
Virtual/Augmented Reality for Rehabilitation Applications Using Electromyography as Control/Biofeedback: Systematic Literature Review

 , , , , , and
, , , , , and
Abstract
:1. Introduction
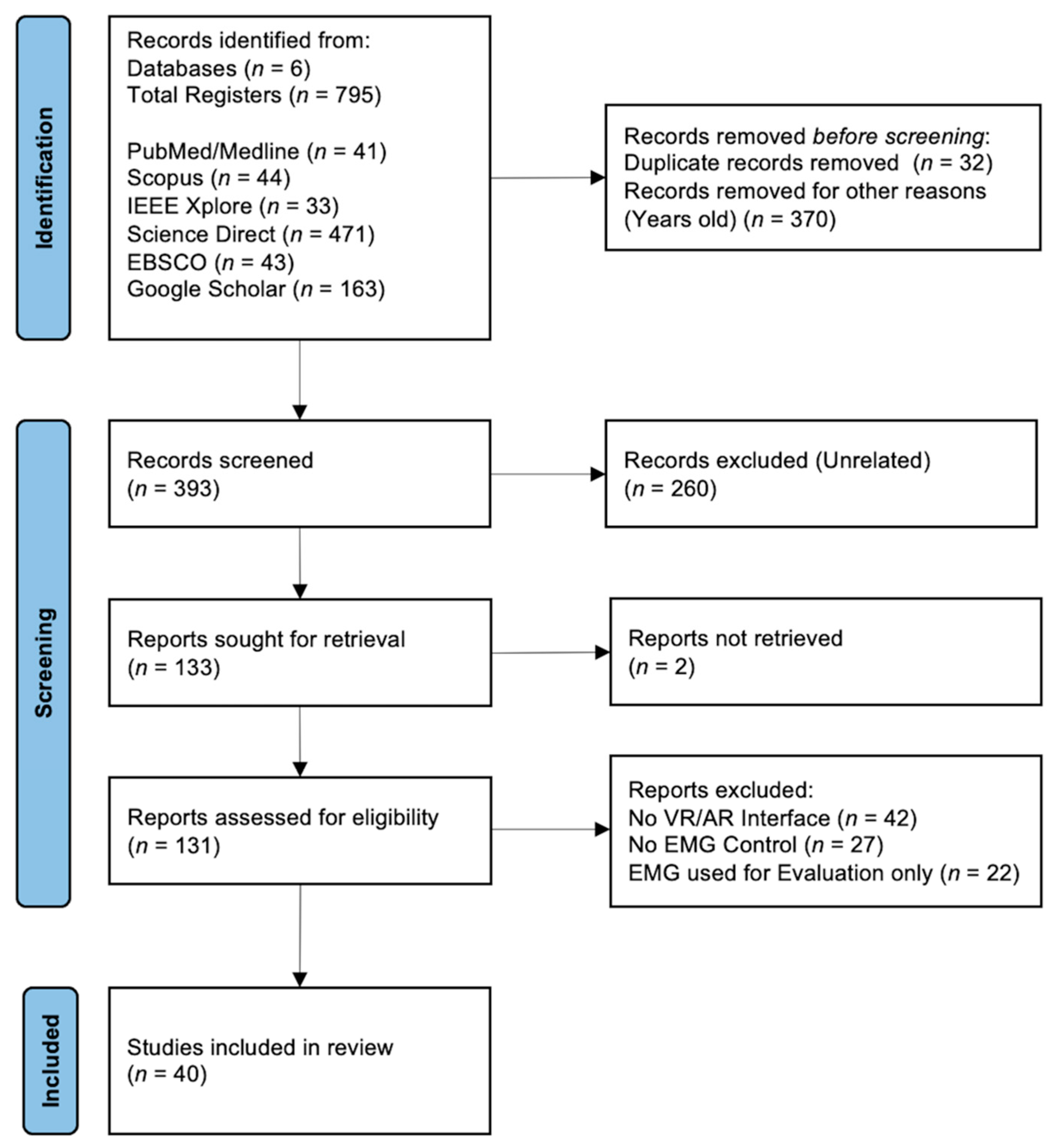
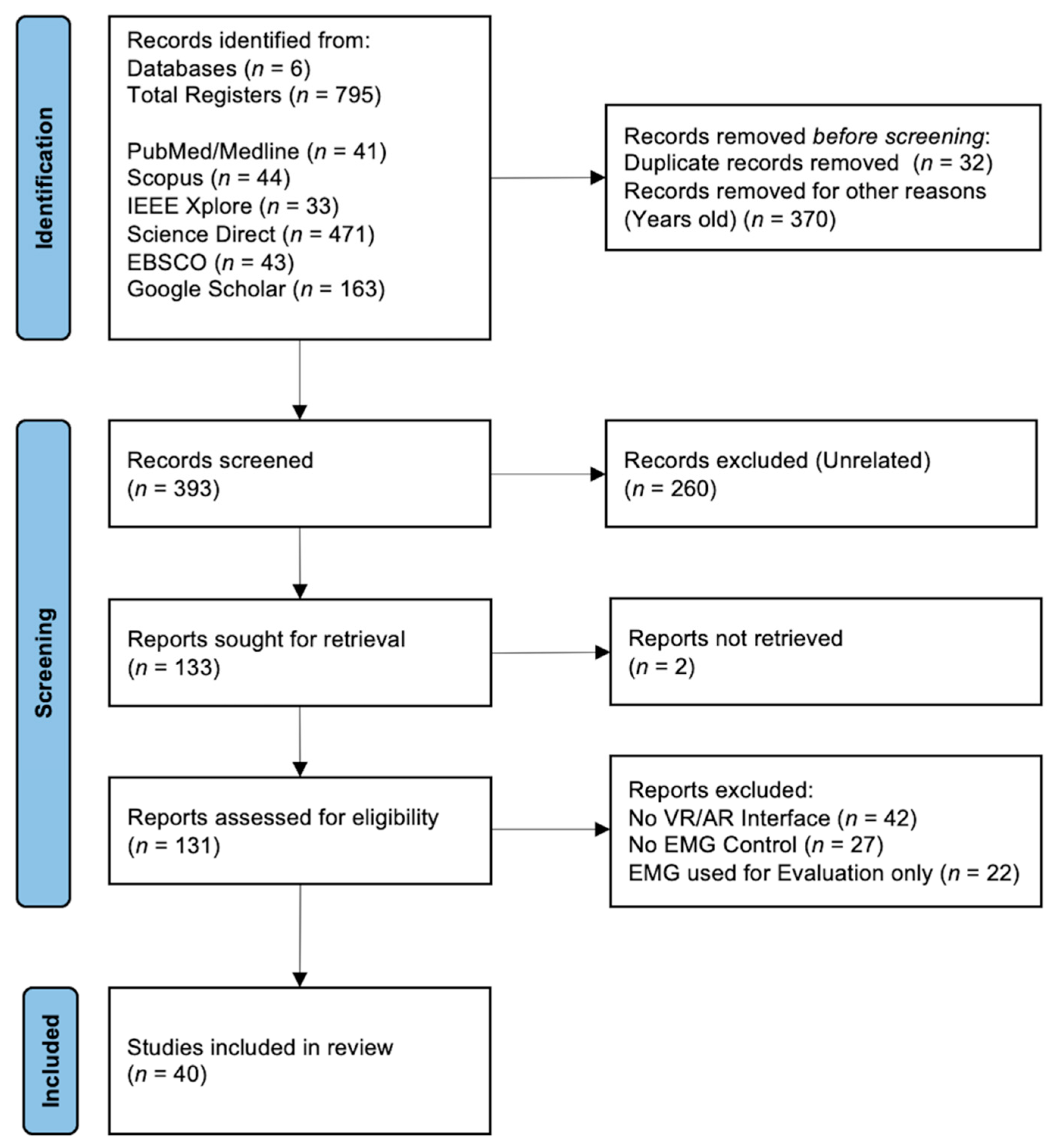
