
Feasibility of Multiplex Cytokine Profiling in Preterm Labor: Towards Biomarker Discovery
 , , , ,
, , , ,
Simple Summary
Abstract

1. Introduction
2. Results
2.1. Descriptive Characteristics of Population
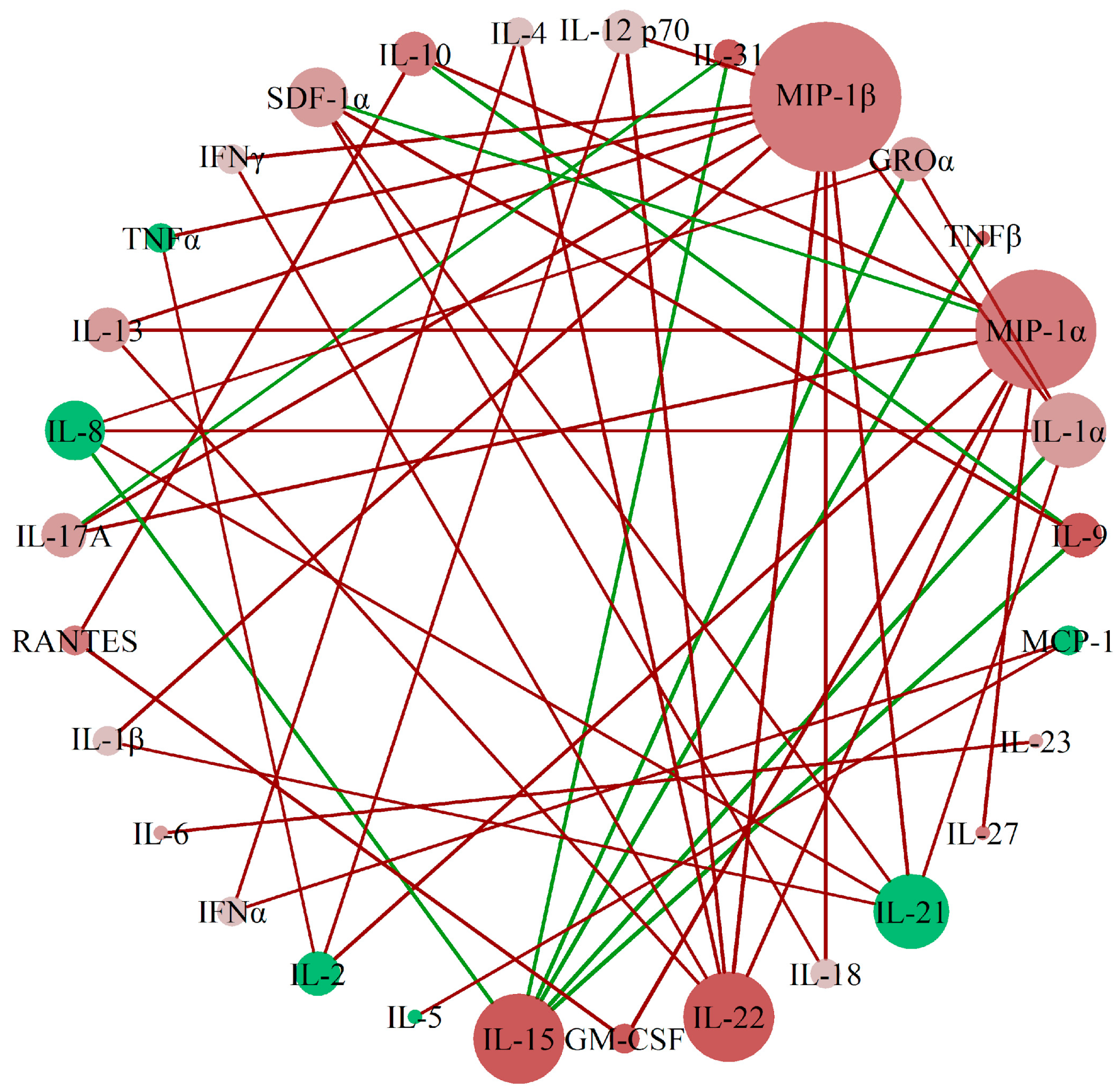
2.2. MIP-1β, MIP-1α, IL-15, and IL-22 Are Identified as Relevant Cytokines for Preterm Delivery
2.3. Urine IL-1β, IL-1Ra, IL-31, and IL-5 Levels Are Associated with Duration of Pregnancy
3. Discussion
4. Materials and Methods
4.1. Study Description and Population
4.2. Specimen Collection and Preparation
4.3. Cytokine Analysis
4.4. Statistical Analysis
4.4.1. Assessment of the Correlation Between Cytokine Levels in Preterm and Term Gestations
4.4.2. Assessment of the Influence of Gestational Age and Obstetric Features at the Time of Sample Collection
4.4.3. Assessment of the Association Between Cytokine Levels and Duration of Pregnancy
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| GAMLSS | Generalized Additive Models for Location, Scale, and Shape |
| GAM | Generalized Additive Models |
| AIC | Akaike Information Criterion |
| DGCA | Differential Gene Correlation Analysis |
| AMN | Amniocentesis |
| TPL | Threatened Preterm Labor |
| CSR | Cesarean |
References
- Ohuma, E.O.; Moller, A.-B.; Bradley, E.; Chakwera, S.; Hussain-Alkhateeb, L.; Lewin, A.; Okwaraji, Y.B.; Mahanani, W.R.; Johansson, E.W.; Lavin, T.; et al. National, Regional, and Global Estimates of Preterm Birth in 2020, with Trends from 2010: A Systematic Analysis. Lancet 2023, 402, 1261–1271. [Google Scholar] [CrossRef] [PubMed]
- Jacob, J.; Lehne, M.; Mischker, A.; Klinger, N.; Zickermann, C.; Walker, J. Cost Effects of Preterm Birth: A Comparison of Health Care Costs Associated with Early Preterm, Late Preterm, and Full-Term Birth in the First 3 Years after Birth. Eur. J. Health Econ. 2017, 18, 1041–1046. [Google Scholar] [CrossRef] [PubMed]
- Romero, R.; Dey, S.K.; Fisher, S.J. Preterm Labor: One Syndrome, Many Causes. Science 2014, 345, 760–765. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Lopez, N.; Galaz, J.; Miller, D.; Farias-Jofre, M.; Liu, Z.; Arenas-Hernandez, M.; Garcia-Flores, V.; Shaffer, Z.; Greenberg, J.M.; Theis, K.R.; et al. The Immunobiology of Preterm Labor and Birth: Intra-Amniotic Inflammation or Breakdown of Maternal–Fetal Homeostasis. Reproduction 2022, 164, R11–R45. [Google Scholar] [CrossRef]
- Gomez-Lopez, N.; Stlouis, D.; Lehr, M.A.; Sanchez-Rodriguez, E.N.; Arenas-Hernandez, M. Immune Cells in Term and Preterm Labor. Cell Mol. Immunol. 2014, 11, 571–581. [Google Scholar] [CrossRef]
