
Survival Rate and Prosthetic and Sinus Complications of Zygomatic Dental Implants for the Rehabilitation of the Atrophic Edentulous Maxilla: A Systematic Review and Meta-Analysis


 and
and
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Focused Question
2.3. Databases and Search Strategy
2.4. Study Selection
2.5. Data Extraction and Study Outcomes
2.6. Methodological Quality Assessment
2.7. Quantitative Synthesis—Meta-Analysis
3. Results
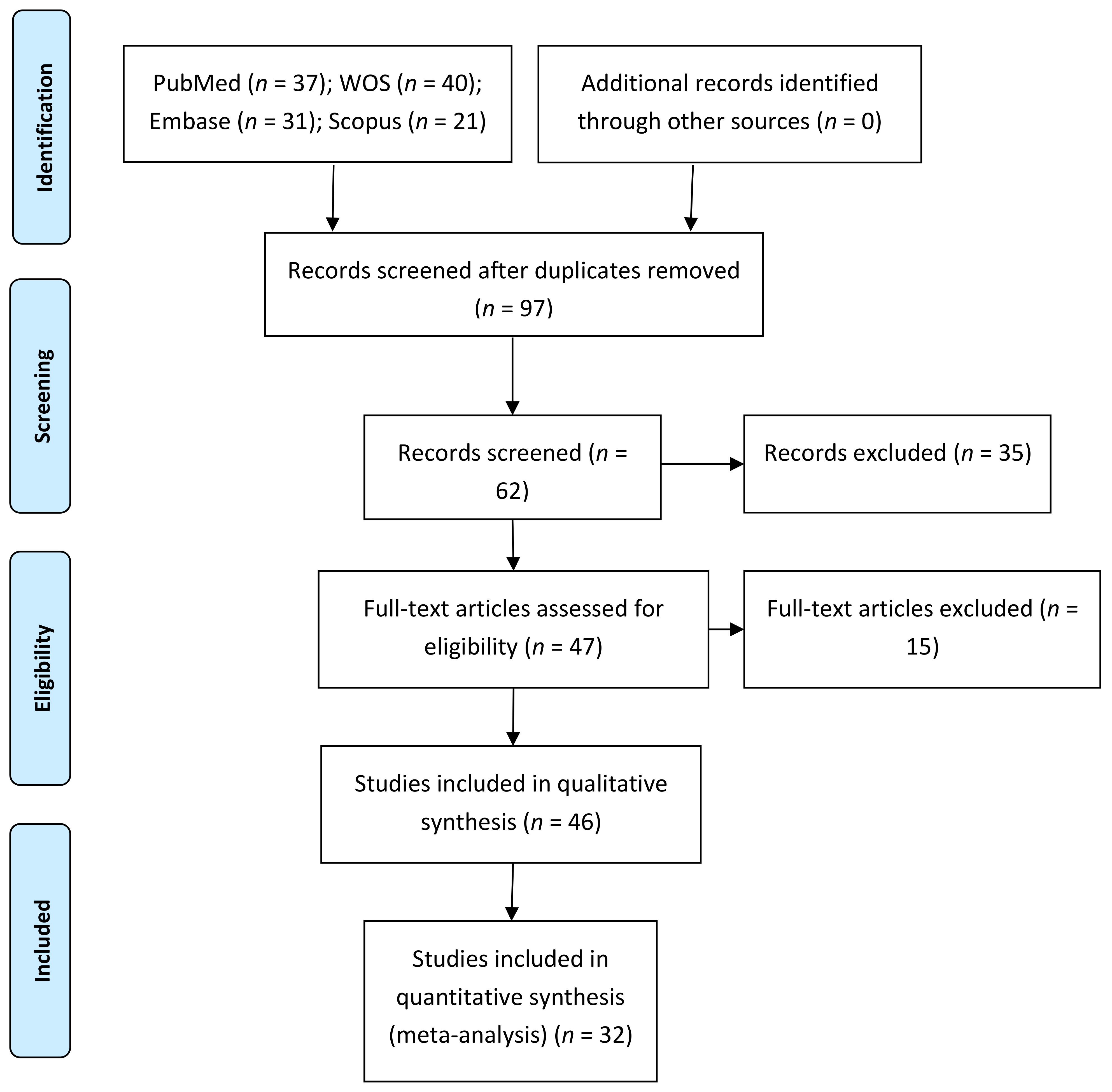
3.1. Flow Diagram
3.2. Qualitative Analysis
3.3. Quality Assessment
3.4. Quantitative Analysis
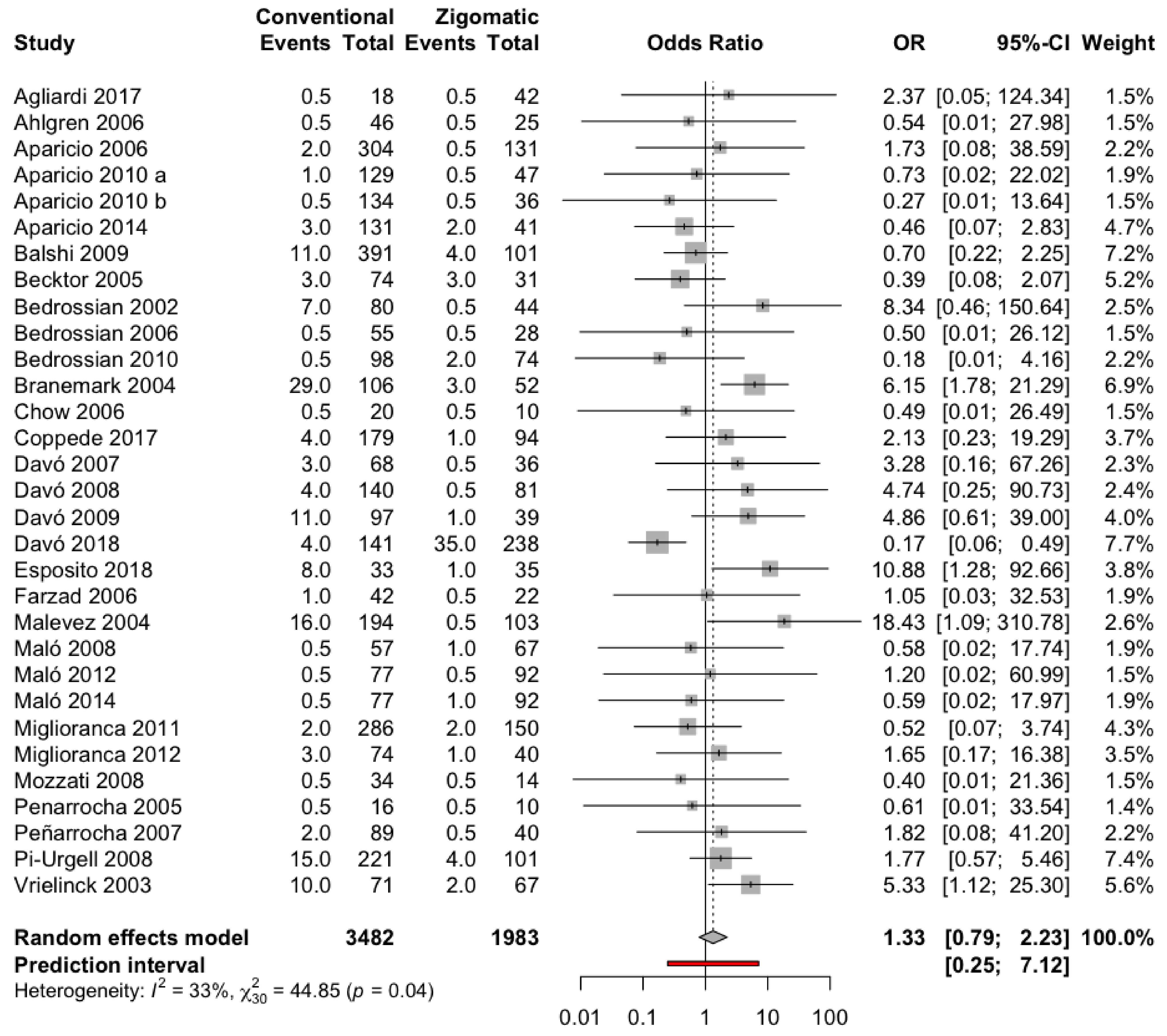
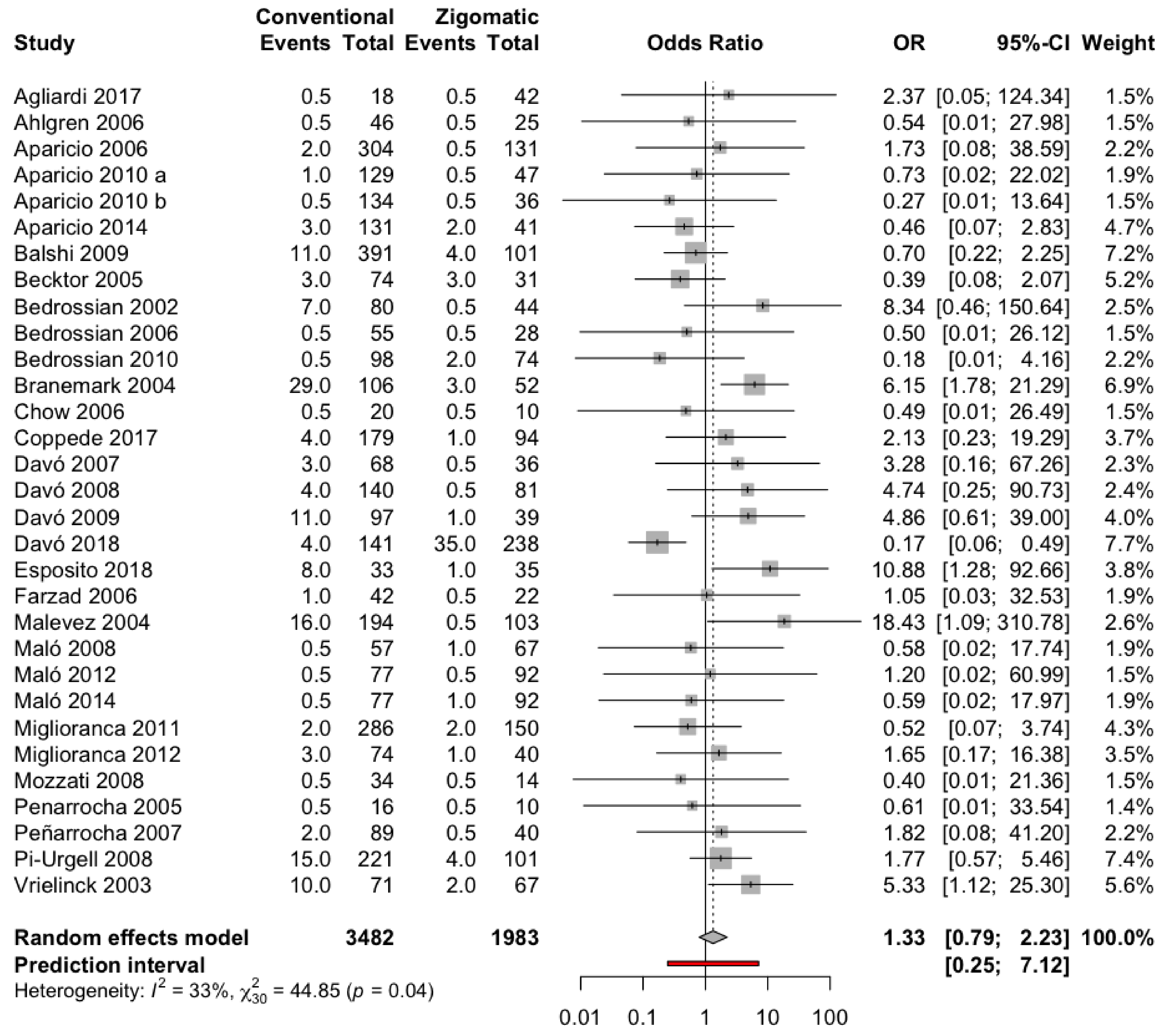
3.4.1. Failure Rate of Zygomatic and Conventional Dental Implants
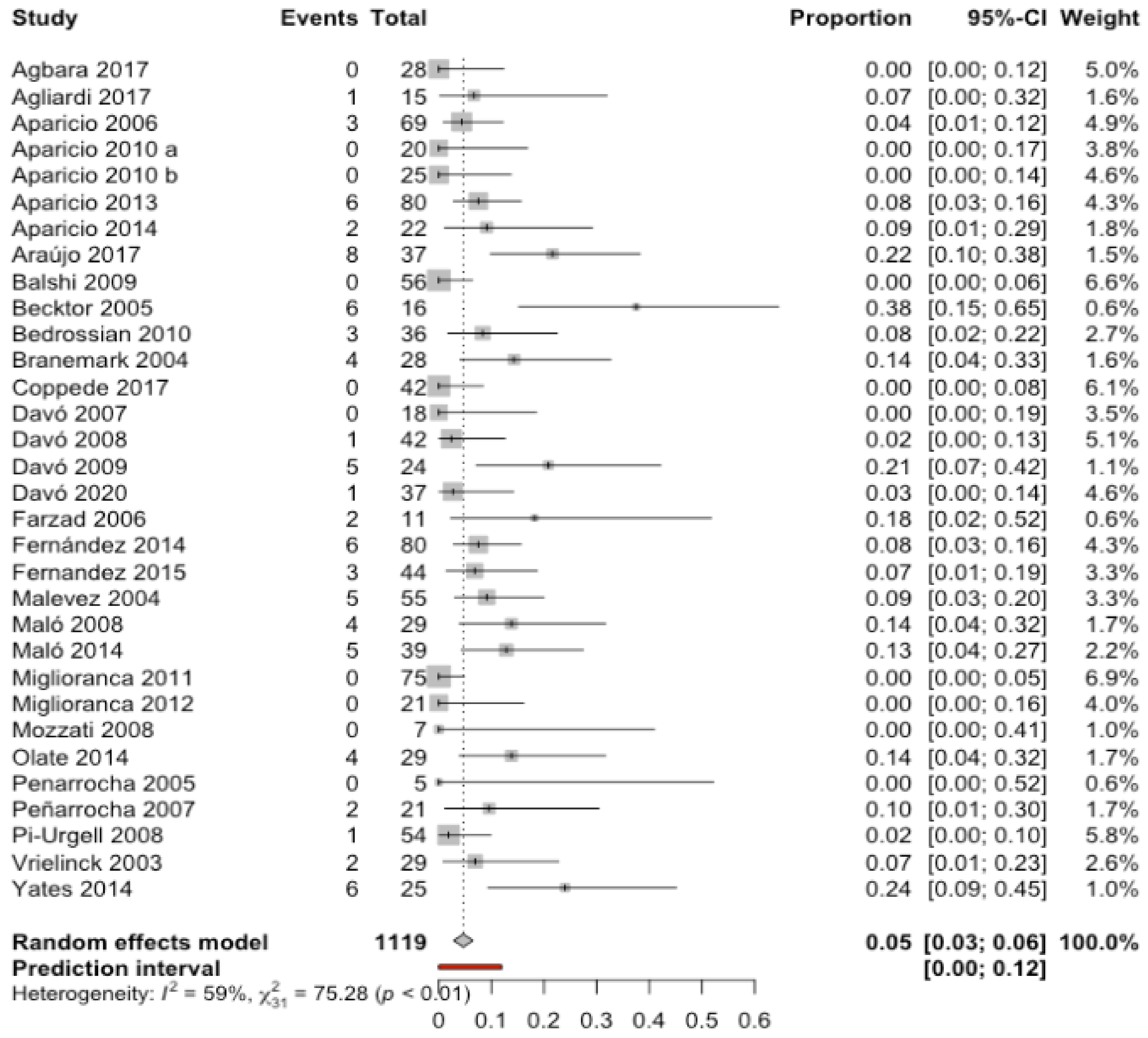
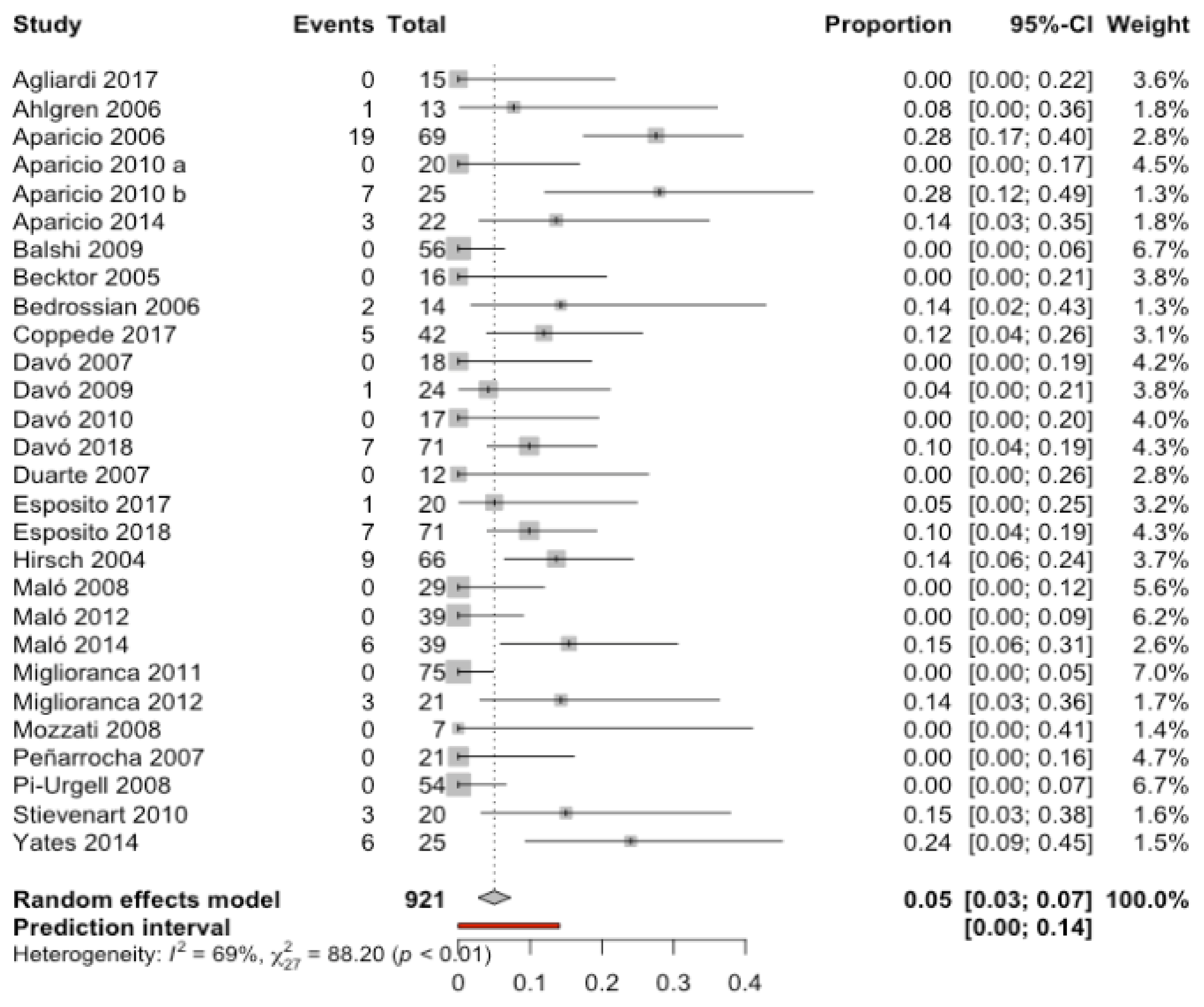
3.4.2. Incidence of Prosthetic Complications in Patients with Zygomatic Implants
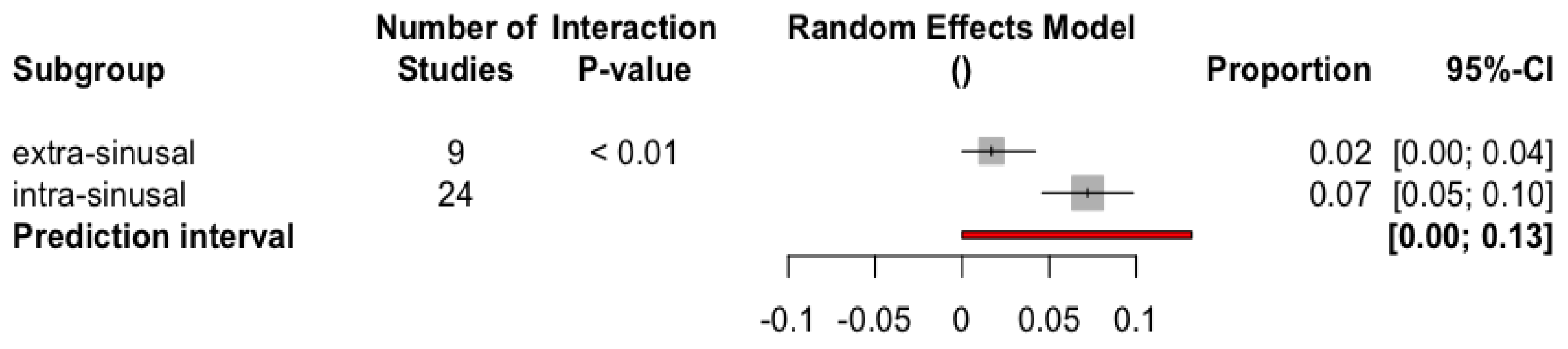
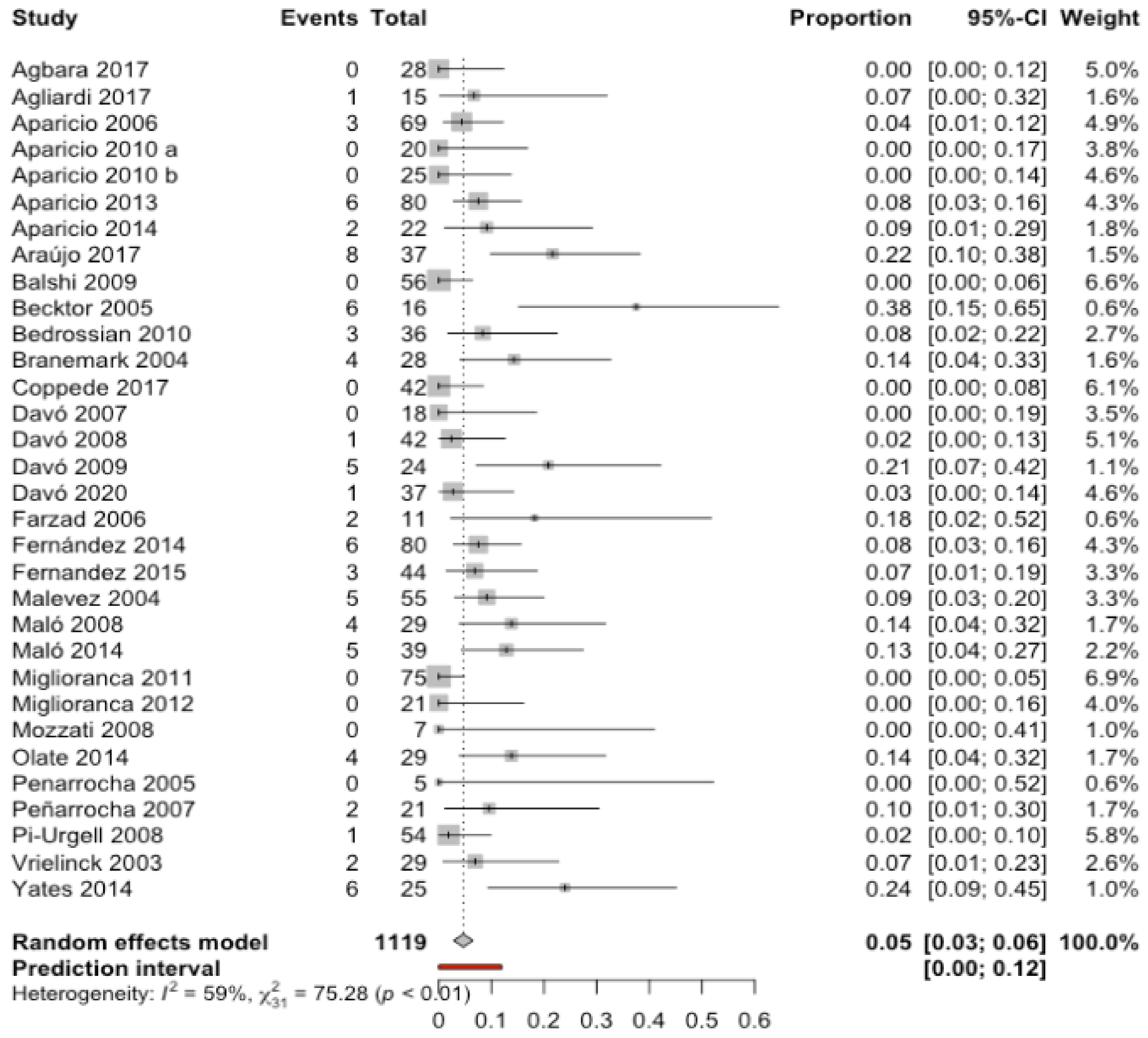
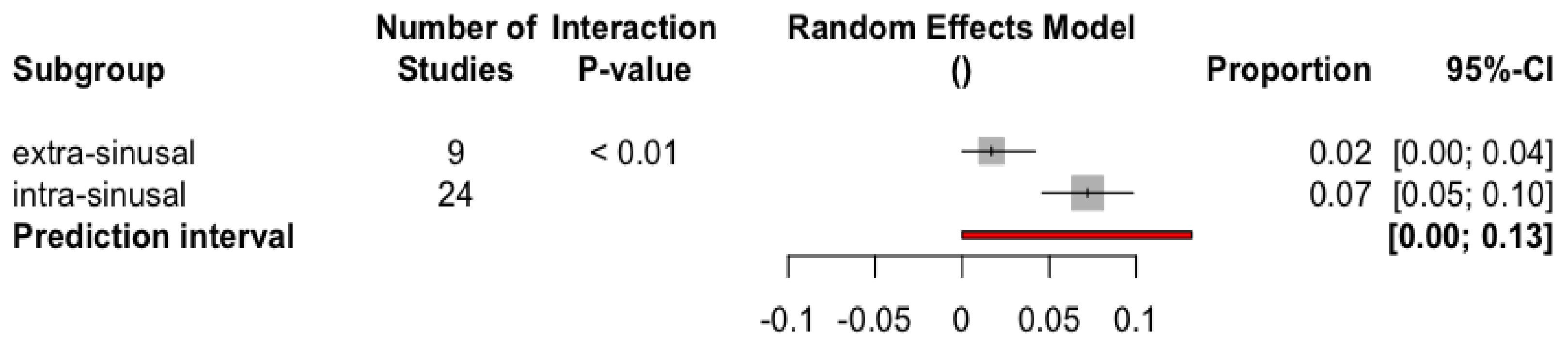
3.4.3. Incidence of Sinusitis in Patients with Zygomatic Implants
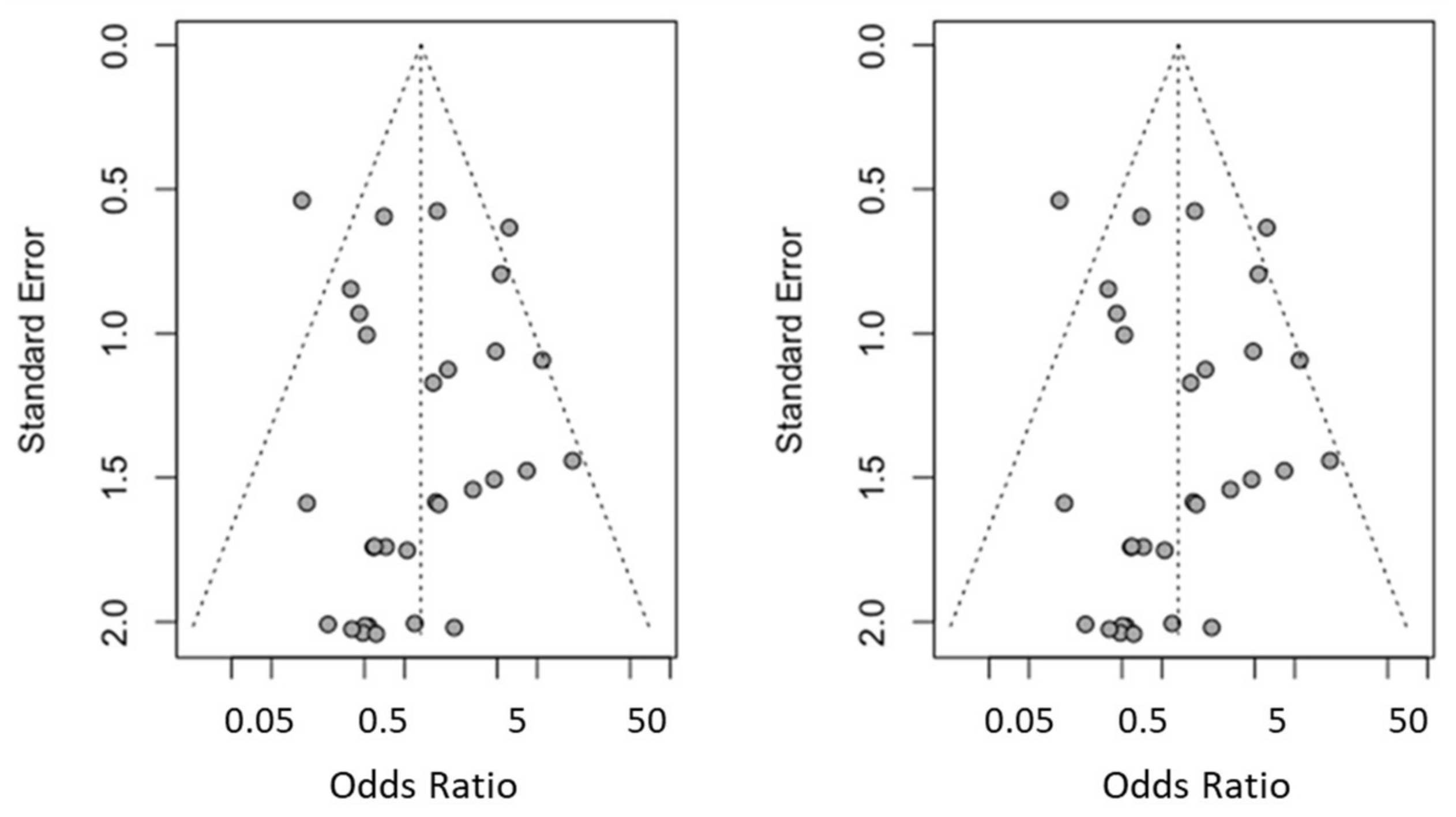
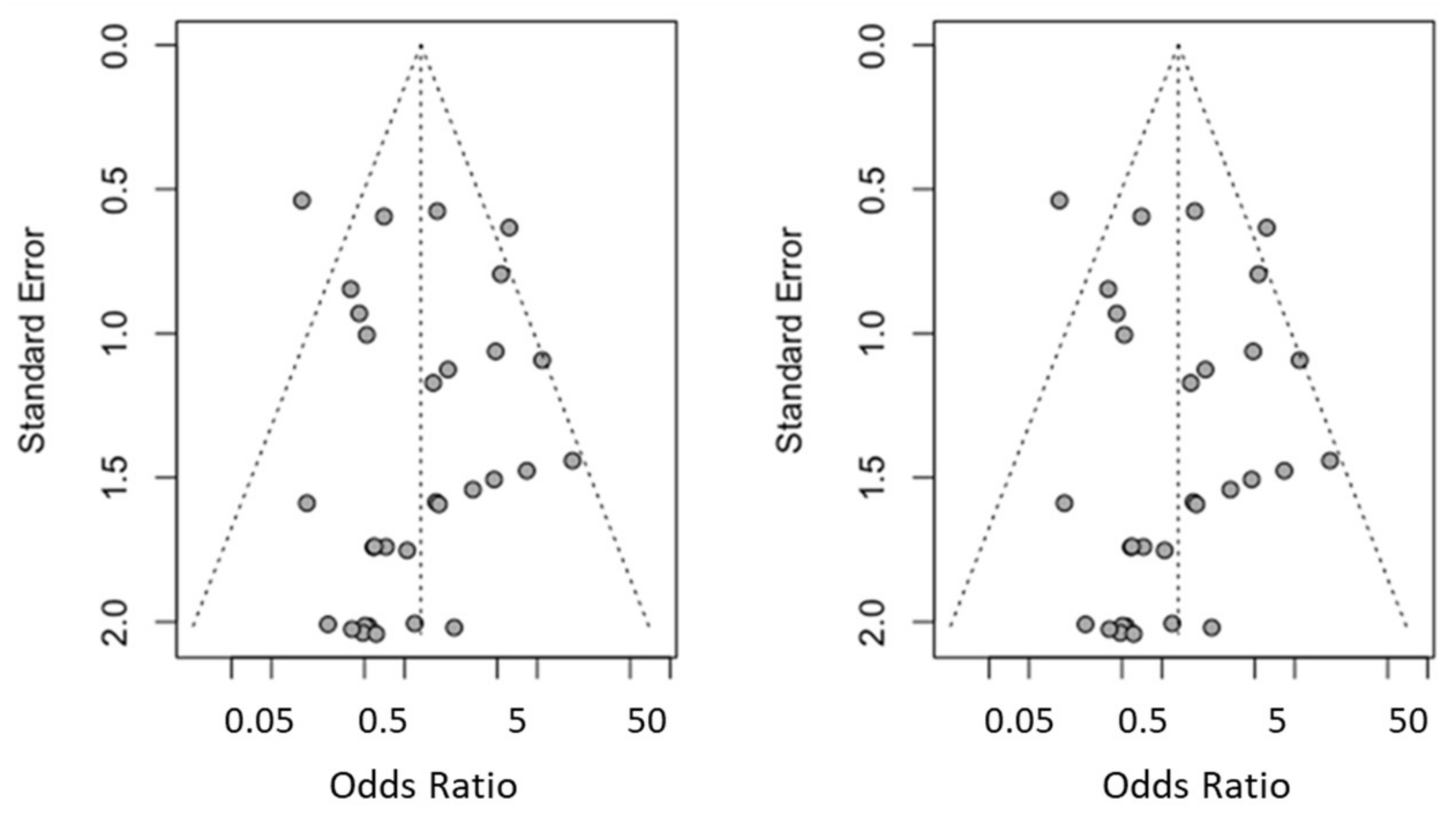
3.5. Publication Bias
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aparicio, C.; Manresa, C.; Francisco, K.; Ouazzani, W.; Claros, P.; Potau, J.M.; Aparicio, A. The long-term use of zygomatic implants: A 10-year clinical and radiographic report. Clin. Implant Dent. Relat. Res. 2014, 16, 447–459. [Google Scholar] [CrossRef] [PubMed]
- Nystrom, L.; Ahlqvist, J.; Legrell, P.E.; Kahnberg, K. Bone graft remodelling and implant success rate in the treatment of the severely resorbed maxilla: A 5-year longitudinal study. Int. J. Oral Maxillofac. Surg. 2002, 31, 158–164. [Google Scholar] [CrossRef]
- Nyström, E.; Nilson, H.; Gunne, J.; Lundgren, S. Reconstruction of the atrophic maxilla with interpositional bone grafting/Le Fort I osteotomy and endosteal implants: A 11–16 year follow-up. Int. J. Oral Maxillofac. Surg. 2009, 38, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Jensen, J.; Sindet-Pedersen, S.; Oliver, A.J. Varying treatment strategies for reconstruction of maxillary atrophy with implants: Results in 98 patients. J. Oral Maxillofac. Surg. 1994, 52, 210–218. [Google Scholar] [CrossRef]
- Kahnberg, K.E.; Nilsson, P.; Rasmusson, L. Le Fort I osteotomy with interpositional bone grafts and implants for rehabilitation of the severely resorbed maxilla: A 2-stage procedure. Int. J. Oral Maxillofac. Implants 1999, 14, 571–578. [Google Scholar]
- Jemt, T.; Lekholm, U. Implant treatment in edentulous maxillae: A 5-year follow-up report on patients with different degrees of jaw resorption. Int. J. Oral Maxillofac. Implants 1995, 10, 303–311. [Google Scholar]
- Becktor, J.P.; Isaksson, S.; Abrahamsson, P.; Sennerby, L. Evaluation of 31 zygomatic implants and 74 regular dental implants used in 16 patients for prosthetic reconstruction of the atrophic maxilla with cross-arch fixed bridges. Clin. Implant Dent. Relat. Res. 2005, 7, 159–165. [Google Scholar] [CrossRef] [Green Version]
- Isola, G.; Polizzi, A.; Alibrandi, A.; Williams, R.C.; Lo Giudice, A. Analysis of galectin-3 levels as a source of coronary heart disease risk during periodontitis. J. Periodontal Res. 2021, 56, 597–605. [Google Scholar] [CrossRef]
- Ghassib, I.; Chen, Z.; Zhu, J.; Wang, H.L. Use of IL-1 β, IL-6, TNF-α, and MMP-8 biomarkers to distinguish peri-implant diseases: A systematic review and meta-analysis. Clin. Implant Dent. Relat. Res. 2019, 21, 190–207. [Google Scholar] [CrossRef]
- Bedrossian, E.; Rangert, B.; Stumpel, L.; Indresano, T. Immediate function with the zygomatic implant: A graftless solution for the patient with mild to advanced atrophy of the maxilla. Int. J. Oral Maxillofac. Implants 2006, 21, 937–942. [Google Scholar]
- Davó, R.; Malevez, C.; Rojas, J.; Rodríguez, J.; Regolf, J. Clinical outcome of 42 patients treated with 81 immediately loaded zygomatic implants: A 12-to-42 month retrospective study. Eur. J. Oral Implantol. 2008, 1, 141–150. [Google Scholar]
