
Efficacy of Exercise-Based Rehabilitation Programs for Improving Muscle Function and Size in People with Hip Osteoarthritis: A Systematic Review with Meta-Analysis


Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy with Study Identification
2.2. Study Selection
2.2.1. Population
2.2.2. Interventions
2.2.3. Comparisons
2.2.4. Outcomes
2.2.5. Study Design
2.3. Data Extraction
2.4. Data Analysis
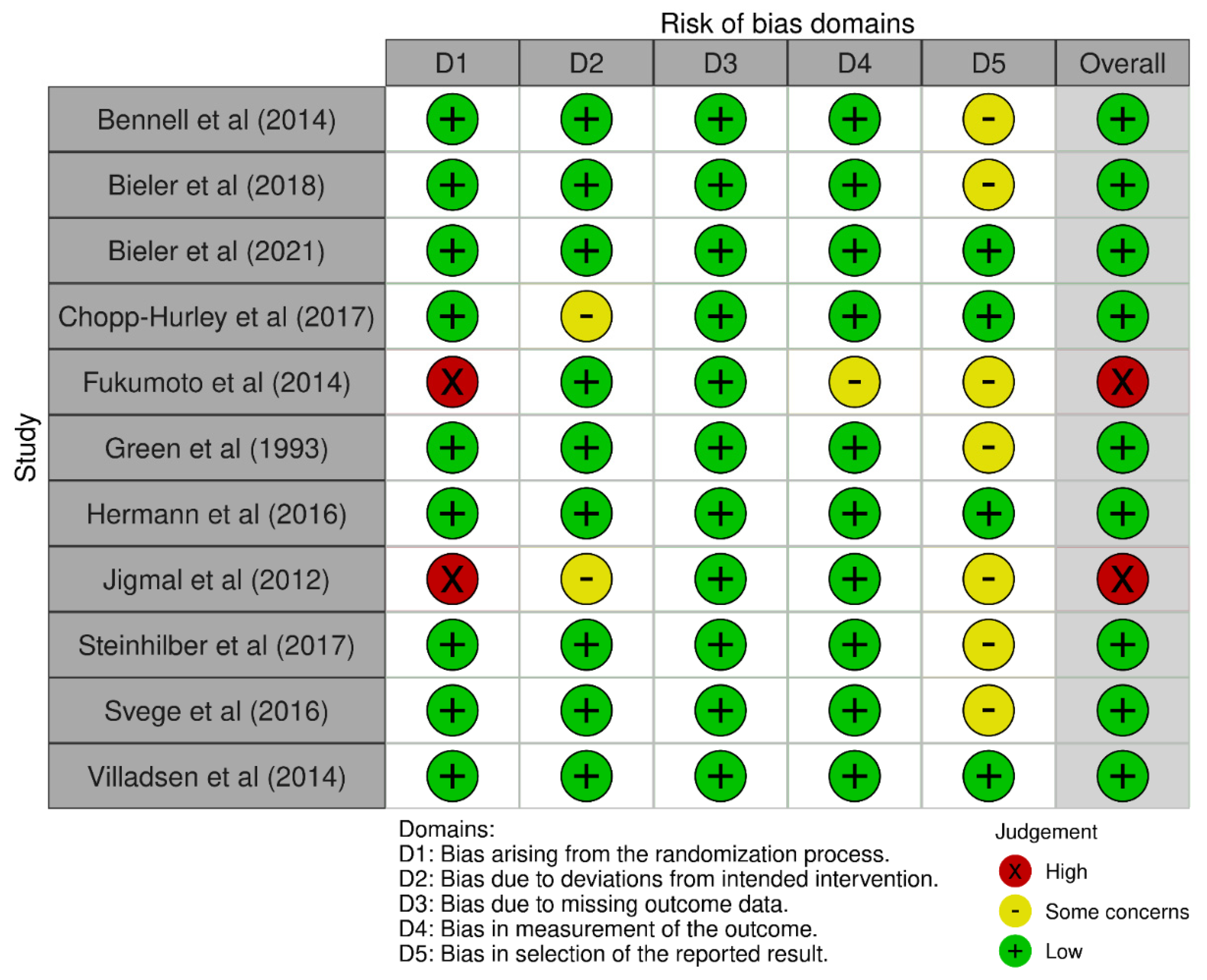
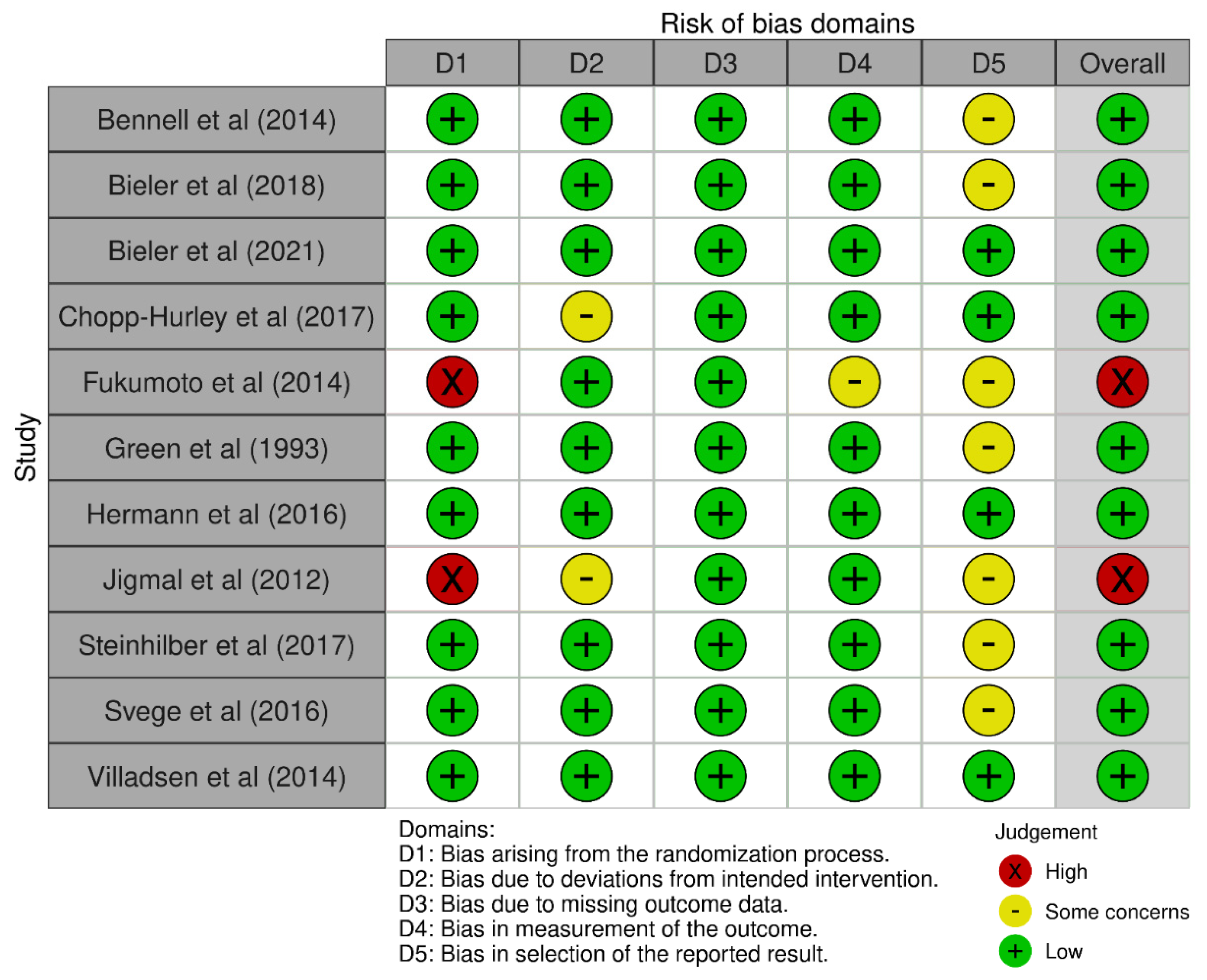
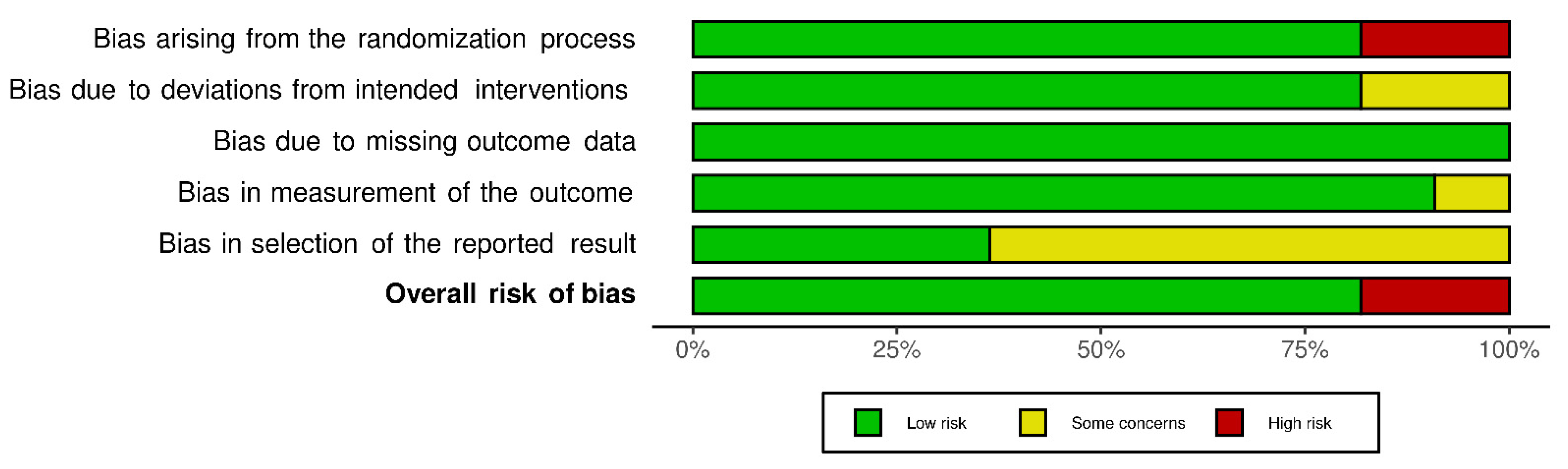
2.5. Quality Assessment
3. Results
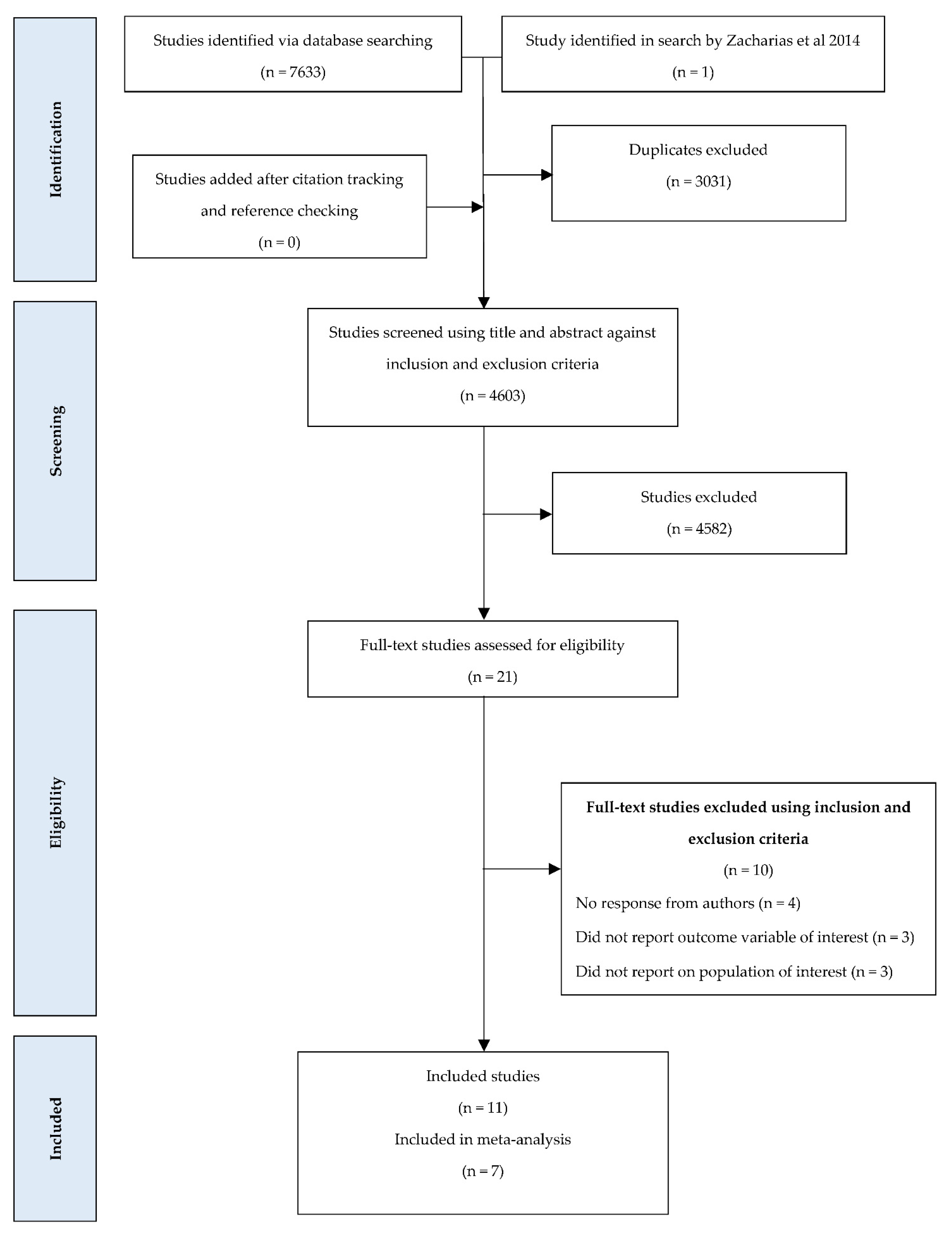
3.1. Yield
3.2. Results of Meta-Analysis
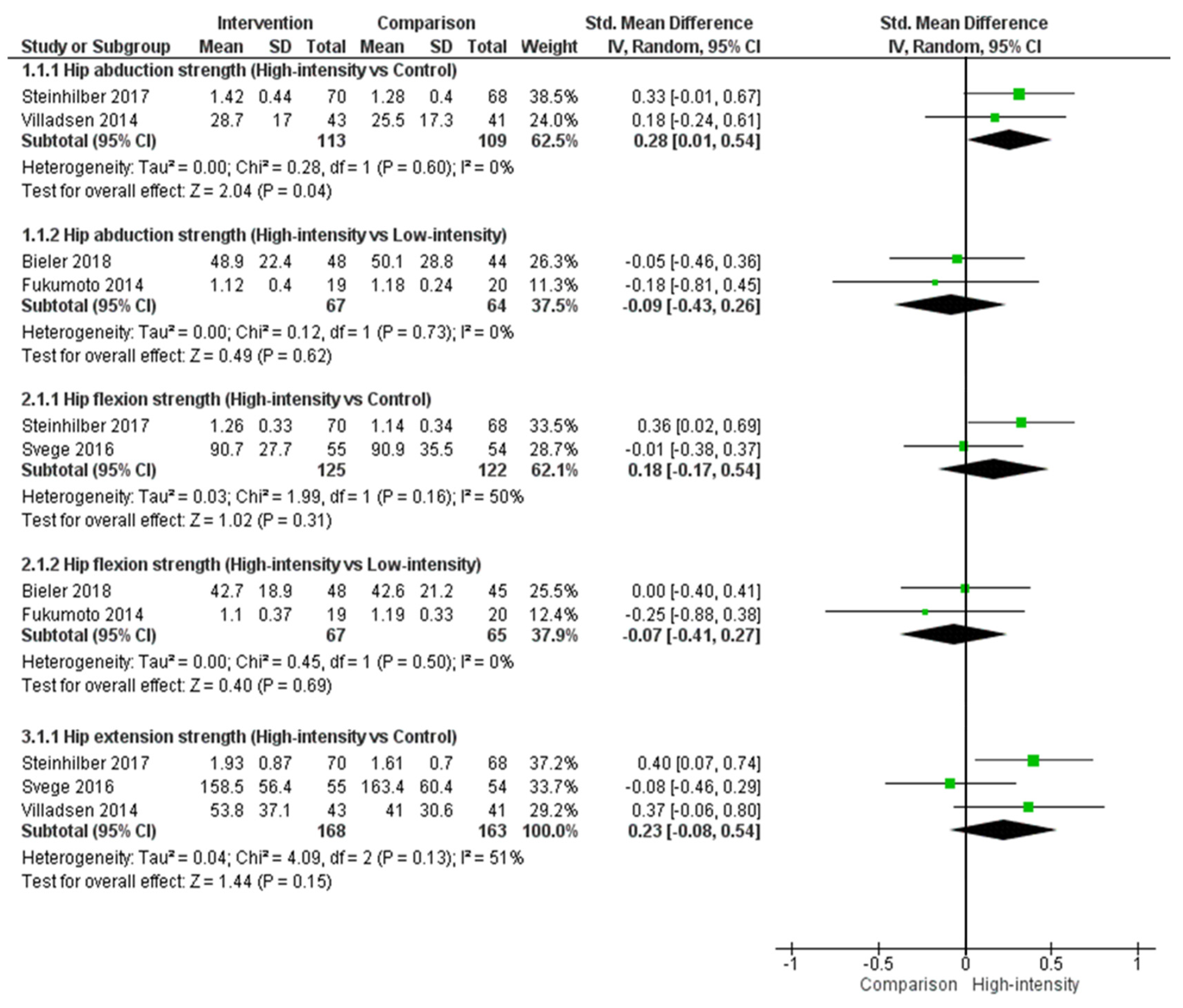
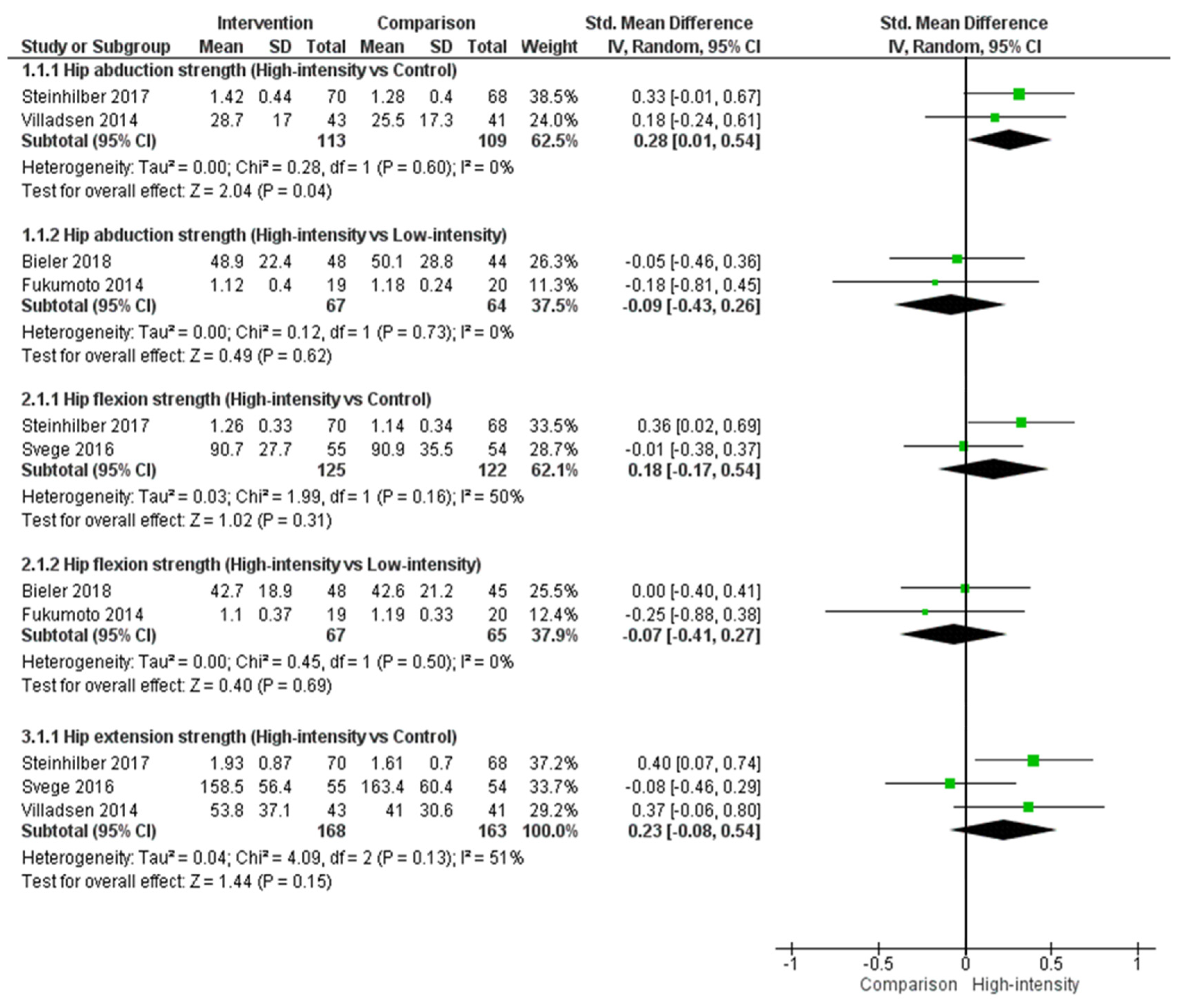
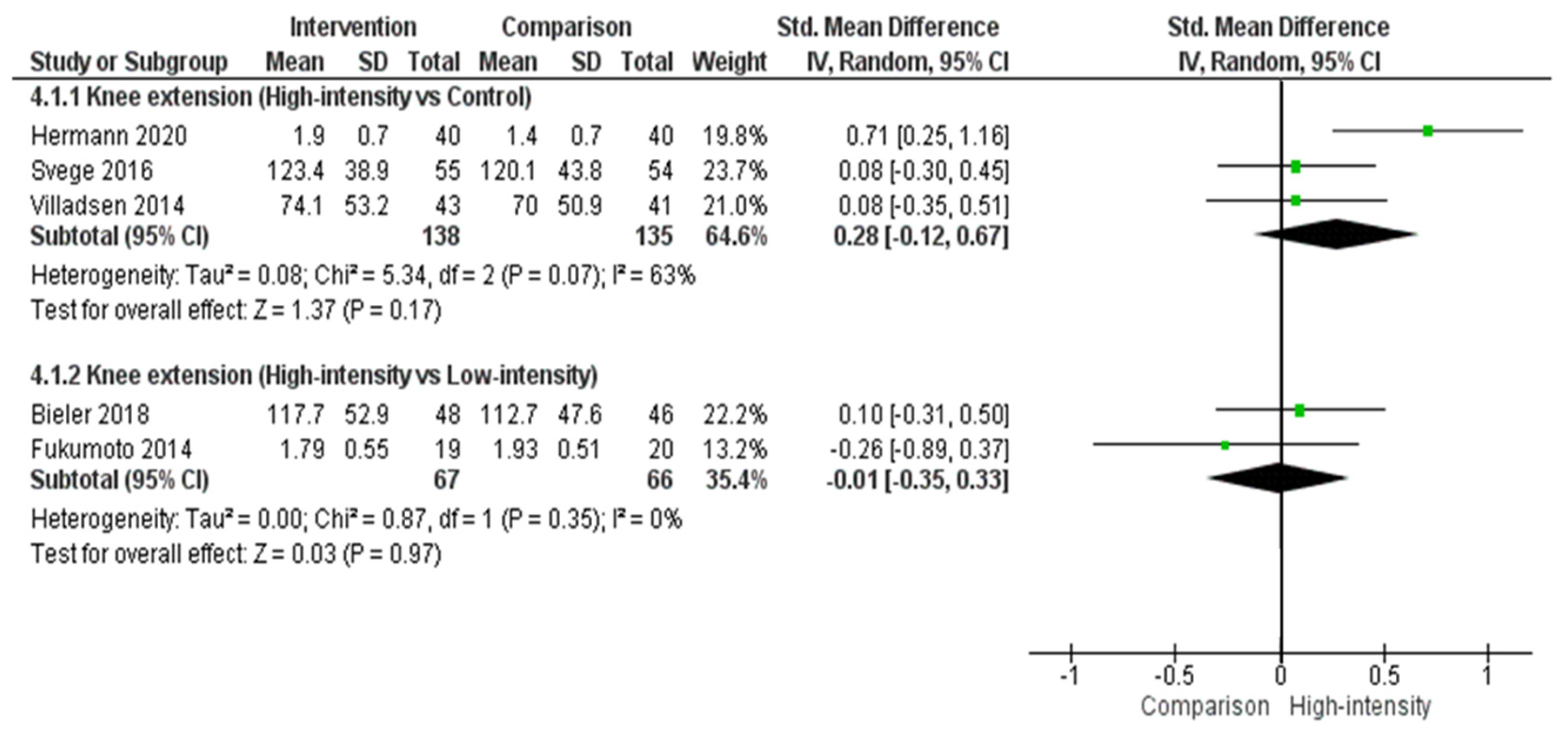
High-Intensity Resistance Exercise vs. Comparison (i.e., Low-Intensity Resistance Exercise and/or Control)
3.3. Other Comparisons
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| SOF Table of Hip Function (Hip Extension) For High-Intensity Resistance vs. Comparison in People with Hip Osteoarthritis | ||||
| Patient or population: People with hip osteoarthritis Intervention: High-intensity resistance Comparison: Control | ||||
| Outcomes | Effect size: SMD (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments |
| With high-intensity resistance exercise | ||||
| High-intensity vs. control | SMD 0.23 (−0.08–0.54) | 331 (3 RCTs) | ⊕⊕⊕⊝ MODERATE * | Effect size: This may represent no effect |
| SOF Table of Hip Function (Hip Abduction) for High-Intensity Resistance vs. Comparison in People with Hip Osteoarthritis | ||||
| Patient or population: People with hip osteoarthritis Intervention: High-intensity resistance Comparison: Control and/or low-intensity | ||||
| Outcomes | Effect size: SMD (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments |
| With high-intensity resistance exercise | ||||
| High-intensity vs. control | SMD 0.28 (0.01–0.54) | 222 (2 RCTs) | ⊕⊕⊝⊝ LOW * | Effect size: This represents a small effect |
| High-intensity vs. low-intensity | SMD −0.09 (−0.43–0.26) | 131 (2 RCTs) | ⊕⊕⊝⊝ LOW * | Effect size: This may represent no effect |
| SOF Table of Hip Function (Hip Flexion) for High-Intensity Resistance vs. Comparison in People with Hip Osteoarthritis | ||||
| Patient or population: People with hip osteoarthritis Intervention: High-intensity resistance Comparison: Control and/or low-intensity | ||||
| Outcomes | Effect size: SMD (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments |
| With high-intensity resistance exercise | ||||
| High-intensity vs. control | SMD 0.18 (−0.17–0.54) | 247 (2 RCTs) | ⊕⊕⊝⊝ LOW * | Effect size: This may represent no effect |
| High-intensity vs. low-intensity | SMD −0.07 (−0.41–0.27) | 132 (2 RCTs) | ⊕⊕⊝⊝ LOW * | Effect size: This may represent no effect |
| SOF Table of Knee Function (Knee Extension) for High-Intensity Resistance vs. Comparison in People with Hip Osteoarthritis | ||||
| Patient or population: People with hip osteoarthritis Intervention: High-intensity resistance Comparison: Control and/or low-intensity | ||||
| Outcomes | Effect size: SMD (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments |
| With high-intensity resistance exercise | ||||
| High-intensity vs. control | SMD 0.28 (−0.12–0.67) | 273 (3 RCTs) | ⊕⊕⊝⊝ LOW * | Effect size: This may represent no effect |
| High-intensity vs. low-intensity | SMD −0.01 (−0.35–0.33) | 133 (2 RCTs) | ⊕⊕⊝⊝ LOW * | Effect size: This may represent no effect |
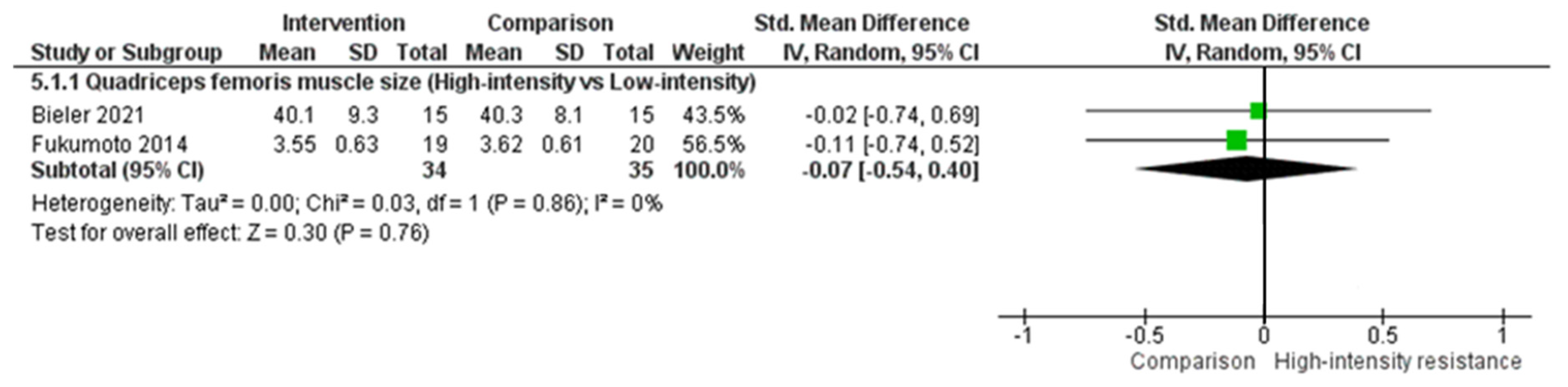
| SOF Table of Muscle Size (Quadriceps Femoris) for High-Intensity Resistance vs. Comparison in People with Hip Osteoarthritis | ||||
| Patient or population: People with hip osteoarthritis Intervention: High-intensity resistance Comparison: Low-intensity resistance | ||||
| Outcomes | Effect size: SMD (95% CI) | No of participants (studies) | Quality of the evidence (GRADE) | Comments |
| With high-intensity resistance exercise | ||||
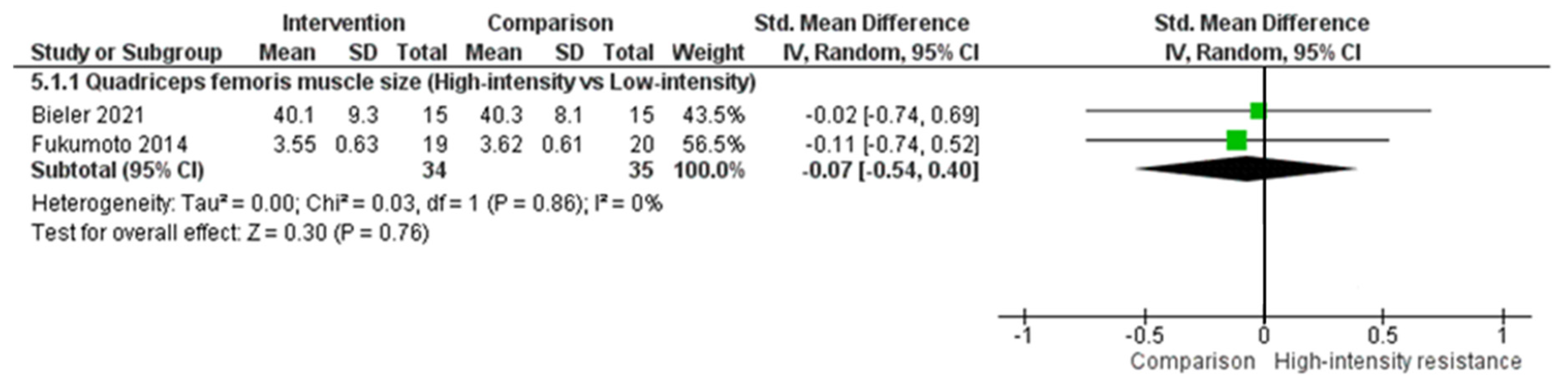
| High-intensity vs. low-intensity | SMD −0.07 (−0.54–0.4) | 69 (2 RCTs) | ⊕⊝⊝⊝ VERY LOW †,* | Effect size: This may represent no effect |
References
