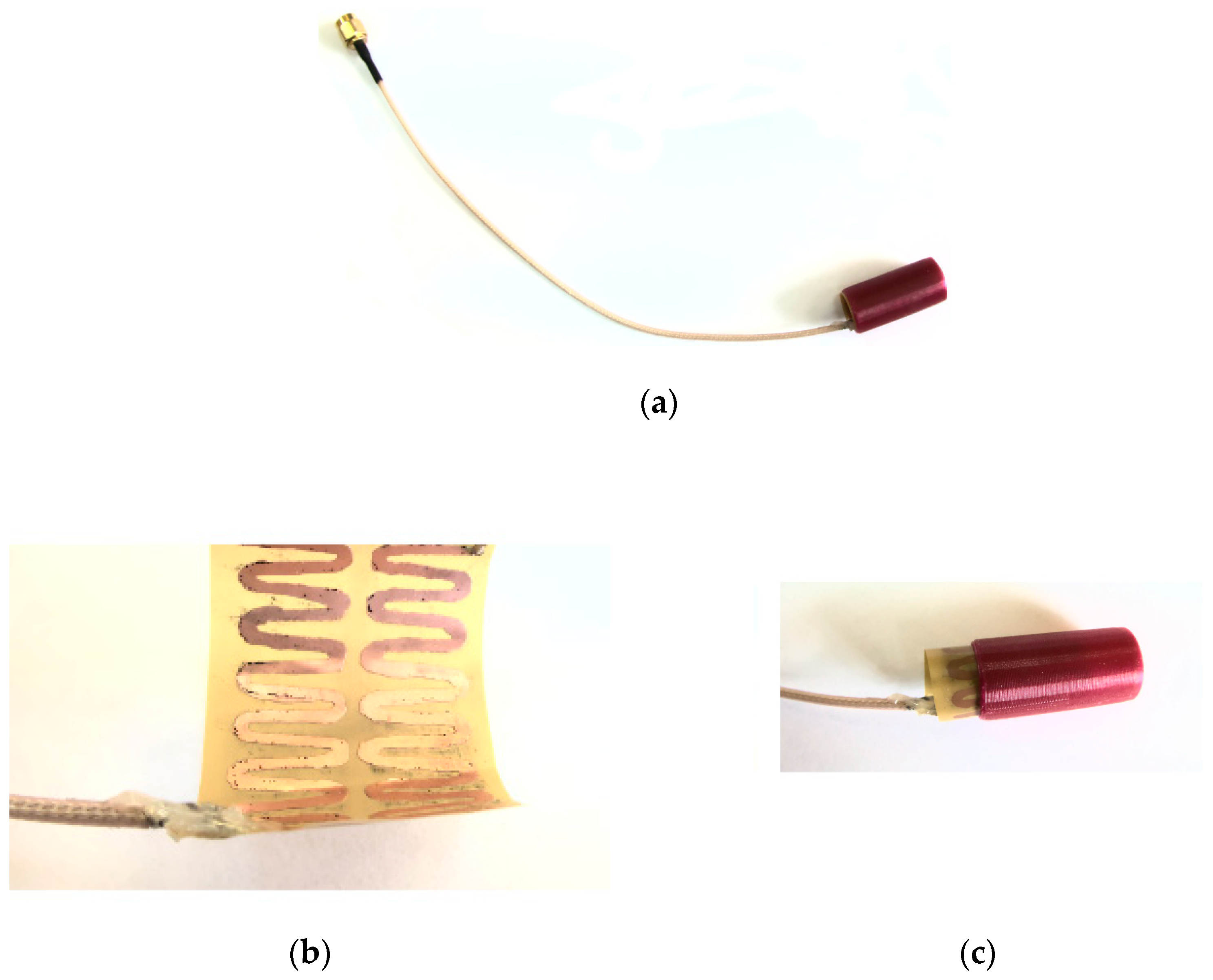
Figure 1 presents examples of capsule antenna radiators (metallic parts). The first one (
Figure 1a) [
14] was designed for much shorter waves as it operates in 2.40 GHz band. It has a spatial structure (2 layers separated by dielectric) and was fabricated on Rogers 3010 non-flexible substrate that makes this design difficult to fit into endoscopic capsule. The feeding point is attached between radiators that are on opposite sides of the dielectric substrate. Compared with other antennas presented in
Figure 1 it is not matched to MICS band in which the wireless capsule operates. The next two antennas (
Figure 1b [
19] and
Figure 1c [
21]) have conformal structures and were fabricated on a flexible laminate. The antenna presented in
Figure 1b consists of meander in the form of “F” structure and slotted L-shaped ground plane. The feeding point is attached between “F” structure and ground plane. Due to the high sensitivity of the antenna bandwidth to open slots, antenna detuning may be caused by both manufacturing flaws and variations in the tissues surrounding the antenna. The antenna shown in
Figure 1c was designed in the form of a closed-loop meander that is a loop dipole with reduced size thanks to the meander section. It is however sensitive to the surrounding material since it changes significant impedance matching for different implantation depths [
21].
Since the meander structure was successfully used to form different radiators of endoscopic capsule antenna, the radiator of the antenna utilized this shape.
Figure 1d presents the antenna proposed in this study which was optimized to reduce attenuation between capsule end receivers located on the patient body. This antenna consists of two meanders and has open-loop structure. The shape of meanders were optimized and were designed to be manufactured on flexible laminate.
In this article, the research on a folded zig-zag antenna for a wireless capsule is presented which allows to reduce attenuation of signal between the endoscope and external antennas by 9 dB. The proposed antenna utilizes to meander shape, can be fabricated on flexible laminate and then wrapped around the capsule under its shell. The impedance matching of the antenna prototype was measured in a simplified cylindrical human body model filled with tissue simulant liquid. The designed antenna was verified with computer simulations together with the model of the endoscopic capsule. The model of the capsule contains different elements such as a battery or camera. The design of the improved endoscopic antenna is presented together with impedance matching and an analysis of transmitted power efficiency. Simulations were carried out in different tissues which may surround the capsule during movement inside the digestive tract. The antenna together with the capsule model were applied to the improved version of the localization algorithm.
