
High-Intensity Interval Training Improves Cardiac Autonomic Function in Patients with Type 2 Diabetes: A Randomized Controlled Trial

 ,
,  , and
, and 
Abstract
Simple Summary
Abstract
1. Introduction
2. Materials and Methods
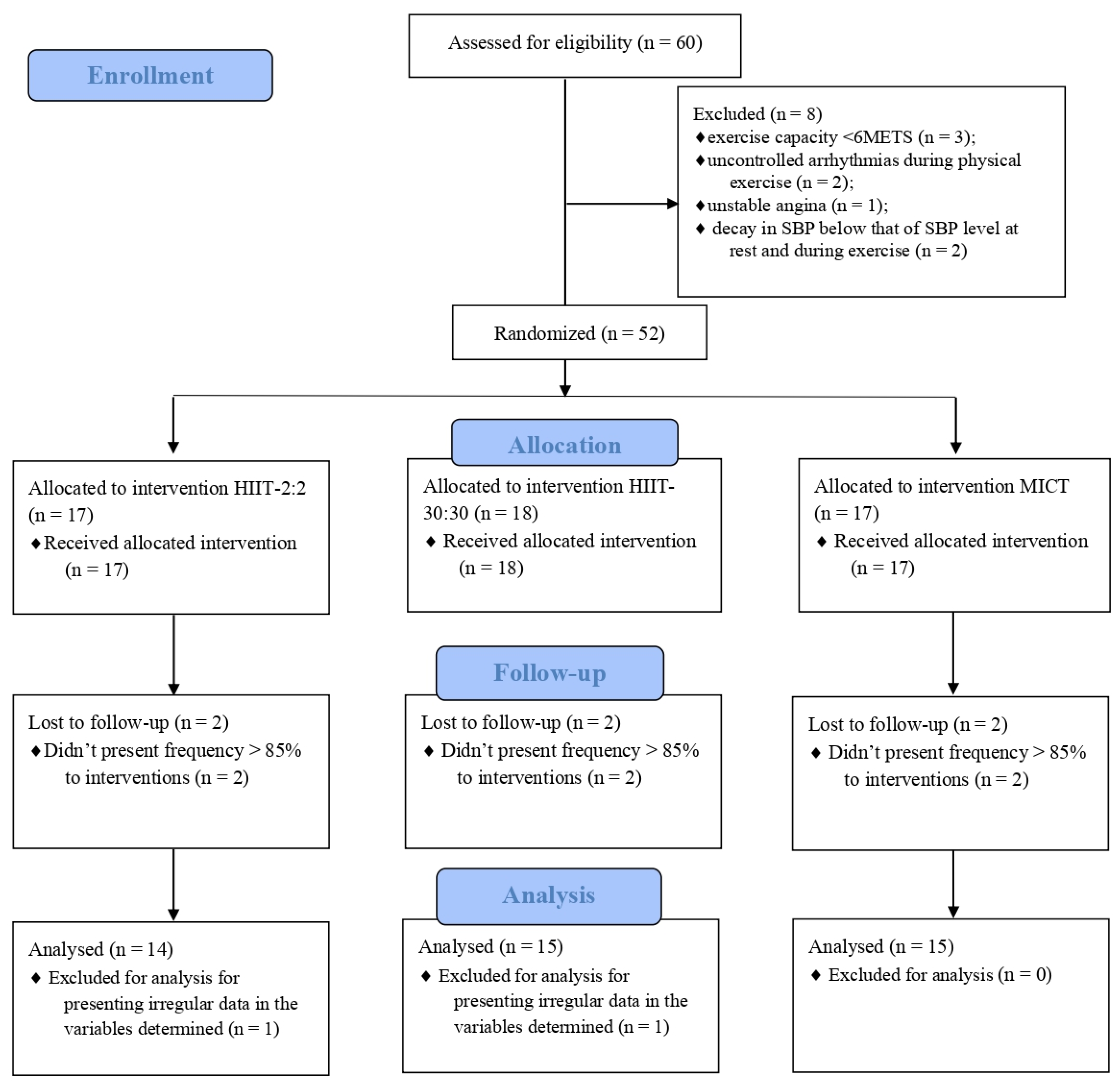
2.1. Study Design
2.2. Test Protocols
2.2.1. Cardiopulmonary Exercise Test (CPET)
- (1)
- discontinuity of stride during the treadmill running phase;
- (2)
- reaching the predicted maximum heart rate (HRmax) for the patient’s age;
- (3)
- respiratory exchange ratio > 1.15.