- Buckwalter, J.A.; Mankin, H.J.; Grodzinsky, A.J. Articular cartilage and osteoarthritis. Instr. Course Lect. 2005, 54, 465. [Google Scholar]
- Katz, J.N.; Arant, K.R.; Loeser, R.F. Diagnosis and treatment of hip and knee osteoarthritis: A review. JAMA 2021, 325, 568–578. [Google Scholar] [CrossRef]
- Australian Institute of Health Welfare. Osteoarthritis; AIHW: Canberra, Australia, 2019; Cat. no: PHE 232. [Google Scholar]
- Garstang, S.V.; Stitik, T.P. Osteoarthritis: Epidemiology, risk factors, and pathophysiology. Am. J. Phys. Med. Rehabil. 2006, 85, S2–S11. [Google Scholar] [CrossRef]
- O’Neill, T.W.; McCabe, P.S.; McBeth, J. Update on the epidemiology, risk factors and disease outcomes of osteoarthritis. Best Pract. Res. Clin. Rheumatol. 2018, 32, 312–326. [Google Scholar] [CrossRef]
- Zacharias, A.; Pizzari, T.; English, D.J.; Kapakoulakis, T.; Green, R.A. Hip abductor muscle volume in hip osteoarthritis and matched controls. Osteoarthr. Cart. 2016, 24, 1727–1735. [Google Scholar] [CrossRef] [Green Version]
- Loureiro, A.; Mills, P.M.; Barrett, R.S. Muscle weakness in hip osteoarthritis: A systematic review. Arthritis Care Res. 2013, 65, 340–352. [Google Scholar] [CrossRef]
- Marshall, A.R.; Noronha, M.d.; Zacharias, A.; Kapakoulakis, T.; Green, R. Structure and function of the abductors in patients with hip osteoarthritis: Systematic review and meta-analysis. J. Back Musculoskelet. Rehabil. 2016, 29, 191–204. [Google Scholar] [CrossRef]
- Zacharias, A.; Pizzari, T.; Semciw, A.I.; English, D.J.; Kapakoulakis, T.; Green, R.A. Gluteus medius and minimus activity during stepping tasks: Comparisons between people with hip osteoarthritis and matched control participants. Gait Posture 2020, 80, 339–346. [Google Scholar] [CrossRef]
- Arokoski, M.H.; Arokoski, J.P.; Haara, M.; Kankaanpää, M.; Vesterinen, M.; Niemitukia, L.H.; Helminen, H.J. Hip muscle strength and muscle cross sectional area in men with and without hip osteoarthritis. J. Rheumatol. 2002, 29, 2185–2195. [Google Scholar]
- Momose, T.; Inaba, Y.; Choe, H.; Kobayashi, N.; Tezuka, T.; Saito, T. CT-based analysis of muscle volume and degeneration of gluteus medius in patients with unilateral hip osteoarthritis. BMC Musculoskelet. Disord. 2017, 18, 457. [Google Scholar] [CrossRef] [Green Version]
- Rasch, A.; Byström, A.H.; Dalen, N.; Berg, H.E. Reduced muscle radiological density, cross-sectional area, and strength of major hip and knee muscles in 22 patients with hip osteoarthritis. Acta Orthop. 2007, 78, 505–510. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zacharias, A.; Pizzari, T.; Semciw, A.I.; English, D.J.; Kapakoulakis, T.; Green, R.A. Comparison of gluteus medius and minimus activity during gait in people with hip osteoarthritis and matched controls. Scand. J. Med. Sci. Sports 2019, 29, 696–705. [Google Scholar] [CrossRef]
- Diamond, L.E.; Hoang, H.X.; Barrett, R.S.; Loureiro, A.; Constantinou, M.; Lloyd, D.G.; Pizzolato, C. Individuals with mild-to-moderate hip osteoarthritis walk with lower hip joint contact forces despite higher levels of muscle co-contraction compared to healthy individuals. Osteoarthr. Cart. 2020, 28, 924–931. [Google Scholar] [CrossRef]
- Brosseau, L.; Pelland, L.; Wells, G.; Macleay, L.; Lamothe, C.; Michaud, G.; Lambert, J.; Robinson, V.; Tugwell, P. Efficacy of aerobic exercises for osteoarthritis (part II): A meta-analysis. Phys. Ther. Rev. 2004, 9, 125–145. [Google Scholar] [CrossRef]
- Bennell, K. Physiotherapy management of hip osteoarthritis. J. Physiother. 2013, 59, 145–157. [Google Scholar] [CrossRef] [Green Version]
- Uthman, O.A.; van der Windt, D.A.; Jordan, J.L.; Dziedzic, K.S.; Healey, E.L.; Peat, G.M.; Foster, N.E. Exercise for lower limb osteoarthritis: Systematic review incorporating trial sequential analysis and network meta-analysis. BMJ 2013, 347, f5555. [Google Scholar] [CrossRef] [Green Version]
- Fransen, M.; McConnell, S.; Hernandez-Molina, G.; Reichenbach, S. Exercise for osteoarthritis of the hip. Cochrane Database Syst. Rev. 2014, 4. [Google Scholar] [CrossRef] [Green Version]