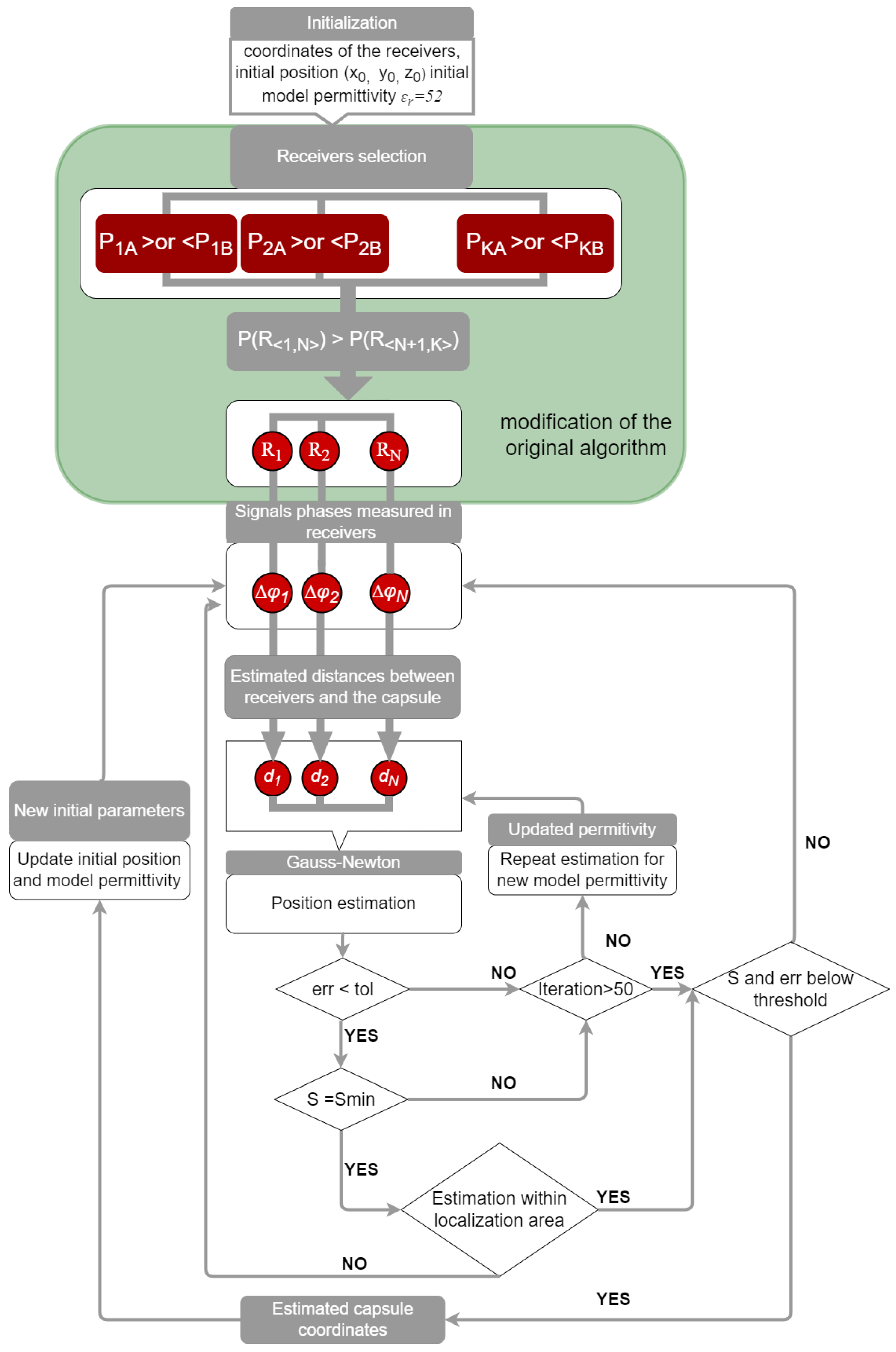
In this paper we present also the novel version of localization algorithm that automatically selects receivers from a redundant set. In our previous study, it was observed that the number of external receivers as well as their position on the patient’s body has a significant impact on the accuracy of endoscope localization. For better localization accuracy this algorithm has now the possibility to select the receivers that provide data. Below, the impact of the proposed antenna with capsule model and the improved localization algorithm on localization error are investigated.
3. Results
The proposed antenna at the first stage was verified using computer simulations. It was designed assuming that it will be sourounded by a tissue simulant material. The parameters of tissues which directly surround the capsule in the digestive tract were choosen for simplified models to validate antenna performance and to check its impedance matching in the digestive tract. To investigate its performance in the proximity of different tissues a series of simulations were performed for tissue simulant material of diferent electric properties. They were selected to correspond to the parameters of the tissues that build the organs through which the endoscopic capsule moves. Parameters of selected materials are presented in
Table 2. At the first stage of the research the average model for human body with permittivity
εr = 57 and conductivity
S = 0.76 S/m was applied. This is a commonly used approach in the design of wireless systems operating in the area of the human body [
24]. During simulation in Remcom XFdtd software the antenna was implanted in the middle of the cylindrical model as presented in
Figure 2. In the simulation the Gaussian-shaped signal was used as an excitation.
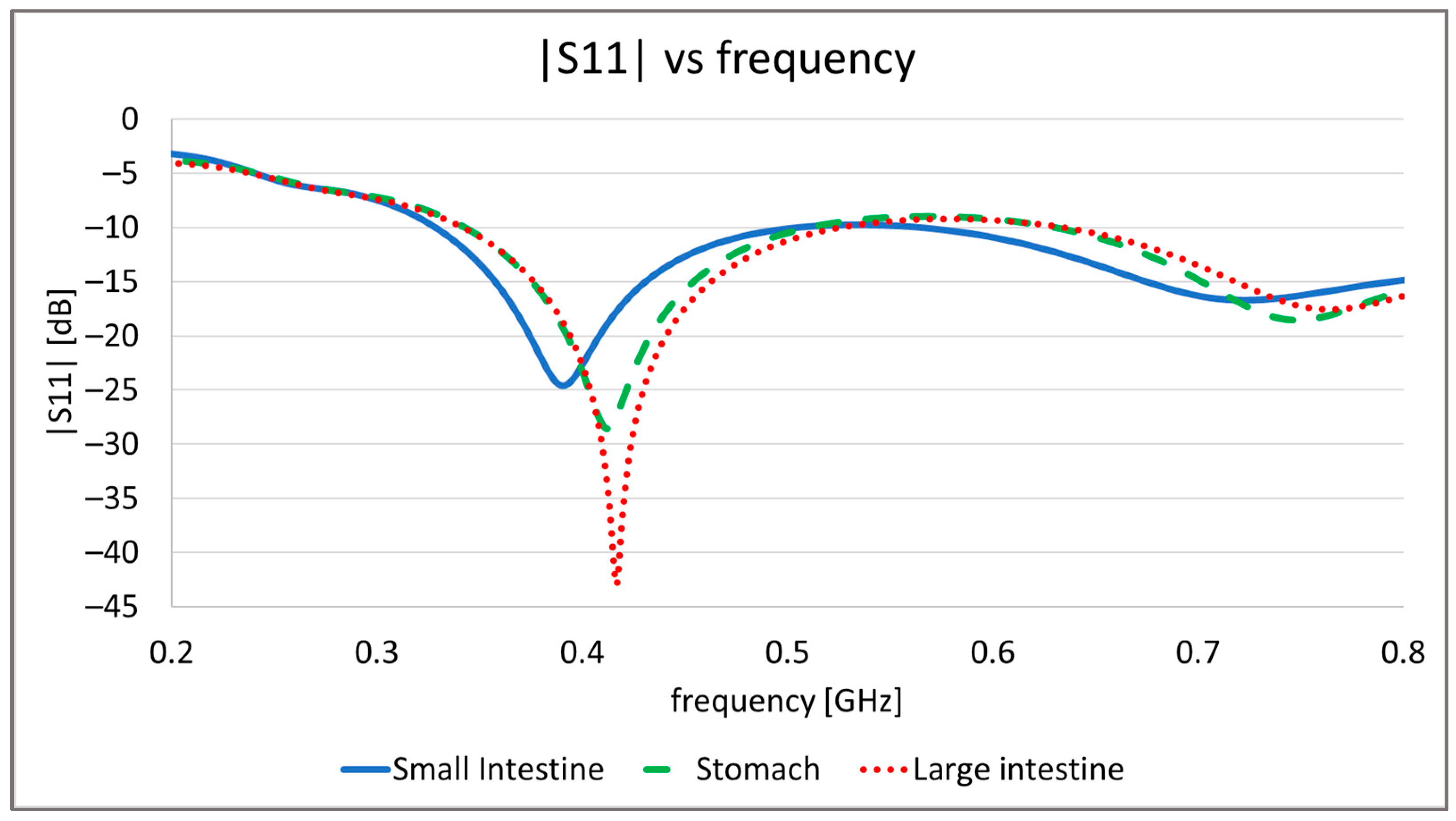
In
Figure 9 the simulation results of antenna impedance matching to 50 Ω are presented. Simulations with an average body model show that in such an environment, the proposed antenna has a wide bandwidth from 200 MHz to 1.1 GHz. In the case of antennas that are implanted and can move inside body it can suffer from impedance detuning. Simulations performed with models that had properties of different tissues confirm this. This can be seen especially for the small intestine. Taking into account results for all examined tissues, the effective bandwidth for the proposed antenna remains in the range from 380 MHz to 480 MHz. This means that it can be applied for the MICS band.
