
SEM-EDX Analysis of Metal Particles Deposition from Surgical Burs after Implant Guided Surgery Procedures

 ,
, 
 ,
,  , , ,
, , ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Samples Preparation
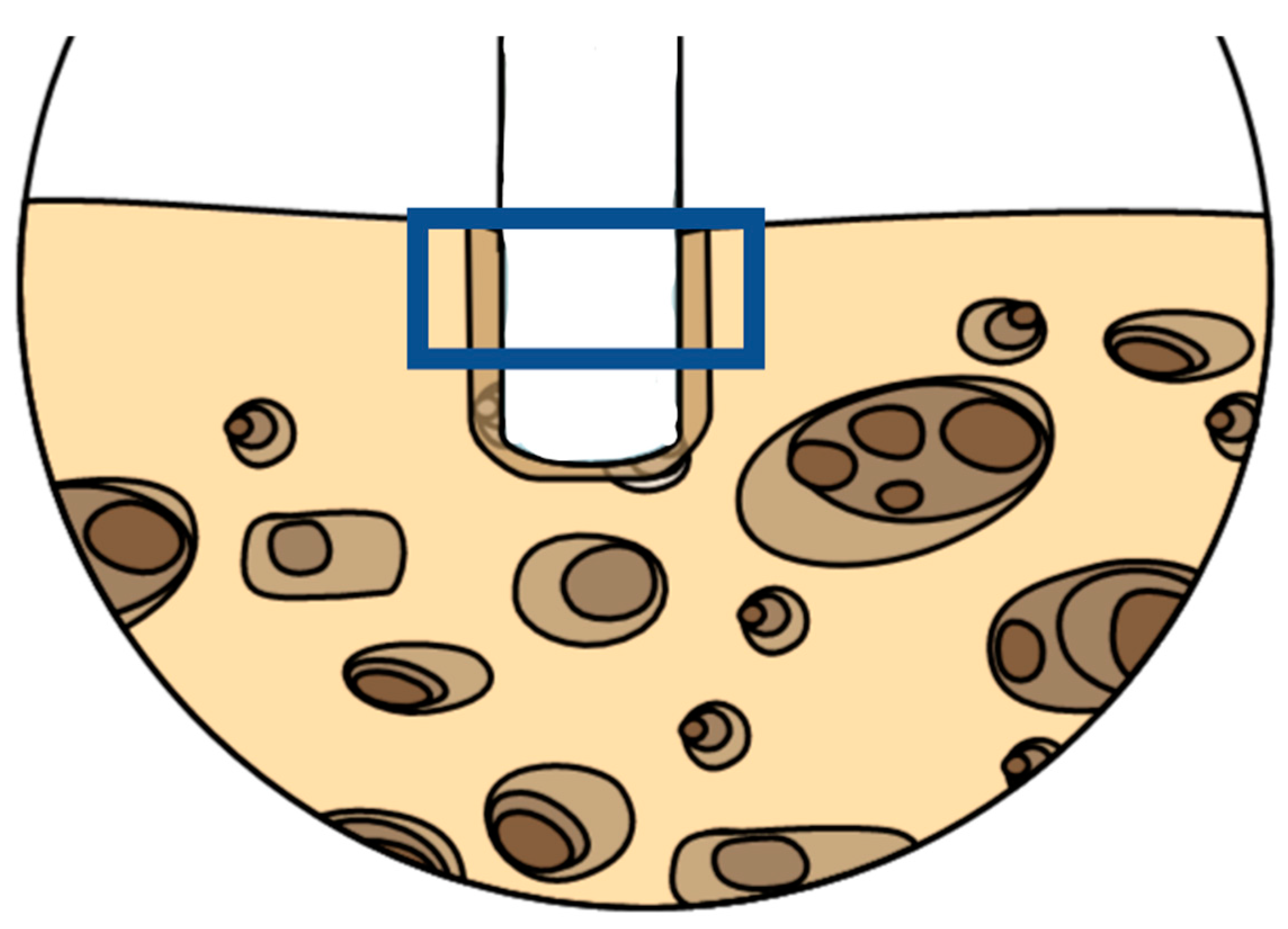
2.2. Guided Surgery Protocol
- -
- As a first step, the use of the lanceolate bur;
- -
- The subsequent corticotomy with the 2 mm diameter (2D) and 6 mm length bur;
- -
- Deepening of the preparation with the D2 and 11.5 mm length bur;
- -
- Expansion of the site with burs in sequence:
- -
- A bur of 2.8 mm diameter and 11.5 mm length;
- -
- A bur of 3.2 mm diameter and 11.5 mm length;
- -
- Final preparation with a bur of 3.65 diameter and 11.5 mm length.
