
A Decision-Support Informatics Platform for Minimally Invasive Aortic Valve Replacement


 , ,
, , 

Abstract
:1. Introduction
2. Materials and Methods
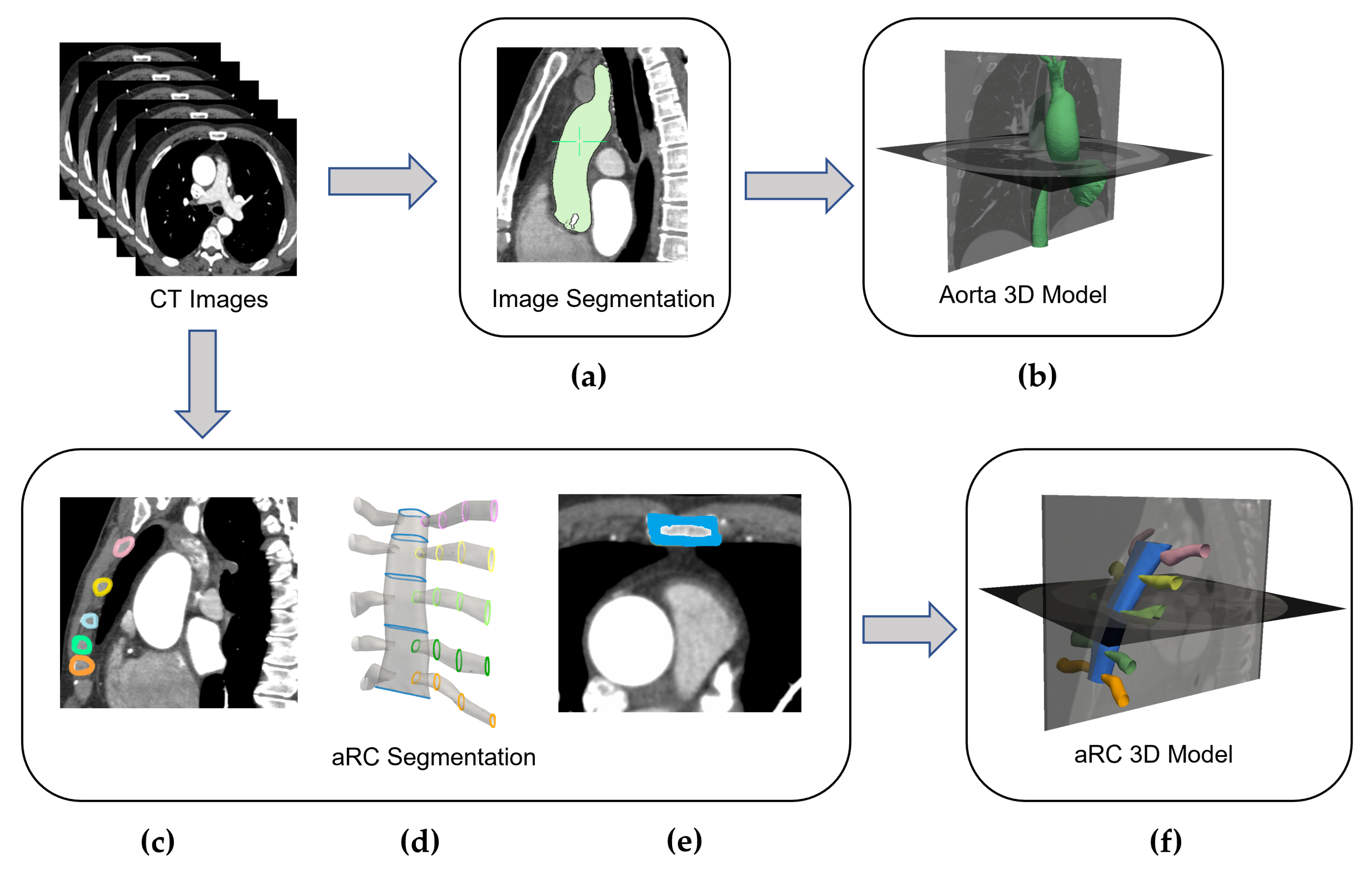
2.1. Image Analysis
2.2. Aorta and aRC 3D Models Reconstruction
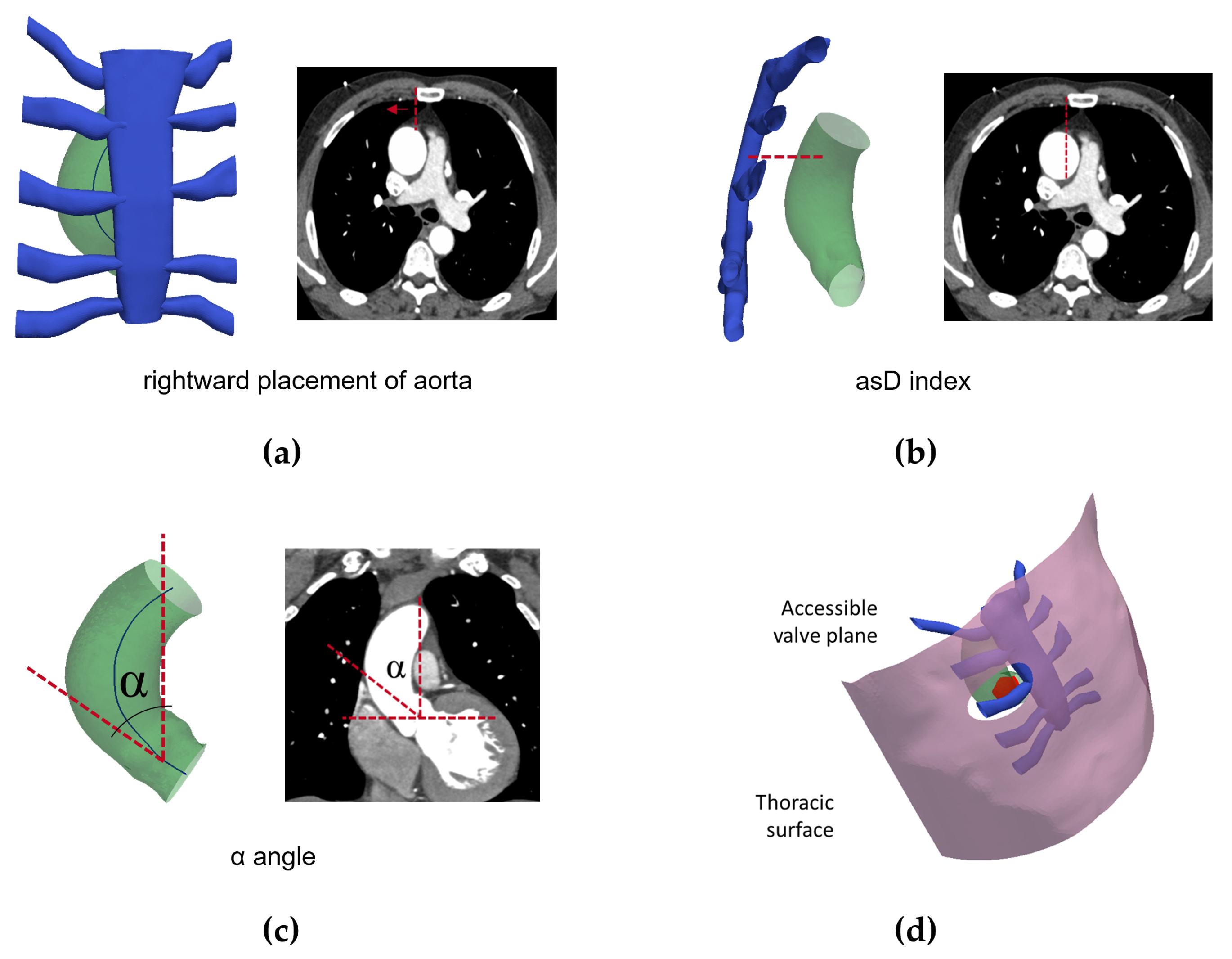
2.3. RT Inclusion Criteria Evaluation and Geometric Parameters Extraction
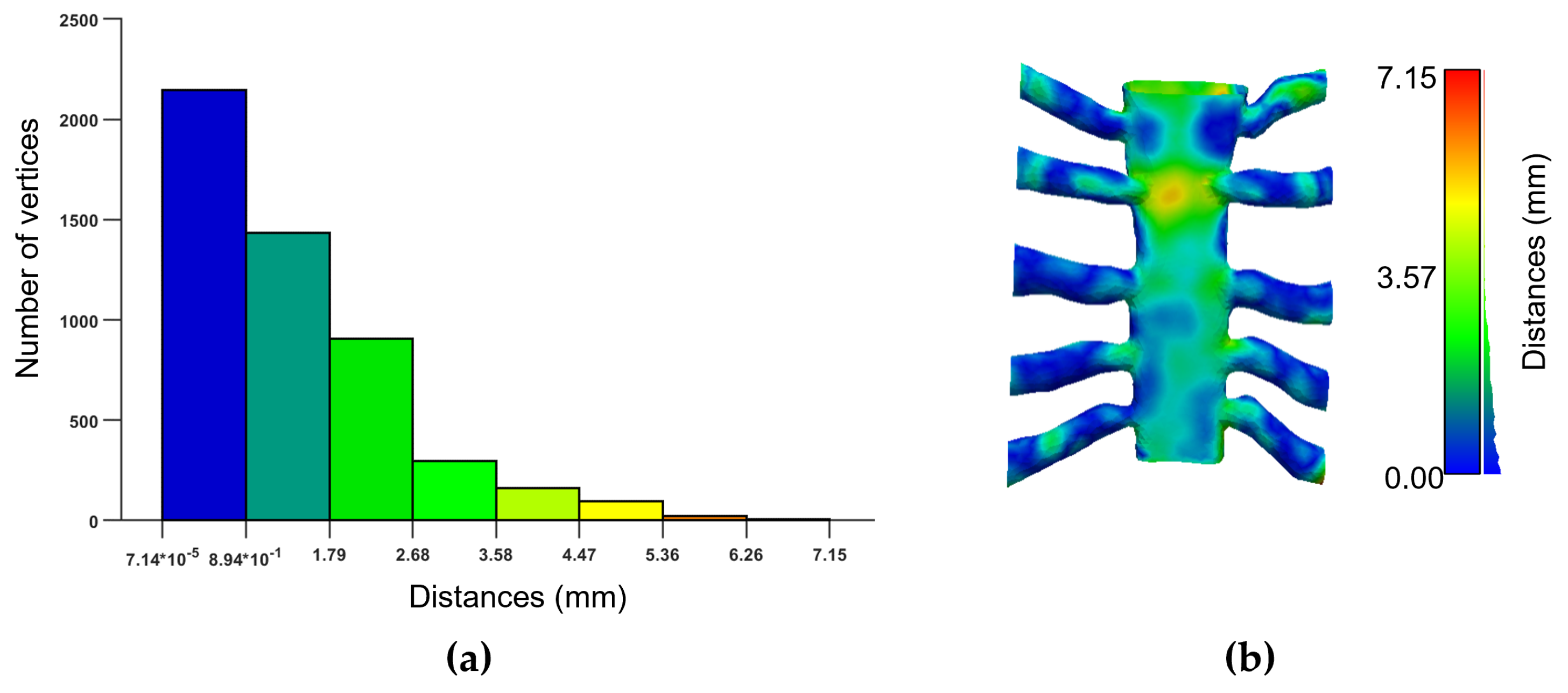
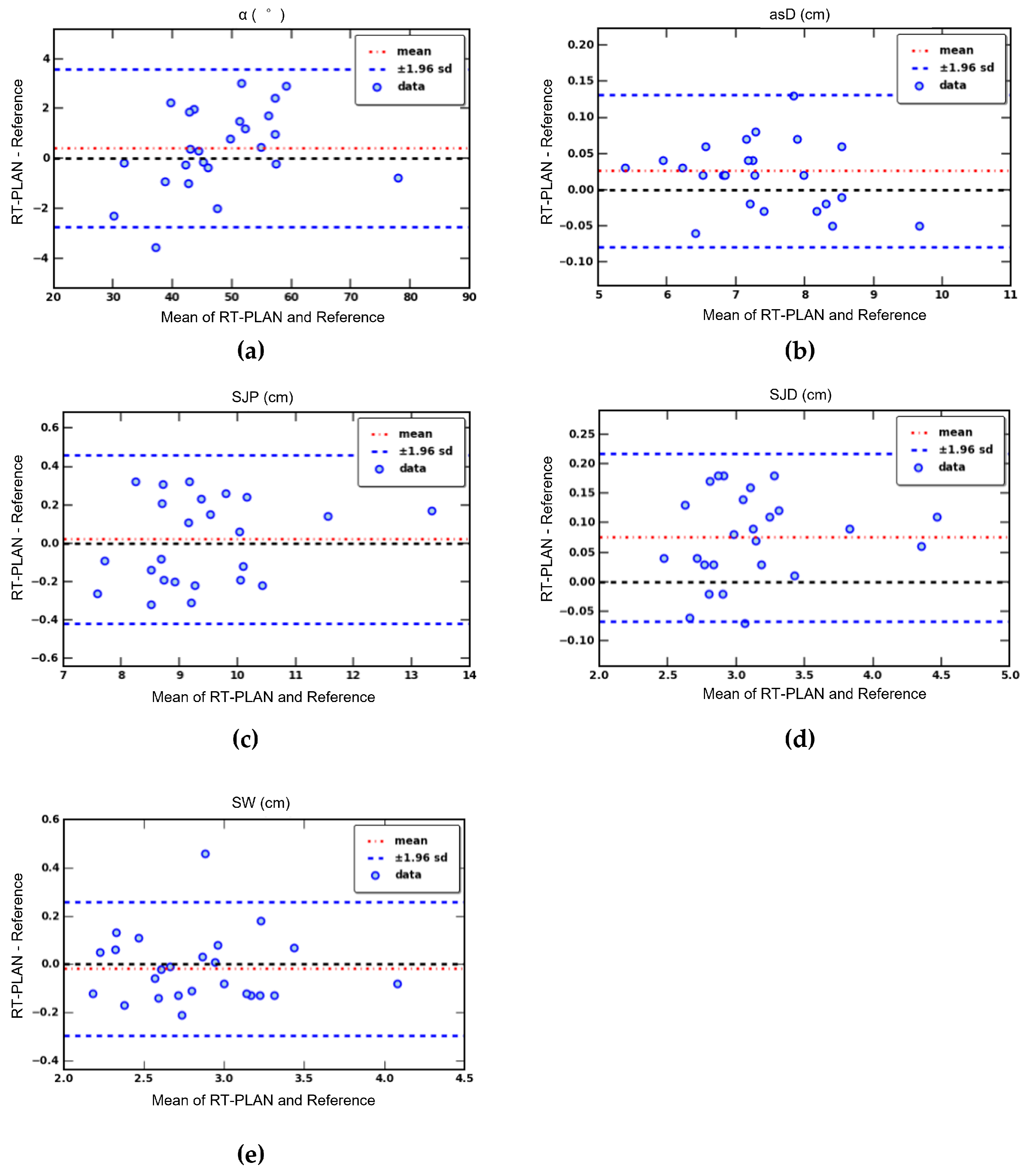
2.4. Validation and Statistical Analysis
3. Results
3.1. Segmentation and 3D Model Reconstruction
3.2. RT Inclusion Criteria Evaluation and Geometric Parameters Extraction
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Goldbarg, S.H.; Elmariah, S.; Miller, M.A.; Fuster, V. Insights into degenerative aortic valve disease. J. Am. Coll. Cardiol. 2007, 50, 1205–1213. [Google Scholar] [CrossRef] [Green Version]
- Hartley, A.; Hammond-Haley, M.; Marshall, D.C.; Salciccioli, J.D.; Malik, I.S.; Khamis, R.Y.; Shalhoub, J. Trends in Mortality From Aortic Stenosis in Europe: 2000–2017. Front. Cardiovasc. Med. 2021, 8, 748137. [Google Scholar] [CrossRef]
- Carabello, B.A.; Paulus, W.J. Aortic stenosis. Lancet 2009, 373, 956–966. [Google Scholar] [CrossRef]
- Coffey, S.; Cairns, B.J.; Iung, B. The modern epidemiology of heart valve disease. Heart 2016, 102, 75–85. [Google Scholar] [CrossRef]
- Cosgrove, D.M.; Sabik, J.F. Minimally invasive approach for aortic valve operations. Ann. Thorac. Surg. 1996, 62, 596–597. [Google Scholar] [CrossRef]