Depending on the position of the capsule, the human body can significantly attenuate the wave transmitted from the endoscope. The appropriate power level is also important for the proper phase detection in the individual external receivers located on the patient’s body. Therefore, the value of power received in external receivers for the helical antenna and the proposed conformal antenna was compared. For this purpose, simulations were carried out for four simplified models of the human body with different electrical properties. The models were selected to correspond with the tissues in which the endoscopic capsule can be found: stomach, large intestine, and small intestine. Moreover, the averaged model was used due to the fact that the power of the received signal is affected by all tissues of the human body through which the radio wave propagates. Parameters of individual models are presented in the
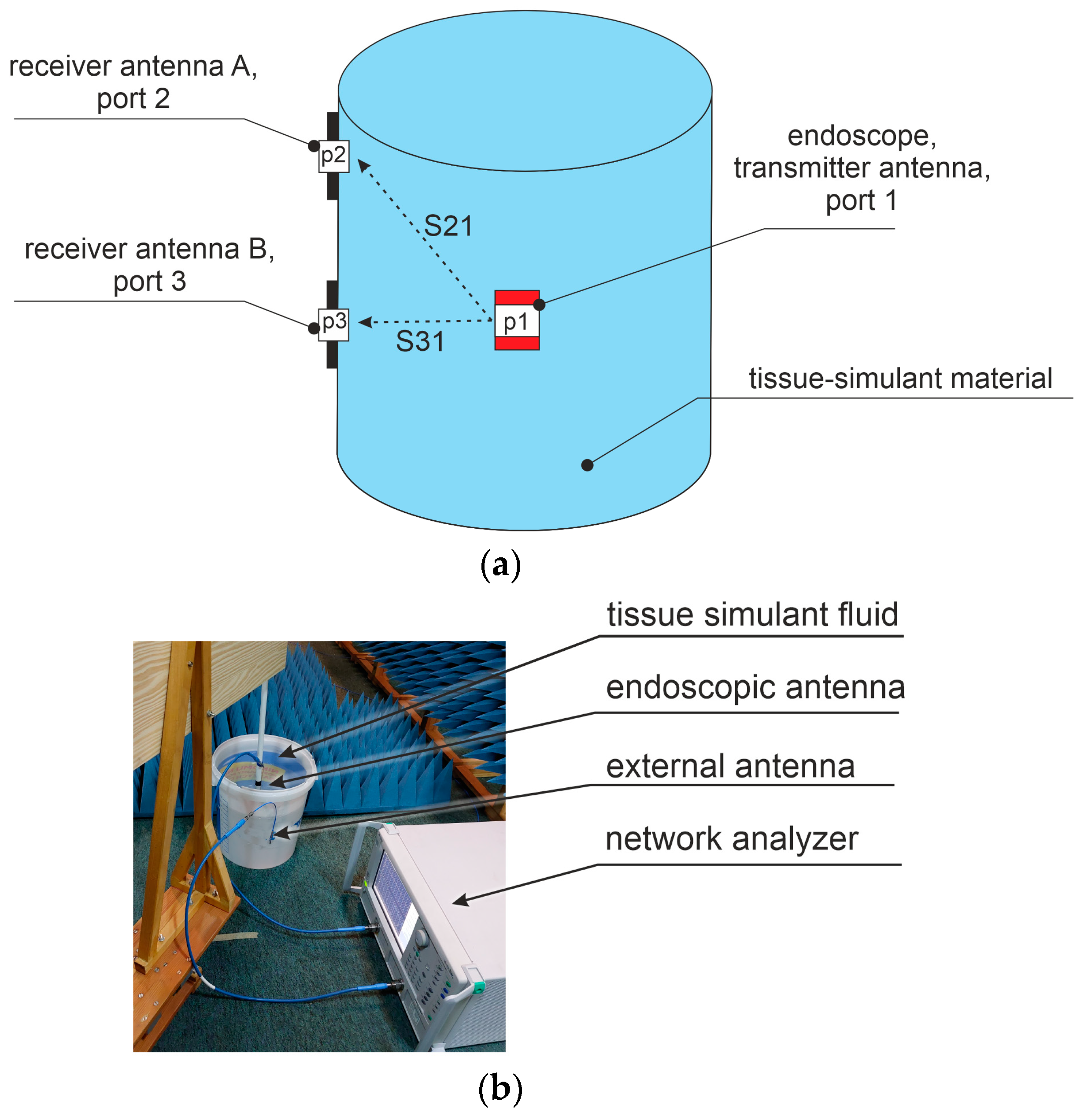
Table 2. The antenna verification setup is presented in
Figure 10. External antennas A and B were placed next to the model fabricated in the form of a cylinder. The capsule was placed in the middle of the model. The attenuation of signal between antennas was simulated as the system loss, using scattering matrix parameters that represent coupling between antenna ports.
Table 3 presents the values of S
21 and S
31 achieved respectively for receiver A with port 2 and receiver B with port 3. The proposed conformal antenna provides significant improvement compared with the helical antenna. The difference varies from around 9 dB to 7dB. This improvement is very important for the adaptive receiver selection algorithm as the received power level is used to decide which receivers should be chosen.
