
Improved Boron Neutron Capture Therapy Using Integrin αvβ3-Targeted Long-Retention-Type Boron Carrier in a F98 Rat Glioma Model
 , , , , ,
, , , , ,  , and
, and
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Boron Carriers
2.2. Cell Culture
2.3. F98 Glioma-Bearing Rat Brain Tumor Model
2.4. In Vitro Cellular Uptake Experiments
2.5. In Vitro Neutron-Irradiation Experiments
2.6. Biodistribution of Boron in the F98 Glioma-Bearing Rats after Intravenous Administration of Each Boron Carrier
2.7. Survival Analysis of the In Vivo Neutron-Irradiation Experiments
2.8. Estimated Physical Dose and Biologically Photon-Equivalent Dose
2.9. Statistical Analysis
3. Results
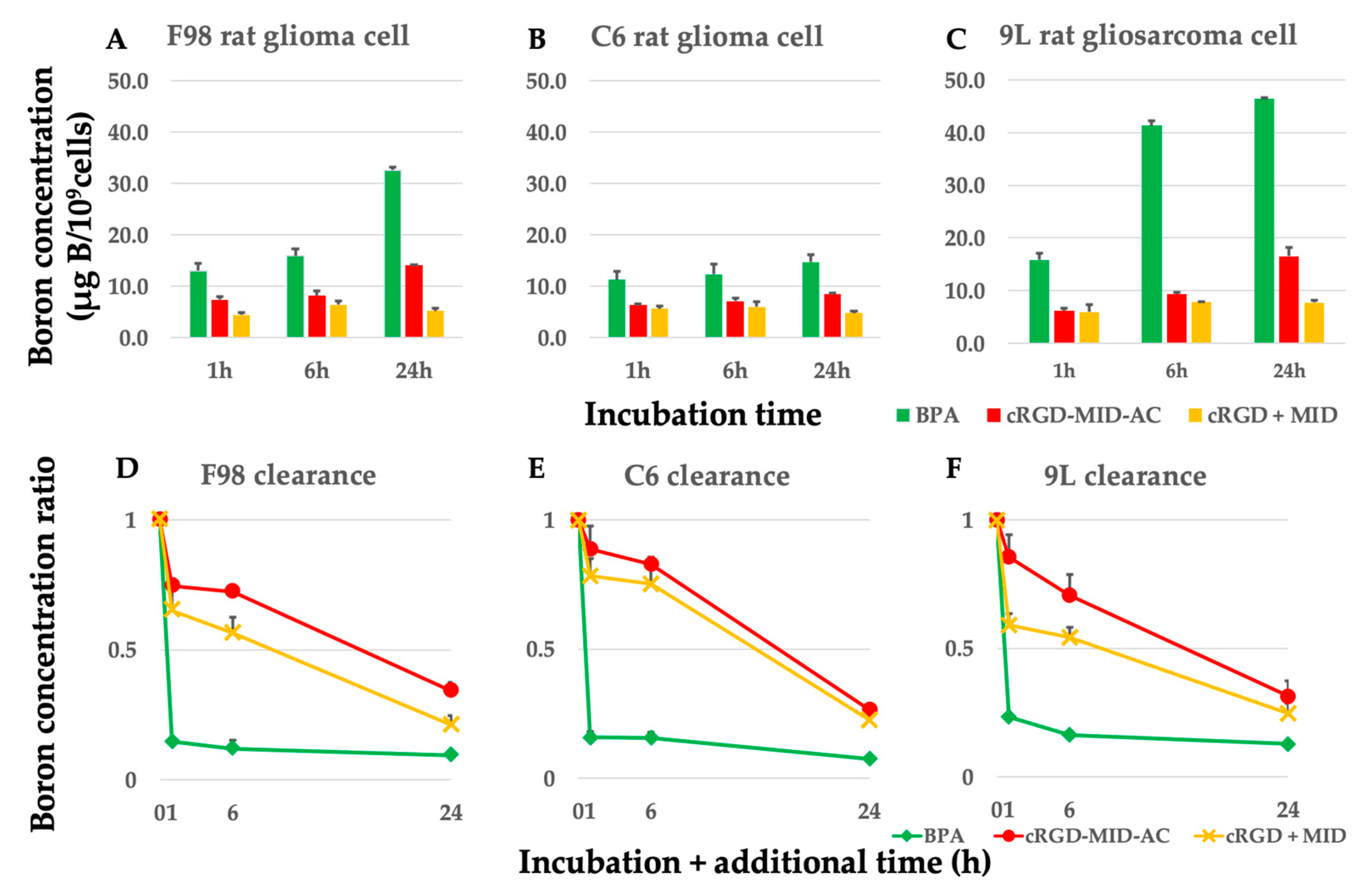
3.1. In Vitro Cellular Boron Uptake Experiments in F98, C6 Glioma, and 9L Gliosarcoma Cells
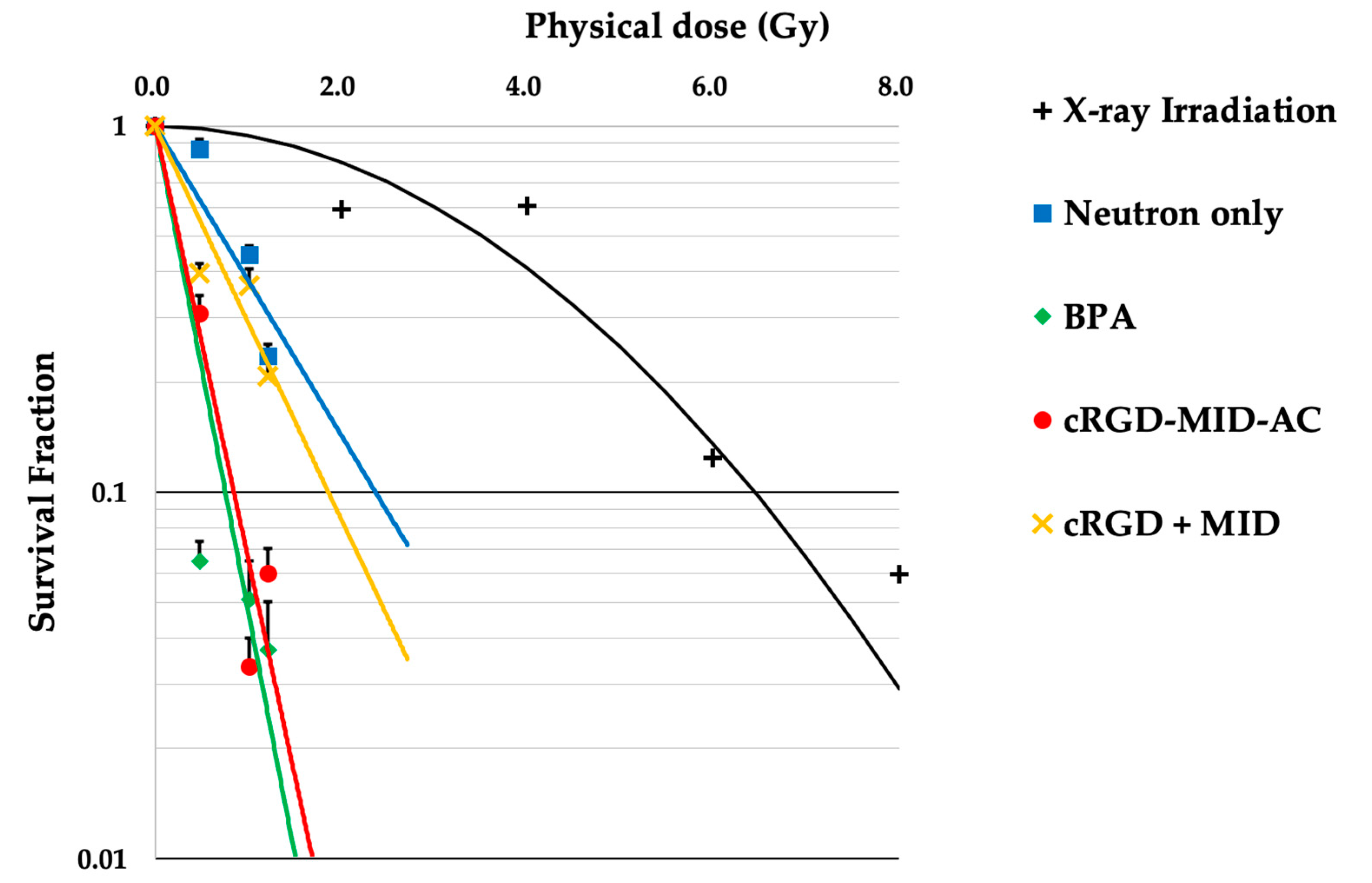
3.2. Neutron Irradiation in the In Vitro Experiments
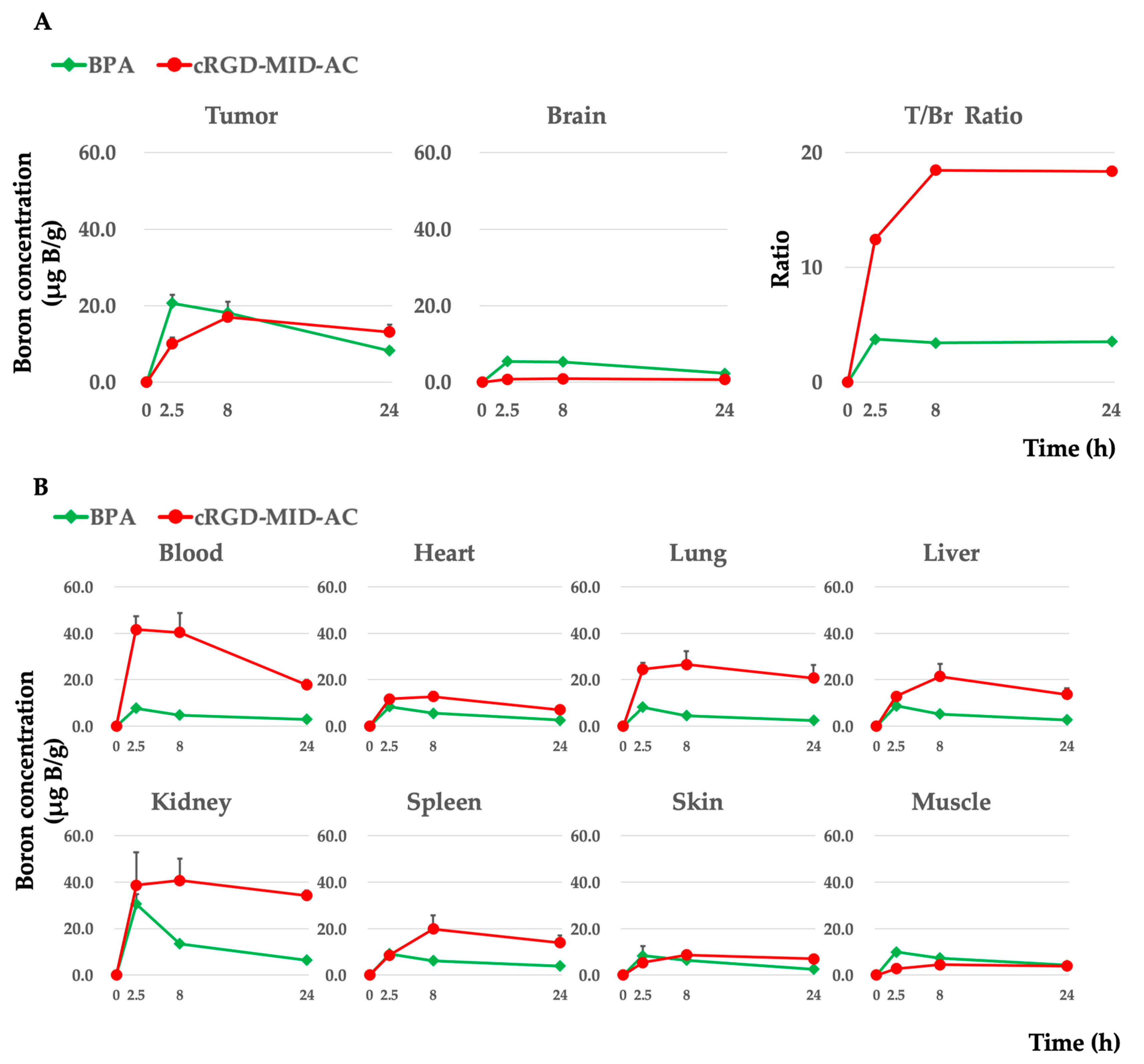
3.3. Biodistribution of Boron in the F98 Glioma-Bearing Rats after Intravenous Administration of Each Boron Carrier
3.4. Survival Analysis of the In Vivo Neutron-Irradiation Experiments
3.5. Estimation of Physical and Biologically Photon-Equivalent Doses
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Boron Carrier a | Boron Concentration (µg B/109 Cells) ± SD b | |||||
|---|---|---|---|---|---|---|
| 1 h | 6 h | 24 h | 24 + 1 h | 24 + 6 h | 24 + 24 h | |
| BPA | 12.9 ± 1.4 | 15.8 ± 1.4 | 32.6 ± 0.6 | 4.8 ± 0.2 | 3.9 ± 1.1 | 3.1 ± 0.5 |
| cRGD-MID-AC | 7.3 ± 0.6 | 8.1 ± 1.0 | 14.0 ± 0.1 | 10.5 ± 0.4 | 10.1 ± 0.2 | 4.8 ± 0.4 |
| cRGD + MID | 4.3 ± 0.5 | 6.4 ± 0.7 | 5.1 ± 0.5 | 3.3 ± 0.3 | 2.9 ± 0.04 | 1.1 ± 0.1 |
| Boron Carrier a | Boron Concentration (µg B/109 Cells) ± SD b | |||||
|---|---|---|---|---|---|---|
| 1 h | 6 h | 24 h | 24 + 1 h | 24 + 6 h | 24 + 24 h | |
| BPA | 11.2 ± 1.6 | 12.3 ± 2.1 | 14.7 ± 1.5 | 2.31 ± 0.1 | 2.29 ± 0.1 | 1.1 ± 0.1 |
| cRGD-MID-AC | 6.3 ± 0.3 | 7.1 ± 0.5 | 8.4 ± 0.2 | 7.5 ± 1.1 | 7.0 ± 1.1 | 2.2 ± 0.1 |
| cRGD + MID | 5.6 ± 0.6 | 6.0 ± 1.0 | 4.8 ± 0.3 | 3.7 ± 0.3 | 3.6 ± 0.2 | 1.1 ± 0.03 |
| Boron Carrier a | Boron Concentration (µg B/109 Cells) ± SD b | |||||
|---|---|---|---|---|---|---|
| 1 h | 6 h | 24 h | 24 + 1 h | 24 + 6 h | 24 + 24 h | |
| BPA | 15.8 ± 1.3 | 41.3 ± 0.9 | 46.4 ± 0.2 | 10.8 ± 0.3 | 7.6 ± 0.7 | 5.9 ± 0.3 |
| cRGD-MID-AC | 6.1 ± 0.5 | 9.4 ± 0.4 | 16.5 ± 1.6 | 14.2 ± 1.5 | 11.7 ± 0.9 | 5.2 ± 0.7 |
| cRGD + MID | 6.0 ± 1.4 | 7.9 ± 0.1 | 7.8 ± 0.4 | 4.6 ± 0.2 | 4.2 ± 0.1 | 1.9 ± 0.2 |
References
- Stupp, R.; Hegi, M.E.; Mason, W.P.; Van Den Bent, M.J.; Taphoorn, M.J.; Janzer, R.C.; Ludwin, S.K.; Allgeier, A.; Fisher, B.; Belanger, K.; et al. Effects of radiotherapy with concomitant and adjuvant temozolomide versus radiotherapy alone on survival in glioblastoma in a randomised phase III study: 5-year analysis of the EORTC-NCIC trial. Lancet Oncol. 2009, 10, 459–466. [Google Scholar] [CrossRef]