- Johnston, W.F.; Ailawadi, G. Surgical management of minimally invasive aortic valve operations. Semin. Cardiothorac. Vasc. Anesth. 2012, 16, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, D.H.; Vo, A.T.; Le, K.M.; Vu, T.T.; Nguyen, T.T.; Vu, T.T.; Pham, C.V.; Truong, B.Q. Minimally Invasive Ozaki procedure in aortic valve disease: The preliminary results. Innovations 2018, 13, 332–337. [Google Scholar] [CrossRef]
- Di Bacco, L.; Miceli, A.; Glauber, M. Minimally invasive aortic valve surgery. J. Thorac. Dis. 2021, 13, 1945. [Google Scholar] [CrossRef]
- Merk, D.R.; Lehmann, S.; Holzhey, D.M.; Dohmen, P.; Candolfi, P.; Misfeld, M.; Mohr, F.W.; Borger, M.A. Minimal invasive aortic valve replacement surgery is associated with improved survival: A propensity-matched comparison. Eur. J. Cardio-Thorac. Surg. 2015, 47, 11–17. [Google Scholar] [CrossRef] [Green Version]
- Glauber, M.; Ferrarini, M.; Miceli, A. Minimally invasive aortic valve surgery: State of the art and future directions. Ann. Cardiothorac. Surg. 2015, 4, 26. [Google Scholar]
- Bruno, P.; Cammertoni, F.; Rosenhek, R.; Mazza, A.; Pavone, N.; Iafrancesco, M.; Nesta, M.; Chiariello, G.A.; Spalletta, C.; Graziano, G.; et al. Improved patient recovery with minimally invasive aortic valve surgery: A propensity-matched study. Innovations 2019, 14, 419–427. [Google Scholar] [CrossRef] [PubMed]