2.2.2. Heart Rate Variability (HRV)
2.2.3. Symbolic Analysis and Shannon’s Entropy
2.2.4. Monoexponential Analyses
2.3. Exercise Protocols
2.4. Statistical Analyses
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Cho, N.H.; Shaw, J.E.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.D.; Ohlrogge, A.W.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef]
- Williams, R.; Karuranga, S.; Malanda, B.; Saeedi, P.; Basit, A.; Besançon, S.; Bommer, C.; Esteghamati, A.; Ogurtsova, K.; Zhang, P.; et al. Global and regional estimates and projections of diabetes-related health expenditure: Results from the International Diabetes Federation Diabetes Atlas, 9th edition. Diabetes Res. Clin. Pract. 2020, 162, 108072. [Google Scholar] [CrossRef]
- Shaffer, F.; Ginsberg, J.P. An Overview of Heart Rate Variability Metrics and Norms. Front. Public Health 2017, 5, 258. [Google Scholar] [CrossRef]
- Baldi, J.C.; Wilson, G.A.; Wilson, L.C.; Wilkins, G.T.; Lamberts, R.R. The Type 2 Diabetic Heart: Its Role in Exercise Intolerance and the Challenge to Find Effective Exercise Interventions. Sports Med. 2016, 46, 1605–1617. [Google Scholar] [CrossRef]
- Stockhorst, U.; Huenig, A.; Ziegler, D.; Scherbaum, W.A. Unconditioned and conditioned effects of intravenous insulin and glucose on heart rate variability in healthy men. Physiol. Behav. 2011, 103, 31–38. [Google Scholar] [CrossRef]
- Silva, L.R.B.E.; Zamunér, A.R.; Gentil, P.; Alves, F.M.; Leal, A.G.F.; Soares, V.; Silva, M.S.; Vieira, M.F.; Simões, K.; Pedrino, G.R.; et al. Cardiac Autonomic Modulation and the Kinetics of Heart Rate Responses in the on- and off-Transient during Exercise in Women with Metabolic Syndrome. Front. Physiol. 2017, 8, 542. [Google Scholar] [CrossRef]
- Silva, L.R.B.; Gentil, P.; Seguro, C.S.; de Oliveira, G.T.; Silva, M.S.; Zamunér, A.R.; Beltrame, T.; Rebelo, A.C.S. High Fasting Glycemia Predicts Impairment of Cardiac Autonomic Control in Adults With Type 2 Diabetes: A Case-Control Study. Front. Endocrinol. 2021, 12, 760292. [Google Scholar] [CrossRef]
- Dhoble, A.; Lahr, B.D.; Allison, T.G.; Kopecky, S.L. Cardiopulmonary fitness and heart rate recovery as predictors of mortality in a referral population. J. Am. Heart Assoc. 2014, 3, e000559. [Google Scholar] [CrossRef]
- Pedersen, B.K.; Saltin, B. Exercise as medicine—Evidence for prescribing exercise as therapy in 26 different chronic diseases. Scand. J. Med. Sci. Sport. 2015, 25, 1–72. [Google Scholar] [CrossRef]
- Rasmussen, M.G.; Grøntved, A.; Blond, K.; Overvad, K.; Tjønneland, A.; Jensen, M.K.; Østergaard, L. Associations between Recreational and Commuter Cycling, Changes in Cycling, and Type 2 Diabetes Risk: A Cohort Study of Danish Men and Women. PLoS Med. 2016, 13, e1002076. [Google Scholar] [CrossRef]
- Abrignani, M.G. Physical exercise and risk of arterial hypertension and diabetes mellitus. Let’s move, it is never too late. Eur. J. Prev. Cardiol. 2018, 25, 1063–1064. [Google Scholar] [CrossRef] [PubMed]
- Winding, K.M.; Munch, G.W.; Iepsen, U.W.; Van Hall, G.; Pedersen, B.K.; Mortensen, S.P. The effect on glycaemic control of low-volume high-intensity interval training versus endurance training in individuals with type 2 diabetes. Diabetes Obes. Metab. 2018, 20, 1131–1139. [Google Scholar] [CrossRef]