- Kawabata, S.; Miyatake, S.-I.; Kuroiwa, T.; Yokoyama, K.; Doi, A.; Iida, K.; Miyata, S.; Nonoguchi, N.; Michiue, H.; Takahashi, M.; et al. Boron Neutron Capture Therapy for Newly Diagnosed Glioblastoma. J. Radiat. Res. 2009, 50, 51–60. [Google Scholar] [CrossRef]
- Henriksson, R.; Capala, J.; Michanek, A.; Lindahl, S.A.; Salford, L.G.; Franzén, L.; Blomquist, E.; Westlin, J.E.; Bergenheim, A.T. Boron neutron capture therapy (BNCT) for glioblastoma multiforme: A phase II study evaluating a prolonged high-dose of boronophenylalanine (BPA). Radiother. Oncol. 2008, 88, 183–191. [Google Scholar] [CrossRef]
- Yamamoto, T.; Nakai, K.; Kageji, T.; Kumada, H.; Endo, K.; Matsuda, M.; Shibata, Y.; Matsumura, A. Boron neutron capture therapy for newly diagnosed glioblastoma. Radiother. Oncol. 2009, 91, 80–84. [Google Scholar] [CrossRef]
- Sköld, K.; Gorlia, T.; Pellettieri, L.; Giusti, V.; H-Stenstam, B.; Hopewell, J.W. Boron neutron capture therapy for newly diagnosed glioblastoma multiforme: An assessment of clinical potential. Br. J. Radiol. 2010, 83, 596–603. [Google Scholar] [CrossRef]
- Miyatake, S.-I.; Kawabata, S.; Yokoyama, K.; Kuroiwa, T.; Michiue, H.; Sakurai, Y.; Kumada, H.; Suzuki, M.; Maruhashi, A.; Kirihata, M.; et al. Survival benefit of Boron neutron capture therapy for recurrent malignant gliomas. J. Neuro Oncol. 2009, 91, 199–206. [Google Scholar] [CrossRef]
- Pellettieri, L.; H-Stenstam, B.; Rezaei, A.; Giusti, V.; Sköld, K. An investigation of boron neutron capture therapy for recurrent glioblastoma multiforme. Acta Neurol. Scand. 2008, 117, 191–197. [Google Scholar] [CrossRef]
- Kawabata, S.; Suzuki, M.; Hirose, K.; Tanaka, H.; Kato, T.; Goto, H.; Narita, Y.; Miyatake, S.-I. Accelerator-based BNCT for patients with recurrent glioblastoma: A multicenter phase II study. Neuro Oncol. Adv. 2021, 3, vdab067. [Google Scholar] [CrossRef]
- Hirose, K.; Konno, A.; Hiratsuka, J.; Yoshimoto, S.; Kato, T.; Ono, K.; Otsuki, N.; Hatazawa, J.; Tanaka, H.; Takayama, K.; et al. Boron neutron capture therapy using cyclotron-based epithermal neutron source and borofalan (10B) for recurrent or locally advanced head and neck cancer (JHN002): An open-label phase II trial. Radiother. Oncol. 2021, 155, 182–187. [Google Scholar] [CrossRef]
- Wittig, A.; Sauerwein, W.A.; Coderre, J.A. Mechanisms of transport of p-borono-phenylalanine through the cell membrane in vitro. Radiat. Res. 2000, 153, 173–180. [Google Scholar] [CrossRef]
- Ono, K.; Masunaga, S.-I.; Kinashi, Y.; Takagaki, M.; Akaboshi, M.; Kobayashi, T.; Akuta, K. Radiobiological evidence suggesting heterogeneous microdistribution of boron compounds in tumors: Its relation to quiescent cell population and tumor cure in neutron capture therapy. Int. J. Radiat. Oncol. Biol. Phys. 1996, 34, 1081–1086. [Google Scholar] [CrossRef]
