CoVid-19 Pandemic Trend Modeling and Analysis to Support Resilience Decision-Making



Abstract
1. Introduction
- a downward trajectory of reported influenza-like illnesses (ILI).
- a downward trajectory of reported CoVid-19-like syndromic cases.
- the verification of data reporting and trends;
- guidance to support decision-making with predicted recovery trajectories;
- the intercomparison of trends of cities, states, regions and countries;
- determination of the overall infection growth rates due to random infections followed by incubation;
- establishment of the existence or absence of consistent learning trends of recovery and the effectiveness of “lockdown” countermeasures and
- easy-to-use formulas for predictive and scoping purposes.
2. Theoretical Framework and Data
- a)
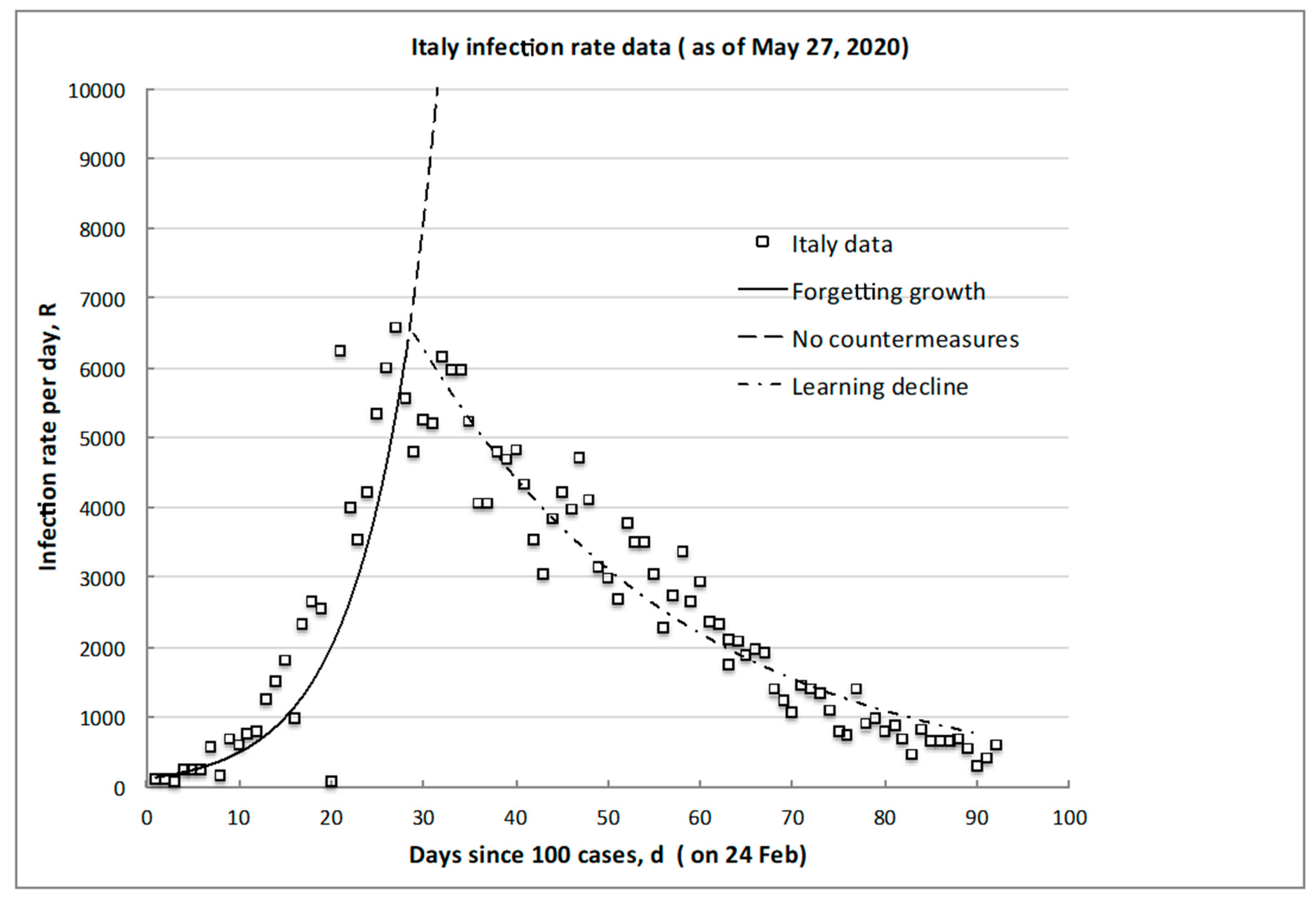
- initial increase up to a peak value, with a characteristic e-folding (forgetting) growth timescale due to incubation, consistent with the known case-tracking data.
