



Enhancing Elderly Health Monitoring: Achieving Autonomous and Secure Living through the Integration of Artificial Intelligence, Autonomous Robots, and Sensors
 , , ,
, , ,  , and
, and 
Abstract
1. Introduction
- Insufficient knowledge and awareness of risk factors: there is a lack of knowledge and understanding of the determinants that contribute to adverse health outcomes in elderly population [9].
- Prescription requirements: Older people tend to rely on an extensive list of medications to be taken at specific intervals. This increases the complexity associated with appropriate medication intake, administration, and adherence [13].
- Psycho-emotional concerns: isolation, mental strain, and challenges associated with time management are notable psychological and emotional issues facing older people [14].
- Presentation of a working and complete system architecture involving four actors (including carers, doctors, and the elderly) and several technologies (including AI, sensors, and robots);
- Five key lessons emerged from the study.
2. Related Works
3. Materials and Methods
3.1. Interviews and Requirements Analysis
- Monitoring: the aim of the proposed system is to ensure constant monitoring of the elderly person’s health by capturing his or her vital parameters, as well as his or her emotional state. Wearable sensors make it possible to measure vital signs. It should be remembered that the parameters to be measured refer to the MEWS table. This table provides for the measurement of the response to stimuli. Such a measurement has not yet been carried out, and we will address this issue in future work. It is also essential to monitor the correct intake of medication therapy in order to avoid possible complications. With regard to this functionality, it is good to specify that currently the monitoring of medical therapy is done through a series of questions that QTrobot asks the elderly person at a specific time. We will discuss possible further implementations in future developments.
- Communication: the purpose of the proposed system is to provide accurate information on the health status of the assisted person by detecting vital parameters and generating an alarm if any problems are detected, with the necessary additional transmission of the vital parameters that led to the emergency call. It would also be desirable to display appropriate manoeuvres to be performed in the event of a delay in the arrival of help, should this be necessary.
3.2. The Architecture of the Proposed System
- (1)
- NodeRed Container is responsible for collecting the vital signs data collected by the sensors. This container acts as an interface for data collection and processing, ensuring accurate transmission to the system.
- (2)
- AI Model Container plays a crucial role in the workflow of the system. It receives vital signs from the NodeRed container and uses the model to predict the health status of the elderly person. These predictions are based on an evaluation of the vital signs captured by sensors, using the MEWS table, allowing early detection of any signs of deterioration. The model, trained using synthetic data, assists in determining health status. Synthetic data refers to artificially generated data that reflect the statistical properties of the original dataset without revealing any personally identifiable information. The generation of synthetic data is becoming increasingly important in various fields, particularly healthcare. Accurate categorisation and representation of the data is essential to provide reliable input to the classification algorithm. The generation process must be representative to ensure effective learning and accurate classification of the health status of elderly individuals. Synthetic data has shown promise in the field of AI and is seen as a prominent technology for the future, capable of mathematically and statistically replicating real events with precision [51,52].
- (1)
- Humanoid robot: This actor interacts with the elderly person, using machine learning (ML) algorithms, specifically the algorithm, to assess their emotional state. In addition, the humanoid robot employs sensors to measure the vital signs of the elderly. These vital signs serve as input to another ML algorithm, referred to as , which categorises the measurements and determines whether the elderly person is in a healthy or unhealthy state.
- (2)
- Elderly people: This actor represents the elderly population in need of continuous care, assistance, and companionship. The overall aim is to provide a system that ensures their safety and takes account of their health and mental state, enabling them to live independently in their own homes for an extended period of time.
- (3)
- Medical staff: This actor is responsible for monitoring the vital signs and the decisions made by the algorithm. By continuously monitoring these factors, medical staff can ensure the elderly person’s well-being.
- (4)
- Caregiver: The carer is an additional person who can monitor the elderly person around the clock. Their responsibilities cover a wide range of tasks, including managing the elderly person’s prescribed medical therapy and keeping abreast of the elderly person’s daily activities.
3.3. Humanoid Robot Selection
- Robot Emotion: implements the expression of the robot’s facial emotions. This allows the control and modulation of facial expressions to communicate specific emotions.