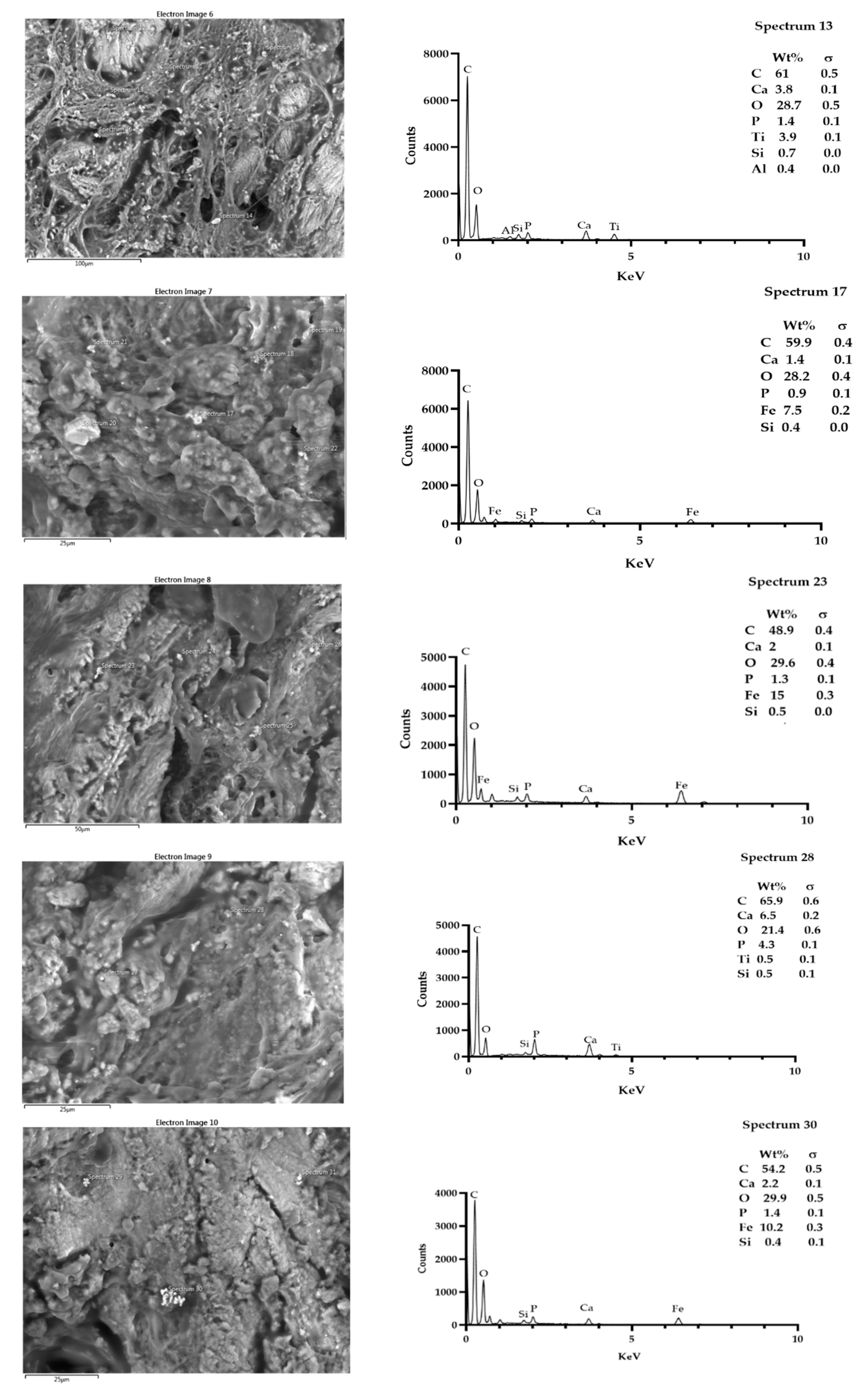
2.3. SEM-EDX
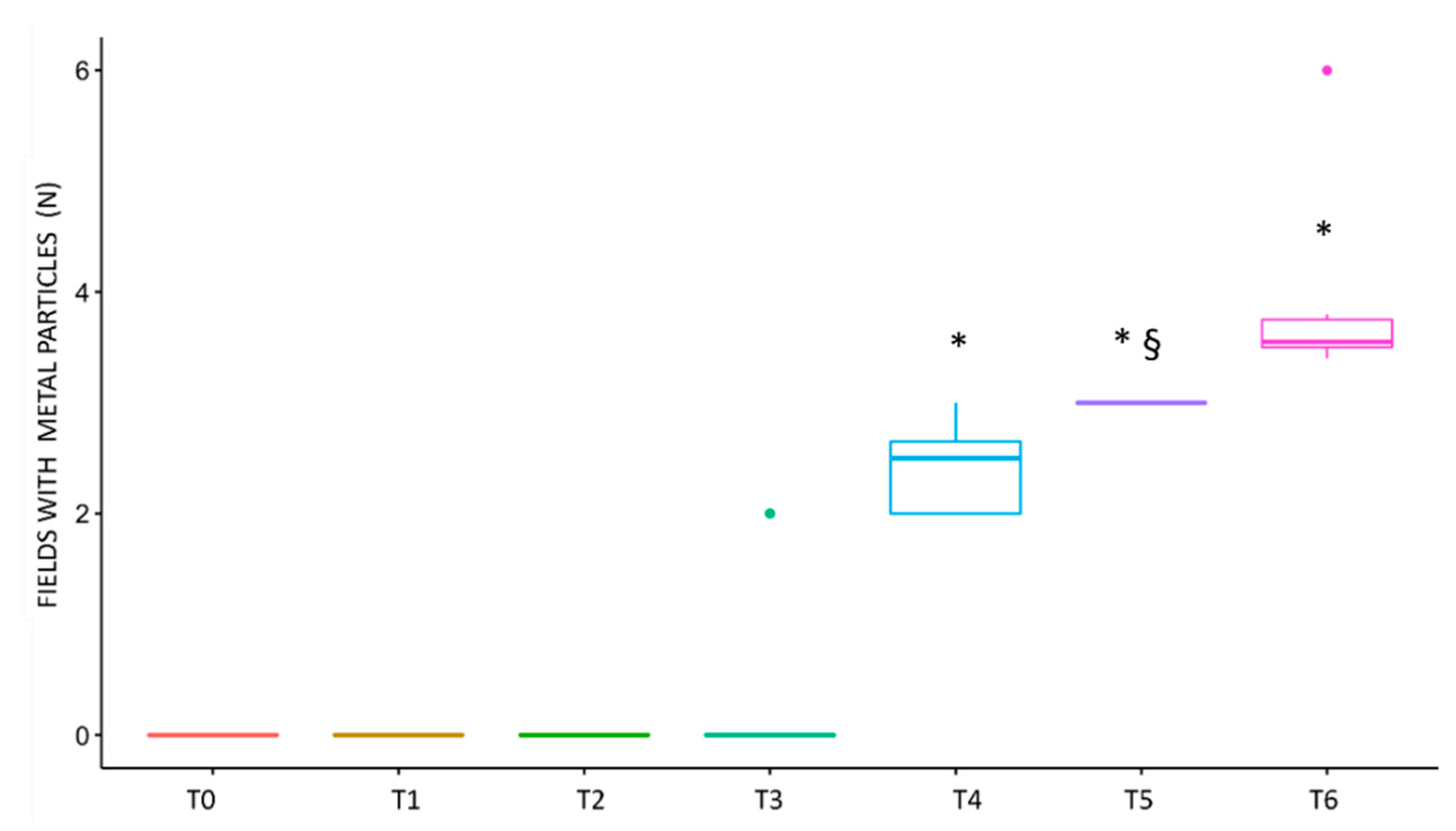
2.4. Statistical Analysis
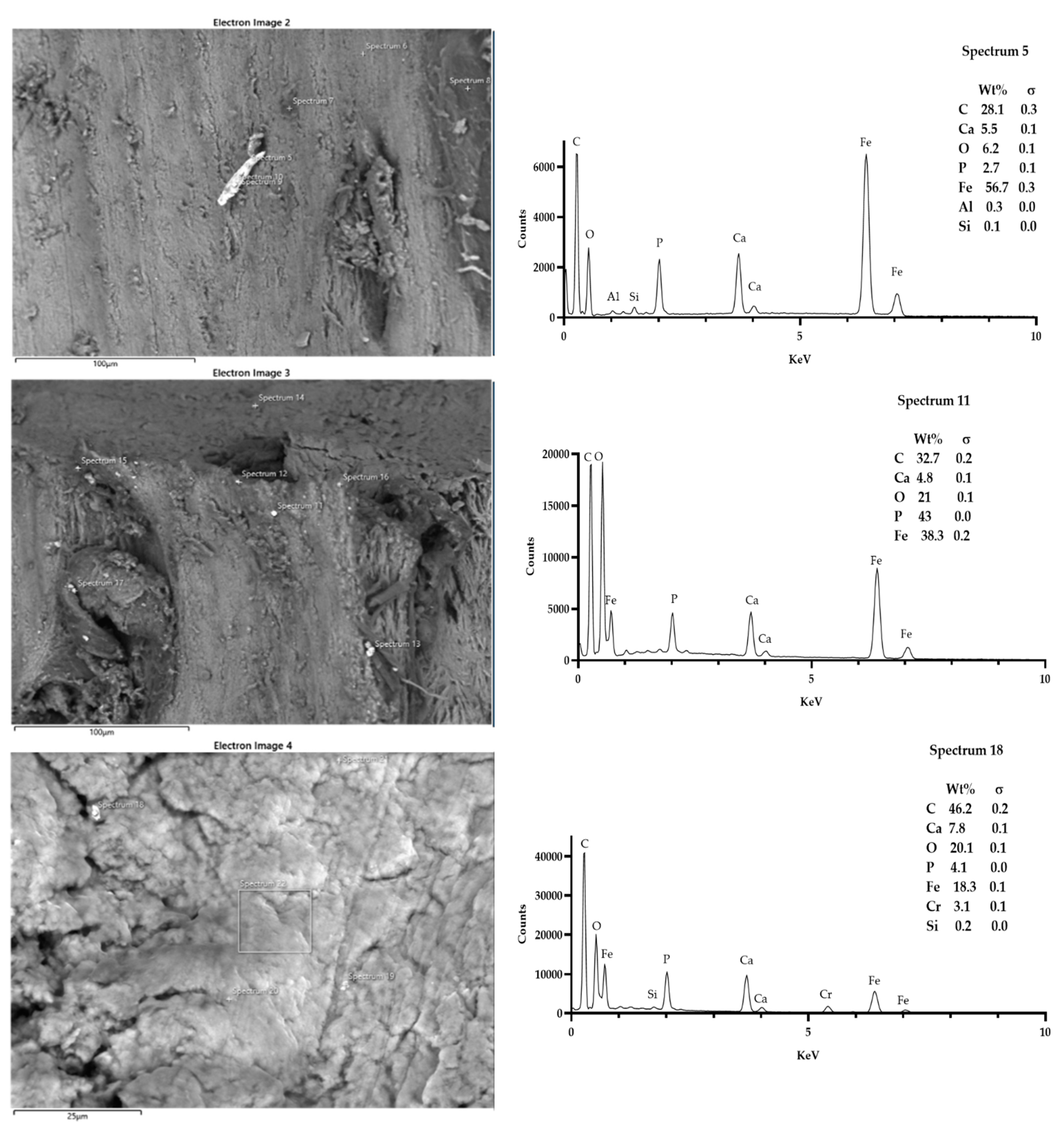
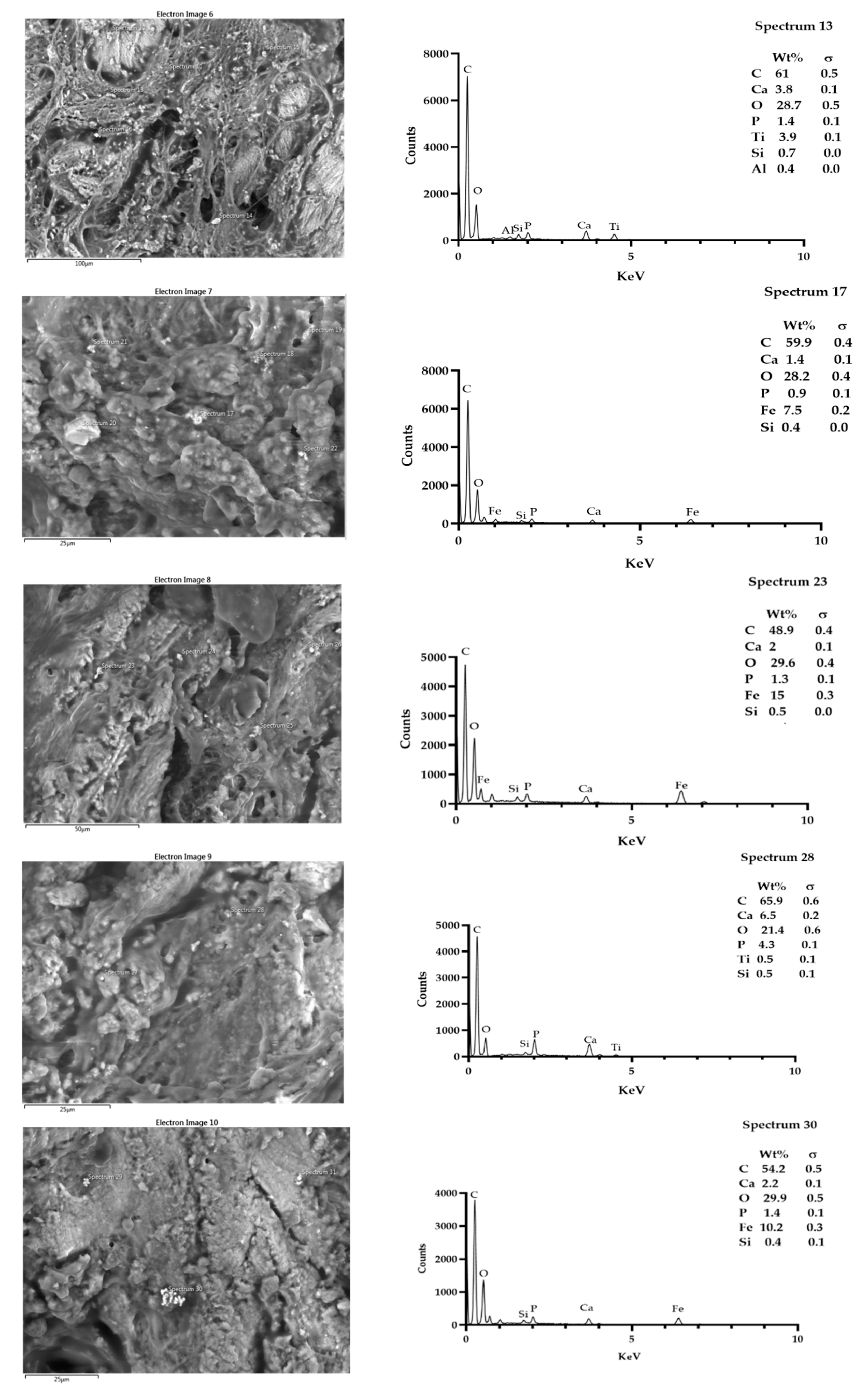
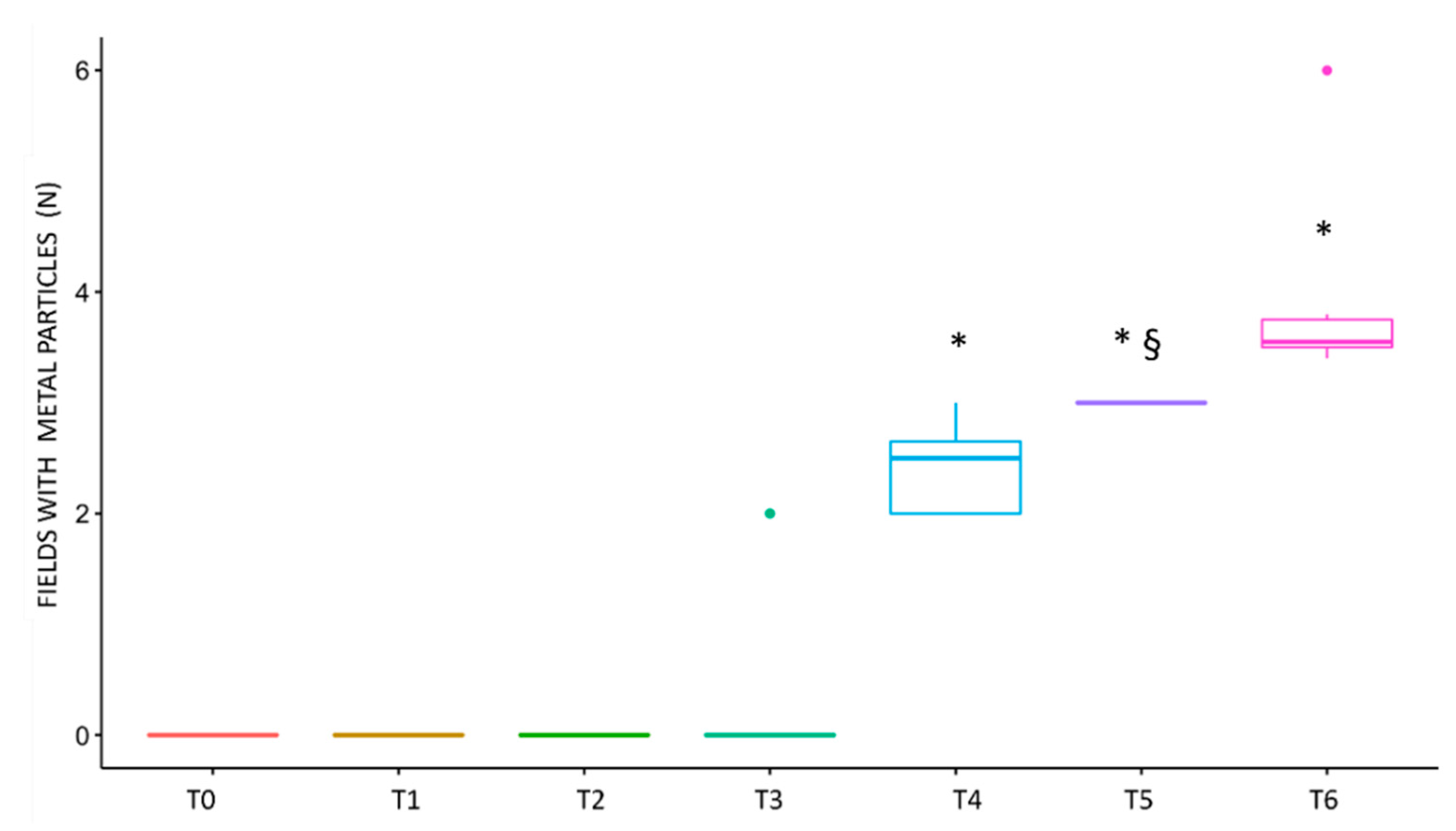
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Misch, C.E.; Perel, M.L.; Wang, H.L.; Sammartino, G.; Galindo-Moreno, P.; Trisi, P.; Steigmann, M.; Rebaudi, A.; Palti, A.; Pikos, M.A.; et al. Implant success, survival, and failure: The International Congress of Oral Implantologists (ICOI) Pisa Consensus Conference. Implant. Dent. 2008, 17, 5–15. [Google Scholar] [CrossRef] [Green Version]
- Özcan, M.; Hämmerle, C. Titanium as a reconstruction and implant material in dentistry: Advantages and pitfalls. Materials 2012, 5, 1528–1545. [Google Scholar] [CrossRef] [Green Version]
- Bernardi, S.; Bianchi, S.; Botticelli, G.; Rastelli, E.; Tomei, A.R.; Palmerini, M.G.; Continenza, M.A.; Macchiarelli, G. Scanning electron microscopy and microbiological approaches for the evaluation of salivary microorganisms behaviour on anatase titanium surfaces: In vitro study. Morphologie 2018, 102, 1–6. [Google Scholar] [CrossRef]
- Bianchi, S.; Fantozzi, G.; Bernardi, S.; Antonouli, S.; Continenza, M.A.; Macchiarelli, G. Commercial oral hygiene products and implant collar surfaces: Scanning electron microscopy observations. Can. J. Dent. Hyg. 2020, 54, 26–31. [Google Scholar] [PubMed]
