
Intermittent Sequential Pneumatic Compression Improves Coupling between Cerebral Oxyhaemoglobin and Arterial Blood Pressure in Patients with Cerebral Infarction

 ,
,
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Participants
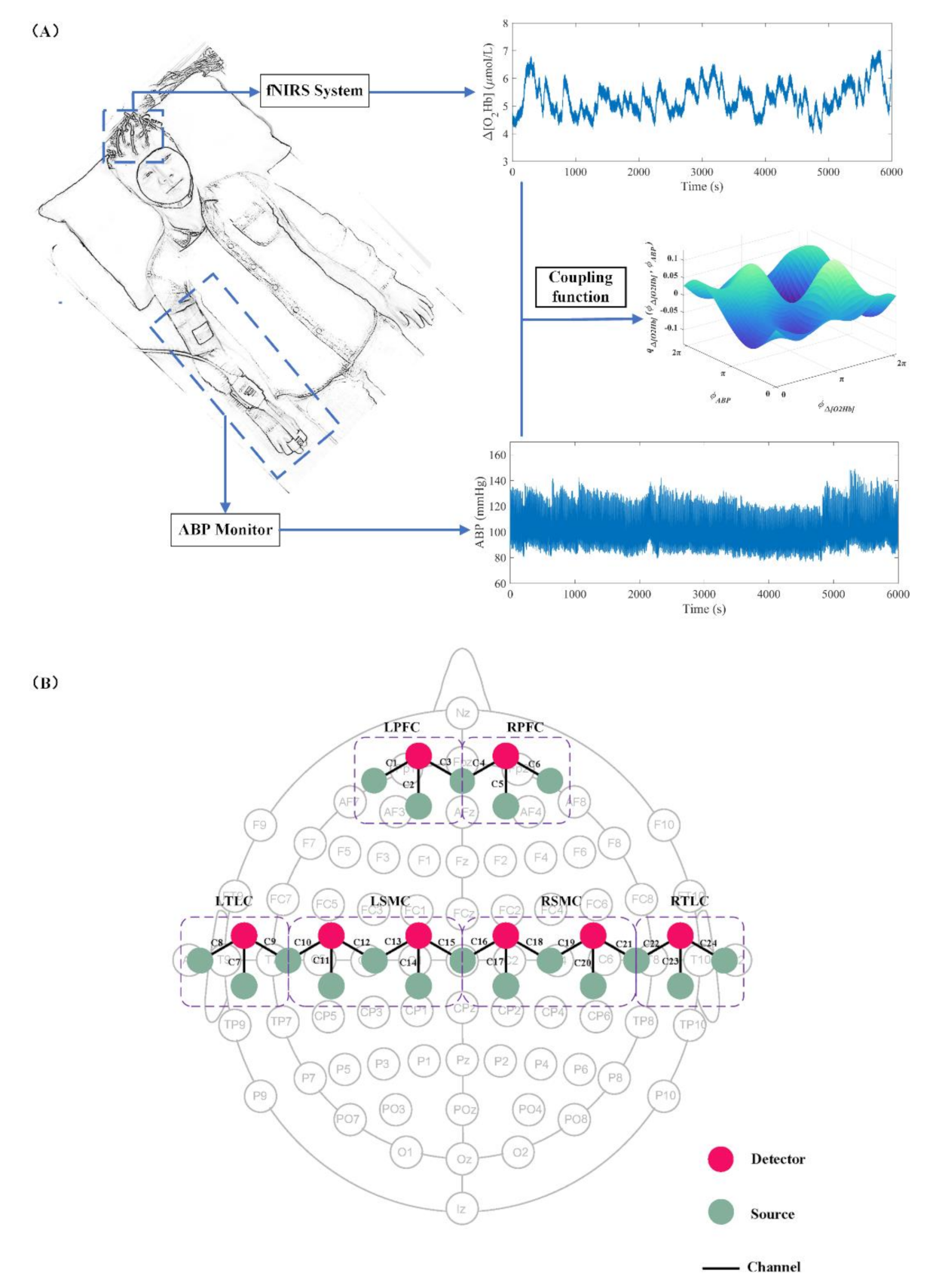
2.2. Instrumentation
2.3. Experimental Design
2.4. Data Preprocessing and Spectral Analysis
2.4.1. Data Preprocessing
2.4.2. Phase Extraction and Coupling Analysis
2.5. Statistical Analysis
3. Results
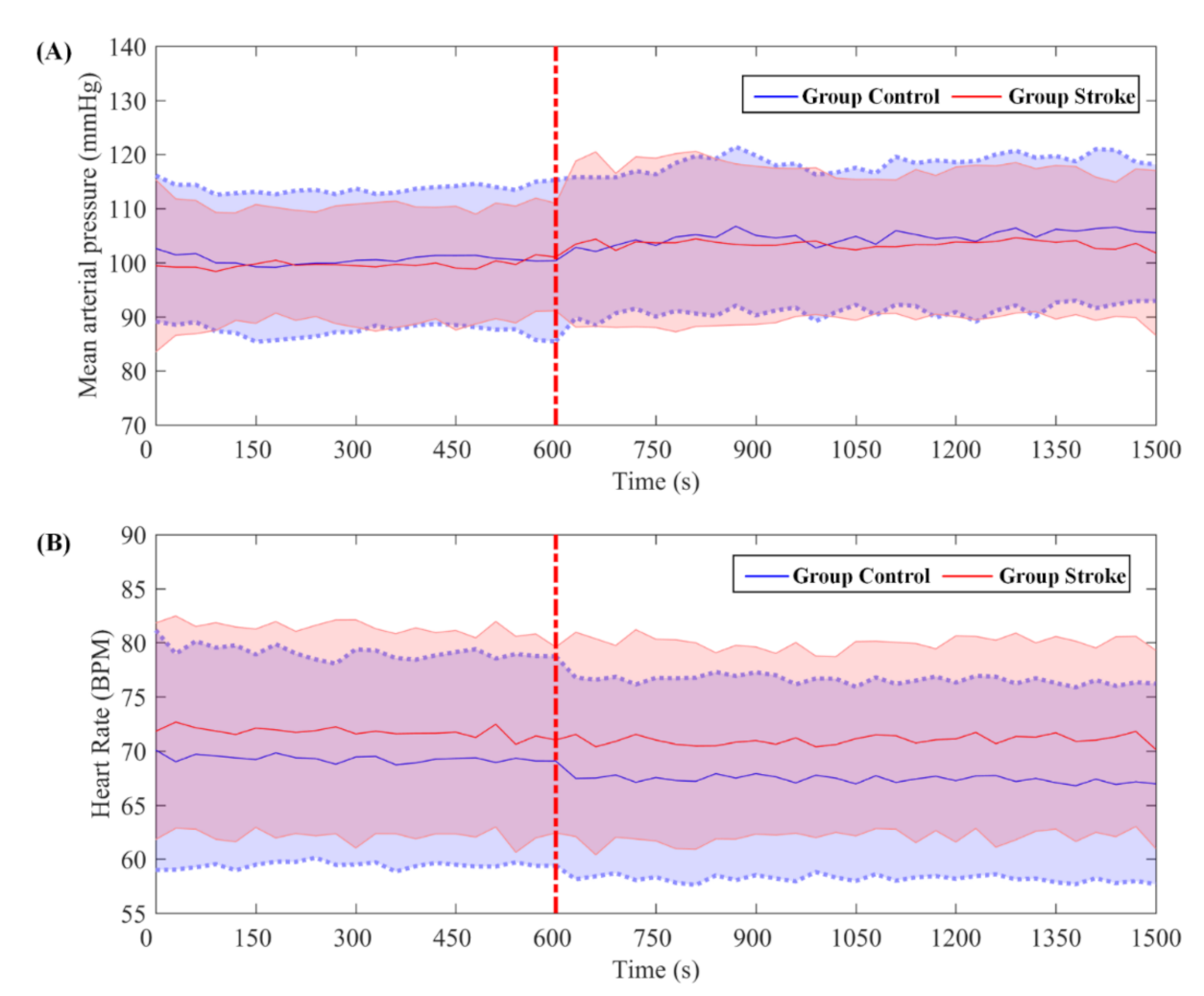
3.1. Systemic Measurements
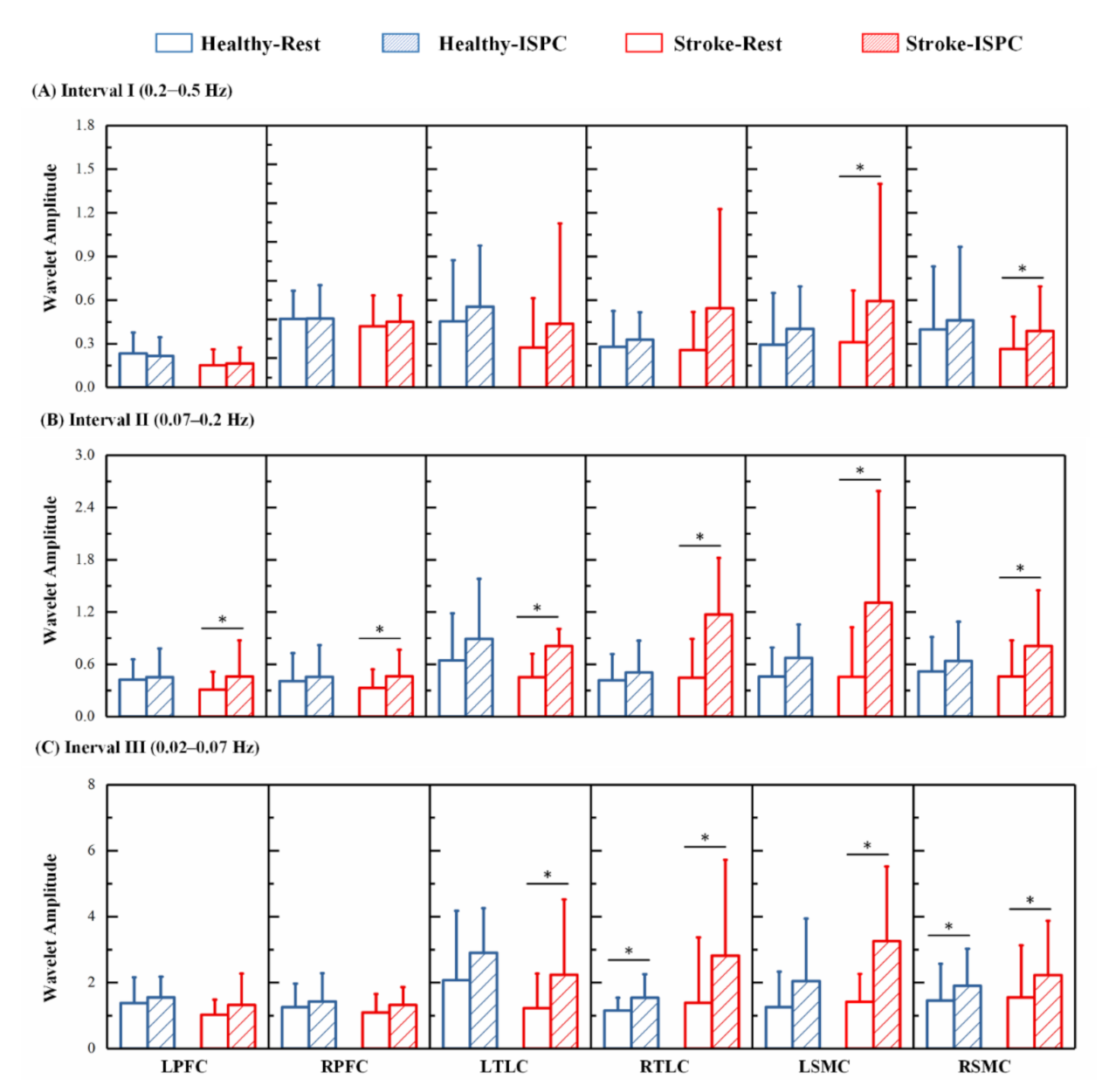
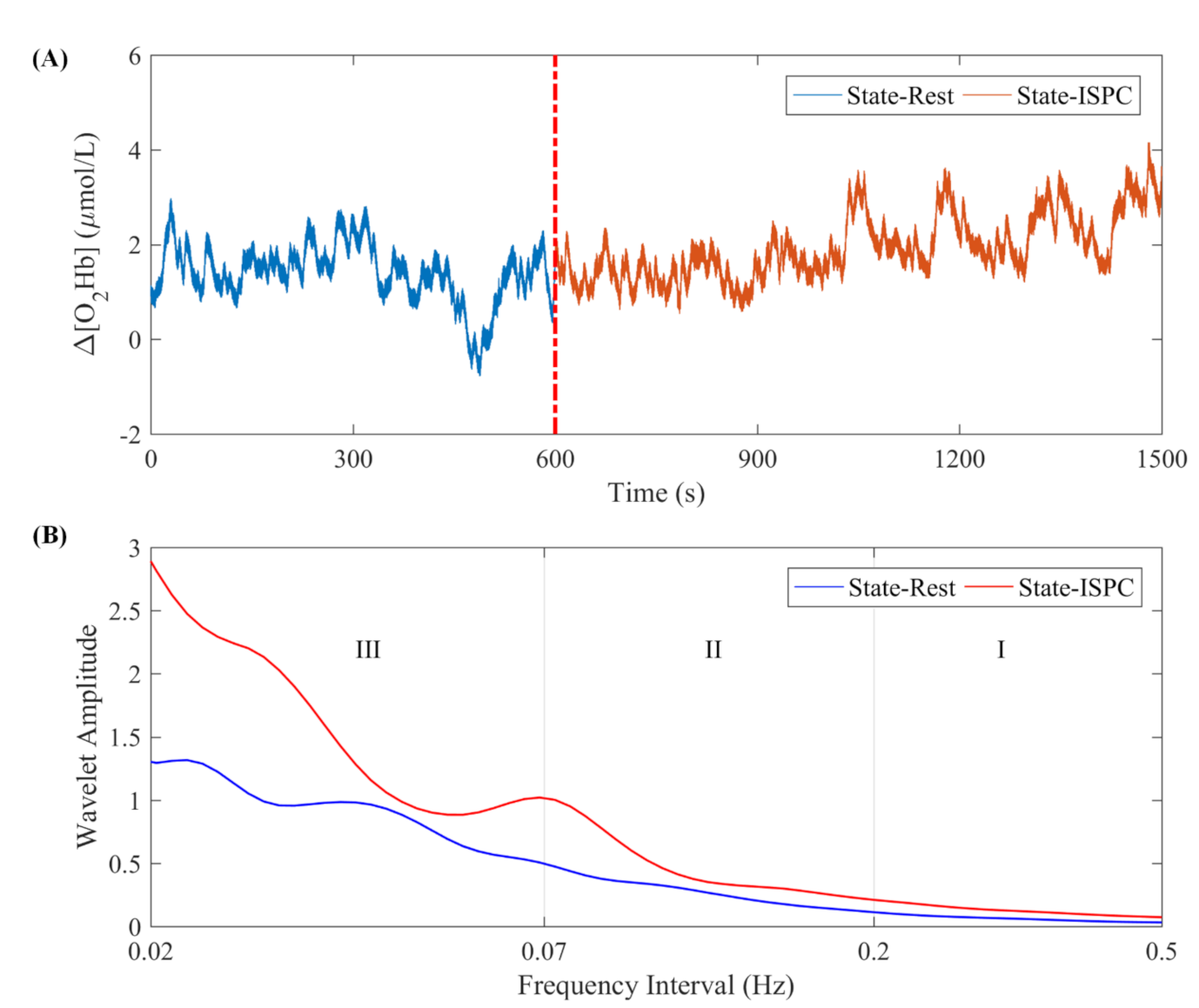
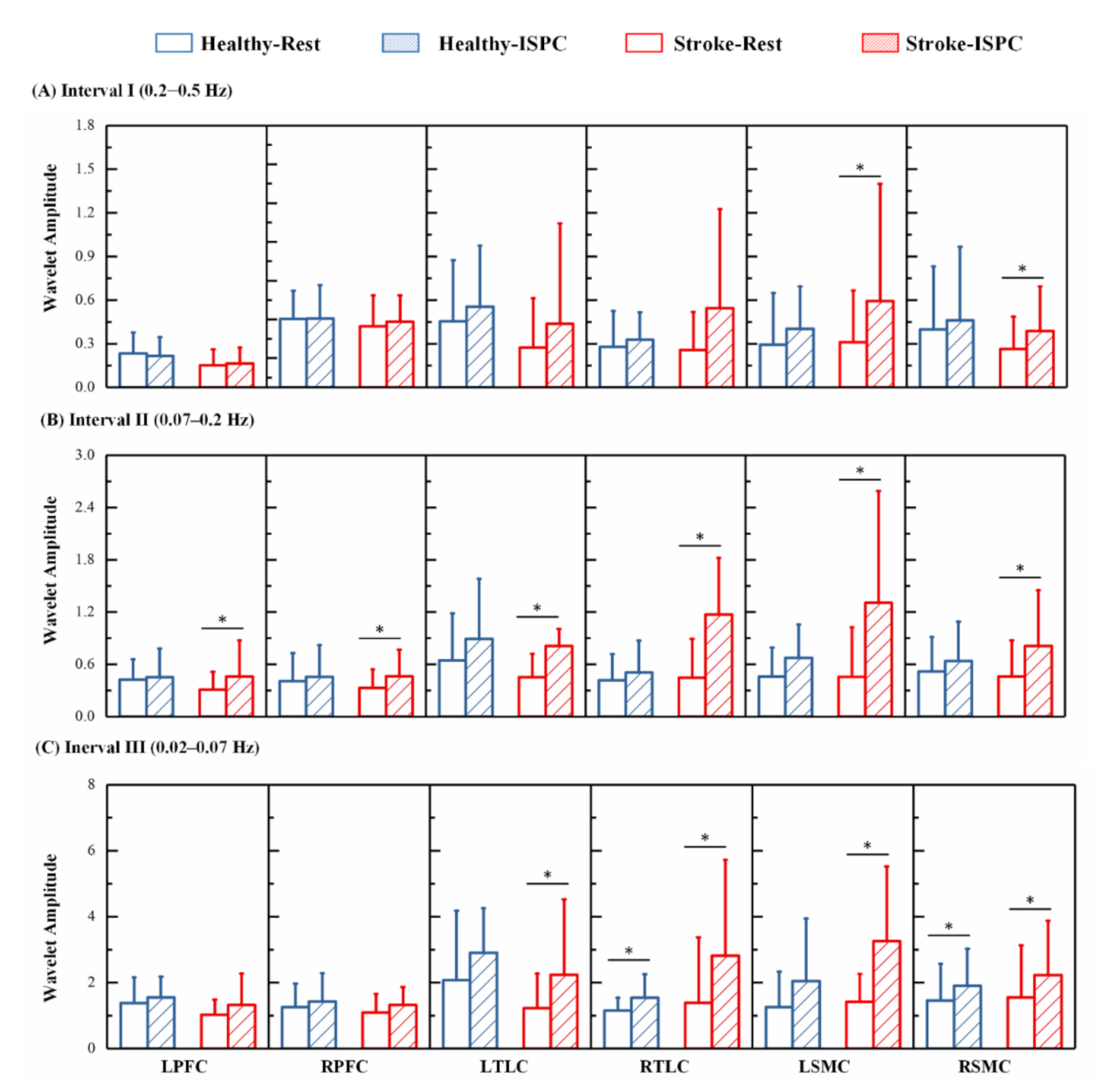
3.2. Cerebral Oscillation Measurements
3.3. Relationship between the Cerebral and Systemic Oscillations
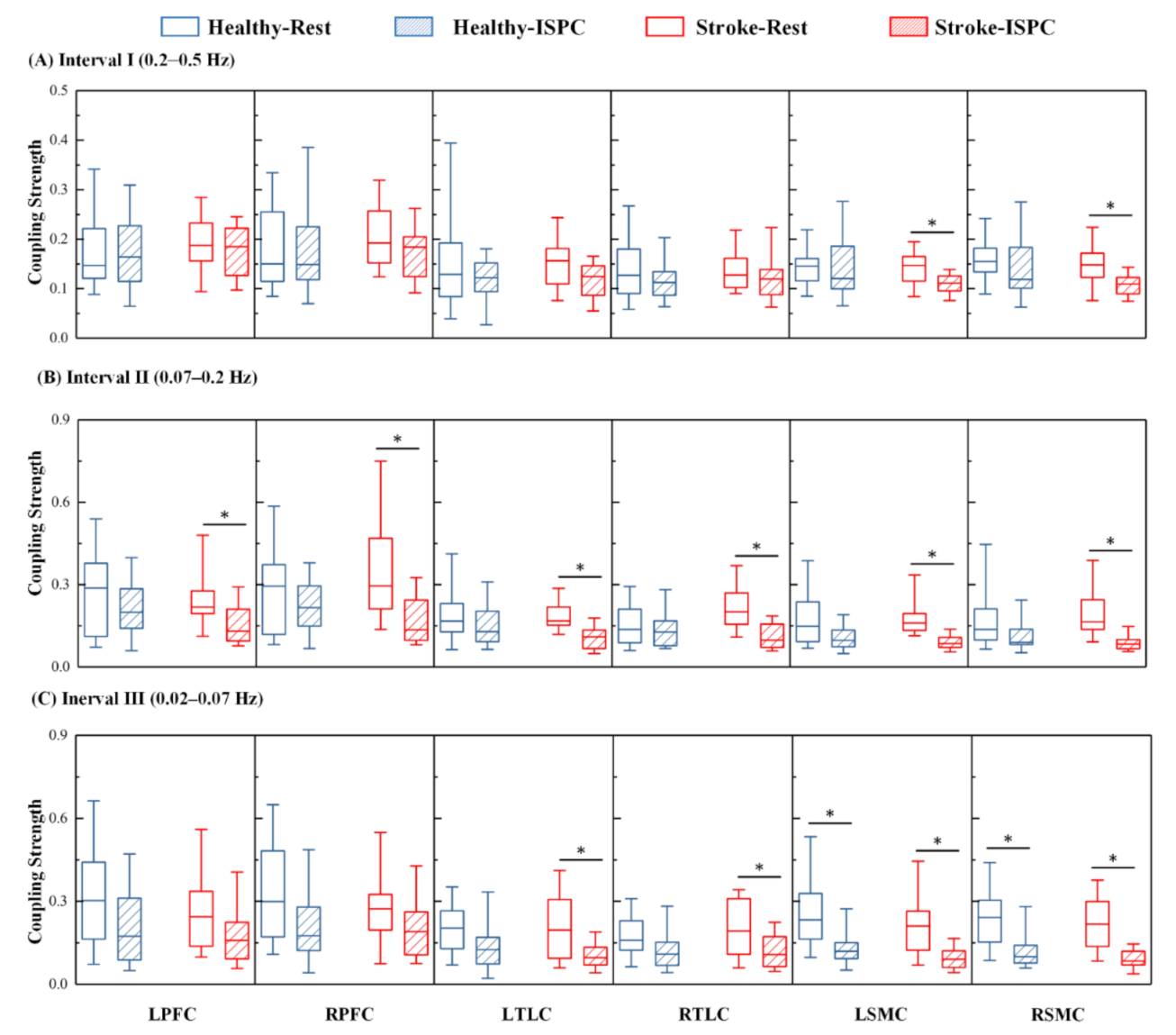
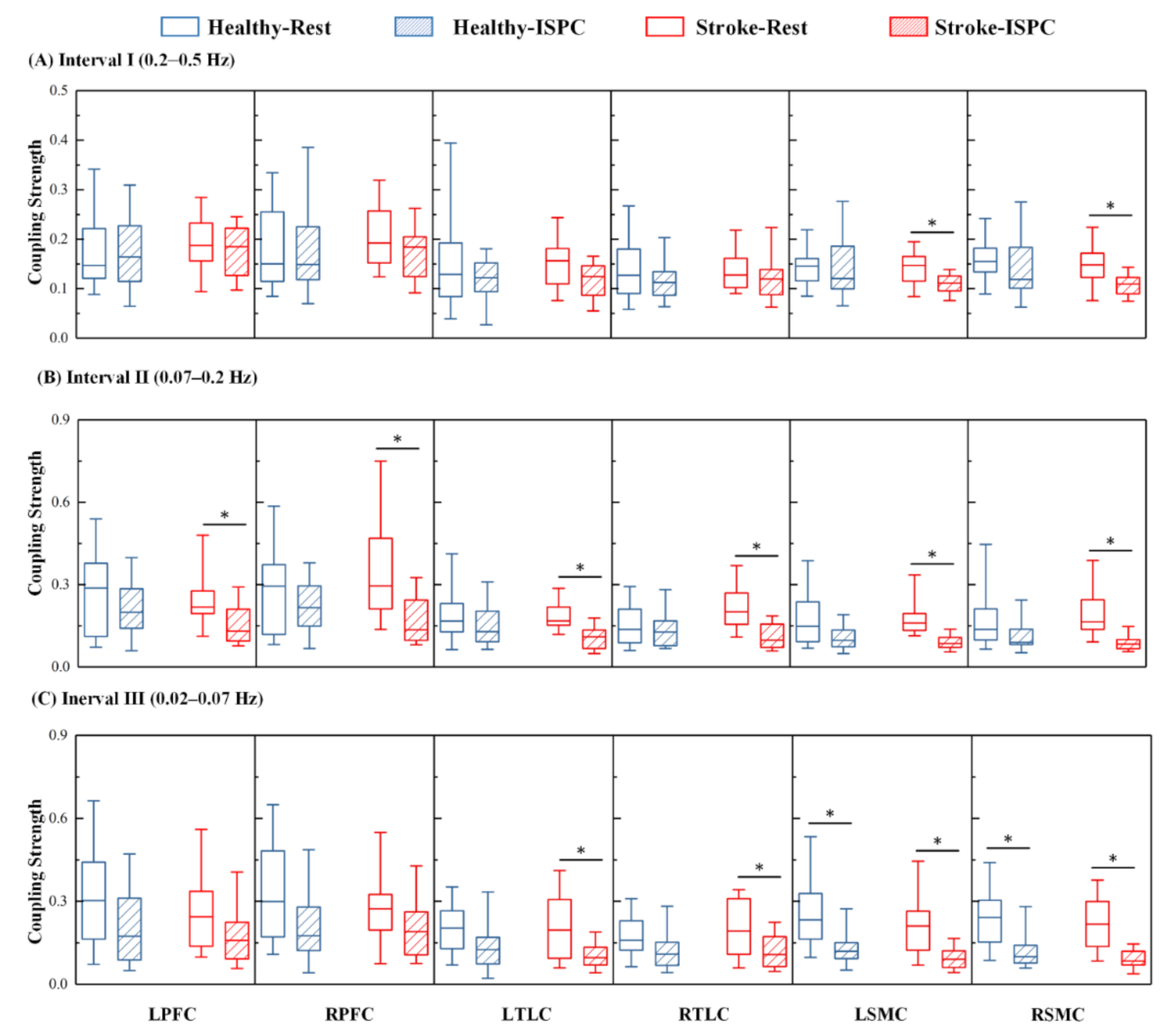
3.4. Changes in the Coupling Strength
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Feigin, V.L.; Forouzanfar, M.H.; Krishnamurthi, R.; Mensah, G.A.; Connor, M.; Bennett, D.A.; Moran, A.E.; Sacco, R.L.; Anderson, L.; Truelsen, T.; et al. Global and regional burden of stroke during 1990-2010: Findings from the global burden of disease study 2010. Lancet 2014, 383, 245–255. [Google Scholar] [CrossRef]
- Bajaj, S.; Butler, A.J.; Drake, D.; Dhamala, M. Functional organization and restoration of the brain motor-execution network after stroke and rehabilitation. Front. Hum. Neurosci. 2015, 9, 173. [Google Scholar] [CrossRef] [Green Version]
- Stankovski, T.; Petkoski, S.; Raeder, J.; Smith, A.F.; McClintock, P.V.; Stefanovska, A. Alterations in the coupling functions between cortical and cardio-respiratory oscillations due to anaesthesia with propofol and sevoflurane. Philos. Trans. R. Soc. A 2016, 374, 20150186. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chi, N.-F.; Hu, H.-H.; Chan, L.; Wang, C.-Y.; Chao, S.-P.; Huang, L.-K.; Ku, H.-L.; Hu, C.-J. Impaired cerebral autoregulation is associated with poststroke cognitive impairment. Ann. Clin. Transl. Neurol. 2020, 7, 1092–1102. [Google Scholar] [CrossRef] [PubMed]