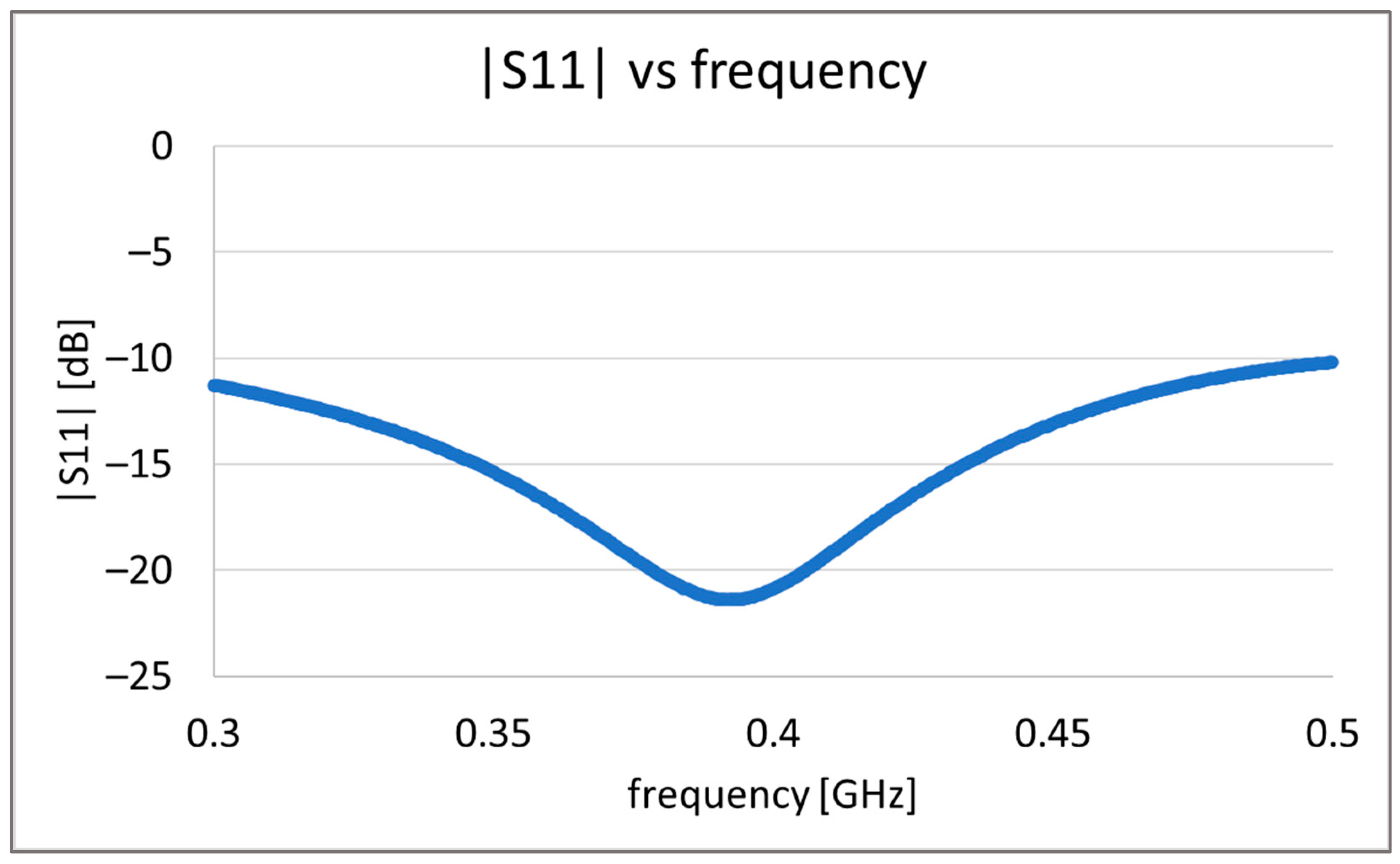
Due to technological limitation we decided to fabricate the antenna prototype replacing capsule materials with PLA material. For this reason simulation with PLA material was performed. The results obtained from simulations show that material of capsule shell mainly impacts antenna impedance matching. Slightly increasing the antenna height by 3 mm, it is possible to achieve impedance matching for 400 MHz frequency as presented in
Figure 11. The antenna adopted to be placed in PLA capsule shell is within the dimensions typical for commonly used capsules. The antenna radiator is fabricated of Pyralux 25-micron thick Polymide laminate covered with 45 um copper. Its structure presented in
Figure 12b was printed on laminate and then etched using sodium persulfate and soldered to coaxial cable. The antenna radiator was rolled up and inserted between two 3D-printed elements as presented on
Figure 12c.
At the next stage, the proposed antenna was validated by measurements in the simplified human body phantom. The body model was fabricated of a thin-walled plastic vessel filled with tissue simulant liquid. It had the same dimensions as the one shown in the
Figure 2 used in the simulations. In the proposed experiment it was assumed that the fluid should have parameters similar to average values of the human body. For this a solution of water, sugar, and salt was prepared. The proportions of this solution were defined experimentally in previous research [
8] and has the following values: 1 L of water, 350 g of sugar, and 15 g of salt. Depending on the source of the water used for the solution its electrical parameters may change the properties of the achieved liquid. For this reason, the values of permittivity and conductivity were measured with the DiLine measurement setup procedure by Index Sar Company [
27] presented on
Figure 13. This uses a vector network analyzer connected to the TEM line filled with prepared liquid to measure the electric length and loss of line. At the temperature of 23 °C and at 400 MHz permittivity was equal to
εr = 57, and the conductivity was σ = 0.75 S/m. In our research we used the Anritsu MS 4647B Vector Network Analyzer for measuring the liquid properties as well as for antenna characterization and signal attenuation measurement.
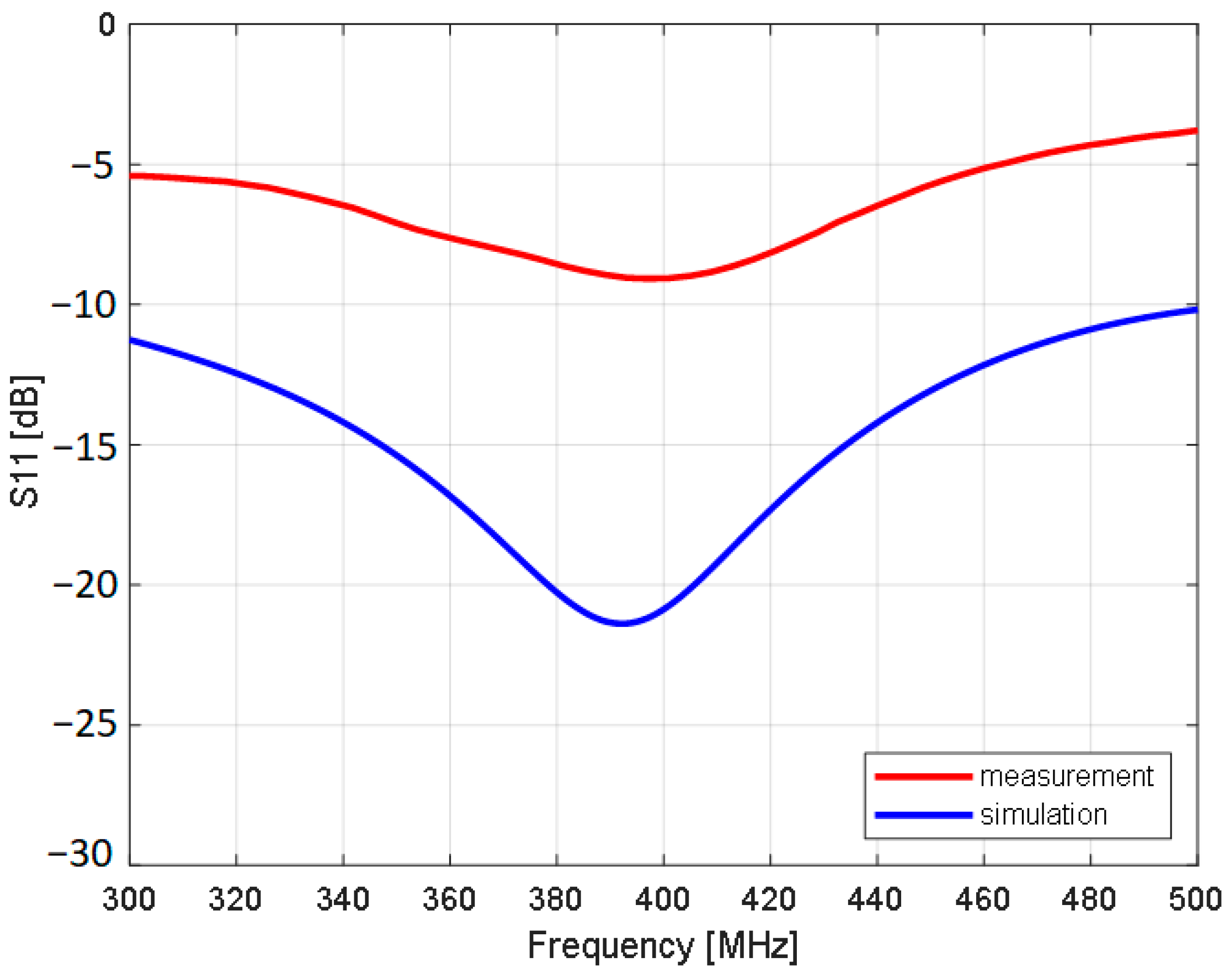
In
Figure 14 the measurements results of antenna impedance matching to 50 Ω are presented.