- Duarte, L.; Filho, H.; Francischone, C.; Peredo, L.; Branemark, P. The establishment of a protocol for the total rehabilitation of atrophic maxillae employing four zygomatic fixtures in an immediate loading system: A 30-month clinical and radiographic follow-up. Clin. Implant Dent. Relat. Res. 2007, 9, 186–196. [Google Scholar] [CrossRef]
- Maló, P.; de Araujo, M.; Lopes, I. A new approach to rehabilitate the severely atrophic maxilla using extramaxillary anchored implants in immediate function: A pilot study. J. Prosthet. Dent. 2008, 100, 354–366. [Google Scholar] [CrossRef]
- Aparicio, C.; Ouazzani, W.; Hatano, N. The use of zygomatic implants for prosthetic rehabilitation of the severely resorbed maxilla. Periodontology 2000 2008, 47, 162–171. [Google Scholar] [CrossRef]
- Malevez, C.; Abarca, M.; Durdu, F.; Daelemans, P. Clinical outcome of 103 consecutive zygomatic implants: A 6–48 months follow-up study. Clin. Oral Implants Res. 2004, 15, 18–22. [Google Scholar] [CrossRef] [PubMed]
- Davo, R.; Pons, O.; Rojas, J.; Carpio, E. Immediate function of four zygomatic implants: A 1-year report of a prospective study. Eur. J. Oral Implantol. 2010, 3, 323–334. [Google Scholar] [PubMed]
- Liberati, A.; Banzi, R.; Moja, L. Measuring the impact of evidence: The Cochrane systematic review of organized stroke care. Intern. Emerg. Med. 2009, 4, 507–510. [Google Scholar]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Davó, R.; Felice, P.; Pistilli, R.; Barausse, C.; Marti-Pages, C.; Ferrer-Fuertes, A.; Ippolito, D.R.; Esposito, M. Immediately loaded zygomatic implants vs conventional dental implants in augmented atrophic maxillae: 1-year post-loading results from a multicentre randomised controlled trial. Eur. J. Oral Implantol. 2018, 11, 145–161. [Google Scholar]
- Esposito, M.; Barausse, C.; Balercia, A.; Pistilli, R.; Ippolito, D.R.; Felice, P. Conventional drills vs. piezoelectric surgery preparation for placement of four immediately loaded zygomatic oncology implants in edentulous maxillae: Results from 1-year split-mouth randomised controlled trial. Eur. J. Oral Implantol. 2017, 10, 147–158. [Google Scholar]
- Esposito, M.; Davó, R.; Marti-Pages, C.; Ferrer-Fuertes, A.; Barausse, C.; Pistilli, R.; Ippolito, D.R.; Felice, P. Immediately loaded zygomatic implants vs conventional dental implants in augmented atrophic maxillae: 4 months post-loading results from a multicentre randomised controlled trial. Eur. J. Oral Implantol. 2018, 11, 11–28. [Google Scholar]
- Fernández Olarte, H.; Gómez-Delgado, A.; Trujillo-Saldarriaga, S.; Castro-Núñez, J. Inferior Meatal Antrostomy as a Prophylactic Maneuver to Prevent Sinusitis After Zygomatic Implant Placement Using the Intrasinusal Technique. Int. J. Oral Maxillofac. Implants 2015, 30, 862–867. [Google Scholar] [CrossRef] [Green Version]
- Agliardi, E.L.; Romeo, D.; Panigatti, S.; de Araújo Nobre, M.; Maló, P. Immediate full-arch rehabilitation of the severely atrophic maxilla supported by zygomatic implants: A prospective clinical study with minimum follow-up of 6 years. Int. J. Oral Maxillofac. Surg. 2017, 46, 1592–1599. [Google Scholar] [CrossRef]
- Ahlgren, F.; Størksen, K.; Tornes, K. A study of 25 zygomatic dental implants with 11 to 49 months’ follow-up after loading. Int. J. Oral Maxillofac. Implants 2006, 21, 421–425. [Google Scholar]
- Aparicio, C.; Ouazzani, W.; Aparicio, A.; Fortes, V.; Muela, R.; Pascual, A.; Codesal, M.; Barluenga, N.; Manresa, C.; Franch, M. Extrasinus zygomatic implants: Three year experience from a new surgical approach for patients with pronounced buccal concavities in the edentulous maxilla. Clin. Implant Dent. Relat. Res. 2010, 12, 55–61. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, C.; Ouazzani, W.; Garcia, R.; Arevalo, X.; Muela, R.; Fortes, V. A prospective clinical study on titanium implants in the zygomatic arch for prosthetic rehabilitation of the atrophic edentulous maxilla with a follow-up of 6 months to 5 years. Clin. Implant Dent. Relat. Res. 2006, 8, 114–122. [Google Scholar] [CrossRef]