- Smith, D.R.; Chandra, S.; Coderre, J.A.; Morrison, G.H. Ion microscopy imaging of 10B from p-boronophenylalanine in a brain tumor model for boron neutron capture therapy. Cancer Res. 1996, 56, 4302–4306. [Google Scholar]
- Yokoyama, K.; Miyatake, S.-I.; Kajimoto, Y.; Kawabata, S.; Doi, A.; Yoshida, T.; Okabe, M.; Kirihata, M.; Ono, K.; Kuroiwa, T. Analysis of boron distribution in vivo for boron neutron capture therapy using two different boron compounds by secondary ion mass spectrometry. Radiat. Res. 2007, 167, 102–109. [Google Scholar] [CrossRef]
- Yoshida, F.; Matsumura, A.; Shibata, Y.; Yamamoto, T.; Nakauchi, H.; Okumura, M.; Nose, T. Cell cycle dependence of boron uptake from two boron compound used for clinical neutron capture therapy. Cancer Lett. 2002, 187, 135–141. [Google Scholar] [CrossRef]
- Capala, J.; Stenstam, B.H.; Sköld, K.; Munck af Rosenschöld, P.; Giusti, V.; Persson, C.; Wallin, E.; Brun, A.; Franzen, L.; Carlsson, J.; et al. Boron neutron capture therapy for glioblastoma multiforme: Clinical studies in Sweden. J. Neuro Oncol. 2003, 62, 135–144. [Google Scholar] [CrossRef]
- Kashiwagi, H.; Kawabata, S.; Yoshimura, K.; Fukuo, Y.; Kanemitsu, T.; Takeuchi, K.; Hiramatsu, R.; Nishimura, K.; Kawai, K.; Takata, T.; et al. Boron neutron capture therapy using dodecaborated albumin conjugates with maleimide is effective in a rat glioma model. Investig. New Drugs 2022, 40, 255–264. [Google Scholar] [CrossRef]
- Lin, T.; Zhao, P.; Jiang, Y.; Tang, Y.; Jin, H.; Pan, Z.; He, H.; Yang, V.C.; Huang, Y. Blood-Brain-Barrier-Penetrating Albumin Nanoparticles for Biomimetic Drug Delivery via Albumin-Binding Protein Pathways for Antiglioma Therapy. ACS Nano 2016, 10, 9999–10012. [Google Scholar] [CrossRef]
- Elsadek, B.; Kratz, F. Impact of albumin on drug delivery—New applications on the horizon. J. Control. Release 2012, 157, 4–28. [Google Scholar] [CrossRef]
- Kikuchi, S.; Kanoh, D.; Sato, S.; Sakurai, Y.; Suzuki, M.; Nakamura, H. Maleimide-functionalized closo-dodecaborate albumin conjugates (MID-AC): Unique ligation at cysteine and lysine residues enables efficient boron delivery to tumor for neutron capture therapy. J. Control. Release 2016, 237, 160–167. [Google Scholar] [CrossRef]
- Malric, L.; Monferran, S.; Gilhodes, J.; Boyrie, S.; Dahan, P.; Skuli, N.; Sesen, J.; Filleron, T.; Kowalski-Chauvel, A.; Moyal, E.C.-J.; et al. Interest of integrins targeting in glioblastoma according to tumor heterogeneity and cancer stem cell paradigm: An update. Oncotarget 2017, 8, 86947–86968. [Google Scholar] [CrossRef]
- Ellert-Miklaszewska, A.; Poleszak, K.; Pasierbinska, M.; Kaminska, B. Integrin Signaling in Glioma Pathogenesis: From Biology to Therapy. Int. J. Mol. Sci. 2020, 21, 888. [Google Scholar] [CrossRef]