- Robot Speech: implements the robot’s speech functionality. This allows text to be converted into speech using appropriate speech synthesis. Text can be sent to the robot through this interface for it to speak.
- Robot Behaviour: allows you to implement more complex behaviour by combining the basic functionality of the robot. Through these actions, such as the robot’s facial expressions, voice, and movements, the robot’s facial expressions, voice, and movements create a coherent and interactive behaviour.
- Robot Setup: implements some basic robot settings, such as controlling the volume of the robot’s speakers. Through this interface, it is possible to change the robot’s settings to suit the user’s preferences or the environment in which the robot is located.
3.4. Understanding the Health of Older People
- Heart rate: measured in beats per minute (bpm).
- Systolic blood pressure: measured in millimetres of mercury (mmHg).
- Respiratory rate: measured in breaths per minute.
- Body temperature: measured in degrees Celsius (°C).
- Level of consciousness: assessed using various methods, our current approach involves the recognition of emotions and expressions exhibited by the robotic system employed. Specifically:
- –
- A denotes an “alert” level of consciousness, indicating an awake patient.
- –
- B denotes a “reacting to voice” level of consciousness, signifying a patient responding to verbal stimuli.
- –
- C denotes a “reacting to pain” level of consciousness, suggesting a patient responding to painful stimuli. However, further research is required to validate and refine this aspect.
- –
- D denotes an “unresponsive” level of consciousness.
4. Bot Telegram
- Users can send commands through messages in a chat;
- It is possible to send commands via inline requests, where the user enters the name of the bot, preceded by the ‘@’ symbol, followed by a request into the Bot’s command line.
4.1. Feature Overview
- /parametri: Allows users to view current patient parameters, providing information on health-relevant measurements;
- /storico: Users can access a history of patient parameters (weekly, monthly, and yearly), allowing them to examine trends and changes over time;
- /terapia: Provides access to the patient’s daily schedule of prescribed medications, enabling effective therapy management. Users can view medication intake times, record actual intake, and access a detailed history;
- /aiuto: Offers users the ability to send requests for help and receive immediate assistance. It can be used to report emergency situations or request urgent information.
4.1.1. Parameter Visualization
- send_params(...): Deals with sending the elderly person’s current data and saving it in a json file;