- Aparicio, C.; Manresa, C.; Francisco, K.; Claros, P.; Alández, J.; González-Martín, O.; Albrektsson, T. Zygomatic implants: Indications, techniques and outcomes, and the zygomatic success code. Periodontology 2000 2014, 66, 41–58. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, C.; Ouazzani, W.; Aparicio, A.; Fortes, V.; Muela, R.; Pascual, A.; Codesal, M.; Barluenga, N.; Franch, M. Immediate/Early loading of zygomatic implants: Clinical experiences after 2 to 5 years of follow-up. Clin. Implant Dent. Relat. Res. 2010, 12, e77–e82. [Google Scholar] [CrossRef] [PubMed]
- Bedrossian, E. Rehabilitation of the edentulous maxilla with the zygoma concept: A 7-year prospective study. Int. J. Oral Maxillofac. Implants 2010, 25, 1213–1221. [Google Scholar]
- Bedrossian, E.; Stumpel, L., 3rd; Beckely, M.L.; Indresano, T. The zygomatic implant: Preliminary data on treatment of severely resorbed maxillae. A clinical report. Int. J. Oral Maxillofac. Implants 2002, 17, 861–865, Erratum in 2003, 18, 292. [Google Scholar]
- Brånemark, P.I.; Gröndahl, K.; Öhrnell, L.O.; Nilsson, P.; Petruson, B.; Svensson, B.; Engstrand, P.; Nannmark, U. Zygoma fixture in the management of advanced atrophy of the maxilla: Technique and long-term results. Scand. J. Plast. Reconstr. Surg. Hand Surg. 2004, 38, 70–85. [Google Scholar] [CrossRef]
- Boyes-Varley, J.G.; Howes, D.G.; Lownie, J.F.; Blackbeard, G.A. Surgical modifications to the Brånemark zygomaticus protocol in the treatment of the severely resorbed maxilla: A clinical report. Int. J. Oral Maxillofac. Implants 2003, 18, 232–237. [Google Scholar]
- Hirsch, J.-M.; Öhrnell, L.-O.; Henry, P.J.; Andreasson, L.; Brånemark, P.-I.; Chiapasco, M.; Gynther, G.; Finne, K.; Higuchi, K.W.; Isaksson, S.; et al. A clinical evaluation of the Zygoma fixture: One year of follow-up at 16 clinics. J. Oral Maxillofac. Surg. 2004, 62, 22–29. [Google Scholar] [CrossRef] [PubMed]
- Farzad, P.; Andersson, L.; Gunnarsson, S.; Johansson, B. Rehabilitation of severely resorbed maxillae with zygomatic implants: An evaluation of implant stability, tissue conditions, and patients’ opinion before and after treatment. Int. J. Oral Maxillofac. Implants 2006, 21, 399–404. [Google Scholar]
- Vrielinck, L.; Politis, C.; Schepers, S.; Pauwels, M.; Naert, I. Image-based planning and clinical validation of zygoma and pterygoid implant placement in patients with severe bone atrophy using customized drill guides. Preliminary results from a prospective clinical follow-up study. Int. J. Oral Maxillofac. Surg. 2003, 32, 7–14. [Google Scholar] [CrossRef]
- Migliorança, R.M.; Sotto-Maior, B.S.; Senna, P.M.; Francischone, C.E.; Del Bel Cury, A.A. Immediate occlusal loading of extrasinus zygomatic implants: A prospective cohort study with a follow-up period of 8 years. Int. J. Oral Maxillofac. Surg. 2012, 41, 1072–1076. [Google Scholar] [CrossRef]
- Aparicio, C.; Manresa, C.; Francisco, K.; Aparicio, A.; Nunes, J.; Claros, P.; Potau, J.M. Zygomatic implants placed using the zygomatic anatomy-guided approach versus the classical technique: A proposed system to report rhinosinusitis diagnosis. Clin. Implant Dent. Relat. Res. 2014, 16, 627–642. [Google Scholar] [CrossRef] [PubMed]
- Coppedê, A.; de Mayo, T.; de Sá Zamperlini, M.; Amorin, R.; de Pádua, A.P.A.T.; Shibli, J.A. Three-year clinical prospective follow-up of extrasinus zygomatic implants for the rehabilitation of the atrophic maxilla. Clin. Implant Dent. Relat. Res. 2017, 19, 926–934. [Google Scholar] [CrossRef]
- Agbara, R.; Goetze, E.; Koch, F.; Wagner, W. Zygoma implants in oral rehabilitation: A review of 28 cases. Dent. Res. J. 2017, 14, 370–375. [Google Scholar] [CrossRef] [PubMed]
- Balshi, S.F.; Wolfinger, G.J.; Balshi, T.J. A retrospective analysis of 110 zygomatic implants in a single-stage immediate loading protocol. Int. J. Oral Maxillofac. Implants 2009, 24, 335–341. [Google Scholar]
- Davó, R.; Bankauskas, S.; Laurincikas, R.; Koçyigit, I.D.; de Val, J.E.M.S. Clinical Performance of Zygomatic Implants—Retrospective Multicenter Study. J. Clin. Med. 2020, 9, 480. [Google Scholar] [CrossRef] [Green Version]
