
Shoulder Positioning during Superior Capsular Reconstruction: Computational Analysis of Graft Integrity and Shoulder Stability

 , , and
, , and {kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:Simple Summary
Abstract
1. Introduction
2. Materials and Methods
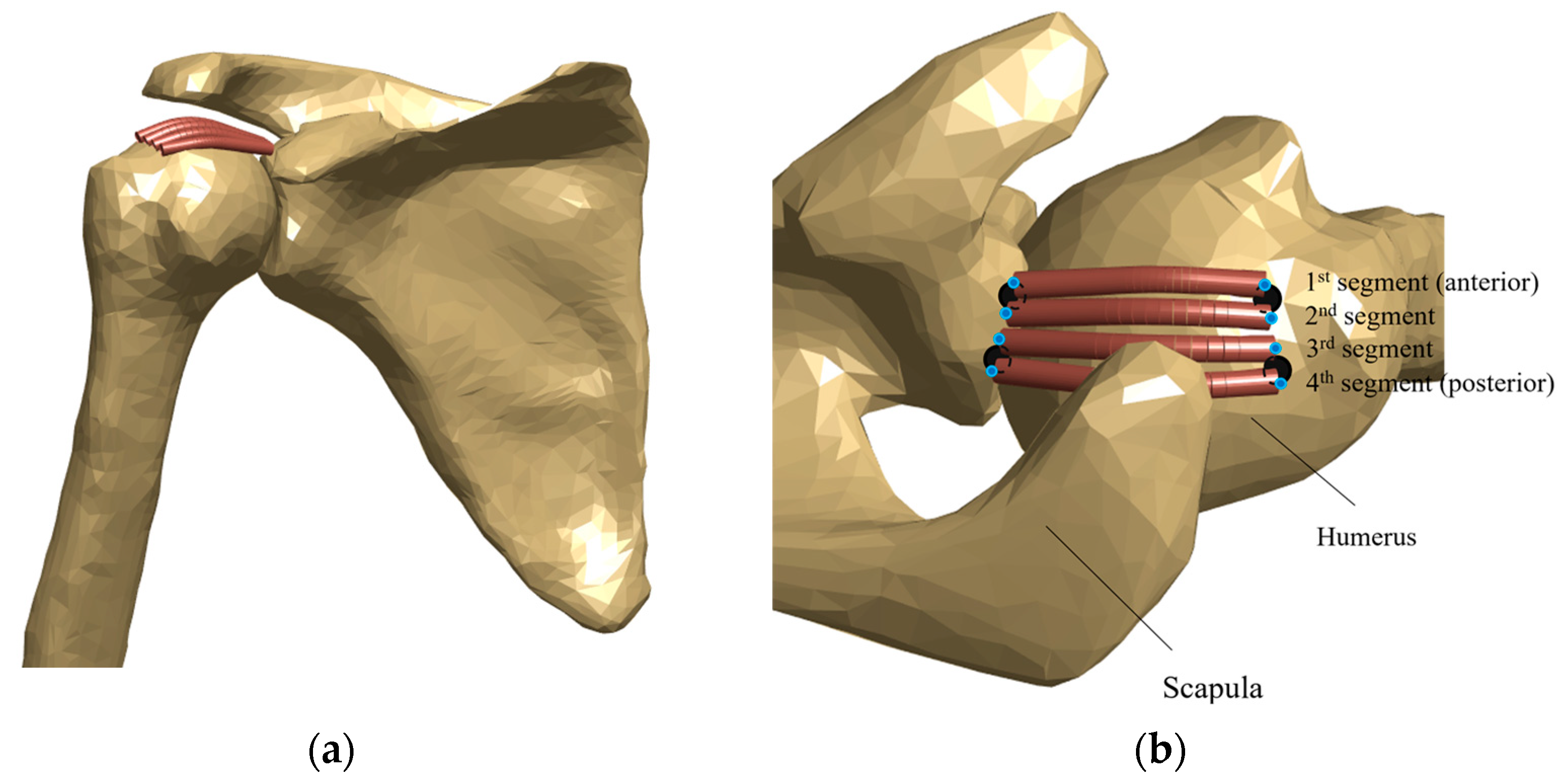
2.1. Computational Modelling
2.2. Shoulder Positions
2.3. Musculoskeletal Simulations
2.4. Biomechanical Evaluation of ASCR
2.5. Statistical Analysis
3. Results
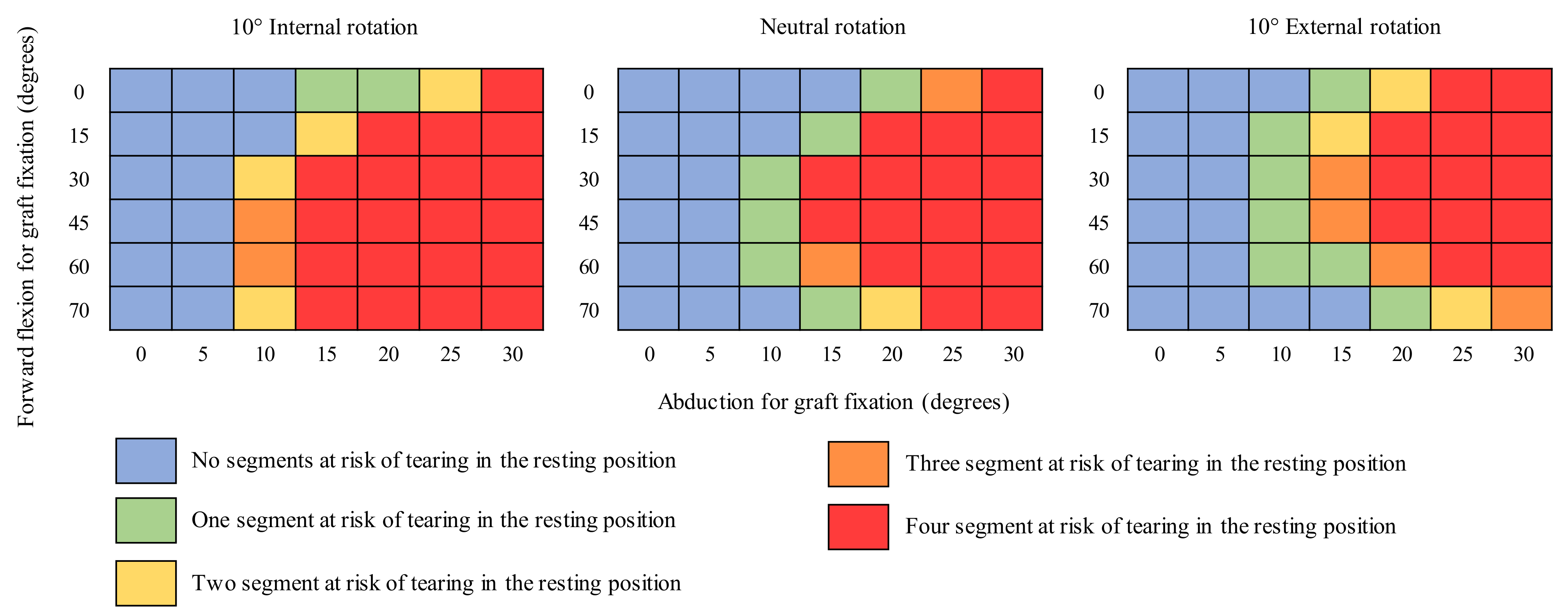
3.1. Risk of Tear
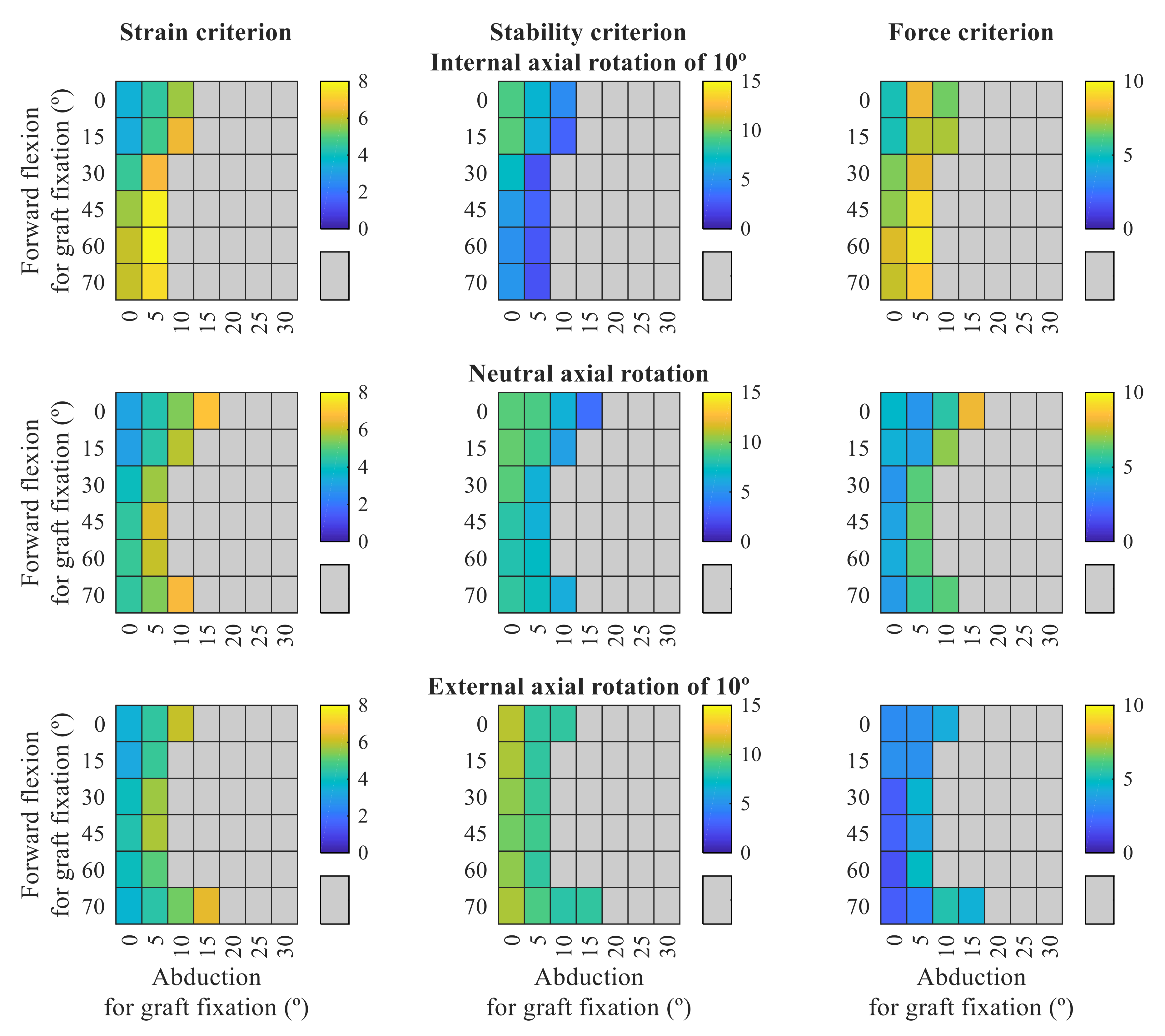
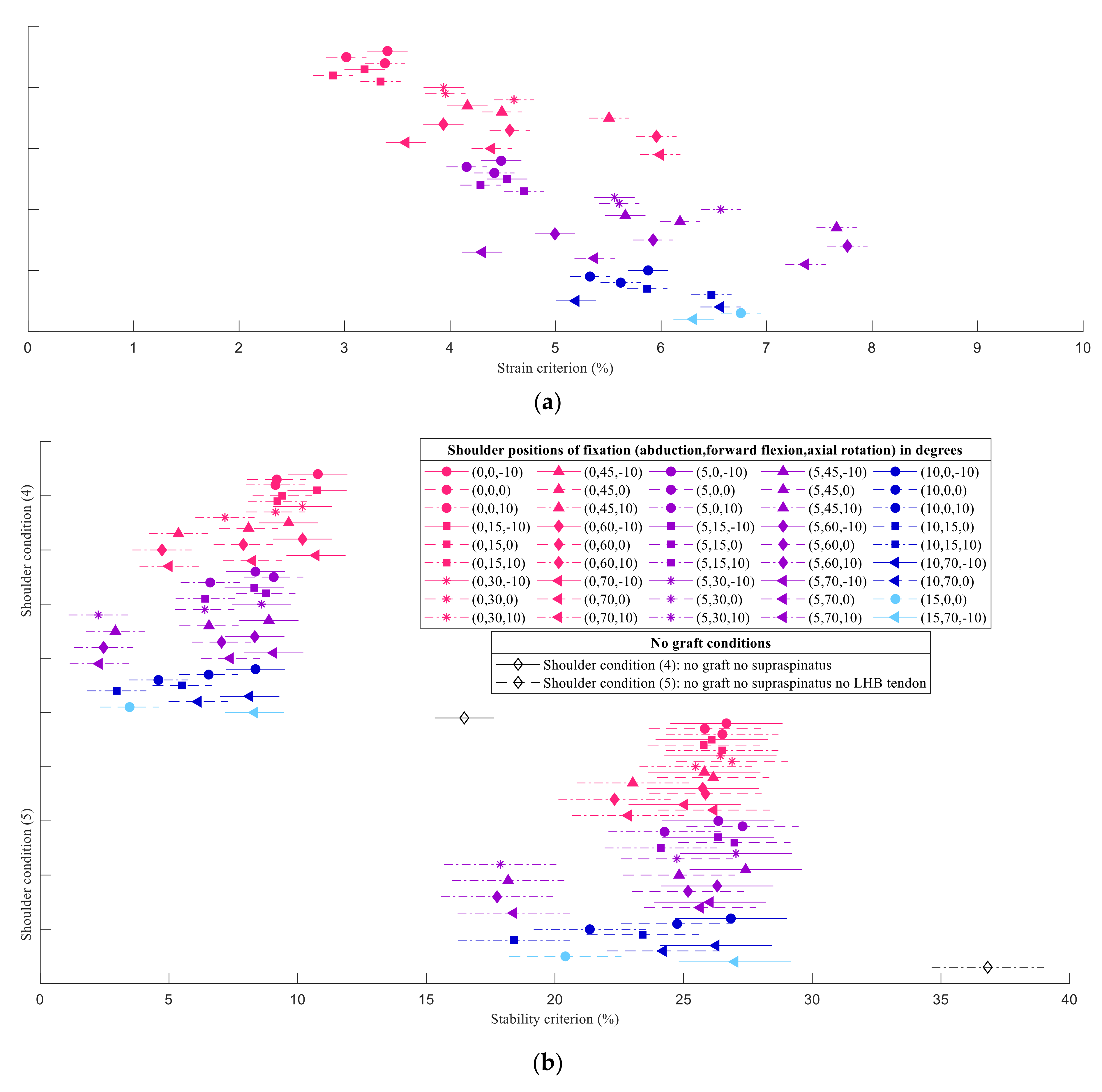
3.2. Biomechanical Performance of ASCR
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Terry, G.C.; Chopp, T.M. Functional Anatomy of the Shoulder. J. Athl. Train. 2000, 35, 248–255. [Google Scholar] [CrossRef] [Green Version]
- Veeger, H.E.J.; van der Helm, F.C.T. Shoulder Function: The Perfect Compromise between Mobility and Stability. J. Biomech. 2007, 40, 2119–2129. [Google Scholar] [CrossRef]
- Wilk, K.E.; Arrigo, C.A.; Andrews, J.R. Current Concepts: The Stabilizing Structures of the Glenohumeral Joint. J. Orthop. Sports Phys. Ther. 1997, 25, 364–379. [Google Scholar] [CrossRef] [Green Version]
- Habermeyer, P.; Schuller, U.; Wiedemann, E. The Intra-Articular Pressure of the Shoulder: An Experimental Study on the Role of the Glenoid Labrum in Stabilizing the Joint. Arthrosc. J. Arthrosc. Relat. Surg. 1992, 8, 166–172. [Google Scholar] [CrossRef]
- Lugo, R.; Kung, P.; Ma, C.B. Shoulder Biomechanics. Eur. J. Radiol. 2008, 68, 16–24. [Google Scholar] [CrossRef] [PubMed]