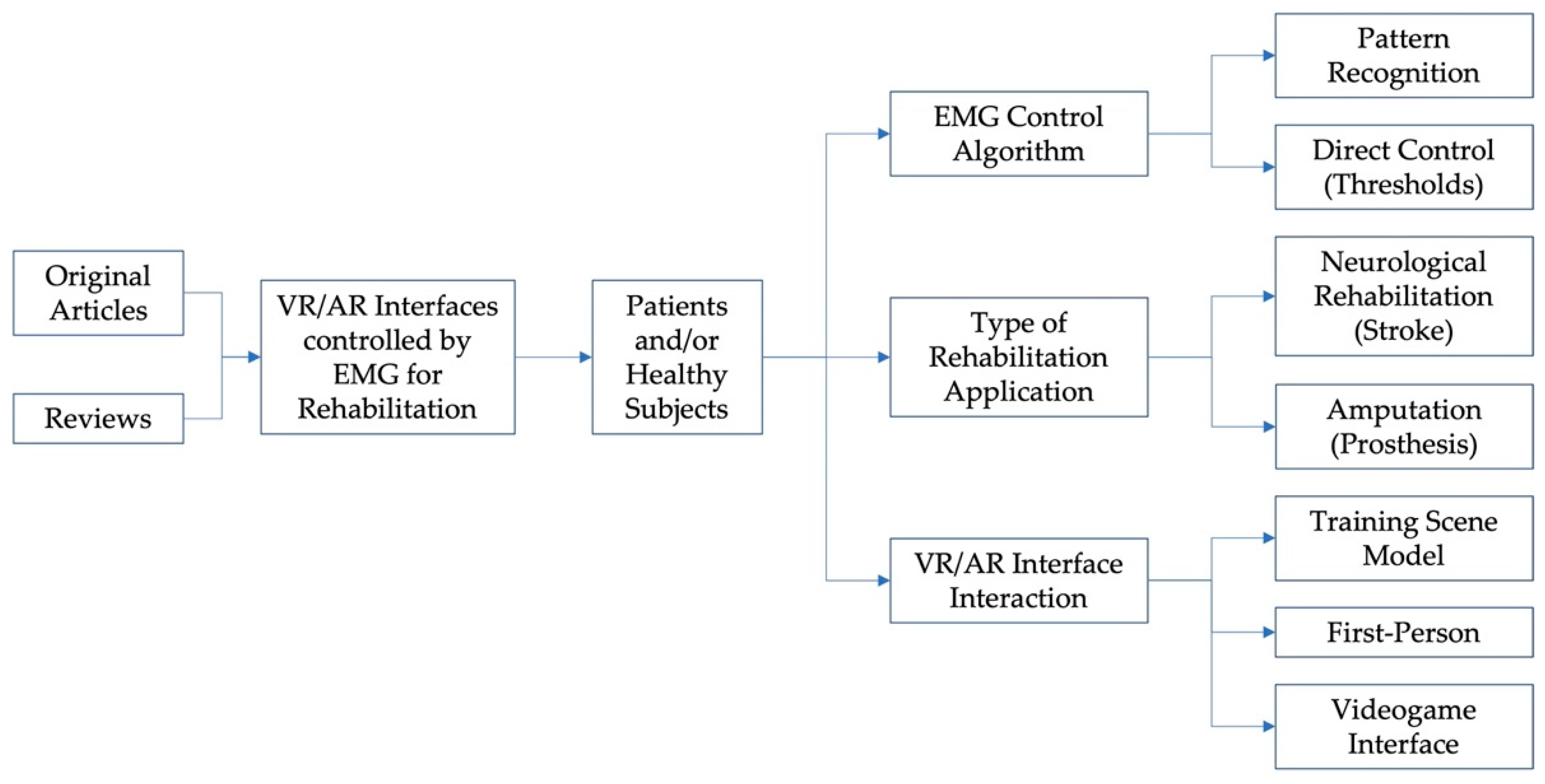
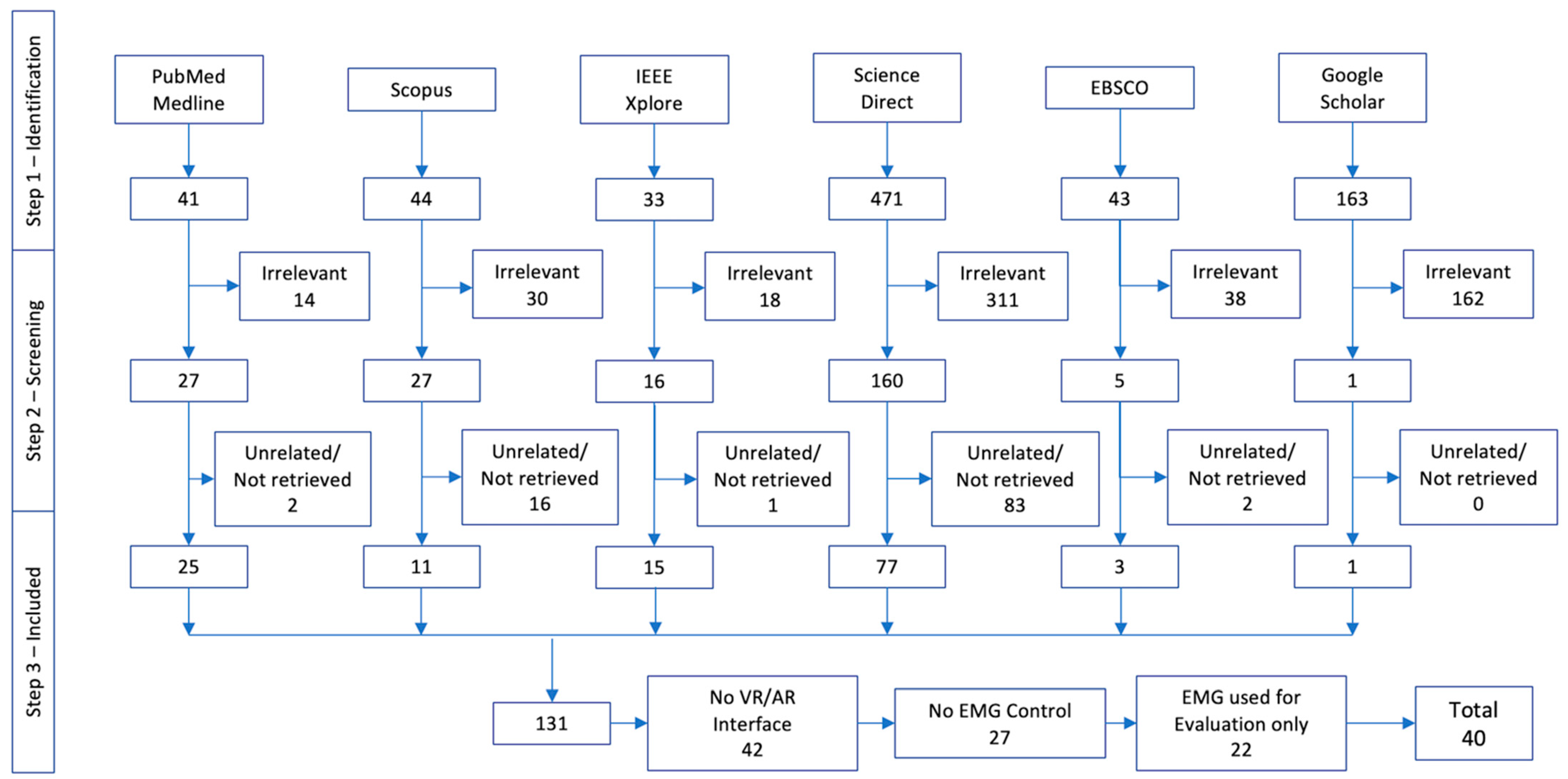
2. Materials and Methods
- RQ1:
- What is the share in the use of VR and AR interfaces in rehabilitation?
- RQ2:
- Which is the target anatomical region aimed to be rehabilitated?