- Bernardi, S.; Bianchi, S.; Tomei, A.R.; Continenza, M.A.; Macchiarelli, G. Microbiological and SEM-EDS evaluation of titanium surfaces exposed to periodontal gel: In vitro study. Materials 2019, 12, 1448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ercoli, C.; Funkenbusch, P.D.; Lee, H.J.; Moss, M.E.; Graser, G.N. The influence of drill wear on cutting efficiency and heat production during osteotomy preparation for dental implants: A study of drill durability. Int J. Oral Maxillofac. Implant. 2004, 19, 335–349. [Google Scholar]
- Tretto, P.H.W.; Fabris, V.; Cericato, G.O.; Sarkis-Onofre, R.; Bacchi, A. Does the instrument used for the implant site preparation influence the bone–implant interface? A systematic review of clinical and animal studies. Int. J. Oral Maxillofac. Surg. 2019, 48, 97–107. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scarano, A.; Carinci, F.; Quaranta, A.; Di Iorio, D.; Assenza, B.; Piattelli, A. Effects of bur wear during implant site preparation: An in vitro study. Int. J. Immunopathol. Pharm. 2007, 20, 23–26. [Google Scholar] [CrossRef]
- Pedowitz, R.A.; Billi, F.; Kavanaugh, A.; Colbert, A.; Liu, S.; Savoie, F.H.; You, Z. Arthroscopic surgical tools: A source of metal particles and possible joint damage. Arthrosc. J. Arthrosc. Relat. Surg. 2013, 29, 1559–1565. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berryman, Z.; Bridger, L.; Hussaini, H.M.; Rich, A.M.; Atieh, M.; Tawse-Smith, A. Titanium particles: An emerging risk factor for peri-implant bone loss. Saudi Dent. J. 2020, 32, 283–292. [Google Scholar] [CrossRef]