- Cassidy, S.; Vaidya, V.; Houghton, D.; Zalewski, P.; Seferovic, J.P.; Hallsworth, K.; MacGowan, G.A.; Trenell, M.I.; Jakovljevic, D.G. Unsupervised high-intensity interval training improves glycaemic control but not cardiovascular autonomic function in type 2 diabetes patients: A randomised controlled trial. Diabetes Vasc. Dis. Res. 2019, 16, 69–76. [Google Scholar] [CrossRef] [PubMed]
- Helal, L.; Umpierre, D.; Moraes, R.S. High-intensity aerobic interval training improves aerobic fitness and HbA1c among persons diagnosed with type 2 diabetes: Considerations regarding HbA1c starting levels and intervention design. Eur. J. Appl. Physiol. 2017, 117, 2365–2366. [Google Scholar] [CrossRef]
- Kawada, T. Effect of high-intensity aerobic exercise on aerobic fitness and HbA1c in patients with type 2 diabetes. Eur. J. Appl. Physiol. 2017, 117, 1519–1520. [Google Scholar] [CrossRef]
- Støa, E.M.; Meling, S.; Nyhus, L.K.; Glenn, S.; Mangerud, K.M.; Helgerud, J.; Bratland-Sanda, S.; Støren, Ø. High-intensity aerobic interval training improves aerobic fitness and HbA1c among persons diagnosed with type 2 diabetes. Eur. J. Appl. Physiol. 2017, 117, 455–467. [Google Scholar] [CrossRef]
- De Nardi, A.T.; Tolves, T.; Lenzi, T.L.; Signori, L.U.; Silva, A.M.V. da High-intensity interval training versus continuous training on physiological and metabolic variables in prediabetes and type 2 diabetes: A meta-analysis. Diabetes Res. Clin. Pract. 2018, 137, 149–159. [Google Scholar] [CrossRef]
- Guiraud, T.; Nigam, A.; Gremeaux, V.; Meyer, P.; Juneau, M.; Bosquet, L. High-intensity interval training in cardiac rehabilitation. Sport. Med. 2012, 42, 587–605. [Google Scholar] [CrossRef]
- Gillen, J.B.; Gibala, M.J. Is high-intensity interval training a time-efficient exercise strategy to improve health and fitness? Appl. Physiol. Nutr. Metab. 2014, 39, 409–412. [Google Scholar] [CrossRef]
- Souza, D.; Coswig, V.; de Lira, C.A.B.; Gentil, P. H″IT″ting the Barriers for Exercising during Social Isolation. Biology 2020, 9, 245. [Google Scholar] [CrossRef]
- Kilpatrick, M.W.; Martinez, N.; Little, J.P.; Jung, M.E.; Jones, A.M.; Price, N.W.; Lende, D.H. Impact of high-intensity interval duration on perceived exertion. Med. Sci. Sport Exerc. 2015, 47, 1038–1045. [Google Scholar] [CrossRef]
- Martinez, N.; Kilpatrick, M.W.; Salomon, K.; Jung, M.E.; Little, J.P. Affective and Enjoyment Responses to High-Intensity Interval Training in Overweight-to-Obese and Insufficiently Active Adults. J. Sport Exerc. Psychol. 2015, 37, 138–149. [Google Scholar] [CrossRef]
- Viana, R.B.; de Lira, C.A.B.; Naves, J.P.A.; Coswig, V.S.; Del Vecchio, F.B.; Ramirez-Campillo, R.; Vieira, C.A.; Gentil, P. Can We Draw General Conclusions from Interval Training Studies? Sports Med. 2018, 48, 2001–2009. [Google Scholar] [CrossRef]
- Viana, R.B.; Naves, J.P.A.; Coswig, V.S.; de Lira, C.A.B.; Steele, J.; Fisher, J.P.; Gentil, P. Is interval training the magic bullet for fat loss? A systematic review and meta-analysis comparing moderate-intensity continuous training with high-intensity interval training (HIIT). Br. J. Sports Med. 2019, 53, bjsports-2018-099928. [Google Scholar] [CrossRef]
