
How Can a Community Pursue Equitable Health and Well-Being after a Severe Shock? Ideas from an Exploratory Simulation Model



{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
- Affirm racial justice and full inclusion for all people;
- Strengthen belonging and civic muscle by working across differences, which, in turn, unlocks new assets for concerted action;
- Expand all vital conditions with local stewards in the lead;
- Renew civic life; economic life; and social, emotional, and spiritual life.
2. Materials and Methods
2.1. Extending an Earlier Line of Research
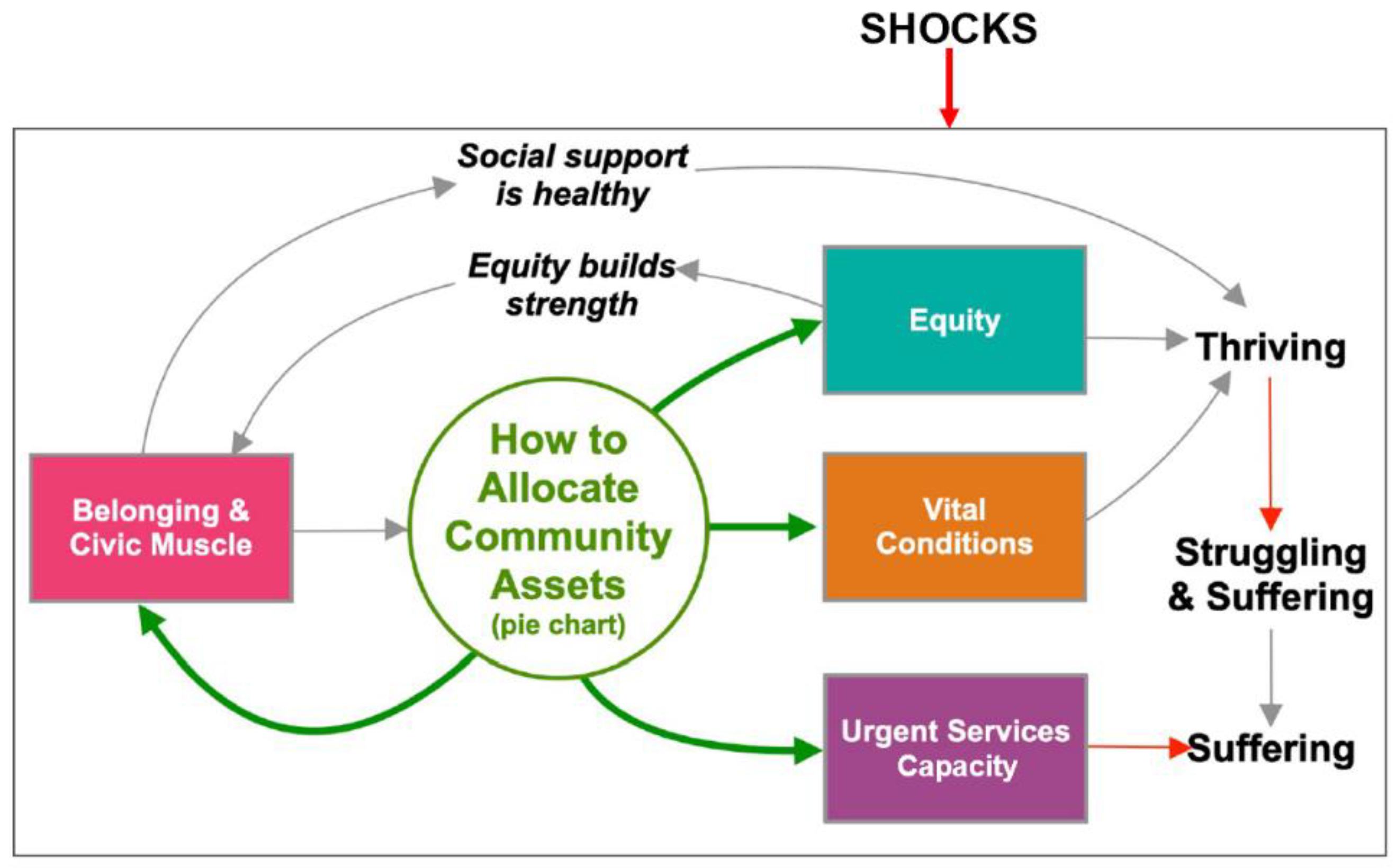
2.2. Representing Well-Being and Its Drivers
2.3. Model Structure
2.4. Gathering Assets
2.5. Allocating Assets
2.6. Parametric Assumptions
2.7. Summary Measures
2.8. Illustrative Model Tests
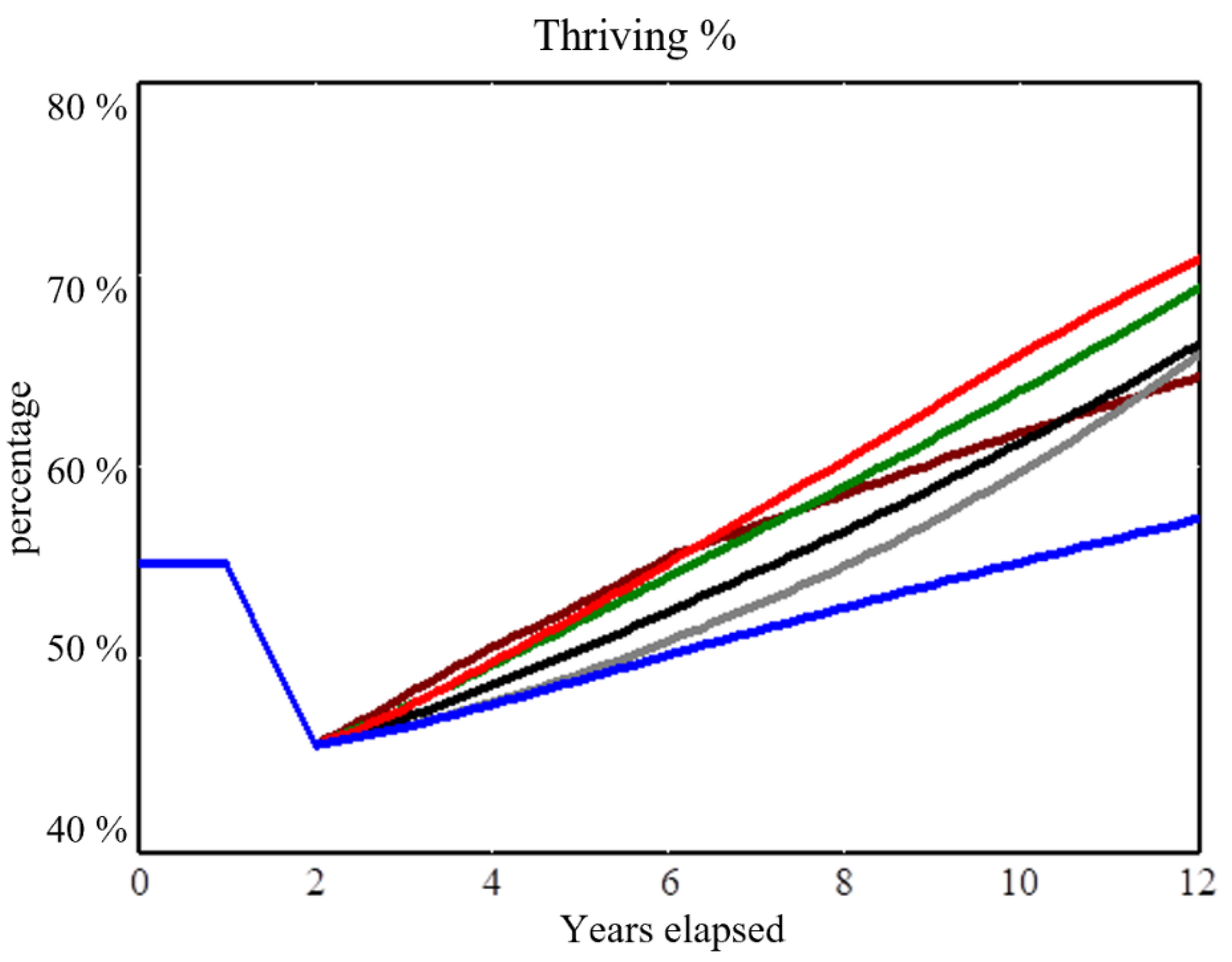
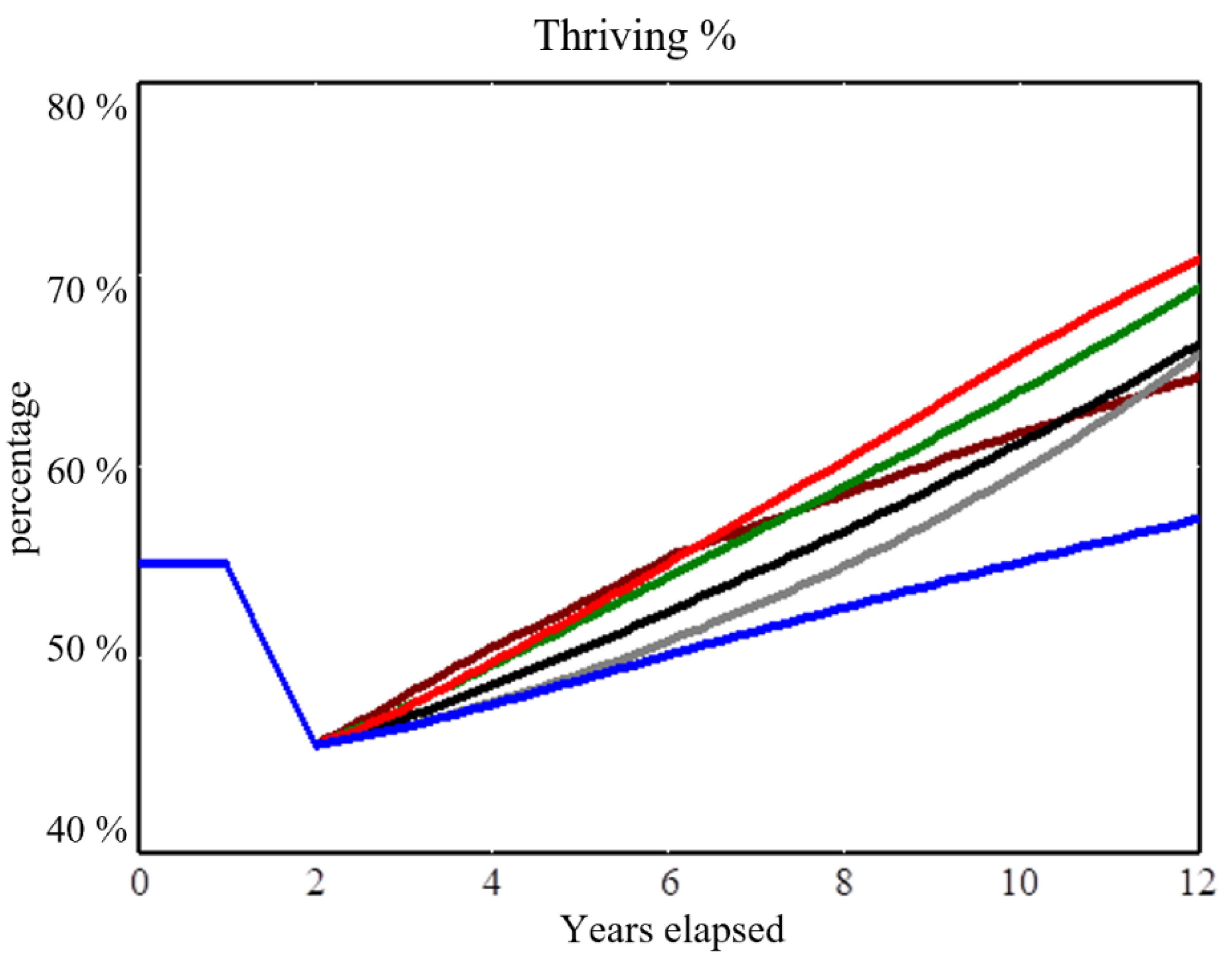