- Bennell, K.L.; Egerton, T.; Martin, J.; Abbott, J.H.; Metcalf, B.; McManus, F.; Sims, K.; Pua, Y.-H.; Wrigley, T.V.; Forbes, A. Effect of physical therapy on pain and function in patients with hip osteoarthritis: A randomized clinical trial. JAMA 2014, 311, 1987–1997. [Google Scholar] [CrossRef]
- Zacharias, A.; Green, R.; Semciw, A.; Kingsley, M.; Pizzari, T. Efficacy of rehabilitation programs for improving muscle strength in people with hip or knee osteoarthritis: A systematic review with meta-analysis. Osteoarthr. Cart. 2014, 22, 1752–1773. [Google Scholar] [CrossRef] [Green Version]
- Schoenfeld, B.J. The mechanisms of muscle hypertrophy and their application to resistance training. J. Strength Cond. Res. 2010, 24, 2857–2872. [Google Scholar] [CrossRef] [Green Version]
- Pescatello, L.S. ACSMs guidelines for exercise testing and prescription. In Guidelines for Exercise Testing and Prescription, 9th ed.; Wolters Kluwer/Lippincott Williams & Wilkins Health: Philadelphia, PA, USA, 2014; pp. 42–43. [Google Scholar]
- Green, J.; McKenna, F.; Redfern, E.; Chamberlain, M. Home exercises are as effective as outpatient hydrotherapy for osteoarthritis of the hip. Rheumatology 1993, 32, 812–815. [Google Scholar] [CrossRef] [PubMed]
- Maly, M.R.; Marriott, K.A.; Chopp-Hurley, J.N. Osteoarthritis year in review 2019: Rehabilitation and outcomes. Osteoarthr. Cart. 2020, 28, 249–266. [Google Scholar] [CrossRef]
- Sandstedt, E.; Fasth, A.; Eek, M.N.; Beckung, E. Muscle strength, physical fitness and well-being in children and adolescents with juvenile idiopathic arthritis and the effect of an exercise programme: A randomized controlled trial. Pediatr. Rheumatol. 2013, 11, 7. [Google Scholar] [CrossRef] [Green Version]
- Moritani, T. Neural factors versus hypertrophy in the time course of muscle strength gain. Am. J. Phys. Med. Rehabil. 1979, 58, 115–130. [Google Scholar]
- Counts, B.R.; Buckner, S.L.; Mouser, J.G.; Dankel, S.J.; Jessee, M.B.; Mattocks, K.T.; Loenneke, J.P. Muscle growth: To infinity and beyond? Muscle Nerve 2017, 56, 1022–1030. [Google Scholar] [CrossRef] [PubMed]
- Garber, C.E.; Blissmer, B.; Deschenes, M.R.; Franklin, B.A.; Lamonte, M.J.; Lee, I.-M.; Nieman, D.C.; Swain, D.P. American college of sports medicine position stand. quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: Guidance for prescribing exercise. Med. Sci. Sports Exerc. 2011, 43, 1334–1359. [Google Scholar] [CrossRef] [PubMed]
- Fukumoto, Y.; Tateuchi, H.; Ikezoe, T.; Tsukagoshi, R.; Akiyama, H.; So, K.; Kuroda, Y.; Ichihashi, N. Effects of high-velocity resistance training on muscle function, muscle properties, and physical performance in individuals with hip osteoarthritis: A randomized controlled trial. Clin. Rehabil. 2014, 28, 48–58. [Google Scholar] [CrossRef] [PubMed]
- Conceição, F.; Fernandes, J.; Lewis, M.; Gonzaléz-Badillo, J.J.; Jimenéz-Reyes, P. Movement velocity as a measure of exercise intensity in three lower limb exercises. J. Sports Sci. 2016, 34, 1099–1106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Higgins JPT, G.S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0, The Cochrane Collaboration. 2011. Available online: www.handbook.cochrane.org (accessed on 13 November 2021).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: London, UK, 2013; pp. 79–81. [Google Scholar]
- Sterne, J.A.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balshem, H.; Helfand, M.; Schünemann, H.J.; Oxman, A.D.; Kunz, R.; Brozek, J.; Vist, G.E.; Falck-Ytter, Y.; Meerpohl, J.; Norris, S. GRADE guidelines: 3. Rating the quality of evidence. J. Clin. Epidemiol. 2011, 64, 401–406. [Google Scholar] [CrossRef] [PubMed]
- Andrews, J.; Guyatt, G.; Oxman, A.D.; Alderson, P.; Dahm, P.; Falck-Ytter, Y.; Nasser, M.; Meerpohl, J.; Post, P.N.; Kunz, R. GRADE guidelines: 14. Going from evidence to recommendations: The significance and presentation of recommendations. J. Clin. Epidemiol. 2013, 66, 719–725. [Google Scholar] [CrossRef]
- Bieler, T.; Siersma, V.; Magnusson, S.P.; Kjaer, M.; Beyer, N. Exercise induced effects on muscle function and range of motion in patients with hip osteoarthritis. Physiother. Res. Int. 2018, 23, e1697. [Google Scholar] [CrossRef]