- Wei, J.; Zhu, X.; Xia, L.; Zhao, Y.; Yang, G.; Han, Q.; Shen, J. Intermittent pneumatic compression combined with rehabilitation training improves motor function deficits in patients with acute cerebral infarction. Acta Neurol. Belg. 2020. [Google Scholar] [CrossRef]
- Sheldon, R.D.; Roseguini, B.T.; Laughlin, M.H.; Newcomer, S.C. New insights into the physiologic basis for intermittent pneumatic limb compression as a therapeutic strategy for peripheral artery disease. J. Vasc. Surg. 2013, 58, 1688–1696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scholkmann, F.; Kleiser, S.; Metz, A.J.; Zimmermann, R.; Mata Pavia, J.; Wolf, U.; Wolf, M. A review on continuous wave functional near-infrared spectroscopy and imaging instrumentation and methodology. Neuroimage 2014, 85 Pt 1, 6–27. [Google Scholar] [CrossRef]
- Vasta, R.; Cutini, S.; Cerasa, A.; Gramigna, V.; Olivadese, G.; Arabia, G.; Quattrone, A. Physiological aging influence on brain hemodynamic activity during task-switching: A fnirs study. Front. Aging Neurosci. 2018, 9, 433. [Google Scholar] [CrossRef] [Green Version]
- Agbangla, N.F.; Audiffren, M.; Albinet, C.T. Use of near-infrared spectroscopy in the investigation of brain activation during cognitive aging: A systematic review of an emerging area of research. Ageing Res. Rev. 2017, 38, 52–66. [Google Scholar] [CrossRef]
- Tian, F.; Tarumi, T.; Liu, H.; Zhang, R.; Chalak, L. Wavelet coherence analysis of dynamic cerebral autoregulation in neonatal hypoxic–ischemic encephalopathy. Neuroimage Clin. 2016, 11, 124–132. [Google Scholar] [CrossRef] [Green Version]
- Tgavalekos, K.; Pham, T.; Krishnamurthy, N.; Sassaroli, A.; Fantini, S. Frequency-resolved analysis of coherent oscillations of local cerebral blood volume, measured with near-infrared spectroscopy, and systemic arterial pressure in healthy human subjects. PLoS ONE 2019, 14, e0211710. [Google Scholar] [CrossRef] [PubMed]
- Addison, P.S. A review of wavelet transform time-frequency methods for nirs-based analysis of cerebral autoregulation. IEEE Rev. Biomed. Eng. 2015, 8, 78–85. [Google Scholar] [CrossRef]
- Stankovski, T.; Ticcinelli, V.; McClintock, P.V.; Stefanovska, A. Coupling functions in networks of oscillators. New J. Phys. 2015, 17, 035002. [Google Scholar] [CrossRef]
