Abstract
Atopic dermatitis, the most common form of eczema, is a chronic, relapsing inflammatory skin condition that occurs with dry skin, persistent itching, and scaly lesions. This debilitating condition significantly compromises the patient’s quality of life due to the intractable itching and other associated factors such as disfigurement, sleeping disturbances, and social stigmatization from the visible lesions. The treatment mainstay of atopic dermatitis involves applying topical glucocorticosteroids and calcineurin inhibitors, combined with regular use of moisturizers. However, conventional treatments possess a certain degree of adverse effects, which raised concerns among the patients resulting in non-adherence to treatment. Hence, the modern use of moisturizers to improve barrier repair and function is of great value. One of the approaches includes incorporating bioactive ingredients with clinically proven therapeutic benefits into dermocosmetics emollient. The current evidence suggests that these dermocosmetics emollients aid in the improvement of the skin barrier and alleviate inflammation, pruritus and xerosis. We carried out a critical and comprehensive narrative review of the literature. Studies and trials focusing on moisturizers that include phytochemicals, natural moisturizing factors, essential fatty acids, endocannabinoids, and antioxidants were identified by searching electronic databases (PubMed and MEDLINE). We introduce the current knowledge on the roles of moisturizers in alleviating symptoms of atopic dermatitis. We then further summarize the science and rationale of the active ingredients in dermocosmetics and medical device emollients for treating atopic dermatitis. Finally, we highlight the limitations of the current evidence and future perspectives of cosmeceutical research on atopic dermatitis.
Keywords:
atopic eczema; moisturizers; emollients; active ingredients; skin barrier; skin physiology 1. Introduction
Atopic dermatitis (AD) is a chronic inflammatory skin disease [1] that usually starts in early childhood. AD affects 15–20% of children worldwide and can extend well into adulthood at an incidence of 1–3% [2,3]. A wide variation of prevalence is reported, where AD is reported more frequently in developed nations with more than a 15% prevalence rate [3,4]. It can be diagnosed clinically following validated diagnostic criteria, such as the Hanifin and Rajka diagnostic criteria [5]. Eczematous rashes are itchy and can be acute, subacute, or chronic. Though able to affect any part of the body, eczematous rashes appear with age-related morphology and distribution. It is found to be associated with other atopic diseases. Children with atopic eczema are at risk of cutaneous infections. AD was found to be associated with poorer quality of life (QoL) [6]. The epidermal barrier plays a pivotal role in atopic eczema pathogenesis. The treatment of AD focuses on maximizing skin barrier repair and reducing inflammation. Topical corticosteroids (TCS) are the first-line anti-inflammatory treatment for AD. However, chronic usage of topical corticosteroids may further lead to skin barrier defects by inhibiting epidermal proliferation, differentiation, and lipid production [7].
Twice daily application of moisturizer improves skin hydration, reduces AD symptoms, flares, and severity, and reduces the amount of topical anti-inflammatory medication needed [8,9,10]. Conventional moisturizer consists of three main ingredients: emollients, humectants, and occlusive agents [9,11]. These ingredients reduce transepidermal water loss (TEWL) via various mechanisms. Emollients lubricate and soften the skin, while occlusive agents form a hydrophobic layer on the stratum corneum (SC) and prevent water evaporation. Meanwhile, humectants increase the amount of water retained by the SC through their hydrophilic nature [8,9,11]. In recent years, medical device emollient creams (MDEC) containing active ingredients have started to become the trend in the current cosmeceutical research, owing to their ability to alleviate cutaneous inflammation while repairing skin barriers [12,13,14]. Studies on various active ingredients with in vivo and in vitro efficacy have been published. Some are reported to be non-inferior to low potency corticosteroids [15].
In this article, we aim to review the current understanding of the pathophysiology for atopic eczema, as well as the mechanism of action, safety, and efficacy of common active ingredients that were found to be beneficial in alleviating symptoms of atopic eczema.
2. Pathophysiology of AD
A fundamental argument on the etiology of AD is whether it is primarily induced by epidermal barrier dysfunction (outside–inside hypothesis) or primarily by an immune response to environmental triggers (inside–outside hypothesis) [16]. Nevertheless, the clinical manifestation of AD is believed to involve a multifactorial interplay among gene and epidermal barrier dysfunction, Th2 immune dysregulation, environmental triggers, and skin microbiome abnormalities [16,17,18]. Additionally, skin pH levels [19,20] and the deficiency of endogenous natural moisturizing factors (NMFs) [21,22] were also found to play a role.
2.1. Gene Dysfunction and Epidermal Barrier Dysfunction
FLG gene mutation was found in 20–40% of patients with atopic dermatitis. It encodes the pre-protein profilaggrin, which will then be translated to filaggrin monomer. Filaggrin is required for keratinization, moisturization, and maintenance of the stratum corneum homeostasis [23]. The lack of filaggrin will lead to disruption of barrier function. FLG gene expression may be further downregulated when it is cross-linked with the T-helper type 2 cells (Th2) derived cascades.
SC and tight junctions play the most critical roles in the epidermal barrier. SC is made up of corneocytes intermixed in a matrix of intercellular lipids (ceramides, cholesterol, and fatty acids) [3,23]. Environmental triggers, including irritants, pruritogens, hot and dry climate, and ultraviolet radiation, can disrupt the epidermal barrier leading to higher skin pH levels, increased TEWL, altered lipid composition, reduced level of ceramides, and higher serine protease activity [13,24]. Ceramide plays an essential structural role in forming the permeability barrier that functions as a water reservoir, holding the water molecules in the multilamellar structures. The prolonged compromised global lipid composition of SC in AD sufferers and the further deficiency in ceramide fraction eventually lead to barrier dysfunction, decreased SC hydration, S. aureus colonization, as well as allergen penetration. Hence, the mitigation of the barrier abnormality in AD requires topical aid that adequately delivers the key lipids that mediate barrier function, which is ideally provided in a ceramide-dominant proportion [25,26,27].
2.2. Th2 Mediated Immune Dysregulation and Neuroimmune Interactions
The Th2-mediated immune response is currently at the center of AD pathogenesis. The exposure of irritants and pruritogens to the disrupted epidermal barrier initiates an immunological cascade that stimulates Th2 pro-inflammatory cytokine production, such as interleukin-4 (IL-4), IL-5, and IL-13 [16,23]. Subsequently, IL-4 and IL-13 stimulate the production of IL-31, which results in pruritus, triggering excessive scratching and further aggravation of the inflammatory response (Figure 1).
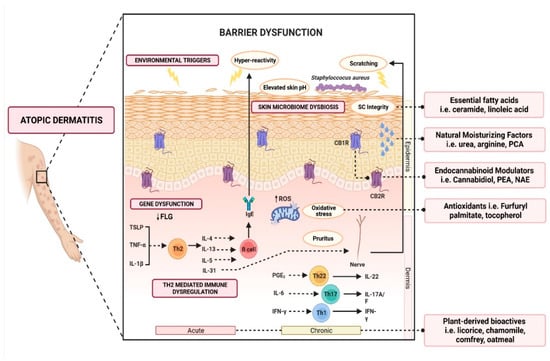
Figure 1.
Schematic illustration of various active ingredients and the targeted mechanisms in alleviating atopic dermatitis.
2.3. Skin Microbiome Dysbiosis
The skin microbiome plays a pivotal role in maintaining the homeostasis of the skin, and colonization of Staphylococcus aureus strains in AD is thought to be associated with the clinical manifestation and pathogenesis of flares. S. aureus colonization was observed in up to 90% of lesional skin and 40% of non-lesional skin as opposed to being almost absent in healthy skin [28,29,30]. The dysbiosis contributes to the elevated pH levels that are observed throughout atopic dermatitis flares [31,32]. Furthermore, S. aureus colonies were found to secrete a group of virulence factors, such as superantigens (Sag), α-toxin, δ-toxin, protein A, and phenol-soluble modulins (PSM), that may exacerbate keratinocyte inflammation [28,29,30], release cytosolic granules (such as histamine, IL-3, and IL-13), aid in biofilm development and promote Staphylococcal colonization [30].
2.4. Other Factors Affecting Barrier Function
2.4.1. Acid Mantle in Epidermal Barrier Function
Skin pH is a vital component in maintaining the normal functions of the skin [33,34]. The film of the outermost layer of the skin, known as the acid mantle, bears a pH range of 4.0–6.0, depending on body parts [34]. Neonatal skin pH is near-neutral, where it requires several weeks of acidification processes to attain physiological skin surface pH range, making it vulnerable to external irritants during this period [35]. Dysregulation of this acidification process leads to shifts in skin pH to a mean of 6.25 in AD [33,36,37]. The disruption of the acidification mechanism alters phospholipid A2, β-glucocerebrosidase, serine proteases, kallikrein 5, and acid sphingomyelinase activities, which are important for the maintenance of the lipid structure in SC [34,35,38]. The alteration of skin pH will impair the antimicrobial defenses of the skin [34,35,38]. Endogenous factors (such as the FLG gene and its amino acid breakdown, such as histidine) and exogenous factors (such as acidic and alkaline substances) have been proposed to affect the acid mantle of the skin [35,38,39].
2.4.2. Natural Moisturizing Factors
Natural moisturizing factors (NMFs) refer to endogenous, highly hygroscopic substances that play a pivotal role in the maintenance of SC hydration [40]. NMFs also contribute to the maintenance of functional hydrolytic enzymes involved in desquamation and aid in optimum SC barrier function [40]. Amino acids account for 40–50% of NMFs, followed by pyrrolidone carboxylic acid (PCA) (12%), lactic acid (12%), urea (7%), inorganic salts, sugar, glycerol, and a variety of ions [40,41]. These water-soluble substances are highly efficient humectants that comprise 20–30% of the dry weight of SC mass [41]. The deficiency or reduction in NMFs is associated with an increased risk of AD and various SC abnormalities that manifest as dry skin, scaling, flaking, and increased surface pH [21,22].
3. Role of Moisturizers in the Treatment of AD
Multiple clinical guidelines recommend the use of moisturizers for the treatment of AD [42]. This helps in reducing the frequency of AD flares (3.74 times reduced risk) [42] and the total amount of steroid use (up to 15.30 g less within six weeks, p = 0.003) [42]. Although a large variety of moisturizers are available in the market, not all are beneficial. Some formulations may contain allergens (e.g., fragrance, benzyl alcohol, D-limonene, Lavandula angustifolia oil, and Melaleuca alternifolia oil), leading to contact dermatitis and worsening of the inflammation [43]. Carefully designed moisturizers should be hypoallergenic, pH-balanced, and contain humectants, emollients, and active ingredients that help to reduce inflammation [43,44,45]. Some medical device emollient creams (MDEC) are found to be suitable for alleviating AD symptoms [46,47]. MDECs are clinically designed to not only improve hydration but also repair and protect the skin’s barrier function. According to the European Commission, some MDECs are classified as class IIa medical devices due to their primary action relying on mechanical or physical means [48]. Several notable MDECs, such as Atopiclair® (Menarini, Italy), Dexyane MeD® (Ducray Laboratoires Dermatologiques, France), and VEL-091604 (BSI Beauty Science Intelligence, Germany) have shown comparable clinical efficacy with corticosteroids in alleviating symptoms of moderate to severe AD, which will be discussed in the next section.