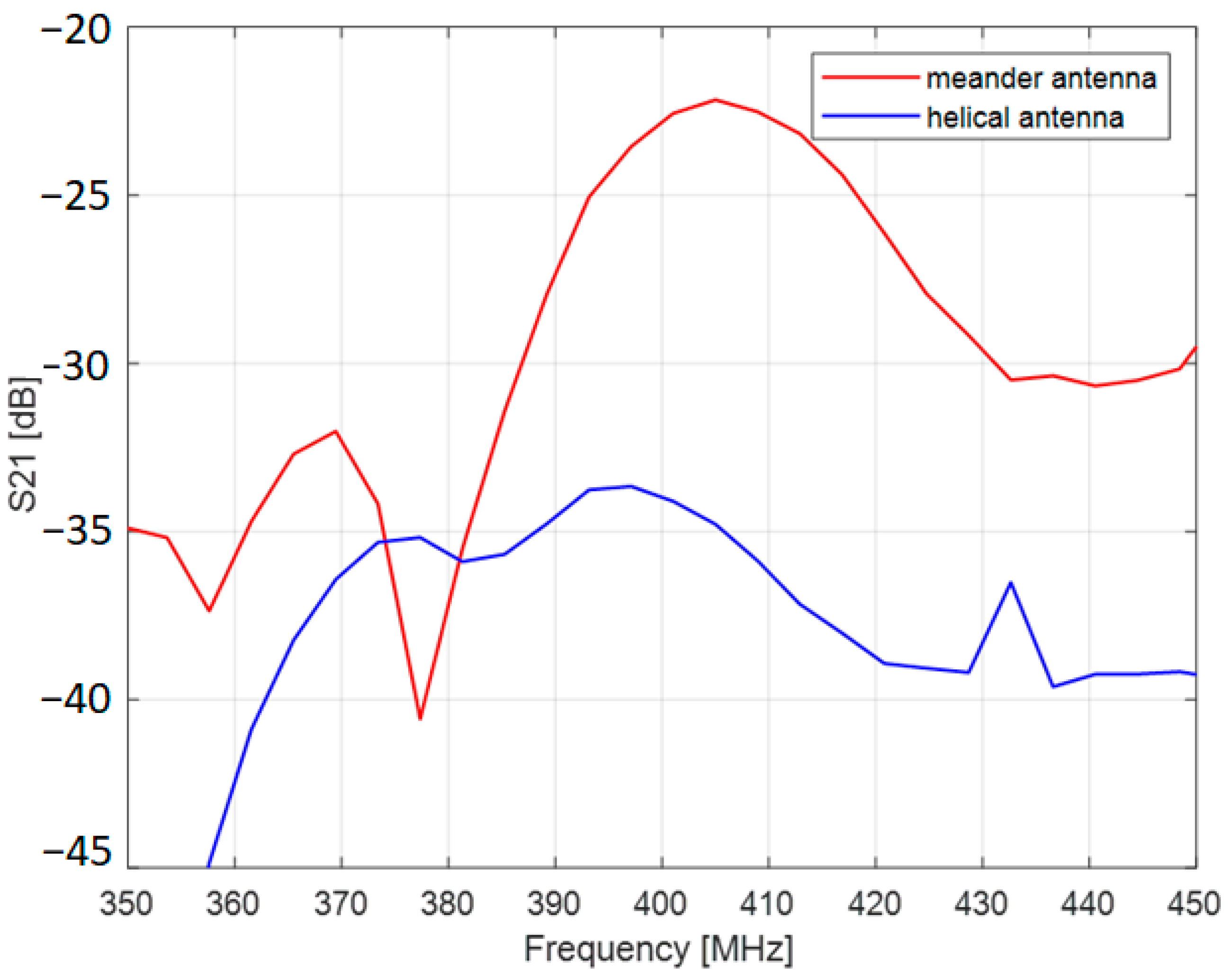
Figure 15 shows the result of S21 measurements between endoscopic antenna and external helical antenna. The endoscopic antenna was placed in the middle of the body phantom.
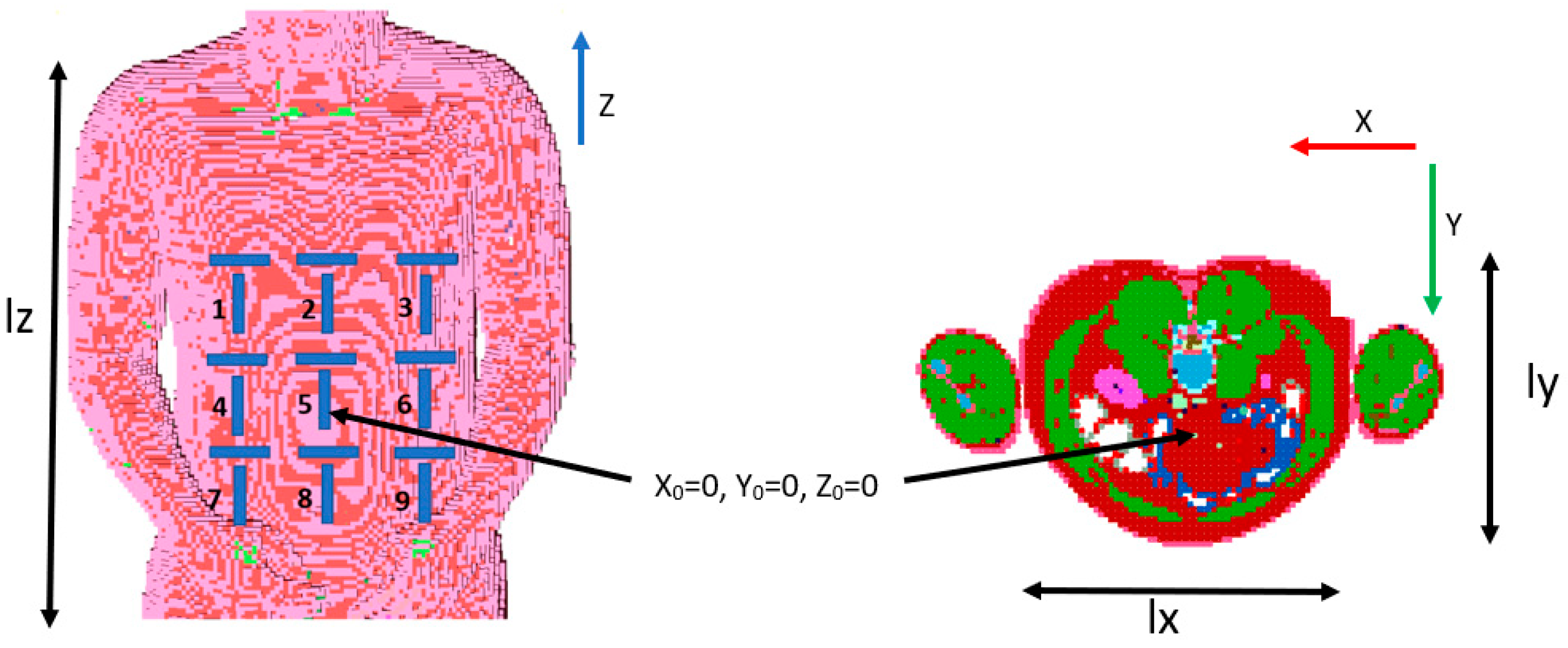
The antenna performance was then validated with the algorithm for capsule localization. Input data were obtained with computer simulations. Remcom XFdtd software version 7.8.1 and its NMR heterogenous human body model with a 5 mm voxel size were used for this purpose. The adopted heterogenous model represents the exact structure of the human body defined by 39 different materials [
25]. Each organ consists of cuboids with which electrical parameters correspond to parameters of human tissues. The cross section of the adopted body model is presented in
Figure 16, different tissues are represented with different materials colors. In the simulated scenario, a set of 160 predefined capsule positions in the area of the digestive system was examined. Taking into account dimensions of the model and coordinate system presented in
Figure 16, capsule positions were changed in the following range: x = ±70 mm, y = ±30 mm, and z = ±150 mm. As the endoscope operates mainly in MICS band, simulations were carried out for frequencies 401 MHz and 406 MHz.