- Chopp-Hurley, J.N.; Brenneman, E.C.; Wiebenga, E.G.; Bulbrook, B.; Keir, P.J.; Maly, M.R. Randomized controlled trial investigating the role of exercise in the workplace to improve work ability, performance, and patient-reported symptoms among older workers with osteoarthritis. J. Occup. Environ. Med. 2017, 59, 550–556. [Google Scholar] [CrossRef] [PubMed]
- Jigami, H.; Sato, D.; Tsubaki, A.; Tokunaga, Y.; Ishikawa, T.; Dohmae, Y.; Iga, T.; Minato, I.; Yamamoto, N.; Endo, N. Effects of weekly and fortnightly therapeutic exercise on physical function and health-related quality of life in individuals with hip osteoarthritis. J. Orthop. Sci. 2012, 17, 737–744. [Google Scholar] [CrossRef]
- Steinhilber, B.; Haupt, G.; Miller, R.; Janssen, P.; Krauss, I. Exercise therapy in patients with hip osteoarthritis: Effect on hip muscle strength and safety aspects of exercise-results of a randomized controlled trial. Mod. Rheumatol. 2017, 27, 493–502. [Google Scholar] [CrossRef] [PubMed]
- Svege, I.; Fernandes, L.; Nordsletten, L.; Holm, I.; Risberg, M.A. Long-term effect of exercise therapy and patient education on impairments and activity limitations in people with hip osteoarthritis: Secondary outcome analysis of a randomized clinical trial. Phys. Ther. 2016, 96, 818–827. [Google Scholar] [CrossRef] [Green Version]
- Villadsen, A.; Overgaard, S.; Holsgaard-Larsen, A.; Christensen, R.; Roos, E.M. Immediate efficacy of neuromuscular exercise in patients with severe osteoarthritis of the hip or knee: A secondary analysis from a randomized controlled trial. J. Rheumatol. 2014, 41, 1385–1394. [Google Scholar] [CrossRef] [PubMed]
- Hermann, A.; Holsgaard-Larsen, A.; Zerahn, B.; Mejdahl, S.; Overgaard, S. Preoperative progressive explosive-type resistance training is feasible and effective in patients with hip osteoarthritis scheduled for total hip arthroplasty–a randomized controlled trial. Osteoarthr. Cart. 2016, 24, 91–98. [Google Scholar] [CrossRef] [Green Version]
- Bieler, T.; Kristensen, A.L.R.; Nyberg, M.; Magnusson, S.P.; Kjaer, M.; Beyer, N. Exercise in patients with hip osteoarthritis–effects on muscle and functional performance: A randomized trial. Physiother. Theory Pract. 2021, 1–12. [Google Scholar] [CrossRef]
- Frontera, W.R.; Meredith, C.N.; O’Reilly, K.P.; Knuttgen, H.G.; Evans, W.J. Strength conditioning in older men: Skeletal muscle hypertrophy and improved function. J. Appl. Physiol. 1988, 64, 1038–1044. [Google Scholar] [CrossRef]
- Fry, A.C. The role of resistance exercise intensity on muscle fibre adaptations. Sports Med. 2004, 34, 663–679. [Google Scholar] [CrossRef] [PubMed]
- Rhea, M.R.; Alvar, B.A.; Burkett, L.N.; Ball, S.D. A meta-analysis to determine the dose response for strength development. Med. Sci. Sports Exerc. 2003, 35, 456–464. [Google Scholar] [CrossRef] [PubMed]
- Rostron, Z.P.J.; Green, R.; Kingsley, M.; Zacharias, A. Associations between measures of physical activity and muscle size and strength: A systematic review. Arch. Rehabil. Res. Clin. Transl. 2021, 3, 100124. [Google Scholar] [CrossRef] [PubMed]
- Semciw, A.I.; Green, R.A.; Murley, G.S.; Pizzari, T. Gluteus minimus: An intramuscular EMG investigation of anterior and posterior segments during gait. Gait Posture 2014, 39, 822–826. [Google Scholar] [CrossRef] [Green Version]
- Semciw, A.I.; Pizzari, T.; Murley, G.S.; Green, R.A. Gluteus medius: An intramuscular EMG investigation of anterior, middle and posterior segments during gait. J. Electromyogr. Kinesiol. 2013, 23, 858–864. [Google Scholar] [CrossRef] [Green Version]
- Fernandopulle, S.; Perry, M.; Manlapaz, D.; Jayakaran, P. Effect of land-based generic physical activity interventions on pain, physical function, and physical performance in hip and knee osteoarthritis: A systematic review and meta-analysis. Am. J. Phys. Med. Rehabil. 2017, 96, 773–792. [Google Scholar] [CrossRef]
- Pisters, M.F.; Veenhof, C.; Schellevis, F.G.; Twisk, J.W.; Dekker, J.; De Bakker, D.H. Exercise adherence improving long-term patient outcome in patients with osteoarthritis of the hip and/or knee. Arthritis Care Res. 2010, 62, 1087–1094. [Google Scholar] [CrossRef] [Green Version]