Over the last few years, emollients have been supplemented with different powerful bioactive ingredients to improve epidermal action. These additives are increasingly investigated as preventative and treatment aids for AD. Notably, these additives are categorized as compounds derived from plants, natural moisturizing factors, physiological lipids and ceramide, cannabinoid receptor modulators, and antioxidants (Figure 1). Herein, a summary of evidence-based cosmeceutical research on additives in emollients indicated for AD is presented.
4. Active Ingredients Beneficial in Alleviating Atopic Eczema Inflammation
4.1. Plant-Derived Active Ingredients
4.1.1. Licorice-Derived Bioactives
Licorice, the root of the Glycyrrhiza species, is known to have application in the treatment of various inflammatory skin diseases, particularly in eczematous skin disorders, supported by extraordinary evidence in clinical research [46,47,49,50,51,52,53,54,55,56,57]. Licorice-containing creams were found to be as effective as mild to medium-potency TCS, 1% hydrocortisone, and 1% desonide cream in treating moderate-to-severe AD [47]. Nearly 400 bioactive compounds have been isolated from Glycyrrhiza spp., most of which fall into the classes of flavonoids and triterpene saponins. Licorice has been used in food and herbal medicine across the world. In particular, Glycyrrhiza glabra L. (Fabaceae), Glycyrrhiza uralensis Fisch. Ex DC., and Glycyrrhiza inflata Bat. are the three licorice species registered in the Chinese Pharmacopoeia 2015. Common ingredients used in dermatology are licochalcone A, glycyrrhetinic acid (GA), and glycyrrhizin.
Licochalcone A is an oxygenated chalconoid phenol derived specifically from the root of Xinjiang licorice, G. inflata. Vast clinical trials demonstrated the positive anti-inflammatory and anti-pruritic results of topical semi-solid formulations which contain Licochalcone A [15,58,59,60]. On the other hand, GA, a pentacyclic triterpenoid saponin compound, is a bioactive marker of G. glabra and G. ularensis. Meanwhile, glycyrrhizin is the major water-soluble bioactive compound of G. glabra, found at concentrations of 1–9% at its stem [61]. The chemical structure of glycyrrhizin carries a molecule of GA with two molecules of glucuronic acid [61,62]. Both GA and glycyrrhizin have a long history in traditional medicine in ancient Indian, Egyptian and Chinese cultures [63]. It is widely reported to possess anti-allergic and anti-inflammatory properties, the effects of which are similar to those of topical corticosteroids for the treatment of skin diseases, including atopic dermatitis, contact dermatitis, and psoriasis [55,64,65].
The anti-inflammatory mode of action of Lichochalcone, GA, and glycyrrhizin are directed towards the suppression of pro-inflammatory mediators, such as prostaglandin E2 (PGE2) from cyclooxygenase-2 (COX-2), as well as leukotriene B4 (LTB4), IL-1 and IL-6 by the residential skin cells and the cells of the innate and adaptive immune system [57,63]. In addition, these bioactive compounds also exhibit antimicrobial activity against multidrug-resistant S. aureus [66] and have been shown to suppress of translocation of nuclear factor (NF-κB)-regulated gene products and inhibit TNF-α induced inflammation [67]. GA and glycyrrhizin possess the ability to reduce oedema through inhibition 12-O-tetradecanoylphorbol-13-acetate-induced glucose transport, whereas the reduction in pruritus was associated with the inhibition of leukotriene B4 (LTB4) [53]. Additionally, glycyrrhizin was reported to bind directly to high-mobility group box 1 (HMGB1) protein, consequently inhibiting the HMGB1 signalling cascade, leading to the suppression of inflammatory cytokines [57].
Studies have demonstrated that a 0.025% Licochalcone A-containing moisturizer significantly improved AD clinical characteristics and itch intensity [66,68]. The improvement was found to be comparable to 1% hydrocortisone [15]. Furthermore, there is also a pronounced decrease in S. aureus colonization. These improvements can take place as soon as seven days after the initial treatment [58]. It also significantly reduces flare by 60% compared to its vehicle [59]. Similarly, thrice daily preparation of 1% GA- and 2% GA-based gels showed a significant reduction in erythema scores of 35.02% and 60.76%, respectively, followed by 56.64% and 83.76% reduction in oedema scores, as well as a reduction in pruritus scores of 44.1% and 72.53% [55]. In multiple multi-centered, randomized, vehicle-controlled studies, a cream containing GA, Vitis vinifera L. extract, and telmestine (Atopiclair®) demonstrated significant symptomatic relief and skin barrier improvement [49,50,51,54]. This allows it to be authorized in US and EU as a medical device cream for symptomatic relief in the management of AD [49]. Some adverse effects, including rash, stinging sensation, and burning sensation were observed in a small percentage of the patients, however, it is considered rare and not more frequent than the vehicle [49,51]. The evidence of GA was further demonstrated by other medical devices with GA, namely Dexyane MeD® and VEL-091604, which also demonstrated promising clinical efficacy for mild to moderate AD, either as a stand-alone treatment or in combination with TCS [46,47,56].
It is worth mentioning that the above formulas are not the sole active ingredients. These products are commonly formulated with other antioxidative or anti-inflammatory agents such as allantoin, bisabolol, and other natural extracts. Thus, the efficacy of these medical devices might be enhanced by the synergistic effects between these botanical-derived bioactive compounds and other antioxidative agents.
Certain researchers shared the concern that the utilization of GA and glycyrrhizin may lead to increased systemic glucocorticoid and mineralocorticoid toxic effects [69]. This may be attributed to its ability to inhibit 11-hydroxysteroid dehydrogenase, an enzyme responsible for converting endogenous cortisol to cortisone. These indications were only reported in oral ingestion and intravenous injection of GA and glycyrrhizin combined with the prescription of hydrocortisone or prednisolone [68]. To date, no evidence of such effects due to topical GA and glycyrrhizin has been reported [70].
To conclude, these are significant results considering that the current AD treatments depend heavily on the recurrent use of topical corticosteroids for acute flare treatment and prevention, and show that various phytochemicals-formulated emollients should be included in future larger-scale clinical studies.
4.1.2. Chamomile-Derived Bioactives
Matricaria chamomilla L., generally known as chamomile, has a long-standing history in herbal medicine in the treatment of dry skin, inflammatory skin disorders, pruritic skin disorders, and various dermatoses owing to its anti-inflammatory, anti-histaminic, mild astringent, soothing, and healing potential [71,72]. Several in vitro and animal studies have reported the significant efficacy of chamomile extracts and oil in eczematous atopic models [72,73,74]. It modulates the type-2 inflammation response by altering the Th2 cell activation, which results in the downregulation of IL-4 production [72,73]. It also demonstrated anti-pruritic effects by suppressing IgE over-production and hindering the binding of histamine to its receptor, which eventually reduces the histamine release from mast cells [72]. In addition, chamomile oil also regulated the Th17 cell differentiation pathway, leading to a decreased level of IL-17, inhibition of NF-κB activation, and suppression of the pro-inflammatory factors TNF-α and IL-6 which ultimately reduces inflammation in eczema [74]. Indeed, an over-the-counter chamomile extract containing a cream, Kamillosan® (MEDA Pharma, Germany), was found to ameliorate mild-to-moderate AD in several clinical studies. The studies demonstrated marginal superiority against 5% bufexamac and 0.75% fluocortin butyl ester and equally effective therapeutic results compared to 0.25–0.5% hydrocortisone [75,76].
Chamomile’s therapeutic benefits for treating eczema are associated with its major sesquiterpene constituents, including azulene, bisabolol, and elemenes [74]. In particular, α-bisabolol, also known as levomenol, accounts for its potent anti-inflammatory effects, among others [72,74]. Moreover, α-bisabolol is known for its ability as a percutaneous penetration and absorption enhancer [77]. It was reported that α-bisabolol increased the permeability coefficient of triamcinolone acetonide by 73-fold in human skin samples with respect to untreated skin [77]. This is likely due to its effect of increasing the lipid fluidity of SC, permitting the increase in diffusion rate across the skin barrier [77,78]. Dermocosmetics containing α-bisabolol have shown soothing effects and eczema associated-inflammation reduction as observed through reduced TEWL and improvement in SCORAD, TESS, ESS, and VAS scores [79,80,81,82,83,84]. The efficacy was also found among paediatric populations [79,80,81,84].
In a relatively small percentage of the population, chamomile may induce allergic contact dermatitis reactions. This hypersensitive reaction, known as Compositae mix allergy, is initiated by several species of plants in the Compositae or Asteraceae family [85]. The common allergens in the Compositae family are sesquiterpene lactones, polyacetylenes, and thiophenes. Bisabolol is considered a potential cause of allergic contact dermatitis in AD patients with a history of moisturizer intolerance [86]. However, it is to be noted that the frequency of allergic reactions to chamomile and bisabolol is low even within the other Compositae allergens [85]. This was evident in the fact that allergic reactions to the mixture of Compositae extracts were observed in only 118 out of 3851 subjects [87]. Furthermore, among the allergenic subjects, chamomile elicited lesser allergic reactions (65 subjects) in comparison with feverfew (82 subjects), chrysanthemums (75 subjects), and tansy (71 subjects) [87].
Taking this evidence into account, α-bisabolol and α-bisabolol-rich oil may prove to be meaningful active ingredients in cosmeceutical and pharmaceuticals application on eczematous skin cases, though clinicians and patients should be made aware of its allergenic potential.
4.1.3. Comfrey-Derived Bioactive
Commonly known as comfrey, Symphytum officinale L. is a perennial herb native to the United Kingdom but also commonly found in Europe, North America, and North Asia [88]. It has been extensively utilized in European indigenous medicine as poultice or ointment to soothe irritated and inflamed tissue, promote wound healing, and reduce osteoarticular inflammation [89,90]. Though its pharmacological effects are undoubted, the oral consumption of comfrey is widely prohibited due to its hepatotoxicity from some of its pyrrolizidine alkaloids constituents, such as lasiocarpine, echimidine, symphytine [91,92,93]. Fortunately, external application of comfrey and its extracts have proved to be safe, with no report of major adverse effects, mainly due to poor cutaneous penetration and absorption of these alkaloids [94,95]. In fact, the therapeutic effects and clinical efficacy of topical comfrey-containing creams and ointments are supported by several clinical studies that evaluated their effects in treating pain, cutaneous wounds, and inflammation from sprains and bruises [96,97,98]. These anti-inflammatory and tissue healing activities are attributed to their bioactive constituents, including allantoin and rosmarinic acid [71,88,89].