- Burgett, M.E.; Lathia, J.D.; Roth, P.; Nowacki, A.S.; Galileo, D.S.; Pugacheva, E.; Huang, P.; Vasanji, A.; Li, M.; Byzova, T.; et al. Direct contact with perivascular tumor cells enhances integrin alphavbeta3 signaling and migration of endothelial cells. Oncotarget 2016, 7, 43852–43867. [Google Scholar] [CrossRef]
- Schnell, O.; Krebs, B.; Wagner, E.; Romagna, A.; Beer, A.J.; Grau, S.J.; Thon, N.; Goetz, C.; Kretzschmar, H.A.; Tonn, J.C.; et al. Expression of integrin alphavbeta3 in gliomas correlates with tumor grade and is not restricted to tumor vasculature. Brain Pathol. 2008, 18, 378–386. [Google Scholar] [CrossRef]
- Ruoslahti, E. RGD and other recognition sequences for integrins. Annu. Rev. Cell Dev. Biol. 1996, 12, 697–715. [Google Scholar] [CrossRef]
- Schnell, O.; Krebs, B.; Carlsen, J.; Miederer, I.; Goetz, C.; Goldbrunner, R.H.; Wester, H.J.; Haubner, R.; Pöpperl, G.; Holtmannspötter, M.; et al. Imaging of integrin alpha(v)beta(3) expression in patients with malignant glioma by [18F] Galacto-RGD positron emission tomography. Neuro Oncol. 2009, 11, 861–870. [Google Scholar] [CrossRef]
- Miura, Y.; Takenaka, T.; Toh, K.; Wu, S.; Nishihara, H.; Kano, M.R.; Ino, Y.; Nomoto, T.; Matsumoto, Y.; Koyama, H.; et al. Cyclic RGD-linked polymeric micelles for targeted delivery of platinum anticancer drugs to glioblastoma through the blood-brain tumor barrier. ACS Nano 2013, 7, 8583–8592. [Google Scholar] [CrossRef]
- Chen, C.; Duan, Z.; Yuan, Y.; Li, R.; Pang, L.; Liang, J.; Xu, X.; Wang, J. Peptide-22 and Cyclic RGD Functionalized Liposomes for Glioma Targeting Drug Delivery Overcoming BBB and BBTB. ACS Appl. Mater. Interfaces 2017, 9, 5864–5873. [Google Scholar] [CrossRef]
- Temming, K.; Schiffelers, R.M.; Molema, G.; Kok, R.J. RGD-based strategies for selective delivery of therapeutics and imaging agents to the tumour vasculature. Drug Resist. Updates 2005, 8, 381–402. [Google Scholar] [CrossRef]
- Kawai, K.; Nishimura, K.; Okada, S.; Sato, S.; Suzuki, M.; Takata, T.; Nakamura, H. Cyclic RGD-Functionalized closo-Dodecaborate Albumin Conjugates as Integrin Targeting Boron Carriers for Neutron Capture Therapy. Mol. Pharm. 2020, 17, 3740–3747. [Google Scholar] [CrossRef]
- Ishii, S.; Sato, S.-I.; Asami, H.; Hasegawa, T.; Kohno, J.-Y.; Nakamura, H. Design of S-S bond containing maleimide-conjugated closo-dodecaborate (SSMID): Identification of unique modification sites on albumin and investigation of intracellular uptake. Org. Biomol. Chem. 2019, 17, 5496–5499. [Google Scholar] [CrossRef]
- Coderre, J.A.; Button, T.M.; Micca, P.L.; Fisher, C.D.; Nawrocky, M.M.; Liu, H.B. Neutron capture therapy of the 9L rat gliosarcoma using the p-boronophenylalanine-fructose complex. Int. J. Radiat. Oncol. Biol. Phys. 1994, 30, 643–652. [Google Scholar] [CrossRef]