- send_historical(...): Allows the user to choose which historian to view (weekly, monthly, or yearly) via a button menu; a list of parameters is displayed for each of the options, managed by three different methods:
- –
- weekly_report(...): Handles the weekly report by retrieving from the json file for all days of the week the parameters captured at a given time;
- –
- monthly_report(...): Handles the monthly report by fetching from the json file for all weeks of the month the parameters captured on a given day and time;
- –
- yearly_report(...): Handles the annual report by fetching from the json file for all months of the year the parameters captured at a given day and time of the month.
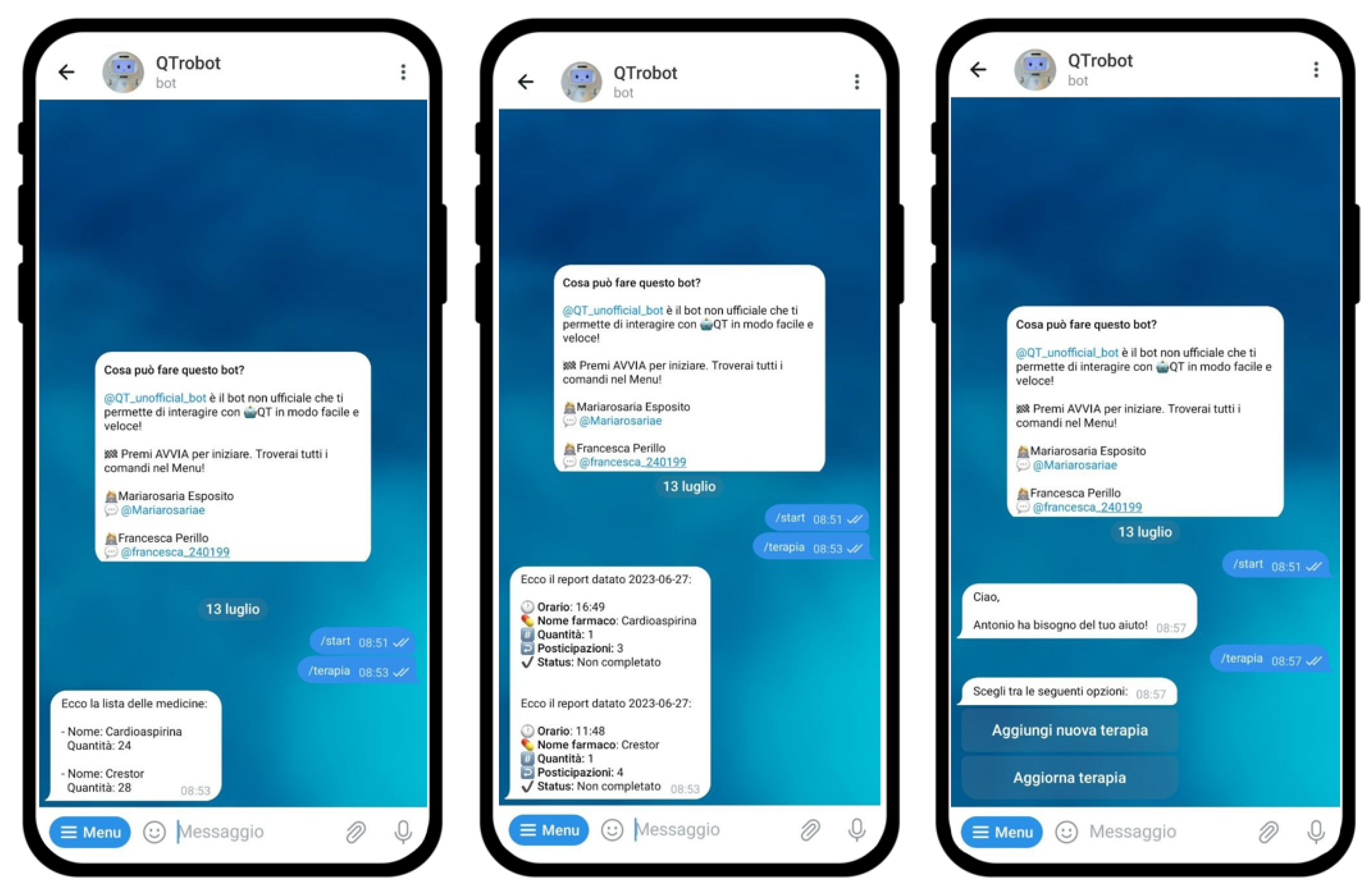
4.1.2. Visualization and Therapy Management
- View the medication list by taking from the diary the medication the elderly person is taking;
- View today’s therapy report by taking from the diary the report for today’s date;
- View the therapy report of a date of the user’s choice by viewing a calendar, which allows the user to choose a specific year, month, and day by then picking up the report of the selected date;
- Manage therapy by removing, editing, or inserting prescriptions.
4.1.3. Help Request
5. System Demonstration
5.1. Emotional State Detection and Management
5.2. Automatic Forwarding of Requests for Help in Case of Alarming Vital Parameters
5.3. Therapy Monitoring
5.4. Current and Historical Status of Parameters
- List of vital sign values: An up-to-date list of the current values of the measured vital parameters can be displayed, including vital information such as blood pressure, heart rate, body temperature, etc. This list provides an immediate overview of the user’s current health status, enabling timely monitoring and preliminary assessment.
- Weekly, monthly or yearly history: For a more in-depth view, actors can access a history of vital parameters measured over time. This history can be viewed on a weekly, monthly, or annual basis as required. Access to a broader history allows for the identification of trends, variations, and significant changes over time, providing a more comprehensive assessment and understanding of the user’s health status.
5.5. Therapy Management
- Monitor medication intake: users have the ability to check whether they have correctly taken their prescribed medications today or the past day, through direct questions that QTrobot asks the elderly person at specific times. This feature provides an easy way to keep track of intakes and promote proper medication compliance.
- View the list of prescribed medicines: users can view a complete list of medications they have been prescribed. This function provides a clear overview of the medications to be taken, helping to maintain complete control over the prescribed therapy.