- Karimov, J.H.; Santarelli, F.; Murzi, M.; Glauber, M. A technique of an upper V-type ministernotomy in the second intercostal space. Interact. Cardiovasc. Thorac. Surg. 2009, 9, 1021–1022. [Google Scholar] [CrossRef] [PubMed]
- Brown, M.L.; McKellar, S.H.; Sundt, T.M.; Schaff, H.V. Ministernotomy versus conventional sternotomy for aortic valve replacement: A systematic review and meta-analysis. J. Thorac. Cardiovasc. Surg. 2009, 137, 670–679. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khoshbin, E.; Prayaga, S.; Kinsella, J.; Sutherland, F. Mini-sternotomy for aortic valve replacement reduces the length of stay in the cardiac intensive care unit: Meta-analysis of randomised controlled trials. BMJ Open 2011, 1, e000266. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Plass, A.; Scheffel, H.; Alkadhi, H.; Kaufmann, P.; Genoni, M.; Falk, V.; Grünenfelder, J. Aortic valve replacement through a minimally invasive approach: Preoperative planning, surgical technique, and outcome. Ann. Thorac. Surg. 2009, 88, 1851–1856. [Google Scholar] [CrossRef]
- Miceli, A.; Ferrarini, M.; Glauber, M. Right anterior minithoracotomy for aortic valve replacement. Ann. Cardiothorac. Surg. 2015, 4, 91. [Google Scholar]
- Castrovinci, S.; Emmanuel, S.; Moscarelli, M.; Murana, G.; Caccamo, G.; Bertolino, E.C.; Nasso, G.; Speziale, G.; Fattouch, K. Minimally invasive aortic valve surgery. J. Geriatr. Cardiol. JGC 2016, 13, 499. [Google Scholar]
