
Development of an Electrooculogram (EOG) and Surface Electromyogram (sEMG)-Based Human Computer Interface (HCI) Using a Bone Conduction Headphone Integrated Bio-Signal Acquisition System


Abstract
:1. Introduction
2. Materials and Methods
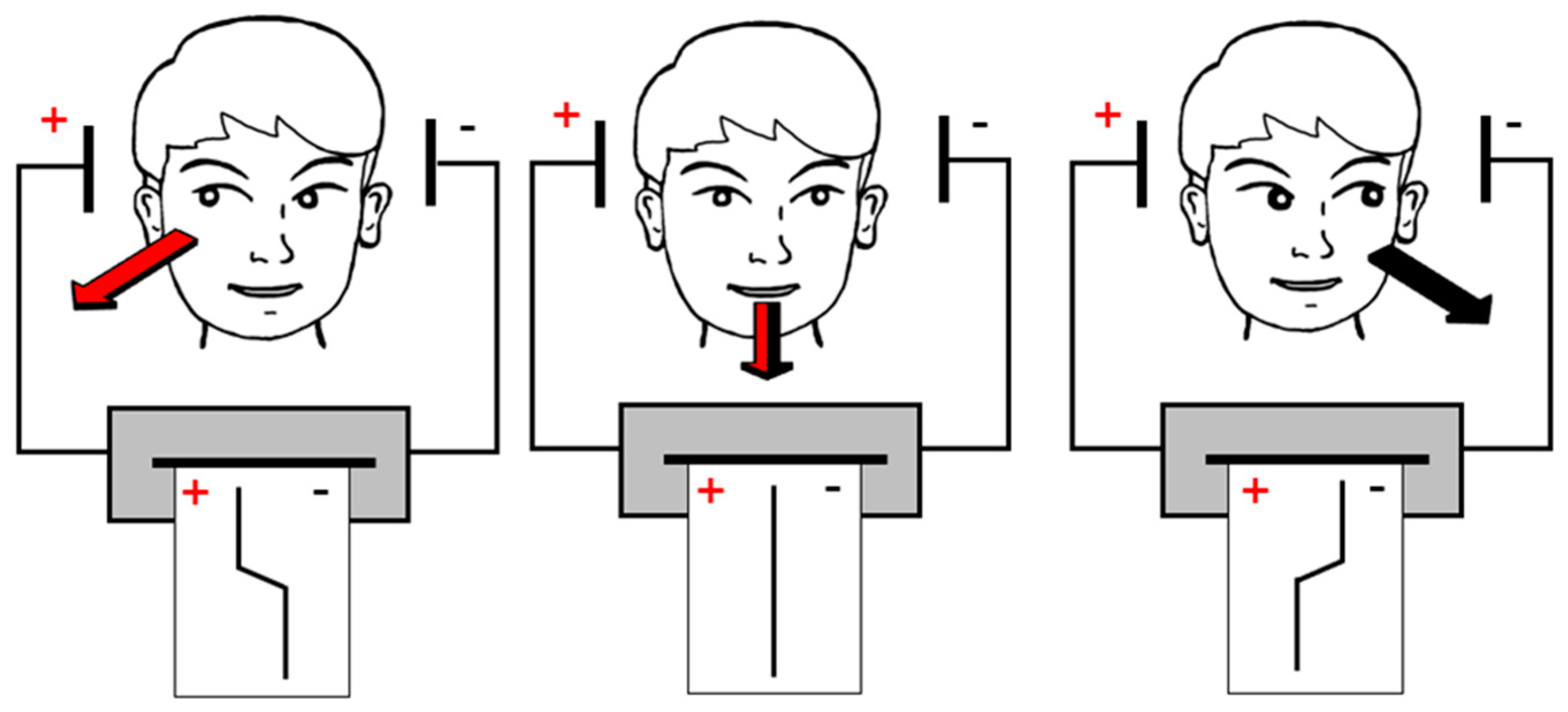
2.1. EOG and EMG Signals
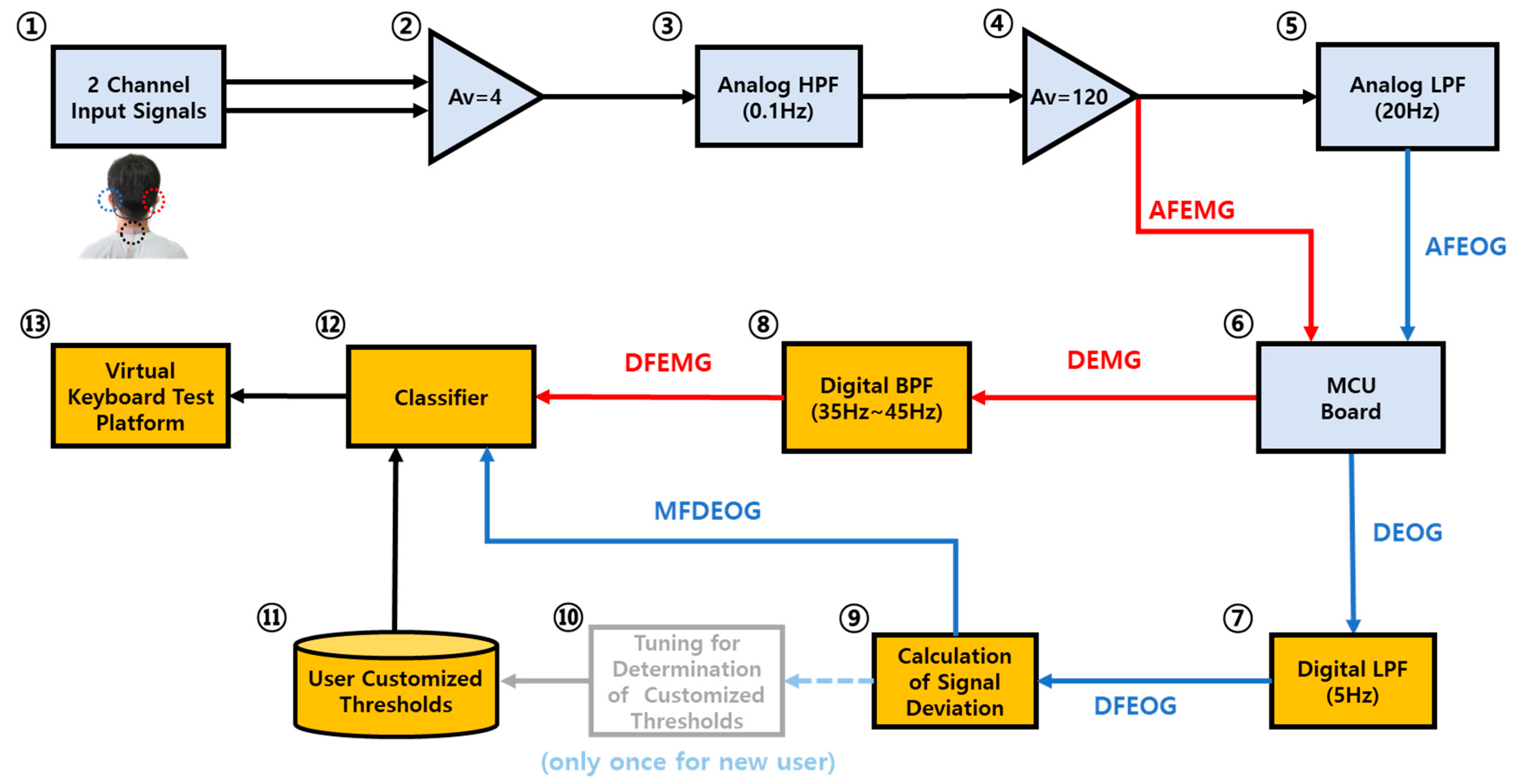
2.2. EOG and EMG Signal Acquisition System
2.2.1. Bone Conduction Headphone-Integrated Electrodes
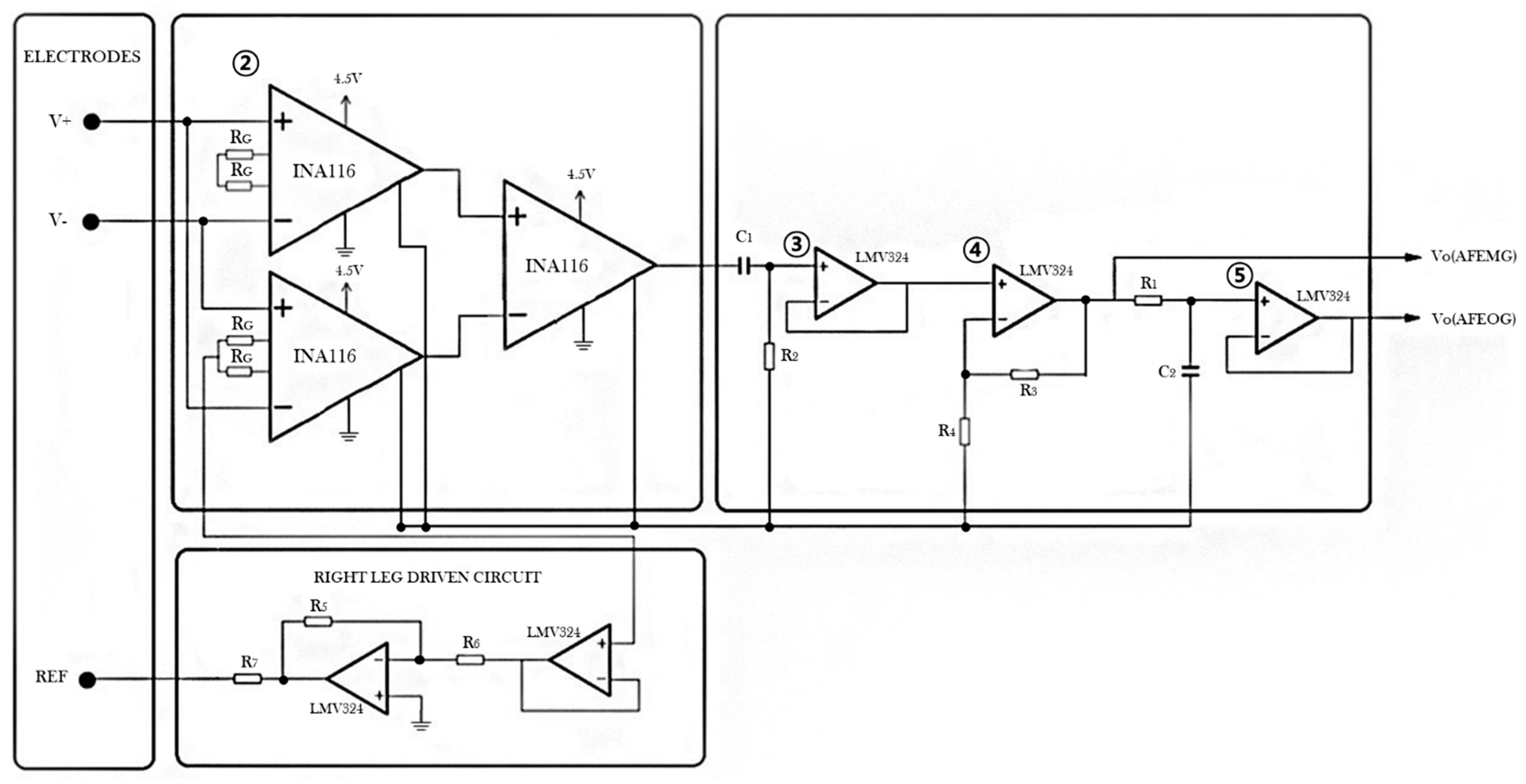
2.2.2. Signal Amplifier and Analog Filters
2.2.3. MCU Unit for A/D Conversion and Serial Communication
2.3. Moving Average Filtered Deviation of EOG (MFDEOG) Signal for Feature Extraction
2.4. Classification
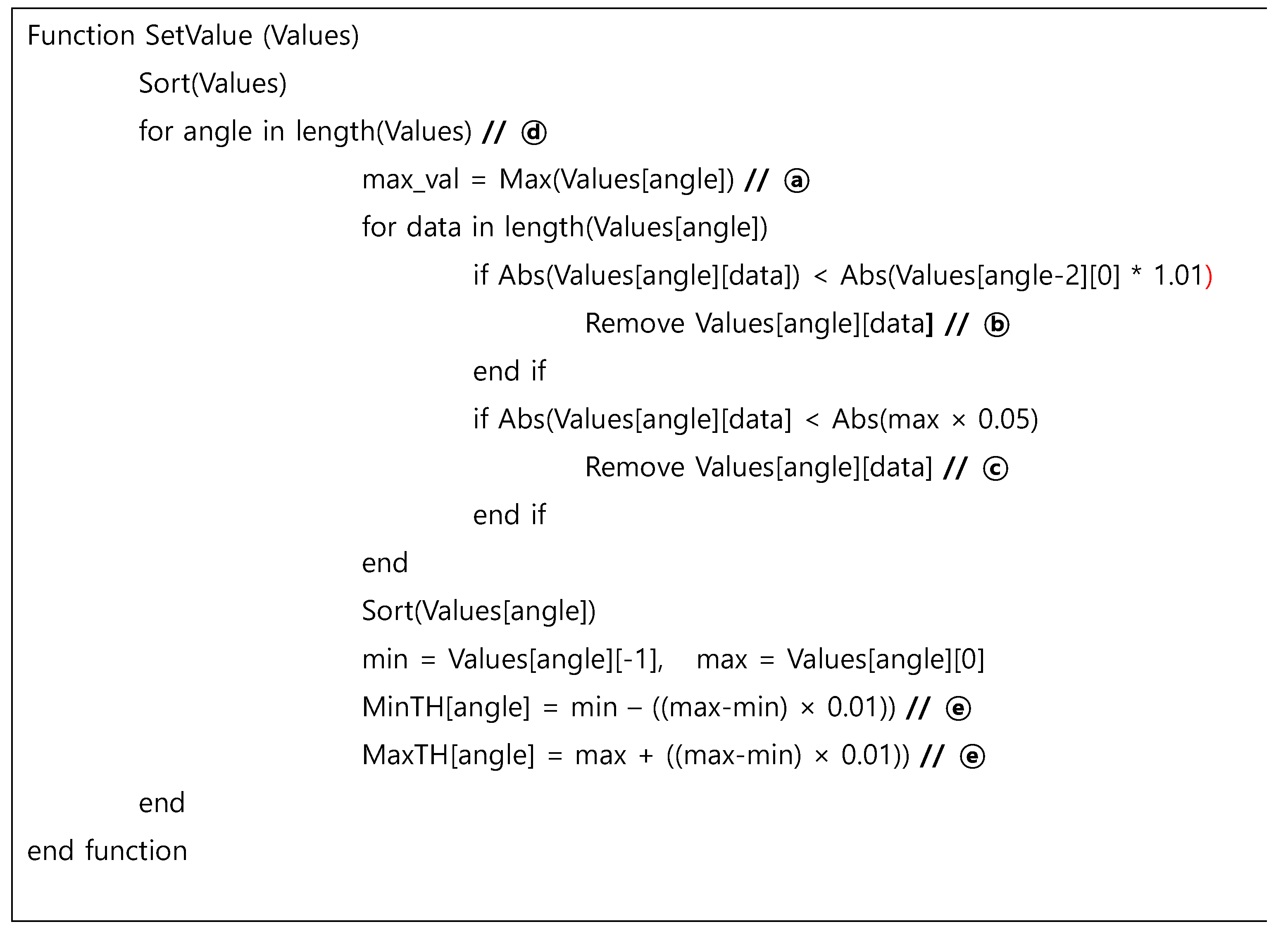
2.4.1. Individual Threshold-Based EOG Signal Classification of the Angle of Eye Movement
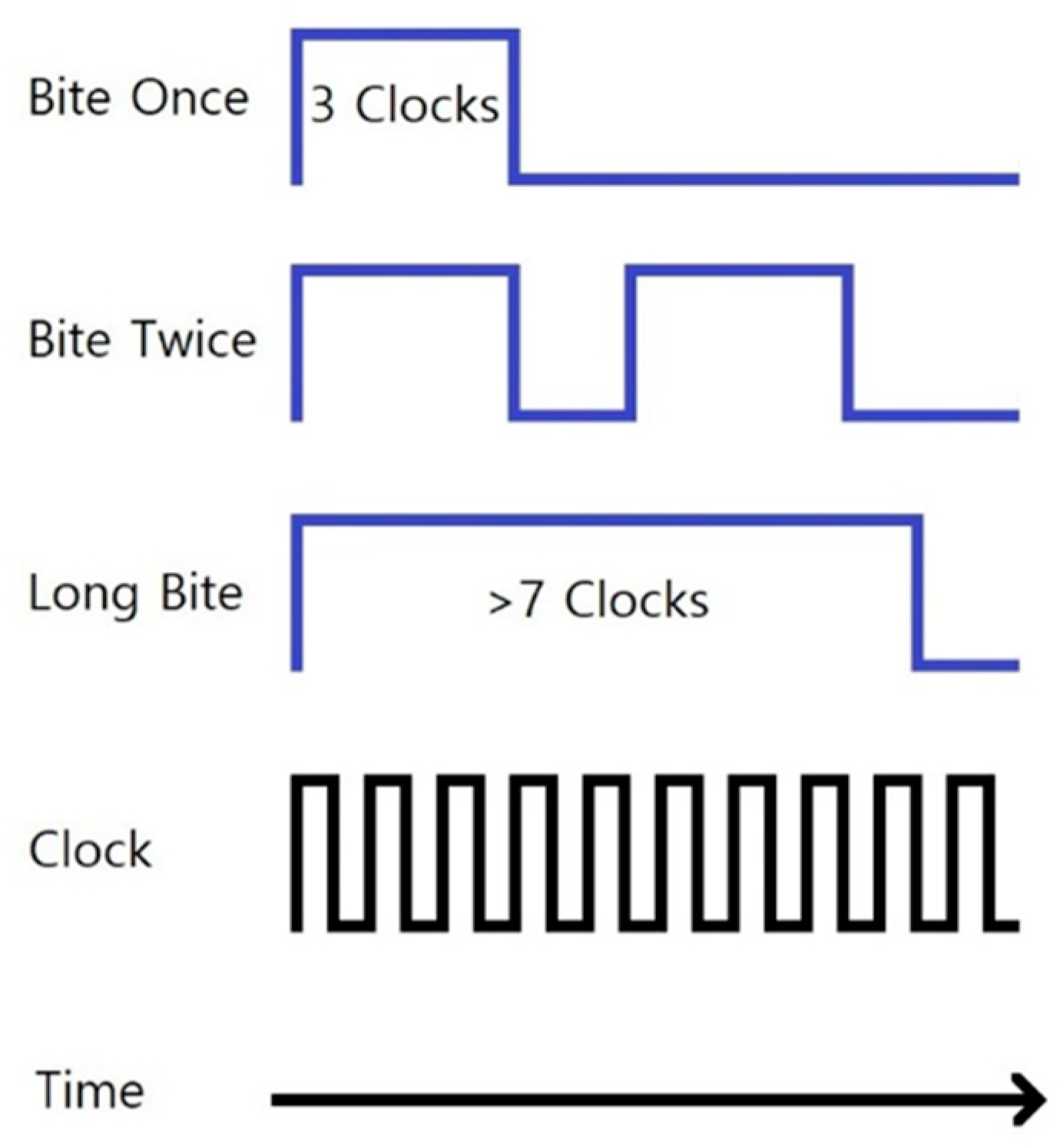
2.4.2. Classification of EMG of the Masseter Muscle
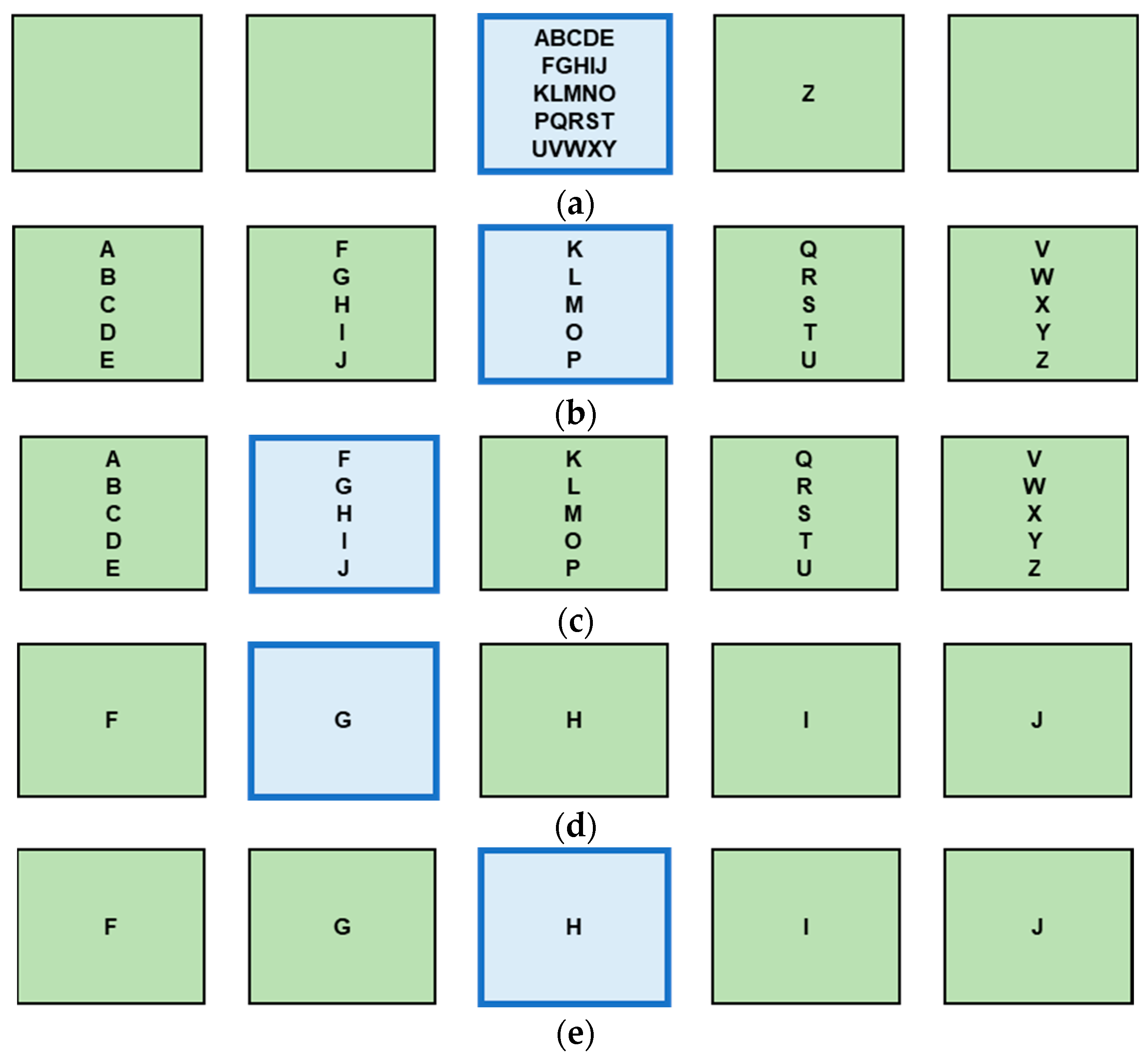
2.5. Design of Virtual Keyboard Interface
3. Results and Discussion
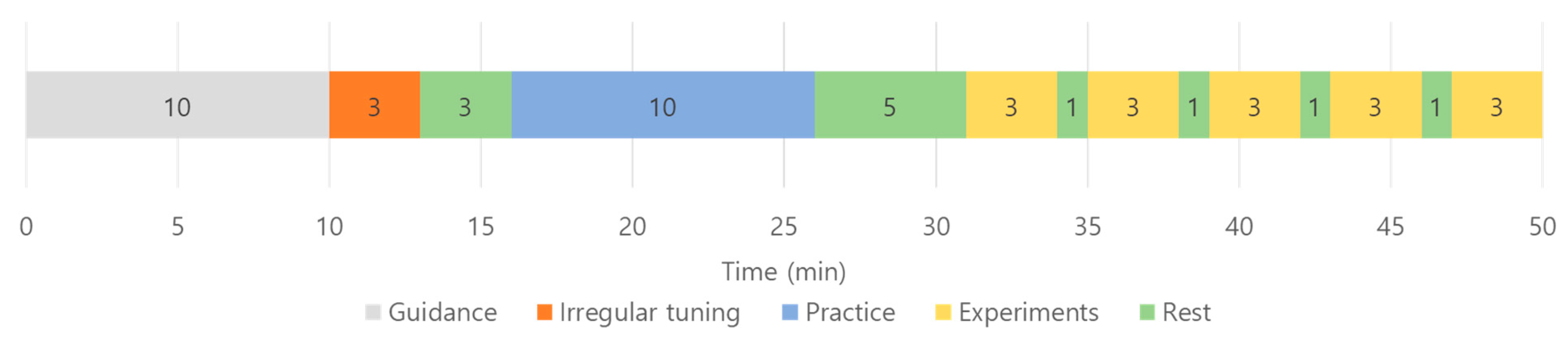
3.1. Experiment Environment and Subject Information
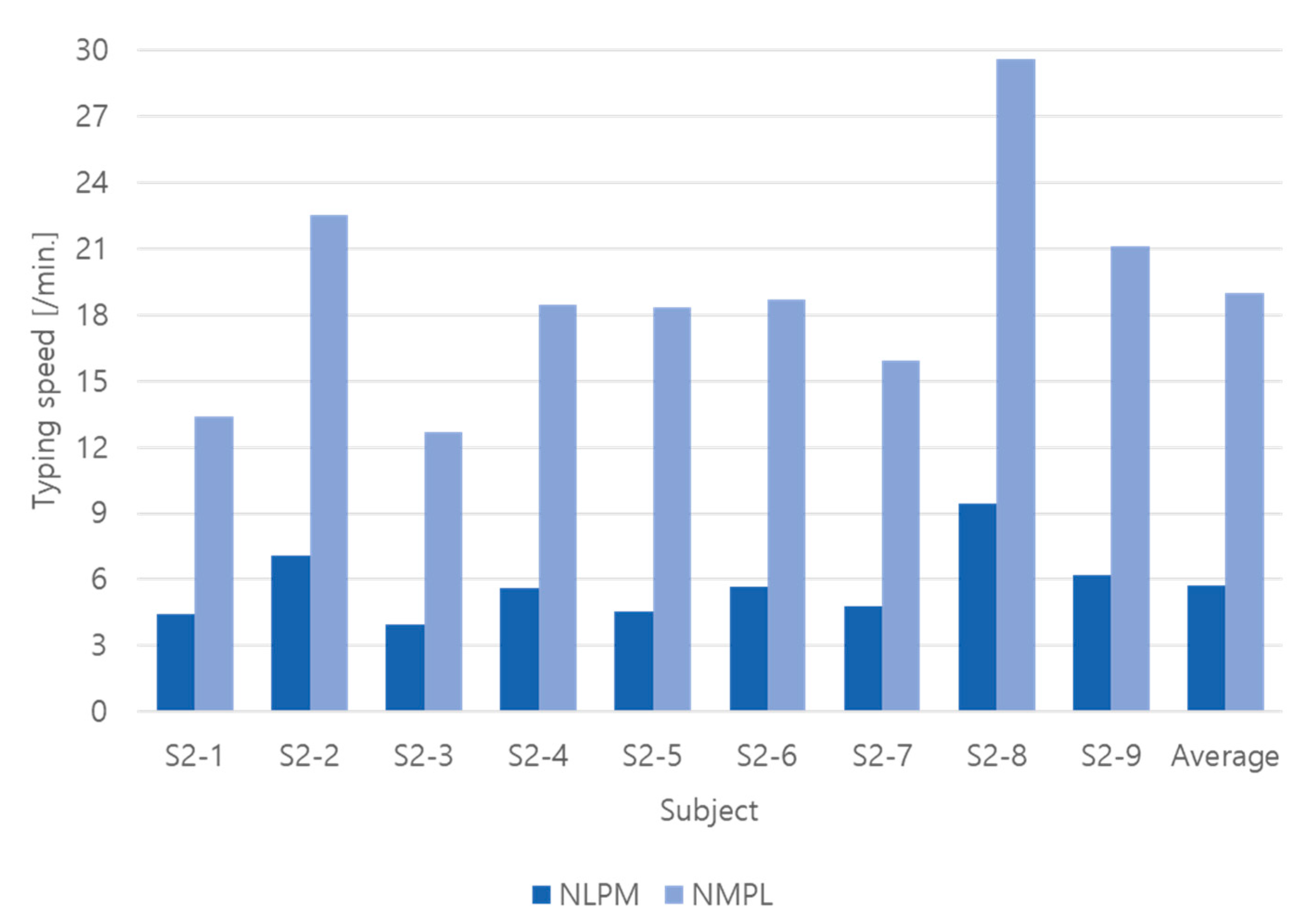
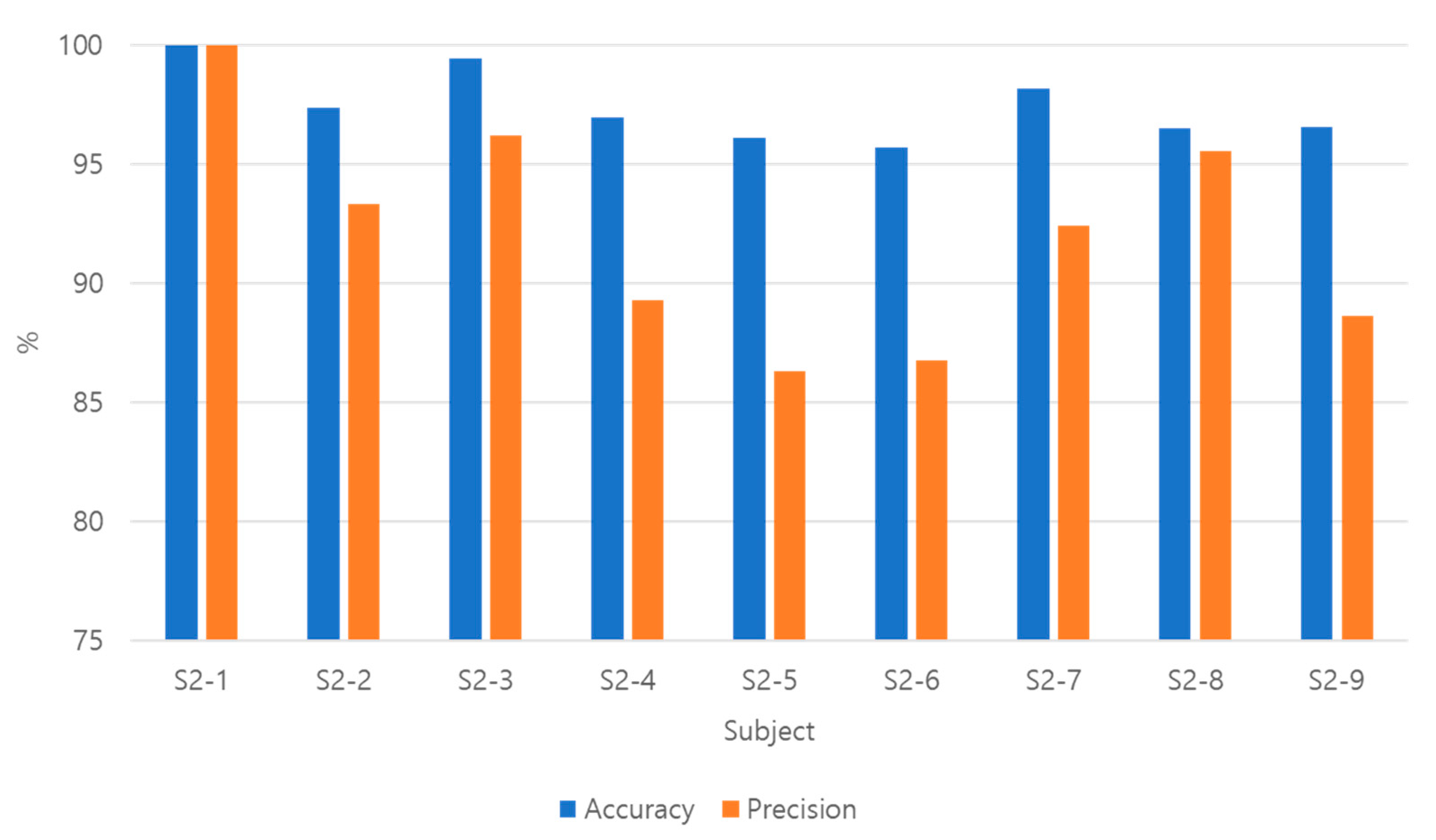
3.2. Experiment Result
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Postelnicu, C.; Girbacia, F.; Talaba, D. EOG-based visual navigation interface development. Expert Syst. Appl. 2012, 39, 10857–10866. [Google Scholar] [CrossRef]