- Li, W.; Zhang, M.; Huo, C.; Xu, G.; Chen, W.; Wang, D.; Li, Z. Time-evolving coupling functions for evaluating the interaction between cerebral oxyhemoglobin and arterial blood pressure with hypertension. Med. Phys. 2021, 48, 2027–2037. [Google Scholar] [CrossRef] [PubMed]
- Stankovski, T.; Pereira, T.; Mcclintock, P.V.E.; Stefanovska, A. Coupling functions: Universal insights into dynamical interaction mechanisms. Rev. Mod. Phys. 2017, 89, 045001. [Google Scholar] [CrossRef] [Green Version]
- Puh, U.; Vovk, A.; Sevsek, F.; Suput, D. Increased cognitive load during simple and complex motor tasks in acute stage after stroke. Int. J. Psychophysiol. 2007, 63, 173–180. [Google Scholar] [CrossRef]
- Schaechter, J.D. Motor rehabilitation and brain plasticity after hemiparetic stroke. Prog. Neurobiol. 2004, 73, 61–72. [Google Scholar] [CrossRef]
- Tachtsidis, I.; Scholkmann, F. False positives and false negatives in functional near-infrared spectroscopy: Issues, challenges, and the way forward. Neurophotonics 2016, 3, 031405. [Google Scholar]
- Holper, L.; Scholkmann, F.; Wolf, M. Between-brain connectivity during imitation measured by fnirs. Neuroimage 2012, 63, 212–222. [Google Scholar] [CrossRef]
- van de Ven, V.G.; Formisano, E.; Prvulovic, D.; Roeder, C.H.; Linden, D.E. Functional connectivity as revealed by spatial independent component analysis of fmri measurements during rest. Hum. Brain Mapp. 2004, 22, 165–178. [Google Scholar] [CrossRef]
- Zhang, H.; Zhang, Y.-J.; Lu, C.-M.; Ma, S.-Y.; Zang, Y.-F.; Zhu, C.-Z. Functional connectivity as revealed by independent component analysis of resting-state fnirs measurements. Neuroimage 2010, 51, 1150–1161. [Google Scholar] [CrossRef]
- Santosa, H.; Hong, M.J.; Kim, S.P.; Hong, K.S. Noise reduction in functional near-infrared spectroscopy signals by independent component analysis. Rev. Sci. Instrum. 2013, 84, 073106. [Google Scholar] [CrossRef] [PubMed]