- Update therapy: Users can make changes to existing prescriptions, such as adding or removing medications, or changing dosages or intake schedules. This flexibility allows for personalized and adaptive therapy management.
5.6. Automatic Forwarding of Generic Help Requests
6. Lessons Learned and Conclusions
- Highlighting the potential of integrating the Internet of Things (IoT) to improve healthcare for older people. Using a network of sensors, robotics, and AI, the research establishes a possible framework to facilitate continuous health monitoring, emergency response, and emotional support for the elderly population. This integration offers the prospect of promoting the independence and well-being of the elderly, preventing hospitalisation and allowing the elderly to remain comfortably in their homes for longer.
- Exploring the idea of combining technology with healthcare to help doctors care for older people using a special medical scoring system called MEWS. This helps to work out how well an older person is feeling.
- Emphasise the importance of addressing the social isolation of the elderly population through technological solutions. By incorporating emotional state monitoring and facilitating direct communication between carers, doctors, and older people, research suggests a possible way to combat loneliness.
- Illustrate the potential of technology to improve patient-centered care for older people. By offering real-time monitoring, personalised care and direct communication with carers and doctors, the research shows how the integration of robotics, sensors and AI can enable patients to become active participants in their care.
- Illustrate the potential of technology to improve patient-centered care for the elderly.
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Battistoni, P.; Cantone, A.A.; Martino, G.; Passamano, V.; Romano, M.; Sebillo, M.; Vitiello, G. A Cyber-Physical System for Wildfire Detection and Firefighting. Future Internet 2023, 15, 237. [Google Scholar] [CrossRef]
- Gregorio, M.D.; Romano, M.; Sebillo, M.; Vitiello, G.; Vozella, A. Improving human ground control performance in unmanned aerial systems. Future Internet 2021, 13, 188. [Google Scholar] [CrossRef]
- Frolli, A.; Ricci, M.; Cavallaro, A.; Rizzo, S.; Di Carmine, F. Virtual reality improves learning in children with ADHD. In Proceedings of the EDULEARN21 Proceedings, Online Conference, 5–6 July 2021; pp. 9229–9236. [Google Scholar]
- Frolli, A.; Savarese, G.; Di Carmine, F.; Bosco, A.; Saviano, E.; Rega, A.; Carotenuto, M.; Ricci, M.C. Children on the autism spectrum and the use of virtual reality for supporting social skills. Children 2022, 9, 181. [Google Scholar] [CrossRef] [PubMed]
- Di Gregorio, M.; Romano, M.; Sebillo, M.; Vitiello, G. Dyslexeasy-App to Improve Readability through the Extracted Summary for Dyslexic Users. In Proceedings of the CCNC, Las Vegas, NV, USA, 8–11 January 2022; pp. 1–6. [Google Scholar]
- Boutayeb, A. The double burden of communicable and non-communicable diseases in developing countries. Trans. R. Soc. Trop. Med. Hyg. 2006, 100, 191–199. Available online: http://xxx.lanl.gov/abs/https://academic.oup.com/trstmh/article-pdf/100/3/191/5314802/100-3-191.pdf (accessed on 20 July 2023). [CrossRef]
- Khosravi, P. Investigating the effectiveness of technologies applied to assist seniors: A systematic literature review. Int. J. Med. Inform. 2016, 85 1, 17–26. [Google Scholar] [CrossRef]