- López, A.; Fernández, M.; Rodríguez, H.; Ferrero, F.; Postolache, O. Development of an EOG-based system to control a serious game. Measurement 2018, 127, 481–488. [Google Scholar] [CrossRef]
- Ang, A.M.S.; Zhang, Z.G.; Hung, Y.S.; Mak, J.N.F. A User-Friendly Wearable Single-Channel EOG-Based Human-Computer Interface for Cursor Control. In Proceedings of the International IEEE/EMBS Conference on Neural Engineering (NER), Montpellier, France, 22–24 July 2015. [Google Scholar] [CrossRef]
- Barbara, N.; Camilleri, T.A.; Camilleri, K.P. Comparative Performance Analysis of a Commercial Wearable EOG Glasses for an Asynchronous Virtual Keyboard. In Proceedings of the International BCS Human Computer Interaction Conference (HCI), Belfast, UK, 4–6 July 2018. [Google Scholar] [CrossRef]
- Manabe, H.; Fukumoto, M.; Yagi, T. Conductive rubber electrodes for earphone-based eye gesture input interface. Pers. Ubiquit. Comput. 2015, 19, 143–154. [Google Scholar] [CrossRef]
- Hládek, Ľ.; Porr, B.; Brimijoin, W.O. Real-time estimation of horizontal gaze angle by saccade integration using in-ear electrooculography. PLoS ONE 2018, 13, e0190420. [Google Scholar] [CrossRef] [PubMed]
- Keskinoğlu, C.; Aydın, A. EOG—Based Computer Control System for People with Mobility Limitations. Eur. J. Sci. Technol. 2021, 26, 256–261. [Google Scholar] [CrossRef]