- b)
- post-peak recovery decrease from the peak, with a characteristic e-folding (learning) decline timescale dependent on societal learning and the associated countermeasures of control of the spread, consistent with the known world data.
2.1. Foundational Postulates of Learning Theory
2.2. Theoretical Model of Infection Rate Evolution
- Outcomes (infections) occur and are observed randomly but are a systematic function of the risk exposure by person-to-person contact or other transmission spread processes.
- Any and all of the many distributions of infections are equally possibly occurring, with some average or overall characteristic timescale of the incubation process.
- Infections appear and are counted during some observed infection risk exposure interval (here measured in days, d).
- The distribution of the number of infections, n, which is recorded as a function of the infection risk exposure interval, is the most likely, because it is the one that has actually occurred.
- The total number of all possible infections (The magnitude of the total number of possible infections, N, is given by the probability of purely random unabated infection in the entire exposed population and is a maximum fraction of circa 37% (1/e), as demonstrated in [2]; N, and the infection risk exposure interval in days, d, are finite.
- The rate of infections, R, is proportional to the change, dn, in the number of infections during an incremental variation, dd, of the infection risk exposure interval of observation (again, taken equal to a step of 1 day, in our case).
2.3. Data Sources and Analysis
- ○
- World regions (EU, South America and USA) as a whole (interesting, because this is a globalization problem).
- ○
- Italy as a whole and, locally, Lombardy, Lazio, Veneto and Puglia (accessed at [17]), being the largest early outbreak outside of Asia.
- ○
- Some 14 countries with varying geographies, societies, international boundaries and countermeasures to provide comparisons (as listed in Table 1).
- ○