- Scholkmann, F.; Spichtig, S.; Muehlemann, T.; Wolf, M. How to detect and reduce movement artifacts in near-infrared imaging using moving standard deviation and spline interpolation. Physiol. Meas. 2010, 31, 649. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elting, J.W.J.; Tas, J.; Aries, M.J.; Czosnyka, M.; Maurits, N.M. Dynamic cerebral autoregulation estimates derived from near infrared spectroscopy and transcranial doppler are similar after correction for transit time and blood flow and blood volume oscillations. J. Cereb. Blood Flow Metab. 2020, 40, 135–149. [Google Scholar]
- Claassen, J.A.; As, M.V.D.A.; Simpson, D.M.; Panerai, R.B. Transfer function analysis of dynamic cerebral autoregulation: A white paper from the international cerebral autoregulation research network. J. Cereb. Blood Flow Metab. 2016, 36, 665–680. [Google Scholar]
- Shiogai, Y.; Stefanovska, A.; McClintock, P.V. Nonlinear dynamics of cardiovascular ageing. Phys. Rep. 2010, 488, 51–110. [Google Scholar] [CrossRef] [Green Version]
- Sasai, S.; Homae, F.; Watanabe, H.; Sasaki, A.T.; Tanabe, H.C.; Sadato, N.; Taga, G. A nirs–fmri study of resting state network. Neuroimage 2012, 63, 179–193. [Google Scholar] [CrossRef]
- Li, Z.; Zhang, M.; Xin, Q.; Luo, S.; Cui, R.; Zhou, W.; Lu, L. Age-related changes in spontaneous oscillations assessed by wavelet transform of cerebral oxygenation and arterial blood pressure signals. J. Cereb. Blood Flow Metab. 2013, 33, 692–699. [Google Scholar]
- Xu, G.; Zhang, M.; Wang, Y.; Liu, Z.; Huo, C.; Li, Z.; Huo, M. Functional connectivity analysis of distracted drivers based on the wavelet phase coherence of functional near-infrared spectroscopy signals. PLoS ONE 2017, 12, 1–23. [Google Scholar] [CrossRef] [Green Version]
- Stankovski, T.; Ticcinelli, V.; Mcclintock, P.V.E.; Stefanovska, A. Neural cross-frequency coupling functions. Front. Syst. Neurosci. 2017, 11, 33. [Google Scholar] [CrossRef] [Green Version]
- Ticcinelli, V.; Stankovski, T.; Iatsenko, D.; Bernjak, A.; Bradbury, A.E.; Gallagher, A.R.; Clarkson, P.B.M.; McClintock, P.V.E.; Stefanovska, A. Coherence and coupling functions reveal microvascular impairment in treated hypertension. Front. Physiol. 2017, 8, 749. [Google Scholar] [CrossRef]