- Wilson, A.; Hodgetts-Morton, V.A.; Marson, E.J.; Markland, A.D.; Larkai, E.; Papadopoulou, A.; Coomarasamy, A.; Tobias, A.; Chou, D.; Oladapo, O.T.; et al. Tocolytics for Delaying Preterm Birth: A Network Meta-Analysis (0924). Cochrane Database Syst. Rev. 2022, 2022, CD014978. [Google Scholar] [CrossRef]
- Hanley, M.; Sayres, L.; Reiff, E.S.; Wood, A.; Grotegut, C.A.; Kuller, J.A. Tocolysis: A Review of the Literature. Obs. Gynecol. Surv. 2019, 74, 50–55. [Google Scholar] [CrossRef]
- Meertens, L.J.E.; van Montfort, P.; Scheepers, H.C.J.; van Kuijk, S.M.J.; Aardenburg, R.; Langenveld, J.; van Dooren, I.M.A.; Zwaan, I.M.; Spaanderman, M.E.A.; Smits, L.J.M. Prediction Models for the Risk of Spontaneous Preterm Birth Based on Maternal Characteristics: A Systematic Review and Independent External Validation. Acta Obs. Gynecol. Scand. 2018, 97, 907–920. [Google Scholar] [CrossRef]
- Tarca, A.L.; Pataki, B.Á.; Romero, R.; Sirota, M.; Guan, Y.; Kutum, R.; Gomez-Lopez, N.; Done, B.; Bhatti, G.; Yu, T.; et al. Crowdsourcing Assessment of Maternal Blood Multi-Omics for Predicting Gestational Age and Preterm Birth. Cell Rep. Med. 2021, 2, 100323. [Google Scholar] [CrossRef]
- Saade, G.R.; Boggess, K.A.; Sullivan, S.A.; Markenson, G.R.; Iams, J.D.; Coonrod, D.V.; Pereira, L.M.; Esplin, M.S.; Cousins, L.M.; Lam, G.K.; et al. Development and Validation of a Spontaneous Preterm Delivery Predictor in Asymptomatic Women. Am. J. Obs. Gynecol. 2016, 214, 633.e1–633.e24. [Google Scholar] [CrossRef]
- Gupta, J.K.; Care, A.; Goodfellow, L.; Alfirevic, Z.; Lian, L.Y.; Müller-Myhsok, B.; Alfirevic, A.; Phelan, M.M. Metabolic Profiling of Maternal Serum of Women at High-Risk of Spontaneous Preterm Birth Using NMR and MGWAS Approach. Biosci. Rep. 2021, 41, BSR20210759. [Google Scholar] [CrossRef] [PubMed]
- Cantonwine, D.E.; Zhang, Z.; Rosenblatt, K.; Goudy, K.S.; Doss, R.C.; Ezrin, A.M.; Page, G.; Brohman, B.; McElrath, T.F. Evaluation of Proteomic Biomarkers Associated with Circulating Microparticles as an Effective Means to Stratify the Risk of Spontaneous Preterm Birth. Am. J. Obs. Gynecol. 2016, 214, 631.e1–631.e11. [Google Scholar] [CrossRef]
- Aung, M.T.; Yu, Y.; Ferguson, K.K.; Cantonwine, D.E.; Zeng, L.; McElrath, T.F.; Pennathur, S.; Mukherjee, B.; Meeker, J.D. Prediction and Associations of Preterm Birth and Its Subtypes with Eicosanoid Enzymatic Pathways and Inflammatory Markers. Sci. Rep. 2019, 9, 17049. [Google Scholar] [CrossRef]