- Davo, R.; Malevez, C.; Rojas, J. Immediate function in the atrophic maxilla using zygoma implants: A preliminary study. J. Prosthet. Dent. 2007, 97, S44–S51. [Google Scholar] [CrossRef]
- Davó, R. Zygomatic implants placed with a two-stage procedure: A 5-year retrospective study. Eur. J. Oral Implantol. 2009, 2, 115–124. [Google Scholar] [PubMed]
- Pi Urgell, J.; Revilla Gutiérrez, V.; Gay Escoda, C.G. Rehabilitation of atrophic maxilla: A review of 101 zygomatic implants. Med. Oral Patol. Oral Cir. Bucal 2008, 13, E363–E370. [Google Scholar] [PubMed]
- Maló, P.; Nobre Mde, A.; Lopes, A.; Ferro, A.; Moss, S. Five-year outcome of a retrospective cohort study on the rehabilitation of completely edentulous atrophic maxillae with immediately loaded zygomatic implants placed extra-maxillary. Eur. J. Oral Implantol. 2014, 7, 267–281. [Google Scholar]
- Maló, P.; Nobre, M.D.; Lopes, A.; Francischone, C.; Rigolizzo, M. Three-year outcome of a retrospective cohort study on the rehabilitation of completely edentulous atrophic maxillae with immediately loaded extra-maxillary zygomatic implants. Eur. J. Oral Implantol. 2012, 5, 37–46. [Google Scholar] [PubMed]
- Rodríguez-Chessa, J.G.; Olate, S.; Netto, H.D.; Shibli, J.; de Moraes, M.; Mazzonetto, R. Treatment of atrophic maxilla with zygomatic implants in 29 consecutives patients. Int. J. Clin. Exp. Med. 2014, 7, 426–430. [Google Scholar] [PubMed]
- Migliorança, R.M.; Coppedê, A.; Dias Rezende, R.C.; de Mayo, T. Restoration of the edentulous maxilla using extrasinus zygomatic implants combined with anterior conventional implants: A retrospective study. Int. J. Oral Maxillofac. Implants 2011, 26, 665–672. [Google Scholar]
- Fernández, H.; Gómez-Delgado, A.; Trujillo-Saldarriaga, S.; Varón-Cardona, D.; Castro-Núñez, J. Zygomatic implants for the management of the severely atrophied maxilla: A retrospective analysis of 244 implants. J. Oral Maxillofac. Surg. 2014, 72, 887–891. [Google Scholar] [CrossRef]
- Peñarrocha, M.; García, B.; Martí, E.; Boronat, A. Rehabilitation of severely atrophic maxillae with fixed implant-supported prostheses using zygomatic implants placed using the sinus slot technique: Clinical report on a series of 21 patients. Int. J. Oral Maxillofac. Implants 2007, 22, 645–650. [Google Scholar]
- Stiévenart, M.; Malevez, C. Rehabilitation of totally atrophied maxilla by means of four zygomatic implants and fixed prosthesis: A 6-40-month follow-up. Int. J. Oral Maxillofac. Surg. 2010, 39, 358–363. [Google Scholar] [CrossRef]
- Yates, J.; Brook, I.; Patel, R.; Wragg, P.; Atkins, S.; El-Awa, A.; Bakri, I.; Bolt, R. Treatment of the edentulous atrophic maxilla using zygomatic implants: Evaluation of survival rates over 5–10 years. Int. J. Oral Maxillofac. Surg. 2014, 43, 237–242. [Google Scholar] [CrossRef] [PubMed]
- Peñarrocha-Diago, M.; Bernabeu-Mira, J.C.; Fernández-Ruíz, A.; Aparicio, C.; Peñarrocha-Oltra, D. Bone Regeneration and Soft Tissue Enhancement Around Zygomatic Implants: Retrospective Case Series. Materials 2020, 13, 1577. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Araújo, R.T.; Sverzut, A.T.; Trivellato, A.E.; Sverzut, C.E. Retrospective Analysis of 129 Consecutive Zygomatic Implants Used to Rehabilitate Severely Resorbed Maxillae in a Two-Stage Protocol. Int. J. Oral Maxillofac. Implants 2017, 32, 377–384. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chow, J.; Hui, E.; Lee, P.K.; Li, W. Zygomatic implants—Protocol for immediate occlusal loading: A preliminary report. J. Oral Maxillofac. Surg. 2006, 64, 804–811. [Google Scholar] [CrossRef]
- Mozzati, M.; Monfrin, S.B.; Pedretti, G.; Schierano, G.; Bassi, F. Immediate loading of maxillary fixed prostheses retained by zygomatic and conventional implants: 24-month preliminary data for a series of clinical case reports. Int. J. Oral Maxillofac. Implants 2008, 23, 308–314. [Google Scholar]
- Peñarrocha, M.; Uribe, R.; García, B.; Martí, E. Zygomatic implants using the sinus slot technique: Clinical report of a patient series. Int. J. Oral Maxillofac. Implants 2005, 20, 788–792. [Google Scholar]