- Wu, H. Informal care and health behaviors among elderly people with chronic diseases. J. Health Popul. Nutr. 2017, 36, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Song, Y.; Ma, W.; Yi, X.; Wang, S.; Sun, X.; Tian, J.; Wang, S.; Zheng, C.; Zhang, B.; Xu, Z.; et al. Chronic Diseases Knowledge and Related Factors among the Elderly in Jinan, China. PLoS ONE 2013, 8, e68599. [Google Scholar] [CrossRef]
- Cheung, G. Financial difficulty and biopsychosocial predictors of loneliness: A cross-sectional study of community dwelling older adults. Arch. Gerontol. Geriatr. 2019, 85, 103935. [Google Scholar] [CrossRef]
- Kaur, D.; Rasane, P.; Singh, J.; Kaur, S.; Kumar, V.; Mahato, D.K.; Dey, A.; Dhawan, K.; Kumar, S. Nutritional Interventions for Elderly and Considerations for the Development of Geriatric Foods. Curr. Aging Sci. 2019, 12, 15–27. [Google Scholar] [CrossRef]
- Liu, Z. Dietary Micronutrients Intake Status among Chinese Elderly People Living at Home: Data from CNNHS 2010–2012. Nutrients 2019, 11, 1787. [Google Scholar] [CrossRef] [PubMed]
- Van Maanen, A.C.D.; Wilting, I.; Jansen, P.A.F. Prescribing medicines to older people—How to consider the impact of ageing on human organ and body functions. Br. J. Clin. Pharmacol. 2019, 86, 1921–1930. [Google Scholar] [CrossRef]
- Brodsky, J.; Habib, J.; Hirschfeld, M.J. Key Policy Issues in Long-Term Care; World Health Organization: Geneva, Switzerland, 2003. [Google Scholar]
- Carolis, B.D. Simulating empathic behavior in a social assistive robot. Multimed. Tools Appl. 2017, 76, 5073–5094. [Google Scholar] [CrossRef]
- Amato, F.; Di Gregorio, M.; Monaco, C.; Sebillo, M.; Tortora, G.; Vitiello, G. Socially Assistive Robotics combined with Artificial Intelligence for ADHD. In Proceedings of the 2021 IEEE 18th Annual Consumer Communications & Networking Conference(CCNC), Las Vegas, NV, USA, 9–12 January 2021; pp. 1–6. [Google Scholar] [CrossRef]
- Amato, F.; Di Gregorio, M.; Monaco, C.; Sebillo, M.; Tortora, G.; Vitiello, G. The Therapeutic Use of Humanoid Robots for Behavioral Disorders. In Proceedings of the AVI ’20, International Conference on Advanced Visual Interfaces, Salerno, Italy, 28 September–2 October 2020. [Google Scholar] [CrossRef]
- Hu, R.; Kabouteh, A.; Pawlitza, K.; Güttler, J.; Linner, T.; Bock, T. Developing Personalized Intelligent Interior Units to Promote Activity and Customized Healthcare for Aging Society. In Proceedings of the 36th International Symposium on Automation and Robotics in Construction (ISARC), Banff, AB, Canada, 21–24 May 2019; Al-Hussein, M., Ed.; pp. 234–241. [Google Scholar] [CrossRef]
- Fong, T.; Nourbakhsh, I.; Dautenhahn, K. A Survey of Socially Interactive Robots. Robot. Auton. Syst. 2003, 42, 143–166. [Google Scholar] [CrossRef]
- Abdi, J. Scoping review on the use of socially assistive robot technology in elderly care. BMJ Open 2018, 8, e018815. [Google Scholar] [CrossRef]
- Pu, L. The Effectiveness of Social Robots for Older Adults: A Systematic Review and Meta-Analysis of Randomized Controlled Studies. Gerontologist 2018, 59, e37–e51. [Google Scholar] [CrossRef]
- Sinnema, L. The Attitude of Elderly and Young Adults Towards a Humanoid Robot as a Facilitator for Social Interaction. In Proceedings of the Social Robotics: 11th International Conference, ICSR 2019, Madrid, Spain, 26–29 November 2019; pp. 24–33. [Google Scholar] [CrossRef]
- Gardner-Thorpe, J.; Love, N.; Wrightson, J.; Walsh, S.; Keeling, N. The Value of Modified Early Warning Score (MEWS) in Surgical In-Patients: A Prospective Observational Study. Ann. R. Coll. Surg. Engl. 2006, 88, 571–575. [Google Scholar] [CrossRef]
