
Deep Ensemble Model for COVID-19 Diagnosis and Classification Using Chest CT Images

 ,
,  , ,
, ,  , ,
, ,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Literature Review
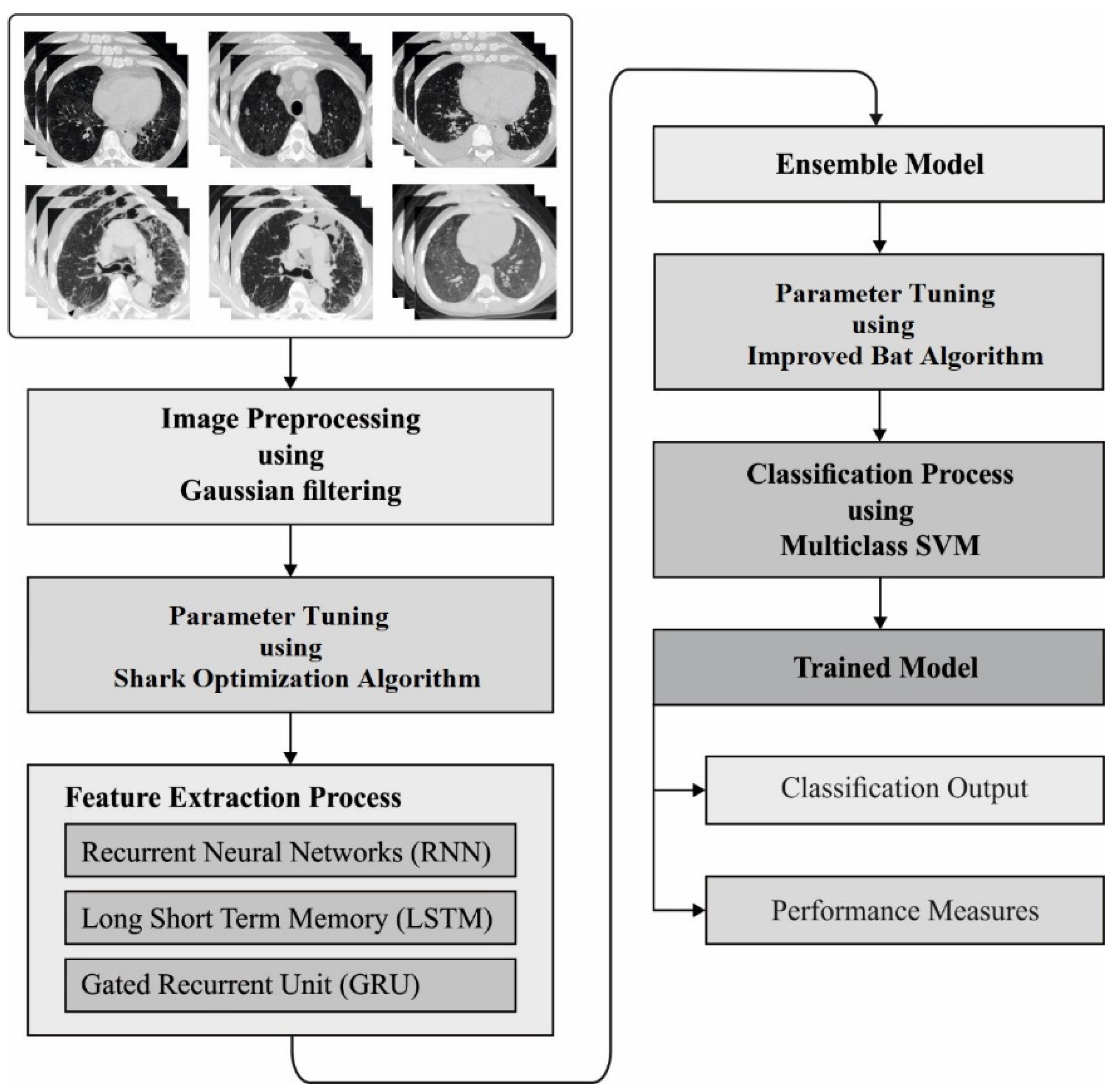
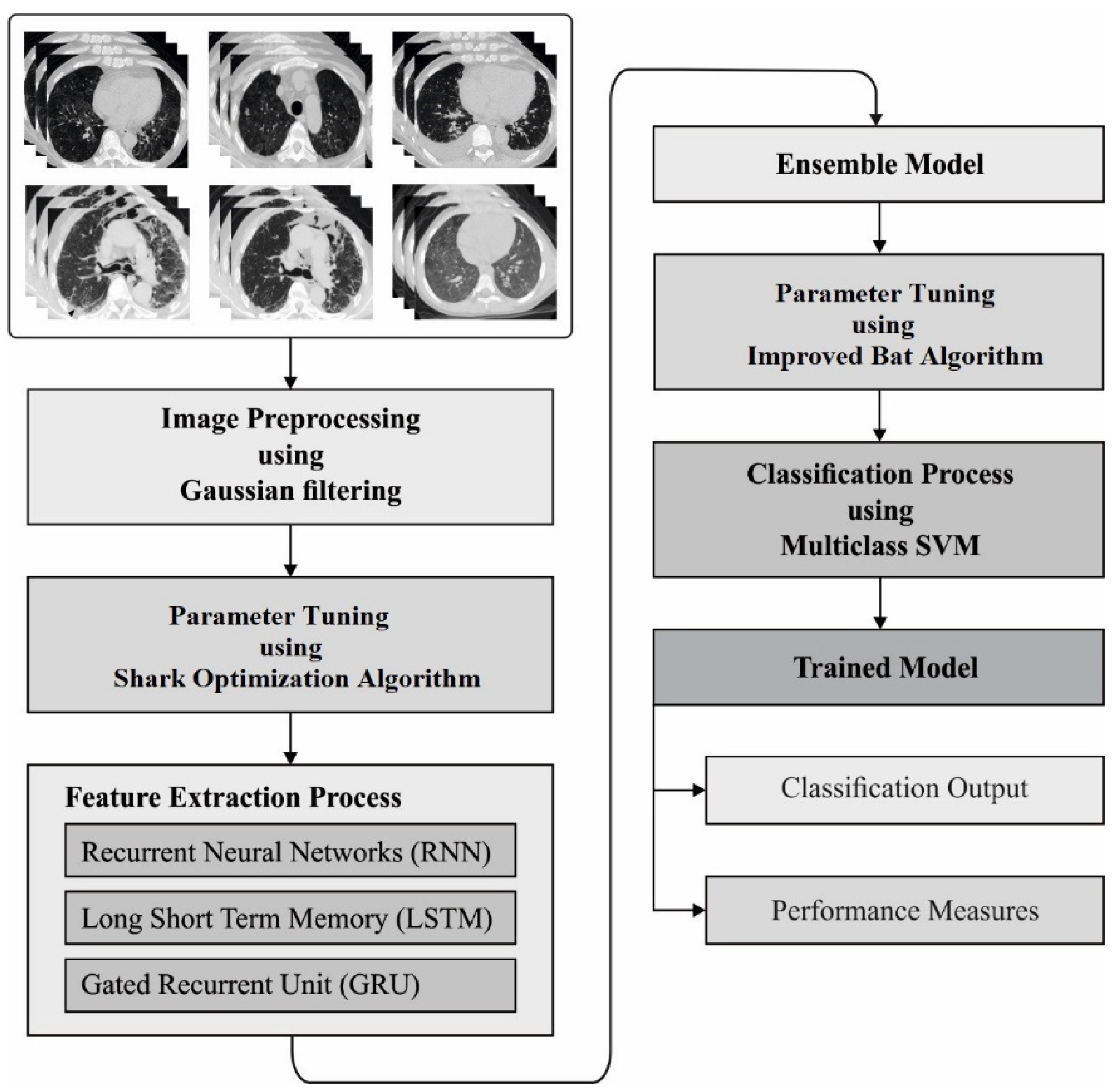
3. The Proposed Model
3.1. Stage 1: Gaussian Filtering (GF)-Based Preprocessing
3.2. Stage 2: Ensemble Feature Extraction
3.2.1. RNN Model
3.2.2. LSTM Model
- The forget gate chooses that measure of long-term state must be omitted;
- An input gate control that measure of must be further to long-term form
- An output gate defines that quantity of must be read and output to and
3.2.3. GRU Model
3.2.4. Ensemble Modeling
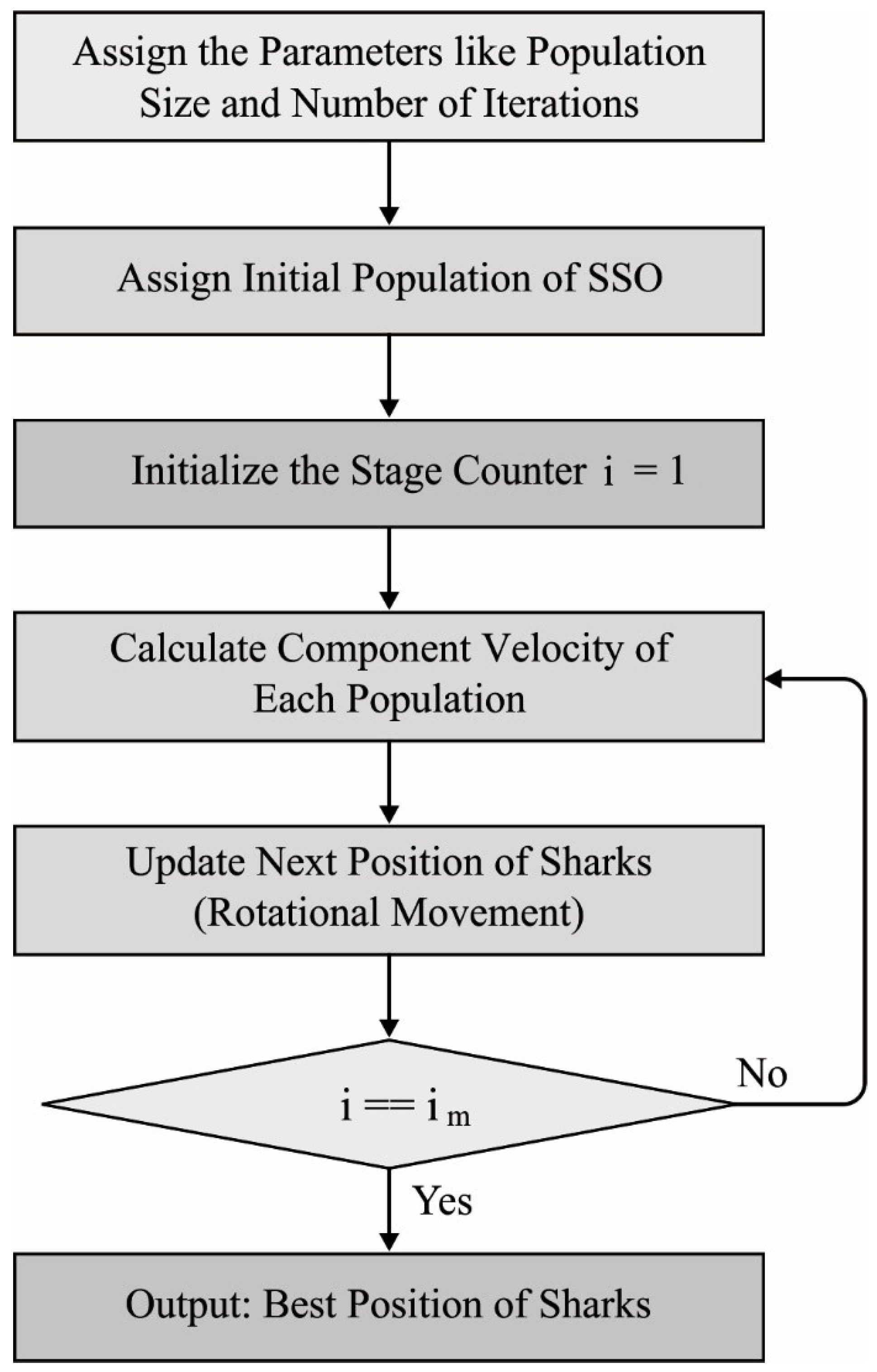
3.2.5. Hyperparameter Tuning
- (1)
- The injured fishes are considered prey to the shark;
- (2)
- The shark tries to discover the injured fish by getting a blood particle from the injured fish’s body;
- (3)
- The velocity of injured fishes is ignored against the shark’s velocity.
3.3. Stage 3: IBA-MSVM-Based Classification
4. Experimental Validation
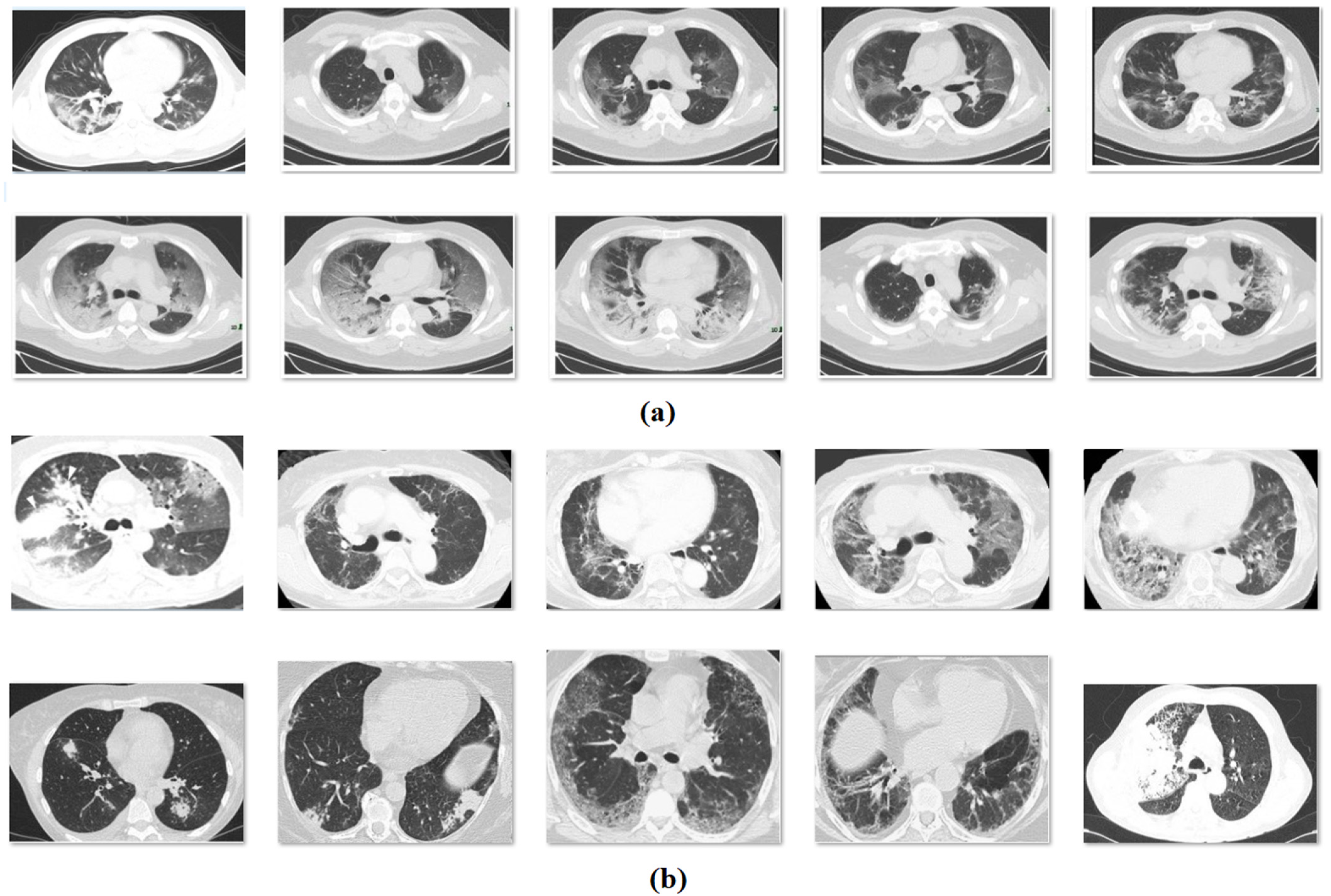
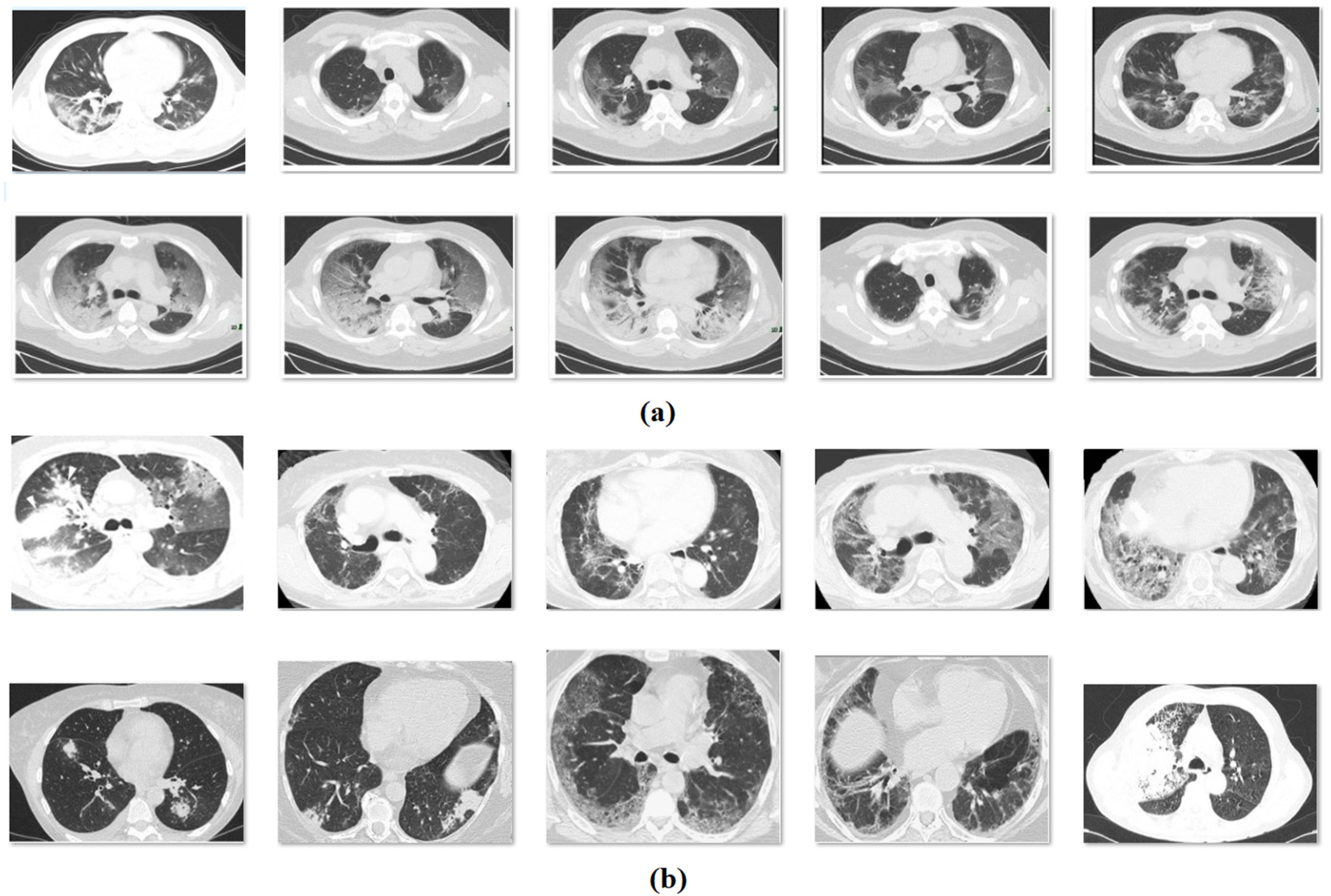
4.1. Data Set Details
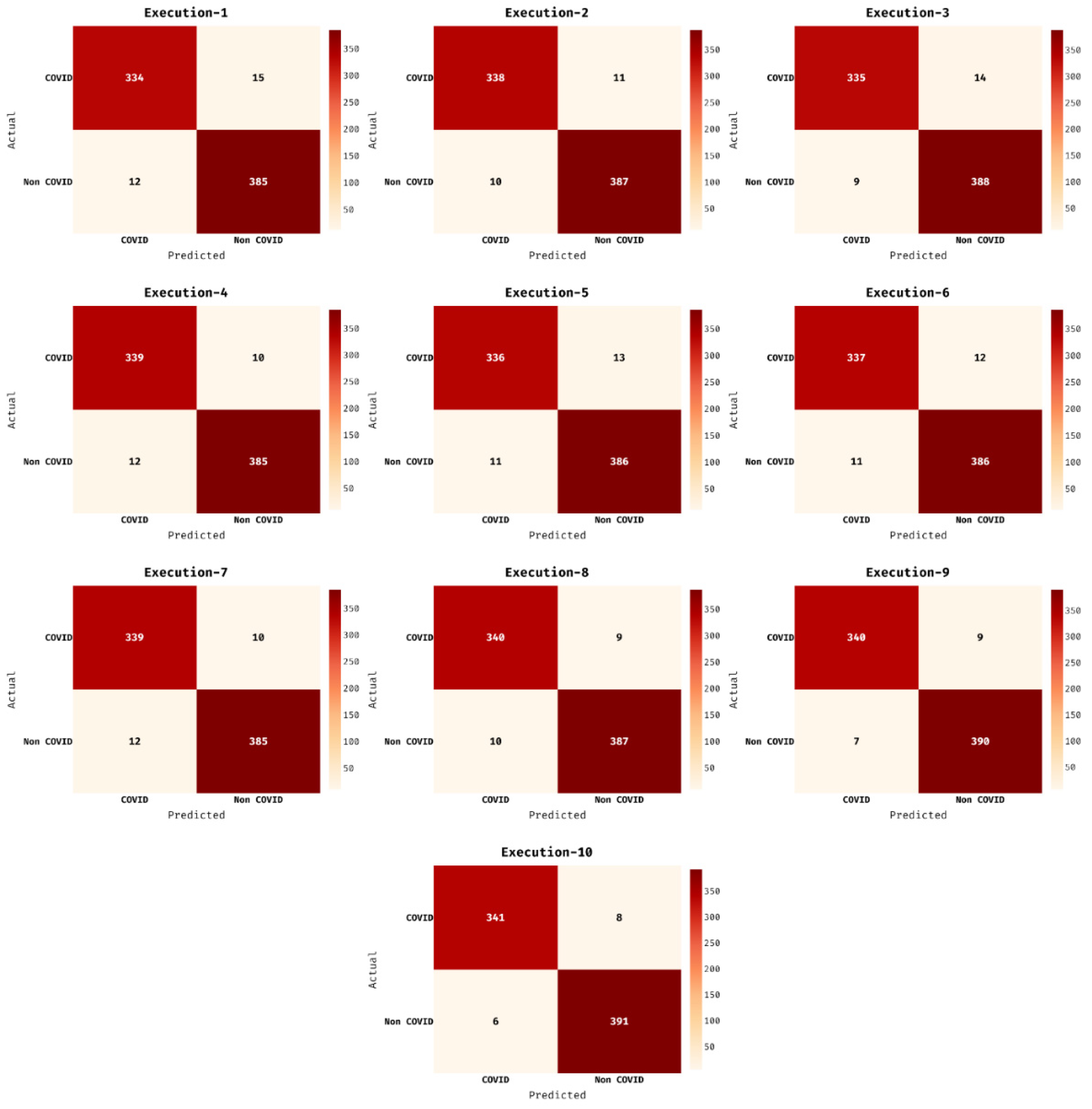
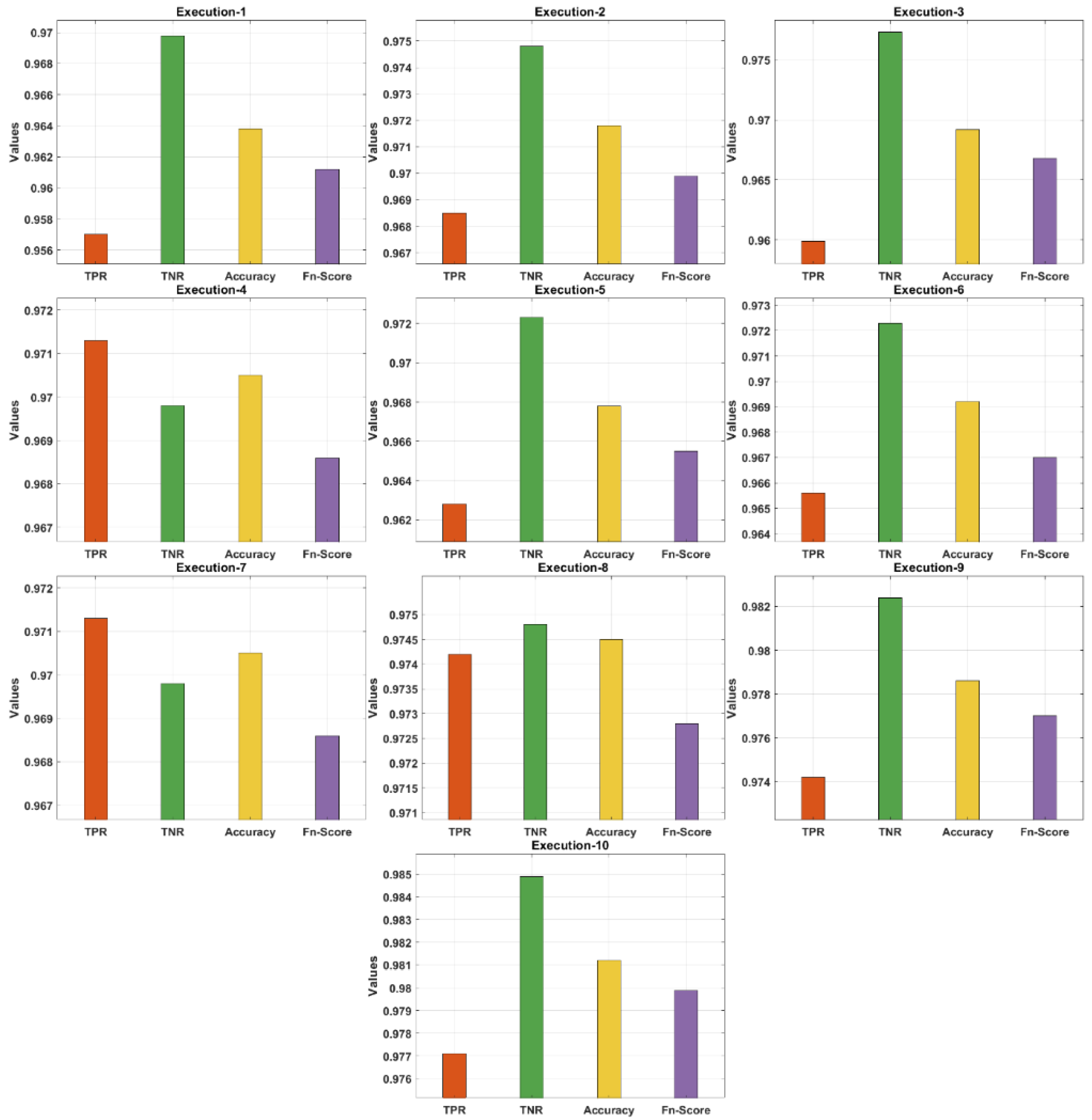