- Goh, S.-L.; Persson, M.S.; Stocks, J.; Hou, Y.; Lin, J.; Hall, M.C.; Doherty, M.; Zhang, W. Efficacy and potential determinants of exercise therapy in knee and hip osteoarthritis: A systematic review and meta-analysis. Ann. Phys. Rehabil. Med. 2019, 62, 356–365. [Google Scholar] [CrossRef]
- Steib, S.; Schoene, D.; Pfeifer, K. Dose-response relationship of resistance training in older adults: A meta-analysis. Med. Sci. Sports. Exerc. 2010, 42, 902–914. [Google Scholar] [CrossRef]
- Faber, J.; Fonseca, L.M. How sample size influences research outcomes. Dental Press J. Orthod. 2014, 19, 27–29. [Google Scholar] [CrossRef]
- Dettori, J.R. Loss to follow-up. Evid. Based Spine Care J. 2011, 2, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
| Concepts | Population | Intervention | Body Region |
|---|---|---|---|
| Keywords | [Osteoarthritis] | [Rehabilitation] | [Hip] |
| OA | Physical therapy | ||
| [Arthritis] | Physiotherapy | ||
| Arth * | [Exercise] |
| No. | Criteria |
|---|---|
| 1 | Must be in the English language |
| 2 | Must include human participants |
| 3 | Must include participants with hip OA (exclude juvenile idiopathic arthritis, femoroacetabular impingement, post hip arthroplasty, secondary OA, and dysplasia) |
| 4 | Must report on outcome variable of interest (i.e., muscle function or muscle size) |
| 5 | Must report on intervention of interest >6 weeks (rehabilitation/exercise program) |
| 6 | Must include original data of a peer-reviewed published paper (not conference proceedings, letters to the editor, or reviews) |
| Rehabilitation Program | Classification Criteria |
|---|---|
| High-intensity resistance | Identified by resistance exercises involving a combination of body weight, externally weighted exercises, and elastic bands. The applied resistance during the main conditioning phase for higher intensity is ≥70% 1RM or multiple sets of <12 repetition range. |
| Low-intensity resistance | Identified by resistance exercises involving a combination of body weight, externally weighted exercises, and elastic bands. The applied resistance during the main conditioning phase for higher intensity is <70% 1RM or multiple sets of ≥12 repetition range. |
| Aerobic | Any other activity incorporating large body movements sustained for >10 min that aim to increase heartrate and oxygen uptake, excluding water-based exercises. |
| Multimodal | Exercise program that includes a combination of rehabilitation programs (e.g., hydrotherapy and low-intensity resistance). |
| Author | Participants | Intervention Duration | Comparison Groups (Classification Used in This Review) | Outcome Measures of Interest | Comparison; Effect Size SMD [95% CI] (Follow-Up Time Point; ST: 6–13, IT: 13–24, and LT: >24) | ||
|---|---|---|---|---|---|---|---|
| Bennell et al. (2014) [19] | Hip OA: mixed unilateral and bilateral Group 1 N = 49 (26F, 23M) Group 2 N = 53 (36F, 17M) Mean age: Group 1: 64.5 ± 8.6 Group 2: 62.7 ± 6.4 | 12 weeks | Group 1—Low-intensity resistance exercise: Manual therapy (hip thrust manipulation, hip lumbar spine mobilisation, deep tissue massage, and muscle stretches), home exercises 4 times per week including HAbd strengthening (progressed through supine, standing, side lying, and standing wall press; 3 × 10 repetitions) and quadriceps strengthening (progressed through sitting elastic band press or KExt, partial squats, partial wall squats, sit-to stand and split sit to stand), balance and gait exercises Group 2—Control: Sham—No exercise instructions, inactive ultrasound | Hand-held dynamometer Isometric strength (Nm/kg): Unilateral hip strength (HAbd, HExt, HFlex, HIR, and HER) 1 Unilateral knee strength (KFlex and KExt) 1 | Low-intensity resistance vs. control (positive—favours low-intensity resistance): | ||
| ST (week 13) 2 | IT | LT | |||||
| HAbd: 0.13 [−0.28, 0.54] HExt: 0.32 [−0.09, 0.74] HFlex: −0.13 [−0.54, 0.28] HlR: −0.05 [−0.46, 0.36] HER: 0.28 [−0.13, 0.70] KExt: 0.07 [−0.34, 0.48] KFlex: 0.19 [−0.23, 0.60] | |||||||