- Messous, R.; Henriques, B.; Bousbaa, H.; Silva, F.S.; Teughels, W.; Souza, J.C.M. Cytotoxic effects of submicron- and nano-scale titanium debris released from dental implants: An integrative review. Clin. Oral Investig. 2021, 25, 1627–1640. [Google Scholar] [CrossRef] [PubMed]
- Lugowski, S.J.; Smith, D.C.; McHugh, A.D.; Van Loon, J.C. Release of metal ions from dental implant materials in vivo: Determination of Al, Co, Cr, Mo, Ni, V, and Ti in organ tissue. J. Biomed. Mater. Res. 1991, 25, 1443–1458. [Google Scholar] [CrossRef] [PubMed]
- Coen, N.; Kadhim, M.A.; Wright, E.G.; Case, C.P.; Mothersill, C.E. Particulate debris from a titanium metal prosthesis induces genomic instability in primary human fibroblast cells. Br. J. Cancer 2003, 88, 548–552. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Goodman, S.B. Wear particles, periprosthetic osteolysis and the immune system. Biomaterials 2007, 28, 5044–5048. [Google Scholar] [CrossRef] [Green Version]
- Schoon, J.; Hesse, B.; Rakow, A.; Ort, M.J.; Lagrange, A.; Jacobi, D.; Winter, A.; Huesker, K.; Reinke, S.; Cotte, M.; et al. Metal-specific biomaterial accumulation in human peri-implant bone and bone marrow. Adv. Sci. 2020, 7, 2000412. [Google Scholar] [CrossRef]
- Senna, P.; Antoninha Del Bel Cury, A.; Kates, S.; Meirelles, L. Surface damage on dental implants with release of loose particles after insertion into bone. Clin. Implant. Dent. Relat. Res. 2015, 17, 681–692. [Google Scholar] [CrossRef] [Green Version]
- Sridhar, S.; Abidi, Z.; Wilson, T.G.J.; Valderrama, P.; Wadhwani, C.; Palmer, K.; Rodrigues, D.C. In vitro evaluation of the effects of multiple oral factors on dental implants surfaces. J. Oral Implant. 2016, 42, 248–257. [Google Scholar] [CrossRef]