- Futamura, G.; Kawabata, S.; Nonoguchi, N.; Hiramatsu, R.; Toho, T.; Tanaka, H.; Masunaga, S.-I.; Hattori, Y.; Kirihata, M.; Ono, K.; et al. Evaluation of a novel sodium borocaptate-containing unnatural amino acid as a boron delivery agent for neutron capture therapy of the F98 rat glioma. Radiat. Oncol. 2017, 12, 26. [Google Scholar] [CrossRef]
- Kanemitsu, T.; Kawabata, S.; Fukumura, M.; Futamura, G.; Hiramatsu, R.; Nonoguchi, N.; Nakagawa, F.; Takata, T.; Tanaka, H.; Suzuki, M.; et al. Folate receptor-targeted novel boron compound for boron neutron capture therapy on F98 glioma-bearing rats. Radiat. Environ. Biophys. 2019, 58, 59–67. [Google Scholar] [CrossRef]
- Fukuo, Y.; Hattori, Y.; Kawabata, S.; Kashiwagi, H.; Kanemitsu, T.; Takeuchi, K.; Futamura, G.; Hiramatsu, R.; Watanabe, T.; Hu, N.; et al. The Therapeutic Effects of Dodecaborate Containing Boronophenylalanine for Boron Neutron Capture Therapy in a Rat Brain Tumor Model. Biology 2020, 9, 437. [Google Scholar] [CrossRef]
- Takeuchi, K.; Hattori, Y.; Kawabata, S.; Futamura, G.; Hiramatsu, R.; Wanibuchi, M.; Tanaka, H.; Masunaga, S.-I.; Ono, K.; Miyatake, S.-I.; et al. Synthesis and Evaluation of Dodecaboranethiol Containing Kojic Acid (KA-BSH) as a Novel Agent for Boron Neutron Capture Therapy. Cells 2020, 9, 1551. [Google Scholar] [CrossRef]
- Kashiwagi, H.; Hattori, Y.; Kawabata, S.; Kayama, R.; Yoshimura, K.; Fukuo, Y.; Kanemitsu, T.; Shiba, H.; Hiramatsu, R.; Takami, T.; et al. Multi-Targeted Neutron Capture Therapy Combined with an 18kDa Translocator Protein-Targeted Boron Compound Is an Effective Strategy in a Rat Brain Tumor Model. Cancers 2023, 15, 1034. [Google Scholar] [CrossRef]
- Barth, R.F.; Kaur, B. Rat brain tumor models in experimental neuro-oncology: The C6, 9L, T9, RG2, F98, BT4C, RT-2 and CNS-1 gliomas. J. Neuro Oncol. 2009, 94, 299–312. [Google Scholar] [CrossRef]
- Barth, R.F.; Carpenter, D.E. Rodent Brain Tumor Models for Studies Focusing on Boron Neutron Capture Therapy. Cancer Biother. Radiopharm. 2022; online ahead of print. [Google Scholar] [CrossRef]
- Rossini, A.E.; Dagrosa, M.A.; Portu, A.; Saint, M.G.; Thorp, S.; Casal, M.; Navarro, A.; Juvenal, G.J.; Pisarev, M.A. Assessment of biological effectiveness of boron neutron capture therapy in primary and metastatic melanoma randoms. Int. J. Radiat. Biol. 2015, 91, 81–89. [Google Scholar] [CrossRef]
- Coderre, J.A.; Makar, M.S.; Micca, P.L.; Nawrocky, M.M.; Liu, H.B.; Joel, D.D.; Slatkin, D.N.; Amols, H.I. Derivations of relative biological effectiveness for the high-let radiations produced during boron neutron capture irradiations of the 9L rat gliosarcoma in vitro and in vivo. Int. J. Radiat. Oncol. Biol. Phys. 1993, 27, 1121–1129. [Google Scholar] [CrossRef]