- Jahangiri, M.; Hussain, A.; Akowuah, E. Minimally invasive surgical aortic valve replacement. Heart 2019, 105, s10–s15. [Google Scholar] [CrossRef]
- Krishna, R.K.; Santana, O.; Mihos, C.G.; Pineda, A.M.; Weiss, U.K.; Lamelas, J. Minimally invasive aortic valve replacement in octogenarians performed via a right anterior thoracotomy approach. J. Heart Valve Dis. 2014, 23, 671–674. [Google Scholar]
- Miceli, A.; Murzi, M.; Gilmanov, D.; Fugà, R.; Ferrarini, M.; Solinas, M.; Glauber, M. Minimally invasive aortic valve replacement using right minithoracotomy is associated with better outcomes than ministernotomy. J. Thorac. Cardiovasc. Surg. 2014, 148, 133–137. [Google Scholar] [CrossRef] [Green Version]
- Olds, A.; Saadat, S.; Azzolini, A.; Dombrovskiy, V.; Odroniec, K.; Lemaire, A.; Ghaly, A.; Lee, L.Y. Improved operative and recovery times with mini-thoracotomy aortic valve replacement. J. Cardiothorac. Surg. 2019, 14, 1–7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Seitz, M.; Goldblatt, J.; Paul, E.; Marcus, T.; Larobina, M.; Yap, C.H. Minimally invasive aortic valve replacement via right anterior mini-thoracotomy: Propensity matched initial experience. Heart Lung Circ. 2019, 28, 320–326. [Google Scholar] [CrossRef] [PubMed]
- Khan, I.; Smith, J.A.; Trehan, N. Minimally Invasive Right Anterior Mini-Thoracotomy Aortic Valve Replacement. In Cardiac Surgery Procedures; IntechOpen: London, UK, 2019. [Google Scholar]