- Naves, J.P.A.; Rebelo, A.C.S.; Silva, L.R.B.E.; Silva, M.S.; Ramirez-Campillo, R.; Ramírez-Vélez, R.; Gentil, P. Cardiorespiratory and perceptual responses of two interval training and a continuous training protocol in healthy young men. Eur. J. Sport Sci. 2019, 19, 653–660. [Google Scholar] [CrossRef]
- Bento Silva, L.R.; Viana Gentil, P.R.; Beltrame, T.; Basso Filho, M.A.; Alves, F.M.; Silva, M.S.; Pedrino, G.R.; Ramirez-Campillo, R.; Coswig, V.; Silva Rebelo, A.C. Exponential model for analysis of heart rate responses and autonomic cardiac modulation during different intensities of physical exercise. R. Soc. Open Sci. 2019, 6, 190639. [Google Scholar] [CrossRef]
- Borg, G.A. Psychophysical bases of perceived exertion. Med. Sci. Sports Exerc. 1982, 14, 377–381. [Google Scholar] [CrossRef] [PubMed]
- Thompson, P.D.; Arena, R.; Riebe, D.; Pescatello, L.S. American College of Sports Medicine ACSM’s New Preparticipation Health Screening Recommendations from ACSM’s Guidelines for Exercise Testing and Prescription, Ninth Edition. Curr. Sports Med. Rep. 2013, 12, 215–217. [Google Scholar] [CrossRef] [PubMed]
- Porta, A.; Faes, L.; Masé, M.; D’Addio, G.; Pinna, G.D.; Maestri, R.; Montano, N.; Furlan, R.; Guzzetti, S.; Nollo, G.; et al. An integrated approach based on uniform quantization for the evaluation of complexity of short-term heart period variability: Application to 24 h Holter recordings in healthy and heart failure humans. Chaos 2007, 17, 015117. [Google Scholar] [CrossRef] [PubMed]
- Porta, A.; Guzzetti, S.; Montano, N.; Furlan, R.; Pagani, M.; Malliani, A.; Cerutti, S. Entropy, entropy rate, and pattern classification as tools to typify complexity in short heart period variability series. IEEE Trans. Biomed. Eng. 2001, 48, 1282–1291. [Google Scholar] [CrossRef] [PubMed]
- Imai, K.; Sato, H.; Hori, M.; Kusuoka, H.; Ozaki, H.; Yokoyama, H.; Takeda, H.; Inoue, M.; Kamada, T. Vagally mediated heart rate recovery after exercise is accelerated in athletes but blunted in patients with chronic heart failure. J. Am. Coll. Cardiol. 1994, 24, 1529–1535. [Google Scholar] [CrossRef]
- Bearden, S.E.; Moffatt, R.J. and heart rate kinetics in cycling: Transitions from an elevated baseline. J. Appl. Physiol. 2001, 90, 2081–2087. [Google Scholar] [CrossRef][Green Version]
- Wisløff, U.; Støylen, A.; Loennechen, J.P.; Bruvold, M.; Rognmo, Ø.; Haram, P.M.; Tjønna, A.E.; Helgerud, J.; Slørdahl, S.A.; Lee, S.J.; et al. Superior cardiovascular effect of aerobic interval training versus moderate continuous training in heart failure patients: A randomized study. Circulation 2007, 115, 3086–3094. [Google Scholar] [CrossRef]
- Billat, L.V. Interval training for performance: A scientific and empirical practice. Special recommendations for middle- and long-distance running. Part II: Anaerobic interval training. Sports Med. 2001, 31, 75–90. [Google Scholar] [CrossRef]
- Cohen, J. A power primer. Psychol. Bull. 1992, 112, 155–159. [Google Scholar] [CrossRef]
- Zoppini, G.; Cacciatori, V.; Gemma, M.L.; Moghetti, P.; Targher, G.; Zamboni, C.; Thomaseth, K.; Bellavere, F.; Muggeo, M. Effect of moderate aerobic exercise on sympatho-vagal balance in Type 2 diabetic patients. Diabet. Med. 2007, 24, 370–376. [Google Scholar] [CrossRef]