- Adams, C.R.; DeMartino, A.M.; Rego, G.; Denard, P.J.; Burkhart, S.S. The Rotator Cuff and the Superior Capsule: Why We Need Both. Arthrosc. J. Arthrosc. Relat. Surg. 2016, 32, 2628–2637. [Google Scholar] [CrossRef]
- Nimura, A.; Kato, A.; Yamaguchi, K.; Mochizuki, T.; Okawa, A.; Sugaya, H.; Akita, K. The Superior Capsule of the Shoulder Joint Complements the Insertion of the Rotator Cuff. J. Shoulder Elb. Surg. 2012, 21, 867–872. [Google Scholar] [CrossRef]
- Cain, P.R.; Mutschler, T.A.; Fu, F.H.; Lee, S.K. Anterior Stability of the Glenohumeral Joint: A Dynamic Model. Am. J. Sports Med. 1987, 15, 144–148. [Google Scholar] [CrossRef] [PubMed]
- Terry, G.C.; Hammon, D.; France, P.; Norwood, L.A. The Stabilizing Function of Passive Shoulder Restraints. Am. J. Sports Med. 1991, 19, 26–34. [Google Scholar] [CrossRef]
- Abboud, J.A.; Soslowsky, L.J. Interplay of the Static and Dynamic Restraints in Glenohumeral Instability. Clin. Orthop. Relat. Res. 2002, 400, 48–57. [Google Scholar] [CrossRef]
- Cvetanovich, G.L.; Waterman, B.R.; Verma, N.N.; Romeo, A.A. Management of the Irreparable Rotator Cuff Tear. J. Am. Acad. Orthop. Surg. 2019, 27, 909–917. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.H.; Park, M.S.; Rhee, S.M. Treatment Strategy for Irreparable Rotator Cuff Tears. CiOS Clin. Orthop. Surg. 2018, 10, 119–134. [Google Scholar] [CrossRef] [PubMed]
- Dang, A.; Davies, M. Rotator Cuff Disease: Treatment Options and Considerations. Sports Med. Arthrosc. Rev. 2018, 26, 129–133. [Google Scholar] [CrossRef]
- Dimock, R.A.C.; Malik, S.; Consigliere, P.; Imam, M.A.; Ali Narvani, A. Superior Capsule Reconstruction: What Do We Know? Arch. Bone Jt. Surg. 2019, 7, 3–11. [Google Scholar] [CrossRef]
