
Risk of COVID-19 in Chagas Disease Patients: What Happen with Cardiac Affectations?

 ,
, 
Simple Summary
Abstract
1. Introduction
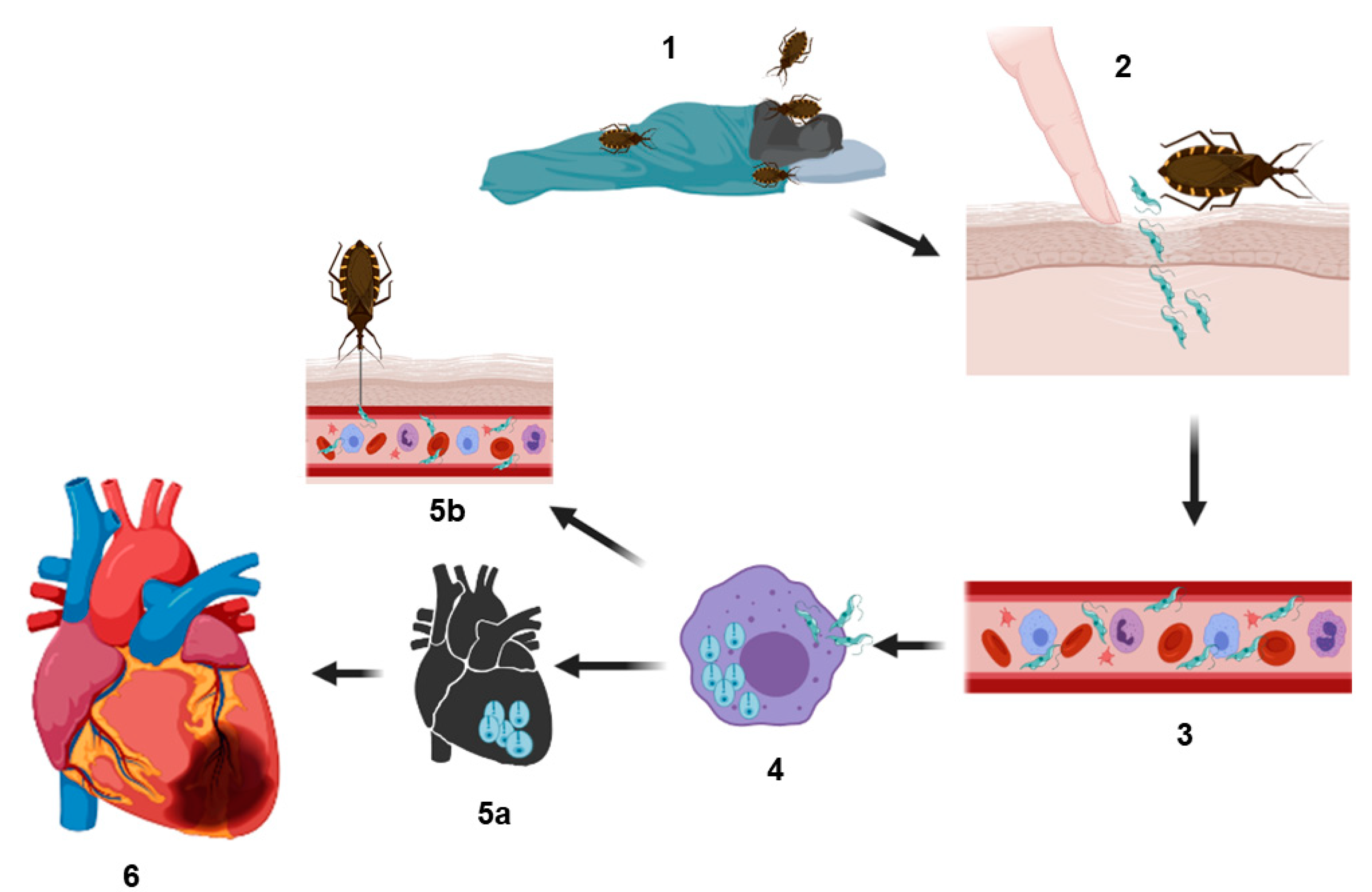
2. Phases of the Chagas Disease
Acute and Chronic Chagas Cardiomyopathy
3. Cardiac Implications, Patients with COVID-19 and Chagas Disease
4. Potential Risk of Heart Damage in Population with Chagas Disease or Other Comorbidities in the COVID-19 Pandemic
5. Influence of COVID-19 Treatment in Patients with Chagas Disease
6. Recommendations for the Prevention of Chagas Disease and COVID-19
7. Conclusions and Perspectives
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Schmunis, G.A.; Yadon, Z.E. Chagas disease: A Latin American health problem becoming a world health problem. Acta Trop. 2010, 115, 14–21. [Google Scholar] [CrossRef]
- Rojo-Medina, J.; Ruiz-Matus, C.; Salazar-Schettino, P.M.; González-Roldán, J.F. Enfermedad de chagas en México. Gac. Med. Mex. 2018, 154, 605–612. [Google Scholar] [CrossRef]
- Bolano-Ortiz, T.R.; Camargo-Caicedo, Y.; Puliafito, S.E.; Ruggeri, M.F.; Bolano-Diaz, S.; Pascual-Flores, R.; Saturno, J.; Ibarra-Espinosa, S.; Mayol-Bracero, O.L.; Torres-Delgado, E.; et al. Spread of SARS-CoV-2 through Latin America and the Caribbean region: A look from its economic conditions, climate and air pollution indicators. Environ. Res. 2020, 191, 109938. [Google Scholar] [CrossRef]
- Suarez, V.; Suarez Quezada, M.; Oros Ruiz, S.; Ronquillo De Jesus, E. Epidemiology of COVID-19 in Mexico: From the 27th of February to the 30th of April 2020. Rev. Clin. Esp. 2020, 220, 463–471. [Google Scholar] [CrossRef] [PubMed]
- Dong, E.; Du, H.; Gardner, L. An interactive web-based dashboard to track COVID-19 in real time. Lancet Infect. Dis. 2020, 20, 533–534. [Google Scholar] [CrossRef]