4.2. Results and Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wang, S.; Zha, Y.; Li, W.; Wu, Q.; Li, X.; Niu, M.; Wang, M.; Qiu, X.; Li, H.; Yu, H.; et al. A fully automatic deep learning system for COVID-19 diagnostic and prognostic analysis. Eur. Respir. J. 2020, 56, 2000775. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus—Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061–1069. [Google Scholar] [CrossRef]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; Yu, T.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Mukherjee, H.; Ghosh, S.; Dhar, A.; Obaidullah, S.M.; Santosh, K.C.; Roy, K. Deep neural network to detect COVID-19: One architecture for both CT Scans and Chest X-rays. Appl. Intell. 2020, 51, 2777–2789. [Google Scholar] [CrossRef]
- Santosh, K.; Ghosh, S. COVID-19 Imaging Tools: How Big Data is Big? J. Med. Syst. 2021, 45, 71. [Google Scholar] [CrossRef] [PubMed]
- Zhai, P.; Ding, Y.; Wu, X.; Long, J.; Zhong, Y.; Li, Y. The epidemiology, diagnosis and treatment of COVID-19. Int. J. Antimicrob. Agents 2020, 55, 105955. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Shi, J.; Ye, Z.; Dong, D.; Yu, D.; Zhou, M.; Liu, Y.; Gevaert, O.; Wang, K.; Zhu, Y.; et al. Predicting EGFR mutation status in lung adenocarcinoma on computed tomography image using deep learning. Eur. Respir. J. 2019, 53, 1800986. [Google Scholar] [CrossRef]
- Angelini, E.; Dahan, S.; Shah, A. Unravelling machine learning: Insights in respiratory medicine. Eur. Respir. J. 2019, 54, 1901216. [Google Scholar] [CrossRef] [PubMed]