- Caton, J.G.; Armitage, G.; Berglundh, T.; Chapple, I.; Jepsen, S.; Kornman, K.S.; Mealey, B.L.; Papapanou, P.N.; Sanz, M.; Tonetti, M.S. A new classification scheme for periodontal and peri-implant diseases and conditions—Introduction and key changes from the 1999 classification. J. Clin. Periodontol. 2018, 45, S1–S8. [Google Scholar] [CrossRef]
- Lafaurie, G.I.; Sabogal, M.A.; Castillo, D.M.; Rincón, M.V.; Gómez, L.A.; Lesmes, Y.A.; Chambrone, L. Microbiome and microbial biofilm profiles of peri-implantitis: A systematic review. J. Periodontol. 2017, 88, 1066–1089. [Google Scholar] [CrossRef]
- Fragkioudakis, I.; Tseleki, G.; Doufexi, A.E.; Sakellari, D. Current concepts on the pathogenesis of peri-implantitis: A narrative review. Eur. J. Dent. 2021, 15, 379–387. [Google Scholar] [CrossRef]
- Di Murro, B.; Moretti, M.; De Smaele, E.; Letizia, C.; Lubrano, C.; Passarelli, P.C.; D’Addona, A.; Pompa, G.; Papi, P. Microbiological profiles of dental implants in metabolic syndrome patients: A case-control study. Antibiotics 2021, 10, 452. [Google Scholar] [CrossRef] [PubMed]
- Harris, W.H. Conquest of a worldwide human disease: Particle-induced periprosthetic osteolysis. Orthop. Relat. Res. 2004, 429, 439–442. [Google Scholar] [CrossRef] [PubMed]
- Lybrand, K.E.; Althausen, P.L. The role of value-based implants in orthopedic trauma. Orthop. Clin. Am. 2018, 49, 437–443. [Google Scholar] [CrossRef]