- Kaewsiri, D.; Panmekiate, S.; Subbalekha, K.; Mattheos, N.; Pimkhaokham, A. The accuracy of static vs. dynamic computer-assited implant surgery in single tooth space: A randomized controlled trial. Clin. Oral Implants Res. 2019, 30, 505–514. [Google Scholar]
- Herklotz, I.; Beuer, F.; Kunz, A.; Hildebrand, D.; Happe, A. Navigation in implantology. Int. J. Comput. Dent. 2017, 20, 9–19. [Google Scholar]
- Widmann, G.; Bale, R.J. Accuracy in Computer-Aided Implant Surgery—A review. Int. J. Oral Maxillofac. Implants 2006, 21, 305–313. [Google Scholar]
- Lal, K.; White, G.S.; Morea, D.N.; Wright, R.F. Use of stereolithographic templates for surgical and prosthodontic implant planning and placement. Part II. A clinical report. J. Prosthodont. 2006, 15, 117–122. [Google Scholar] [CrossRef] [PubMed]
- Jorba-García, A.; Figueiredo, R.; González-Barnadas, A.; Camps-Font, O.; Valmaseda-Castellón, E. Accuracy and the role of experience in dynamic computer guided dental implant surgery: An in-vitro study. Med. Oral Patol. Oral Cir. Bucal 2019, 24, 76–83. [Google Scholar] [CrossRef]
- Tahmaseb, A.; Wu, V.; Wismeijer, D.; Coucke, W.; Evans, C. The accuracy of static computer-aided implant surgery: A systematic review and meta-analysis. Clin. Oral Implants Res. 2018, 16, 416–435. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Stefanelli, L.V.; DeGroot, B.S.; Lipton, D.I.; Mandelaris, G.A. Accuracy of a Dynamic Dental Implant Navigation System in a Private Practice. Int. J. Oral Maxillofac. Implants 2019, 34, 205–213. [Google Scholar] [CrossRef]
- Hoffmann, J.; Westendorff, C.; Gomez-Roman, G.; Reinert, S. Accuracy of navigation-guided socket drilling before implant installation compared to the conventional free-hand method in a synthetic edentulous lower jaw model. Clin. Oral Implants Res. 2005, 16, 609–614. [Google Scholar] [CrossRef]
- Chen, C.K.; Yuh, D.Y.; Huang, R.Y.; Fu, E.; Tsai, C.F.; Chiang, C.Y. Accuracy of implant placement with a navigation system, a laboratory guide, and freehand drilling. Int. J. Oral Maxillofac. Implants 2018, 33, 1213–1218. [Google Scholar] [CrossRef]
- Gargallo-Albiol, J.; Barootchi, S.; Salomó-Coll, O.; Wang, H. Advantages and disadvantages of implant navigation surgery. A systematic review. Ann. Anat. 2019, 225, 1–10. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author/Year | Study Type | Sample (n) | Follow-up Time (Months) | Implant Failure | Prosthetic Complications | Sinusitis |
|---|---|---|---|---|---|---|
| Agbara et al., 2017 [37] | Retrospective study | 42 ZI 123 CI | 51.7 (5–163) | 5/42 ZI (peri-implantitis (n = 4) and accidental intrasinusal placement (n = 1)) | N/A/28 patients | 0/28 patients |
| N/A/123 CI | ||||||
| Agliardi et al., 2017 [21] | NRCT | 42 ZI 18 CI | 85.04 (73–91) | 0/42 ZI 0/18 CI | 0/15 patients | 1/15 patients: intrasinusal placement of the zygomatic dental implants (sinus membrane perforation close to the bone crest, treated with antiseptics (chlorhexidine 0.2%), antibiotics (amoxicillin and clavulanic acid, 1000 mg) and corticosteroids) |
| Ahlgren et al., 2006 [22] | NRCT | 25 ZI 46 CI | 11–49 | 0/25 ZI 0/46 CI | 1/13 patients (allergy to the gold alloy of the overdenture bar) | N/A/13 patients |
| Aparicio et al., 2006 [24] | NRCT | 131 ZI 304 CI | 25.1 (6–60) | 0/131 ZI | 19/69 patients (loosening of the zygomatic implant gold screws (n = 9). Fracture of one gold screw (n = 2). Fracture of the metal resin prosthesis (n = 8)) | 3/69 patients: intrasinusal placement of the zygomatic dental implants (after 14, 23, and 27 months postsurgery and treated by antibiotics) |
| 2/304 CI (pterygoid implant failed 1 month after abutment connection (n = 1) and an anterior implant failed after 27 months in function (n = 1)) | ||||||
| Aparicio et al., 2010a [26] | NRCT | 47 ZI 129 CI | 24–60 | 0/47 ZI | 7/25 patients (fracture of the teeth of metal–resin (n = 4) and metal–porcelain prostheses (n = 1) and a fracture of an abutment screw (n = 1)) | 0/25 patients: intrasinusal (n = 7) and extrasinusal (n = 18) placement of the zygomatic dental implants |