- Yamagishi, K.; Hori, J.; Miyakawa, M. Development of EOG Based Communication System Controlled by Eight Directional Eye Movements. In Proceedings of the 28th IEEE EMBS Annual International Conference, New York, NY, USA, 30 August–3 September 2006. [Google Scholar] [CrossRef]
- Sakurai, K.; Yan, M.; Tanno, K.; Tamura, H. Gaze Estimation Method Using Analysis of Electrooculogram Signals and Kinect Sensor. Comput. Intell. Neurosci. 2017, 2017, 2074752. [Google Scholar] [CrossRef] [PubMed]
- Dhillon, H.S.; Singla, R.; Rekhi, N.S.; Jha, R. EOG and EMG Based Virtual Keyboard: A Brain-Computer Interface. In Proceedings of the IEEE International Conference on Computer Science and Information Technology, Beijing, China, 8–11 August 2009. [Google Scholar] [CrossRef]
- Banerjee, A.; Datta, S.; Pal Konar, A.; Tibarewala, D.N.; Janarthanan, R. Classifying Electrooculogram to Detect Directional Eye Movements. Procedia Technol. 2013, 10, 67–75. [Google Scholar] [CrossRef]
- Heide, W.; Koenig, E.; Trillenberg, P.; Kömpf, D.; Zee, D.S. Electrooculography: Technical standards and applications. The Inter-national Federation of Clinical Neurophysiology. Electroencephalogram Clin. Neurophysiol. Suppl. 1999, 52, 223–240. [Google Scholar]
- Yang, J.-J.; Gang, G.W.; Kim, T.S. Development of EOG-Based Human Computer Interface (HCI) System Using Piecewise Linear Approximation (PLA) and Support Vector Regression (SVR). Electronics 2018, 7, 38. [Google Scholar] [CrossRef]
