

Resilience Development in Multiple Shocks: Lessons in Mental Health and Well-Being Deterioration during COVID-19

Abstract
1. Introduction
2. COVID-19 and Multisystemic Perspectives in Resilience Development
2.1. Resilience Development during COVID-19
2.2. Clinical and Multisystemic Perspectives in Psychological Resilience
2.3. Organizational Resilience and Impact
3. Methods
4. Model Conceptualization
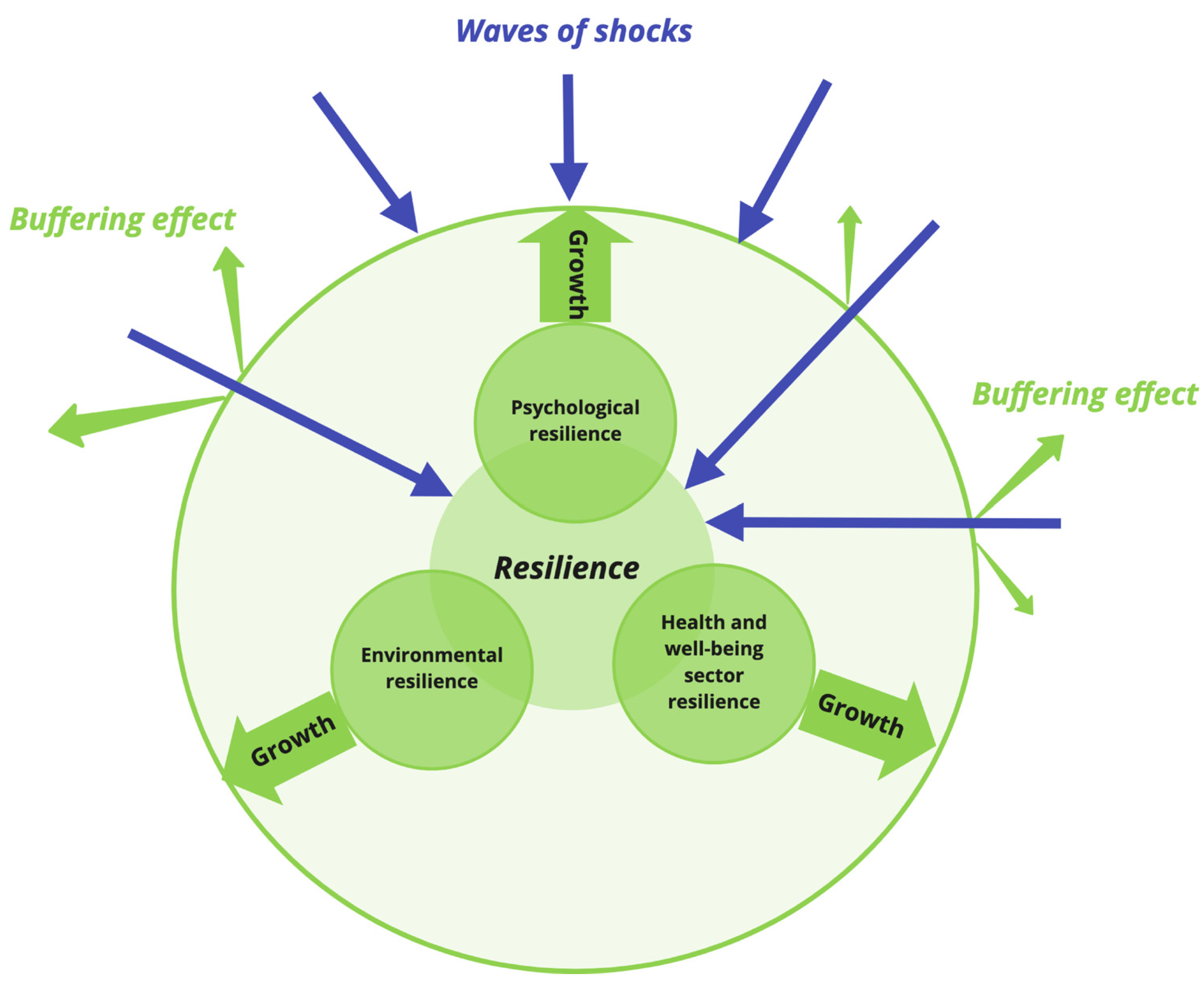
4.1. Resilience and Disturbance
4.2. Psychological Resilience at the Population Level
4.3. Health and Well-Being Service Sector Resilience