- Montgomery, S.P.; Starr, M.C.; Cantey, P.T.; Edwards, M.S.; Meymandi, S.K. Neglected parasitic infections in the United States: Chagas disease. Am. J. Trop. Med. Hyg. 2014, 90, 814–818. [Google Scholar] [CrossRef]
- Balouz, V.; Aguero, F.; Buscaglia, C.A. Chagas Disease Diagnostic Applications: Present Knowledge and Future Steps. Adv. Parasitol. 2017, 97, 1–45. [Google Scholar] [PubMed]
- Herrera-Nebel, M.-T.; Jesús Almonte, L.d.; Mejía Reyes, P. Agencia y pobreza por entidad federativa en México. Éthique Économique Ethics Econ. 2020, 17, 39–64. [Google Scholar]
- Salazar Schettino, P.; Bucio Torres, M.; Rojo Mdina, J.; Manuel Valencia, Y. Manual de Procedimientos para la Enfermedad de Chagas en México; Secretaría de Salud: Mexico, 2019; Available online: https://www.gob.mx/cms/uploads/attachment/file/447946/Manual_de_Procedimientos_para_la_Enfermedad_de_Chagas_en_Mexico.pdf (accessed on 27 April 2021).
- Arnal, A.; Waleckx, E.; Rico-Chavez, O.; Herrera, C.; Dumonteil, E. Estimating the current burden of Chagas disease in Mexico: A systematic review and meta-analysis of epidemiological surveys from 2006 to 2017. PLoS Negl. Trop. Dis. 2019, 13, e0006859. [Google Scholar] [CrossRef] [PubMed]
- Carabarin-Lima, A.; Gonzalez-Vazquez, M.C.; Rodriguez-Morales, O.; Baylon-Pacheco, L.; Rosales-Encina, J.L.; Reyes-Lopez, P.A.; Arce-Fonseca, M. Chagas disease (American trypanosomiasis) in Mexico: An update. Acta Trop. 2013, 127, 126–135. [Google Scholar] [CrossRef]
- SINAVE. Boletín Epidemiológico, Sistema Nacional de Vigilancia Epidemiológica Semana 53; Secretaría de Salud: Mexico, 2020; Available online: https://www.gob.mx/salud/documentos/boletinepidemiologico-sistema-nacional-de-vigilancia-epidemiologica-sistema-unico-de-informacion-231750 (accessed on 27 April 2021).