- Goulopoulou, S.; Baynard, T.; Franklin, R.M.; Fernhall, B.; Carhart, R.; Weinstock, R.; Kanaley, J.A. Exercise training improves cardiovascular autonomic modulation in response to glucose ingestion in obese adults with and without type 2 diabetes mellitus. Metabolism 2010, 59, 901–910. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Goit, R.K.; Pant, B.N.; Shrewastwa, M.K. Moderate intensity exercise improves heart rate variability in obese adults with type 2 diabetes. Indian Heart J. 2018, 70, 486–491. [Google Scholar] [CrossRef] [PubMed]
- Benetos, A.; Rudnichi, A.; Thomas, F.; Safar, M.; Guize, L. Influence of Heart Rate on Mortality in a French Population: Role of Age, Gender, and Blood Pressure. Hypertension 1999, 33, 44–52. [Google Scholar] [CrossRef] [PubMed]
- Paul, L.; Hastie, C.E.; Li, W.S.; Harrow, C.; Muir, S.; John, J.M.; Dominiczak, A.F.; McInnes, G.T.; Padmanabhan, S. Resting heart rate pattern during follow-up and mortality in hypertensive patients. Hypertension 2010, 55, 67–74. [Google Scholar] [CrossRef] [PubMed]
- Zhao, M.X.; Zhao, Q.; Zheng, M.; Liu, T.; Li, Y.; Wang, M.; Yao, S.; Wang, C.; Chen, Y.M.; Xue, H.; et al. Effect of resting heart rate on the risk of all-cause death in Chinese patients with hypertension: Analysis of the Kailuan follow-up study. BMJ Open 2020, 10, e032699. [Google Scholar] [CrossRef]
- Prasada, S.; Oswalt, C.; Yeboah, P.; Saylor, G.; Bowden, D.; Yeboah, J. Heart rate is an independent predictor of all-cause mortality in individuals with type 2 diabetes: The diabetes heart study. World J. Diabetes 2018, 9, 33–39. [Google Scholar] [CrossRef]
- Grace, F.; Herbert, P.; Elliott, A.D.; Richards, J.; Beaumont, A.; Sculthorpe, N.F. High intensity interval training (HIIT) improves resting blood pressure, metabolic (MET) capacity and heart rate reserve without compromising cardiac function in sedentary aging men. Exp. Gerontol. 2018, 109, 75–81. [Google Scholar] [CrossRef]
- Bhatia, C.; Kayser, B. Preoperative high-intensity interval training is effective and safe in deconditioned patients with lung cancer: A randomized clinical trial. J. Rehabil. Med. 2019, 51, 712–718. [Google Scholar] [CrossRef]
- Ramos, J.S.; Dalleck, L.C.; Borrani, F.; Beetham, K.S.; Mielke, G.I.; Dias, K.A.; Wallen, M.P.; Keating, S.E.; Fassett, R.G.; Coombes, J.S. High-intensity interval training and cardiac autonomic control in individuals with metabolic syndrome: A randomised trial. Int. J. Cardiol. 2017, 245, 245–252. [Google Scholar] [CrossRef]
- Dall, C.H.; Snoer, M.; Christensen, S.; Monk-Hansen, T.; Frederiksen, M.; Gustafsson, F.; Langberg, H.; Prescott, E. Effect of high-intensity training versus moderate training on peak oxygen uptake and chronotropic response in heart transplant recipients: A randomized crossover trial. Am. J. Transplant. 2014, 14, 2391–2399. [Google Scholar] [CrossRef] [PubMed]