4.4. Organizational Resilience in the Environment
5. Model Results
5.1. Model Equilibrium
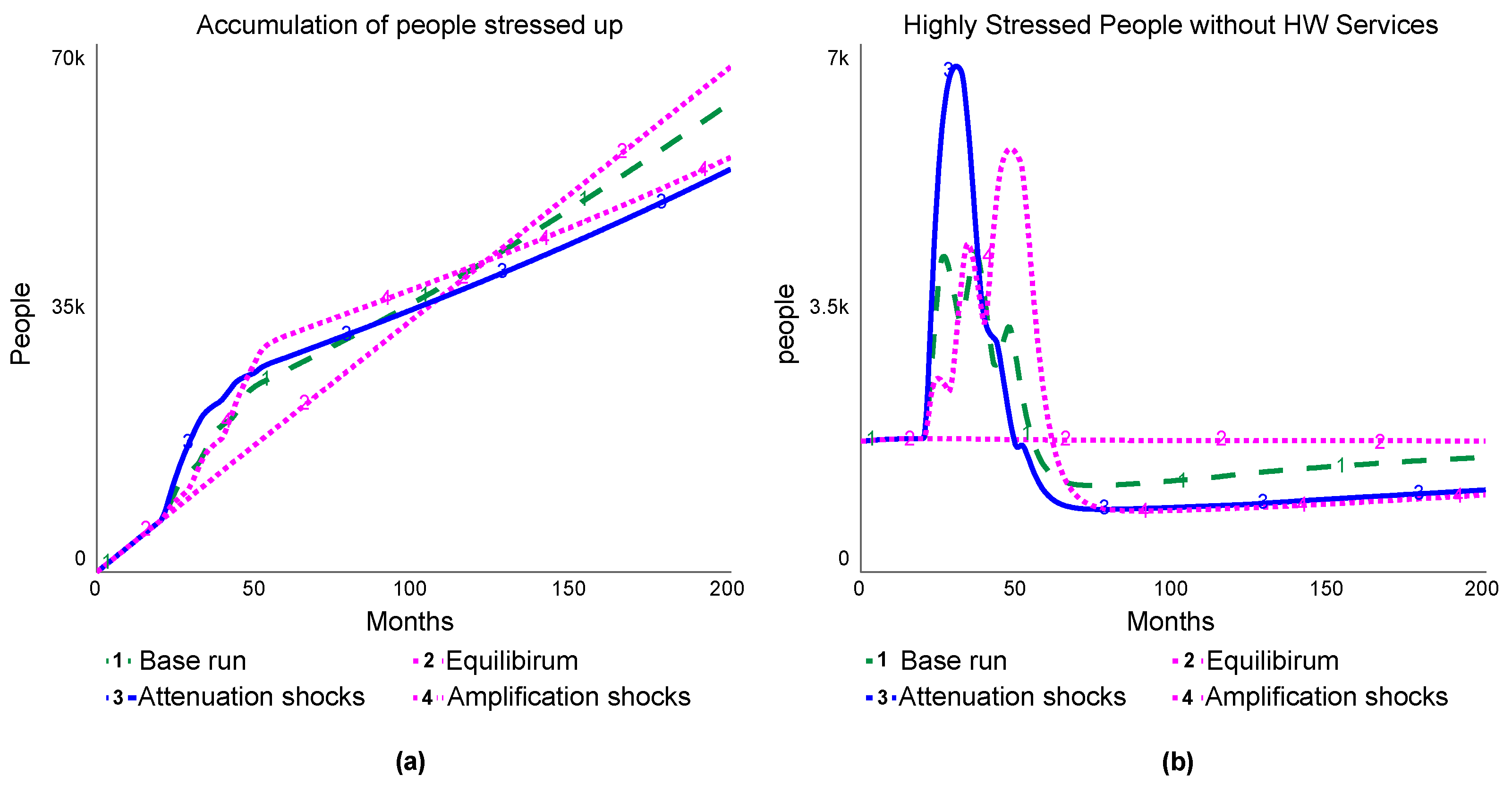
5.2. Multiple Shocks in the Base Run
- Resilience developed in multiple shocks can lower the number of highly stressed people without HW services compared to pre-shock conditions.
- Under the scenario of three consecutive shocks with the same durations and intensities, the psychological resilience at the population level increased over time, but was not sufficiently high enough to decrease the overall risk of deterioration of health and well-being.