- Breniere, S.F.; Waleckx, E.; Barnabe, C. Over Six Thousand Trypanosoma cruzi Strains Classified into Discrete Typing Units (DTUs): Attempt at an Inventory. PLoS Negl. Trop. Dis. 2016, 10, e0004792. [Google Scholar] [CrossRef] [PubMed]
- Botero, L.A.; Mejia, A.M.; Triana, O. Biological and genetic characterization of two Colombian clones of Trypanosoma cruzi groups I and II. Biomedica 2007, 27, 64–74. [Google Scholar] [CrossRef][Green Version]
- Coura, J.R. The main sceneries of Chagas disease transmission. The vectors, blood and oral transmissions--a comprehensive review. Mem. Inst. Oswaldo Cruz 2015, 110, 277–282. [Google Scholar] [CrossRef]
- Forsyth, C.; Meymandi, S.; Moss, I.; Cone, J.; Cohen, R.; Batista, C. Proposed multidimensional framework for understanding Chagas disease healthcare barriers in the United States. PLoS Negl. Trop. Dis. 2019, 13, e0007447. [Google Scholar] [CrossRef]
- Andrade, J.P.d.; Marin Neto, J.A.; Paola, A.A.V.d.; Vilas-Boas, F.; Oliveira, G.M.M.; Bacal, F.; Bocchi, E.A.; Almeida, D.R.; Fragata Filho, A.A.; Moreira, M.d.C.V. I Diretriz Latino-Americana para o diagnóstico e tratamento da cardiopatia chagásica: Resumo executivo. Arq. Bras. Cardiol. 2011, 96, 434–442. [Google Scholar] [CrossRef] [PubMed]
- Rossi, M.A.; Ramos, S.G.; Bestetti, R.B. Chagas’ heart disease: Clinical-pathological correlation. Front. Biosci. 2003, 8, e94–e109. [Google Scholar] [CrossRef] [PubMed]
- Rassi, A., Jr.; Rassi, A.; Marin-Neto, J.A. Chagas disease. Lancet 2010, 375, 1388–1402. [Google Scholar] [CrossRef]
- Tanowitz, H.B.; Machado, F.S.; Jelicks, L.A.; Shirani, J.; de Carvalho, A.C.; Spray, D.C.; Factor, S.M.; Kirchhoff, L.V.; Weiss, L.M. Perspectives on Trypanosoma cruzi-induced heart disease (Chagas disease). Prog. Cardiovasc. Dis. 2009, 51, 524–539. [Google Scholar] [CrossRef]
- Bonney, K.M.; Luthringer, D.J.; Kim, S.A.; Garg, N.J.; Engman, D.M. Pathology and Pathogenesis of Chagas Heart Disease. Annu. Rev. Pathol. 2019, 14, 421–447. [Google Scholar] [CrossRef] [PubMed]
- Benziger, C.P.; do Carmo, G.A.L.; Ribeiro, A.L.P. Chagas Cardiomyopathy: Clinical Presentation and Management in the Americas. Cardiol. Clin. 2017, 35, 31–47. [Google Scholar] [CrossRef] [PubMed]
- Andrade, Z.A. Immunopathology of Chagas disease. Mem. Inst. Oswaldo Cruz 1999, 94, 71–80. [Google Scholar] [CrossRef]
- Campos, S.V.; Strabelli, T.M.; Amato Neto, V.; Silva, C.P.; Bacal, F.; Bocchi, E.A.; Stolf, N.A. Risk factors for Chagas’ disease reactivation after heart transplantation. J. Heart Lung Transpl. 2008, 27, 597–602. [Google Scholar] [CrossRef]
- Gray, E.B.; La Hoz, R.M.; Green, J.S.; Vikram, H.R.; Benedict, T.; Rivera, H.; Montgomery, S.P. Reactivation of Chagas disease among heart transplant recipients in the United States, 2012–2016. Transpl. Infect. Dis. 2018, 20, e12996. [Google Scholar] [CrossRef]