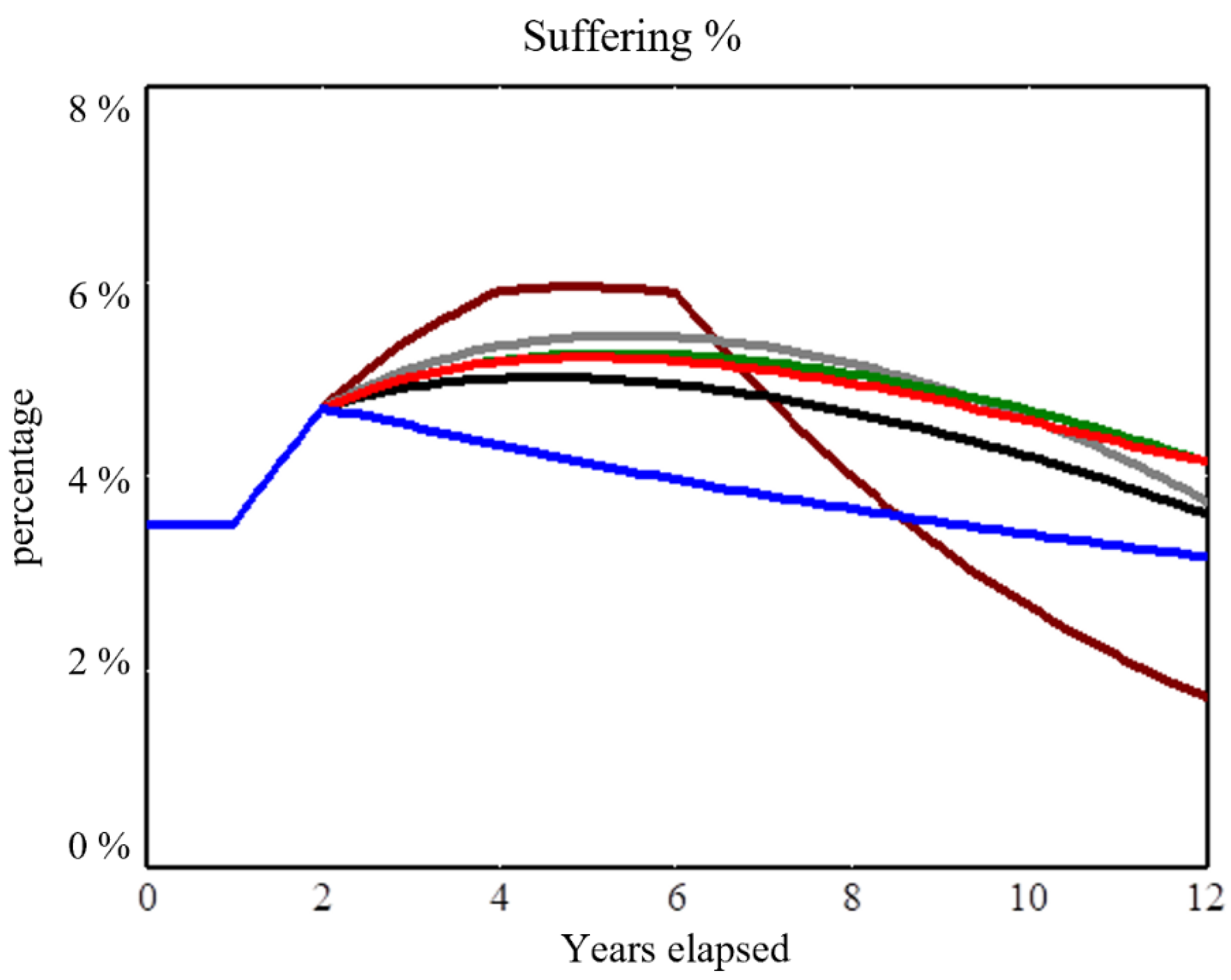
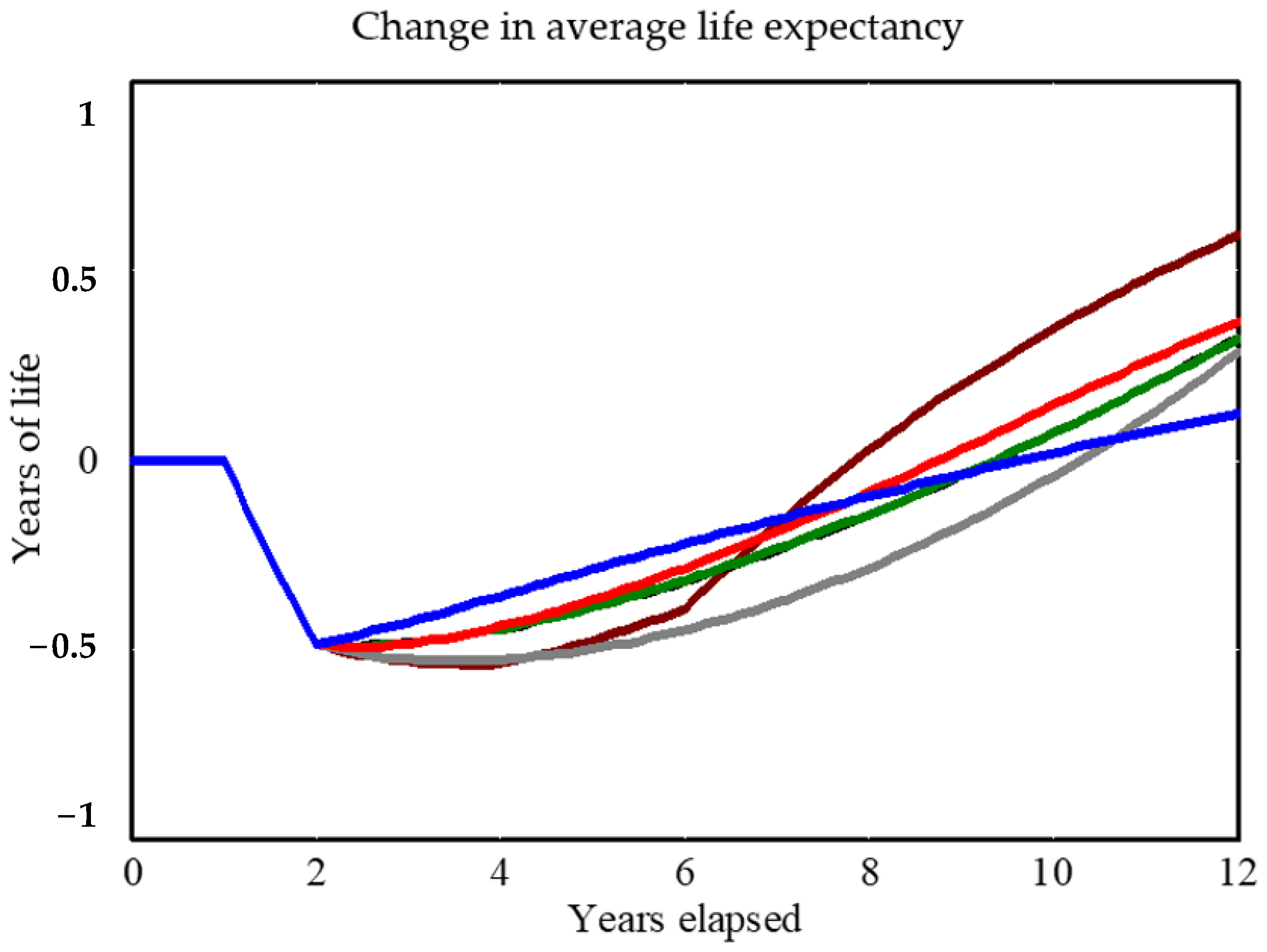
- Status Quo: continue the historical, pre-shock allocation, which gives greatest priority to urgent services capacity (40%) and vital conditions (30%), and far less to equity (15%) and belonging and civic muscle (15%).