- Mihata, T.; McGarry, M.H.; Pirolo, J.M.; Kinoshita, M.; Lee, T.Q. Superior Capsule Reconstruction to Restore Superior Stability in Irreparable Rotator Cuff Tears: A Biomechanical Cadaveric Study. Am. J. Sports Med. 2012, 40, 2248–2255. [Google Scholar] [CrossRef]
- Mihata, T.; Lee, T.Q.; Watanabe, C.; Fukunishi, K.; Ohue, M.; Tsujimura, T.; Kinoshita, M. Clinical Results of Arthroscopic Superior Capsule Reconstruction for Irreparable Rotator Cuff Tears. Arthrosc. J. Arthrosc. Relat. Surg. 2013, 29, 459–470. [Google Scholar] [CrossRef]
- Hirahara, A.M.; Adams, C.R. Arthroscopic Superior Capsular Reconstruction for Treatment of Massive Irreparable Rotator Cuff Tears. Arthrosc. Tech. 2015, 4, e637–e641. [Google Scholar] [CrossRef] [PubMed]
- Walch, G.; Edwards, T.B.; Boulahia, A.; Nové-Josserand, L.; Neyton, L.; Szabo, I. Arthroscopic Tenotomy of the Long Head of the Biceps in the Treatment of Rotator Cuff Tears: Clinical and Radiographic Results of 307 Cases. J. Shoulder Elb. Surg. 2005, 14, 238–246. [Google Scholar] [CrossRef]
- de Campos Azevedo, C.I.; Ângelo, A.C.L.P.G.; Vinga, S. Arthroscopic Superior Capsular Reconstruction With a Minimally Invasive Harvested Fascia Lata Autograft Produces Good Clinical Results. Orthop. J. Sports Med. 2018, 6, 2325967118808242. [Google Scholar] [CrossRef] [Green Version]
- Desai, S.S.; Mata, H.K. Long Head of Biceps Tendon Pathology and Results of Tenotomy in Full-Thickness Reparable Rotator Cuff Tear. Arthrosc. J. Arthrosc. Relat. Surg. 2017, 33, 1971–1976. [Google Scholar] [CrossRef]
- Altintas, B.; Scheidt, M.; Kremser, V.; Boykin, R.; Bhatia, S.; Sajadi, K.R.; Mair, S.; Millett, P.J. Superior Capsule Reconstruction for Irreparable Massive Rotator Cuff Tears: Does It Make Sense? A Systematic Review of Early Clinical Evidence. Am. J. Sports Med. 2020, 48, 3365–3375. [Google Scholar] [CrossRef] [PubMed]