- Bickel, A.; Shturman, A.; Grevtzev, I.; Roguin, N.; Eitan, A. The physiological impact of intermittent sequential pneumatic compression (ispc) leg sleeves on cardiac activity. Am. J. Surg. 2011, 202, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Fanelli, G.; Zasa, M.; Baciarello, M.; Mazzani, R.; Cianni, S.D.; Rossi, M.; Casati, A. Systemic hemodynamic effects of sequential pneumatic compression of the lower limbs: A prospective study in healthy volunteers. J. Clin. Anesth. 2008, 20, 338–342. [Google Scholar] [CrossRef] [PubMed]
- Tzeng, Y.C.; Ainslie, P.N.; Cooke, W.H.; Peebles, K.C.; Willie, C.K.; MacRae, B.A.; Smirl, J.D.; Horsman, H.M.; Rickards, C.A. Assessment of cerebral autoregulation: The quandary of quantification. Am. J. Physiol.-Heart Circ. Physiol. 2012, 303, H658–H671. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, H.; Hamner, J.W.; Ishibashi, K.; Tan, C.O. Relative contributions of systemic hemodynamic variables to cerebral autoregulation during orthostatic stress. J. Appl. Physiol. 2018, 124, 321–329. [Google Scholar] [CrossRef]
- Hamner, J.W.; Tan, C.O. Relative contributions of sympathetic, cholinergic, and myogenic mechanisms to cerebral autoregulation. Stroke 2014, 45, 1771–1777. [Google Scholar] [CrossRef] [Green Version]
- Katura, T.; Tanaka, N.; Obata, A.; Sato, H.; Maki, A. Quantitative evaluation of interrelations between spontaneous low-frequency oscillations in cerebral hemodynamics and systemic cardiovascular dynamics. NeuroImage 2006, 31, 1592–1600. [Google Scholar] [CrossRef]
- Lin, W.; Xiong, L.; Han, J.; Leung Thomas Wai, H.; Soo Yannie Oi, Y.; Chen, X.; Wong Ka Sing, L. External counterpulsation augments blood pressure and cerebral flow velocities in ischemic stroke patients with cerebral intracranial large artery occlusive disease. Stroke 2012, 43, 3007–3011. [Google Scholar] [CrossRef]
- Faraco, G.; Iadecola, C. Hypertension: A harbinger of stroke and dementia. Hypertension 2013, 62, 810–817. [Google Scholar] [CrossRef] [Green Version]
- Liu, J.Y.; Xiong, L.; Stinear, C.M.; Leung, H.; Leung, T.W.; Wong, K.S.L. External counterpulsation enhances neuroplasticity to promote stroke recovery. J. Neurol. Neurosurg. Psychiatry 2019, 90, 361–363. [Google Scholar] [CrossRef]
- Kirkman, E.; Sawdon, M. Neurological and humoral control of blood pressure. Anaesth. Intensive Care Med. 2010, 11, 159–164. [Google Scholar] [CrossRef]