| Bieler et al. (2018) [36] | Hip OA: mixed unilateral and bilateral Group 1 N = 50 (34F, 16M) Group 2 N = 50 (33F, 17M) Group 3 N = 52 (36F, 16M) Mean age: Group 1: 69.6 ± 5.4 Group 2: 70.0 ± 6.3 Group 3: 69.3 ± 6.4 | 16 weeks | Group 1—High-intensity resistance exercise: Strength training—progressive in fitness centre with 3 mandatory resistance exercise machines; 1, leg press; 2, seated KExt; 3, standing HExt. Mixture of unilateral and bilateral exercises. 75% of 1RM for 10 repetitions × 4 sets Group 2—Aerobic exercise: 2 Nordic walking—12–14 on Borg scale (6–20) Group 3—Low-intensity resistance exercise: Unsupervised home-based exercises—hip ROM, stretching and strengthening exercises for the lower extremities using body weight and elastic bands for resistance | Good strength device (Ver 3.14) Isometric strength (Nm): Unilateral knee strength (KFlex and KExt) Hand-held dynamometer Isometric strength (Nm): Unilateral hip strength (HIR, HER, HFlex, HAbd, and HAdd) | High-intensity resistance vs. low-intensity resistance (positive—favours high-intensity resistance): | ||
| ST (week 8) | IT (week 16) 3 | LT (week 52) 3 | |||||
| KExt: 0.10 [−0.31, 0.50] KFlex: −0.04 [−0.45, 0.36] 2 HER: −0.05 [−0.45, 0.36] 2 HIR: −0.13 [−0.54, 0.28] 2 HFlex: 0.00 [−0.40, 0.41] HAbd: −0.05 [−0.46, 0.36] HAdd: −0.12 [−0.52, 0.29] 2 | KExt: 0.11 [−0.30, 0.53] KFlex: −0.05 [−0.46, 0.37] HER: 0.00 [−0.41, 0.41] HIR: −0.15 [−0.57, 0.26] HFlex: −0.04 [−0.46, 0.37] HAbd: −0.04 [−0.45, 0.38] HAdd: −0.15 [−0.56, 0.27] | KExt: −0.01 [−0.47, 0.45] KFlex: −0.24 [−0.70, 0.22] HER: −0.29 [−0.75, 0.18] HIR: −0.33 [−0.80, 0.13] HFlex: −0.23 [−0.69, 0.23] HAbd: −0.19 [−0.65, 0.27] HAdd: −0.32 [−0.78, 0.15] | |||||
| High-intensity resistance vs. aerobic (positive—favours high-intensity resistance): | |||||||
| ST (week 8) | IT (week 16) 3 | LT (week 52) 3 | |||||
| KExt: 0.22 [−0.21, 0.65] KFlex: 0.10 [−0.33, 0.53] 2 HER: −0.05 [−0.48, 0.38] 2 HIR: −0.12 [−0.55, 0.31] 2 HFlex: −0.17 [−0.60, 0.26] HAbd: −0.16 [−0.59, 0.27] HAdd: −0.15 [−0.58, 0.28] 2 | KExt: 0.10 [−0.34, 0.54] KFlex: −0.13 [−0.57, 0.31] HER: −0.21 [−0.65, 0.23] HIR: −0.32 [−0.76, 0.12] HFlex: −0.21 [−0.65, 0.22] HAbd: −0.32 [−0.77, 0.12] HAdd: −0.20 [−0.64, 0.26] | KExt: −0.02 [−0.49, 0.46] KFlex: −0.29 [−0.77, 0.19] HER: −0.34 [−0.82, 0.14] HIR: −0.51 [−1.00, −0.03] HFlex: −0.33 [−0.81, 0.15] HAbd: −0.36 [−0.85, 0.12] HAdd: −0.34 [−0.82, 0.14] | |||||
| Low-intensity resistance vs. aerobic (positive—favours low-intensity resistance): | |||||||
| ST (week 8) 2 | IT (week 16) 3 | LT (week 52) 3 | |||||
| KExt: 0.13 [−0.31, 0.56] KFlex: 0.14 [−0.30, 0.57] HER: 0.00 [−0.43, 0.43] HIR: 0.01 [−0.42, 0.45] HFlex: −0.16 [−0.60, 0.27] HAbd: −0.10 [−0.53, 0.34] HAdd: −0.02 [−0.46, 0.42] | KExt: −0.02 [−0.47, 0.43] KFlex: −0.08 [−0.53, 0.37] HER: −0.18 [−0.63, 0.26] HIR: −0.14 [−0.59, 0.31] HFlex: −0.16 [−0.61, 0.29] HAbd: −0.25 [−0.70, 0.20] HAdd: −0.03 [−0.49, 0.42] | KExt: −0.00 [−0.50, 0.50] KFlex: −0.05 [−0.55, 0.45] HER: −0.04 [−0.54, 0.46] HIR: −0.15 [−0.65, 0.35] HFlex: −0.11 [−0.61, 0.39] HAbd: −0.12 [−0.62, 0.38] HAdd: 0.01 [−0.49, 0.51] | |||||
| Bieler et al. (2021) [43] | Hip OA: mixed unilateral and bilateral Group 1 N = 15 (11F, 4M) Group 2 N = 12 (8F, 4M) Group 3 N = 15 (11F, 4M) Mean age: Group 1: 67.1 ± 3.9 Group 2: 69.1 ± 5.1 Group 3: 67.5 ± 5.2 | 16 weeks | Same participants as Bieler et al. (2018) [36] Only muscle size data used | MRI Cross sectional area (CSAcm2): Unilateral quads 1 | High-intensity resistance vs. low-intensity resistance (positive—favours high-intensity resistance) | ||
| ST | IT (16 weeks) | LT | |||||
| Quads: −0.02 [−0.74, 0.69] | |||||||
| High-intensity resistance vs. aerobic (positive—favours high-intensity resistance): | |||||||
| ST | IT (16 weeks) 2 | LT | |||||
| Quads: 0.06 [−0.70, 0.82] | |||||||
| Low-intensity resistance vs. aerobic (positive—favours low-intensity resistance): | |||||||
| ST | IT (16 weeks) 2 | LT | |||||
| Quads: 0.09 [−0.67, 0.85] | |||||||
| Chopp-Hurley et al. (2017) [37] | Hip and knee OA: mixed unilateral and bilateral Group 1 N = 12 (10F, 2M) Group 2 N = 12 (9F, 3M) Mean age: Group 1: 52.8 ± 6.4 Group 2: 54.9 ± 6.7 | 12 weeks | Group 1—High-intensity resistance exercise: Exercise classes within a sports and recreation facility incorporating static lower limb strengthening exercise, e.g., squats and lunges to elicit moderate activity in lower limb muscles, progressed over time Group 2—Control: No exercise | Fixed dynamometer Isometric strength (Nm/kg): Unilateral knee strength (KFlex and KExt) 1 Unilateral hip strength (HFlex and HExt) 1 | ST (week 12) 4 | IT | LT |