- Vital Conditions 40%: switch at Year 2 to a new stable allocation emphasizing vital conditions (40%), with the other three at 20%.
- Equity 40%: switch at Year 2 to a new stable allocation emphasizing equity (40%), with the other three at 20%.
- Belonging and Civic Muscle 40%: switch at Year 2 to a new stable allocation emphasizing belonging and civic muscle (40%), with the other three at 20%.
- Even Balance 25%: switch at Year 2 to a new stable allocation with all four at 25%.
- Best Pivot: switch at Year 2 to emphasize equity first (65%) and belonging and civic muscle (25%), with the other two at 5% each; then, from Years 4–6, pivot back toward urgent services and vital conditions, for an eventual stable allocation at Year 6 of urgent services (45%), vital conditions (35%), belonging and civic muscle (15%), and equity (5%).
2.9. Tests in a More Disorganized Community
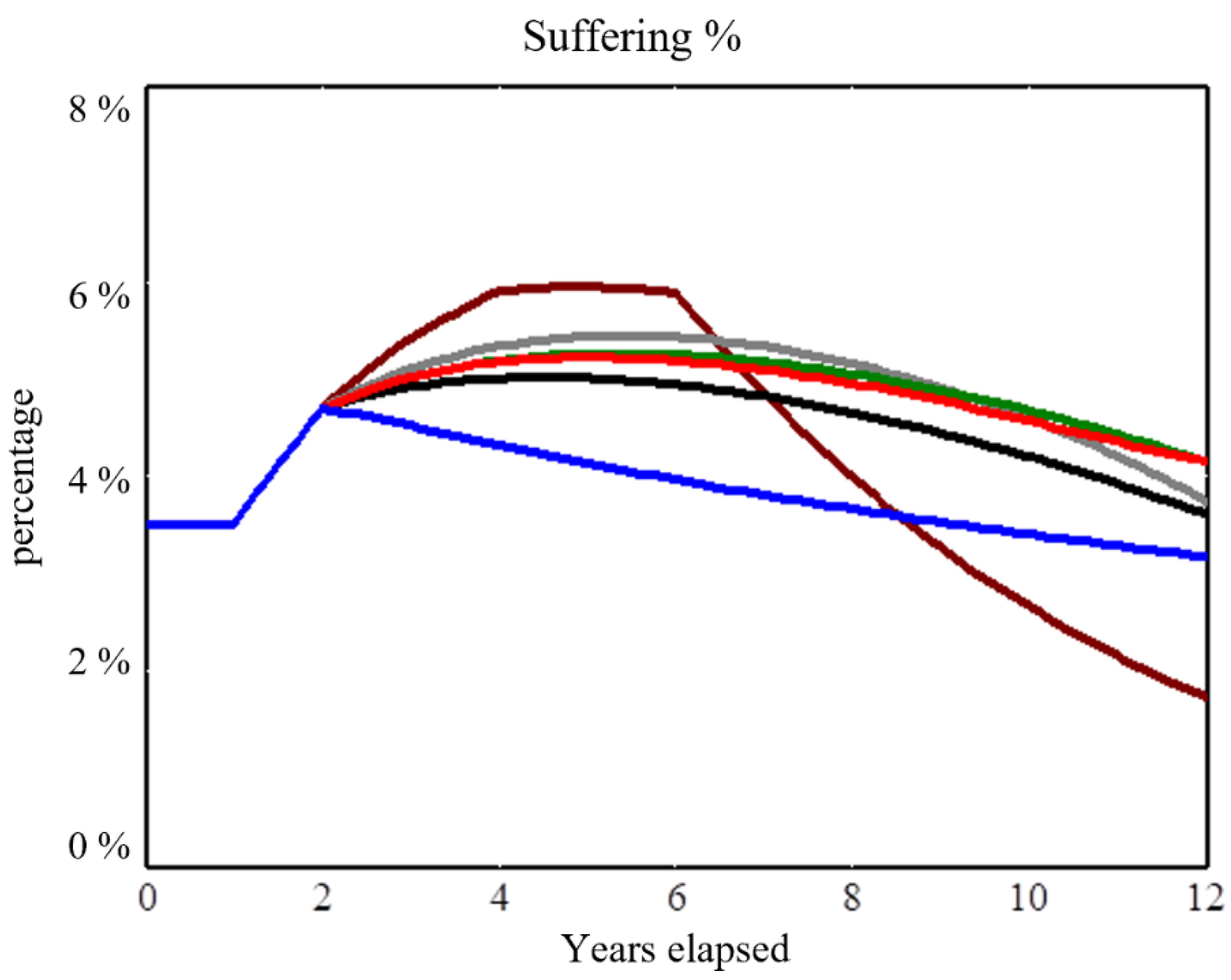
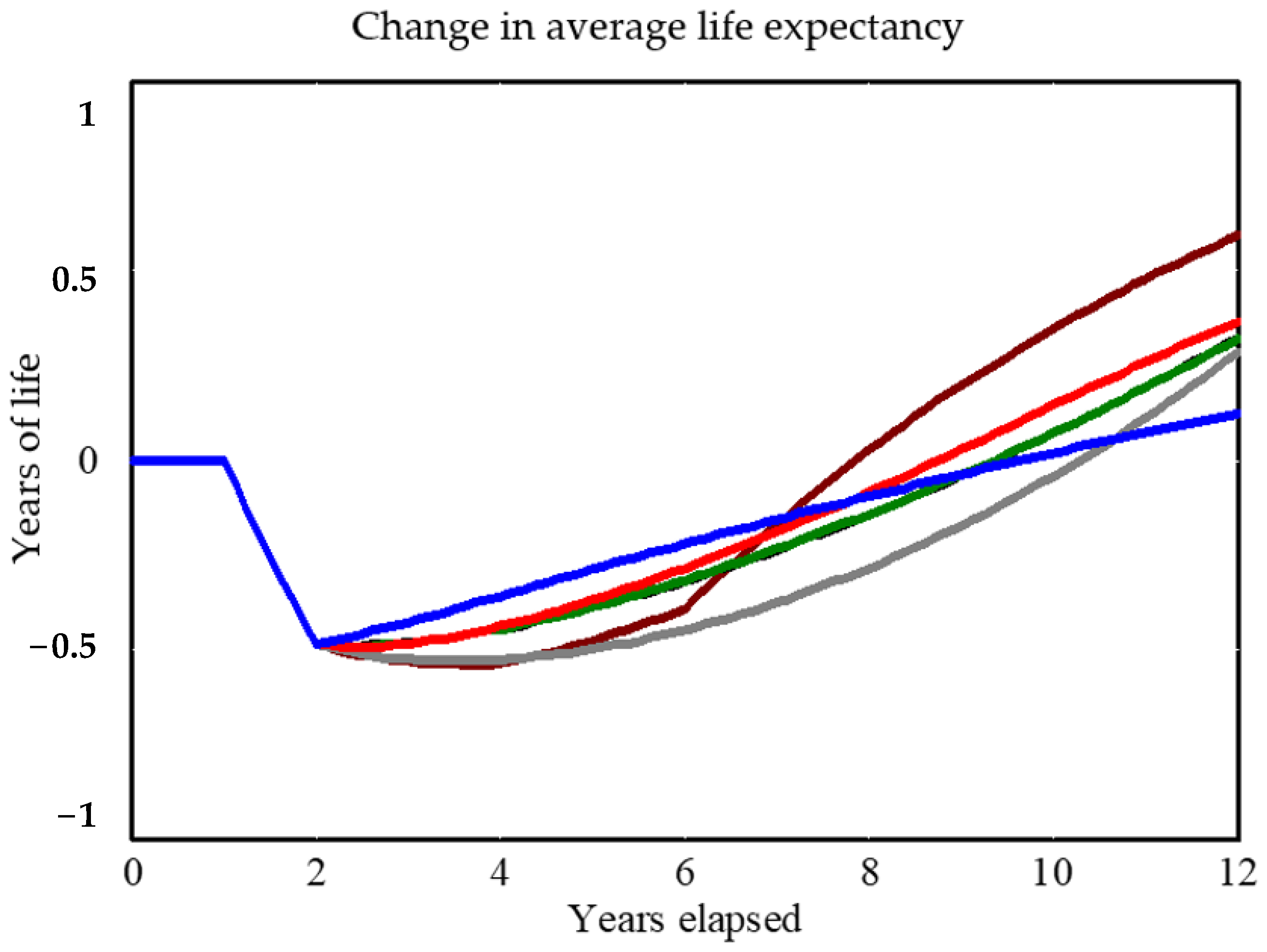
3. Results
4. Discussion
4.1. Tentative Strategic Implications
- The best resilience strategy may require decisive shifts from historical priorities.