- Suzuki, M.; Kato, I.; Aihara, T.; Hiratsuka, J.; Yoshimura, K.; Niimi, M.; Kimura, Y.; Ariyoshi, Y.; Haginomori, S.-I.; Sakurai, Y.; et al. Boron neutron capture therapy outcomes for advanced or recurrent head and neck cancer. J. Radiat. Res. 2014, 55, 146–153. [Google Scholar] [CrossRef]
- Solano, A.G.; Dupuy, J.; Therriault, H.; Liberelle, B.; Faucheux, N.; Lauzon, M.A.; Virgilio, N.; Paquette, B. An alginate-based macroporous hydrogel matrix to trap cancer cells. Carbohydr. Polym. 2021, 266, 118115. [Google Scholar] [CrossRef]
- Desgrosellier, J.S.; Cheresh, D.A. Integrins in cancer: Biological implications and therapeutic opportunities. Nat. Rev. Cancer 2010, 10, 9–22. [Google Scholar] [CrossRef]
- Bello, L.; Francolini, M.; Marthyn, P.; Zhang, J.; Carroll, R.S.; Nikas, D.C.; Strasser, J.F.; Villani, R.; Cheresh, D.A.; Black, P.M. Alpha(v)beta3 and alpha(v)beta5 integrin expression in glioma periphery. Neurosurgery 2001, 49, 380–389. [Google Scholar] [CrossRef]
- Liu, W.; Su, J.; Shi, Q.; Wang, J.; Chen, X.; Zhang, S.; Li, M.; Cui, J.; Fan, C.; Sun, B.; et al. RGD Peptide-Conjugated Selenium Nanocomposite Inhibits Human Glioma Growth by Triggering Mitochondrial Dysfunction and ROS-Dependent MAPKs Activation. Front. Bioeng. Biotechnol. 2021, 9, 1387. [Google Scholar] [CrossRef]
- Stupp, R.; Hegi, M.E.; Gorlia, T.; Erridge, S.C.; Perry, J.; Hong, Y.-K.; Aldape, K.D.; Lhermitte, B.; Pietsh, T.; Grujicic, D.; et al. Cilengitide combined with standard treatment for patients with newly diagnosed glioblastoma with methylated MEMT promoter (CENTRIC EORTC 26071-22072 study): A multicentre, randomised, open-label, phase 3 trial. Lancet Oncol. 2014, 15, 1100–1108. [Google Scholar] [CrossRef]
- Matsumura, Y.; Maeda, H. A new concept for macromolecular therapeutics in cancer chemotherapy: Mechanism of tumoritropic accumulation of proteins and the antitumor agent smancs. Cancer Res. 1986, 46 Pt 1, 6387–6392. [Google Scholar]
- Maeda, H. The 35th Anniversary of the Discovery of EPR Effect: A New Wave of Nanomedicines for Tumor-Targeted Drug Delivery-Personal Remarks and Future Prospects. J. Pers. Med. 2021, 11, 229. [Google Scholar] [CrossRef]
- De Deyne, P.G.; O’Neill, A.; Resneck, W.G.; Dmytrenko, G.M.; Pumplin, D.W.; Bloch, R.J. The vitronectin receptor associates with clathrin-coated membrane domains via the cytoplasmic domain of its beta5 subunit. J. Cell Sci. 1998, 111 Pt 18, 2729–2740. [Google Scholar] [CrossRef]
- Alam, M.R.; Dixit, V.; Kang, H.; Li, Z.B.; Chen, X.; Trejo, J.; Fisher, M.; Juliano, R.L. Intracellular delivery of an anionic antisense oligonucleotide via receptor-mediated endocytosis. Nucleic Acids Res. 2008, 36, 2764–2776. [Google Scholar] [CrossRef]