- RQ3:
- What type of rehabilitation therapy is the interface used for?
- RQ4:
- What are the characteristics of VR/AR interfaces when used for rehabilitation?
- RQ5:
- How are sEMG signals used to interact with VR/AR interfaces for rehabilitation?
- RQ6:
- What hardware is used for signal acquisition?
3. Results
3.1. RQ1: What Is the Share in the Use of VR and AR Interfaces in Rehabilitation?
3.2. RQ2: Which Is the Target Anatomical Region Aimed to Be Rehabilitated?
3.3. RQ3: What Type of Rehabilitation Therapy Is the Interface Used for?
3.4. RQ4: What Are the Characteristics of VR/AR Interfaces When Used for Rehabilitation?
3.5. RQ5: How Are sEMG Signals Used to Interact with VR/AR Interfaces for Rehabilitation?
3.6. RQ6: What Hardware Is Used for Signal Acquisition?

{kind=link}
{kind=link}
{kind=link}
| First Author, Year | Type of Rehabilitation | Type of Interface | Interaction | Subjects | Anatomical Region | Acquisition Hardware | Feature Extraction | Classification Algorithm and Performance | Feedback | |
|---|---|---|---|---|---|---|---|---|---|---|
| Healthy Subject | Patient | |||||||||
| Mazzola, S., 2020 [73] | Neurological Motor Rehabilitation | VR 3D Upper Limbs Precision-based block staking task | Comparison of sEMG signals by means of RMS Voltage | 24 | - | Upper limb/ flexor carpi radialis, extensor digitorum, biceps brachii, triceps brachii bilateral | Vive Pro HMDLeap Motion Delsys Trigno wireless Electrodes 4-channels | RMS from sEMG + | Compare RMS + level from sEMG Signal (with and without the VR Interface) | Visual feedback |
| Lydakis, A., 2017 [69] | Neurological Motor Rehabilitation | VR Videogame Interface Movement Imitation | 3D Avatar (1) Assessment experiment (2) Action observation (3) Combined motor imagery and action observation | - | 4 post-stroke | Upper limb/ Musculi flexor pollicis longus, flexor digitorum superficialis and flexor carpi radialis | Myo Armband+ R7 AR Glasses + IMU g.Hlamp | RMS from sEMG + | Thresholds | Visual feedback |
| Woodward, R.B., 2019 [67] | Prosthesis Training | VR Virtual forest virtual crossbow in real-time | sEMG control of real-time hand grasps | 16 | 4 amputees (3 transradial, 1 wrist dislocation) | Upper limb/ Forearm Hand gestures (no motion, hand open, hand close, wrist pronation, wrist supination, wrist flexion, and wrist extension) | Custom-fabricated sEMG acquisition armbands included six pairs of stainless-steel dome electrodes TI ADS1299 bioinstrumentation chip | Movement velocity (advanced proportional control algorithm) Speed (smoothed) MRV, WVL, ZC SSC, and ARF from sEMG + | Pattern recognition 3D Target Achievement Control Test LDA *** | Visual feedback |
| Summa, S., 2019 [74] | Neurological Motor Rehabilitation | VR Robotic platform (Dynamic Oriented Rehabilitative Integrated System–DORIS) + motion analysis + sEMG | Training of equilibrium and gait Game experiences for VR | - | - | Lower limb Core Equilibrium and gait | Unreal VR Headset + Leap Motion + Vicon/sEMG Server – DORIS | - | - | Visual feedback |
| Kluger, D.T., 2019 [6] | Prosthesis Training | VR Virtual Modular Prosthetic Limb | Closed-loop virtual task | - | 2 amputees (transradial) | 19 contact sensors at the hand | MAV + from sEMG | Modified Kalman-filter-based decode | Visual feedback | |
| Meng, Q., 2019 [9] | Neurological Motor Rehabilitation | VR Rehabilitation Game | Virtual rehabilitation game | 8 | - | Upper limb/ Wrist flexion– extension | Property Design | Moving average window Autoregressive model (AR)parameter model in time domain | SVM *** Recognition of action 96.3% | Visual feedback |
| Nissler, C., 2019 [68] | Prosthesis Training | VR Environment Serious Games (Unity) | Box and Block Test At virtual living room and kitchen | 15 | 1 amputee (uses prosthesis) | Upper limb | Myo Armband | - | Intent detection | Visual feedback |
| Covaciu, F., 2021 [81] | Neurological Motor Rehabilitation | VR Collect Apples | Foot movements | 10 | - | Lower limb/ Ankle | Gyroscope Accelerometer Myoware | - | KNN *** 5-fold cross-validation 81.35% | Visual/functional feedback |
| Llorens, R., 2021 [53] | Neurological Motor Rehabilitation | VR Pick up Apples that grow before they disappeared | Intention of action while administering transcranial direct current stimulation | - | 29 | Upper limb/ brachioradialis, palmaris longus, and flexors and extensors of the fingers | Myo Armband | - | Intention of action while administering transcranial direct current stimulation | Audiovisual and tactile feedback |
| Li, K., 2019 [29] | Neurological Motor Rehabilitation | VR Environment Virtual Hand | Control with sEMG Electrotactile stimulation module Force proportional to intensity | 10 | - | Upper limb | Multichannel sEMG Acquisition System Elonxi Ltd. | sEMG intensity | - | Visual Feedback: Numerical indicators of force and deformation ElectrotactileStimulation Closed-loop |
| Cardoso, V.F., 2019 [75] | Neurological Motor Rehabilitation | VR Immersive Serious Game | EEG sEMG Robotic Monocycle | 8 (5 males) | - | Lower limb | Property sEMG acquisition 4-channels | - | - | Visual feedback |
| Li, X., 2019 [55] | Neurological Motor Rehabilitation | VR Kitchen Scene (open door, clean table, ventilator, cut food) | Control with sEMG | 4 | - | Upper limb | Wireless acquisition module | MAV, RMS, SD from sEMG + MAV, singular values of wavelet coefficients | SVM, PNN *** 95% for wavelet coefficients | Visual feedback |
| Bank, P., 2017 [78] | Neurological Motor Rehabilitation | VR Imitation Game | Control with sEMG | 18 | - | Upper limb/ wrist flexor carpi radialis and extensor carpi radialis | Porti7 22 bits A/D fs = 2000 Hz | MVC from sEMG + | Task Performance 96.6% Effort 100% Co-contraction 99.8% | Visuomotor tracking |
| Ruiz-Olaya, A.F., 2019 [58] | Neurological Motor Rehabilitation | VR Environments and/or Headsets | Control left/right position of virtual car High-density surface sEMG EEG | - | - | Upper limb, lower limb, full body Exoskeletons | Several | - | . | Visual feedback Haptic Exoskeleton |
| Castellini, C., 2020 [82] | Neurological Motor Rehabilitation | VR/AR Avatar Upper Limb Interaction | Control with sEMG | - | - | Upper limb | - | MVC from sEMG + | ML *** Pattern Recognition | Visual feedback (Positive psychological effects) |
| Raz, G., 2020 [71] | Neurological Motor Rehabilitation | VR Environment | Headset Sit in real table Arms represented in virtual world | - | - | Upper limb | - | - | - | Visual feedback |
| Bhagat, N.A., 2020 [56] | Neurological Motor Rehabilitation | VR Outreach task | BMI detects motion intention from sEMG and EEG motor intent to trigger exoskeleton for assistance | - | 10 chronic post-stroke | Upper limb/ biceps brachii, triceps brachii | Proprietary sEMG | RMS from sEMG + | sEMG threshold + EEG motor intent | Think of movement Visual feedback |
| Heerschop, A., 2020 [83] | Prosthesis Training | VR Serious Games:Control a grabber, free catching task, following task | Control from sEMG | 43 | - | Upper limb/ flexor-extensor of wrist | Otto Bock 13E200 Electrodes 2-channels | - | - | Visual feedback |