- Villelabeitia-Jaureguizar, K.; Vicente-Campos, D.; Senen, A.B.; Jiménez, V.H.; Garrido-Lestache, M.E.B.; Chicharro, J.L. Effects of high-intensity interval versus continuous exercise training on post-exercise heart rate recovery in coronary heart-disease patients. Int. J. Cardiol. 2017, 244, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Qiu, S.; Cai, X.; Sun, Z.; Li, L.; Zuegel, M.; Steinacker, J.M.; Schumann, U. Heart rate recovery and risk of cardiovascular events and all-cause mortality: A meta-analysis of prospective cohort studies. J. Am. Heart Assoc. 2017, 6, e005505. [Google Scholar] [CrossRef] [PubMed]
- Qiu, S.H.; Xue, C.; Sun, Z.L.; Steinacker, J.M.; Zügel, M.; Schumann, U. Attenuated heart rate recovery predicts risk of incident diabetes: Insights from a meta-analysis. Diabet. Med. 2017, 34, 1676–1683. [Google Scholar] [CrossRef] [PubMed]
- Besnier, F.; Labrunée, M.; Pathak, A.; Pavy-Le Traon, A.; Galès, C.; Sénard, J.M.; Guiraud, T. Exercise training-induced modification in autonomic nervous system: An update for cardiac patients. Ann. Phys. Rehabil. Med. 2017, 60, 27–35. [Google Scholar] [CrossRef]
- Fu, Q.; Levine, B.D. Exercise and the autonomic nervous system. Handb. Clin. Neurol. 2013, 117, 147–160. [Google Scholar] [CrossRef]
- Fisher, J.P.; Young, C.N.; Fadel, P.J. Autonomic adjustments to exercise in humans. Compr. Physiol. 2015, 5, 475–512. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variables | HIIT-30:30 (n = 15) | HIIT-2:2 (n = 14) | MICT (n = 15) |
|---|---|---|---|
| Age, years | 59.13 ± 5.57 | 61.20 ± 2.88 | 58.50 ± 5.26 |
| Sex (M/F) | 6/9 | 6/8 | 7/8 |
| Fasting blood glucose | 142.70 ± 63.01 | 145.47 ± 66.00 | 129.79 ± 57.12 |
| HbA1c, % | 9.62 ± 1.90 | 9.85 ± 2.79 | 8.50 ± 2.43 |
| Diagnosis time | >5 years | >5 years | >5 years |
| Biguandas, % | 80 (12) | 73.33 (11) | 71.42 (10) |
| Medicines for sulphonylurea, % | - | 6.66 (1) | 21.42 (3) |
| SGLT2 inhibitors, % | - | 13.33 (2) | 7.14 (1) |
| DPP-4 inhibitors, % | 6.66 (1) | 6.66 (1) | 7.14 (1) |
| GLP-1 analogue, % | 6.66 (1) | - | 14.28 (2) |
| Pioglitazone, % | 6.66 (1) | - | 7.14 (1) |
| Insulin, % | 46.66 (7) | 53.33(8) | 35.71 (5) |
| Hypertension, % | 100 (15) | 100 (15) | 100 (14) |
| Beta-blockers, % | - | - | - |
| ACE inhibitors, % | 46,66 (7) | 35,71 (5) | 28,57 (4) |
| Diuretics, % | 53,33 (8) | 64,28 (9) | 46,66 (7) |
| Dyslipidemia, % | 80 (12) | 86.66 (13) | 78.57 (11) |
| Variables | HIIT-30:30 (n = 15) | ES | HIIT-2:2 (n = 14) | ES | MICT (n = 15) | ES | Group | Time | Group*Time | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | |||||||
| HRrest, bpm | 82.86 ± 9.64 | 72.13 ± 8.62 | 0.50(medium) | 84.85 ± 10.28 | 77.92 ± 8.96 | 0.33(medium) | 78.86 ± 8.56 | 80.73 ± 9.43 | −0.10(small) | 0.278 | 0.009 | 0.031 |
| HRpeak, bpm | 152.46 ± 13.42 | 160.20 ± 14.06 | −0.56(medium) | 152.00 ± 21.37 | 158.35 ± 19.26 | −0.31(medium) | 146.40 ± 14.27 | 141.26 ± 17.46 | 0.15(small) | 0.009 | 0.408 | 0.274 |
| R-Ri, ms | 821.2 ± 147.55 | 905.0 ± 178.9 | −0.24(small) | 822.7 ± 73.55 | 866.2 ± 85.7 | −0.26(small) | 867.33 ± 105.0 | 718.0 ± 275.5 | 0.33(medium) | 0.224 | 0.832 | 0.015 |
| Linear Anaysis | ||||||||||||
| SDNN, ms | 20.13 ± 9.67 | 33.80 ± 22.04 | −0.37(medium) | 23.45 ± 15.12 | 28.65 ± 18.08 | −0.15(small) | 29.22 ± 20.92 | 21.85 ± 9.11 | 0.22(small) | 0.932 | 0.133 | 0.036 |
| rMSSD, ms | 23.63 ± 13.87 | 38.39 ± 27.76 | −0.31(medium) | 18.51 ± 9.73 | 25.07 ± 10.33 | −0.31(medium) | 29.22 ± 23.19 | 22.16 ± 13.89 | 0.18(small) | 0.150 | 0.217 | 0.065 |