| 1/129 CI (pterygoid implant failed 52 months of loading (n = 1)) | ||||||
| Aparicio et al., 2010b [23] | NRCT | 36 ZI 104 CI | 36–48 | 0/36 ZI 0/104 CI | 0/20 patients | 0/20 patients: extrasinusal placement of the zygomatic dental implants |
| Aparicio et al., 2013 [35] | NRCT | 41 classic procedure ZI 156 ZAGA | 135,24 classic procedure ZI 55.44 ZAGA | 3/41 classic procedure ZI 0/156 ZAGA | 2/197 | 1/22 patients: intrasinusal technique 1/80 ZAGA technique |
| Aparicio et al., 2014 [1] | NRCT | 41 ZI 131 CI | 120 | 2/41 ZI (extreme peri-implant infection with complete dissolution of the palatal bone) | 23/22 patients (fracture of the framework (n = 1), loosening of gold ZI screws (n = 4), fracture of gold screws (n = 4), loosening of the abutment screw (n = 3), fracture of ceramic prosthetic teeth (n = 5), fracture of resin prostheses (n = 2), disconnected abutments (n = 4)) | 5/22 patients: intrasinusal placement of the zygomatic dental implants.Sinusitis was treated with antibiotics |
| 3/131 CI (anterior implant failure 1 month after abutment connection (n = 1) and 3 years of function placed in the subnasal area (n = 1), and in the pterygoid area previous to prosthesis installation (n = 1)) | ||||||
| Araújo et al., 2014 [52] | Retrospective study | 129 ZI | 12 | 2/129 (failures occurred 5–7 months postoperatively) | N/A/37 patients | 8/37 patients: sinus slot technique of the zygomatic dental implants |
| Balshi et al., 2009 [38] | Retrospective study | 101 ZI 391 CI | 9–60 | 4/101 ZI 11/391 CI | 0/56 patients | N/A/56 patients |
| Becktor et al., 2005 [7] | Retrospective study | 31 ZI 74 CI | 46.4 (9–69) | 3/31 ZI 3/74 CI | 0/16 patients | 6/16 patients: intrasinusal placement of the zygomatic dental implants |
| Bedrossian et al., 2002 [28] | NRCT | 44 ZI 80 CI | 34 | 0/44 ZI 7/80 CI | N/A/22 patients | N/A/22 patients |
| Bedrossian et al., 2006 [8] | Retrospective study | 28 ZI 55 CI | 12 | 0/28 ZI 0/55 CI | 2/14 patients (partial fractures in the denture around the zygomatic implant cylinder) | N/A/14 patients |
| Bedrossian et al., 2010 [27] | NRCT | 74 ZI 98 CI | 84 | 2/74 ZI 0/98 CI | N/A/36 patients | 3/36 patients: intrasinusal placement of the zygomatic dental implants |
| Boyes-Varley et al., 2003 [30] | NRCT | 77 ZI | 30 | 0/77 ZI | N/A/45 patients | N/A/45 patients |
| Branemark et al., 2004 [29] | NRCT | 52 ZI 106 CI | 60–120 | 3/52 ZI 29/106 CI | N/A/28 patients | 4/28 patients: intrasinusal placement of the zygomatic dental implants |
| Chow et al., 2006 [53] | Case series | 10 ZI 20 CI | 6–10 | 0/10 ZI 0/20 CI | N/A/5 patients | N/A/5 patients |
| Coppede et al., 2017 [36] | NRCT | 94 ZI 179 CI | 36 | 1/94 ZI 4/179 CI | 5/42 patients (five fractures or detachments of one or more acrylic teeth) | 0/42 patients: extrasinusal placement of the zygomatic dental implants |
| Davó et al., 2007 [41] | Retrospective study | 36 ZI 68 CI | 6–29 | 0/36 ZI 3/68 CI | 0/18 patients | 0/18 patients: intrasinusal placement of the zygomatic dental implants |
| Davó et al., 2008 [9] | Retrospective study | 81 ZI 140 CI | 12–24 | 0/81 ZI 4/140 CI | N/A/42 patients | 1/42 patients: sinus slot technique (n = 15 ZI) and intrasinusal placement of the zygomatic dental implants (n = 66 ZI) |
| Davó, 2009 [42] | Retrospective study | 39 ZI 97 CI | 60 | 1/39 ZI 11/97 CI | 1/24 patients | 5/24 patients C |
| Davó et al., 2010 [14] | NRCT | 68 ZI | 12 | 0/68 ZI | 0/17 patients | N/A/17 patients |
| Davó et al., 2018 [17] | RCT | 238 ZI 141 CI | 6 | 35/238 ZI 4/141 CI | 7/71 patients | N/A/71 patients |
| Davó et al., 2020 [39] | Retrospective study | 182 ZI | 10.5 | 0/182 ZI | N/A/37 patients | 1/37 patients: intrasinusal (6%) and extrasinusal placement of the zygomatic dental implants (94%) |
| Duarte et al.,2007 [10] | NRCT | 48 ZI | 6–30 | 2/48 ZI | 0/12 patients | N/A/12 patients |
| Esposito et al., 2017 [18] | RCT | 80 ZI | 12 | 2/80 ZI | 1/20 patients (fracture of provisional prosthesis) | N/A/20 patients |
| Esposito et al., 2018 [19] | RCT | 35 ZI 33 CIAug | 4 | 1/35 ZI 8/33 CIAug | 7/71 patients | N/A/71 patients |