Allantoin is a heterocyclic organic compound and a uric acid oxidation product [89,90], widely used in various personal care products as a skin conditioner, emollient agent, mild keratolytic agent, and soothing agent [88,90]. At the same time, allantoin has been shown to stimulate healthy cell proliferation, epithelization, and wound healing. A clinical study revealed that an emulsion with a 5% concentration of allantoin had significant wound-healing effects by promoting fibroblastic proliferation and extracellular matrix, which contribute to the accelerated re-establishment of healthy skin in comparison to the vehicle [99]. The anti-inflammatory activity of allantoin was also observed in a murine allergic model by reducing IgE levels and IL-4 and IL-5 production [100].
Allantoin-containing moisturizers were shown to positively relieve mild-to-moderate atopic dermatitis [83,101,102]. Curel® moisture cream (Kao, Japan), which contains 0.5% allantoin and pseudo-ceramide, was found to be a beneficial adjunct to topical corticosteroids in providing symptom relief and improved skin texture in adults and children with mild-to-moderate AD [102]. Its use was found to significantly improve the quality of life, mean SCORAD, and mean POEM. Twice-daily regular application also resulted in the significantly reduced frequency of flares. Furthermore, 12.5% of 40 subjects discontinued the use of TCS by the end of the four weeks of study [102]. Similar outcomes were reported in another trial [101]. Trials subjects were found to have high compliance, tolerability, and acceptability of allantoin in topical preparations with no related or severe adverse effects observed [101,102].
Rosmarinic acid is an esterified caffeic acid and 3,4-dihydroxyphenyl lactic acid [103]. It exerts a plethora of biological activities, including anti-inflammatory, antioxidant and antibacterial effects. Rosmarinic acid demonstrated an anti-inflammatory effect by inhibiting the expression of IL-1β, IL-6, and TNF-α and downregulating the NF- κB pathway. These anti-inflammatory effects were found in various in vitro and animal studies [104]. It was also found to hamper the infiltration of CD4+ helper T cells, CD8+ cytotoxic T cells, and mast cells to DNFB-induced skin lesions in NC/Nga mice, leading to the suppression of IFN-γ and IL-4 via activated T cells and reduced levels of total serum IgE [105]. Clinically, topical applications of 0.3% rosmarinic acid emulsion were proven to provide symptomatic relief for eczematous lesions by demonstrating a significant improvement in erythema, crusting, pruritus, SCORAD, skin thickness, and TEWL [106]. It is to be noted that the use of both systemic and topical corticosteroids was eliminated throughout the study. This indicates the possibility of introducing rosmarinic acid as a TCS-sparing agent for AD, albeit more extensive studies have to be carried out to establish firmer clinical evidence [106].
4.1.4. Colloidal Oatmeal
Colloidal oatmeal is widely known to alleviate the disease hallmarks of AD. It was found that daily application of colloidal oatmeal extracts-containing lotion showed significant clinical improvements in 50 subjects with severely dry skin in as little as three weeks of treatment [107]. The efficacy is also demonstrated by another over-the-counter 1% colloidal oatmeal cream for pediatrics suffering from mild-to-moderate AD [108,109]. During the three weeks of the study period, significant improvements were demonstrated in clinical (EASI, IGA, and pruritus score) and objective assessment (erythema, dryness, skin hydration). This efficacy is non-inferior to a controlled prescribed cream (EpiCeram®, Primus Pharmaceuticals, US) [108,109]. Colloidal oatmeal is thought to induce the repair of barrier damage, regulate lipid complex in SC, and enhance pH-buffering capacity, which aids in protection against irritants and normalizing cutaneous pH to its acidic range [107]. This may be associated with its ability to form a protective, occlusive barrier that retards water loss from the epidermis. In addition, the phytochemicals in oatmeal, such as saponins, may contribute to maintaining skin pH by solubilizing dirt, oil, and sebaceous secretions [108,109]. As a result of the evident pharmacological benefits, dermatologists have increasingly recommended the use of colloidal oatmeal-containing moisturizers for the treatment and prevention of AD.
4.2. Natural Moisturizing Factors
Urea is one of the first and most studied NMF compounds that has been formulated in moisturizing emollients since 1943 [110]. Urea, also known as carbamide, is an organic compound with the chemical structure of a carbonyl group attached to two amine residues. Besides acting as a humectant, urea also acts as a mild keratolytic agent when formulated at higher concentrations (>10% urea) [111]. The efficacy and safety of topical urea creams in treating AD have been proven through substantial clinical evidence. Older clinical studies mainly include the application of 10% urea cream as a stand-alone treatment [112] or in combination with 1% hydrocortisone [113,114,115]. These studies conclusively reported a significant improvement in SC hydration, water-binding capacity, and TEWL in atopic skin [112,113,114,115]. On top of that, the efficacy of the combination treatment was clinically superior to that of hydrocortisone alone [115]. It should be noted that a higher dose of urea might cause a certain degree of burning and stinging sensation in 8–45% of patients [113,115]. Therefore, more recent clinical studies adopted formulations with lower doses of urea from 1% [116] to 5% [117,118], combined with other ingredients such as vitamin B12, profilaggrin complex, polidicanol, glycyrrhetinic acid, and high overall lipid content of >20% [116,117,118]. The efficacy of these multi-component urea creams was evident in the recovery of barrier dysfunction, reduced clinical severity of AD, and higher QoL of the sufferers, as observed in improved EASI, IGA, PIQoL scores [116,117,118].
Arginine, as one of the amino acid precursors of urea, PCA, and lactic acid, has been included in several multi-component moisturizer formulations targeted at the treatment of mild-to-moderate AD patients [119,120,121]. The safety and efficacy of these NMF-containing moisturizers in treating adults and paediatric AD patients were evident in multiple extensive studies [119,120,121]. NMFs have been used safely and effectively in large populations of patients. Hence, in particular, urea should remain a viable clinical treatment option for AD.
4.3. Ceramides and Fatty Acids Organization in Permeability Barrier Function
Regular application of semi-solid preparations with triple-physiologic lipids in a 3:1:1 molar ratio of ceramide, cholesterol, and free fatty acids, respectively, have been shown to significantly reduce the need for topical steroid application [12,122,123]. An open-label study has first revealed that substituting standard moisturizers with an over-the-counter ceramide-dominant cream (TriCeram®, Osmotics, New York, NY, USA) in the treatment regime of severe, paediatric AD patients resulted in the dramatic improvement of SC integrity, hydration, and SCORAD assessment [25]. It was found that the physiologic lipids in the lipid-enriched moisturizers traverse both intact and disrupted SC, which is taken up by keratinocytes and enhances the nascent lamellar membrane, thereby accelerating the recovery of the permeability barrier function. Several clinical studies support the tolerability and efficacy of these ceramide-dominant moisturizers in AD patients [124,125]. Indeed, some were clinically approved by the FDA as a treatment for pruritus and inflammation related to xerosis in AD [124]. Dermatologist evaluation on day 14 and day 28 showed significant improvement in disease severity, assessed as SCORAD index, as well as decreased pruritus intensity and higher sleeping quality, which is on a par with that of fluticasone, a medium-potency TCS, suggesting that it could potentially be used as an effective monotherapy or ancillary remedy for AD [123]. These results are consistent with the following study, where this ceramide-dominant cream showed clear or almost clear IGA scores in 54% of the 207 participants with mild-to-moderate AD [126]. Interestingly, the efficacy of the ceramide cream as a monotherapy was non-inferior to TCS or tacrolimus ointment [126]. In addition, significant pruritus score reductions were also reported in patients with moderate-to-severe pruritus, reflecting an average reduction of 38% from the baseline score [126]. Notably, some early studies revealed that ceramide might potentially bring about negative impacts on the barrier function when used alone [127,128]. Hence, the key physiologic lipids, particularly ceramide, free fatty acid, and cholesterol must be provided with an appropriate ratio in order to improve the barrier function following the impairment of the normal epidermal barrier [12]. This evidence indicates that physiologic lipid-based topical emulsion could be considered an effective monotherapy for patients with mild-to-moderate cases or ancillary therapy for moderate-to-severe AD, which may open up possibilities in reducing the usage of TCS in AD therapy.
4.4. Endocannabinoid System—A New Star in the Therapy of Eczema
Over the past few years, there has been an increase in interest in the endocannabinoid system (ECS)’s role in inflammatory skin diseases, including eczematous eruption [129,130,131,132]. The ECS is an endogenous metabolic system comprised of receptors with binding affinity to delta-9-tetrahydrocannabinol (THC). These receptors, including cannabinoid receptor 1 (CB1R), and cannabinoid receptor 2 (CB2R), are reportedly present on the skin [132,133]. CB1R is found at the stratum spinosum and granulosum, while CB2R is present at the basal layer [133]. The activation of these endocannabinoid receptors may increase DNA methylation via the p38 MAP kinase pathway, thereby inhibiting keratinocyte proliferation [132]. Furthermore, cutaneous ECS activation selectively reduces the secretion of thymic stromal lymphopoietin (TSLP), a pro-inflammatory mediator, and enhances the expression of anti-inflammatory and T-regulatory cytokines, including IL-10 and TGF-β [129,130]. Thus, manipulation of CB1R and CB2R is thought to be potentially able to treat a variety of dermatological conditions [131,132]. Cutaneous endocannabinoid activation is reported to reduce histamine-induced pruritus by hindering synaptic transmission in cutaneous C-fibers and the following neuropeptide release [129]. In addition, endocannabinoid bioactive compounds are also found to exhibit anti-pruritic properties via the inhibition of TRPV 1 [134].
Cannabinoids represent a class of compounds whose structures and physicochemical makeup are similar to psychoactive THC, found in Cannabis sativa L. Cannabinoids consist of three main classes—endocannabinoids, phytocannabinoids, and synthetic cannabinoids. The role of cannabinoids in eczematous eruption has been reported in both in vitro and in vivo animal studies [135,136,137,138]. Cannabidiol (CBD) is a phytocannabinoid from the cannabis plant whose structure differs slightly from THC and has demonstrated physiologic effects, including anti-inflammatory and anti-pruritic role in atopic skin. In a recent observational study with 14 adult participants with mild-to-moderate AD, regularly applying 1% CBD-containing gel significantly improved disease severity and pruritus [139]. These improvements were evident through a 34.5% average reduction in EASI scores (p < 0.005) and a 29% average decrease in the VAS scale (p < 0.05) in comparison to the baseline level [139]. Another clinical study was performed to assess the role of CBD-containing cream on atopic eczema, psoriasis, and scarring [140]. It was found that the CBD-containing cream increased hydration, transepidermal water loss, and elastic fibers of the skin [140]. However, SCORAD was not properly reported in the results. The potential benefits of cannabinoids in alleviating the clinical manifestations of AD are not negligible, and hence deserve recognition in its ongoing clinical research.