- Jamal, M. Signal Acquisition Using Surface EMG and Circuit Design Considerations for Robotic Prosthesis. In Computational Intelligence in Electromyography Analysis: A Perspective on Current Applications and Future Challenges; Naik, G., Ed.; IntechOpen: London, UK, 2012. [Google Scholar] [CrossRef]
- INA116 Datasheet. Available online: https://www.ti.com/product/INA116 (accessed on 27 July 2022).
- Kumar, D.; Poole, E. Classification of EOG for Human Computer Interface. In Proceedings of the Second Joint 24th Annual Conference and the Annual Fall Meeting of the Biomedical Engineering Society, Engineering in Medicine and Biology, Houston, TX, USA, 23–26 October 2002. [Google Scholar] [CrossRef]
- Shin, Y.; Lim, H.; Kang, M.; Seong, M.; Cho, H.; Kim, J. Normal range of eye movement and its relationship to age. Acta Ophthalmol. 2016, 94, S256. [Google Scholar] [CrossRef]
- Boghen, D.; Troost, B.T.; Daroff, R.B.; Dell’Osso, L.F.; Birkett, J.E. Velocity characteristics of normal human saccades. Invest Ophthalmol. 1974, 13, 619–623. [Google Scholar]
- Yee, R.D.; Schiller, V.L.; Lim, V.; Baloh, F.G.; Baloh, R.W.; Honrubia, V. Velocities of vertical saccades with different eye movement recording methods. Invest Ophthalmol Vis Sci. 1985, 26, 938–944. [Google Scholar]
- Yu, D.; Cho, H.G.; Kim, S.; Moon, B. Application of eye tracker for assessing saccadic eye movements. J. Korean Ophthalmic Opt. Soc. 2018, 23, 135–141. [Google Scholar] [CrossRef]