- Regional Department of Health data for selected USA states with a range of infection rates and “lockdown” countermeasures (Arkansas, California, Idaho, Illinois, Iowa, Georgia, Missouri, Nebraska, New York and Wyoming).
- ○
- Large cities or urban centers with varying population densities and countermeasures (New York, St Louis and Chicago).
3. Results, Correlations and Universal Predictions
3.1. Growth of Transmission Trajectory
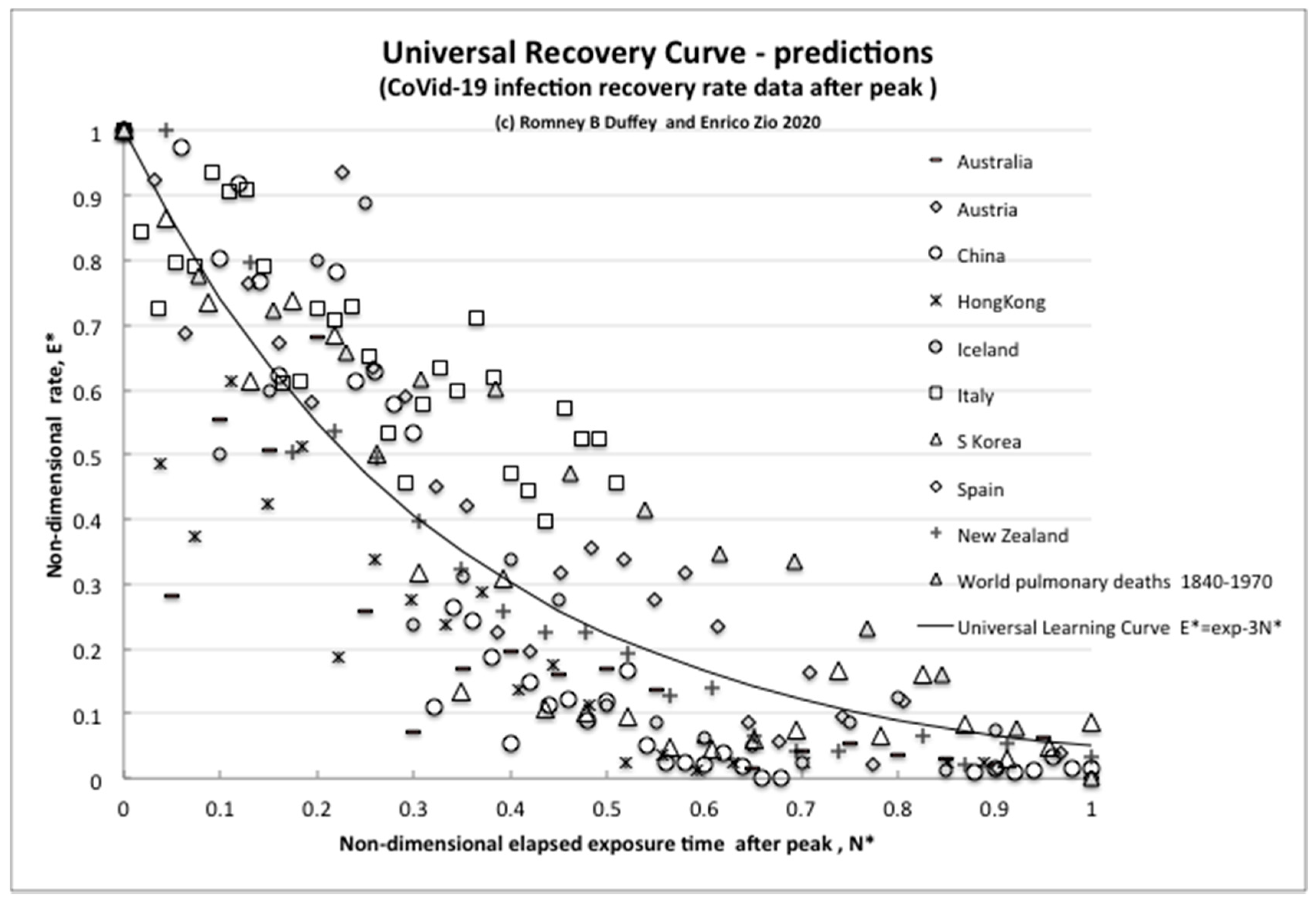
3.2. Decline (Recovery) Trend Predictions
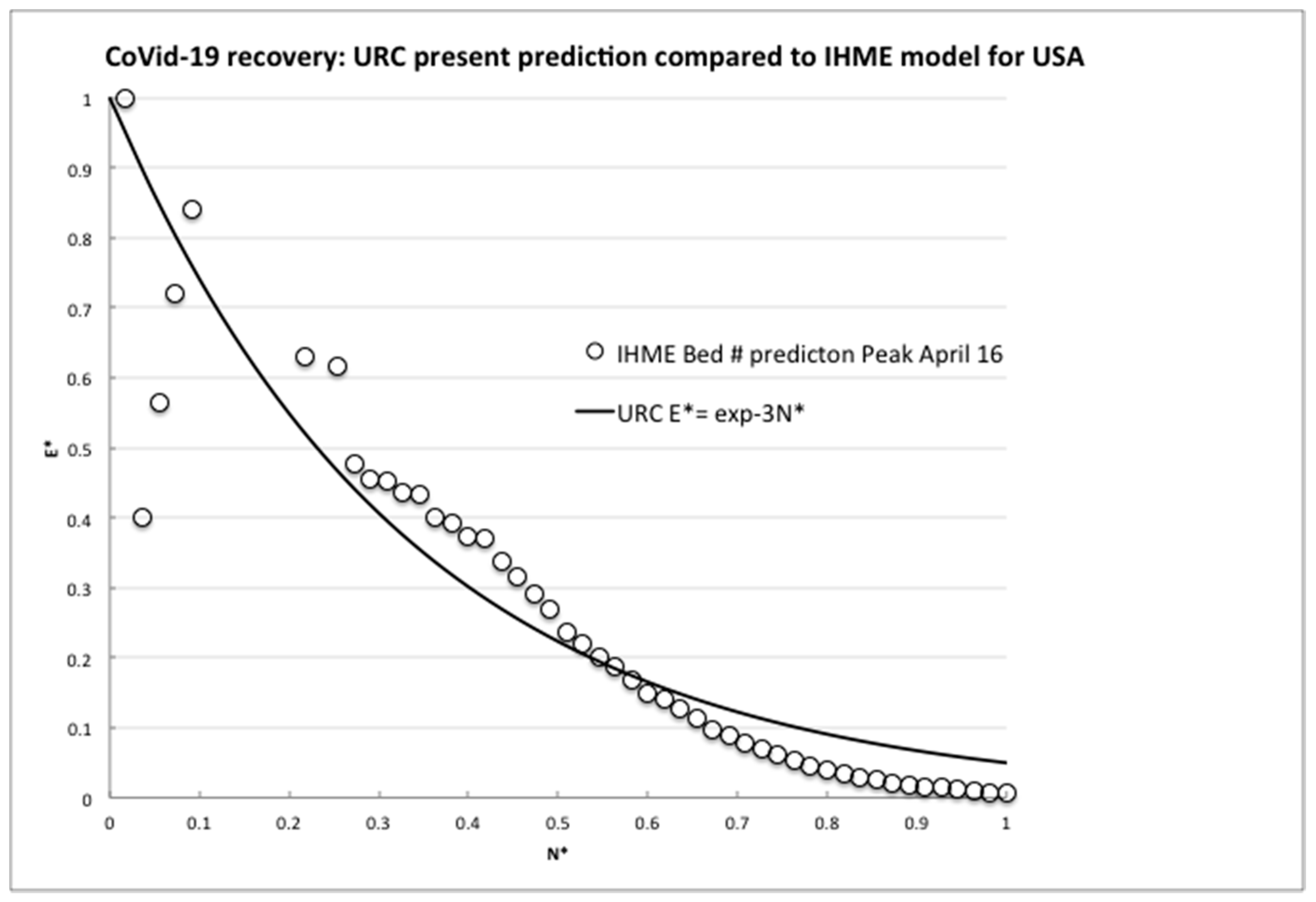
3.3. Comparison of the Theory to a Computational Model for Resilience Planning Purposes
3.4. Imperfect Learning: Plateaux, Periodicity, “Spikes” and Countermeasures Effectiveness
4. Conclusions
- the growth of the rate of infections is exponential and consistent with random transmission, and
- the decline of the rate of infections is also exponential and reflects that countermeasures have similar overall effects everywhere.
- the acceptance of a minimum of residual risk and corresponding definition of the value of the minimum attainable/manageable infection rate,
- demonstration and verification of a steady decline in the infection rate(s), consistent with the model,
- a prediction of the time at which the minimum attainable/manageable infection rate will be reached, if not yet done,
- continuous monitoring of the situation by extended clinical testing, both systematic and random, with feedback of the test results to the predictive model,
- clear rules to identify and isolate possible local increases in the infection rate and means to manage them,
- continuous and resilient medical capacities to treat the infection cases that emerge,
- the deployment of effective, and reasonable for the situation, measures of control and containment of the virus in public and work places and
- the ethics of resilience [21]
Author Contributions
Funding
Conflicts of Interest
References
- White House. Guidelines: Opening Up America Again. Available online: https://www.whitehouse.gov/openingamerica (accessed on 7 May 2020).