- Chen, L.-E.; Liu, K.; Qi, W.-N.; Joneschild, E.; Tan, X.; Seaber, A.V.; Stamler, J.S.; Urbaniak, J.R. Role of nitric oxide in vasodilation in upstream muscle during intermittent pneumatic compression. J. Appl. Physiol. 2002, 92, 559–566. [Google Scholar] [CrossRef] [Green Version]
- Sheldon, R.D.; Roseguini, B.T.; Thyfault, J.P.; Crist, B.D.; Laughlin, M.H.; Newcomer, S.C. Acute impact of intermittent pneumatic leg compression frequency on limb hemodynamics, vascular function, and skeletal muscle gene expression in humans. J. Appl. Physiol. 2012, 112, 2099–2109. [Google Scholar] [CrossRef] [Green Version]
- Peterka, R.J.; Loughlin, P.J. Dynamic regulation of sensorimotor integration in human postural control. J. Neurophysiol. 2004, 91, 410–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, B.; Ming, Z.; Bu, L.; Xu, L.; Wei, W.; Li, Z. Posture-related changes in brain functional connectivity as assessed by wavelet phase coherence of nirs signals in elderly subjects. Behav. Brain Res. 2016, 312, 238–245. [Google Scholar] [CrossRef]
- Su, H.; Huo, C.; Wang, B.; Li, W.; Xu, G.; Liu, Q.; Li, Z. Alterations in the coupling functions between cerebral oxyhaemoglobin and arterial blood pressure signals in post-stroke subjects. PLoS ONE 2018, 13, e0195936. [Google Scholar] [CrossRef] [Green Version]
- Billinger, S.A.; Coughenour, E.; MacKay-Lyons, M.J.; Ivey, F.M. Reduced cardiorespiratory fitness after stroke: Biological consequences and exercise-induced adaptations. Stroke Res. Treat. 2012, 2012, 959120. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Teixeira-Salmela, L.F.; Parreira, V.F.; Britto, R.R.; Brant, T.C.; Inácio, É.P.; Alcântara, T.O.; Carvalho, I.F. Respiratory pressures and thoracoabdominal motion in community-dwelling chronic stroke survivors. Arch. Phys. Med. Rehabil. 2005, 86, 1974–1978. [Google Scholar] [CrossRef]
- Michaels, A.D.; Accad, M.; Ports, T.A.; Grossman, W. Left ventricular systolic unloading and augmentation of intracoronary pressure and doppler flow during enhanced external counterpulsation. Circulation 2002, 106, 1237–1242. [Google Scholar] [CrossRef] [Green Version]