- Bacal, F.; Silva, C.P.; Bocchi, E.A.; Pires, P.V.; Moreira, L.F.; Issa, V.S.; Moreira, S.A.; das Dores Cruz, F.; Strabelli, T.; Stolf, N.A.; et al. Mychophenolate mofetil increased chagas disease reactivation in heart transplanted patients: Comparison between two different protocols. Am. J. Transpl. 2005, 5, 2017–2021. [Google Scholar] [CrossRef] [PubMed]
- Ziegler, C.G.K.; Allon, S.J.; Nyquist, S.K.; Mbano, I.M.; Miao, V.N.; Tzouanas, C.N.; Cao, Y.; Yousif, A.S.; Bals, J.; Hauser, B.M.; et al. SARS-CoV-2 Receptor ACE2 Is an Interferon-Stimulated Gene in Human Airway Epithelial Cells and Is Detected in Specific Cell Subsets across Tissues. Cell 2020, 181, 1016–1035 e1019. [Google Scholar] [CrossRef] [PubMed]
- Dhama, K.; Khan, S.; Tiwari, R.; Sircar, S.; Bhat, S.; Malik, Y.S.; Singh, K.P.; Chaicumpa, W.; Bonilla-Aldana, D.K.; Rodriguez-Morales, A.J. Coronavirus Disease 2019-COVID-19. Clin. Microbiol. Rev. 2020, 33. [Google Scholar] [CrossRef] [PubMed]
- Hoffmann, M.; Kleine-Weber, H.; Schroeder, S.; Kruger, N.; Herrler, T.; Erichsen, S.; Schiergens, T.S.; Herrler, G.; Wu, N.H.; Nitsche, A.; et al. SARS-CoV-2 Cell Entry Depends on ACE2 and TMPRSS2 and Is Blocked by a Clinically Proven Protease Inhibitor. Cell 2020, 181, 271–280 e278. [Google Scholar] [CrossRef]
- Ortiz-Prado, E.; Simbana-Rivera, K.; Gomez-Barreno, L.; Rubio-Neira, M.; Guaman, L.P.; Kyriakidis, N.C.; Muslin, C.; Jaramillo, A.M.G.; Barba-Ostria, C.; Cevallos-Robalino, D.; et al. Clinical, molecular, and epidemiological characterization of the SARS-CoV-2 virus and the Coronavirus Disease 2019 (COVID-19), a comprehensive literature review. Diagn. Microbiol. Infect. Dis. 2020, 98, 115094. [Google Scholar] [CrossRef] [PubMed]
- Harrison, A.G.; Lin, T.; Wang, P. Mechanisms of SARS-CoV-2 Transmission and Pathogenesis. Trends Immunol. 2020, 41, 1100–1115. [Google Scholar] [CrossRef]
- Perlman, S.; Netland, J. Coronaviruses post-SARS: Update on replication and pathogenesis. Nat. Rev. Microbiol. 2009, 7, 439–450. [Google Scholar] [CrossRef]
- Oudit, G.Y.; Kassiri, Z.; Jiang, C.; Liu, P.P.; Poutanen, S.M.; Penninger, J.M.; Butany, J. SARS-coronavirus modulation of myocardial ACE2 expression and inflammation in patients with SARS. Eur. J. Clin. Investig. 2009, 39, 618–625. [Google Scholar] [CrossRef]
- Chen, L.; Li, X.; Chen, M.; Feng, Y.; Xiong, C. The ACE2 expression in human heart indicates new potential mechanism of heart injury among patients infected with SARS-CoV-2. Cardiovasc. Res. 2020, 116, 1097–1100. [Google Scholar] [CrossRef]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: A single-centered, retrospective, observational study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef]
- Zaidel, E.J.; Forsyth, C.J.; Novick, G.; Marcus, R.; Ribeiro, A.L.P.; Pinazo, M.J.; Morillo, C.A.; Echeverria, L.E.; Shikanai-Yasuda, M.A.; Buekens, P.; et al. COVID-19: Implications for People with Chagas Disease. Glob. Heart 2020, 15, 69. [Google Scholar] [CrossRef] [PubMed]