- Wang, S.; Zhou, M.; Liu, Z.; Liu, Z.; Gu, D.; Zang, Y.; Dong, D.; Gevaert, O.; Tian, J. Central focused convolutional neural networks: Developing a data-driven model for lung nodule segmentation. Med. Image Anal. 2017, 40, 172–183. [Google Scholar] [CrossRef]
- Serte, S.; Demirel, H. Deep learning for diagnosis of COVID-19 using 3D CT scans. Comput. Biol. Med. 2021, 132, 104306. [Google Scholar] [CrossRef] [PubMed]
- Li, Z.; Zhong, Z.; Li, Y.; Zhang, T.; Gao, L.; Jin, D.; Sun, Y.; Ye, X.; Yu, L.; Hu, Z.; et al. From community-acquired pneumonia to COVID-19: A deep learning–based method for quantitative analysis of COVID-19 on thick-section CT scans. Eur. Radiol. 2020, 30, 6828–6837. [Google Scholar] [CrossRef]
- Alshazly, H.; Linse, C.; Barth, E.; Martinetz, T. Explainable COVID-19 Detection Using Chest CT Scans and Deep Learning. Sensors 2021, 21, 455. [Google Scholar] [CrossRef]
- Yousefzadeh, M.; Esfahanian, P.; Movahed, S.M.S.; Gorgin, S.; Rahmati, D.; Abedini, A.; Nadji, S.A.; Haseli, S.; Bakhshayesh Karam, M.; Kiani, A.; et al. ai-corona: Radiologist-assistant deep learning framework for COVID-19 diagnosis in chest CT scans. PLoS ONE 2021, 16, e0250952. [Google Scholar]
- Hasan, A.M.; Al-Jawad, M.M.; Jalab, H.A.; Shaiba, H.; Ibrahim, R.W.; AL-Shamasneh, A.A.R. Classification of COVID-19 coronavirus, pneumonia and healthy lungs in CT scans using Q-deformed entropy and deep learning features. Entropy 2020, 22, 517. [Google Scholar] [CrossRef]