| Liew, S.L., 2022 [59] | Neurological Motor Rehabilitation | VR Serious Games | Control from sEMG to trigger FES * | - | - | Upper limb/ lower limb | Several | - | - | Visual feedback FES * activation |
| Ida, H., 2022 [84] | Neurological Motor Rehabilitation | VR Videogame | Postural adjustment after perturbation (rReal vs VR) Single-leg obstacle avoidance task | 10 | - | Lower limb | Myopac RUN | Mean + SD from sEMG + | - | Visual feedback |
| Montoya-Vega, M.F., 2019 [52] | Prosthesis Training | VR Serious Games Force Defense | Change difficulty of videogame depending on fatigue | 12 | - | Upper limb/ biceps brachii | Myo Armband | Fatigue | Motor Learning | Muscle fatigue as feedback |
| Mazzola, S., 2020 [73] | Neurological Motor Rehabilitation | VR Gesture-level hand tracking | Stack blocks using dominant hand | 24 | - | Upper limb/ flexor carpi radialis, extensor digitorum, biceps brachii and triceps brachii Bilateral | Delsys Trigno wireless electrodes | Amplitude RMS from sEMG + Completion Task Time | - | Visual feedback |
| Kisiel-Sajewicz, K., 2020 [72] | Neurological Motor Rehabilitation | VR Headset Virtual Upper Extremity | Reaching task precision fine grasping | 1 | 1 | Upper limb | OTbioLab ELSCHO064LS | MVC, Sub-MVC (20% MVC) from sEMG + | - | Visual feedback |
| First Author, Year | Type of Rehabilitation | Type of Interface | Interaction | Subjects | Anatomical Region | Acquisition Hardware | Feature Extraction | Classification Algorithm and Performance | Feedback | |
|---|---|---|---|---|---|---|---|---|---|---|
| Healthy Subject | Patient | |||||||||
| Wang, L., 2017 [51] | Neurological Motor Rehabilitation | VR Videogame Interface | Training scene model | 4 | 4 post-stroke | Upper limb/ hand gestures | eego™sports, Delsys | SE, MPF from sEMG + | SVM *** to identify action patterns – 99.5% healthy subjects (4) 94.75% stroke patients (4) | EEG and sEMGfatigue status to adapt level of difficulty |
| Lai, J., 2017 [79] | Prosthesis Training | VR Real-time interaction | Visual feedback real time response of sEMG control | 1 | - | Upper Limb/ Forearm | Danyang Prosthetic Electrodes 4-channel and UBS6351 NI | ×5 20 repetitions trials | SVM *** Training and pattern recognition | Visual feedback |
| Dash, A., 2019 [47] | Neurological Motor Rehabilitation | VR Videogame Interface Basketball tower, 3 goal posts | sEMG biofeedback for strength inference and EDA for tonic mean | 6 | 6 post-stroke hemiplegic | Upper limb/ flexor carpi radialis and extensor carpi radialis longus | Biopac MP150 fs = 1000 Hz | MAV from sEMG + | Levels of strength | Audio-visual feedback |
| Trifonov, A.A., 2020 [57] | Prosthesis Training | VR Movement Imitation | Replicates movements in VR, sEMG used as input of an exoskeleton that places the limb at given coordinates | 1 | - | Upper limb | Proprietary AD8232 2-channels – Exoskeleton | RMS, MAV from sEMG + | ANN *** (Two layers: Kohonen and Grossberg) | Visual feedback |
| Nasri, N. 2020 [64] | Neurological Motor Rehabilitation | VR (Unity) Serious Games | sEMG control | - | 4 | Upper limb/ hand gestures | Myo Armband | - | DL Model Conv-GRU architecture | Visual feedback |
| Dash, A., 2020 [42] | Neurological Motor Rehabilitation | VR (Unity) Fountains, Basketball court | sEMG control triggered grip exercise (move VR objects according to hand gesture) | 8 | 12 post-stroke | Upper limb | Biopac MP150 | MAV + from sEMG sEMG-controlled dynamic positioning of VR object | - | Visual feedback |
| Lukyanenko, P., 2021 [70] | Prosthesis Training | VR Representation of a prosthetic hand | Activate virtual hand using EMG | - | 2 | Upper limb | Chronically implanted EMG (ciEMG) electrodes Ripple Grapevine system collected ciEMG fs = 2000 Hz 15–350 Hz filter | MAV + from EMG | KNN mapping technique | Visual feedback |
| Hashim, N., 2021 [43] | Neurological Motor Rehabilitation | VR Videogames Crate Whacker, Race the Sun, Fruit Ninja, andKaiju Carnage | 1-h sessions 4-week rehabilitation program Box and Block Test sEMG Assessment | 5 | 5 amputees Transradial | Upper limb/ forearm | Myo Armband | MVC + from sEMG to randomly select a game | - | Visual feedback Timer and score visible |
| Quinayás, C., 2019 [65] | Prosthesis Training | VR Environment to locate & grasp object (Unity) | Hand grasps: rest, open hand, power, and precision grip 20 trials | - | 1 | Upper limb/ forearm | Property sEMG Bracelet fs = 1000 Hz | ASS, MSR from sEMG + | Online recognition of motion intention 86.6% | Visual feedback |
| Yassin, M.M., 2021 [85] | Neurological Motor Rehabilitation | VR Cellphone Apps (Patient + therapist) Car game (gauge & bar) | Control from sEMG | 5 | - | Upper limb | Property sEMG microcontroller—based on ARM Cortex 32- bit M3 architecture | RMS+ from sEMG | - | Visual feedback (gauge and bar) |
| Ma, L., 2018 [66] | Neurological Motor Rehabilitation | VR Videogame Interface (Hamster, Flappy Bird) | Picture guidance Gesture recognition of hand movement generates game character movement | 6 validation only | 9 post-stroke (pre-, mid-, post-rehab) (5–right hemiplegia) | Upper limb/ hand grasps (relax, open hand, close hand) | Delsys 4-channels, dry electrode, fs = 2000 Hz | SSC, ZC, RMS, WL, MDF, and MNF from sEMG + | ML *** 2-fold model fusion of Stacking – 95% in healthy subjects 90% 2 post-rehab patients’ hemiplegic side | Visual feedback |
| First Author, Year | Type of Rehabilitation | Type of Interface | Interaction | Subjects | Anatomical Region | Acquisition Hardware | Feature Extraction | Classification Algorithm and Performance | Feedback | |
|---|---|---|---|---|---|---|---|---|---|---|
| Melero, M., 2019 [60] | Prosthesis Training | AR Visualization of muscle activity Dance game Imitation | Score when movements are performed correctly Perform choreographed dance containing hand gestures involved in upper limb rehabilitation therapy | 3 | - | Upper limb/ hand gestures | Wired intramuscular sEMG recording implant 4-channels Myo Armband Microsoft Kinect | 10 trials | Myo Armband Software 77% Accuracy Hand Gesture Classification | Visual feedback |
| Gazzoni, M., 2021 [62] | Neurological Motor Rehabilitation | AR Superimposed muscles Smartglasses | Control from sEMG | 1 | - | Upper limb/ lower limb | Due 14-channels | RMS from sEMG + | Threshold sEMG | |
| Liu, L., 2020 [63] | Prosthesis Training | AR Imitation game | Exercise finger movements | 100 | - | Upper limb/ aand | Myo Armband | Spectogram | CNN * Pattern Recognition 10 gestures 97.8% | Visual feedback |
| Palermo, F., 2019 [61] | Prosthesis Training | AR Portable Environment | AR Environment renders a table, a hand and bottle, a screwdriver, tennis ball, pen, can Control with sEMG | 5 | 5 amputees Transradial | Upper limb | Microsoft HoloLens Myo Armband | - | Pattern recognition with Myo Software | Visual feedback |
4. Discussion
Future Directions
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Stucki, G. Advancing the Rehabilitation Sciences. Front. Rehabil. Sci. 2021, 1, 617749. [Google Scholar] [CrossRef]
- Reddy, N.P.; Unnikrishnan, R. EMG Interfaces for VR and Telematic Control Applications. IFAC Proc. Vol. 2001, 34, 443–446. [Google Scholar] [CrossRef]