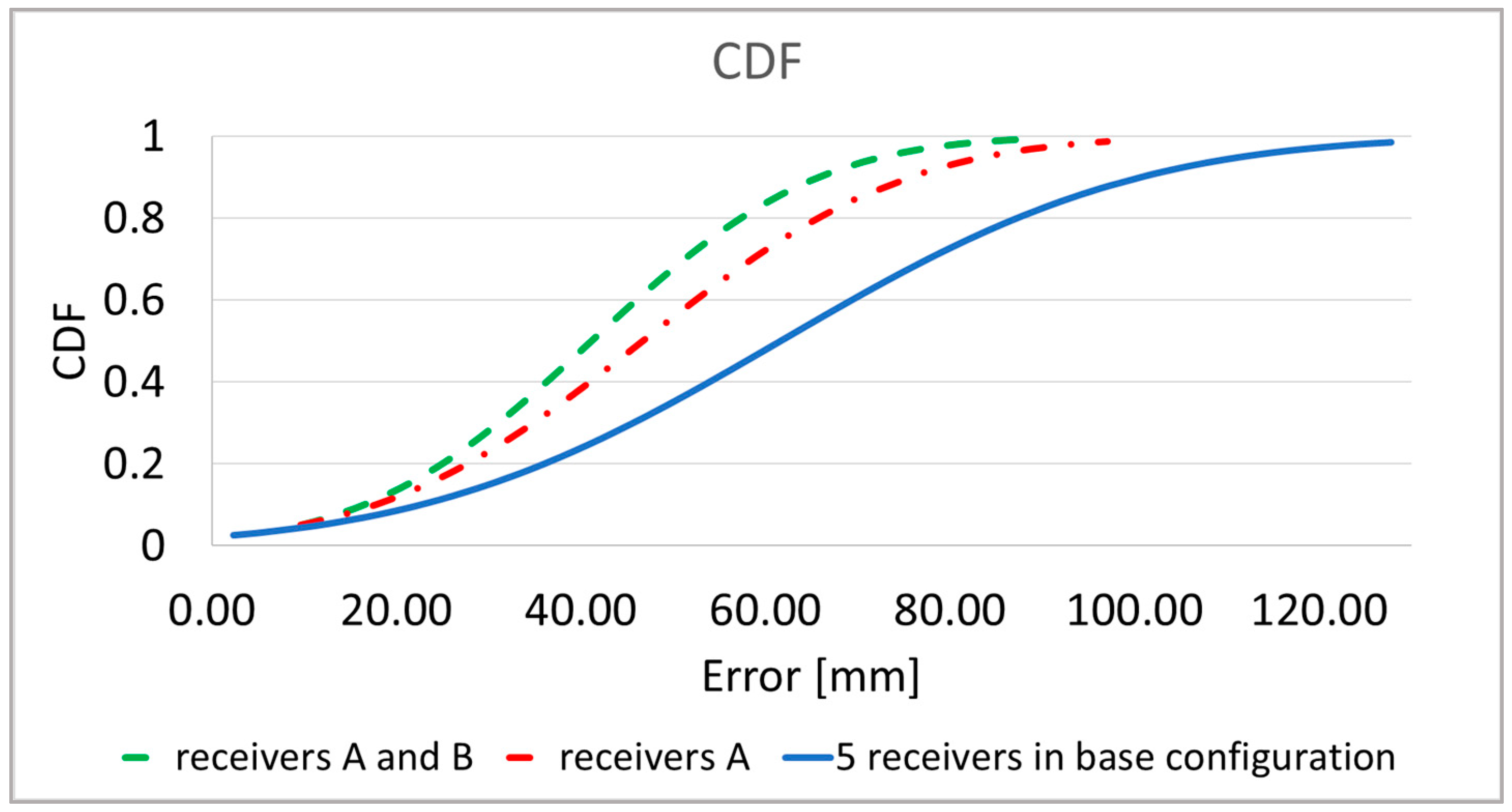
Figure 17 shows the results of the analysis of the localization error with the adaptive body model and the algorithm for the automatic external receivers selection. Taking into account the fact that the orientation of the endoscopic capsule affects the location error, two versions of the receiver arrangement were compared: receivers arranged vertically (A
k) and receivers arranged vertically and horizontally (A
k and B
k). The presented location error described by Formula (9) [
8] was defined as the distance between the actual position of the capsule and the estimated position.
where
xt, yt, zt is the actual position;
xest, yest, zest is the estimated position.
The dynamic recivers selection together with the proposed conformal zig-zag antenna improves localization accuracy by about 35%.