- Leigh, R.J.; Zee, D.S. The Neurology of Eye Movements, 5th ed.; Oxford University Press: New York, NY, USA, 2015; pp. 189–220. [Google Scholar]
- Hosni, S.M.; Shedeed, H.A.; Mabrouk, M.S.; Tolba, M.F. EEG-EOG based Virtual Keyboard: Toward Hybrid Brain Computer Interface. Neuroinformatics 2019, 17, 323–341. [Google Scholar] [CrossRef] [PubMed]
- Kherlopian, A.R.; Gerrein, J.P.; Yue, M.; Kim, K.E. Electrooculogram based System for Computer Control using A Multiple Feature Classification Model. In Proceedings of the 28th IEEE EMBS Annual International Conference, New York, NY, USA, 30 August–3 September 2006. [Google Scholar] [CrossRef]
- Lee, T.; Sung, K. Basics of Eye Movements and Nystagmus. J. Korean Bal. Soc. 2004, 3, 7–24. [Google Scholar]
- Ohl, S.; Brandt, S.A.; Kliegl, R. Secondary (micro-)saccades: The influence of primary saccade end point and target eccentricity on the process of postsaccadic fixation. Vis. Res. 2011, 51, 2340–2347. [Google Scholar] [CrossRef] [PubMed]
- Saravanakumar, D.; Vishnupriya, R.; Reddy, M.R. A Novel EOG based Synchronous and Asynchronous Visual Keyboard System. In Proceedings of the IEEE EMBS International Conference on Information Technology Applications in Biomedicine, Chicago, IL, USA, 19–22 September 2019. [Google Scholar] [CrossRef]
- Heo, J.; Yoon, H.; Park, K.S. A Novel Wearable Forehead EOG Measurement System for Human Computer Interfaces. Sensors 2017, 17, 1485. [Google Scholar] [CrossRef] [PubMed]