- Rice, G.E. Cytokines and the Initiation of Parturition. Front. Horm. Res. 2001, 27, 113–146. [Google Scholar] [CrossRef]
- Svenvik, M.; Jenmalm, M.C.; Brudin, L.; Raffetseder, J.; Hellberg, S.; Axelsson, D.; Lindell, G.; Blomberg, M.; Ernerudh, J. Chemokine and Cytokine Profiles in Preterm and Term Labor, in Preterm Prelabor Rupture of the Membranes, and in Normal Pregnancy. J. Reprod. Immunol. 2024, 164, 104278. [Google Scholar] [CrossRef] [PubMed]
- Jarmund, A.H.; Giskeødegård, G.F.; Ryssdal, M.; Steinkjer, B.; Stokkeland, L.M.T.; Madssen, T.S.; Stafne, S.N.; Stridsklev, S.; Moholdt, T.; Heimstad, R.; et al. Cytokine Patterns in Maternal Serum From First Trimester to Term and Beyond. Front. Immunol. 2021, 12, 752660. [Google Scholar] [CrossRef] [PubMed]
- Park, S.; You, Y.-A.; Yun, H.; Choi, S.-J.; Hwang, H.-S.; Choi, S.-K.; Lee, S.M.; Kim, Y.J. Cervicovaginal Fluid Cytokines as Predictive Markers of Preterm Birth in Symptomatic Women. Obs. Gynecol. Sci. 2020, 63, 455–463. [Google Scholar] [CrossRef]
- Sirera, R.; Salvador, A.; Roldán, I.; Talens, R.; González-Molina, A.; Rivera, M. Quantification of Proinflammatory Cytokines in the Urine of Congestive Heart Failure Patients. Its Relationship with Plasma Levels. Eur. J. Heart Fail. 2003, 5, 27–31. [Google Scholar] [CrossRef]
- Liu, C.; Chu, D.; Kalantar-Zadeh, K.; George, J.; Young, H.A.; Liu, G. Cytokines: From Clinical Significance to Quantification. Adv. Sci. 2021, 8, 2004433. [Google Scholar] [CrossRef]
- Purohit, S.; Sharma, A.; She, J.-X. Luminex and Other Multiplex High Throughput Technologies for the Identification of, and Host Response to, Environmental Triggers of Type 1 Diabetes. Biomed. Res. Int. 2015, 2015, 326918. [Google Scholar] [CrossRef]
- Hartmann, F.J.; Bendall, S.C. Immune Monitoring Using Mass Cytometry and Related High-Dimensional Imaging Approaches. Nat. Rev. Rheumatol. 2020, 16, 87–99. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, M.; Johnson, K. Data Pre-Processing. In Applied Predictive Modeling; Kuhn, M., Johnson, K., Eds.; Springer: New York, NY, USA, 2013; pp. 27–59. ISBN 978-1-4614-6849-3. [Google Scholar]
- Voudouris, V.; Gilchrist, R.; Rigby, R.; Sedgwick, J.; Stasinopoulos, D. Modelling Skewness and Kurtosis with the BCPE Density in GAMLSS. J. Appl. Stat. 2012, 39, 1279–1293. [Google Scholar] [CrossRef]