5.3. Attenuation of Multiple Shocks
- When the intensity and duration of the shocks decreased over time, the system’s rapid responses in providing health services and environmental stabilization in the first significant shock were critical in improving the population’s resilience in addressing the risk of health and well-being deterioration in later shocks.
5.4. Amplification of Multiple Shocks
- When the intensity and duration of the shocks increased over time, while the direct consequences of the first minor and mild shocks can be relatively smaller, a higher risk of health and well-being deterioration can present in the following major shock if the resilience development process does not sufficiently prepare the system.
6. Policy Testing
7. Discussion, Limitations, and Implications
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A. Model Equations
References
- World Health Organization WHO Coronavirus (COVID-19) Dashboard|WHO Coronavirus (COVID-19) Dashboard with Vaccination Data. Available online: https://covid19.who.int/info/ (accessed on 28 August 2022).
- Office for Health Improvement & Disparities COVID-19 Mental Health and Wellbeing Surveillance: Report. Available online: https://www.gov.uk/government/publications/covid-19-mental-health-and-wellbeing-surveillance-report (accessed on 15 December 2021).
- Gao, X.; Davillas, A.; Jones, A.M. The COVID-19 Pandemic and Its Impact on Socioeconomic Inequality in Psychological Distress in the UK: An Update; Institute of Labor Economics (IZA): Bonn, Germany, 2021. [Google Scholar]
- Ellwardt, L.; Präg, P. Heterogeneous Mental Health Development during the COVID-19 Pandemic in the United Kingdom. Sci. Rep. 2021, 11, 15958. [Google Scholar] [CrossRef] [PubMed]
- Fletcher, D.; Sarkar, M. Psychological Resilience: A Review and Critique of Definitions, Concepts, and Theory. Eur. Psychol. 2013, 18, 12–23. [Google Scholar] [CrossRef]
- Schwarz, S. Resilience in Psychology: A Critical Analysis of the Concept. Theory Psychol. 2018, 28, 528–541. [Google Scholar] [CrossRef]
- Burnard, K.; Bhamra, R. Organisational Resilience: Development of a Conceptual Framework for Organisational Responses. Int. J. Prod. Res. 2011, 49, 5581–5599. [Google Scholar] [CrossRef]
- Ungar, M. The Social Ecology of Resilience: Addressing Contextual and Cultural Ambiguity of a Nascent Construct. Am. J. Orthopsychiatry 2011, 81, 1–17. [Google Scholar] [CrossRef]
- Ungar, M.; Theron, L. Resilience and Mental Health: How Multisystemic Processes Contribute to Positive Outcomes. Lancet Psychiatry 2020, 7, 441–448. [Google Scholar] [CrossRef]
- Rahmandad, H.; Lim, T.Y.; Sterman, J. Estimating COVID-19 Under-Reporting Across 86 Nations: Implications for Projections and Control; Social Science Research Network: Rochester, NY, USA, 2020. [Google Scholar]
- Vogus, T.; Sutcliffe, K. Organizing for Resilience. In Positive Organizational Scholarship: Foundations of a New Discipline, Cameron, K., Dutton, J.E., Quinn, R.E., Eds.; Berrett-Koehler: Oakland, CA, USA, 2003; pp. 94–110. [Google Scholar]
- Weick, K.E.; Sutcliffe, K.M. Managing the Unexpected: Sustained Performance in a Complex World/Karl E. Weick, Kathleen M. Sutcliffe., 3rd ed.; Wiley: Hoboken, NJ, USA, 2015; ISBN 978-1-118-86241-4. [Google Scholar]
- BlackDeer, A.A.; Hovmand, P.S.; Chew, K.; Zhou, K.; Fowler, P.J.; Auslander, W. Resiliency from a Feedback Perspective. Available online: https://exchange.iseesystems.com/public/psh/human-resiliency/index.html#page1 (accessed on 15 December 2021).