| pNN50, % | 1.92 ± 3.21 | 9.70 ± 12.31 | −0.39(medium) | 1.02 ± 1.97 | 3.76 ± 3.61 | −0.42(medium) | 6.00 ± 8.59 | 12.85 ± 12.75 | −0.30(medium) | 0.008 | 0.002 | 0.485 |
| Nonlinear Analysis | ||||||||||||
| 0V% | 39.23 ± 25.05 | 28.20 ± 11.14 | 0.27(small) | 41.89 ± 25.50 | 31.09 ± 14.65 | 0.25(small) | 38.33 ± 20.98 | 47.59 ± 27.75 | −0.18(small) | 0.226 | 0.355 | 0.111 |
| 1V% | 33.67 ± 14.32 | 33.78 ± 13.97 | −0.00(trivial) | 31.93 ± 16.75 | 36.41 ± 12.11 | −0.15(small) | 35.20 ± 12.99 | 27.41 ± 12.18 | 0.29(small) | 0.692 | 0.718 | 0.234 |
| 2LV% | 9.62 ± 9.82 | 9.54 ± 5.58 | 0.00(trivial) | 8.12 ± 5.16 | 8.37 ± 6.25 | −0.02(trivial) | 7.71 ± 7.37 | 7.05 ± 7.15 | 0.04(trivial) | 0.482 | 0.918 | 0.970 |
| 2UV% | 17.46 ± 10.72 | 28.47 ± 7.88 | −0.50(medium) | 16.78 ± 9.64 | 24.57 ± 7.00 | −0.41(medium) | 18.96 ± 8.21 | 17.73 ± 9.96 | 0.06(trivial) | 0.146 | 0.003 | 0.029 |
| SE | 2.90 ± 1.29 | 3.18 ± 1.14 | −0.11(small) | 2.65 ± 1.38 | 2.94 ± 0.90 | −0.12(small) | 3.14 ± 1.01 | 2.68 ± 1.02 | 0.22(small) | 0.724 | 0.888 | 0.380 |
| Variables | HIIT-30:30 (n = 15) | ES | HIIT-2:2 (n = 14) | ES | MICT (n = 15) | ES | Group | Time | Group*Time | |||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Pre | Post | Pre | Post | Pre | Post | |||||||
| offAMP | 160.21 ± 16.77 | 179.73 ± 29.88 | −0.37(medium) | 160.17 ± 25.00 | 175.36 ± 44.06 | −0.20(small) | 153.21 ± 20.21 | 172.53 ± 67.22 | −0.18(small) | 0.756 | 0.030 | 0.972 |
| offTAU | 123.19 ± 65.98 | 72.18 ± 29.20 | 0.44(medium) | 131.39 ± 71.05 | 92.05 ± 33.17 | 0.33(medium) | 135.08 ± 99.20 | 170.44 ± 98.46 | −0.17(small) | 0.012 | 0.237 | 0.048 |
| offTMR | 140.36 ± 75.72 | 96.95 ± 23.61 | 0.36(medium) | 142.44 ± 67.87 | 136.24 ± 30.84 | 0.05(trivial) | 153.00 ± 100.63 | 224.82 ± 112.65 | −0.31(medium) | 0.002 | 0.651 | 0.015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Silva, L.R.B.; Gentil, P.; Seguro, C.S.; de Oliveira, J.C.M.; Silva, M.S.; Marques, V.A.; Beltrame, T.; Rebelo, A.C.S. High-Intensity Interval Training Improves Cardiac Autonomic Function in Patients with Type 2 Diabetes: A Randomized Controlled Trial. Biology 2022, 11, 66. https://doi.org/10.3390/biology11010066
Silva LRB, Gentil P, Seguro CS, de Oliveira JCM, Silva MS, Marques VA, Beltrame T, Rebelo ACS. High-Intensity Interval Training Improves Cardiac Autonomic Function in Patients with Type 2 Diabetes: A Randomized Controlled Trial. Biology. 2022; 11(1):66. https://doi.org/10.3390/biology11010066
Chicago/Turabian StyleSilva, Lucas Raphael Bento, Paulo Gentil, Camila Simões Seguro, Jordana Campos Martins de Oliveira, Maria Sebastiana Silva, Vitor Alves Marques, Thomas Beltrame, and Ana Cristina Silva Rebelo. 2022. "High-Intensity Interval Training Improves Cardiac Autonomic Function in Patients with Type 2 Diabetes: A Randomized Controlled Trial" Biology 11, no. 1: 66. https://doi.org/10.3390/biology11010066
APA StyleSilva, L. R. B., Gentil, P., Seguro, C. S., de Oliveira, J. C. M., Silva, M. S., Marques, V. A., Beltrame, T., & Rebelo, A. C. S. (2022). High-Intensity Interval Training Improves Cardiac Autonomic Function in Patients with Type 2 Diabetes: A Randomized Controlled Trial. Biology, 11(1), 66. https://doi.org/10.3390/biology11010066