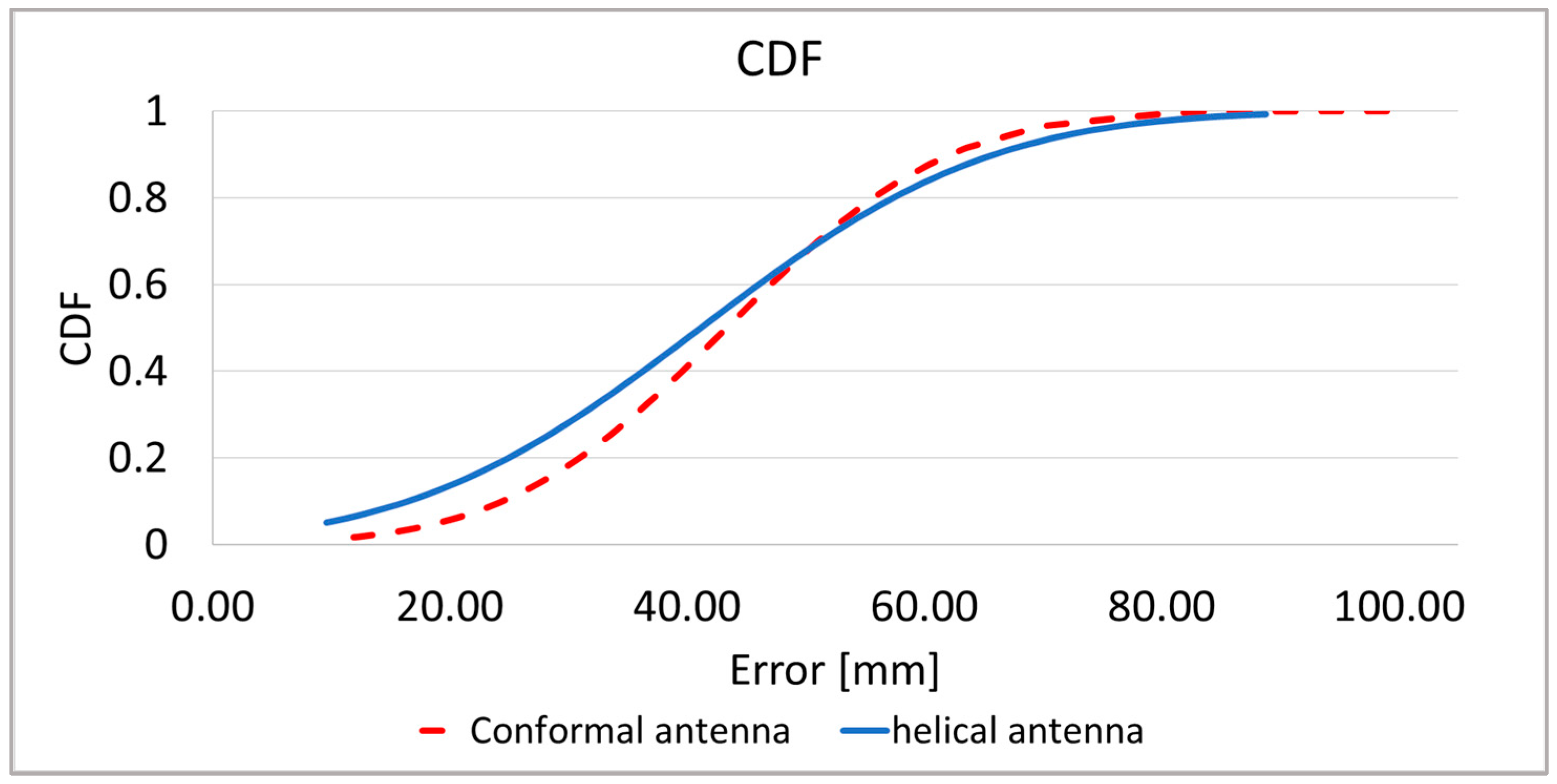
Figure 18 presents the localization error collectively for around 160 investigated capsule positions in different parts of the digestive tract. Results shows that the proposed antenna allows to reduce maximum localization error while the average error is similar to the helical antenna.
In the localization process capsule that travels along the digestive tract is surrounded by different tissues and the localization error may be dependent on attenuation introduced by different tissues.
Figure 19 shows localization error for the capsule that was palced in different parts of digestive tract obtained with the heterogenus human body model. The worst localization accuray is observed in the large intestine despite the fact that according to
Table 3 the attenuation here is the smallest. In the heterogenous model, different parts of digestive system (tissues in
Figure 16) are loceted at different distances to the receiving antennas which also affect received signal strength, delay, and overall performance of the localization system.
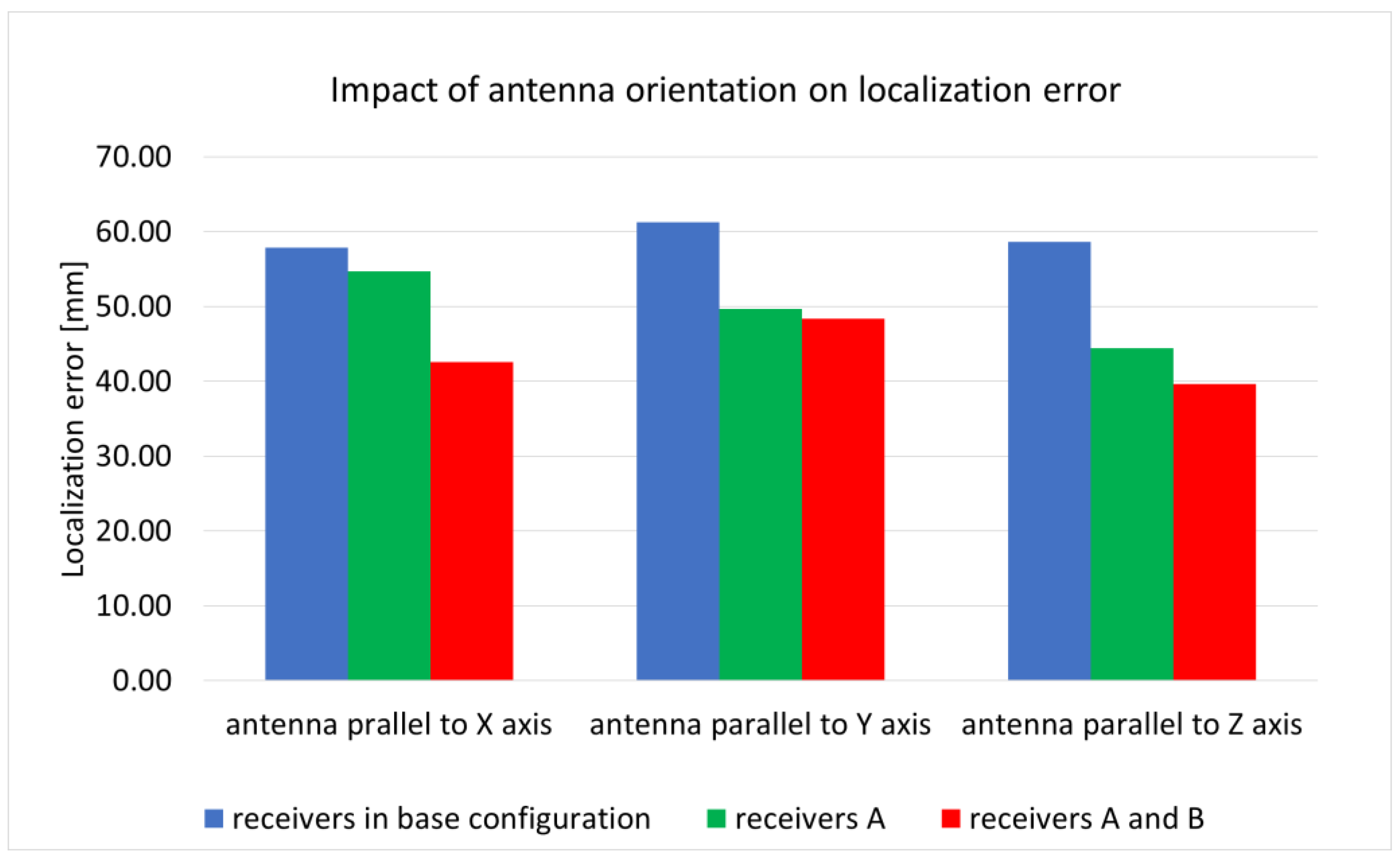
The endoscopic capsule, moving along the digestive tract, changes its orientation in relation to external receivers. The orientation of the capsule has an impact on the signal as well as the human body. The research carried out so far showed that in the case of a helical antenna, a change in orientation can increase the average location error by up to 10 mm. For this reason, additional B receivers arranged horizontally as presented on
Figure 7b were introduced to minimize the influence of the capsule antenna orientation on the localization accuracy. To check antenna orientation, the impact of localization accuracy simulations were carried out in which the capsule antenna was rotated by 90° around the X and Y axis. Results presented in the
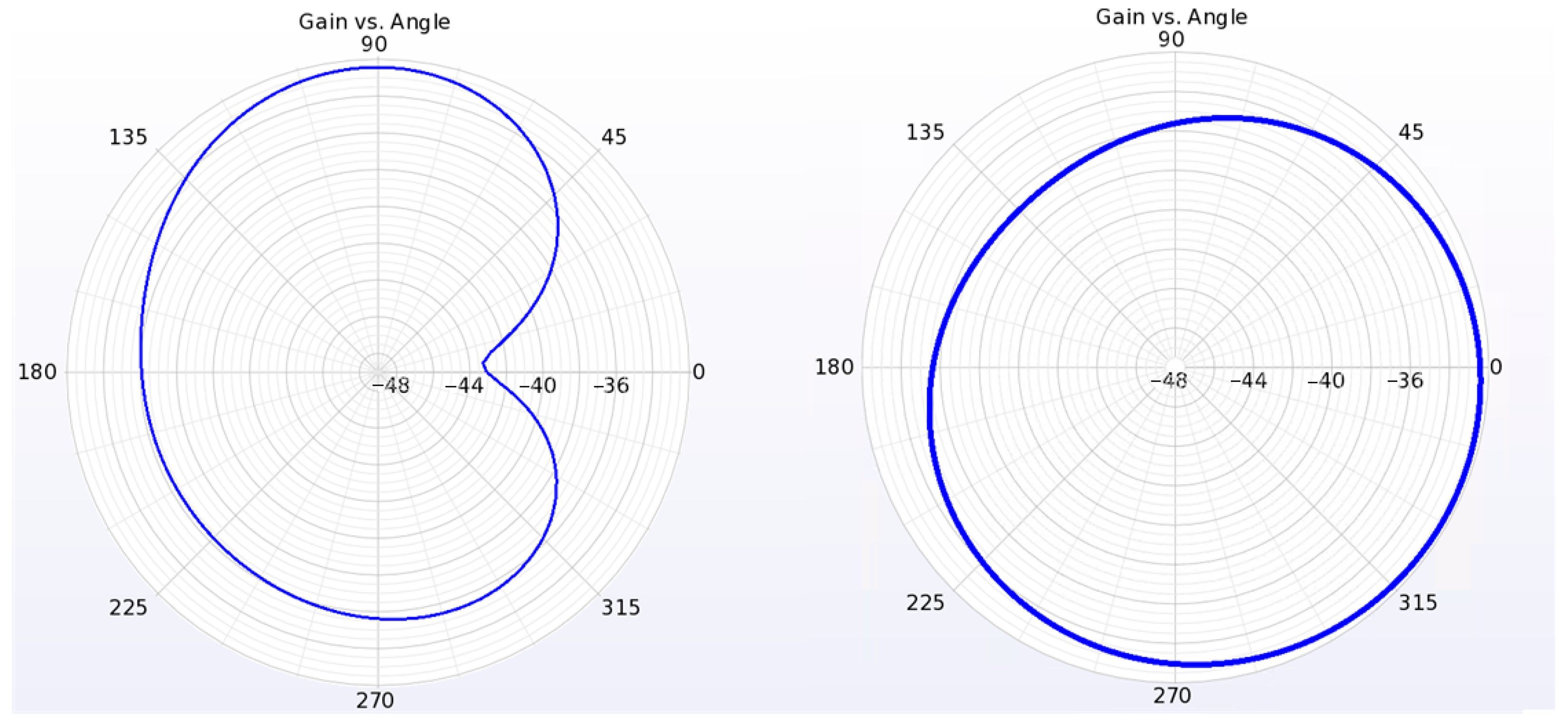
Figure 20 show that additional receivers improved localization accuracy. This is the most visible when the antenna is parallel to the X axis. The lowest improvement is visible when the antenna is parallel to the Y axis. This is because according to radiation pattern presented on
Figure 6 the radiation efficiency for the proposed conformal antenna is the lowest in the direction of the Y axis.
4. Discussion
The results of antenna impedance matching simulations show that the conformal zig-zag antenna has a bandwidth within the 400 MHz band that is dedicated to endoscopic capsules. As it was presented in
Figure 9 the antenna preserves good impedance matching being exposed to different tissue materials. As presented in
Figure 14 the results of antenna impedance matching differ between measurement and simulation. Even if the frequency for which the minimum of S11 is the same (400 MHz), the value in the case of measurement is greater than 12 dB. This is the result of differences between the numerical model and fabricated prototype. As presented in
Figure 12, the antenna radiator is fabricated on a thin film substrate. During prototype antenna assembly the air gap had to be applied to insert the radiator between the inner and outer piece of cover. This can result in radiator displacement towards the cover. Moreover, the soldering pads and coaxial connection was not included in the simulation. The antenna was etched in sodium persulfate. The etching process requires applying a mask to the flexible laminate. In our case, a laser printer was used, but due to the poor adhesion of the toner to the laminate, the mask had imperfections. For this reason, the shape of the antenna used in the simulation slightly differs from the prototype. This can also be the cause of discrepancies between the simulation and measurement results.