- Shah, V.; Keniya, R.; Shridharani, A.; Punjabi, M.; Shah, J.; Mehendale, N. Diagnosis of COVID-19 using CT scan images and deep learning techniques. Emerg. Radiol. 2021, 28, 497–505. [Google Scholar] [CrossRef] [PubMed]
- Zheng, C.; Deng, X.; Fu, Q.; Zhou, Q.; Feng, J.; Ma, H.; Liu, W.; Wang, X. Deep learning-based detection for COVID-19 from chest CT using weak label. MedRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Shalbaf, A.; Vafaeezadeh, M. Automated detection of COVID-19 using ensemble of transfer learning with deep convolutional neural network based on CT scans. Int. J. Comput. Assist. Radiol. Surg. 2021, 16, 115–123. [Google Scholar]
- Wu, X.; Chen, C.; Zhong, M.; Wang, J.; Shi, J. COVID-AL: The diagnosis of COVID-19 with deep active learning. Med. Image Anal. 2021, 68, 101913. [Google Scholar] [CrossRef]
- Särkkä, S.; Sarmavuori, J. Gaussian filtering and smoothing for continuous-discrete dynamic systems. Signal Processing 2013, 93, 500–510. [Google Scholar] [CrossRef]
- Hochreiter, S.; Schmidhuber, J. Long short-term memory. Neural Comput. 1997, 9, 1735–1780. [Google Scholar] [CrossRef]
- Lynn, H.M.; Pan, S.B.; Kim, P. A deep bidirectional GRU network model for biometric electrocardiogram classification based on recurrent neural networks. IEEE Access 2019, 7, 145395–145405. [Google Scholar] [CrossRef]