- Guzik, T.J.; Mohiddin, S.A.; Dimarco, A.; Patel, V.; Savvatis, K.; Marelli-Berg, F.M.; Madhur, M.S.; Tomaszewski, M.; Maffia, P.; D’Acquisto, F.; et al. COVID-19 and the cardiovascular system: Implications for risk assessment, diagnosis, and treatment options. Cardiovasc. Res. 2020, 116, 1666–1687. [Google Scholar] [CrossRef] [PubMed]
- dos Santos-Neto, L.L.; Polcheira, M.F.; Castro, C.; Lima, R.A.; Simaan, C.K.; Correa-Lima, F.A. Trypanosoma cruzi high parasitemia in patient with systemic lupus erythematosus. Rev. Soc. Bras. Med. Trop. 2003, 36, 613–615. [Google Scholar] [CrossRef]
- Schett, G.; Sticherling, M.; Neurath, M.F. COVID-19: Risk for cytokine targeting in chronic inflammatory diseases? Nat. Rev. Immunol. 2020, 20, 271–272. [Google Scholar] [CrossRef] [PubMed]
- Crema, E.; Monteiro Ide, O.; Gomes, M.G.; Silva, A.A.; Rodrigues Junior, V. Evaluation of cytokines (MIG, IFN-gamma, TNF-alpha, IL-4, IL-5, and IL-10) during the different evolutive phases of chagasic esophagopathy. Clin. Immunol. 2006, 119, 213–218. [Google Scholar] [CrossRef]
- de Araujo, F.F.; Lima Torres, K.C.; Viana Peixoto, S.; Pinho Ribeiro, A.L.; Vaz Melo Mambrini, J.; Bortolo Rezende, V.; Lima Silva, M.L.; Loyola Filho, A.I.; Teixeira-Carvalho, A.; Lima-Costa, M.F.; et al. CXCL9 and CXCL10 display an age-dependent profile in Chagas patients: A cohort study of aging in Bambui, Brazil. Infect. Dis. Poverty 2020, 9, 51. [Google Scholar] [CrossRef]
- Echeverria, L.E.; Marcus, R.; Novick, G.; Sosa-Estani, S.; Ralston, K.; Zaidel, E.J.; Forsyth, C.; ALP, R.I.; Mendoza, I.; Falconi, M.L.; et al. WHF IASC Roadmap on Chagas Disease. Glob. Heart 2020, 15, 26. [Google Scholar] [CrossRef]
- Opoka-Winiarska, V.; Grywalska, E.; Rolinski, J. Could hemophagocytic lymphohistiocytosis be the core issue of severe COVID-19 cases? BMC Med. 2020, 18, 214. [Google Scholar] [CrossRef]
- Lopez, L.; Arai, K.; Gimenez, E.; Jimenez, M.; Pascuzo, C.; Rodriguez-Bonfante, C.; Bonfante-Cabarcas, R. C-reactive protein and interleukin-6 serum levels increase as Chagas disease progresses towards cardiac failure. Rev. Esp. Cardiol. 2006, 59, 50–56. [Google Scholar] [CrossRef]
- Komarowska, I.; Coe, D.; Wang, G.; Haas, R.; Mauro, C.; Kishore, M.; Cooper, D.; Nadkarni, S.; Fu, H.; Steinbruchel, D.A.; et al. Hepatocyte Growth Factor Receptor c-Met Instructs T Cell Cardiotropism and Promotes T Cell Migration to the Heart via Autocrine Chemokine Release. Immunity 2015, 42, 1087–1099. [Google Scholar] [CrossRef]
- Siripanthong, B.; Nazarian, S.; Muser, D.; Deo, R.; Santangeli, P.; Khanji, M.Y.; Cooper, L.T., Jr.; Chahal, C.A.A. Recognizing COVID-19-related myocarditis: The possible pathophysiology and proposed guideline for diagnosis and management. Heart Rhythm. 2020, 17, 1463–1471. [Google Scholar] [CrossRef]