- Liu, R.; Liang, Z.J.; Liao, X.X.; Hu, C.L.; Jiang, L.; Dai, G.; Li, Y.Q.; Wei, H.Y.; Wu, G.F.; Li, X. Enhanced external counterpulsation improves cerebral blood flow following cardiopulmonary resuscitation. Am. J. Emerg. Med. 2013, 31, 1638–1645. [Google Scholar] [CrossRef]
- Lin, W.; Xiong, L.; Han, J.; Leung, H.; Leung, T.; Soo, Y.; Chen, X.; Wong, K.S.L. Increasing pressure of external counterpulsation augments blood pressure but not cerebral blood flow velocity in ischemic stroke. J. Clin. Neurosci. 2014, 21, 1148–1152. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | Group Control | Group Stroke | p for Difference |
|---|---|---|---|
| Age (years old) | 59.8 ± 5.9 | 63.9 ± 12.5 | 0.188 |
| Body Mass Index | 24.8 ± 3.1 | 25.8 ± 3.4 | 0.311 |
| Female Sex (%) | 10% | 13.6% | 0.724 |
| NO. | Gender | Age (years old) | Hemiplegia Side | Post Stroke (month) | Lesion Location | Other Diseases |
|---|---|---|---|---|---|---|
| 1 | M | 72 | L | 3 | R cerebellum | HT, HLP |
| 2 | F | 81 | R | 2.5 | L basal ganglia, frontal lobe | HLP |
| 3 | F | 67 | L | 1 | R basilar artery | HT, HLP |
| 4 | M | 74 | R | 1.5 | L basal ganglia | HT, HLP |
| 5 | M | 77 | R | 3 | L ventricle, thalamus | HT, DM |
| 6 | M | 49 | R | 4 | L basal ganglia | HT, HLP |
| 7 | M | 61 | R | 1.5 | L pons | HT, DM, HLP |
| 8 | M | 74 | R | 3 | L basal ganglia | HT, HLP |
| 9 | M | 61 | R | 2.5 | L pons | HT, DM, HLP |
| 10 | M | 46 | L | 1.5 | R basal ganglia | / |
| 11 | M | 55 | L | 2 | R pons | HT, HLP |
| 12 | M | 61 | R | 1.5 | L thalamus | HT, DM, HLP |
| 13 | M | 74 | R | 4 | L basal ganglia | HT, HLP |
| 14 | M | 46 | L | 2.5 | R basal ganglia | / |
| 15 | M | 82 | L | 6 | R brainstem | DM, HLP |
| 16 | M | 46 | L | 3.5 | R basal ganglia | / |
| 17 | M | 61 | R | 1.5 | L thalamus | HT, DM, HLP |
| 18 | M | 74 | R | 3 | L temporal lobe, parietal lobe | HT, HLP |
| 19 | M | 82 | L | 6 | R brainstem | DM, HLP |
| 20 | F | 48 | R | 1 | L frontal lobe, insular cortex, basal ganglia | HT, DM, HLP |
| 21 | M | 61 | R | 6 | L thalamus | HT, HLP |
| 22 | M | 53 | R | 3 | L basal ganglia, pons, thalamus, temporal lobe | HT |
| Interval I | Interval II | Interval III | ||||
|---|---|---|---|---|---|---|
| Group | p value | Group | p value | Group | p value | |