- Dey, R.; Salem, F.M. Gate-variants of gated recurrent unit (GRU) neural networks. In Proceedings of the 2017 IEEE 60th International Midwest Symposium on Circuits and Systems (MWSCAS), Boston, MA, USA, 6–9 August 2017; pp. 1597–1600. [Google Scholar]
- Abedinia, O.; Amjady, N.; Ghasemi, A. A new metaheuristic algorithm based on shark smell optimization. Complexity 2016, 21, 97–116. [Google Scholar] [CrossRef]
- Mohammadi, M.; Talebpour, F.; Safaee, E.; Ghadimi, N.; Abedinia, O. Small-Scale Building Load Forecast based on Hybrid Forecast Engine. Neural Process. Lett. 2018, 48, 329–351. [Google Scholar] [CrossRef]
- Zhou, Y.; Ye, J.; Du, Y.; Sheykhahmad, F.R. New improved optimized method for medical image enhancement based on modified shark smell optimization algorithm. Sens. Imaging 2020, 21, 20. [Google Scholar] [CrossRef]
- Seifi, A.; Ehteram, M.; Soroush, F. Uncertainties of instantaneous influent flow predictions by intelligence models hybridized with multi-objective shark smell optimization algorithm. J. Hydrol. 2020, 587, 124977. [Google Scholar] [CrossRef]
- Manzo, M.; Pellino, S. Fighting Together against the Pandemic: Learning Multiple Models on Tomography Images for COVID-19 Diagnosis. AI 2021, 2, 261–273. [Google Scholar] [CrossRef]