- Bitar, D.; Parvizi, J. Biological response to prosthetic debris. World Orthop. 2015, 6, 172–189. [Google Scholar] [CrossRef]
- Fretwurst, T.; Nelson, K.; Tarnow, D.P.; Wang, H.L.; Giannobile, W.V. Is metal particle release associated with peri-implant bone destruction? An emerging concept. Dent. Res. 2018, 97, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Ozan, O.; Şeker, E.; Çakmak, G.; Guo, X.; Yilmaz, B. Effect of guide sleeve material, region, diameter, and number of times drills were used on the material loss from sleeves and drills used for surgical guides: An in vitro study. Prosthet. Dent. 2021, 1–8. [Google Scholar] [CrossRef]
- Pearce, A.I.; Richards, R.G.; Milz, S.; Schneider, E.; Pearce, S.G. Animal models for implant biomaterial research in bone: A review. Eur. Cell Mater. 2007, 13, 1–10. [Google Scholar] [CrossRef]
- Misch, C.E. Bone character: Second vital implant criterion. Today 1988, 7, 39–40. [Google Scholar]
- Vesley, D.; Langholz, A.C.; Rohlfing, S.R.; Foltz, W.E. Fluorimetric detection of a bacillus stearothermophilus spore-bound enzyme, alpha-d-glucosidase, for rapid indication of flash sterilization failure. Appl. Environ. Microbiol. 1992, 58, 717–719. [Google Scholar] [CrossRef] [Green Version]
- Walzak, M.J.; Davidson, R.; Biesinger, M. The use of XPS, FTIR, SEM/EDX, contact angle, and AFM in the characterization of coatings. J. Mater. Eng. Perform. 1998, 7, 317–323. [Google Scholar] [CrossRef]