- Duffey, R.B.; Zio, E. Analysing recovery from pandemics by Learning Theory: the case of CoVid-19. Medxiv 2020. [Google Scholar] [CrossRef]
- Heesterbeek, J.A.P. A brief history of R0 and a recipe for its calculation. Acta Biotheor. 2002, 50, 189–204. [Google Scholar] [CrossRef] [PubMed]
- Jones, J.H. Notes on R0; Department of Earth System Science, Stanford University: Stanford, CA, USA, 2019; Available online: web.stanford.edu/class/earthsys214/notes/Jones_R0_notes2019.pdf (accessed on 8 May 2020).
- Holme, P.; Masuda, N. The Basic Reproduction Number as a Predictor for Epidemic Outbreaks in Temporal Networks. PLoS ONE 2015, 10, e0120567. [Google Scholar] [CrossRef]
- National Academics. Disaster Resilience: A National Imperative; National Academies Press: Washington, DC, USA, 2012. [Google Scholar] [CrossRef]
- Casella, F. Can the COVID-19 epidemic be controlled on the basis of daily test reports? arXiv 2020, arXiv:2003.06967. [Google Scholar]
- IHME COVID-19 Health Service Utilization Forecasting Team. Forecasting COVID-19 impact on hospital bed-days, ICU-days, ventilator days and deaths by US state in the next 4 months. MedRxiv. 2020. [Google Scholar] [CrossRef]
- Ohlsson, S. Learning from performance errors. Psychol. Rev. 1996, 103, 241–262. [Google Scholar] [CrossRef]
- Anderson, J.R. Cognitive Psychology and its Implications, 3rd ed.; W.H. Freeman: San Francisco, CA, USA, 1990; ISBN 0-7167-2085-X. [Google Scholar]
- Rushbrooke, G.S. Introduction to Statistical Mechanics; Oxford University Press: London, UK, 1949. [Google Scholar]
- Greiner, W.; Neise, L.; Stocker, H. Thermodynamics and Statistical Mechanics; Springer: New York, NY, USA, 1995; ISBN 0-387-94299-8. [Google Scholar]
- Duffey, R.B.; Saull, J.W. Managing Risk: The Human Element; John and Wiley and Sons: Hoboken, NJ, USA, 2008; ISBN 978-0-470-69976-8. [Google Scholar]
- Lewis, E.E. Introduction to Reliability Engineering, 2nd ed.; John Wiley and Sons: New York, NY, USA, 1994. [Google Scholar]
- WHO. World Health Organization. Available online: www.who.int/emergencies/diseases/novel-coronavirus-2019/situation-reports/ (accessed on 18 May 2020).