- The best strategy requires investing early in both equity and belonging and civic muscle so that one may build on those assets later: a kind of self-reinforcing, asset-building maneuver. The value of those early investments is not only because they support thriving by helping people connect and heal through collective trauma. It is also because they support the infrastructure needed for shared stewardship. In a diverse and divided community, it takes dedicated resources to establish greater interdependence and enable stewards to work across differences, devise shared plans, gather and manage assets, and adapt to challenges over time.
- Efforts to transition toward an equitable, thriving future may involve some inevitable sacrifice of greater suffering in the shorter term; a “worse before better” dynamic. This dynamic has been described previously with respect to downstream and upstream health investments [14], as well as business process improvements and the concept of the “capability trap” [15].
- A risk-averse approach (changing priorities little from the status quo and leaving them fixed over time) may avoid the worse-before-better pattern, but the lack of a decisive pivot will result in a mediocre trajectory over time. Safe, static allocation avoids sacrifice, but it does not build the reservoirs of equity or belonging and civic muscle needed to both boost thriving and drive down suffering.
- A community that can pivot strongly toward building equity and belonging and civic muscle after a severe shock may be best positioned to spring forward and maximize well-being over time. Although that maneuver is superior in principle (under the conditions of this analysis), it may be perceived as infeasible in practice–especially if it entails somewhat greater suffering immediately after a shock. Actual feasibility, however, depends on how effectively community stewards make the case for equitable system change [16]. For instance, savvy casemakers could portray long-overdue investments in equity and belonging and civic muscle as a decisive break from a status quo that for generations has caused far greater unjust suffering and would otherwise continue to leave the entire community weaker and more vulnerable.
4.2. Contributions
- A focus on summary measures of population-level health and well-being, as opposed to focusing only on a particular subset of health or social outcomes. The model’s main outcome measures (i.e., the Cantril categories of people thriving, struggling, and suffering) are routinely tracked across the US and around the world, allowing standardized comparisons over time and geography.
- Representation of equity as a structural driver affecting the entire system, as opposed to only accounting for differences among certain subpopulations (e.g., by race, gender, or income).
- Broad analytic boundary, encompassing concepts of well-being, vital conditions, urgent services, equity, and belonging and civic muscle and portraying their dynamic interactions.
- Ability to explore alternative paths toward equitable renewal over a decade. The model does not tell leaders what to do, but rather strengthens their ability to interpret local data and negotiate local priorities, spot opportunities, weigh tradeoffs, and think creatively about navigating a multiyear path from crisis to renewal.
- Ability to explain the dynamics of shock and renewal by tracking a suite of interacting variables and outcome metrics over time.
4.3. Limitations and Extensions
Supplementary Materials
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Botchwey, N.; Dannenberg, A.; Frumkin, H. Making Healthy Places: Designing and Building for Well-Being, Equity, and Sustainability, 2nd ed.; Island Press: Washington, DC, USA, 2022. [Google Scholar]
- Braveman, P.; Cubbin, C.; Egerter, S.; Pedregon, V. Neighborhoods and Health; Robert Wood Johnson Foundation: Princeton, NJ, USA, 2011; Available online: https://www.rwjf.org/en/library/research/2011/05/neighborhoods-and-health-.html (accessed on 5 August 2022).
- Milstein, B. Thriving Together through Shared Stewardship. ReThink Health. 2021. Available online: http://tiny.cc/SharedStewardshipVideo (accessed on 5 August 2022).
- Rethink Health. Vital Conditions for Well-Being and Justice. 2022. Available online: http://www.rethinkhealth/about/#1 (accessed on 5 August 2022).
- Institute of Medicine. Healthy, Resilient, and Sustainable Communities after Disasters: Strategies, Opportunities, and Planning for Recovery; National Academies Press: Washington, DC, USA, 2015; Available online: https://nap.nationalacademies.org/catalog/18996/healthy-resilient-and-sustainable-communities-after-disasters-strategies-opportunities-and (accessed on 5 August 2022).
- Walpole, E.H.; Loerzel, J.; Dillard, M. A Review of Community Resilience Frameworks and Assessment Tools: An Annotated Bibliography; National Institute for Standards and Technology: Washington, DC, USA, 2021. Available online: https://nvlpubs.nist.gov/nistpubs/TechnicalNotes/NIST.TN.2172.pdf (accessed on 5 August 2022).