- Dudley, D.J.; Spencer, S.; Edwin, S.; Mitchell, M.D. Regulation of Human Decidual Cell Macrophage Inflammatory Protein-1α (MIP-1α) Production by Inflammatory Cytokines. Am. J. Reprod. Immunol. 1995, 34, 231–235. [Google Scholar] [CrossRef]
- Guan, S.; Bai, X.; Ding, J.; Zhuang, R. Circulating Inflammatory Cytokines and Hypertensive Disorders of Pregnancy: A Two-Sample Mendelian Randomization Study. Front. Immunol. 2023, 14, 1297929. [Google Scholar] [CrossRef]
- Rossol, M.; Heine, H.; Meusch, U.; Quandt, D.; Klein, C.; Sweet, M.J.; Hauschildt, S. LPS-Induced Cytokine Production in Human Monocytes and Macrophages. Crit. Rev. Trade Immunol. 2011, 31, 379–446. [Google Scholar] [CrossRef] [PubMed]
- Toth, B.; Haufe, T.; Scholz, C.; Kuhn, C.; Friese, K.; Karamouti, M.; Makrigiannakis, A.; Jeschke, U. Placental Interleukin-15 Expression in Recurrent Miscarriage. Am. J. Reprod. Immunol. 2010, 64, 402–410. [Google Scholar] [CrossRef]
- Hansson, M.; Silverpil, E.; Lindén, A.; Glader, P. Interleukin-22 Produced by Alveolar Macrophages during Activation of the Innate Immune Response. Inflamm. Res. 2013, 62, 561–569. [Google Scholar] [CrossRef]
- Gershater, M.; Romero, R.; Arenas-Hernandez, M.; Galaz, J.; Motomura, K.; Tao, L.; Xu, Y.; Miller, D.; Pique-Regi, R.; Martinez, G.; et al. IL-22 Plays a Dual Role in the Amniotic Cavity: Tissue Injury and Host Defense against Microbes in Preterm Labor. J. Immunol. 2022, 208, 1595–1615. [Google Scholar] [CrossRef]
- Jha, P.; Raghu, P.; Kennedy, A.M.; Sugi, M.; Morgan, T.A.; Feldstein, V.; Pōder, L.; Penna, R. Assessment of Amniotic Fluid Volume in Pregnancy. RadioGraphics 2023, 43, e220146. [Google Scholar] [CrossRef]
- Kennedy, C.E.; Yeh, P.T.; Gholbzouri, K.; Narasimhan, M. Self-Testing for Pregnancy: A Systematic Review and Meta-Analysis. BMJ Open 2022, 12, e054120. [Google Scholar] [CrossRef]
- Burdet, J.; Sacerdoti, F.; Cella, M.; Franchi, A.M.; Ibarra, C. Role of TNF-α in the Mechanisms Responsible for Preterm Delivery Induced by Stx2 in Rats. Br. J. Pharmacol. 2013, 168, 946–953. [Google Scholar] [CrossRef]
- Li, W.; Zhao, X.; Li, S.; Chen, X.; Cui, H.; Chang, Y.; Zhang, R. Upregulation of TNF-α and IL-6 Induces Preterm Premature Rupture of Membranes by Activation of ADAMTS-9 in Embryonic Membrane Cells. Life Sci. 2020, 260, 118237. [Google Scholar] [CrossRef]
- Peng, J.; Jiang, J.; Wang, H.; Feng, X.; Dong, X. MiR-199a-3p Suppresses Cervical Epithelial Cell Inflammation by Inhibiting the HMGB1/TLR4/NF-κB Pathway in Preterm Birth. Mol. Med. Rep. 2020, 22, 926–938. [Google Scholar] [CrossRef]