- World in Data. Available online: ourworldindata.org/grapher/covid-confirmed-cases-since-100th-case (accessed on 18 May 2020).
- Available online: lab.gedidigital.it/gedi-visual/2020/coronavirus-i-contagi-in-italia (accessed on 18 May 2020).
- Ghinai, I.; Woods, S.; Ritger, K.A.; McPherson, T.D.; Black, S.R.; Sparrow, L.; Fricchione, M.; Kerins, J.L.; Pacilli, M.; Ruestow, P.S.; et al. Community Transmission of SARS-CoV-2 at Two Family Gatherings in Chicago, Illinois, February-March 2020; US Department of Health and Human Services: Washington, DC, USA, 2020; Volume 69, pp. 446–450. Available online: https://www.cdc.gov/mmwr/ (accessed on 21 April 2020).
- Becker, J.A.; Klinkenberg, D.; Wallinga, J. Incubation period of 2019 novel coronavirus (2019-nCoV) infections among travellers from Wuhan, China, 20–28 January 2020. Eurosurveillance 2020, 25, 2000062. [Google Scholar] [CrossRef]
- McKeown, T. Determinants of Health. In Understanding and Applying Medical Anthropology; Brown, P.J., Closser, S., Eds.; Routledge: New York, NY, USA, 2016; pp. 60–67. [Google Scholar]
- Rajaonah, B.; Zio, E. Contributing to Disaster Management as an Individual Member of a Collectivity: Resilient Ethics and Ethics of Resilience. Open Arch. HAL 2020, 02533290. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Country/State | Growth Exponent Per Day, G | Coefficient of Determination, R2 | Peak Rate RM |
|---|---|---|---|
| China | 0.26 | 0.86 | 4000 |
| Belgium | 0.18 | 0.93 | 2000 |
| Brazil | 0.13 | 0.86 | 3000 |
| Canada | 0.1 | 0.79 | 1600 |
| Germany | 0.18 | 0.88 | 6200 |
| Italy | 0.13 | 0.76 | 6000 |
| Spain | 0.19 | 0.88 | 10000 |
| California | 0.2 | 0.95 | 2200 |
| S Korea | 0.16 | 0.7 | 900 |
| Sweden | 0.1 | 0.81 | 730 |
| Turkey | 0.15 | 0.88 | 5100 |
| UK | 0.17 | 0.95 | 6000 |
| USA | 0.2 | 0.91 | 53000 |
| EU | 0.15 | 0.92 | 8700 |
| S America | 0.13 | 0.87 | 5500 |
| Average | 0.17 | 0.86 | 7700 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Duffey, R.B.; Zio, E. CoVid-19 Pandemic Trend Modeling and Analysis to Support Resilience Decision-Making. Biology 2020, 9, 156. https://doi.org/10.3390/biology9070156
Duffey RB, Zio E. CoVid-19 Pandemic Trend Modeling and Analysis to Support Resilience Decision-Making. Biology. 2020; 9(7):156. https://doi.org/10.3390/biology9070156
Chicago/Turabian StyleDuffey, Romney B., and Enrico Zio. 2020. "CoVid-19 Pandemic Trend Modeling and Analysis to Support Resilience Decision-Making" Biology 9, no. 7: 156. https://doi.org/10.3390/biology9070156
APA StyleDuffey, R. B., & Zio, E. (2020). CoVid-19 Pandemic Trend Modeling and Analysis to Support Resilience Decision-Making. Biology, 9(7), 156. https://doi.org/10.3390/biology9070156