| Farzad et al., 2006 [32] | NRCT | 22 ZI 42 CI | 18–46 | 0/22 ZI 1/42 CI | N/A/11 patients | 2/11 patients: intrasinusal placement of the zygomatic dental implants |
| Fernández et al., 2014 [47] | Retrospective study | 244 ZI | 6–48 | 1/244 ZI | N/A/80 patients | 6/80 patients: intrasinusal placement of the zygomatic dental implants |
| Fernández et al., 2015 [20] | RCT | 41 ZI | 3 | 1/19 ZI without inferior meatal antrostomy 0/22 ZI with inferior meatal antrostomy | N/A/44 patients | 3/44 patients: intrasinusal placement of the zygomatic dental implants without inferior meatal antrostomy |
| Hirsch et al., 2004 [31] | NRCT | 124 ZI | 12 | 3/124 ZI | 9/66 patients | N/A/66 patients |
| Malevez et al., 2004 [13] | Retrospective study | 103 ZI 194 CI | 6–48 | 0/103 ZI 16/194 CI | N/A/55 patients | 5/55 patients: intrasinusal placement of the zygomatic dental implants |
| Maló et al., 2008 [11] | NRCT | 67 ZI 57 CI | 13(6–18) | 1/67 ZI 0/57 CI | 0/29 patients | 4/29 patients: extrasinusal placement of the zygomatic dental implants |
| Maló et al., 2012 [44] | Retrospective study | 92 ZI 77 CI | 36 | 0/92 ZI 0/77 CI | 0/39 patients | 5/39 patients: extrasinusal placement of the zygomatic dental implants |
| Maló et al., 2014 [43] | Retrospective study | 92 ZI 77 CI | 60 | 1/92 ZI 0/77 CI | 6/39 patients | 5/39 patients: extrasinusal placement of the zygomatic dental implants |
| Miglioranca et al., 2011 [46] | Retrospective study | 150 ZI 286 CI | 12 | 2/150 ZI 2/286 CI | 0/75 patients | 0/75 patients: extrasinusal placement of the zygomatic dental implants |
| Miglioranca et al., 2012 [34] | NRCT | 40 ZI 74 CI | 96 | 1/40 ZI 3/74 CI | 3/21 patients (the metal bar was broken in patient 8; 2 patients reported difficulty in cleaning around the abutment connected to the zygomatic implant) | 0/21 patients: extrasinusal placement of the zygomatic dental implants |
| Mozzati et al., 2008 [54] | Case series | 14 ZI 34 CI | 24 | 0/14 ZI 0/34 CI | 0/7 patients | 0/7 patients: intrasinusal placement of the zygomatic dental implants |
| Rodríguez-Chessa, 2014 [45] | Retrospective study | 67 ZI 84 CI | 20 | 14/67 ZI N/A/84 CI | N/A/29 patients | 4/29 patients: sinus slot technique of the zygomatic dental implants |
| Peñarrocha et al., 2005 [55] | Case series | 10 ZI 16 CI | 12–18 | 0/10 ZI 0/16 CI | N/A/5 patients | 0/5 patients: sinus slot technique of the zygomatic dental implants |
| Peñarrocha et al., 2007 [48] | Retrospective study | 40 ZI 89 CI | 29 (12–45) | 0/40 ZI 2/89 CI | 0/21 patients | 2/21 patients: sinus slot technique of the zygomatic dental implants |
| Peñarrocha-Diago et al., 2020 [51] | Retrospective study | 31 ZI | 12 | 0/31 ZI | N/A/19 patients | N/A/19 patients |
| Pi-Urgell et al., 2008 [42] | Retrospective study | 101 ZI 221 CI | 1–72 | 4/101 ZI 15/221 CI | 0/54 patients | 1/54 patients: intrasinusal placement of the zygomatic dental implants |
| Stievenart et al., 2010 [49] | Retrospective study | 80 ZI | 6–40 | 3/80 ZI | 3/20 patients | N/A/20 patients |
| Vrielinck et al., 2003 [33] | NRCT | 67 ZI 71 CI | 24 | 2/67 ZI 10/71 CI | N/A/29 patients | 2/29 patients: intrasinusal placement of the zygomatic dental implants |
| Yates et al., 2014 [50] | Retrospective study | 43 ZI | 60–120 | 6/43 ZI | 6/25 patients | 6/25 patients: sinus slot technique of the zygomatic dental implants |
| Jadad Criteria | ||||||
|---|---|---|---|---|---|---|
| Author/Year | Is the Study Described as Randomized? | Is the Study Described as Double-Blinded? | Was There a Description of Withdrawals and Dropouts? | Was the Method of Randomization Adequate? | Was the Method of Blinding Appropriate? | Score |
| Agbara et al., 2017 [37] | N/A | N/A | N/A | N/A | N/A | N/A |
| Agliardi et al., 2017 [21] | 0 | 0 | 0 | 0 | 0 | 0 |
| Ahlgren et al., 2006 [22] | 0 | 0 | 0 | 0 | 0 | 0 |
| Aparicio et al., 2006 [24] | 0 | 0 | 0 | 0 | 0 | 0 |
| Aparicio et al., 2010a [26] | 0 | 0 | 0 | 0 | 0 | 0 |
| Aparicio et al., 2010b [23] | 0 | 0 | 0 | 0 | 0 | 0 |
| Aparicio et al., 2013 [35] | 0 | 0 | 0 | 0 | 0 | 0 |
| Aparicio et al., 2014 [1] | 0 | 0 | 0 | 0 | 0 | 0 |