- Wang, Y.; Moreira Mda, C.; Heringer-Walther, S.; Ebermann, L.; Schultheiss, H.P.; Wessel, N.; Siems, W.E.; Walther, T. Plasma ACE2 activity is an independent prognostic marker in Chagas’ disease and equally potent as BNP. J. Card. Fail. 2010, 16, 157–163. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Moreira Mda, C.; Heringer-Walther, S.; Schultheiss, H.P.; Siems, W.E.; Wessel, N.; Walther, T. Beta blockers prevent correlation of plasma ACE2 activity with echocardiographic parameters in patients with idiopathic dilated cardiomyopathy. J. Cardiovasc. Pharmacol. 2015, 65, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Gembardt, F.; Sterner-Kock, A.; Imboden, H.; Spalteholz, M.; Reibitz, F.; Schultheiss, H.P.; Siems, W.E.; Walther, T. Organ-specific distribution of ACE2 mRNA and correlating peptidase activity in rodents. Peptides 2005, 26, 1270–1277. [Google Scholar] [CrossRef]
- Epelman, S.; Tang, W.H.; Chen, S.Y.; Van Lente, F.; Francis, G.S.; Sen, S. Detection of soluble angiotensin-converting enzyme 2 in heart failure: Insights into the endogenous counter-regulatory pathway of the renin-angiotensin-aldosterone system. J. Am. Coll. Cardiol. 2008, 52, 750–754. [Google Scholar] [CrossRef] [PubMed]
- Lambert, D.W.; Yarski, M.; Warner, F.J.; Thornhill, P.; Parkin, E.T.; Smith, A.I.; Hooper, N.M.; Turner, A.J. Tumor necrosis factor-alpha convertase (ADAM17) mediates regulated ectodomain shedding of the severe-acute respiratory syndrome-coronavirus (SARS-CoV) receptor, angiotensin-converting enzyme-2 (ACE2). J. Biol. Chem. 2005, 280, 30113–30119. [Google Scholar] [CrossRef] [PubMed]
- Greenberg, B. An ACE in the hole alternative pathways of the renin angiotensin system and their potential role in cardiac remodeling. J. Am. Coll. Cardiol. 2008, 52, 755–757. [Google Scholar] [CrossRef] [PubMed]
- Fung, J.W.; Yu, C.M.; Yip, G.; Chan, S.; Yandle, T.G.; Richards, A.M.; Nicholls, M.G.; Sanderson, J.E. Effect of beta blockade (carvedilol or metoprolol) on activation of the renin-angiotensin-aldosterone system and natriuretic peptides in chronic heart failure. Am. J. Cardiol. 2003, 92, 406–410. [Google Scholar] [CrossRef]
- Nunes, M.C.P.; Beaton, A.; Acquatella, H.; Bern, C.; Bolger, A.F.; Echeverria, L.E.; Dutra, W.O.; Gascon, J.; Morillo, C.A.; Oliveira-Filho, J.; et al. Chagas Cardiomyopathy: An Update of Current Clinical Knowledge and Management: A Scientific Statement From the American Heart Association. Circulation 2018, 138, e169–e209. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.H.; Cai, L.; Cheng, Z.S.; Cheng, H.; Deng, T.; Fan, Y.P.; Fang, C.; Huang, D.; Huang, L.Q.; Huang, Q.; et al. A rapid advice guideline for the diagnosis and treatment of 2019 novel coronavirus (2019-nCoV) infected pneumonia (standard version). Mil. Med. Res. 2020, 7, 4. [Google Scholar] [CrossRef] [PubMed]
- Nishiga, M.; Wang, D.W.; Han, Y.; Lewis, D.B.; Wu, J.C. COVID-19 and cardiovascular disease: From basic mechanisms to clinical perspectives. Nat. Rev. Cardiol. 2020, 17, 543–558. [Google Scholar] [CrossRef]
- OECD. The Heavy Burden of Obesity; OECD: Paris, France, 2019. [Google Scholar]
- INEGI. Censo de Población y Vivienda; Mexico, 2020. Available online: https://www.inegi.org.mx/programas/ccpv/2020/default.html#Resultados_generales (accessed on 27 April 2021).