- Owen, J.C.; Garrick, S.P.; Peterson, B.M.; Berger, P.J.; Nold, M.F.; Sehgal, A.; Nold-Petry, C.A. The Role of Interleukin-1 in Perinatal Inflammation and Its Impact on Transitional Circulation. Front. Pediatr. 2023, 11, 1130013. [Google Scholar] [CrossRef] [PubMed]
- Ma, J.; Chen, T.; Mandelin, J.; Ceponis, A.; Miller, N.E.; Hukkanen, M.; Ma, G.F.; Konttinen, Y.T. Regulation of Macrophage Activation. Cell Mol. Life Sci. 2003, 60, 2334–2346. [Google Scholar] [CrossRef]
- Nadeau-Vallée, M.; Obari, D.; Quiniou, C.; Lubell, W.D.; Olson, D.M.; Girard, S.; Chemtob, S. A Critical Role of Interleukin-1 in Preterm Labor. Cytokine Growth Factor. Rev. 2016, 28, 37–51. [Google Scholar] [CrossRef] [PubMed]
- Milacic, M.; Beavers, D.; Conley, P.; Gong, C.; Gillespie, M.; Griss, J.; Haw, R.; Jassal, B.; Matthews, L.; May, B.; et al. The Reactome Pathway Knowledgebase 2024. Nucleic Acids Res. 2024, 52, D672–D678. [Google Scholar] [CrossRef] [PubMed]
- Alfirevic, Z.; Navaratnam, K.; Mujezinovic, F. Amniocentesis and Chorionic Villus Sampling for Prenatal Diagnosis. Cochrane Database Syst. Rev. 2017, 2017, CD003252. [Google Scholar] [CrossRef]
- Dahlquist, K.; Stuart, A.; Källén, K. Planned Cesarean Section vs Planned Vaginal Delivery among Women without Formal Medical Indication for Planned Cesarean Section: A Retrospective Cohort Study of Maternal Short-term Complications. Acta Obs. Gynecol. Scand. 2022, 101, 1026–1032. [Google Scholar] [CrossRef]
- Vosoughian, M.; Dahi, M.; Dabir, S.; Moshari, M.; Tabashi, S.; Mosavi, Z. Effects of General Anesthesia Versus Spinal Anesthesia on Serum Cytokine Release After Cesarean Section: A Randomized Clinical Trial. Anesth. Pain. Med. 2021, 11, e111272. [Google Scholar] [CrossRef]
- Rigby, R.A.; Stasinopoulos, D.M. Generalized Additive Models for Location, Scale and Shape. J. R. Stat. Soc. Ser. C Appl. Stat. 2005, 54, 507–554. [Google Scholar] [CrossRef]
- Wood, S.N. Generalized Additive Models; Chapman and Hall/CRC: New York, NY, USA, 2017; ISBN 9781315370279. [Google Scholar]
- Kosmidis, I.; Firth, D. A Generic Algorithm for Reducing Bias in Parametric Estimation. Electron. J. Stat. 2010, 4, 1097–1112. [Google Scholar] [CrossRef]
- McKenzie, A.T.; Katsyv, I.; Song, W.-M.; Wang, M.; Zhang, B. DGCA: A Comprehensive R Package for Differential Gene Correlation Analysis. BMC Syst. Biol. 2016, 10, 106. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021; Available online: https://www.R-project.org (accessed on 11 June 2025).