- Boch, A.; Ryan, S.; Kriebitz, A.; Amugongo, L.M.; Lütge, C. Beyond the Metal Flesh: Understanding the Intersection between Bio- and AI Ethics for Robotics in Healthcare. Robotics 2023, 12, 110. [Google Scholar] [CrossRef]
- Mintrom, M.; Sumartojo, S.; Kulic, D.; Tian, L.; Carreno, P.; Allen, A. Robots in public spaces: Implications for policy design. Policy Des. Pract. 2021, 5, 123–139. [Google Scholar] [CrossRef]
- Alboksmaty, A.; Solomons, N.; Gul, S.; Neves, A.; Aylin, P. Remote patient monitoring at home using ambient sensors: A systematic review. Eur. J. Public Health 2022, 32, ckac130.065. Available online: http://xxx.lanl.gov/abs/https://academic.oup.com/eurpub/article-pdf/32/Supplement_3/ckac130.065/48592155/ckac130.065.pdf (accessed on 20 July 2023). [CrossRef]
- Aminosharieh Najafi, T.; Abramo, A.; Kyamakya, K.; Affanni, A. Development of a Smart Chair Sensors System and Classification of Sitting Postures with Deep Learning Algorithms. Sensors 2022, 22, 5585. [Google Scholar] [CrossRef] [PubMed]
- Evans, J.; Papadopoulos, A.; Silvers, C.; Charness, N.; Boot, W.; Schlachta-Fairchild, L.; Crump, C.; Martinez, M.; Ent, C. Remote Health Monitoring for Older Adults and Those with Heart Failure: Adherence and System Usability. Telemed. J. e-Health Off. J. Am. Telemed. Assoc. 2015, 22, 480–488. [Google Scholar] [CrossRef]
- Fujioka, J.K.; Budhwani, S.; Thomas-Jacques, T.; De Vera, K.; Challa, P.; Fuller, K.; Hogeveen, S.; Gordon, D.; Shahid, S.; Seto, E.; et al. Challenges and Strategies for Promoting Health Equity in Virtual Care: Protocol for a Scoping Review of Reviews. JMIR Res. Protoc. 2020, 9, e22847. [Google Scholar] [CrossRef]
- Stavropoulos, T.; Papastergiou, A.; Mpaltadoros, L.; Nikolopoulos, S.; Kompatsiaris, I. IoT Wearable Sensors and Devices in Elderly Care: A Literature Review. Sensors 2020, 20, 2826. [Google Scholar] [CrossRef] [PubMed]
- Abidoye, A. Using Wearable Sensors for Remote Healthcare Monitoring System. J. Sens. Technol. 2011, 1, 22–28. [Google Scholar] [CrossRef]
- Schall, M.; Sesek, R.; Cavuoto, L. Barriers to the Adoption of Wearable Sensors in the Workplace: A Survey of Occupational Safety and Health Professionals. Hum. Factors 2018, 60, 18720817753907. [Google Scholar] [CrossRef] [PubMed]
- Botsis, T.; Demiris, G.; Pedersen, S.; Hartvigsen, G. Home telecare technologies for the elderly. J. Telemed. Telecare 2008, 14, 333–337. [Google Scholar] [CrossRef] [PubMed]
- Van den Berg, N.; Schumann, M.; Kraft, K.; Hoffmann, W. Telemedicine and Telecare for Older Patients—A Systematic Review. Maturitas 2012, 73, 94–114. [Google Scholar] [CrossRef]
- Zaman, S.B.; Khan, R.; Evans, R.; Thrift, A.; Maddison, R.; Shariful Islam, S.M. Exploring barriers to, and enablers of, the adoption of information and communication technology for the care of older adults with chronic diseases: A scoping review. JMIR Aging 2020, 5, e25251. [Google Scholar] [CrossRef]
- López, N.; Ponce, S.; Piccinini, D.; Berenguer, E.; Roberti, M. From Hospital to Home Care: Creating a Domotic Environment for Elderly and Disabled People. IEEE Pulse 2016, 7, 38–41. [Google Scholar] [CrossRef]
- Martin, S.; Kelly, G.; Kernohan, W.; Mccreight, B.; Nugent, C. Smart Home technologies for Health and Social Care Support. Cochrane Database Syst. Rev. 2008, 8, CD006412. [Google Scholar] [CrossRef]
- Liu, L.; Stroulia, E.; Nikolaidis, I.; Cruz, A.; Ríos-Rincón, A.M. Smart homes and home health monitoring technologies for older adults: A systematic review. Int. J. Med. Inform. 2016, 91, 44–59. [Google Scholar] [CrossRef]