- Liu, S.; Hall, D.J.; McCarthy, S.M.; Jacobs, J.J.; Urban, R.M.; Pourzal, R. Fourier transform infrared spectroscopic imaging of wear and corrosion products within joint capsuletissue from total hip replacements patients. Biomed. Mater. Res. 2020, 108B, 513–526. [Google Scholar] [CrossRef]
- Frisch, E.; Wild, V.; Ratka-krüger, P.; Kirstin, V.; Sennhenn-kirchner, S. Long-term results of implants and implant-supported prostheses under systematic supportive implant therapy: A retrospective 25-year study. Clin. Implant. Dent. Relat. 2020, 22, 689–696. [Google Scholar] [CrossRef]
- Matusiewicz, H. Potential release of in vivo trace metals from metallic medical implants in the human body: From ions to nanoparticles—A systematic anal–tical review. Acta Biomater. 2014, 10, 2379–2403. [Google Scholar] [CrossRef]
- Rauner, M.; Sipos, W.; Pietschmann, P. Osteoimmunology. Int. Arch. Allergy Immunol. 2007, 143, 31–48. [Google Scholar] [CrossRef] [PubMed]
- Holt, G.; Murnaghan, C.; Reilly, J.; Meek, R.M.D. The biology of aseptic osteolysis. Clin. Orthop. Relat. Res. 2007, 460, 240–252. [Google Scholar] [CrossRef] [PubMed]
- Cadosch, D.; Gautschi, O.P.; Chan, E.; Simmen, H.P.; Filgueira, L. Titanium induced production of chemokines CCL17/TARC and CCL22/MDC in human osteoclasts and osteoblasts. J. Biomed. Mater. Res. A 2010, 92, 475–483. [Google Scholar] [CrossRef]
- Harris, B.H.; Kohles, S.S. Effects of mechanical and thermal fatigue on dental drill performance. Int. J. Oral Maxillofac. Implant. 2001, 16, 819–826. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Type | Cr wt% | Ni wt% | Cu wt% | Cb-Ta wt% | C wt% | Mn wt% | P wt% | S wt% | Si wt% |