- Denard, P.J.; Brady, P.C.; Adams, C.R.; Tokish, J.M.; Burkhart, S.S. Preliminary Results of Arthroscopic Superior Capsule Reconstruction with Dermal Allograft. Arthrosc. J. Arthrosc. Relat. Surg. 2018, 34, 93–99. [Google Scholar] [CrossRef]
- Lim, S.; AlRamadhan, H.; Kwak, J.M.; Hong, H.; Jeon, I.H. Graft Tears after Arthroscopic Superior Capsule Reconstruction (ASCR): Pattern of Failure and Its Correlation with Clinical Outcome. Arch. Orthop. Trauma Surg. 2019, 139, 231–239. [Google Scholar] [CrossRef] [PubMed]
- de Campos Azevedo, C.I.; Ângelo, A.C.L.P.G.; Campos-Correia, D.; Delgado, L.; Ferreira, N.; Sevivas, N. Clinical Importance of Graft Integrity in Arthroscopic Superior Capsular Reconstruction Using a Minimally Invasively Harvested Midthigh Fascia Lata Autograft: 3-Year Clinical and Magnetic Resonance Imaging Outcomes. Am. J. Sports Med. 2020, 48, 2115–2128. [Google Scholar] [CrossRef] [PubMed]
- de Campos Azevedo, C.I.; Andrade, R.; Leiria Pires Gago Ângelo, A.C.; Espregueira-Mendes, J.; Ferreira, N.; Sevivas, N. Fascia Lata Autograft Versus Human Dermal Allograft in Arthroscopic Superior Capsular Reconstruction for Irreparable Rotator Cuff Tears: A Systematic Review of Clinical Outcomes. Arthrosc. J. Arthrosc. Relat. Surg. 2020, 36, 579–591.e2. [Google Scholar] [CrossRef]
- Mihata, T.; McGarry, M.H.; Kahn, T.; Goldberg, I.; Neo, M.; Lee, T.Q. Biomechanical Effect of Thickness and Tension of Fascia Lata Graft on Glenohumeral Stability for Superior Capsule Reconstruction in Irreparable Supraspinatus Tears. Arthrosc. J. Arthrosc. Relat. Surg. 2016, 32, 418–426. [Google Scholar] [CrossRef]