- Schraa, A.J.; Kok, R.J.; Berendsen, A.D.; Moorlag, H.E.; Bos, E.J.; Meijer, D.K.; de Leij, L.F.; Molema, G. Endothelial cells internalize and degrade RGD-modified proteins developed for tumor vasculature targeting. J. Control. Release 2002, 83, 241–251. [Google Scholar] [CrossRef]
- Sancey, L.; Lucie, S.; Garanger, E.; Elisabeth, G.; Foillard, S.; Stéphanie, F.; Schoehn, G.; Guy, S.; Hurbin, A.; Amandine, H.; et al. Clustering and internalization of integrin alphavbeta3 with a tetrameric RGD-synthetic peptide. Mol. Ther. 2009, 17, 837–843. [Google Scholar] [CrossRef]
- Barth, R.F.; Mi, P.; Yang, W. Boron delivery agents for neutron capture therapy of cancer. Cancer Commun. 2018, 38, 35. [Google Scholar] [CrossRef]
- Wang, D.; Wang, C.; Wang, L.; Chen, Y. A comprehensive review in improving delivery of small-molecule chemotherapeutic agents overcoming the blood-brain/brain tumor barriers for glioblastoma treatment. Drug Deliv. 2019, 26, 551–565. [Google Scholar] [CrossRef] [PubMed]
- Pardridge, W.M. Drug transport across the blood-brain barrier. J. Cereb. Blood Flow Metab. 2012, 32, 1959–1972. [Google Scholar] [CrossRef]
- Van Tellingen, O.; Yetkin-Arik, B.; De Gooijer, M.C.; Wesseling, P.; Wurdinger, T.; De Vries, H.E. Overcoming the blood-brain tumor barrier for effective glioblastoma treatment. Drug Resist. Updates 2015, 19, 1–12. [Google Scholar] [CrossRef]
- Galldiks, N.; Langen, K.-J.; Albert, N.-L.; Law, I.; Kim, M.M.; Villanueva-Meyer, J.E.; Soffietti, R.; Wen, P.Y.; Weller, M.; Tonn, J.C. Investigational PET tracers in neuro-oncology—What’s on the horizon? A report of the PET/RANO group. Neuro Oncol. 2022, 24, 1815–1826. [Google Scholar] [CrossRef]
- Beer, A.J.; Grosu, A.L.; Carlsen, J.; Kolk, A.; Sarbia, M.; Stangier, I.; Watzlowik, P.; Wester, H.-J.; Haubner, R.; Schwaiger, M. [18F]galacto-RGD positron emission tomography for imaging of alphavbeta3 expression on the neovasculature in patients with squamous cell carcinoma of the head and neck. Clin. Cancer Res. 2007, 13 Pt 1, 6610–6616. [Google Scholar] [CrossRef]
- Beer, A.J.; Haubner, R.; Wolf, I.; Goebel, M.; Luderschmidt, S.; Niemeyer, M.; Grosu, A.-L.; Martinez, M.-J.; Wester, H.J.; Weber, W.A.; et al. PET-based human dosimetry of 18F-galacto-RGD, a new radiotracer for imaging alpha v beta3 expression. J. Nucl. Med. 2006, 47, 763–769. [Google Scholar]
- Liolios, C.; Sachpekidis, C.; Kolocouris, A.; Dimitrakopoulou-Strauss, A.; Bouziotis, P. PET diagnostic molecules utilizing multimeric cyclic RGD peptide analogs for imaging integrin alphavbeta3 receptors. Molecules 2021, 26, 1792. [Google Scholar] [CrossRef]




| Boron Carrier a | Time b (h) | n c | Boron Concentration ± SD (µg B/g) d | Ratio | |||
|---|---|---|---|---|---|---|---|
| Tumor | Brain | Blood | T/Br e | T/Bl f | |||
| cRGD-MID-AC | 2.5 | 4 | 10.1 ± 1.6 | 0.8 ± 0.2 | 41.6 ± 5.6 | 12.5 | 0.2 |