N-palmitoylethanolamine (PEA), also known as Palmitate MEA, belongs to the family of N-acylethanolamine (NAE). NAE is able to downregulate inflammatory response via cannabinomimetic action of CB receptor. PEA exhibits little affinity to CB receptors, but instead acts as an “entourage” to endogenous cannabinoids such as anandamide (arachinodylethanolamine) at the cannabinoid receptors, inhibiting their inactivation [134]. A cream containing PEA was found to significantly reduce the dermatological hallmarks of atopic dermatitis, including erythema, pruritus, scaliness, lichenification, and dryness by 54–66% in a global study [141]. It also reduced the need for the topical application of corticosteroids by 62% in mild-to-moderate AD patients, where 56% of the participants were able to discontinue TCS altogether [141]. The QoL of the patients was seen to be increased through 60% sleep quality improvement [141]. The efficacy was also demonstrable in alternative preparations of PEA- and NAE-containing cream [142]. These findings promise that ECS modulators containing moisturizers may potentially be utilised as TCS-sparing treatment, or adjuncts for eczematous skin conditions, though further progress in clinical research is strictly necessary.
4.5. Furfuryl Derivatives and Antioxidants
Given the compelling research on the role of oxidative stress in AD, moisturizers enriched in antioxidants, can serve as a substantial aid in the treatment of eczematous skin. Furfuryl derivatives act as antioxidants that exert remarkable quenching properties of reactive oxygen species (ROS), especially singlet oxygen (1O2) [143]. The imbalance of the highly reactive singlet oxygen induces the state of oxidative stress, which has been implicated in the pathogenesis of AD [144,145]. This state of oxidative stress is known to promote tissue inflammation through gene upregulation that leads to increased production of pro-inflammatory cytokines [144]. Pieces of evidence such as excess production of ROS during AD exacerbation and inefficient cellular antioxidant defense capacity in AD sufferers were reported in both in vitro and in vivo studies [144,145].
Furfuryl alcohol and its derivatives effectively inhibit the production of 1O2 [146,147]. This inhibition ability is attributed to the presence of a conjugated diene that interacts with O2 by either conversion to oxygen in the triplet state or sequestering the radical through a Dies–Alder-type diene dienophile addition reaction [143]. Furfuryl palmitate is an ester derivative from furfuryl alcohol and palmitic acid, which demonstrated efficacy and high tolerability in multiple clinical studies on eczematous skin. It is noteworthy that the esterification of the furyl ring in furfuryl palmitate increases the penetration capacity, hence promoting better skin absorption [143]. Of the five clinical investigations, moisturizers containing furfuryl palmitate and another widely known antioxidant, tocopherol (vitamin E), were able to significantly contrast the signs and manifestations of mild-to-moderate AD in both paediatric and adult patients [84,148,149,150,151]. Additionally, excellent positive outcomes were reported through the reduction in erythema, pruritus scores, and disease severity, showing the clear superiority of furfuryl palmitate-based moisturizers with respect to vehicle cream [149,151], and even showing non-inferiority with respect to TCS [150]. It is worth mentioning that during these trials, no major adverse effects were reported and the results were associated with high compliance and tolerability [143]. All in all, due to its efficacy and tolerability, furfuryl derivatives-enriched emollients could be considered a valuable steroid-free treatment option for AD sufferers.
5. Limitations of Current Cosmeceutical Research on AD
Though there is an increasing amount of research involving dermocosmetics, it is imperative to note that they are currently at a low level of clinical evidence. This is attributed to the fact that most of the clinically investigated formulas involved a combination of various active agents or a mixture of extracts. The observed efficacy from these multi-component formulas might not reflect the biological effect of a single active agent, but is likely due to the synergistic effects of two or more ingredients.
The majority of the studies are conducted with small sample sizes and poor study designs. Furthermore, there is a lack of harmonization in the clinical assessment measures, affecting the systemic review of the evidence as well as the meta-analysis. Future studies should be conducted with proper randomization. A controlled arm (i.e., head-to-head, placebo-controlled) should be introduced to allow the safety and efficacy of one bioactive compound to be better demonstrated without bias [152]. The utilization of proper blinding will further improve the study quality. However, such study design requires significant resources that are notably scarce in the realm of dermocosmetics.
6. Conclusions
Our review identified active ingredients such as plant-derived ingredients (e.g., licorice, chamomile, comfrey, oatmeal, and cannabinoids), essential lipids (e.g., ceramide, linoleic acid), natural moisturizing factors (e.g., urea, arginine, PCA, lactic acid) and antioxidants (e.g., furfuryl palmitate, vitamin E) that are potentially safe and effective treatments to alleviate symptoms of atopic eczema. Notably, the efficacy of some of the active ingredients is comparable to low- to medium-potency corticosteroids. Furthermore, these actives-containing moisturizers yield high treatment compliance, tolerability, as well as reduced levels of corticosteroid use. However, current poor study designs contributed to low-level clinical evidence for the recommendation of these ingredients for clinical use. More head-to-head clinical trials, homogenization of clinical outcomes and improvement of the study designs will provide better insight into the clinical roles of active ingredients in moisturizers.
Author Contributions
Conceptualization, K.N.H., W.S.L.W.A.K. and Z.W.L.; methodology, V.V.V. and K.N.H.; software, V.V.V.; validation, V.V.V. and K.N.H.; formal analysis, V.V.V.; investigation, V.V.V.; resources, V.V.V., K.N.H., W.S.L.W.A.K. and Z.W.L.; data curation, V.V.V.; writing—original draft preparation, V.V.V., K.N.H., W.S.L.W.A.K. and Z.W.L.; writing—review and editing, V.V.V. and K.N.H.; visualization, V.V.V.; supervision, K.N.H.; project administration, V.V.V. and K.N.H.; funding acquisition, K.N.H. All authors have read and agreed to the published version of the manuscript.
Funding
This work and the APC was funded by Kementerian Pendidikan Malaysia (Ministry of Education), under the Fundamental Research Grant Scheme (FRGS/1/2020/SKK01/UPM/02/).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
The authors thank Foo Jhi Biau (Taylor’s University, Malaysia) for his help in procuring publication license for the figure illustration.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Langan, S.M.; Irvine, A.D.; Weidinger, S. Atopic dermatitis. Lancet 2020, 396, 345–360. [Google Scholar] [CrossRef]
- Avena-Woods, C. Overview of atopic dermatitis. Am. J. Manag. Care 2017, 23, S115–S123. [Google Scholar] [PubMed]
- Nutten, S. Atopic dermatitis: Global epidemiology and risk factors. Ann. Nutr. Metab. 2015, 66, 8–16. [Google Scholar] [CrossRef] [PubMed]
- Silverberg, J.I.; Barbarot, S.; Gadkari, A.; Simpson, E.L.; Weidinger, S.; Mina-Osorio, P.; Rossi, A.B.; Brignoli, L.; Saba, G.; Guillemin, I.; et al. Atopic dermatitis in the pediatric population: A cross-sectional, international epidemiologic study. Ann. Allergy Asthma Immunol. 2021, 126, 417–428.e412. [Google Scholar] [CrossRef]
- Hanifin, J.M.; Rajka, G. Diagnostic features of atopic dermatitis. Acta Derm. Venereol. 1980, 1980, 44–47. [Google Scholar]
- Patel, K.R.; Immaneni, S.; Singam, V.; Rastogi, S.; Silverberg, J.I. Association between atopic dermatitis, depression, and suicidal ideation: A systematic review and meta-analysis. J. Am. Acad. Dermatol. 2019, 80, 402–410. [Google Scholar] [CrossRef]
- Li, A.W.; Yin, E.S.; Antaya, R.J. Topical corticosteroid phobia in atopic dermatitis: A systematic review. JAMA Dermatol. 2017, 153, 1036–1042. [Google Scholar] [CrossRef]
- Barrett, A.; Hahn-Pedersen, J.; Kragh, N.; Evans, E.; Gnanasakthy, A. Patient-Reported Outcome Measures in atopic dermatitis and chronic hand eczema in adults. Patient 2019, 12, 445–459. [Google Scholar] [CrossRef]
- Sidbury, R.; Davis, D.M.; Cohen, D.E.; Cordoro, K.M.; Berger, T.G.; Bergman, J.N.; Chamlin, S.L.; Cooper, K.D.; Feldman, S.R.; Hanifin, J.M.; et al. Guidelines of care for the management of atopic dermatitis: Section 3. Management and treatment with phototherapy and systemic agents. J. Am. Acad. Dermatol. 2014, 71, 327–349. [Google Scholar] [CrossRef]