- Adams, C.R.; Comer, B.; Scheiderer, B.; Imhoff, F.B.; Morikawa, D.; Kia, C.; Muench, L.N.; Baldino, J.B.; Mazzocca, A.D. The Effect of Glenohumeral Fixation Angle on Deltoid Function during Superior Capsule Reconstruction: A Biomechanical Investigation. Arthrosc. J. Arthrosc. Relat. Surg. 2020, 36, 400–408. [Google Scholar] [CrossRef] [PubMed]
- Hast, M.W.; Schmidt, E.C.; Kelly, J.D.; Baxter, J.R. Computational Optimization of Graft Tension in Simulated Superior Capsule Reconstructions. J. Orthop. Res. 2018, 36, 2789–2796. [Google Scholar] [CrossRef] [Green Version]
- Quental, C.; Folgado, J.; Ambrósio, J.; Monteiro, J. Critical Analysis of Musculoskeletal Modelling Complexity in Multibody Biomechanical Models of the Upper Limb. Comput. Methods Biomech. Biomed. Eng. 2015, 18, 749–759. [Google Scholar] [CrossRef]
- Quental, C.; Margarida, A.; Jorge, A.; Gonalves, S.B.; João, F. Influence of the Musculotendon Dynamics on the Muscle Force-Sharing Problem of the Shoulder-A Fully Inverse Dynamics Approach. J. Biomech. Eng. 2018, 140, 71005. [Google Scholar] [CrossRef]
- de Campos Azevedo, C.I.; Ângelo, A.C.L.P.G.; Quental, C.; Gonçalves, S.; Folgado, J.; Ferreira, N.; Sevivas, N. Proximal and Mid-Thigh Fascia Lata Graft Constructs Used for Arthroscopic Superior Capsule Reconstruction Show Equivalent Biomechanical Properties. An in Vitro Human Cadaver Study. JSES Int. 2021, 5, 439–446. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Lin, J.H.; McGorry, R.W. A Regression-Based 3-D Shoulder Rhythm. J. Biomech. 2014, 47, 1206–1210. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pashuck, T.D.; Hirahara, A.M.; Cook, J.L.; Cook, C.R.; Andersen, W.J.; Smith, M.J. Superior Capsular Reconstruction Using Dermal Allograft Is a Safe and Effective Treatment for Massive Irreparable Rotator Cuff Tears: 2-Year Clinical Outcomes. Arthrosc. J. Arthrosc. Relat. Surg. 2021, 37, 489–496.e1. [Google Scholar] [CrossRef] [PubMed]