- Segera, D.; Mbuthia, M.; Nyete, A. Particle Swarm Optimized Hybrid Kernel-Based Multiclass Support Vector Machine for Microarray Cancer Data Analysis. BioMed Res. Int. 2019, 2019, 4085725. [Google Scholar] [CrossRef] [Green Version]
- Aizerman, M.A. Theoretical foundations of the potential function method in pattern recognition learning. Autom. Remote Control. 1964, 25, 821–837. [Google Scholar]
- Rodrigues, D.; Pereira, L.A.; Nakamura, R.Y.; Costa, K.A.; Yang, X.S.; Souza, A.N.; Papa, J.P. A wrapper approach for feature selection based on bat algorithm and optimum-path forest. Expert Syst. Appl. 2014, 41, 2250–2258. [Google Scholar] [CrossRef]
- Mansour, R.F.; Aljehane, N.O. An optimal segmentation with deep learning based inception network model for intracranial hemorrhage diagnosis. Neural Comput. Appl. 2021, 33, 13831–13843. [Google Scholar] [CrossRef]
- Li, L.; Sun, L.; Xue, Y.; Li, S.; Huang, X.; Mansour, R.F. Fuzzy Multilevel Image Thresholding Based on Improved Coyote Optimization Algorithm. IEEE Access 2021, 9, 33595–33607. [Google Scholar] [CrossRef]
- Haklı, H.; Uğuz, H. A novel particle swarm optimization algorithm with Levy flight. Appl. Soft Comput. 2014, 23, 333–345. [Google Scholar] [CrossRef]
- Zhao, J.; Zhang, Y.; He, X.; Xie, P. COVID-CT-Dataset: A CT Scan Dataset about COVID-19. arXiv 2020, arXiv:2003.13865. Available online: https://github.com/UCSD-AI4H/COVID-CT (accessed on 18 October 2021).