- Mejia, J.A.; Hernandez, G.; Toledo, C.; Mercado, J.; Vera, A.; Leija, L.; Gutierrez, J. Upper Limb Rehabilitation Therapies Based in Videogames Technology Review. In Proceedings of the 2019 Global Medical Engineering Physics Exchanges/Pan American Health Care Exchanges (GMEPE/PAHCE) 2019, Buenos Aires, Argentina, 26–31 March 2019; pp. 1–5. [Google Scholar]
- González-González, C.S.; Toledo-Delgado, P.A.; Muñoz-Cruz, V.; Torres-Carrion, P.V. Serious games for rehabilitation: Gestural interaction in personalized gamified exercises through a recommender system. J. Biomed. Inform. 2019, 97, 103266. [Google Scholar] [CrossRef] [PubMed]
- Cerritelli, F.; Chiera, M.; Abbro, M.; Megale, V.; Esteves, J.; Gallace, A.; Manzotti, A. The Challenges and Perspectives of the Integration Between Virtual and Augmented Reality and Manual Therapies. Front. Neurol. 2021, 12, 700211. [Google Scholar] [CrossRef] [PubMed]
- Kluger, D.T.; Joyner, J.S.; Wendelken, S.M.; Davis, T.S.; George, J.A.; Page, D.M.; Hutchinson, D.T.; Benz, H.L.; Clark, G.A. Virtual Reality Provides an Effective Platform for Functional Evaluations of Closed-Loop Neuromyoelectric Control. IEEE Trans. Neural Syst. Rehabil. Eng. 2019, 27, 876–886. [Google Scholar] [CrossRef]
- Huang, J.; Lin, M.; Fu, J.; Sun, Y.; Fang, Q. An Immersive Motor Imagery Training System for Post-Stroke Rehabilitation Combining VR and EMG-based Real-Time Feedback. In Proceedings of the 2021 43rd Annual International Conference of the IEEE Engineering in Medicine & Biology Society (EMBC), Guadalajara, Mexico, 1–5 November 2021; pp. 7590–7593. [Google Scholar]
- Muri, F.; Carbajal, C.; Echenique, A.M.; Fernández, H.; López, N.M. Virtual reality upper limb model controlled by EMG signals. J. Phys. Conf. Ser. 2013, 477, 012041. [Google Scholar] [CrossRef]
- Meng, Q.; Zhang, J.; Yang, X. Virtual Rehabilitation Training System Based on Surface EMG Feature Extraction and Analysis. J. Med. Syst. 2019, 43, 48. [Google Scholar] [CrossRef] [PubMed]
- Montoya, M.F.; Munoz, J.E.; Henao, O.A. Enhancing Virtual Rehabilitation in Upper Limbs With Biocybernetic Adaptation: The Effects of Virtual Reality on Perceived Muscle Fatigue, Game Performance and User Experience. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 740–747. [Google Scholar] [CrossRef]
- Thériault, L.; Robert, J.-M.; Baron, L. Virtual Reality Interfaces for Virtual Environments. Virtual Reality International Conference. Available online: https://www.researchgate.net/publication/259576863 (accessed on 20 April 2022).
- Liang, Y.; Wu, D.; Ledesma, D.; Davis, C.; Slaughter, R.; Guo, Z. Virtual Tai-Chi System: A smart-connected modality for rehabilitation. Smart Health 2018, 9–10, 232–249. [Google Scholar] [CrossRef]
- Chen, P.-J.; Penn, I.-W.; Wei, S.-H.; Chuang, L.-R.; Sung, W.-H. Augmented reality-assisted training with selected Tai-Chi movements improves balance control and increases lower limb muscle strength in older adults: A prospective randomized trial. J. Exerc. Sci. Fit. 2020, 18, 142–147. [Google Scholar] [CrossRef]
- Muñoz, J.E.; Montoya, M.F.; Boger, J. From Exergames to Immersive Virtual Reality Systems: Serious Games for Supporting Older Adults, 1st ed.; Elsevier Inc.: Amsterdam, The Netherlands, 2021; pp. 141–204. [Google Scholar]
- Barrett, A.M.; Oh-Park, M.; Chen, P.; Ifejika, N.L. Neurorehabilitation: Five new things. Neurol. Clin. Pract. 2013, 3, 484–492. [Google Scholar] [CrossRef] [Green Version]
- Giggins, O.M.; Persson, U.M.; Caulfield, B. Biofeedback in rehabilitation. J. Neuroeng. Rehabil. 2013, 10, 60. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dosen, S.; Markovic, M.; Somer, K.; Graimann, B.; Farina, D. EMG Biofeedback for online predictive control of grasping force in a myoelectric prosthesis. J. Neuroeng. Rehabil. 2015, 12, 55. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ogourtsova, T.; Archambault, P.S.; Lamontagne, A. Let’s do groceries-a novel virtual assessment for post-stroke unilateral spatial neglect Effects of virtual scene complexity and knowledge translation initiatives. In Proceedings of the 2017 International Conference on Virtual Rehabilitation (Icvr), Montreal, QC, Canada, 19–22 June 2017. [Google Scholar]
- Tao, G.; Archambault, P.S.; Levin, M.F. Evaluation of Kinect skeletal tracking in a virtual reality rehabilitation system for upper limb hemiparesis. In Proceedings of the 2013 International Conference on Virtual Rehabilitation, ICVR 2013, Philadelphia, PA, USA, 26–29 August 2013; pp. 164–165. [Google Scholar]
- Wada, T.; Takeuchi, T. A Training System for EMG Prosthetic Hand in Virtual Environment. In Proceedings of the Human Factors and Ergonomics Society Annual Meeting, New York, NY, USA, 22–26 September 2008; Volume 52, pp. 2112–2116. [Google Scholar]
- Sime, D.W. Potential Application of Virtual Reality for Interface Customisation (and Pre-training) of Amputee Patients as Preparation for Prosthetic Use. Adv. Exp. Med. Biol. 2019, 1120, 15–24. [Google Scholar] [CrossRef] [PubMed]
- Clemente, F.; D’Alonzo, M.; Controzzi, M.; Edin, B.B.; Cipriani, C. Non-Invasive, Temporally Discrete Feedback of Object Contact and Release Improves Grasp Control of Closed-Loop Myoelectric Transradial Prostheses. IEEE Trans. Neural Syst. Rehabil. Eng. 2016, 24, 1314–1322. [Google Scholar] [CrossRef] [PubMed]
- Markovic, M.; Schweisfurth, M.A.; Engels, L.F.; Bentz, T.; Wüstefeld, D.; Farina, D.; Dosen, S. The clinical relevance of advanced artificial feedback in the control of a multi-functional myoelectric prosthesis. J. Neuroeng. Rehabil. 2018, 15, 28. [Google Scholar] [CrossRef] [Green Version]
- Thomas, G.P.; Jobst, B.C. Feedback-Sensitive and Closed-Loop Solutions; Elsevier Inc.: Amsterdam, The Netherlands, 2017. [Google Scholar]
- Svensson, P.; Wijk, U.; Björkman, A.; Antfolk, C. A review of invasive and non-invasive sensory feedback in upper limb prostheses. Expert Rev. Med. Devices 2017, 14, 439–447. [Google Scholar] [CrossRef]
- Earnshaw, R.; Liggett, S.; Excell, P.; Thalmann, D. Technology, Design and the Arts-Opportunities and Challenges; Springer International Publishing: Cham, Switzerland, 2020. [Google Scholar]
- Casellato, C.; Ambrosini, E.; Galbiati, A.; Biffi, E.; Cesareo, A.; Beretta, E.; Lunardini, F.; Zorzi, G.; Sanger, T.D.; Pedrocchi, A. EMG-based vibro-tactile biofeedback training: Effective learning accelerator for children and adolescents with dystonia? A pilot crossover trial. J. Neuroeng. Rehabil. 2019, 16, 150. [Google Scholar] [CrossRef] [PubMed]
- Gutiérrez, Á.; Sepúlveda-Muñoz, D.; Gil-Agudo, Á.; de los Reyes Guzman, A. Serious Game Platform with Haptic Feedback and EMG Monitoring for Upper Limb Rehabilitation and Smoothness Quantification on Spinal Cord Injury Patients. Appl. Sci. 2020, 10, 963. [Google Scholar] [CrossRef] [Green Version]
- Li, K.; Boyd, P.; Zhou, Y.; Ju, Z.; Liu, H. Electrotactile Feedback in a Virtual Hand Rehabilitation Platform: Evaluation and Implementation. IEEE Trans. Autom. Sci. Eng. 2019, 16, 1556–1565. [Google Scholar] [CrossRef] [Green Version]