- Romero, R.; Grivel, J.-C.; Tarca, A.L.; Chaemsaithong, P.; Xu, Z.; Fitzgerald, W.; Hassan, S.S.; Chaiworapongsa, T.; Margolis, L. Evidence of Perturbations of the Cytokine Network in Preterm Labor. Am. J. Obs. Gynecol. 2015, 213, 836.e1–836.e18. [Google Scholar] [CrossRef]
- Sheskin, D.J. Handbook of Parametric and Nonparametric Statistical Procedures; Chapman and Hall/CRC: New York, NY, USA, 2020; ISBN 9780429186196. [Google Scholar]
- Benjamini, Y.; Hochberg, Y. Controlling the False Discovery Rate: A Practical and Powerful Approach to Multiple Testing. J. R. Stat. Soc. Ser. B Stat. Methodol. 1995, 57, 289–300. [Google Scholar] [CrossRef]
- Eilers, P.H.C.; Marx, B.D. Flexible Smoothing with B-Splines and Penalties. Stat. Sci. 1996, 11, 89–121. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Criteria | AMN Group (N = 34) | TPL Group (N = 16) | CSR Group (N = 29) |
|---|---|---|---|
| Age (years) | 38.7 (2.7) | 32.2 (3.7) | 35.3 (4.8) |
| Weight (kg) | 67.1 (10.2) | 65.3 (7.6) | 77.7 (13.5) |
| Height (m) | 1.63 (0.06) | 1.61 (0.03) | 1.62 (0.07) |
| Body mass index (kg/m2) | 25.4 (4.2) | 25.2 (3.0) | 29.8 (5.1) |
| Smoking patients (n) | 5 (14.7) | 2 (12.5) | 4 (13.8) |
| Obstetrical Characteristics | AMN Group (N = 34) | TPL Group (N = 16) | CSR Group (N = 29) | Total (N = 79) | p Value |
|---|---|---|---|---|---|
| Time to delivery (weeks) | 23.2 (1.9) | 7.1 (3.6) | 0.0 (0.0) | - | |
| Amenorrhea at sampling (weeks) | 16.2 (0.8) | 30.3 (2.6) | 39.0 (0.9) | - | |
| Amenorrhea at delivery (weeks) | 39.5 (1.9) | 37.5 (3.8) | 39.0 (0.9) | - | |
| Number of previous gestations (n) | 0.696 | ||||
| 0 | 11 (32.4) | 8 (50.0) | 12 (41.4) | 31 (39.2) | |
| 1 | 13 (38.2) | 7 (43.8) | 9 (31.0) | 29 (36.7) | |
| 2 | 4 (11.8) | 0 (0.0) | 5 (17.2) | 9 (11.4) | |
| 3 | 3 (8.8) | 1 (6.2) | 2 (6.9) | 6 (7.6) | |
| 4 | 1 (2.9) | 0 (0.0) | 1 (3.4) | 2 (2.5) | |
| 5 | 2 (5.9) | 0 (0.0) | 0 (0.0) | 2 (2.5) | |
| Parturition type I (n) | 0.002 | ||||
| At term | 26 (76.5) | 13 (81.2) | 0 (0.0) | 39 (49.4) | |
| Preterm | 2 (5.9) | 3 (18.8) | 0 (0.0) | 5 (6.3) | |
| Cesarean | 6 (17.6) | 0 (0.0) | 29 (100.0) | 35 (44.3) | |
| Parturition type II (n) | 0.038 | ||||
| Nonpremature | 32 (94.1) | 13 (81.2) | 29 (100.0) | 74 (93.7) | |
| Premature | 2 (5.9) | 3 (18.8) | 0 (0.0) | 5 (6.3) | |
| Number of previous parturitions (n) | 0.076 | ||||
| 0 | 16 (47.1) | 9 (56.2) | 25 (86.2) | 50 (63.3) | |
| 1 | 14 (41.2) | 6 (37.5) | 3 (10.3) | 23 (29.1) | |
| 2 | 3 (8.8) | 1 (6.2) | 1 (3.4) | 5 (6.3) | |
| 3 | 1 (2.9) | 0 (0.0) | 0 (0.0) | 1 (1.3) | |
| Type of previous parturitions (n) | 0.453 | ||||
| At term | 19 (95.0) | 6 (85.7) | 13 (86.7) | 38 (90.5) | |
| Preterm | 1 (5.0) | 1 (14.3) | 2 (13.3) | 4 (9.5) | |
| Number of previous cesarean deliveries (n) | 0.009 | ||||
| 0 | 31 (91.2) | 16 (100.0) | 18 (62.1) | 65 (82.3) | |
| 1 | 2 (5.9) | 0 (0.0) | 9 (31.0) | 11 (13.9) | |
| 2 | 1 (2.9) | 0 (0.0) | 2 (6.9) | 3 (3.8) | |
| Number of previous abortions (excluding induced abortions) (n) | 0.669 | ||||
| 0 | 23 (67.6) | 14 (87.5) | 24 (82.8) | 61 (77.2) | |
| 1 | 8 (23.5) | 2 (12.5) | 3 (10.3) | 13 (16.5) | |