- Rudolph, J.W.; Repenning, N.P. Disaster Dynamics: Understanding the Role of Quantity in Organizational Collapse. Adm. Sci. Q. 2002, 47, 1–30. [Google Scholar] [CrossRef]
- Sterman, J.D. Business Dynamics: Systems Thinking and Modeling for a Complex World /John D. Sterman; Irwin/McGraw-Hill: Boston, MA, USA, 2000; ISBN 0-07-231135-5. [Google Scholar]
- Lane, D.C.; Schwaninger, M. Theory Building with System Dynamics: Topic and Research Contributions. Syst. Res. Behav. Sci. 2008, 25, 439–445. [Google Scholar] [CrossRef]
- de Gooyert, V.; Größler, A. On the Differences between Theoretical and Applied System Dynamics Modeling. Syst. Dyn. Rev. 2018, 34, 575–583. [Google Scholar] [CrossRef]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A.; et al. Impact of COVID-19 Pandemic on Mental Health in the General Population: A Systematic Review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Daly, M.; Robinson, E. Psychological Distress Associated with the Second COVID-19 Wave: Prospective Evidence from the UK Household Longitudinal Study. J. Affect. Disord. 2022, 310, 274–278. [Google Scholar] [CrossRef]
- Barry, V.; Stout, M.E.; Lynch, M.E.; Mattis, S.; Tran, D.Q.; Antun, A.; Ribeiro, M.J.; Stein, S.F.; Kempton, C.L. The Effect of Psychological Distress on Health Outcomes: A Systematic Review and Meta-Analysis of Prospective Studies. J. Health Psychol. 2020, 25, 227–239. [Google Scholar] [CrossRef] [PubMed]
- Ahrens, K.F.; Neumann, R.J.; Kollmann, B.; Brokelmann, J.; von Werthern, N.M.; Malyshau, A.; Weichert, D.; Lutz, B.; Fiebach, C.J.; Wessa, M.; et al. Impact of COVID-19 Lockdown on Mental Health in Germany: Longitudinal Observation of Different Mental Health Trajectories and Protective Factors. Transl. Psychiatry 2021, 11, 392. [Google Scholar] [CrossRef] [PubMed]
- Manchia, M.; Gathier, A.W.; Yapici-Eser, H.; Schmidt, M.V.; de Quervain, D.; van Amelsvoort, T.; Bisson, J.I.; Cryan, J.F.; Howes, O.D.; Pinto, L.; et al. The Impact of the Prolonged COVID-19 Pandemic on Stress Resilience and Mental Health: A Critical Review across Waves. Eur. Neuropsychopharmacol. 2022, 55, 22–83. [Google Scholar] [CrossRef] [PubMed]
- Haldane, V.; De Foo, C.; Abdalla, S.M.; Jung, A.-S.; Tan, M.; Wu, S.; Chua, A.; Verma, M.; Shrestha, P.; Singh, S.; et al. Health Systems Resilience in Managing the COVID-19 Pandemic: Lessons from 28 Countries. Nat. Med. 2021, 27, 964–980. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, N.; Brooks, S.K.; Wessely, S.; Tracy, D.K. How Might the NHS Protect the Mental Health of Health-Care Workers after the COVID-19 Crisis? Lancet Psychiatry 2020, 7, 733–734. [Google Scholar] [CrossRef]
- Bryce, C.; Ring, P.; Ashby, S.; Wardman, J.K. Resilience in the Face of Uncertainty: Early Lessons from the COVID-19 Pandemic. J. Risk Res. 2020, 23, 880–887. [Google Scholar] [CrossRef]
- Sakurai, M.; Chughtai, H. Resilience against Crises: COVID-19 and Lessons from Natural Disasters. Eur. J. Inf. Syst. 2020, 29, 585–594. [Google Scholar] [CrossRef]
- Sawyer, A.T.; Bailey, A.K.; Green, J.F.; Sun, J.; Robinson, P.S. Resilience, Insight, Self-Compassion, and Empowerment (RISE): A Randomized Controlled Trial of a Psychoeducational Group Program for Nurses. J. Am. Psychiatr. Nurses Assoc. 2021. [Google Scholar] [CrossRef]
- Milioni, M.; Alessandri, G.; Eisenberg, N.; Caprara, G.V. The Role of Positivity as Predictor of Ego-Resiliency from Adolescence to Young Adulthood. Personal. Individ. Differ. 2016, 101, 306–311. [Google Scholar] [CrossRef]
- Gentili, C.; Rickardsson, J.; Zetterqvist, V.; Simons, L.E.; Lekander, M.; Wicksell, R.K. Psychological Flexibility as a Resilience Factor in Individuals with Chronic Pain. Front. Psychol. 2019, 10, 2016. [Google Scholar] [CrossRef] [PubMed]
- Fritz, J.; de Graaff, A.M.; Caisley, H.; van Harmelen, A.-L.; Wilkinson, P.O. A Systematic Review of Amenable Resilience Factors That Moderate and/or Mediate the Relationship Between Childhood Adversity and Mental Health in Young People. Front. Psychiatry 2018, 9, 230. [Google Scholar] [CrossRef] [PubMed]