- Castro-Juárez, C.J.; Cabrera-Pivaral, C.E.; Ramírez-García, S.A.; García-Sierra, L.; Morales-Pérez, L.; Ramírez-Concepción, H.R. Factores de riesgo para enfermedad cardiovascular en adultos mexicanos/Risk factors for cardiovascular disease in Mexican adults. Rev. Méd. MD 2017, 9, 152–162. [Google Scholar]
- Parra-Bracamonte, G.M.; Lopez-Villalobos, N.; Parra-Bracamonte, F.E. Clinical characteristics and risk factors for mortality of patients with COVID-19 in a large data set from Mexico. Ann. Epidemiol. 2020, 52, 93–98. [Google Scholar] [CrossRef]
- Pablos-Mendez, A.; Vega, J.; Aranguren, F.P.; Tabish, H.; Raviglione, M.C. Covid-19 in Latin America. BMJ 2020, 370, m2939. [Google Scholar] [CrossRef]
- Urbina, J.A. Ergosterol biosynthesis and drug development for Chagas disease. Mem. Inst. Oswaldo Cruz 2009, 104, 311–318. [Google Scholar] [CrossRef]
- Scarim, C.B.; de Andrade, C.R.; da Rosa, J.A.; Dos Santos, J.L.; Chin, C.M. Hydroxymethylnitrofurazone treatment in indeterminate form of chronic Chagas disease: Reduced intensity of tissue parasitism and inflammation-A histopathological study. Int. J. Exp. Pathol. 2018, 99, 236–248. [Google Scholar] [CrossRef]
- Bern, C. Antitrypanosomal therapy for chronic Chagas’ disease. N. Engl. J. Med. 2011, 364, 2527–2534. [Google Scholar] [CrossRef] [PubMed]
- Vallejo, M.; Montenegro, P.; Reyes, P.A. How much does the medical treatment of chronic Chagas cardiopathy cost? Direct costs in a cardiology hospital. Arch. Cardiol. Mex. 2002, 72, 129–137. [Google Scholar]
- Flores-Ocampo, J.; Nava, S.; Marquez, M.F.; Gomez-Flores, J.; Colin, L.; Lopez, A.; Celaya, M.; Trevino, E.; Gonzalez-Hermosillo, J.A.; Iturralde, P. Clinical predictors of ventricular arrhythmia storms in Chagas cardiomyopathy patients with implantable defibrillators. Arch. Cardiol. Mex. 2009, 79, 263–267. [Google Scholar]
- Curran, C.S.; Rivera, D.R.; Kopp, J.B. COVID-19 Usurps Host Regulatory Networks. Front. Pharmacol. 2020, 11, 1278. [Google Scholar] [CrossRef] [PubMed]
- Hossen, M.S.; Barek, M.A.; Jahan, N.; Safiqul Islam, M. A Review on Current Repurposing Drugs for the Treatment of COVID-19: Reality and Challenges. SN Compr. Clin. Med. 2020, 2, 1777–1789. [Google Scholar] [CrossRef] [PubMed]
- Ault, S. Chagas disease and neglected diseases: Chalenging poverty and exclusion. Enferm. Chagas Puerta 2007, 100, 1909–2006. [Google Scholar]
- Abad-Franch, F.; Diotaiuti, L.; Gurgel-Goncalves, R.; Gurtler, R.E. Certifying the interruption of Chagas disease transmission by native vectors: Cui bono? Mem. Inst. Oswaldo Cruz 2013, 108, 251–254. [Google Scholar] [CrossRef] [PubMed]
- Fabbro, D.L.; Danesi, E.; Olivera, V.; Codebo, M.O.; Denner, S.; Heredia, C.; Streiger, M.; Sosa-Estani, S. Trypanocide treatment of women infected with Trypanosoma cruzi and its effect on preventing congenital Chagas. PLoS Negl. Trop. Dis. 2014, 8, e3312. [Google Scholar] [CrossRef]
- World Health Organization. Overview of Public Health and Social Measures in the Context of COVID-19: Interim Guidance, 18 May 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Stone, T.E.; Kunaviktikul, W.; Omura, M.; Petrini, M. Facemasks and the Covid 19 pandemic: What advice should health professionals be giving the general public about the wearing of facemasks? Nurs. Health Sci. 2020, 22, 339–342. [Google Scholar] [CrossRef]
- Johnson, M.; Chetty, K. Corona Prevention and Control-A Preview. Int. Res. Med. Health Sci. 2021, 4, 8–22. [Google Scholar]