- Milstein, B.; Roulier, M.; Hartig, E.; Kelleher, C.; Wegley, S. (Eds.) Thriving Together: A Springboard for Equitable Recovery and Resilience in Communities across America; Well Being Trust: Oakland, CA, USA, 2020; Available online: http://www.thriving.us (accessed on 5 August 2022).
- Milstein, B.; Homer, J. Which Priorities for Health and Well-Being Stand out after Accounting for Tangled Threats and Costs? Simulating Potential Intervention Portfolios in Large Urban Counties. Milbank Q. 2020, 98, 372–398. [Google Scholar] [CrossRef] [PubMed]
- University of Wisconsin Population Health Institute. County Health Rankings & Roadmaps; University of Wisconsin Population Health Institute: Madison, WI, USA, 2022; Available online: http://www.countyhealthrankings.org (accessed on 5 August 2022).
- Gallup. Understanding How Gallup Uses the Cantril Scale: Development of the “Thriving, Struggling, Suffering” Categories. 2020. Available online: https://news.gallup.com/poll/122453/understanding-gallup-uses-cantril-scale.aspx (accessed on 5 August 2022).
- World Bank. Gini Index for the United States. Available online: https://fred.stlouisfed.org/series/SIPOVGINIUSA (accessed on 5 August 2022).
- Witters, D.; Harter, J. In U.S., Life Ratings Plummet to 12-Year Low. Gallup. 2020. Available online: https://news.gallup.com/poll/308276/life-ratings-plummet-year-low.aspx (accessed on 5 August 2022).
- Arora, A.; Spatz, E.; Herrin, J.; Riley, C.; Roy, B.; Kell, K.; Coberley, C.; Rula, E.; Krumholz, H.M. Population Well-Being Measures Help Explain Geographic Disparities in Life Expectancy at the County Level. Health Aff. 2016, 35, 2075–2082. Available online: http://content.healthaffairs.org/content/35/11/2075.abstract (accessed on 5 August 2022). [CrossRef] [PubMed]
- Homer, J.B.; Hirsch, G.B. System Dynamics Modeling for Public Health: Background and Opportunities. Am. J. Public Health 2006, 96, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Repenning, N.P.; Sterman, J.D. Nobody Ever Gets Credit for Fixing Problems That Never Happened: Creating and Sustaining Process Improvement. Calif. Manag. Rev. 2001, 43, 64–88. [Google Scholar] [CrossRef]
- Manuel, T.; Milstein, B. To Catalyze System Change, Become a Better Casemaker. ReThink Health, 10 March 2020. Available online: https://rethinkhealth.org/blog/Resource/to-catalyze-system-change-become-a-better-casemaker/ (accessed on 5 September 2022).
- Ostrom, E. Beyond Markets and States: Polycentric Governance of Complex Economic Systems. Stockholm, Sweden: Nobel Prize Lecture, 2009. Available online: http://www.nobelprize.org/nobel_prizes/economic-sciences/laureates/2009/ostrom-lecture.html (accessed on 5 August 2022).
- Milstein, B.; Homer, J.; Soderquist, C.; Belsky, M. Playbill for the Thriving Together Theater. ReThink Health. Available online: http://tiny.cc/thriving-playbill (accessed on 5 August 2022).
- Sterman, J.D. Business Dynamics: Systems Thinking and Modeling for a Complex World; Irwin McGraw-Hill: Boston, MA, USA, 2000. [Google Scholar]
- Homer, J. Best Practices in System Dynamics Modeling, Revisited: A Practitioner’s View. Syst. Dyn. Rev. 2019, 35, 177–181. [Google Scholar] [CrossRef]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Milstein, B.; Homer, J.; Soderquist, C. How Can a Community Pursue Equitable Health and Well-Being after a Severe Shock? Ideas from an Exploratory Simulation Model. Systems 2022, 10, 158. https://doi.org/10.3390/systems10050158
Milstein B, Homer J, Soderquist C. How Can a Community Pursue Equitable Health and Well-Being after a Severe Shock? Ideas from an Exploratory Simulation Model. Systems. 2022; 10(5):158. https://doi.org/10.3390/systems10050158
Chicago/Turabian StyleMilstein, Bobby, Jack Homer, and Chris Soderquist. 2022. "How Can a Community Pursue Equitable Health and Well-Being after a Severe Shock? Ideas from an Exploratory Simulation Model" Systems 10, no. 5: 158. https://doi.org/10.3390/systems10050158
APA StyleMilstein, B., Homer, J., & Soderquist, C. (2022). How Can a Community Pursue Equitable Health and Well-Being after a Severe Shock? Ideas from an Exploratory Simulation Model. Systems, 10(5), 158. https://doi.org/10.3390/systems10050158