- Iancu, I.; Iancu, B. Elderly in the Digital Era. Theoretical Perspectives on Assistive Technologies. Technologies 2017, 5, 60. [Google Scholar] [CrossRef]
- Zsiga, K.; Edelmayer, G.; Rumeau, P.; Péter, O.; Tóth, A.; Fazekas, G. Home care robot for socially supporting the elderly: Focus group studies in three European countries to screen user attitudes and requirements. Int. J. Rehabil. Res. 2013, 36, 375–378. [Google Scholar] [CrossRef]
- Jose, F.; Livaldo, Mahardhika, M.; Sukiman, N.; Spits Warnars, H.L.H.; Ramadhan, A.; Herry Utomo, W. Mobile Application for Elderly Care. In Proceedings of the 2022 Second International Conference on Artificial Intelligence and Smart Energy (ICAIS), Coimbatore, India, 23–25 February 2022; pp. 968–974. [Google Scholar] [CrossRef]
- Portenhauser, A.; Terhorst, Y.; Schultchen, D.; Sander, L.; Denkinger, M.; Stach, M.; Waldherr, N.; Dallmeier, D.; Baumeister, H.; Messner, E. Mobile Apps for Older Adults: Systematic Search and Evaluation Within Online Stores. JMIR Aging 2021, 4, e23313. [Google Scholar] [CrossRef] [PubMed]
- Sasama, R. An Experiment for Motivating Elderly People with Robot Guided Interaction. In Universal Access in Human-Computer Interaction. Users Diversity; Stephanidis, C., Ed.; Springer: Berlin/Heidelberg, Germany, 2011. [Google Scholar] [CrossRef]
- Görer, B. An autonomous robotic exercise tutor for elderly people. Auton. Robot. 2017, 41, 657–678. [Google Scholar] [CrossRef]
- Tanaka, M. Effect of a human-type communication robot on cognitive function in elderly women living alone. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2012, 18, CR550–CR557. [Google Scholar] [CrossRef]
- Piasek, J. Acceptance and Long-Term Use of a Social Robot by Elderly Users in a Domestic Environment. In Proceedings of the 2018 11th International Conference on Human System Interaction (HSI), Gdansk, Poland, 4–6 July 2018. [Google Scholar] [CrossRef]
- Sakairi, K. Research of robot-assisted activity for the elderly with senile dementia in a group home. In Proceedings of the SICE 2004 Annual Conference, Sapporo, Japan, 4–6 August 2004. [Google Scholar] [CrossRef]
- Wada, K. Robot assisted activity for elderly people and nurses at a day service center. In Proceedings of the 2002 IEEE International Conference on Robotics and Automation (Cat. No.02CH37292), Washington, DC, USA, 11–15 May 2002. [Google Scholar] [CrossRef]
- Gasteiger, N. Older adults’ experiences and perceptions of living with Bomy, an assistive dailycare robot: A qualitative study. Assist. Technol. 2021, 34, 487–497. [Google Scholar] [CrossRef] [PubMed]
- Kolstad, M.; Yamaguchi, N.; Babic, A.; Nishihara, Y. Integrating Socially Assistive Robots into Japanese Nursing Care. Stud. Health Technol. Inform. 2020, 270, 1323–1324. [Google Scholar]
- Abufadda, M.; Mansour, K. A Survey of Synthetic Data Generation for Machine Learning. In Proceedings of the 22nd International Arab Conference on Information Technology (ACIT), Muscat, Oman, 21–23 December 2021; pp. 1–7. [Google Scholar] [CrossRef]
- Jordon, J.; Szpruch, L.; Houssiau, F.; Bottarelli, M.; Cherubin, G.; Maple, C.; Cohen, S.; Weller, A. Synthetic Data–What, Why and How? The Alan Turing Institute; The Royal Society: London, UK, 2022. [Google Scholar]
- LuxAI. QTrobot V2–Humanoid Social Robot for Human AI Research & Teaching. Available online: https://luxai.com/humanoid-social-robot-for-research-and-teaching/ (accessed on 20 July 2023).