| 2 | 1 (2.9) | 0 (0.0) | 1 (3.4) | 2 (2.5) | |
| 3 | 2 (5.9) | 0 (0.0) | 1 (3.4) | 3 (1.3) | |
| Number of induced abortions (n) | 0.685 | ||||
| 0 | 33 (97.1) | 16 (100.0) | 27 (93.1) | 76 (96.2) | |
| 1 | 1 (2.9) | 0 (0.0) | 1 (3.4) | 2 (2.5) | |
| 3 | 0 (0.0) | 0 (0.0) | 1 (3.4) | 1 (1.3) | |
| Type of previous abortions (n) | 0.371 | ||||
| Early | 10 (90.9) | 1 (50.0) | 5 (71.4) | 16 (80.0) | |
| Late | 1 (9.1) | 1 (50.0) | 2 (28.6) | 4 (20.0) | |
| Number of uterine curettages (n) | 0.928 | ||||
| 0 | 28 (82.4) | 14 (87.5) | 24 (82.8) | 66 (83.5) | |
| 1 | 4 (11.8) | 2 (12.5) | 4 (13.8) | 10 (12.7) | |
| 2 | 1 (2.9) | 0 (0.0) | 0 (0.0) | 1 (1.3) | |
| 3 | 1 (2.9) | 0 (0.0) | 1 (3.4) | 2 (2.5) | |
| Number of previous amniocenteses (n) | 0.002 | ||||
| 0 | 0 (0.0) | 14 (87.5) | 26 (89.7) | 40 (50.6) | |
| 1 | 34 (100.0) | 2 (12.5) | 3 (10.3) | 39 (49.4) |
| AMN Group (N = 34) | TPL Group (N = 16) | CSR Group (N = 29) | |
|---|---|---|---|
| Inclusion criteria | |||
| Common to all groups | Pregnant women of legal age Expressed voluntary and informed consent | ||
| Category-specific | |||
| Patient stratification | Patients subjected to amniocentesis for prenatal diagnosis | Patients diagnosed with threatened preterm labor | Patients who underwent cesarean delivery at term |
| Gestational week range | 14 + 5 to 18 | 24 + 0 to 34 + 6 | 37 + 0 to 42 + 0 |
| Exclusion criteria | |||
| Common to all groups | Patients carrying infectious or autoimmune diseases Patients being treated with corticoids, immunosuppressants or NSAIDs Hypertensive states of pregnancy Treatment with antimicrobial drugs Feverish condition Gestational diabetes Twin gestations | ||
| Category-specific | |||
| Patient conditions at the time of sample collection | Premature rupture of membranes Not eligible for uterine contraction inhibition treatment | Premature rupture of membranes Labor | |
| Obstetric conditions at the time of sample collection | Fetal chromosomal alterations Fetal malformations | Mullerian malformations Hydramnios Known cervical incompetence | |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Llano, R.; Ardao, I.; Brea, J.M.; Romero, L.; Pata, M.P.; Martínez, A.L.; Macía, M.; Loza, M.I. Feasibility of Multiplex Cytokine Profiling in Preterm Labor: Towards Biomarker Discovery. Biology 2025, 14, 714. https://doi.org/10.3390/biology14060714
Llano R, Ardao I, Brea JM, Romero L, Pata MP, Martínez AL, Macía M, Loza MI. Feasibility of Multiplex Cytokine Profiling in Preterm Labor: Towards Biomarker Discovery. Biology. 2025; 14(6):714. https://doi.org/10.3390/biology14060714
Chicago/Turabian StyleLlano, Ruth, Inés Ardao, José Manuel Brea, Luz Romero, María P. Pata, Antón L. Martínez, Manuel Macía, and María Isabel Loza. 2025. "Feasibility of Multiplex Cytokine Profiling in Preterm Labor: Towards Biomarker Discovery" Biology 14, no. 6: 714. https://doi.org/10.3390/biology14060714
APA StyleLlano, R., Ardao, I., Brea, J. M., Romero, L., Pata, M. P., Martínez, A. L., Macía, M., & Loza, M. I. (2025). Feasibility of Multiplex Cytokine Profiling in Preterm Labor: Towards Biomarker Discovery. Biology, 14(6), 714. https://doi.org/10.3390/biology14060714