- Williams, H.C.; Burney, P.G.; Pembroke, A.C.; Hay, R.J. The U.K. Working Party’s diagnostic criteria for atopic dermatitis. III. Independent hospital validation. Br. J. Dermatol. 1994, 131, 406–416. [Google Scholar] [CrossRef]
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed]
- Elias, P.M.; Wakefield, J.S.; Man, M.Q. Moisturizers versus current and next-generation barrier repair therapy for the management of atopic dermatitis. Skin Pharmacol. Physiol. 2019, 32, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Luger, T.; Amagai, M.; Dreno, B.; Dagnelie, M.-A.; Liao, W.; Kabashima, K.; Schikowski, T.; Proksch, E.; Elias, P.M.; Simon, M.; et al. Atopic dermatitis: Role of the skin barrier, environment, microbiome, and therapeutic agents. J. Dermatol. Sci. 2021, 102, 142–157. [Google Scholar] [CrossRef]
- Sörensen, A.; Landvall, P.; Lodén, M. Moisturizers as cosmetics, medicines, or medical device? The regulatory demands in the European Union. In Treatment of dry Skin Syndrome; Springer: Berlin/Heidelberg, Germany, 2011; Volume 8, pp. 3–16. [Google Scholar]
- Wananukul, S.; Chatproedprai, S.; Chunharas, A.; Limpongsanuruk, W.; Singalavanija, S.; Nitiyarom, R.; Wisuthsarewong, W. Randomized, double-blind, split-side, comparison study of moisturizer containing licochalcone A and 1% hydrocortisone in the treatment of childhood atopic dermatitis. J. Med. Assoc. Thai. 2013, 96, 1135–1142. [Google Scholar]
- Nakahara, T.; Kido-Nakahara, M.; Tsuji, G.; Furue, M. Basics and recent advances in the pathophysiology of atopic dermatitis. J. Dermatol. 2021, 48, 130–139. [Google Scholar] [CrossRef] [PubMed]
- Bønnelykke, K.; Sparks, R.; Waage, J.; Milner, J.D. Genetics of allergy and allergic sensitization: Common variants, rare mutations. Curr. Opin. Immunol. 2015, 36, 115–126. [Google Scholar] [CrossRef]
- Eyerich, K.; Novak, N. Immunology of atopic eczema: Overcoming the Th1/Th2 paradigm. Allergy 2013, 68, 974–982. [Google Scholar] [CrossRef]
- Jang, H.; Matsuda, A.; Jung, K.; Karasawa, K.; Matsuda, K.; Oida, K.; Ishizaka, S.; Ahn, G.; Amagai, Y.; Moon, C.; et al. Skin pH Is the master switch of kallikrein 5-mediated skin barrier destruction in a murine atopic dermatitis model. J. Investig. Dermatol. 2016, 136, 127–135. [Google Scholar] [CrossRef]
- Zhu, Y.; Underwood, J.; Macmillan, D.; Shariff, L.; O’Shaughnessy, R.; Harper, J.I.; Pickard, C.; Friedmann, P.S.; Healy, E.; Di, W.L. Persistent kallikrein 5 activation induces atopic dermatitis-like skin architecture independent of PAR2 activity. J. Allergy Clin. Immunol. 2017, 140, 1310–1322.e1315. [Google Scholar] [CrossRef]
- Basu, M.N.; Mortz, C.G.; Jensen, T.K.; Barington, T.; Halken, S. Natural moisturizing factors in children with and without eczema: Associations with lifestyle and genetic factors. J. Eur. Acad. Dermatol. Venereol. 2022, 36, 255–262. [Google Scholar] [CrossRef]
- Nouwen, A.E.M.; Karadavut, D.; Pasmans, S.; Elbert, N.J.; Bos, L.D.N.; Nijsten, T.E.C.; Arends, N.J.T.; Pijnenburg, M.W.H.; Koljenović, S.; Puppels, G.J.; et al. Natural moisturizing factor as a clinical marker in atopic dermatitis. Allergy 2020, 75, 188–190. [Google Scholar] [CrossRef] [PubMed]
- Yang, G.; Seok, J.K.; Kang, H.C.; Cho, Y.Y.; Lee, H.S.; Lee, J.Y. Skin barrier abnormalities and immune dysfunction in atopic dermatitis. Int. J. Mol. Sci. 2020, 21, 2867. [Google Scholar] [CrossRef] [PubMed]
- Kantor, R.; Silverberg, J.I. Environmental risk factors and their role in the management of atopic dermatitis. Expert Rev. Clin. Immunol. 2017, 13, 15–26. [Google Scholar] [CrossRef] [PubMed]
- Chamlin, S.L.; Kao, J.; Frieden, I.J.; Sheu, M.Y.; Fowler, A.J.; Fluhr, J.W.; Williams, M.L.; Elias, P.M. Ceramide-dominant barrier repair lipids alleviate childhood atopic dermatitis: Changes in barrier function provide a sensitive indicator of disease activity. J. Am. Acad. Dermatol. 2002, 47, 198–208. [Google Scholar] [CrossRef]
- Koppes, S.A.; Brans, R.; Ljubojevic Hadzavdic, S.; Frings-Dresen, M.H.; Rustemeyer, T.; Kezic, S. Stratum corneum tape stripping: Monitoring of inflammatory mediators in atopic dermatitis patients using topical therapy. Int. Arch. Allergy Immunol. 2016, 170, 187–193. [Google Scholar] [CrossRef]
- Somjorn, P.; Kamanamool, N.; Kanokrungsee, S.; Rojhirunsakool, S.; Udompataikul, M. A cream containing linoleic acid, 5% dexpanthenol and ceramide in the treatment of atopic dermatitis. Asian Pac. J. Allergy Immunol. 2021. [Google Scholar] [CrossRef]
- Iwamoto, K.; Moriwaki, M.; Miyake, R.; Hide, M. Staphylococcus aureus in atopic dermatitis: Strain-specific cell wall proteins and skin immunity. Allergol. Int. 2019, 68, 309–315. [Google Scholar] [CrossRef]
- Williams, M.R.; Gallo, R.L. The role of the skin microbiome in atopic dermatitis. Curr. Allergy Asthma Rep. 2015, 15, 65. [Google Scholar] [CrossRef]
- Yamazaki, Y.; Nakamura, Y.; Núñez, G. Role of the microbiota in skin immunity and atopic dermatitis. Allergol Int. 2017, 66, 539–544. [Google Scholar] [CrossRef]
- Byrd, A.L.; Belkaid, Y.; Segre, J.A. The human skin microbiome. Nat. Rev. Microbiol. 2018, 16, 143–155. [Google Scholar] [CrossRef]
- Kong, H.H.; Oh, J.; Deming, C.; Conlan, S.; Grice, E.A.; Beatson, M.A.; Nomicos, E.; Polley, E.C.; Komarow, H.D.; Murray, P.R.; et al. Temporal shifts in the skin microbiome associated with disease flares and treatment in children with atopic dermatitis. Genome Res. 2012, 22, 850–859. [Google Scholar] [CrossRef] [PubMed]
- Eberlein-König, B.; Schäfer, T.; Huss-Marp, J.; Darsow, U.; Möhrenschlager, M.; Herbert, O.; Abeck, D.; Krämer, U.; Behrendt, H.; Ring, J. Skin surface pH, stratum corneum hydration, trans-epidermal water loss and skin roughness related to atopic eczema and skin dryness in a population of primary school children. Acta Derm. Venereol. 2000, 80, 188–191. [Google Scholar] [CrossRef] [PubMed]
- Surber, C.; Humbert, P.; Abels, C.; Maibach, H. The acid mantle: A myth or an essential part of skin health? Curr. Probl. Dermatol. 2018, 54, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Lukić, M.; Pantelić, I.; Savić, S.D. Towards optimal pH of the skin and topical formulations: From the current state of the art to tailored products. Cosmetics 2021, 8, 69. [Google Scholar] [CrossRef]
- Karna, R.V. The investigation on correlation between pH and the likelihood of developing atopic dermatitis on paediatrics and adults population in Indonesia. In Proceedings of the Asian Australasian Regional Conference of Dermatology, Surabaya, Indonesia, 8–11 August 2018. [Google Scholar]
- Sparavigna, A.; Setaro, M.; Gualandri, V. Cutaneous pH in children affected by atopic dermatitis and in healthy children: A multicenter study. Skin Res. Technol. 1999, 5, 221–227. [Google Scholar] [CrossRef]
- Panther, D.J.; Jacob, S.E. The importance of acidification in atopic eczema: An underexplored avenue for treatment. J. Clin. Med. 2015, 4, 970–978. [Google Scholar] [CrossRef]
- Gupta, J.; Margolis, D.J. Filaggrin gene mutations with special reference to atopic dermatitis. Curr. Treat. Options Allergy 2020, 7, 403–413. [Google Scholar] [CrossRef]
- Gunnarsson, M.; Mojumdar, E.H.; Topgaard, D.; Sparr, E. Extraction of natural moisturizing factor from the stratum corneum and its implication on skin molecular mobility. J. Colloid Interface Sci. 2021, 604, 480–491. [Google Scholar] [CrossRef]
- Maeno, K. Direct quantification of natural moisturizing factors in stratum corneum using direct analysis in real time mass spectrometry with inkjet-printing technique. Sci. Rep. 2019, 9, 17789. [Google Scholar] [CrossRef]
- van Zuuren, E.J.; Fedorowicz, Z.; Christensen, R.; Lavrijsen, A.; Arents, B.W.M. Emollients and moisturisers for eczema. Cochrane Database Syst. Rev. 2017, 2, CD012119. [Google Scholar] [CrossRef]
- Xu, S.; Kwa, M.; Lohman, M.E.; Evers-Meltzer, R.; Silverberg, J.I. Consumer Preferences, Product Characteristics, and Potentially Allergenic Ingredients in Best-selling Moisturizers. JAMA Dermatol. 2017, 153, 1099–1105. [Google Scholar] [CrossRef] [PubMed]
- Draelos, Z.D. The science behind skin care: Moisturizers. J. Cosmet. Dermatol. 2018, 17, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Shi, V.Y.; Tran, K.; Lio, P.A. A comparison of physicochemical properties of a selection of modern moisturizers: Hydrophilic index and pH. J. Drugs Dermatol. 2012, 11, 633–636. [Google Scholar] [PubMed]
- Pinter, A.; Thouvenin, M.-D.; Bacquey, A.; Rossi, A.B.; Nocera, T. Tolerability and efficacy of a medical device repairing emollient cream in children and adults with mild to moderate atopic dermatitis. Dermatol. Ther. 2019, 9, 309–319. [Google Scholar] [CrossRef] [PubMed]
- Rossi, A.B.; Bacquey, A.; Nocera, T.; Thouvenin, M.D. Efficacy and tolerability of a medical device repairing emollient cream associated with a topical corticosteroid in adults with atopic dermatitis: An open-label, intra-individual randomized controlled study. Dermatol. Ther. 2018, 8, 217–228. [Google Scholar] [CrossRef]