- Markovic, M.; Varel, M.; Schweisfurth, M.A.; Schilling, A.F.; Dosen, S. Closed-Loop Multi-Amplitude Control for Robust and Dexterous Performance of Myoelectric Prosthesis. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 498–507. [Google Scholar] [CrossRef] [PubMed]
- Parker, P.; Englehart, K.; Hudgins, B. Myoelectric signal processing for control of powered limb prostheses. J. Electromyogr. Kinesiol. 2006, 16, 541–548. [Google Scholar] [CrossRef] [PubMed]
- Youn, W.; Kim, J. Development of a compact-size and wireless surface EMG measurement system. In Proceedings of the ICCAS-SICE 2009-ICROS-SICE International Joint Conference 2009, Fukuoka, Japan, 18–21 August 2009; pp. 1625–1628. [Google Scholar]
- Lowery, M.; Weir, R.; Kuiken, T. Simulation of Intramuscular EMG Signals Detected Using Implantable Myoelectric Sensors (IMES). IEEE Trans. Biomed. Eng. 2006, 53, 1926–1933. [Google Scholar] [CrossRef] [PubMed]
- Reategui, J.; Callupe, R. Surface EMG multichannel array using active dry sensors for forearm signal extraction. In Proceedings of the 2017 IEEE 24th International Congress on Electronics, Electrical Engineering and Computing, INTERCON 2017, Cusco, Peru, 15–18 August 2017; pp. 1–4. [Google Scholar]
- Drost, G.; Stegeman, D.F.; van Engelen, B.G.; Zwarts, M.J. Clinical applications of high-density surface EMG: A systematic review. J. Electromyogr. Kinesiol. 2006, 16, 586–602. [Google Scholar] [CrossRef]
- Xie, L.; Yang, G.; Xu, L.; Seoane, F.; Chen, Q.; Zheng, L. Characterization of dry biopotential electrodes. In Proceedings of the 2013 35th Annual International Conference of the IEEE Engineering in Medicine and Biology Society (EMBC), Osaka, Japan, 3–7 July 2013; pp. 1478–1481. [Google Scholar]
- Roche, A.D.; Rehbaum, H.; Farina, D.; Aszmann, O.C. Prosthetic Myoelectric Control Strategies: A Clinical Perspective. Curr. Surg. Rep. 2014, 2, 44. [Google Scholar] [CrossRef]
- Cordella, F.; Ciancio, A.L.; Sacchetti, R.; Davalli, A.; Cutti, A.G.; Guglielmelli, E.; Zollo, L. Literature Review on Needs of Upper Limb Prosthesis Users. Front. Neurosci. 2016, 10, 209. [Google Scholar] [CrossRef]
- Pallavicini, F.; Ferrari, A.; Mantovani, F. Video Games for Well-Being: A Systematic Review on the Application of Computer Games for Cognitive and Emotional Training in the Adult Population. Front. Psychol. 2018, 9, 2127. [Google Scholar] [CrossRef] [Green Version]
- Reilly, C.A.; Greeley, A.B.; Jevsevar, D.S.; Gitajn, I.L. Virtual reality-based physical therapy for patients with lower extremity injuries: Feasibility and acceptability. OTA Int. Open Access J. Orthop. Trauma 2021, 4, e132. [Google Scholar] [CrossRef]
- Gil, M.J.V.; Gonzalez-Medina, G.; Lucena-Anton, D.; Perez-Cabezas, V.; Ruiz-Molinero, M.D.C.; Martín-Valero, R. Augmented Reality in Physical Therapy: Systematic Review and Meta-analysis. JMIR Serious Games 2021, 9, e30985. [Google Scholar] [CrossRef]
- Dash, A.; Lahiri, U. Design of Virtual Reality-Enabled Surface Electromyogram-Triggered Grip Exercise Platform. IEEE Trans. Neural Syst. Rehabil. Eng. 2020, 28, 444–452. [Google Scholar] [CrossRef]
- Hashim, N.A.; Razak, N.A.A.; Gholizadeh, H.; Osman, N.A.A. Video Game–Based Rehabilitation Approach for Individuals Who Have Undergone Upper Limb Amputation: Case-Control Study. JMIR Serious Games 2021, 9, e17017. [Google Scholar] [CrossRef] [PubMed]
- Seo, N.J.; Barry, A.; Ghassemi, M.; Triandafilou, K.M.; Stoykov, M.E.; Vidakovic, L.; Roth, E.; Kamper, D.G. Use of an EMG-Controlled Game as a Therapeutic Tool to Retrain Hand Muscle Activation Patterns Following Stroke: A Pilot Study. J. Neurol. Phys. Ther. 2022, 46, 198–205. [Google Scholar] [CrossRef] [PubMed]
- Pereira, M.F.; Prahm, C.; Kolbenschlag, J.; Oliveira, E.; Rodrigues, N.F. Application of AR and VR in hand rehabilitation: A systematic review. J. Biomed. Inform. 2020, 111, 103584. [Google Scholar] [CrossRef] [PubMed]
- Merians, A.S.; Jack, D.; Boian, R.; Tremaine, M.; Burdea, G.C.; Adamovich, S.V.; Recce, M.; Poizner, H. Virtual Reality–Augmented Rehabilitation for Patients Following Stroke. Phys. Ther. 2002, 82, 898–915. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dash, A.; Yadav, A.; Lahiri, U. Physiology-sensitive Virtual Reality based Strength Training Platform for Post-stroke Grip Task. In Proceedings of the 2019 IEEE EMBS International Conference on Biomedical & Health Informatics (BHI), Chicago, IL, USA, 19–22 May 2019; pp. 1–4. [Google Scholar]
- Peng, L.; Hou, Z.G.; Peng, L.; Luo, L.; Wang, W. Robot assisted upper limb rehabilitation training and clinical evaluation: Results of a pilot study. In Proceedings of the 2017 IEEE International Conference on Robotics and Biomimetics, ROBIO 2017, Macau, Macao, 5–8 December 2017; pp. 1–6. [Google Scholar]
- Wei, X.; Chen, Y.; Jia, X.; Chen, Y.; Xie, L. Muscle Activation Visualization System Using Adaptive Assessment and Forces-EMG Mapping. IEEE Access 2021, 9, 46374–46385. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Wang, L.; Du, S.; Liu, H.; Yu, J.; Cheng, S.; Xie, P. A virtual rehabilitation system based on EEG-EMG feedback control. In Proceedings of the 2017 Chinese Automation Congress (CAC), Jinan, China, 20–22 October 2017; pp. 4337–4340. [Google Scholar]
- Vega, M.F.M.; Henao, O.A. Cross-validation of a classification method applied in a database of sEMG contractions collected in a body interaction videogame. J. Phys. Conf. Ser. 2019, 1247, 012049. [Google Scholar] [CrossRef]
- Llorens, R.; Fuentes, M.A.; Borrego, A.; Latorre, J.; Alcañiz, M.; Colomer, C.; Noé, E. Effectiveness of a combined transcranial direct current stimulation and virtual reality-based intervention on upper limb function in chronic individuals post-stroke with persistent severe hemiparesis: A randomized controlled trial. J. Neuroeng. Rehabil. 2021, 18, 108. [Google Scholar] [CrossRef]
- Li, Y.; Chen, J.; Yang, Y. A Method for Suppressing Electrical Stimulation Artifacts from Electromyography. Int. J. Neural Syst. 2019, 29, 1850054. [Google Scholar] [CrossRef]
- Li, X.; Zhou, Z.; Liu, W.; Ji, M. Wireless sEMG-based identification in a virtual reality environment. Microelectron. Reliab. 2019, 98, 78–85. [Google Scholar] [CrossRef]
- Bhagat, N.A.; Yozbatiran, N.; Sullivan, J.L.; Paranjape, R.; Losey, C.; Hernandez, Z.; Keser, Z.; Grossman, R.; Francisco, G.E.; O’Malley, M.K.; et al. Neural activity modulations and motor recovery following brain-exoskeleton interface mediated stroke rehabilitation. Neuroimage Clin. 2020, 28, 102502. [Google Scholar] [CrossRef] [PubMed]
- Trifonov, A.A.; Kuzmin, A.A.; Filist, S.A.; Degtyarev, S.v.; Petrunina, E.v. Biotechnical System for Control to the Exoskeleton Limb Based on Surface Myosignals for Rehabilitation Complexes. In Proceedings of the 2020 IEEE 14th International Conference on Application of Information and Communication Technologies (AICT), Tashkent, Uzbekistan, 7–9 October 2020. [Google Scholar]
- Ruiz-Olaya, A.F.; Lopez-Delis, A.; da Rocha, A.F. Upper and lower extremity exoskeletons. In Handbook of Biomechatronics; Elsevier: Amsterdam, The Netherlands; pp. 283–317.