- Niitsu, K.; Rice, M.J.; Houfek, J.F.; Stoltenberg, S.F.; Kupzyk, K.A.; Barron, C.R. A Systematic Review of Genetic Influence on Psychological Resilience. Biol. Res. Nurs. 2019, 21, 61–71. [Google Scholar] [CrossRef] [PubMed]
- de Leon, H.J.H.; Kopainsky, B. Do You Bend or Break? System Dynamics in Resilience Planning for Food Security. Syst. Dyn. Rev. 2019, 35, 287–309. [Google Scholar] [CrossRef]
- van der Vegt, G.S.; Essens, P.; Wahlström, M.; George, G. Managing Risk and Resilience. Acad. Manag. J. 2015, 58, 971–980. [Google Scholar] [CrossRef]
- Meyer, A.D. Adapting to Environmental Jolts. Adm. Sci. Q. 1982, 27, 515–537. [Google Scholar] [CrossRef]
- Petriglieri, G.; Petriglieri, J.L. The Return of the Oppressed: A Systems Psychodynamic Approach to Organization Studies. Acad. Manag. Ann. 2020, 14, 411–449. [Google Scholar] [CrossRef]
- Brown, A.; Starkey, K. Organizational Identity and Learning: A Psychodynamic Perspective. Acad. Manag. Rev. 2000, 25, 102–120. [Google Scholar] [CrossRef]
- Pring, E.T.; Malietzis, G.; Kendall, S.W.H.; Jenkins, J.T.; Athanasiou, T. Crisis Management for Surgical Teams and Their Leaders, Lessons from the COVID-19 Pandemic; A Structured Approach to Developing Resilience or Natural Organisational Responses. Int. J. Surg. 2021, 91, 105987. [Google Scholar] [CrossRef]
- Williams, T.; Gruber, D.; Sutcliffe, K.; Shepherd, D.; Zhao, E.Y. Organizational Response to Adversity: Fusing Crisis Management and Resilience Research Streams. Acad. Manag. Ann. 2017, 11, 733–769. [Google Scholar] [CrossRef]
- Ilseven, E.; Puranam, P. Measuring Organizational Resilience as a Performance Outcome. J. Organ. Des. 2021, 10, 127–137. [Google Scholar] [CrossRef]
- Kahn, W.A.; Barton, M.A.; Fellows, S. Organizational Crises and the Disturbance of Relational Systems. Acad. Manage. Rev. 2013, 38, 377–396. [Google Scholar] [CrossRef]
- Homer, J.B.; Hirsch, G.B. System Dynamics Modeling for Public Health: Background and Opportunities. Am. J. Public Health 2006, 96, 452–458. [Google Scholar] [CrossRef] [PubMed]
- Homer, J.; Hirsch, G.; Milstein, B. Chronic Illness in a Complex Health Economy: The Perils and Promises of Downstream and Upstream Reforms. Syst. Dyn. Rev. 2007, 23, 313–343. [Google Scholar] [CrossRef]
- Chichakly, K. Behavioral Implications in COVID-19 Spread and Vaccinations. Systems 2021, 9, 72. [Google Scholar] [CrossRef]
- Rooney-Varga, J.N.; Kapmeier, F.; Sterman, J.D.; Jones, A.P.; Putko, M.; Rath, K. The Climate Action Simulation. Simul. Gaming 2020, 51, 114–140. [Google Scholar] [CrossRef]
- Randers, J.; Rockström, J.; Stoknes, P.-E.; Goluke, U.; Collste, D.; Cornell, S.E.; Donges, J. Achieving the 17 Sustainable Development Goals within 9 Planetary Boundaries. Glob. Sustain. 2019, 2, e24. [Google Scholar] [CrossRef]
- Rahmandad, H.; Ton, Z. If Higher Pay Is Profitable, Why Is It So Rare? Modeling Competing Strategies in Mass Market Services. Organ. Sci. 2020, 31, 1053–1071. [Google Scholar] [CrossRef]
- Jalali, M.S.; Rahmandad, H.; Bullock, S.L.; Ammerman, A. Dynamics of Implementation and Maintenance of Organizational Health Interventions. Int. J. Environ. Res. Public. Health 2017, 14, 917. [Google Scholar] [CrossRef]
- de Gooyert, V. Developing Dynamic Organizational Theories; Three System Dynamics Based Research Strategies. Qual. Quant. 2019, 53, 653–666. [Google Scholar] [CrossRef]
- Zimmermann, N. Dynamics of Drivers of Organizational Change; Gabler Verlag: Wiesbaden, Germany, 2011; ISBN 978-3-8349-3051-4. [Google Scholar]
- Sastry, M.A. Problems and Paradoxes in a Model of Punctuated Organizational Change. Adm. Sci. Q. 1997, 42, 237–275. [Google Scholar] [CrossRef]
- Repenning, N.P. A Simulation-Based Approach to Understanding the Dynamics of Innovation Implementation. Organ. Sci. 2002, 13, 109–127. [Google Scholar] [CrossRef]