- Celi, S.; Martini, N.; Emilio Pastormerlo, L.; Positano, V.; Berti, S. Multimodality imaging for interventional cardiology. Curr. Pharm. Des. 2017, 23, 3285–3300. [Google Scholar] [CrossRef]
- Daubert, M.A.; Tailor, T.; James, O.; Shaw, L.J.; Douglas, P.S.; Koweek, L. Multimodality cardiac imaging in the 21st century: Evolution, advances and future opportunities for innovation. Br. J. Radiol. 2021, 94, 20200780. [Google Scholar] [CrossRef]
- Van der Hoeven, B.L.; Schalij, M.J.; Delgado, V. Multimodality imaging in interventional cardiology. Nat. Rev. Cardiol. 2012, 9, 333–346. [Google Scholar] [CrossRef]
- Celi, S.; Gasparotti, E.; Capellini, K.; Vignali, E.; Fanni, B.M.; Ali, L.A.; Cantinotti, M.; Murzi, M.; Berti, S.; Santoro, G.; et al. 3D printing in modern cardiology. Curr. Pharm. Des. 2021, 27, 1918–1930. [Google Scholar] [CrossRef]
- Capellini, K.; Vignali, E.; Costa, E.; Gasparotti, E.; Biancolini, M.E.; Landini, L.; Positano, V.; Celi, S. Computational fluid dynamic study for aTAA hemodynamics: An integrated image-based and radial basis functions mesh morphing approach. J. Biomech. Eng. 2018, 140, 111007. [Google Scholar] [CrossRef] [PubMed]
- Volonghi, P.; Tresoldi, D.; Cadioli, M.; Usuelli, A.M.; Ponzini, R.; Morbiducci, U.; Esposito, A.; Rizzo, G. Automatic extraction of three-dimensional thoracic aorta geometric model from phase contrast MRI for morphometric and hemodynamic characterization. Magn. Reson. Med. 2016, 75, 873–882. [Google Scholar] [CrossRef]