- Maccarone, N.; Guerri, I.; Franchi, M.; Fricelli, C.; Perretta, L.; Zagli, G.; Spina, R.; Linden, M.; Bonizzoli, M.; Peris, A. Impact of a systematic MEWS introduction on preoperative and postoperative evaluation in urgent/emergency surgery. Crit. Care 2010, 14, P255. [Google Scholar] [CrossRef][Green Version]












{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Participant ID | Age | Sex | Specialization | Readhesion |
|---|---|---|---|---|
| 1 | 35 | M | Geriatrician, cardiologist | x |
| 2 | 51 | M | Geriatrician, internist | |
| 3 | 56 | F | Geriatrician | x |
| 4 | 39 | M | Geriatrician, angiologist, | x |
| 5 | 45 | F | Geriatrician, cardiologist, hepatologist | |
| 6 | 67 | M | Geriatrician, cardiologist, internist | |
| 7 | 46 | M | Geriatrician, angiologist, | |
| 8 | 49 | F | Geriatrician, cardiologist | |
| 9 | 68 | F | Geriatrician, cardiologist, hepatologist | x |
| 10 | 37 | M | Geriatrician, cardiologist, internist |
| Category | Requirement | Actor |
|---|---|---|
| Monitoring | Display the current status of the parameters; | E C D |
| Display of parameter history (weekly, monthly, annual); | E C D | |
| Monitoring of daily therapy or a specific date; | E C D Q | |
| Display of the list of prescribed medicines; | E C D | |
| Detection of elderly person; | Q | |
| Management of therapy; | C D Q | |
| Communication | Automatic submission of help requests in case of alarming vital signs; | Q |
| Emotional state detection and management; | Q | |
| Automatic forwarding of generic help requests, allowing the elderly to request assistance in case of non-specific need. | C Q |
| Robot Name | Microcontroller/ Processors/OS | Sensors/ Actuators | Mobility | Communication |
|---|---|---|---|---|
| QTrobot for Research V2 | Raspberry Pi 4 Model B; 8th Gen quad-core Intel (R) NUC 10 Core (TM) i5/i7 processor; Ubuntu - ROS Noetic | 4× High Performance Far Field Microphone Array; RealSense(TM) depth camera D4555 | none | USB-C USB 3.0; WiFi IEEE 802.22 Ethernet HDMI |
| Parameters | 3 | 2 | 1 | 0 | 1 | 2 | 3 |
|---|---|---|---|---|---|---|---|
| Blood pressure | ≤70 | 71–80 | 81–100 | 101–199 | ≥200 | ||
| Heart rate | <40 | 41/50 | 51/100 | 101–110 | 111–129 | ≥130 | |
| Respiratory rate | <9 | 9/14 | 15/20 | 21/29 | ≥30 | ||
| Temperature | <35 | 35–38.4 | ≥38.5 | ||||
| Level of consciousness | A | B | C | D |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cantone, A.A.; Esposito, M.; Perillo, F.P.; Romano, M.; Sebillo, M.; Vitiello, G. Enhancing Elderly Health Monitoring: Achieving Autonomous and Secure Living through the Integration of Artificial Intelligence, Autonomous Robots, and Sensors. Electronics 2023, 12, 3918. https://doi.org/10.3390/electronics12183918
Cantone AA, Esposito M, Perillo FP, Romano M, Sebillo M, Vitiello G. Enhancing Elderly Health Monitoring: Achieving Autonomous and Secure Living through the Integration of Artificial Intelligence, Autonomous Robots, and Sensors. Electronics. 2023; 12(18):3918. https://doi.org/10.3390/electronics12183918
Chicago/Turabian StyleCantone, Andrea Antonio, Mariarosaria Esposito, Francesca Pia Perillo, Marco Romano, Monica Sebillo, and Giuliana Vitiello. 2023. "Enhancing Elderly Health Monitoring: Achieving Autonomous and Secure Living through the Integration of Artificial Intelligence, Autonomous Robots, and Sensors" Electronics 12, no. 18: 3918. https://doi.org/10.3390/electronics12183918
APA StyleCantone, A. A., Esposito, M., Perillo, F. P., Romano, M., Sebillo, M., & Vitiello, G. (2023). Enhancing Elderly Health Monitoring: Achieving Autonomous and Secure Living through the Integration of Artificial Intelligence, Autonomous Robots, and Sensors. Electronics, 12(18), 3918. https://doi.org/10.3390/electronics12183918