- Hovmand, P.; Gillespie, D. Implementation of Evidence-Based Practice and Organizational Performance. J. Behav. Health Serv. Res. 2010, 37, 79–94. [Google Scholar] [CrossRef] [PubMed]
- Schwaninger, M.; Grösser, S. System Dynamics as Model-Based Theory Building. Syst. Res. Behav. Sci. 2008, 25, 447–465. [Google Scholar] [CrossRef]
- Homer, J.B. Why We Iterate: Scientific Modeling in Theory and Practice. Syst. Dyn. Rev. 1996, 12, 1–19. [Google Scholar] [CrossRef]
- Newman, E.A. Disturbance Ecology in the Anthropocene. Front. Ecol. Evol. 2019, 7, 147. [Google Scholar] [CrossRef]
- White, P.S.; Pickett, S.T.A. Chapter 1—Natural Disturbance and Patch Dynamics: An Introduction. In The Ecology of Natural Disturbance and Patch Dynamics; Pickett, S.T.A., White, P.S., Eds.; Academic Press: San Diego, CA, USA, 1985; pp. 3–13. ISBN 978-0-12-554520-4. [Google Scholar]
- Henderson, M.; Fitzsimons, E.; Ploubidis, G.; Richards, M.; Patalay, P. Mental Health during Lockdown: Evidence from Four Generations. Lond. UCL Cent. Longitud. Stud. 2020, 20, 1–17. [Google Scholar]
- Homer, J. Levels of Evidence in System Dynamics Modeling. Syst. Dyn. Rev. 2014, 30, 75–80. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Policy | Policy Description | Dynamic Principle | Targeted Loops |
|---|---|---|---|
| P1: Environment-based fast adjustments | Speeding up the environment’s adjustments in providing temporary solutions. Organizations monitor changes, quickly respond to crises, and attempt to develop temporary plans and revisit them quickly once the shock hits the system. | The organizational response time is one month (base run is three months), the time needed for temporary plans equals two months (base run is four months), and every six months (base run is 12 months), the organization revisits the plan. | B2, B1a, B1b |
| P2: Health service sector-based fast responses | Providing health services to support health and well-being throughout crises. The health service sector responds to the demands of health services quickly and provides programs to encourage the use of health services. | The fraction of people reaching out to health and well-being services is 0.8 (base run is 0.5). The waiting time to access these services equals two months (base run is four months), and the time to hire new staff is now three months (base run is 12 months). | R1, B3, B4, B2b, B1a, B1b |
| P3: Collective growth | Facilitating organizations’ and individuals’ evolvement and adjustment for long-term stabilization in crises. Specifically, individuals develop more resilience in tolerating distress and adversities through self-recovery and using health services. Moreover, organizations can provide stabilized adjustments (such as guidelines, arrangements, long-term strategies, and solutions) more quickly in crises. | The emotional tolerance acquired from the recovery process is four times that of the original baseline, which is now 4 (base run is 1), and the time for organizations to settle their stabilization adjustment is now three months (base run is 12 months). | B2a, B2b, B5, B1a, B1b |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhou, K.; Zhang, M. Resilience Development in Multiple Shocks: Lessons in Mental Health and Well-Being Deterioration during COVID-19. Systems 2022, 10, 183. https://doi.org/10.3390/systems10050183
Zhou K, Zhang M. Resilience Development in Multiple Shocks: Lessons in Mental Health and Well-Being Deterioration during COVID-19. Systems. 2022; 10(5):183. https://doi.org/10.3390/systems10050183
Chicago/Turabian StyleZhou, Ke, and Mengru Zhang. 2022. "Resilience Development in Multiple Shocks: Lessons in Mental Health and Well-Being Deterioration during COVID-19" Systems 10, no. 5: 183. https://doi.org/10.3390/systems10050183
APA StyleZhou, K., & Zhang, M. (2022). Resilience Development in Multiple Shocks: Lessons in Mental Health and Well-Being Deterioration during COVID-19. Systems, 10(5), 183. https://doi.org/10.3390/systems10050183