- Staal, J.; van Ginneken, B.; Viergever, M.A. Automatic rib segmentation and labeling in computed tomography scans using a general framework for detection, recognition and segmentation of objects in volumetric data. Med. Image Anal. 2007, 11, 35–46. [Google Scholar] [CrossRef] [PubMed]
- Xu, Z.; Bagci, U.; Jonsson, C.; Jain, S.; Mollura, D.J. Efficient ribcage segmentation from CT scans using shape features. In Proceedings of the 2014 36th Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Chicago, IL, USA, 26–30 August 2014; IEEE: Piscataway, NJ, USA, 2014; pp. 2899–2902. [Google Scholar]
- Niiya, A.; Murakami, K.; Kobayashi, R.; Sekimoto, A.; Saeki, M.; Toyofuku, K.; Kato, M.; Shinjo, H.; Ito, Y.; Takei, M.; et al. Development of an artificial intelligence-assisted computed tomography diagnosis technology for rib fracture and evaluation of its clinical usefulness. Sci. Rep. 2022, 12, 8363. [Google Scholar] [CrossRef]
- Fantazzini, A.; Esposito, M.; Finotello, A.; Auricchio, F.; Pane, B.; Basso, C.; Spinella, G.; Conti, M. 3D automatic segmentation of aortic computed tomography angiography combining multi-view 2D convolutional neural networks. Cardiovasc. Eng. Technol. 2020, 11, 576–586. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | RT-PLAN | Reference |
|---|---|---|
| (cm) | 7.50 ± 1.10 | 7.47 ± 1.10 |
| α (°) | 48.16 ± 10.2 | 47.76 ± 9.64 |
| (cm) | 9.57 ± 1.46 | 9.55 ± 1.38 |
| (cm) | 3.15 ± 0.48 1 | 3.08 ± 0.47 |