- Stecco, C. Functional Atlas of the Human Fascial System, 1st ed.; Elsevier: Amsterdam, The Netherlands, 2015; ISBN 9780702063275. [Google Scholar]
- Otsuka, S.; Yakura, T.; Ohmichi, Y.; Ohmichi, M.; Naito, M.; Nakano, T.; Kawakami, Y. Site Specificity of Mechanical and Structural Properties of Human Fascia Lata and Their Gender Differences: A Cadaveric Study. J. Biomech. 2018, 77, 69–75. [Google Scholar] [CrossRef]
- Quental, C.; Folgado, J.; Ambrósio, J. A Window Moving Inverse Dynamics Optimization for Biomechanics of Motion. Multibody Syst. Dyn. 2016, 38, 157–171. [Google Scholar] [CrossRef]
- Klemt, C.; Nolte, D.; Grigoriadis, G.; di Federico, E.; Reilly, P.; Bull, A.M.J. The Contribution of the Glenoid Labrum to Glenohumeral Stability under Physiological Joint Loading Using Finite Element Analysis. Comput. Methods Biomech. Biomed. Eng. 2017, 20, 1613–1622. [Google Scholar] [CrossRef]
- Arora, J.S. Introduction to Optimum Design, 4th ed.; Elsevier: Amsterdam, The Netherlands, 2016; ISBN 9780128009185. [Google Scholar]
- Tukey, J.W. The Collected Works of John W. Tukey; Brillinger, D.R., Cox, D.R., Braun, H.I., Eds.; Taylor & Francis: Abingdon, UK, 1984; ISBN 0534033032. [Google Scholar]
- Steenbrink, F.; de Groot, J.H.; Veeger, H.E.J.; van der Helm, F.C.T.; Rozing, P.M. Glenohumeral Stability in Simulated Rotator Cuff Tears. J. Biomech. 2009, 42, 1740–1745. [Google Scholar] [CrossRef]