- Liew, S.-L.; Lin, D.J.; Cramer, S.C. Interventions to Improve Recovery After Stroke, 7th ed; Elsevier Inc.: Amsterdam, The Netherlands, 2022. [Google Scholar]
- Melero, M.; Hou, A.; Cheng, E.; Tayade, A.; Lee, S.C.; Unberath, M.; Navab, N. Upbeat: Augmented Reality-Guided Dancing for Prosthetic Rehabilitation of Upper Limb Amputees. J. Healthc. Eng. 2019, 2019, 2163705. [Google Scholar] [CrossRef] [Green Version]
- Palermo, F.; Cognolato, M.; Eggel, I.; Atzori, M.; Müller, H. An augmented reality environment to provide visual feedback to amputees during sEMG data acquisitions. In Lecture Notes in Computer Science (Including Subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer: Cham, Switzerland, 2019; Volume 11650, pp. 3–14. [Google Scholar]
- Gazzoni, M.; Cerone, G.L. Augmented Reality Biofeedback for Muscle Activation Monitoring: Proof of Concept. In IFMBE Proceedings; Springer: Cham, Switzerland, 2021; Volume 80, pp. 143–150. [Google Scholar]
- Liu, L.; Cui, J.; Niu, J.; Duan, N.; Yu, X.; Li, Q.; Yeh, S.-C.; Zheng, L.-R. Design of Mirror Therapy System Base on Multi-Channel Surface-Electromyography Signal Pattern Recognition and Mobile Augmented Reality. Electronics 2020, 9, 2142. [Google Scholar] [CrossRef]
- Nasri, N.; Orts-Escolano, S.; Cazorla, M. An sEMG-Controlled 3D Game for Rehabilitation Therapies: Real-Time Time Hand Gesture Recognition Using Deep Learning Techniques. Sensors 2020, 20, 6451. [Google Scholar] [CrossRef] [PubMed]
- Quinayás, C.; Barrera, F.; Ruiz, A.; Delis, A. Virtual Hand Training Platform Controlled Through Online Recognition of Motion Intention. In Lecture Notes in Computer Science (including subseries Lecture Notes in Artificial Intelligence and Lecture Notes in Bioinformatics); Springer: Cham, Switzerland, 2019; Volume 11896, pp. 761–768. [Google Scholar]
- Ma, L.; Zhao, X.; Li, Z.; Zhao, M.; Xu, Z. A sEMG-based Hand Function Rehabilitation System for Stroke Patients. In Proceedings of the 2018 3rd International Conference on Advanced Robotics and Mechatronics (ICARM), Singapore, 18–20 July 2018; pp. 497–502. [Google Scholar]
- Woodward, R.B.; Hargrove, L.J. Adapting myoelectric control in real-time using a virtual environment. J. Neuroeng. Rehabil. 2019, 16, 11. [Google Scholar] [CrossRef]
- Nissler, C.; Nowak, M.; Connan, M.; Büttner, S.; Vogel, J.; Kossyk, I.; Márton, Z.-C.; Castellini, C. VITA—an everyday virtual reality setup for prosthetics and upper-limb rehabilitation. J. Neural Eng. 2019, 16, 026039. [Google Scholar] [CrossRef] [Green Version]
- Lydakis, A.; Meng, Y.; Munroe, C.; Wu, Y.N.; Begum, M. A learning-based agent for home neurorehabilitation. In Proceedings of the IEEE International Conference on Rehabilitation Robotics, London, UK, 17–20 July 2017; pp. 1233–1238. [Google Scholar]
- Lukyanenko, P.; Dewald, H.A.; Lambrecht, J.; Kirsch, R.F.; Tyler, D.J.; Williams, M.R. Stable, simultaneous and proportional 4-DoF prosthetic hand control via synergy-inspired linear interpolation: A case series. J. Neuroeng. Rehabil. 2021, 18, 50. [Google Scholar] [CrossRef]
- Raz, G.; Gurevitch, G.; Vaknin, T.; Aazamy, A.; Gefen, I.; Grunstein, S.; Azouri, G.; Goldway, N. Electroencephalographic evidence for the involvement of mirror-neuron and error-monitoring related processes in virtual body ownership. NeuroImage 2020, 207, 116351. [Google Scholar] [CrossRef]
- Kisiel-Sajewicz, K.; Marusiak, J.; Rojas-Martínez, M.; Janecki, D.; Chomiak, S.; Mencel, J.; Mañanas, M.; Jaskólski, A.; Jaskólska, A. High-density surface electromyography maps after computer-aided training in individual with congenital transverse deficiency: A case study. BMC Musculoskelet. Disord. 2020, 21, 682. [Google Scholar] [CrossRef]
- Mazzola, S.; Prado, A.; Agrawal, S.K. An upper limb mirror therapy environment with hand tracking in virtual reality. In Proceedings of the 2020 8th IEEE RAS/EMBS International Conference for Biomedical Robotics and Biomechatronics (BioRob), New York, NY, USA, 29 November–1 December 2020; pp. 752–758. [Google Scholar]
- Summa, S.; Gori, R.; Castelli, E.; Petrarca, M. Development of a dynamic oriented rehabilitative integrated system. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, EMBS, Berlin, Germany, 23–27 July 2019; pp. 5245–5250. [Google Scholar]
- Cardoso, V.F.; Pomer-Escher, A.; Longo, B.B.; Loterio, F.A.; Nascimento, S.S.G.; Laiseca, M.A.R.; Delisle-Rodriguez, D.; Frizera-Neto, A.; Bastos-Filho, T. Neurorehabilitation platform based on EEG, sEMG and virtual reality using robotic monocycle. In IFMBE Proceedings; Springer: Singapore; Volume 70, pp. 315–321.
- Braza, D.W.; Martin, J.N.Y. Upper Limb Amputations. In Essentials of Physical Medicine and Rehabilitation: Musculoskeletal Disorders, Pain, and Rehabilitation; Elsevier: Amsterdam, The Netherlands; pp. 651–657.