- Tangsuksant, W.; Aekmunkhongpaisal, C.; Cambua, P.; Charoenpong, T.; Chanwimalueang, T. Directional Eye Movement Detection System for Virtual Keyboard Controller. In Proceedings of the 5th 2012 Biomedical Engineering International Conference, Muang, Thailand, 5–7 December 2012. [Google Scholar] [CrossRef]
- Usakli., A.B.; Gurkan, S.; Aloise, F.; Vecchiato, G.; Babiloni, F. A Hybrid Platform Based on EOG and EEG Signals to Restore Communication for Patients Afflicted with Progressive Motor Neuron Diseases. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Minneapolis, MN, USA, 3–6 September 2009. [Google Scholar] [CrossRef]
- López, A.; Ferrero, F.; Yangüela, D.; Álvarez, C.; Postolache, O. Development of a Computer Writing System Based on EOG. Sensors 2017, 17, 1505. [Google Scholar] [CrossRef] [PubMed]
- Barbara, N.; Camilleri, T.A. Interfacing with a Speller Using EOG Glasses. In Proceedings of the IEEE International Conference on Systems, Man, and Cybernetics (SMC), Budapest, Hungary, 9–12 October 2016. [Google Scholar] [CrossRef]










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Subject | EOG | sEMG |
|---|---|---|
| S2-1 | 100 | 91.7 |
| S2-2 | 93.3 | 97.4 |
| S2-3 | 96.18 | 97.9 |
| S2-4 | 89.27 | 99.4 |
| S2-5 | 86.32 | 97.8 |
| S2-6 | 86.76 | 95.6 |
| S2-7 | 92.4 | 95.7 |
| S2-8 | 95.54 | 98.4 |
| S2-9 | 88.63 | 91 |
| Average | 92.04 | 96.10 |
| Subject | NLPM | NMPM |