- Subhalakshmi, R.T.; Balamurugan, S.A.A.; Sasikala, S. Deep learning based fusion model for COVID-19 diagnosis and classification using computed tomography images. Concurr. Eng. 2021, 1–12. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
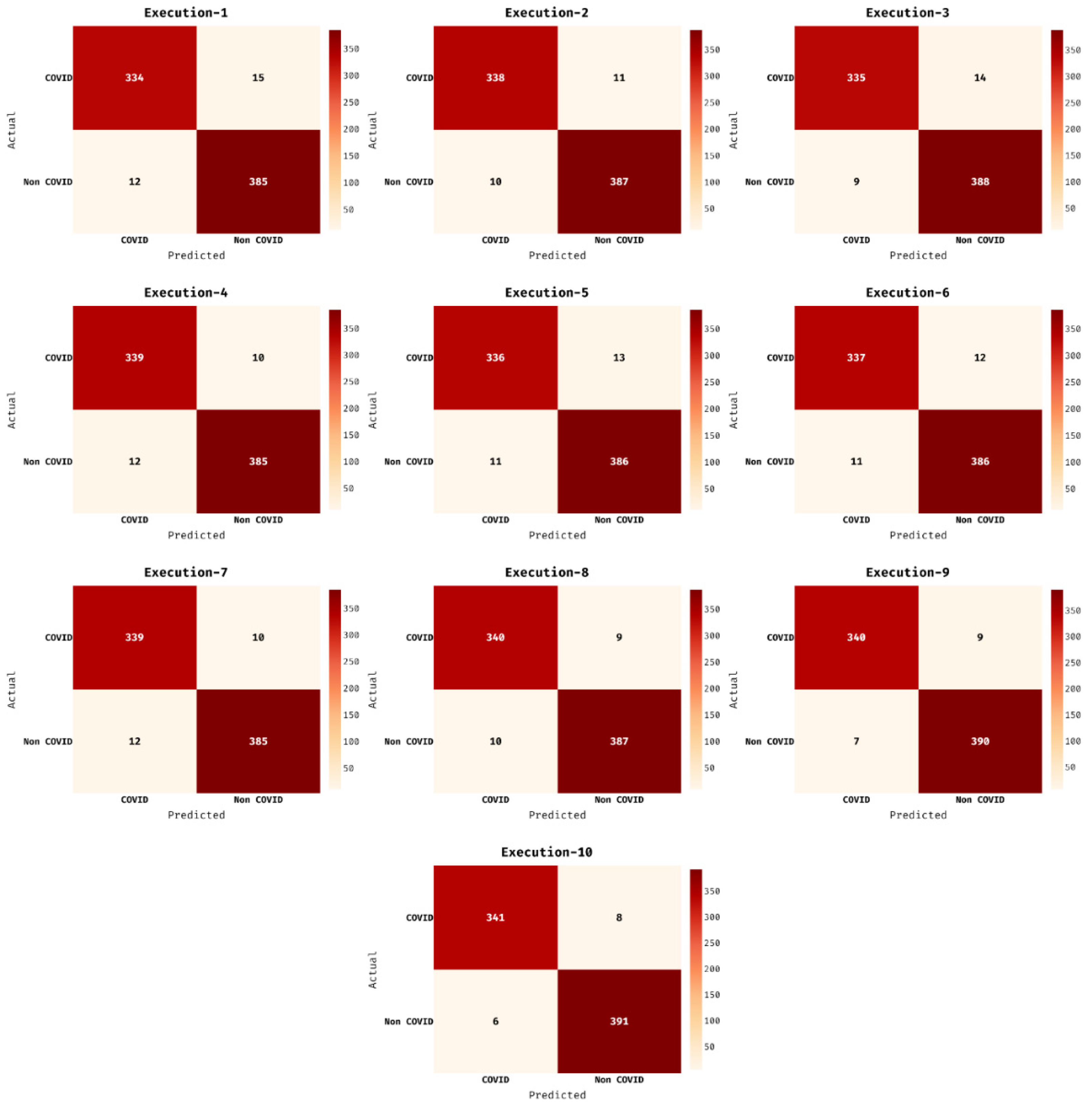
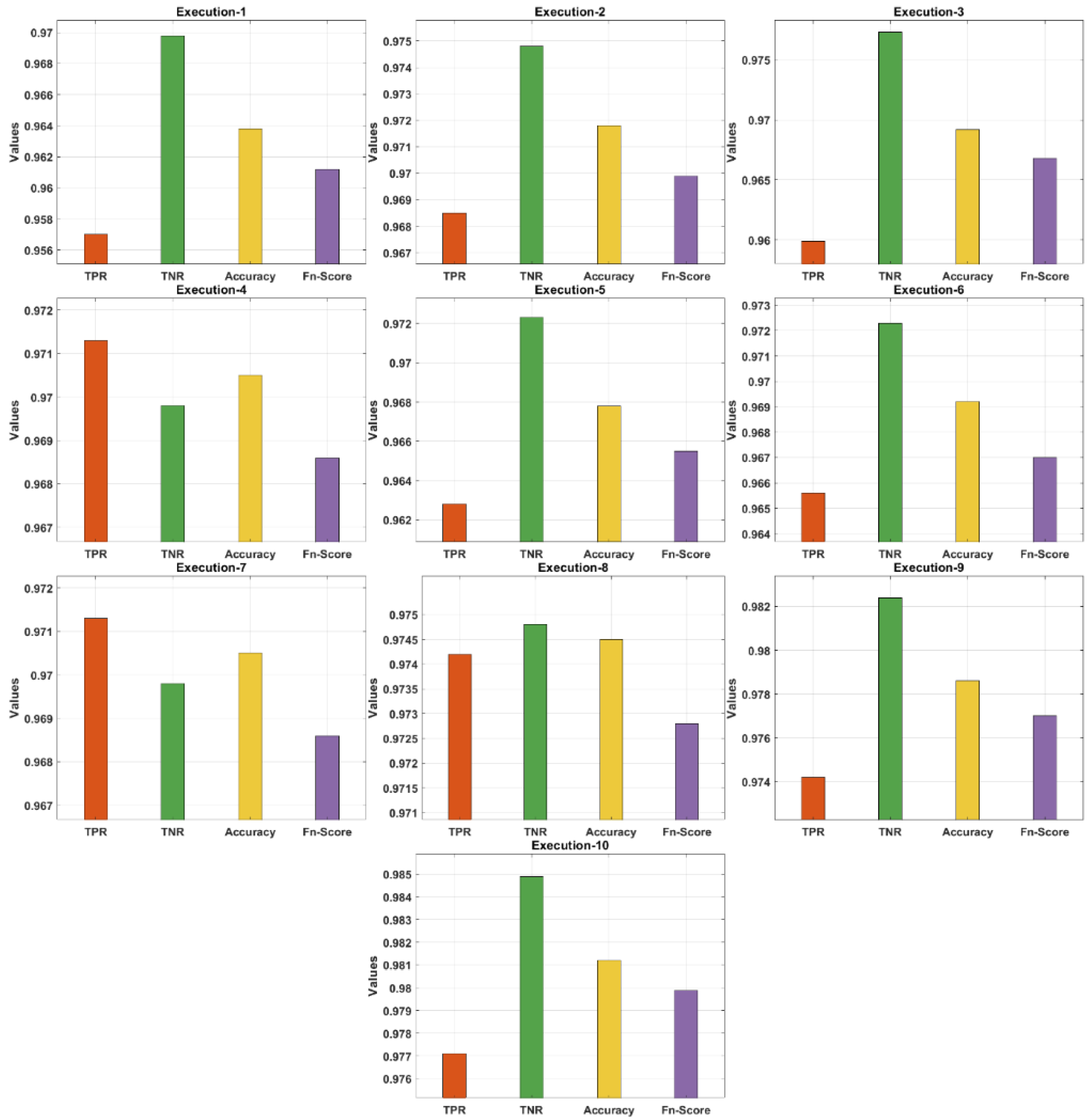
| No. of Execution | TPR | TNR | Accuracy | F-Score |
|---|---|---|---|---|
| Execution-1 | 0.9570 | 0.9698 | 0.9638 | 0.9612 |
| Execution-2 | 0.9685 | 0.9748 | 0.9718 | 0.9699 |
| Execution-3 | 0.9599 | 0.9773 | 0.9692 | 0.9668 |
| Execution-4 | 0.9713 | 0.9698 | 0.9705 | 0.9686 |
| Execution-5 | 0.9628 | 0.9723 | 0.9678 | 0.9655 |
| Execution-6 | 0.9656 | 0.9723 | 0.9692 | 0.9670 |
| Execution-7 | 0.9713 | 0.9698 | 0.9705 | 0.9686 |
| Execution-8 | 0.9742 | 0.9748 | 0.9745 | 0.9728 |
| Execution-9 | 0.9742 | 0.9824 | 0.9786 | 0.9770 |
| Execution-10 | 0.9771 | 0.9849 | 0.9812 | 0.9799 |
| Average | 0.9682 | 0.9748 | 0.9717 | 0.9697 |
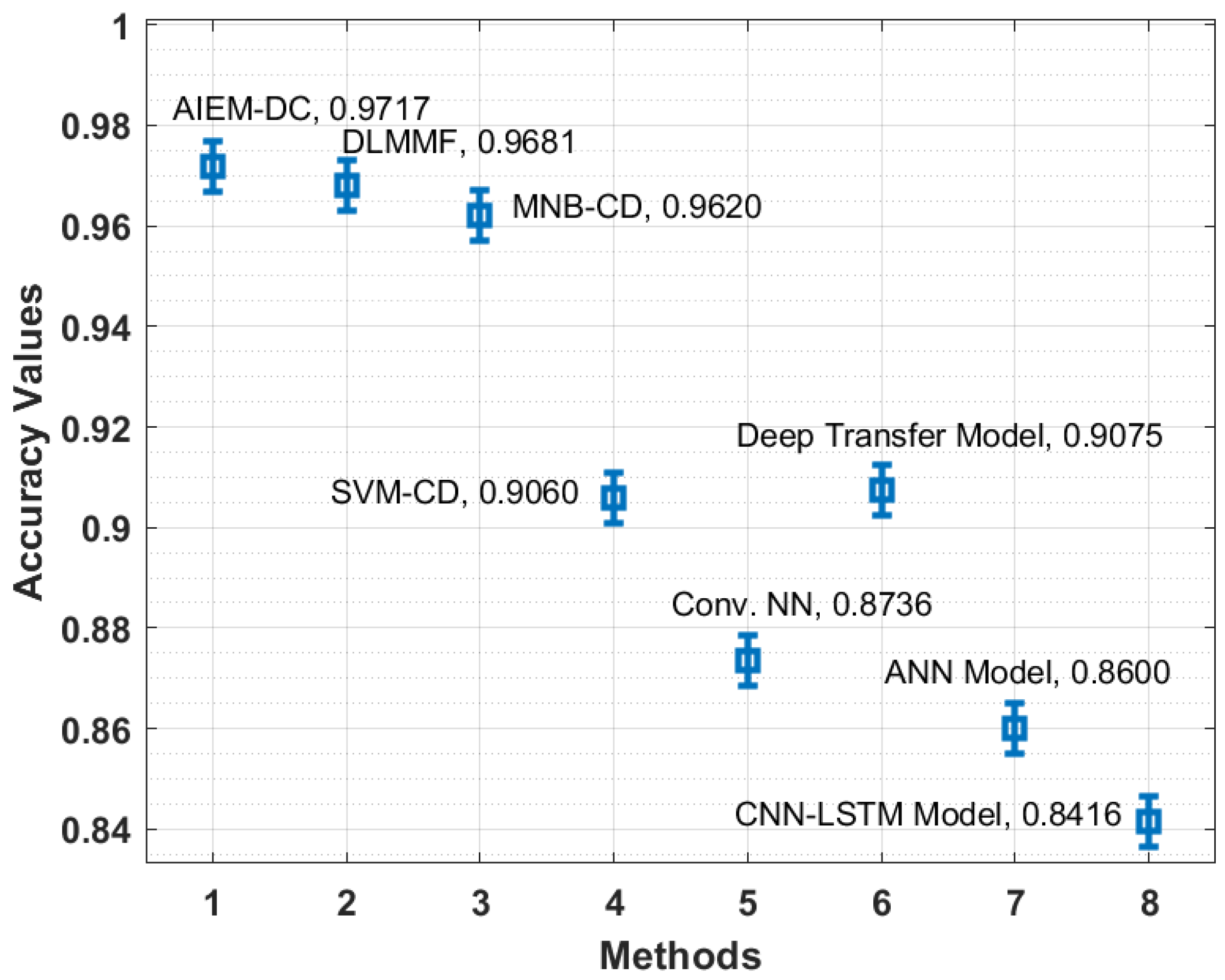
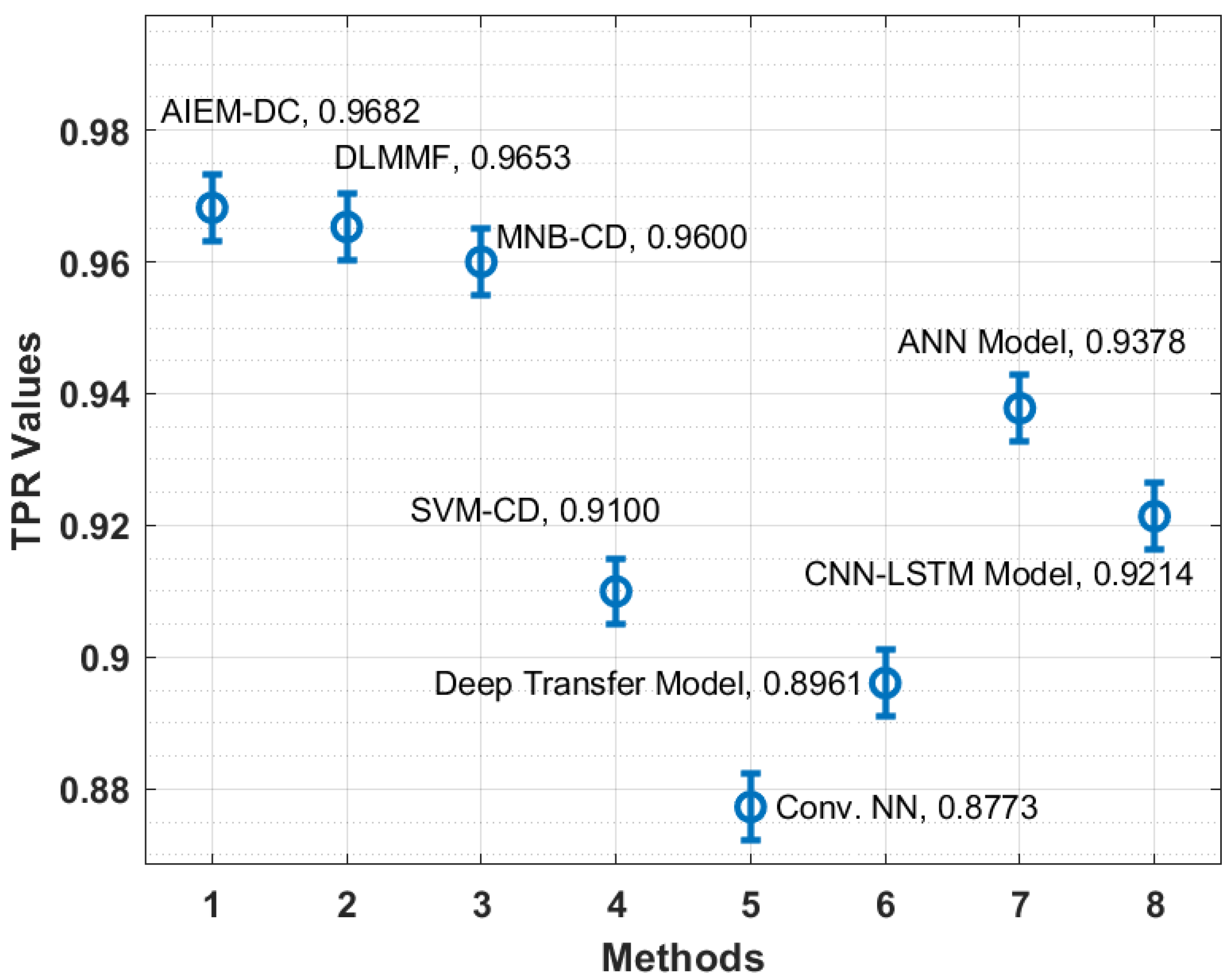
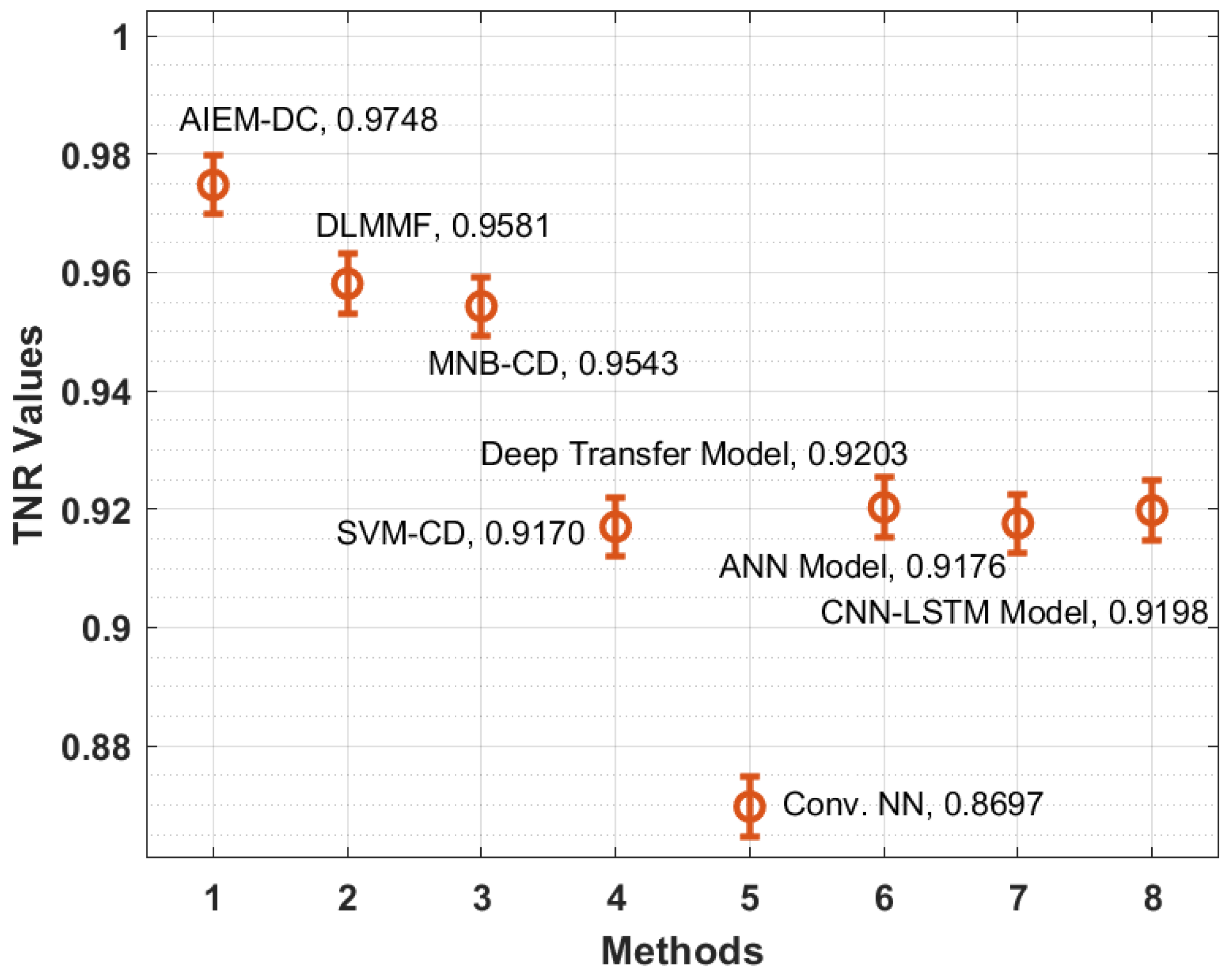
| Methods | TPR | TNR | Accuracy | F-Score |
|---|---|---|---|---|
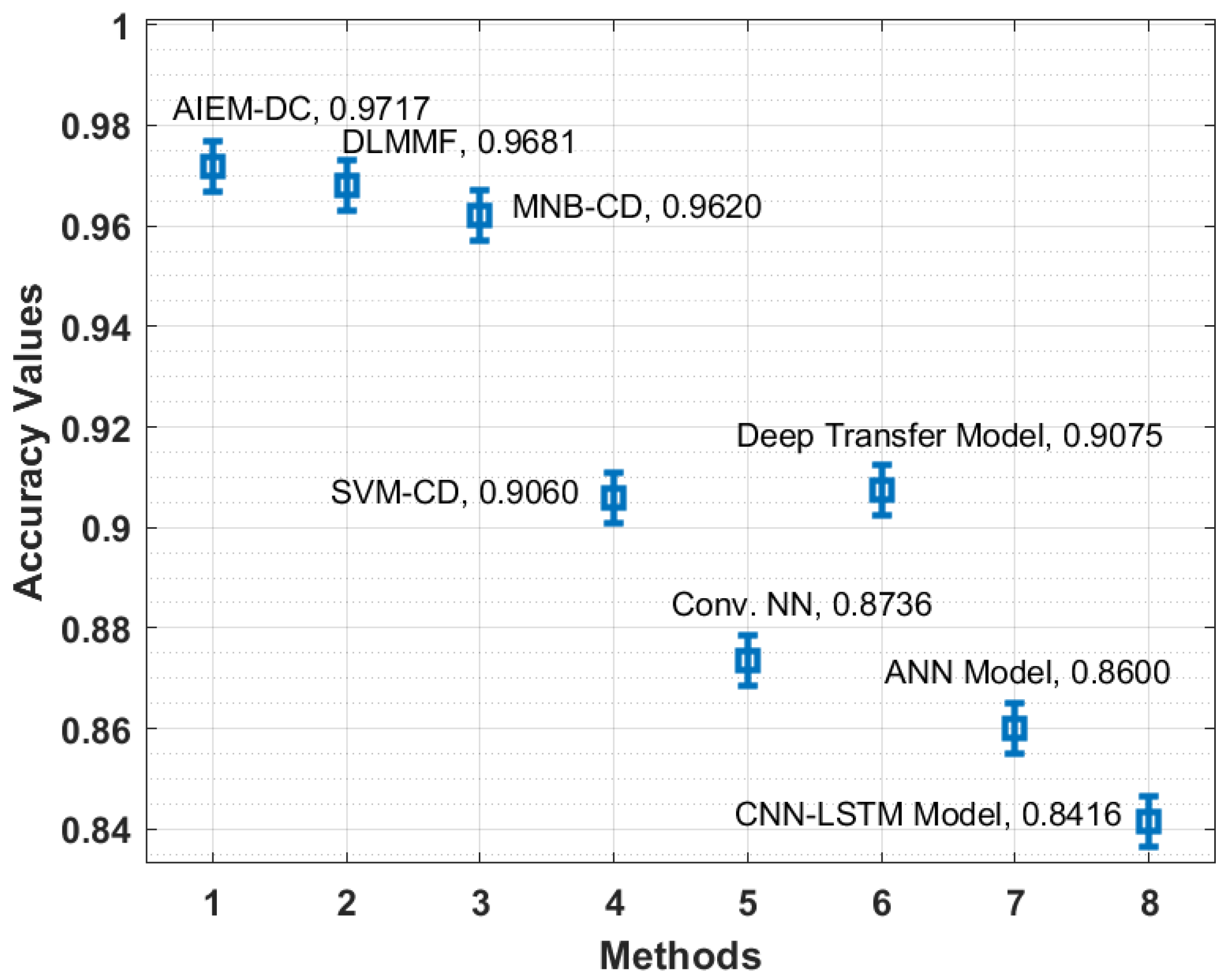
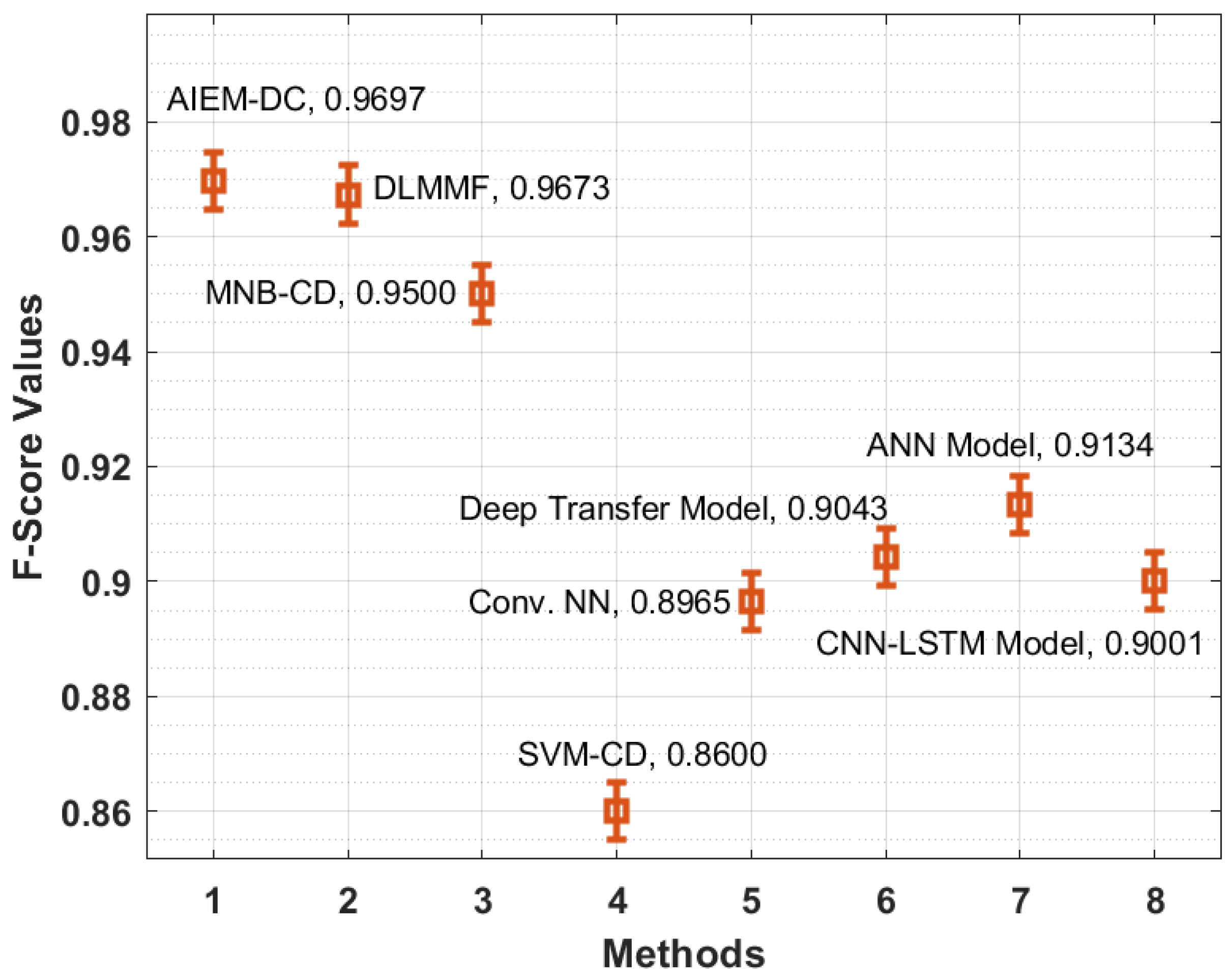
| AIEM-DC (Ours) | 0.9682 | 0.9748 | 0.9717 | 0.9697 |
| DLMMF | 0.9653 | 0.9581 | 0.9681 | 0.9673 |
| MNB-CD | 0.9600 | 0.9543 | 0.9620 | 0.9500 |