| Araújo et al., 2017 [52] | N/A | N/A | N/A | N/A | N/A | N/A |
| Balshi et al., 2009 [38] | N/A | N/A | N/A | N/A | N/A | N/A |
| Becktor et al., 2005 [7] | N/A | N/A | N/A | N/A | N/A | N/A |
| Bedrossian et al., 2002 [28] | 0 | 0 | 0 | 0 | 0 | 0 |
| Bedrossian et al., 2006 [8] | N/A | N/A | N/A | N/A | N/A | N/A |
| Bedrossian et al., 2010 [27] | 0 | 0 | 0 | 0 | 0 | 0 |
| Boyes-Varley et al., 2003 [30] | 0 | 0 | 0 | 0 | 0 | 0 |
| Branemark et al., 2004 [29] | 0 | 0 | 0 | 0 | 0 | 0 |
| Chow et al., 2006 [53] | N/A | N/A | N/A | N/A | N/A | N/A |
| Coppede et al., 2017 [36] | 0 | 0 | 0 | 0 | 0 | 0 |
| Davó et al., 2007 [41] | N/A | N/A | N/A | N/A | N/A | N/A |
| Davó et al., 2008 [9] | N/A | N/A | N/A | N/A | N/A | N/A |
| Davó, 2009 [42] | N/A | N/A | N/A | N/A | N/A | N/A |
| Davó et al., 2010 [14] | 0 | 0 | 1 | 0 | 0 | 1 |
| Davó et al., 2018 [17] | 1 | 1 | 1 | 1 | 1 | 5 |
| Davó et al., 2020 [39] | N/A | N/A | N/A | N/A | N/A | N/A |
| Duarte et al.,2007 [10] | 0 | 0 | 0 | 0 | 0 | 0 |
| Esposito et al., 2017 [18] | 1 | 0 | 1 | 1 | 0 | 3 |
| Esposito et al., 2018 [19] | 1 | 0 | 1 | 1 | 0 | 3 |
| Farzad et al., 2006 [32] | 0 | 0 | 0 | 0 | 0 | 0 |
| Fernández et al., 2014 [47] | N/A | N/A | N/A | N/A | N/A | N/A |
| Fernández et al., 2015 [20] | 1 | 1 | 1 | 1 | 1 | 5 |
| Hirsch et al., 2004 [31] | 0 | 0 | 0 | 0 | 0 | 0 |
| Malevez et al., 2004 [13] | N/A | N/A | N/A | N/A | N/A | N/A |
| Maló et al., 2008 [11] | 0 | 0 | 0 | 0 | 0 | 0 |
| Maló et al., 2012 [44] | N/A | N/A | N/A | N/A | N/A | N/A |
| Maló et al., 2014 [43] | N/A | N/A | N/A | N/A | N/A | N/A |
| Miglioranca et al., 2011 [46] | N/A | N/A | N/A | N/A | N/A | N/A |
| Miglioranca et al., 2012 [34] | 0 | 0 | 1 | 0 | 0 | 1 |
| Mozzati et al., 2008 [54] | N/A | N/A | N/A | N/A | N/A | N/A |
| Rodríguez-Chessa et al., 2014 [45] | N/A | N/A | N/A | N/A | N/A | N/A |
| Peñarrocha et al., 2005 [55] | N/A | N/A | N/A | N/A | N/A | N/A |
| Peñarrocha et al., 2007 [48] | N/A | N/A | N/A | N/A | N/A | N/A |
| Peñarrocha-Diago et al., 2020 [51] | N/A | N/A | N/A | N/A | N/A | N/A |
| Pi-Urgell et al., 2008 [42] | N/A | N/A | N/A | N/A | N/A | N/A |
| Stievenart et al., 2010 [49] | N/A | N/A | N/A | N/A | N/A | N/A |
| Vrielinck et al., 2003 [33] | 0 | 0 | 0 | 0 | 0 | 0 |
| Yates et al., 2014 [50] | N/A | N/A | N/A | N/A | N/A | N/A |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gutiérrez Muñoz, D.; Obrador Aldover, C.; Zubizarreta-Macho, Á.; González Menéndez, H.; Lorrio Castro, J.; Peñarrocha-Oltra, D.; Montiel-Company, J.M.; Hernández Montero, S. Survival Rate and Prosthetic and Sinus Complications of Zygomatic Dental Implants for the Rehabilitation of the Atrophic Edentulous Maxilla: A Systematic Review and Meta-Analysis. Biology 2021, 10, 601. https://doi.org/10.3390/biology10070601
Gutiérrez Muñoz D, Obrador Aldover C, Zubizarreta-Macho Á, González Menéndez H, Lorrio Castro J, Peñarrocha-Oltra D, Montiel-Company JM, Hernández Montero S. Survival Rate and Prosthetic and Sinus Complications of Zygomatic Dental Implants for the Rehabilitation of the Atrophic Edentulous Maxilla: A Systematic Review and Meta-Analysis. Biology. 2021; 10(7):601. https://doi.org/10.3390/biology10070601
Chicago/Turabian StyleGutiérrez Muñoz, David, Caterina Obrador Aldover, Álvaro Zubizarreta-Macho, Héctor González Menéndez, Juan Lorrio Castro, David Peñarrocha-Oltra, José María Montiel-Company, and Sofía Hernández Montero. 2021. "Survival Rate and Prosthetic and Sinus Complications of Zygomatic Dental Implants for the Rehabilitation of the Atrophic Edentulous Maxilla: A Systematic Review and Meta-Analysis" Biology 10, no. 7: 601. https://doi.org/10.3390/biology10070601
APA StyleGutiérrez Muñoz, D., Obrador Aldover, C., Zubizarreta-Macho, Á., González Menéndez, H., Lorrio Castro, J., Peñarrocha-Oltra, D., Montiel-Company, J. M., & Hernández Montero, S. (2021). Survival Rate and Prosthetic and Sinus Complications of Zygomatic Dental Implants for the Rehabilitation of the Atrophic Edentulous Maxilla: A Systematic Review and Meta-Analysis. Biology, 10(7), 601. https://doi.org/10.3390/biology10070601