- Alshehri, F.M.; Ahmed, S.A.; Ullah, S.; Ghazal, H.; Nawaz, S.; Alzahrani, A.S. The Patterns of Acquired Upper and Lower Extremity Amputation at a Tertiary Centre in Saudi Arabia. Cureus 2022, 14, 4. [Google Scholar] [CrossRef]
- Bank, P.J.; Dobbe, L.R.; Meskers, C.G.; De Groot, J.H.; De Vlugt, E. Manipulation of visual information affects control strategy during a visuomotor tracking task. Behav. Brain Res. 2017, 329, 205–214. [Google Scholar] [CrossRef]
- Lai, J.; Zhao, Y.; Liao, Y.; Hou, W.; Chen, Y.; Zhang, Y.; Li, G.; Wu, X. Design of a multi-degree-of-freedom virtual hand bench for myoelectrical prosthesis. In Proceedings of the 2017 2nd International Conference on Advanced Robotics and Mechatronics (ICARM), Hefei/Tai’an, China, 27–31 August 2017; pp. 345–350. [Google Scholar]
- Pizzolato, S.; Tagliapietra, L.; Cognolato, M.; Reggiani, M.; Müller, H.; Atzori, M. Comparison of six electromyography acquisition setups on hand movement classification tasks. PLoS ONE 2017, 12, e0186132. [Google Scholar] [CrossRef] [Green Version]
- Covaciu, F.; Pisla, A.; Iordan, A.-E. Development of a Virtual Reality Simulator for an Intelligent Robotic System Used in Ankle Rehabilitation. Sensors 2021, 21, 1537. [Google Scholar] [CrossRef] [PubMed]
- Castellini, C. Design Principles of a Light, Wearable Upper Limb Interface for Prosthetics and Teleoperation. In Wearable Robotics; Elsevier: Amsterdam, The Netherlands, 2020; pp. 377–391. [Google Scholar]
- Heerschop, A.; van der Sluis, C.K.; Otten, E.; Bongers, R.M. Performance among different types of myocontrolled tasks is not related. Hum. Mov. Sci. 2020, 70, 102592. [Google Scholar] [CrossRef] [PubMed]
- Ida, H.; Mohapatra, S.; Aruin, A.S. Perceptual distortion in virtual reality and its impact on dynamic postural control. Gait Posture 2021, 92, 123–128. [Google Scholar] [CrossRef] [PubMed]
- Yassin, M.M.; Saber, A.M.; Saad, M.N.; Said, A.M.; Khalifa, A.M. Developing a Low-cost, smart, handheld electromyography biofeedback system for telerehabilitation with Clinical Evaluation. Med. Nov. Technol. Devices 2021, 10, 100056. [Google Scholar] [CrossRef]
- Galido, E.; Esplanada, M.C.; Estacion, C.J.; Migriño, J.P.; Rapisora, J.K.; Salita, J.; Amado, T.; Jorda, R.; Tolentino, L.K. EMG Speed-Controlled Rehabilitation Treadmill With Physiological Data Acquisition System Using BITalino Kit. In Proceedings of the 2018 IEEE 10th International Conference on Humanoid, Nanotechnology, Information Technology, Communication and Control, Environment and Management (HNICEM), Baguio City, Philippines, 29 November–2 December 2018; pp. 1–5. [Google Scholar]
- Osumi, M.; Inomata, K.; Inoue, Y.; Otake, Y.; Morioka, S.; Sumitani, M. Characteristics of Phantom Limb Pain Alleviated with Virtual Reality Rehabilitation. In Pain Medicine; Oxford University Press: Oxford, UK, 2019; Volume 20, pp. 1038–1046. [Google Scholar]
- Sousa, M.; Vieira, J.; Medeiros, D.; Arsénio, A.; Jorge, J. SleeveAR: Augmented reality for rehabilitation using realtime feedback. In Proceedings of the International Conference on Intelligent User Interfaces, Proceedings IUI, Sonoma, CA, USA, 7–10 March 2016; pp. 175–185. [Google Scholar]
- Maier, M.; Ballester, B.R.; Verschure, P.F.M.J. Principles of Neurorehabilitation After Stroke Based on Motor Learning and Brain Plasticity Mechanisms. Front. Syst. Neurosci. 2019, 13, 74. [Google Scholar] [CrossRef]
- Quitadamo, L.R.; Cavrini, F.; Sbernini, L.; Riillo, F.; Bianchi, L.; Seri, S.; Saggio, G. Support vector machines to detect physiological patterns for EEG and EMG-based human–computer interaction: A review. J. Neural Eng. 2017, 14, 011001. [Google Scholar] [CrossRef]
- Brambilla, C.; Pirovano, I.; Mira, R.M.; Rizzo, G.; Scano, A.; Mastropietro, A. Combined Use of EMG and EEG Techniques for Neuromotor Assessment in Rehabilitative Applications: A Systematic Review. Sensors 2021, 21, 7014. [Google Scholar] [CrossRef]
- Marin-Pardo, O.; Laine, C.M.; Rennie, M.; Ito, K.L.; Finley, J.; Liew, S.-L. A Virtual Reality Muscle–Computer Interface for Neurorehabilitation in Chronic Stroke: A Pilot Study. Sensors 2020, 20, 3754. [Google Scholar] [CrossRef]
- Lou, X.; Xiao, S.; Qi, Y.; Hu, X.; Wang, Y.; Zheng, X. Corticomuscular Coherence Analysis on Hand Movement Distinction for Active Rehabilitation. Comput. Math. Methods Med. 2013, 2013, 908591. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, W.-S.; Cho, S.; Ku, J.; Kim, Y.; Lee, K.; Hwang, H.-J.; Paik, N.-J. Clinical Application of Virtual Reality for Upper Limb Motor Rehabilitation in Stroke: Review of Technologies and Clinical Evidence. J. Clin. Med. 2020, 9, 3369. [Google Scholar] [CrossRef] [PubMed]
- Hermens, H.J.; Freriks, B. Guidelines for reporting SEMG data. In The state of the Art on Sensors and Sensor Placement Procedures for Surface Electromyography: A Proposal for Sensor Placement Procedures; Roessingh Research and Development: Enschede, The Netherlands, 1997. [Google Scholar]
- Simon, A.M.; Hargrove, L.J.; Lock, B.A.; Kuiken, T.A.; Simon, A. The Target Achievement Control Test: Evaluating real-time myoelectric pattern recognition control of a multifunctional upper-limb prosthesis. J. Rehabil. Res. Dev. 2011, 48, 619. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Toledo-Peral, C.L.; Vega-Martínez, G.; Mercado-Gutiérrez, J.A.; Rodríguez-Reyes, G.; Vera-Hernández, A.; Leija-Salas, L.; Gutiérrez-Martínez, J. Virtual/Augmented Reality for Rehabilitation Applications Using Electromyography as Control/Biofeedback: Systematic Literature Review. Electronics 2022, 11, 2271. https://doi.org/10.3390/electronics11142271
Toledo-Peral CL, Vega-Martínez G, Mercado-Gutiérrez JA, Rodríguez-Reyes G, Vera-Hernández A, Leija-Salas L, Gutiérrez-Martínez J. Virtual/Augmented Reality for Rehabilitation Applications Using Electromyography as Control/Biofeedback: Systematic Literature Review. Electronics. 2022; 11(14):2271. https://doi.org/10.3390/electronics11142271
Chicago/Turabian StyleToledo-Peral, Cinthya Lourdes, Gabriel Vega-Martínez, Jorge Airy Mercado-Gutiérrez, Gerardo Rodríguez-Reyes, Arturo Vera-Hernández, Lorenzo Leija-Salas, and Josefina Gutiérrez-Martínez. 2022. "Virtual/Augmented Reality for Rehabilitation Applications Using Electromyography as Control/Biofeedback: Systematic Literature Review" Electronics 11, no. 14: 2271. https://doi.org/10.3390/electronics11142271
APA StyleToledo-Peral, C. L., Vega-Martínez, G., Mercado-Gutiérrez, J. A., Rodríguez-Reyes, G., Vera-Hernández, A., Leija-Salas, L., & Gutiérrez-Martínez, J. (2022). Virtual/Augmented Reality for Rehabilitation Applications Using Electromyography as Control/Biofeedback: Systematic Literature Review. Electronics, 11(14), 2271. https://doi.org/10.3390/electronics11142271