| KExt: Group 1: 1.9 ± 0.5, Group 2: 1.6 ± 0.5 KFlex: Group 1: 0.7 ± 0.3, Group 2: 0.9 ± 0.3 HExt: Group 1: 1.4 ± 0.5, Group 2: 1.4 ± 0.7 HFlex: Group 1:0.9 ± 0.3, Group 2: 1.0 ± 0.3 | |||||||
| Fukumoto et al. 5 (2014) [29] | Hip OA: mixed unilateral and bilateral Total N = 46 (46F) Group 1 N = 19 Group 2 N = 20 Mean age: Group 1: 52.4 ± 9.2 Group 2: 52.5 ± 10.1 | 8 weeks | Both groups: daily home-based resistance training programs using elastic bands completing HAbd, HExt, HFlex, and KExt In addition, participants in the high-velocity group were instructed to perform the concentric phase of each repetition as rapidly as possible and then return through the eccentric phase in 3 s. Participants in the low-velocity group performed both the concentric and eccentric phases in 3 s Group 1—High-intensity resistance exercise: High velocity training—concentric phase of each movement as fast as possible and a slow eccentric phase total time = 3 s Group 2—Low-intensity resistance exercise: Low velocity training—completing concentric (3 s) and eccentric phases (3 s) | Hand-held dynamometer Isometric strength (Nm/kg): Unilateral hip strength (HExt, HFlex, and HAbd) 1 Unilateral knee strength (KExt) 1 B-mode ultrasound Muscle thickness (cm): Unilateral GMax, GMed, and Quads 1 | High-intensity resistance vs. low-intensity resistance (positive—favours high-intensity resistance): | ||
| ST (week 8) | IT | LT | |||||
| HAbd: −0.18 [−0.81, 0.45] HExt: −0.24 [−0.87, 0.39] HFlex: −0.25 [−0.88, 0.38] KExt: −0.26 [−0.89, 0.37] GMax: 0.22 [−0.41, 0.85] 6 GMed: 0.10 [−0.53, 0.72] 6 Quads: −0.11 [−0.74, 0.52] | |||||||
| Green et al. (1993) [23] | Hip OA: mixed unilateral and bilateral Group 1 N = 24 (18F, 6M) Group 2 N = 23 (17F, 6M) Mean age: Group 1: 65.7 Group 2: 68.0 | 6 weeks | Group 1—Multimodal exercise: Hydrotherapy with home-based exercises Group 2—Low-intensity resistance exercise: Home-based exercise made up of body weight and joint mobility exercises | Computerised dynamometer Isometric strength (N): Unilateral hip strength (HExt and HAbd) 1 | Low-intensity resistance vs. multimodal (positive—favours low-intensity resistance): | ||
| ST (week 12) 2 | IT | LT | |||||
| HExt: −0.29 [−0.86, 0.29] HAbd: −0.67 [−1.26, 0.08] | |||||||
| Hermann et al. (2020) [42] | Hip OA Group 1 N = 40 (27F, 13M) Group 2 N = 40 (25F, 15M) Mean age: Group 1: 70.0 ± 7.7 Group 2: 70.8 ± 7.5 | 10 weeks | Group 1—High intensity resistance exercise: One hour supervised pre-operative progressive explosive unilateral resistance exercises including HExt, KExt, KFlex, and seated leg press. Exercise was performed explosively, with participants instructed to complete the concentric phase “as fast as possible” and the eccentric phase over “2–3 s” Group 2—Control Care as usual, no prescribed supervised exercise program | Nottingham power rig Isometric power (Watt/kg): Unilateral lower limb power (KExt) | High-intensity resistance vs. control (positive—favours high-intensity resistance): | ||
| ST (week 10) | IT | LT | |||||
| KExt 0.71 [0.25, 1.16] | |||||||
| Jigami et al. (2012) [38] | Hip OA: mixed unilateral and bilateral—tested worse side (WS) and better side (BS) Group 1 N = 15F Group 2 N = 14F Mean age: Group 1: 60.8 ± 8.8 Group 2: 65.6 ± 7.8 | (10 sessions for both groups) 10 weeks 20 weeks | Multimodal exercise: Land-based and aquatic exercises comprised of body weight exercises and stretching with aquatic muscle strengthening, whole body co-ordination and muscle relaxation Group 1: Fortnightly Group 2: Weekly | Hand-held dynamometer Peak force (kg): Unilateral hip peak force (HFlex, HExt and HAbd) Unilateral knee peak force (KFlex and KExt) | ST (week 10) 2 | IT (week 20) 2 | LT |