- European Commission. Medical devices: Guidance Document—Classification of Medical Devices; European Commission: Brussels, Belgium, 2010. [Google Scholar]
- Abramovits, W.; Boguniewicz, M. A multicenter, randomized, vehicle-controlled clinical study to examine the efficacy and safety of MAS063DP (Atopiclair) in the management of mild to moderate atopic dermatitis in adults. J. Drugs Dermatol. 2006, 5, 236–244. [Google Scholar]
- Abramovits, W.; Hebert, A.; Boguniewicz, M.; Kempers, S.; Tschen, E.; Jarratt, M.; Lucky, A.; Cornelison, R.; Swinyer, L.; Jones, T. Patient-reported outcomes from a multicenter, randomized, vehicle-controlled clinical study of MAS063DP (Atopiclair™) in the management of mild-to-moderate atopic dermatitis in adults. J. Dermatol. Treat. 2008, 19, 327–332. [Google Scholar] [CrossRef]
- Boguniewicz, M.; Zeichner, J.A.; Eichenfield, L.F.; Hebert, A.A.; Jarratt, M.; Lucky, A.W.; Paller, A.S. MAS063DP is effective monotherapy for mild to moderate atopic dermatitis in infants and children: A multicenter, randomized, vehicle-controlled study. J. Pediatr. 2008, 152, 854–859. [Google Scholar] [CrossRef]
- Bomstein, Y.; Rozenblat, S. Treatment of atopic dermatitis with KAM-3008, a barrier-based, non-steroidal topical cream. J. Dermatolog. Treat. 2015, 26, 426–430. [Google Scholar] [CrossRef]
- Kowalska, A.; Kalinowska-Lis, U. 18β-Glycyrrhetinic acid: Its core biological properties and dermatological applications. Int. J. Cosmet. Sci. 2019, 41, 325–331. [Google Scholar] [CrossRef]
- Patrizi, A.; Capitanio, B.; Neri, I.; Giacomini, F.; Sinagra, J.; Raone, B.; Berardesca, E. A double-blind, randomized, vehicle-controlled clinical study to evaluate the efficacy and safety of MAS063DP (ATOPICLAIR) in the management of atopic dermatitis in paediatric patients. Pediatr. Allergy Immunol. 2008, 19, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Saeedi, M.; Morteza-Semnani, K.; Ghoreishi, M.R. The treatment of atopic dermatitis with licorice gel. J. Dermatolog. Treat. 2003, 14, 153–157. [Google Scholar] [CrossRef] [PubMed]
- Seiwerth, J.; Tasiopoulou, G.; Hoffmann, J.; Wölfle, U.; Schwabe, K.; Quirin, K.W.; Schempp, C.M. Anti-inflammatory effect of a novel topical herbal composition (VEL-091604) consisting of gentian root, licorice root and willow bark extract. Planta Med. 2019, 85, 608–614. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Zhang, Y.; Peng, G.; Han, X. Glycyrrhizin ameliorates atopic dermatitis-like symptoms through inhibition of HMGB1. Int. Immunopharmacol. 2018, 60, 9–17. [Google Scholar] [CrossRef] [PubMed]
- Angelova-Fischer, I.; Neufang, G.; Jung, K.; Fischer, T.W.; Zillikens, D. A randomized, investigator-blinded efficacy assessment study of stand-alone emollient use in mild to moderately severe atopic dermatitis flares. J. Eur. Acad. Dermatol. Venereol. 2014, 28 (Suppl. 3), 9–15. [Google Scholar] [CrossRef] [PubMed]
- Angelova-Fischer, I.; Rippke, F.; Richter, D.; Filbry, A.; Arrowitz, C.; Weber, T.; Fischer, T.W.; Zillikens, D. Stand-alone emollient treatment reduces flares after discontinuation of topical steroid treatment in atopic dermatitis: A double-blind, randomized, vehicle-controlled, left-right comparison study. Acta. Derm. Venereol. 2018, 98, 517–523. [Google Scholar] [CrossRef]
- Udompataikul, M.; Srisatwaja, W. Comparative trial of moisturizer containing licochalcone A vs. hydrocortisone lotion in the treatment of childhood atopic dermatitis: A pilot study. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 660–665. [Google Scholar] [CrossRef]
- Ashfaq, U.A.; Masoud, M.S.; Nawaz, Z.; Riazuddin, S. Glycyrrhizin as antiviral agent against Hepatitis C Virus. J. Transl. Med. 2011, 9, 112. [Google Scholar] [CrossRef]
- Morinaga, O.; Ishiuchi, K.I.; Ohkita, T.; Tian, C.; Hirasawa, A.; Mitamura, M.; Maki, Y.; Yasujima, T.; Yuasa, H.; Makino, T. Isolation of a novel glycyrrhizin metabolite as a causal candidate compound for pseudoaldosteronism. Sci. Rep. 2018, 8, 15568. [Google Scholar] [CrossRef]
- do Nascimento, M.H.M.; de Araújo, D.R. Exploring the pharmacological potential of glycyrrhizic acid: From therapeutic applications to trends in nanomedicine. Future Pharmacol. 2022, 2, 1–15. [Google Scholar] [CrossRef]
- Nokhodchi, A.; Nazemiyeh, H.; Ghafourian, T.; Hassan-Zadeh, D.; Valizadeh, H.; Bahary, L.A. The effect of glycyrrhizin on the release rate and skin penetration of diclofenac sodium from topical formulations. Farmaco 2002, 57, 883–888. [Google Scholar] [CrossRef]
- Teelucksingh, S.; Mackie, A.D.; Burt, D.; McIntyre, M.A.; Brett, L.; Edwards, C.R. Potentiation of hydrocortisone activity in skin by glycyrrhetinic acid. Lancet 1990, 335, 1060–1063. [Google Scholar] [CrossRef]
- Kim, J.-E.; Yoon, G.; Shim, J.-H.; Cho, S.-S. Broad spectrum antimicrobial activity of licochalcones A and E against MDR (Multidrug Resistant) strains of clinical origin. Nat. Prod. Commun. 2017, 12, 1747–1748. [Google Scholar] [CrossRef]
- Yadav, V.R.; Prasad, S.; Sung, B.; Aggarwal, B.B. The role of chalcones in suppression of NF-κB-mediated inflammation and cancer. Int. Immunopharmacol. 2011, 11, 295–309. [Google Scholar] [CrossRef]
- Chen, M.F.; Shimada, F.; Kato, H.; Yano, S.; Kanaoka, M. Effect of glycyrrhizin on the pharmacokinetics of prednisolone following low dosage of prednisolone hemisuccinate. Endocrinol. Jpn. 1990, 37, 331–341. [Google Scholar] [CrossRef]
- MacKenzie, M.A.; Hoefnagels, W.H.; Kloppenborg, P.W. Glycyrrhetinic acid and potentiation of hydrocortisone activity in skin. Lancet 1990, 335, 1534. [Google Scholar] [CrossRef]
- Sigurjónsdóttir, H.A.; Franzson, L.; Manhem, K.; Ragnarsson, J.; Sigurdsson, G.; Wallerstedt, S. Liquorice-induced rise in blood pressure: A linear dose-response relationship. J. Hum. Hypertens. 2001, 15, 549–552. [Google Scholar] [CrossRef] [PubMed]
- Dawid-Pać, R. Medicinal plants used in treatment of inflammatory skin diseases. Postepy Dermatol. Alergol. 2013, 30, 170–177. [Google Scholar] [CrossRef]
- Lee, S.H.; Heo, Y.; Kim, Y.C. Effect of German chamomile oil application on alleviating atopic dermatitis-like immune alterations in mice. J. Vet. Sci. 2010, 11, 35–41. [Google Scholar] [CrossRef]
- Ortiz-Bautista, R.J.; García-González, L.L.; Ocádiz-González, M.A.; Flores-Tochihuitl, J.; García-Villaseñor, A.; González-Hernández, M.; Muñoz-Hernández, L.; Ortiz-Figueroa, M.C.; Ramírez-Anaya, M.; Reyna-Téllez, S.; et al. Matricaria chamomilla (aqueous extract) improves atopic dermatitis-like lesions in a murine model. Rev. Med. Inst. Mex. Seguro Soc. 2017, 55, 587–593. [Google Scholar]
- Wang, W.; Wang, Y.; Zou, J.; Jia, Y.; Wang, Y.; Li, J.; Wang, C.; Sun, J.; Guo, D.; Wang, F.; et al. The mechanism action of German chamomile (Matricaria recutita L.) in the treatment of eczema: Based on dose-effect weight coefficient network pharmacology. Front. Pharmacol. 2021, 12, 706836. [Google Scholar] [CrossRef] [PubMed]
- Aertgeerts, P.; Albring, M.; Klaschka, F.; Nasemann, T.; Patzelt-Wenczler, R.; Rauhut, K.; Weigl, B. Comparative testing of Kamillosan cream and steroidal (0.25% hydrocortisone, 0.75% fluocortin butyl ester) and non-steroidal (5% bufexamac) dermatologic agents in maintenance therapy of eczematous diseases. Z. Hautkr. 1985, 60, 270–277. [Google Scholar] [PubMed]
- Patzelt-Wenczler, R.; Ponce-Pöschl, E. Proof of efficacy of Kamillosan(R) cream in atopic eczema. Eur. J. Med. Res. 2000, 5, 171–175. [Google Scholar]
- Kadir, R.; Barry, B.W. α-Bisabolol, a possible safe penetration enhancer for dermal and transdermal therapeutics. Int. J. Pharm. 1991, 70, 87–94. [Google Scholar] [CrossRef]
- Kamatou, G.P.P.; Viljoen, A.M. A review of the application and pharmacological properties of α-bisabolol and α-bisabolol-rich oils. J. Am. Oil Chem. Soc. 2010, 87, 1–7. [Google Scholar] [CrossRef]
- Arenberger, P.; Arenbergerová, M.; Drozenová, H.; Hladíková, M.; Holcová, S. Effect of topical heparin and levomenol on atopic dermatitis: A randomized four-arm, placebo-controlled, double-blind clinical study. J. Eur. Acad. Dermatol. Venereol. 2011, 25, 688–694. [Google Scholar] [CrossRef]
- Bocchietto, E.; Pecis, L.; Lisi, P.; Angelini, G.; Ayala, F.; Balato, N.; Bonamonte, D.; Camplone, G.; Fabrizi, G.; Marzatico, F.; et al. Furfuryl palmitate: A new topical anti-oxidant effective in the treatment of dermatitis with eczema. G. Ital. Dermatol. Venereol. 2002, 137, 1–13. [Google Scholar]
- Grassi, A.; Palermi, G.; Paradisi, M. Study of tolerance and efficacy of cosmetic preparations with lenitive action in atopic dermatitis in children. Clin. Ter. 2000, 151, 77–80. [Google Scholar]
- Licari, A.; Ruffinazzi, G.M.D.E.F.; Castagnoli, R.; Marseglia, A.; Agostinis, F.; Puviani, M.; Milani, M.; Marseglia, G.L. A starch, glycyrretinic, zinc oxide and bisabolol based cream in the treatment of chronic mild-to-moderate atopic dermatitis in children: A three-center, assessor blinded trial. Minerva Pediatr. 2017, 69, 470–475. [Google Scholar] [CrossRef]