|---|---|---|---|---|---|---|---|---|---|
| 17-4PH h 900 | Min 15 Max 17.5 | Min 3.0 Max 5.0 | Min 3.0 Max 5.0 | Min 0.15 Max 0.45 | 0.07 * Max | 1.00 Max | 0.04 * Max | 0.03 * Max | 1.00 Max |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Falisi, G.; Foffo, G.; Severino, M.; Di Paolo, C.; Bianchi, S.; Bernardi, S.; Pietropaoli, D.; Rastelli, S.; Gatto, R.; Botticelli, G. SEM-EDX Analysis of Metal Particles Deposition from Surgical Burs after Implant Guided Surgery Procedures. Coatings 2022, 12, 240. https://doi.org/10.3390/coatings12020240
Falisi G, Foffo G, Severino M, Di Paolo C, Bianchi S, Bernardi S, Pietropaoli D, Rastelli S, Gatto R, Botticelli G. SEM-EDX Analysis of Metal Particles Deposition from Surgical Burs after Implant Guided Surgery Procedures. Coatings. 2022; 12(2):240. https://doi.org/10.3390/coatings12020240
Chicago/Turabian StyleFalisi, Giovanni, Giordano Foffo, Marco Severino, Carlo Di Paolo, Serena Bianchi, Sara Bernardi, Davide Pietropaoli, Sofia Rastelli, Roberto Gatto, and Gianluca Botticelli. 2022. "SEM-EDX Analysis of Metal Particles Deposition from Surgical Burs after Implant Guided Surgery Procedures" Coatings 12, no. 2: 240. https://doi.org/10.3390/coatings12020240
APA StyleFalisi, G., Foffo, G., Severino, M., Di Paolo, C., Bianchi, S., Bernardi, S., Pietropaoli, D., Rastelli, S., Gatto, R., & Botticelli, G. (2022). SEM-EDX Analysis of Metal Particles Deposition from Surgical Burs after Implant Guided Surgery Procedures. Coatings, 12(2), 240. https://doi.org/10.3390/coatings12020240