| HFlex: WS: 20.1 ± 4.9, BS: 21.3 ± 5.8 HExt: WS: 19.9 ± 4.6, BS: 21.5 ± 5.4 HAbd: WS: 22.7 ± 3.6, BS: 22.2 ± 4.3 KFlex: WS: 13.3 ± 2.8, BS: 14.4 ± 2.3 KExt: WS: 29.4 ± 5.3, BS: 30.7 ± 6.0 | HFlex: WS: 13.3 ± 3.5, BS: 15.2 ± 4.7 HExt: WS: 14.8 ± 5.2, BS: 17.1 ± 4.9 HAbd: WS: 15.5 ± 4.4, BS: 14.6 ± 4.8 KFlex: WS: 12.2 ± 6.7, BS: 12.9 ± 4.5 KExt: WS: 21.7 ± 8.2. BS: 22.7 ± 9.2 | ||||||
| Steinhilber et al. (2017) [39] | Hip OA: mixed unilateral and bilateral Group 1 N = 70 7 Group 2 N = 68 7 Group 3 N = 70 7 Mean age: Group 1: 58 ± 19 Group 2: 60 ± 9 Group 3: 58 ± 10 | 12 weeks | Group 1—High-intensity resistance exercise: THu¨Ko exercise therapy—a progressive exercise program with a mixture of mobilisation, physical perception of movements, balance, and strengthening of hip muscles using basic exercise equipment, e.g., elastic bands, weight cuffs to a 15 on the Borg scale Group 2—Control: Non-treated control group Group 3—Placebo: 2 Ultrasound group—ultrasound machine invisibly turned off | Isomed 200 isokinetic dynamometer Isometric hip strength (Nm/kg): Bilateral hip strength (HAbd, HAdd, HFlex, and HExt) 8 | High-intensity resistance vs. control (positive—favours high-intensity resistance): | ||
| ST (week 12) | IT | LT | |||||
| HAbd: 0.33 [−0.01, 0.67] HAdd: 0.38 [0.04, 0.71] 2 HFlex: 0.36 [0.02, 0.69] HExt: 0.40 [0.07, 0.74] | |||||||
| Svege et al. (2016) [40] | Hip OA: mixed unilateral and bilateral Group 1 N = 55 (31F, 24M) Group 2 N = 54 (28F, 26M) Mean age: Group 1: 58.4 ± 10.0 Group 2: 57.2 ± 9.8 | 12 weeks | Group 1—High-intensity resistance exercise: Three exercise sessions x week of strengthening, functional and stretching exercises with 1 supervised by a physiotherapist—previously reported (70–80% 1RM) Group 2—Control: Patient education with list of exercises given to participants—3 sessions per week education with 8 week follow-up | Isokinetic dynamometer Isokinetic hip and knee strength (Nm): Unilateral hip strength (HFlex and HExt) Unilateral knee strength (KFlex and KExt) 1 | High-intensity resistance vs. control (positive—favours high-intensity resistance): | ||
| ST | IT (week 16) | LT (week 40) 3 | |||||
| KExt: 0.08 [−0.30, 0.45] KFlex: −0.07 [−0.45, 0.30] 2 HExt: −0.08 [−0.46, 0.29] HFlex: −0.01 [−0.38, 0.37] | KExt: −0.27 [−0.65, 0.11] KFlex: −0.27 [−0.64, 0.11] HExt: −0.37 [−0.75, 0.01] HFlex: −0.42 [−0.80, −0.04] | ||||||
| Villadsen et al. (2014) [41] | Hip and Knee OA (used only Hip OA data) Group 1 N = 43 (22F, 21M) Group 2 N = 41 (21F, 20M) Mean age: Group 1: 68.7 ± 8.4 Group 2: 68.6 ± 7.1 | 8 weeks | Group 1—High-intensity resistance exercise: NEMEX-TJR twice a week for 1 h supervised by physiotherapist and educational program Group 2—Control: Education program, written information provided | Muscle lab power, Ergo test. Unilateral lower limb muscle power (W): Unilateral KExt, HExt, and HAbd 1 | High-intensity resistance vs. control (positive—favours high-intensity resistance): | ||
| ST (week 8) | IT | LT | |||||
| KExt: 0.08 [−0.35, 0.51] HExt: 0.37 [−0.06, 0.80] HAbd: 0.18 [−0.24, 0.61] | |||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rostron, Z.P.J.; Green, R.A.; Kingsley, M.; Zacharias, A. Efficacy of Exercise-Based Rehabilitation Programs for Improving Muscle Function and Size in People with Hip Osteoarthritis: A Systematic Review with Meta-Analysis. Biology 2021, 10, 1251. https://doi.org/10.3390/biology10121251
Rostron ZPJ, Green RA, Kingsley M, Zacharias A. Efficacy of Exercise-Based Rehabilitation Programs for Improving Muscle Function and Size in People with Hip Osteoarthritis: A Systematic Review with Meta-Analysis. Biology. 2021; 10(12):1251. https://doi.org/10.3390/biology10121251
Chicago/Turabian StyleRostron, Zachary P. J., Rodney A. Green, Michael Kingsley, and Anita Zacharias. 2021. "Efficacy of Exercise-Based Rehabilitation Programs for Improving Muscle Function and Size in People with Hip Osteoarthritis: A Systematic Review with Meta-Analysis" Biology 10, no. 12: 1251. https://doi.org/10.3390/biology10121251
APA StyleRostron, Z. P. J., Green, R. A., Kingsley, M., & Zacharias, A. (2021). Efficacy of Exercise-Based Rehabilitation Programs for Improving Muscle Function and Size in People with Hip Osteoarthritis: A Systematic Review with Meta-Analysis. Biology, 10(12), 1251. https://doi.org/10.3390/biology10121251