- Marini, A.; Reinelt, K.; Krutmann, J.; Bilstein, A. Ectoine-containing cream in the treatment of mild to moderate atopic dermatitis: A randomised, comparator-controlled, intra-individual double-blind, multi-center trial. Skin Pharmacol. Physiol. 2014, 27, 57–65. [Google Scholar] [CrossRef]
- Nemelka, O.; Bleidel, D.; Fabrizi, G.; Camplone, G.; Occella, C.; Marzatico, F.; Pecis, L.; Bocchietto, E. Experimental survey of a new topical anti-oxidant based on furfuryl palmitate in the treatment of child’s and baby’s dermatitis with eczema: Results from a multicenter clinical investigation. Minerva Pediatr. 2002, 54, 465–474. [Google Scholar] [PubMed]
- Srivastava, J.K.; Shankar, E.; Gupta, S. Chamomile: A herbal medicine of the past with bright future. Mol. Med. Rep. 2010, 3, 895–901. [Google Scholar] [CrossRef] [PubMed]
- Jacob, S.E.; Matiz, C.; Herro, E.M. Compositae-associated allergic contact dermatitis from bisabolol. Dermatitis 2011, 22, 102–105. [Google Scholar] [CrossRef] [PubMed]
- Hausen, B.M. A 6-year experience with compositae mix. Am. J. Contact Dermat. 1996, 7, 94–99. [Google Scholar] [PubMed]
- Horinouchi, C.D.; Otuki, M.F. Botanical briefs: Comfrey (Symphytum officinale). Cutis 2013, 91, 225–228. [Google Scholar]
- Salehi, B.; Sharopov, F.; Boyunegmez Tumer, T.; Ozleyen, A.; Rodríguez-Pérez, C.M.; Ezzat, S.; Azzini, E.; Hosseinabadi, T.; Butnariu, M.; Sarac, I.; et al. Symphytum species: A comprehensive review on chemical composition, food applications and phytopharmacology. Molecules 2019, 24, 2272. [Google Scholar] [CrossRef]
- Staiger, C. Comfrey root: From tradition to modern clinical trials. Wien. Med. Wochenschr. 2013, 163, 58–64. [Google Scholar] [CrossRef]
- Brown, A.W.; Stegelmeier, B.L.; Colegate, S.M.; Gardner, D.R.; Panter, K.E.; Knoppel, E.L.; Hall, J.O. The comparative toxicity of a reduced, crude comfrey (Symphytum officinale) alkaloid extract and the pure, comfrey-derived pyrrolizidine alkaloids, lycopsamine and intermedine in chicks (Gallus gallus domesticus). J. Appl. Toxicol. 2016, 36, 716–725. [Google Scholar] [CrossRef]
- Mazzocchi, A.; Montanaro, F. Observational study of the use of Symphytum 5CH in the management of pain and swelling after dental implant surgery. Homeopathy 2012, 101, 211–216. [Google Scholar] [CrossRef]
- Mei, N.; Guo, L.; Fu, P.P.; Fuscoe, J.C.; Luan, Y.; Chen, T. Metabolism, genotoxicity, annd carcinogenicity of comfrey. J. Toxicol. Environ. Health-B: Crit. Rev. 2010, 13, 509–526. [Google Scholar] [CrossRef]
- Jedlinszki, N.; Balázs, B.; Csányi, E.; Csupor, D. Penetration of lycopsamine from a comfrey ointment through human epidermis. Regul. Toxicol. Pharmacol. 2017, 83, 1–4. [Google Scholar] [CrossRef]
- Kuchta, K.; Schmidt, M. Safety of medicinal comfrey cream preparations (Symphytum officinale s.l.): The pyrrolizidine alkaloid lycopsamine is poorly absorbed through human skin. Regul. Toxicol. Pharmacol. 2020, 118, 104784. [Google Scholar] [CrossRef] [PubMed]
- Koll, R.; Buhr, M.; Dieter, R.; Pabst, H.; Predel, H.G.; Petrowicz, O.; Giannetti, B.; Klingenburg, S.; Staiger, C. Efficacy and tolerance of a comfrey root extract (Extr. Rad. Symphyti) in the treatment of ankle distorsions: Results of a multicenter, randomized, placebo-controlled, double-blind study. Phytomedicine 2004, 11, 470–477. [Google Scholar] [CrossRef] [PubMed]
- Kucera, M.; Barna, M.; Horácek, O.; Kováriková, J.; Kucera, A. Efficacy and safety of topically applied Symphytum herb extract cream in the treatment of ankle distortion: Results of a randomized controlled clinical double blind study. Wien. Med. Wochenschr. 2004, 154, 498–507. [Google Scholar] [CrossRef]
- Predel, H.G.; Giannetti, B.; Koll, R.; Bulitta, M.; Staiger, C. Efficacy of a comfrey root extract ointment in comparison to a diclofenac gel in the treatment of ankle distortions: Results of an observer-blind, randomized, multicenter study. Phytomedicine 2005, 12, 707–714. [Google Scholar] [CrossRef]
- Araújo, L.U.; Grabe-Guimarães, A.; Mosqueira, V.C.; Carneiro, C.M.; Silva-Barcellos, N.M. Profile of wound healing process induced by allantoin. Acta Cir. Bras. 2010, 25, 460–466. [Google Scholar] [CrossRef] [PubMed]
- Lee, M.Y.; Lee, N.H.; Jung, D.; Lee, J.A.; Seo, C.S.; Lee, H.; Kim, J.H.; Shin, H.K. Protective effects of allantoin against ovalbumin (OVA)-induced lung inflammation in a murine model of asthma. Int. Immunopharmacol. 2010, 10, 474–480. [Google Scholar] [CrossRef] [PubMed]
- Ma, L.; Li, P.; Tang, J.; Guo, Y.; Shen, C.; Chang, J.; Kerrouche, N. Prolonging time to flare in pediatric atopic dermatitis: A randomized, investigator-blinded, controlled, multicenter clinical study of a ceramide-containing moisturizer. Adv. Ther. 2017, 34, 2601–2611. [Google Scholar] [CrossRef] [PubMed]
- Seghers, A.C.; Cai, S.C.; Ho, M.S.; Giam, Y.C.; Tan, L.; Grönhagen, C.M.; Tang, M.B. Evaluation of a pseudoceramide moisturizer in patients with mild-to-moderate atopic dermatitis. Dermatol. Ther. 2014, 4, 83–92. [Google Scholar] [CrossRef][Green Version]
- Luo, C.; Zou, L.; Sun, H.; Peng, J.; Gao, C.; Bao, L.; Ji, R.; Jin, Y.; Sun, S. A review of the anti-inflammatory effects of rosmarinic acid on inflammatory diseases. Front. Pharmacol. 2020, 11, 153. [Google Scholar] [CrossRef]
- Zhou, M.W.; Jiang, R.H.; Kim, K.D.; Lee, J.H.; Kim, C.D.; Yin, W.T.; Lee, J.H. Rosmarinic acid inhibits poly(I:C)-induced inflammatory reaction of epidermal keratinocytes. Life Sci. 2016, 155, 189–194. [Google Scholar] [CrossRef] [PubMed]
- Jang, A.H.; Kim, T.H.; Kim, G.D.; Kim, J.E.; Kim, H.J.; Kim, S.S.; Jin, Y.H.; Park, Y.S.; Park, C.S. Rosmarinic acid attenuates 2,4-dinitrofluorobenzene-induced atopic dermatitis in NC/Nga mice. Int. Immunopharmacol. 2011, 11, 1271–1277. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Jung, E.; Koh, J.; Kim, Y.S.; Park, D. Effect of rosmarinic acid on atopic dermatitis. J. Dermatol. 2008, 35, 768–771. [Google Scholar] [CrossRef] [PubMed]
- Ilnytska, O.; Kaur, S.; Chon, S.; Reynertson, K.; Nebus, J.; Garay, M.; Mahmood, K.; Southall, M. Colloidal oatmeal (Avena Sativa) improves skin barrier through multi-therapy activity. J. Drugs Dermatol. 2016, 15, 684–690. [Google Scholar]
- Lisante, T.A.; Nuñez, C.; Zhang, P. Efficacy and safety of an over-the-counter 1% colloidal oatmeal cream in the management of mild to moderate atopic dermatitis in children: A double-blind, randomized, active-controlled study. J. Dermatol. Treat. 2017, 28, 659–667. [Google Scholar] [CrossRef]
- Lisante, T.A.; Nunez, C.; Zhang, P.; Mathes, B.M. A 1% colloidal oatmeal cream alone is effective in reducing symptoms of mild to moderate atopic dermatitis: Results from two clinical studies. J. Drugs Dermatol. 2017, 16, 671–676. [Google Scholar] [PubMed]
- Celleno, L. Topical urea in skincare: A review. Dermatol. Ther. 2018, 31, e12690. [Google Scholar] [CrossRef]
- Pan, M.; Heinecke, G.; Bernardo, S.; Tsui, C.; Levitt, J. Urea: A comprehensive review of the clinical literature. Dermatol. Online J. 2013, 19, 20392. [Google Scholar] [CrossRef]
- Sasaki, Y.; Tadaki, T.; Tagami, H. The effects of a topical application of urea cream on the function of pathological stratum corneum. Acta Dermatol. Kyoto 1989, 84, 581–586. [Google Scholar]
- Almeyda, J.; Burt, B.W. Double blind controlled study of treatment of atopic eczema with a preparation of hydrocortisone in a new drug delivery system versus betamethasone 17-valerate. Br. J. Dermatol. 1974, 91, 579–583. [Google Scholar] [CrossRef]
- Jacoby, R.H.; Gilkes, J.J. A new urea/hydrocortisone powder-cream compared with other topical corticosteroid preparations: A six-centre study. Curr. Med. Res. Opin. 1974, 2, 474–481. [Google Scholar] [CrossRef] [PubMed]
- Roth, H. Atopic Dermatitis: Treatment with a urea-corticosteriod cream. Cutis 1973, 11, 237–239. [Google Scholar]
- Nistico, S.P.; Del Duca, E.; Tamburi, F.; Pignataro, E.; De Carvalho, N.; Farnetani, F.; Pellacani, G. Superiority of a vitamin B12-barrier cream compared with standard glycerol-petrolatum-based emollient cream in the treatment of atopic dermatitis: A randomized, left-to-right comparative trial. Dermatol. Ther. 2017, 30, e12523. [Google Scholar] [CrossRef] [PubMed]
- de Lucas, R.; García-Millán, C.; Pérez-Davó, A.; Moreno, E.; Redondo, P. New cosmetic formulation for the treatment of mild to moderate infantile atopic dermatitis. Children 2019, 6, 17. [Google Scholar] [CrossRef]
- Hoppe, T.; Winge, M.C.; Bradley, M.; Nordenskjöld, M.; Vahlquist, A.; Törmä, H.; Berne, B. Moisturizing treatment of patients with atopic dermatitis and ichthyosis vulgaris improves dry skin, but has a modest effect on gene expression regardless of FLG genotype. J. Eur. Acad. Dermatol. Venereol. 2015, 29, 174–177. [Google Scholar] [CrossRef]