|---|---|---|
| S2-1 | 4.46 | 13.38 |
| S2-2 | 7.08 | 22.5 |
| S2-3 | 3.98 | 12.7 |
| S2-4 | 5.6 | 18.48 |
| S2-5 | 4.56 | 18.32 |
| S2-6 | 5.66 | 18.69 |
| S2-7 | 4.82 | 15.94 |
| S2-8 | 9.43 | 29.6 |
| S2-9 | 6.18 | 21.11 |
| Average | 5.75 | 18.97 |
| Total: 13,656 | Prediction Positive | Prediction Negative |
|---|---|---|
| Real positive | 1478 (TP) | 155 (FN) |
| Real negative | 229 (FP) | 11,794 (TN) |
| Author | Type | Actions for Interface (Number of Commands) | Total Number of Commands | Accuracy (%) | Typing Speed (Letters/Min) | Number of Electrode | Test Text |
|---|---|---|---|---|---|---|---|
| proposed | C | Left (4), Right (4), Biting (3) | 11 | 97.19 | 5.75–18.97 | 3 | hello world |
| [8] | A | Up, Up-Right, Right, Down-Right, Down, Down-left, Left, Up-left, Blink | 9 | 90.4 | 12.1 | 4 | good morning |
| [23] | C | Left, Right, Eyebrow | 3 | N/A- | 3-6 | 5 | zebra, noisy, igloo, input, punch, pixel |
| [26] | A | Up, Down, Left, Right, Wink (2), Blink (2) | 36 | 94.2–98.78 | 12.42–17.14 | 5 | human computer interface |
| [27] | A | Up, Down, Left, Right, Blink (2) | 6 | 91.25–91.43 | 8.68–10.81 | 4 | Seoul national university |
| [28] | A | Up, Down, Left, Right, Blink | 5 | 95.20 | 2.37 | 6 | hello |
| [29] | A | Up, Down, Left, Right, Blink | 5 | 95 | 12.15 | 5 | water |
| [30] | B | Up, Down, Left, Right, Blink | 5 | 93 | 5.88 | 5 | hello world |