- Dyrna, F.; Berthold, D.P.; Muench, L.N.; Beitzel, K.; Kia, C.; Obopilwe, E.; Pauzenberger, L.; Adams, C.R.; Cote, M.P.; Scheiderer, B.; et al. Graft Tensioning in Superior Capsular Reconstruction Improves Glenohumeral Joint Kinematics in Massive Irreparable Rotator Cuff Tears A Biomechanical Study of the Influence of Superior Capsular Reconstruction on Dynamic Shoulder Abduction. Orthop. J. Sports Med. 2020, 8, 2325967120957424. [Google Scholar] [CrossRef]
- Itoi, E.; Kuechle, D.K.; Newman, S.R.; Morrey, B.F.; An, K.N. Stabilising Function of the Biceps in Stable and Unstable Shoulders. J. Bone Jt. Surg. Ser. B 1993, 75, 546–550. [Google Scholar] [CrossRef] [Green Version]
- Itoi, E.; Motzkin, N.E.; Morrey, B.F.; An, K.N. Stabilizing Function of the Long Head of the Biceps in the Hanging Arm Position. J. Shoulder Elb. Surg. 1994, 3, 135–142. [Google Scholar] [CrossRef]
- Kelkar, R.; Wang, V.M.; Flatow, E.L.; Newton, P.M.; Ateshian, G.A.; Bigliani, L.U.; Pawluk, R.J.; Mow, V.C. Glenohumeral Mechanics: A Study of Articular Geometry, Contact, and Kinematics. J. Shoulder Elb. Surg. 2001, 10, 73–84. [Google Scholar] [CrossRef]
- Rodosky, M.W.; Harner, C.D.; Fu, F.H. The Role of the Long Head of the Biceps Muscle and Superior Glenoid Labrum in Anterior Stability of the Shoulder. Am. J. Sports Med. 1994, 22, 121–130. [Google Scholar] [CrossRef] [PubMed]
- Sarmento, M. Long Head of Biceps: From Anatomy to Treatment. Acta Reumatol. Port. 2015, 2015, 26–33. [Google Scholar]
- Ahrens, P.M.; Boileau, P. The Long Head of Biceps and Associated Tendinopathy. J. Bone Jt. Surg. Ser. B 2007, 89, 1001–1009. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Elser, F.; Braun, S.; Dewing, C.B.; Giphart, J.E.; Millett, P.J. Anatomy, Function, Injuries, and Treatment of the Long Head of the Biceps Brachii Tendon. Arthrosc. J. Arthrosc. Relat. Surg. 2011, 27, 581–592. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, C.R.; Chaffin, D.B.; Hughes, R.E. A Mathematical Musculoskeletal Shoulder Model for Proactive Ergonomic Analysis. Comput. Methods Biomech. Biomed. Eng. 2007, 10, 389–400. [Google Scholar] [CrossRef]
- Quental, C.; Folgado, J.; Ambrósio, J.; Monteiro, J. A New Shoulder Model with a Biologically Inspired Glenohumeral Joint. Med. Eng. Phys. 2016, 38, 969–977. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Antunes, M.; Quental, C.; Folgado, J.; de Campos Azevedo, C.; Ângelo, A.C. Shoulder Positioning during Superior Capsular Reconstruction: Computational Analysis of Graft Integrity and Shoulder Stability. Biology 2021, 10, 1263. https://doi.org/10.3390/biology10121263
Antunes M, Quental C, Folgado J, de Campos Azevedo C, Ângelo AC. Shoulder Positioning during Superior Capsular Reconstruction: Computational Analysis of Graft Integrity and Shoulder Stability. Biology. 2021; 10(12):1263. https://doi.org/10.3390/biology10121263
Chicago/Turabian StyleAntunes, Madalena, Carlos Quental, João Folgado, Clara de Campos Azevedo, and Ana Catarina Ângelo. 2021. "Shoulder Positioning during Superior Capsular Reconstruction: Computational Analysis of Graft Integrity and Shoulder Stability" Biology 10, no. 12: 1263. https://doi.org/10.3390/biology10121263
APA StyleAntunes, M., Quental, C., Folgado, J., de Campos Azevedo, C., & Ângelo, A. C. (2021). Shoulder Positioning during Superior Capsular Reconstruction: Computational Analysis of Graft Integrity and Shoulder Stability. Biology, 10(12), 1263. https://doi.org/10.3390/biology10121263