| SVM-CD | 0.9100 | 0.9170 | 0.9060 | 0.8600 |
| Conv. NN | 0.8773 | 0.8697 | 0.8736 | 0.8965 |
| Deep Transfer Model | 0.8961 | 0.9203 | 0.9075 | 0.9043 |
| ANN Model | 0.9378 | 0.9176 | 0.8600 | 0.9134 |
| CNN-LSTM Model | 0.9214 | 0.9198 | 0.8416 | 0.9001 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ragab, M.; Eljaaly, K.; Alhakamy, N.A.; Alhadrami, H.A.; Bahaddad, A.A.; Abo-Dahab, S.M.; Khalil, E.M. Deep Ensemble Model for COVID-19 Diagnosis and Classification Using Chest CT Images. Biology 2022, 11, 43. https://doi.org/10.3390/biology11010043
Ragab M, Eljaaly K, Alhakamy NA, Alhadrami HA, Bahaddad AA, Abo-Dahab SM, Khalil EM. Deep Ensemble Model for COVID-19 Diagnosis and Classification Using Chest CT Images. Biology. 2022; 11(1):43. https://doi.org/10.3390/biology11010043
Chicago/Turabian StyleRagab, Mahmoud, Khalid Eljaaly, Nabil A. Alhakamy, Hani A. Alhadrami, Adel A. Bahaddad, Sayed M. Abo-Dahab, and Eied M. Khalil. 2022. "Deep Ensemble Model for COVID-19 Diagnosis and Classification Using Chest CT Images" Biology 11, no. 1: 43. https://doi.org/10.3390/biology11010043
APA StyleRagab, M., Eljaaly, K., Alhakamy, N. A., Alhadrami, H. A., Bahaddad, A. A., Abo-Dahab, S. M., & Khalil, E. M. (2022). Deep Ensemble Model for COVID-19 Diagnosis and Classification Using Chest CT Images. Biology, 11(1), 43. https://doi.org/10.3390/biology11010043