| ABP→LPFC | Group Stroke | 0.454 | Group Stroke | 0.001 | Group Stroke | 0.033 |
| Group Healthy | 0.705 | Group Healthy | 0.319 | Group Healthy | 0.112 | |
| ABP→RPFC | Group Stroke | 0.114 | Group Stroke | < 0.001 | Group Stroke | 0.097 |
| Group Healthy | 0.653 | Group Healthy | 0.227 | Group Healthy | 0.085 | |
| ABP→LTLC | Group Stroke | 0.009 | Group Stroke | < 0.001 | Group Stroke | < 0.001 |
| Group Healthy | 0.213 | Group Healthy | 0.343 | Group Healthy | 0.022 | |
| ABP→RTLC | Group Stroke | 0.289 | Group Stroke | < 0.001 | Group Stroke | 0.006 |
| Group Healthy | 0.290 | Group Healthy | 0.238 | Group Healthy | 0.039 | |
| ABP→LSMC | Group Stroke | < 0.001 | Group Stroke | < 0.001 | Group Stroke | < 0.001 |
| Group Healthy | 0.803 | Group Healthy | 0.028 | Group Healthy | 0.001 | |
| ABP→RSMC | Group Stroke | < 0.001 | Group Stroke | < 0.001 | Group Stroke | < 0.001 |
| Group Healthy | 0.400 | Group Healthy | 0.019 | Group Healthy | < 0.001 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Li, W.; Xu, G.; Huo, C.; Xie, H.; Lv, Z.; Zhao, H.; Li, Z. Intermittent Sequential Pneumatic Compression Improves Coupling between Cerebral Oxyhaemoglobin and Arterial Blood Pressure in Patients with Cerebral Infarction. Biology 2021, 10, 869. https://doi.org/10.3390/biology10090869
Li W, Xu G, Huo C, Xie H, Lv Z, Zhao H, Li Z. Intermittent Sequential Pneumatic Compression Improves Coupling between Cerebral Oxyhaemoglobin and Arterial Blood Pressure in Patients with Cerebral Infarction. Biology. 2021; 10(9):869. https://doi.org/10.3390/biology10090869
Chicago/Turabian StyleLi, Wenhao, Gongcheng Xu, Congcong Huo, Hui Xie, Zeping Lv, Haihong Zhao, and Zengyong Li. 2021. "Intermittent Sequential Pneumatic Compression Improves Coupling between Cerebral Oxyhaemoglobin and Arterial Blood Pressure in Patients with Cerebral Infarction" Biology 10, no. 9: 869. https://doi.org/10.3390/biology10090869
APA StyleLi, W., Xu, G., Huo, C., Xie, H., Lv, Z., Zhao, H., & Li, Z. (2021). Intermittent Sequential Pneumatic Compression Improves Coupling between Cerebral Oxyhaemoglobin and Arterial Blood Pressure in Patients with Cerebral Infarction. Biology, 10(9), 869. https://doi.org/10.3390/biology10090869