| 8 | 4 | 17.0 ± 1.8 | 0.9 ± 0.1 | 40.3 ± 8.4 | 18.5 | 0.4 | |
| 24 | 4 | 13.1 ± 1.9 | 0.7 ± 0.1 | 17.7 ± 2.3 | 18.4 | 0.7 | |
| BPA | 2.5 | 4 | 20.6 ± 2.2 | 5.5 ± 0.6 | 7.7 ± 0.5 | 3.8 | 2.7 |
| 8 | 3 | 18.2 ± 2.9 | 5.3 ± 0.5 | 4.8 ± 0.3 | 3.4 | 3.8 | |
| 24 | 4 | 8.2 ± 0.8 | 2.3 ± 0.3 | 2.9 ± 0.4 | 3.6 | 2.8 | |
| Group | n a | Survival Time (Days) | %ILS c | p-Value d | ||
|---|---|---|---|---|---|---|
| Mean ± SD | Median | 95% CI b | ||||
| Untreated | 5 | 30.0 ± 4.0 | 30.0 | 26–34 | - | - |
| Neutron only | 4 | 33.0 ± 7.7 | 35.0 | 22–40 | 16.7 | 0.18 |
| BNCT using BPA 2.5 h | 6 | 43.0 ± 3.8 | 42.0 | 39–50 | 40.0 | 0.0011 |
| BNCT using BPA 8 h | 5 | 40.2 ± 5.6 | 40.0 | 34–48 | 33.3 | 0.0079 |
| BNCT using cRGD-MID-AC 2.5 h | 7 | 42.4 ± 8.6 | 43.0 | 32–47 | 43.3 | 0.0033 |
| BNCT using cRGD-MID-AC 8 h | 6 | 50.3 ± 26.8 | 38.5 | 27- | 28.3 | 0.0499 |
| Group | Physical Dose a (Gy) | Photon-Equivalent Dose b (Gy-Eq) | ||
|---|---|---|---|---|
| Brain | Tumor | Brain | Tumor | |
| Untreated | 0.0 | 0.0 | 0.0 | 0.0 |
| Neutron only | 1.6 | 1.6 | 2.6 | 2.6 |
| BNCT using BPA 2.5 h | 2.2 | 4.6 | 3.4 | 10.9 |
| BNCT using BPA 8 h | 2.2 | 4.2 | 3.3 | 9.9 |
| BNCT using cRGD-MID-AC 2.5 h | 1.5 | 2.9 | - * | 5.8 |
| BNCT using cRGD-MID-AC 8 h | 1.8 | 4.6 | - * | 9.5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tsujino, K.; Kashiwagi, H.; Nishimura, K.; Kayama, R.; Yoshimura, K.; Fukuo, Y.; Shiba, H.; Hiramatsu, R.; Nonoguchi, N.; Furuse, M.; et al. Improved Boron Neutron Capture Therapy Using Integrin αvβ3-Targeted Long-Retention-Type Boron Carrier in a F98 Rat Glioma Model. Biology 2023, 12, 377. https://doi.org/10.3390/biology12030377
Tsujino K, Kashiwagi H, Nishimura K, Kayama R, Yoshimura K, Fukuo Y, Shiba H, Hiramatsu R, Nonoguchi N, Furuse M, et al. Improved Boron Neutron Capture Therapy Using Integrin αvβ3-Targeted Long-Retention-Type Boron Carrier in a F98 Rat Glioma Model. Biology. 2023; 12(3):377. https://doi.org/10.3390/biology12030377
Chicago/Turabian StyleTsujino, Kohei, Hideki Kashiwagi, Kai Nishimura, Ryo Kayama, Kohei Yoshimura, Yusuke Fukuo, Hiroyuki Shiba, Ryo Hiramatsu, Naosuke Nonoguchi, Motomasa Furuse, and et al. 2023. "Improved Boron Neutron Capture Therapy Using Integrin αvβ3-Targeted Long-Retention-Type Boron Carrier in a F98 Rat Glioma Model" Biology 12, no. 3: 377. https://doi.org/10.3390/biology12030377
APA StyleTsujino, K., Kashiwagi, H., Nishimura, K., Kayama, R., Yoshimura, K., Fukuo, Y., Shiba, H., Hiramatsu, R., Nonoguchi, N., Furuse, M., Takami, T., Miyatake, S.-I., Hu, N., Takata, T., Tanaka, H., Suzuki, M., Kawabata, S., Nakamura, H., & Wanibuchi, M. (2023). Improved Boron Neutron Capture Therapy Using Integrin αvβ3-Targeted Long-Retention-Type Boron Carrier in a F98 Rat Glioma Model. Biology, 12(3), 377. https://doi.org/10.3390/biology12030377