| [31] | B | Up, Down, Left, Right, Blink | 5 | 90.59 | 7.11 | 5 | water, good morning, day 0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jo, H.N.; Park, S.W.; Choi, H.G.; Han, S.H.; Kim, T.S. Development of an Electrooculogram (EOG) and Surface Electromyogram (sEMG)-Based Human Computer Interface (HCI) Using a Bone Conduction Headphone Integrated Bio-Signal Acquisition System. Electronics 2022, 11, 2561. https://doi.org/10.3390/electronics11162561
Jo HN, Park SW, Choi HG, Han SH, Kim TS. Development of an Electrooculogram (EOG) and Surface Electromyogram (sEMG)-Based Human Computer Interface (HCI) Using a Bone Conduction Headphone Integrated Bio-Signal Acquisition System. Electronics. 2022; 11(16):2561. https://doi.org/10.3390/electronics11162561
Chicago/Turabian StyleJo, Ha Na, Sung Woo Park, Han Gyeol Choi, Seok Hyun Han, and Tae Seon Kim. 2022. "Development of an Electrooculogram (EOG) and Surface Electromyogram (sEMG)-Based Human Computer Interface (HCI) Using a Bone Conduction Headphone Integrated Bio-Signal Acquisition System" Electronics 11, no. 16: 2561. https://doi.org/10.3390/electronics11162561
APA StyleJo, H. N., Park, S. W., Choi, H. G., Han, S. H., & Kim, T. S. (2022). Development of an Electrooculogram (EOG) and Surface Electromyogram (sEMG)-Based Human Computer Interface (HCI) Using a Bone Conduction Headphone Integrated Bio-Signal Acquisition System. Electronics, 11(16), 2561. https://doi.org/10.3390/electronics11162561