| (cm) | 2.82 ± 0.43 | 2.48 ± 0.44 |
| Patients RT (n = 6) | Patients NO RT (n = 19) | |||
|---|---|---|---|---|
| Parameters | Reference | RT-PLAN | Reference | RT-PLAN |
| (%) | 100 | 100 | 21 | 21 |
| (cm) | ||||
| α (°) | ||||
| (cm) | ||||
| (cm) | ||||
| (cm) | ||||
| (cm) | - | - | ||
| (cm) | - | - | ||
| (cm) | - | - | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Capellini, K.; Positano, V.; Murzi, M.; Farneti, P.A.; Concistrè, G.; Landini, L.; Celi, S. A Decision-Support Informatics Platform for Minimally Invasive Aortic Valve Replacement. Electronics 2022, 11, 1902. https://doi.org/10.3390/electronics11121902
Capellini K, Positano V, Murzi M, Farneti PA, Concistrè G, Landini L, Celi S. A Decision-Support Informatics Platform for Minimally Invasive Aortic Valve Replacement. Electronics. 2022; 11(12):1902. https://doi.org/10.3390/electronics11121902
Chicago/Turabian StyleCapellini, Katia, Vincenzo Positano, Michele Murzi, Pier Andrea Farneti, Giovanni Concistrè, Luigi Landini, and Simona Celi. 2022. "A Decision-Support Informatics Platform for Minimally Invasive Aortic Valve Replacement" Electronics 11, no. 12: 1902. https://doi.org/10.3390/electronics11121902
APA StyleCapellini, K., Positano, V., Murzi, M., Farneti, P. A., Concistrè, G., Landini, L., & Celi, S. (2022). A Decision-Support Informatics Platform for Minimally Invasive Aortic Valve Replacement. Electronics, 11(12), 1902. https://doi.org/10.3390/electronics11121902