The results of antenna radiation pattern simulations (
Figure 6) show that the maximum gain of the antenna that is surrounded by lossy tissues is low (−32.2 dBi). It has omnidirectional distribution of the power gain in the plane that is perpendicular to the antenna axis. This is a desirable feature for antennas intended for use in wireless location systems, since changing the orientation of the antenna has less impact on the level of received power. As a result, the phase shift estimation error is smaller.
The attenuation of the signal between the receiving antenna and capsule was simulated as the system loss, using scattering matrix parameters. It was used to compare the proposed antenna with the helical one used in a previous study. For assumed simulation environment, an improvement of up to 9 dB was obtained. Moreover, the proposed conformal antenna is suitable to be used in endoscope capsules because it can be fabricated in the side of the capsule, preserving the internal volume for other electronic components.
The algorithm with automatic selection of external receivers significantly improves location accuracy. Using only receivers placed vertically, the location error was reduced by about 20% compared with the original algorithm. Adding additional horizontal receivers, the error was lower by about 35%. The average location error was 42 mm. The improvement in localization accuracy was observed in about 85% of cases.
An advantage of the proposed method Is that it can be used for patients with different body proportions and may by implemented in wearable systems. This increases usability of the localization system.
Research on localization the algorithm presented in this paper is limited to computer simulations. This is because in the case of transmitters that are operating inside human body experimental verification with measurements is extremely difficult to be performed and requires the agreement of bio-ethical commission. Only measurements with physical simplified phantoms are possible at this stage of research. Therefore, we performed the antenna measurements in the body phantom. Moreover, the influence of body motion on the localization algorithm was not covered here since we had access to a numerical model of a human body in one pose (lying person). Even small movements of the chest and diaphragm caused by breathing can affect the accuracy of the location, especially from the external receivers placed on the front of the torso. The impact of anatomical differences among different human subjects was not investigated at this stage due to lack of other numerical body models available in our simulation setup.
The results of the simulation clearly show that both the position of external receivers and the transmitting antenna type has an effect on the algorithm’s accuracy. The localization error was reduced by about 20 mm for a zig-zag conformal antenna when the dynamic receiver selections were employed.












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}