- Xu, Y.; Baylink, D.J.; Chen, C.S.; Reeves, M.E.; Xiao, J.; Lacy, C.; Lau, E.; Cao, H. The importance of vitamin d metabolism as a potential prophylactic, immunoregulatory and neuroprotective treatment for COVID-19. J. Transl. Med. 2020, 18, 322. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| COVID-19 | Chagas Disease |
|---|---|
| Rhythm abnormalities: supraventricular and ventricular tachyarrhythmias, bradyarrhythmias and chest pain or chest tightness on exertion [47]. | Rhythm abnormalities: bradyarrhythmias and conduction system abnormalities and atrial/ventricular tachyarrhythmias [55]. |
| Electrocardiogram abnormalities: QT prolongation, pseudo infarct pattern and premature ventricular complexes. Development of cardiac arrest and variations in the myocardial enzyme level [30,47,56]. | Primary ST- and T-wave abnormalities, pathological Q waves or electric inactive areas [55]. Segmental/global wall motion abnormalities, dilated cardiomyopathy and function mitral/tricuspid regurgitation [21,55]. |
| Acute coronary syndrome, venous thromboembolism and elevated levels of troponin T (>0.022 ng/mL) [57]. | Aneurysms: left ventricular apical, other left ventricular segments (inferior and inferolateral walls) and uncommonly right ventricular [55]. |
| Capillary endothelial cells dysfunction and induced micro-circulation disorder [34]. | Thromboembolic events: ischemic attack or stroke, pulmonary or systemic emboli [22]. |
| Pericardial inflammation, microvascular ischemia (through pericytes) and myocardial edema/scar (nonischemic) [47]. | Microvascular abnormalities: precordial/retrosternal chest pain without evidence of epicardial coronary artery disease [22]. |
| Prolonged myocardial inflammation and disseminated intravascular coagulation [31]. | Myocardial scar/interstitial fibrosis and pericarditis [18,22]. |
| Heart failure, including raised jugular venous pressure, peripheral edema and right upper quadrant pain [38]. Cardiac dysfunction and normal/acute injury [44]. | Myocardial micronecrosis [18]. |
| Myocarditis and fulminant myocarditis with presence of febrile and low pulse pressure, cold or mottled extremities, and sinus tachycardia [47]. Proinflammatory cytokines production (IL-6 and TNF-alpha) and high levels of creatinine kinase (>200 U/L) [34,38]. | Myocarditis associated with myocytolysis, myofiber hypertrophy and cardiac remodeling, resulting in a fully enlarged heart [18,21]. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Diaz-Hernandez, A.; Gonzalez-Vazquez, M.C.; Arce-Fonseca, M.; Rodriguez-Morales, O.; Cedilllo-Ramirez, M.L.; Carabarin-Lima, A. Risk of COVID-19 in Chagas Disease Patients: What Happen with Cardiac Affectations? Biology 2021, 10, 411. https://doi.org/10.3390/biology10050411
Diaz-Hernandez A, Gonzalez-Vazquez MC, Arce-Fonseca M, Rodriguez-Morales O, Cedilllo-Ramirez ML, Carabarin-Lima A. Risk of COVID-19 in Chagas Disease Patients: What Happen with Cardiac Affectations? Biology. 2021; 10(5):411. https://doi.org/10.3390/biology10050411
Chicago/Turabian StyleDiaz-Hernandez, Alejandro, Maria Cristina Gonzalez-Vazquez, Minerva Arce-Fonseca, Olivia Rodriguez-Morales, Maria Lilia Cedilllo-Ramirez, and Alejandro Carabarin-Lima. 2021. "Risk of COVID-19 in Chagas Disease Patients: What Happen with Cardiac Affectations?" Biology 10, no. 5: 411. https://doi.org/10.3390/biology10050411
APA StyleDiaz-Hernandez, A., Gonzalez-Vazquez, M. C., Arce-Fonseca, M., Rodriguez-Morales, O., Cedilllo-Ramirez, M. L., & Carabarin-Lima, A. (2021). Risk of COVID-19 in Chagas Disease Patients: What Happen with Cardiac Affectations? Biology, 10(5), 411. https://doi.org/10.3390/biology10050411