- Bianchi, P.; Theunis, J.; Casas, C.; Villeneuve, C.; Patrizi, A.; Phulpin, C.; Bacquey, A.; Redoulès, D.; Mengeaud, V.; Schmitt, A.M. Effects of a new emollient-based treatment on skin microflora balance and barrier function in children with mild atopic dermatitis. Pediatr. Dermatol. 2016, 33, 165–171. [Google Scholar] [CrossRef]
- Hon, K.L.; Pong, N.H.; Wang, S.S.; Lee, V.W.; Luk, N.M.; Leung, T.F. Acceptability and efficacy of an emollient containing ceramide-precursor lipids and moisturizing factors for atopic dermatitis in pediatric patients. Drugs R D 2013, 13, 37–42. [Google Scholar] [CrossRef]
- Spada, F.; Harrison, I.P.; Barnes, T.M.; Greive, K.A.; Daniels, D.; Townley, J.P.; Mostafa, N.; Fong, A.T.; Tong, P.L.; Shumack, S. A daily regimen of a ceramide-dominant moisturizing cream and cleanser restores the skin permeability barrier in adults with moderate eczema: A randomized trial. Dermatol. Ther. 2021, 34, e14970. [Google Scholar] [CrossRef]
- Cork, M.J.; Britton, J.; Butler, L.; Young, S.; Murphy, R.; Keohane, S.G. Comparison of parent knowledge, therapy utilization and severity of atopic eczema before and after explanation and demonstration of topical therapies by a specialist dermatology nurse. Br. J. Dermatol. 2003, 149, 582–589. [Google Scholar] [CrossRef]
- Sugarman, J.L.; Parish, L.C. Efficacy of a lipid-based barrier repair formulation in moderate-to-severe pediatric atopic dermatitis. J. Drugs Dermatol. 2009, 8, 1106–1111. [Google Scholar]
- Lee, Y.B.; Park, H.J.; Kwon, M.J.; Jeong, S.K.; Cho, S.H. Beneficial effects of pseudoceramide-containing physiologic lipid mixture as a vehicle for topical steroids. Eur. J. Dermatol. 2011, 21, 710–716. [Google Scholar] [CrossRef] [PubMed]
- McClanahan, D.; Wong, A.; Kezic, S.; Samrao, A.; Hajar, T.; Hill, E.; Simpson, E.L. A randomized controlled trial of an emollient with ceramide and filaggrin-associated amino acids for the primary prevention of atopic dermatitis in high-risk infants. J. Eur. Acad. Dermatol. Venereol. 2019, 33, 2087–2094. [Google Scholar] [CrossRef] [PubMed]
- Kircik, L.H.; Del Rosso, J.Q.; Aversa, D. Evaluating clinical use of a ceramide-dominant, physiologic lipid-based topical emulsion for atopic dermatitis. J. Clin. Aesthet. Dermatol. 2011, 4, 34–40. [Google Scholar] [PubMed]
- Man, M.M.; Feingold, K.R.; Thornfeldt, C.R.; Elias, P.M. Optimization of physiological lipid mixtures for barrier repair. J. Investig. Dermatol. 1996, 106, 1096–1101. [Google Scholar] [CrossRef]
- Mao-Qiang, M.; Elias, P.M.; Feingold, K.R. Fatty acids are required for epidermal permeability barrier function. J. Clin. Investig. 1993, 92, 791–798. [Google Scholar] [CrossRef]
- Avila, C.; Massick, S.; Kaffenberger, B.H.; Kwatra, S.G.; Bechtel, M. Cannabinoids for the treatment of chronic pruritus: A review. J. Am. Acad. Dermatol. 2020, 82, 1205–1212. [Google Scholar] [CrossRef]
- Eagleston, L.R.M.; Kalani, N.K.; Patel, R.R.; Flaten, H.K.; Dunnick, C.A.; Dellavalle, R.P. Cannabinoids in dermatology: A scoping review. Dermatol. Online J. 2018, 24, 13030/qt7pn8c0sb. [Google Scholar] [CrossRef]
- Sheriff, T.; Lin, M.J.; Dubin, D.; Khorasani, H. The potential role of cannabinoids in dermatology. J. Dermatol. Treat. 2020, 31, 839–845. [Google Scholar] [CrossRef]
- Sivesind, T.E.; Maghfour, J.; Rietcheck, H.; Kamel, K.; Malik, A.S.; Dellavalle, R.P. Cannabinoids for the treatment of dermatologic conditions. JID Innov. 2022, 2, 100095. [Google Scholar] [CrossRef]
- Tóth, K.F.; Ádám, D.; Bíró, T.; Oláh, A. Cannabinoid signaling in the skin: Therapeutic potential of the “c(ut)annabinoid” system. Molecules 2019, 24, 918. [Google Scholar] [CrossRef]
- Muller, C.; Morales, P.; Reggio, P.H. Cannabinoid ligands targeting TRP channels. Front. Mol. Neurosci. 2018, 11, 487. [Google Scholar] [CrossRef] [PubMed]
- Kim, H.J.; Kim, B.; Park, B.M.; Jeon, J.E.; Lee, S.H.; Mann, S.; Ahn, S.K.; Hong, S.-P.; Jeong, S.K. Topical cannabinoid receptor 1 agonist attenuates the cutaneous inflammatory responses in oxazolone-induced atopic dermatitis model. Int. J. Dermatol. 2015, 54, e401–e408. [Google Scholar] [CrossRef] [PubMed]
- Maekawa, T.; Nojima, H.; Kuraishi, Y.; Aisaka, K. The cannabinoid CB2 receptor inverse agonist JTE-907 suppresses spontaneous itch-associated responses of NC mice, a model of atopic dermatitis. Eur. J. Pharmacol. 2006, 542, 179–183. [Google Scholar] [CrossRef] [PubMed]
- Nam, G.; Jeong, S.K.; Park, B.M.; Lee, S.H.; Kim, H.J.; Hong, S.-P.; Kim, B.; Kim, B.-W. Selective cannabinoid receptor-1 agonists regulate mast cell activation in an oxazolone-induced atopic dermatitis model. Ann. Dermatol. 2016, 28, 22–29. [Google Scholar] [CrossRef]
- Petrosino, S.; Verde, R.; Vaia, M.; Allarà, M.; Iuvone, T.; Di Marzo, V. Anti-inflammatory properties of cannabidiol, a nonpsychotropic cannabinoid, in experimental allergic contact dermatitis. J. Pharmacol. Exp. Ther. 2018, 365, 652–663. [Google Scholar] [CrossRef]
- Maghfour, J.; Rundle, C.W.; Rietcheck, H.R.; Dercon, S.; Lio, P.; Mamo, A.; Runion, T.M.; Fernandez, J.; Kahn, J.; Dellavalle, R.P.; et al. Assessing the effects of topical cannabidiol in patients with atopic dermatitis. Dermatol. Online J. 2021, 27, 13030/qt8h50k2vs. [Google Scholar] [CrossRef]
- Palmieri, B.; Laurino, C.; Vadalà, M. A therapeutic effect of CBD-enriched ointment in inflammatory skin diseases and cutaneous scars. Clin. Ter. 2019, 170, e93–e99. [Google Scholar] [CrossRef]
- Eberlein, B.; Eicke, C.; Reinhardt, H.W.; Ring, J. Adjuvant treatment of atopic eczema: Assessment of an emollient containing N-palmitoylethanolamine (ATOPA study). J. Eur. Acad. Dermatol. Venereol. 2008, 22, 73–82. [Google Scholar] [CrossRef]
- Yuan, C.; Wang, X.M.; Guichard, A.; Tan, Y.M.; Qian, C.Y.; Yang, L.J.; Humbert, P. N-palmitoylethanolamine and N-acetylethanolamine are effective in asteatotic eczema: Results of a randomized, double-blind, controlled study in 60 patients. Clin. Interv. Aging 2014, 9, 1163–1169. [Google Scholar] [CrossRef]
- Pigatto, P.D.; Diani, M. Beneficial Effects of Antioxidant Furfuryl Palmitate in Non-pharmacologic Treatments (Prescription Emollient Devices, PEDs) for Atopic Dermatitis and Related Skin Disorders. Dermatol. Ther. 2018, 8, 339–347. [Google Scholar] [CrossRef]
- Ji, H.; Li, X.-K. Oxidative Stress in Atopic Dermatitis. Oxid. Med. Cell. Longev. 2016, 2016, 2721469. [Google Scholar] [CrossRef]
- Sivaranjani, N.; Rao, S.V.; Rajeev, G. Role of reactive oxygen species and antioxidants in atopic dermatitis. J. Clin. Diagn. Res. 2013, 7, 2683–2685. [Google Scholar] [CrossRef] [PubMed]
- Appiani, E.; Ossola, R.; Latch, D.E.; Erickson, P.R.; McNeill, K. Aqueous singlet oxygen reaction kinetics of furfuryl alcohol: Effect of temperature, pH, and salt content. Environ. Sci. Process. Impacts 2017, 19, 507–516. [Google Scholar] [CrossRef]
- Haag, W.R.; Hoigné, J.; Gassman, E.; Braun, A.M. Singlet oxygen in surface waters—Part I: Furfuryl alcohol as a trapping agent. Chemosphere 1984, 13, 631–640. [Google Scholar] [CrossRef]
- Bocchietto, E.; Pecis, L.; Lisi, P.; Angelini, G.; Ayala, F.; Balato, N.; Bonamonte, D.; Camplone, G.; Fabrizi, G.; Marzatico, F.J. Furfuril palmitato: Un nuovo antiossidante topico efficace nel trattamento di dermatiti eczematose. G. Ital. Dermatol. Venereol. 2002, 137, 1–13. [Google Scholar]
- Pigatto, P.D.; Lauriola, M.M.; Vaccari, G. A single-center, randomized, double-blind, perspective, controlled study of efficacy and safety of a furpalmate-containing cream versus vehicle in the treatment of 40 adult patients with mild to moderate atopic dermatitis. In Proceedings of the 20th European Academy of Dermatology and Venereology Congress, Lisbon, Portugal, 20–24 October 2011. [Google Scholar]
- Lauriola, M.M.; Pigatto, P.D.; Pedrelli, V.A. A single-center, randomized, perspective, investigator blinded controlled trial to examine efficacy and safety of a furpalmate cream in comparison to topical corticosteroid in atopic dermatitis of hands of hands of 40 adult patients. In Proceedings of the 20th European Academy of Dermatology and Venereology Congress, Lisbon, Portugal, 20–24 October 2011. [Google Scholar]
- Patrizi, A.; Raone, B.; Raboni, R.; Neri, I. Efficacy and tolerability of a cream containing AR-GG27® (sorbityl furfural palmitate) in the treatment of mild/moderate childhood atopic dermatitis associated with pityriasis alba. A double-blind, placebo-controlled clinical trial. G. Ital. Dermatol. Venereol. 2012, 147, 1–8. [Google Scholar]
- Flacco, M.E.; Manzoli, L.; Boccia, S.; Capasso, L.; Aleksovska, K.; Rosso, A.; Scaioli, G.; De Vito, C.; Siliquini, R.; Villari, P.; et al. Head-to-head randomized trials are mostly industry sponsored and almost always favor the industry sponsor. J. Clin. Epidemiol. 2015, 68, 811–820. [Google Scholar] [CrossRef]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).