Electrochemical Behavior of Rejected Dental Implants in Peri-Implantitis


 , ,
, , 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Materials
2.2. Methods
2.2.1. Open Circuit Potential Measurements
2.2.2. Electrochemical Impedance Spectroscopy
2.2.3. Tafel Analysis
2.2.4. Scanning Electron Microscopy
2.2.5. Statistical Analysis
3. Results
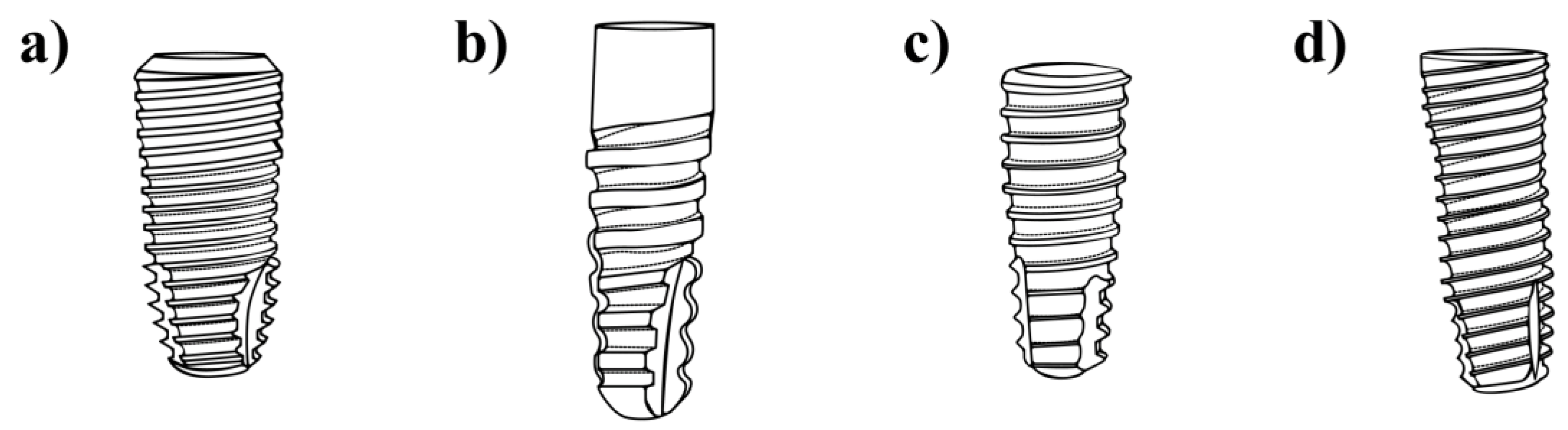
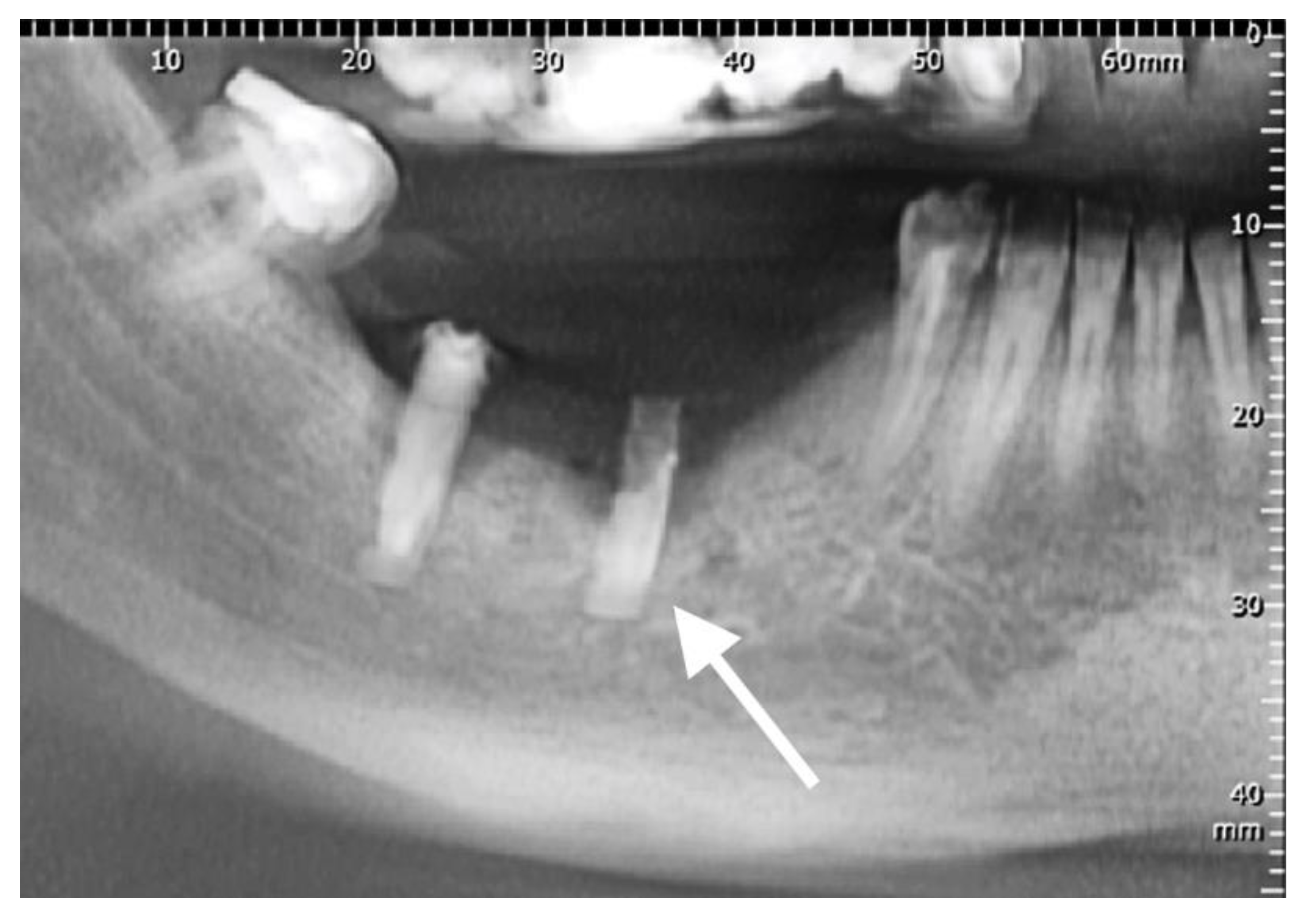
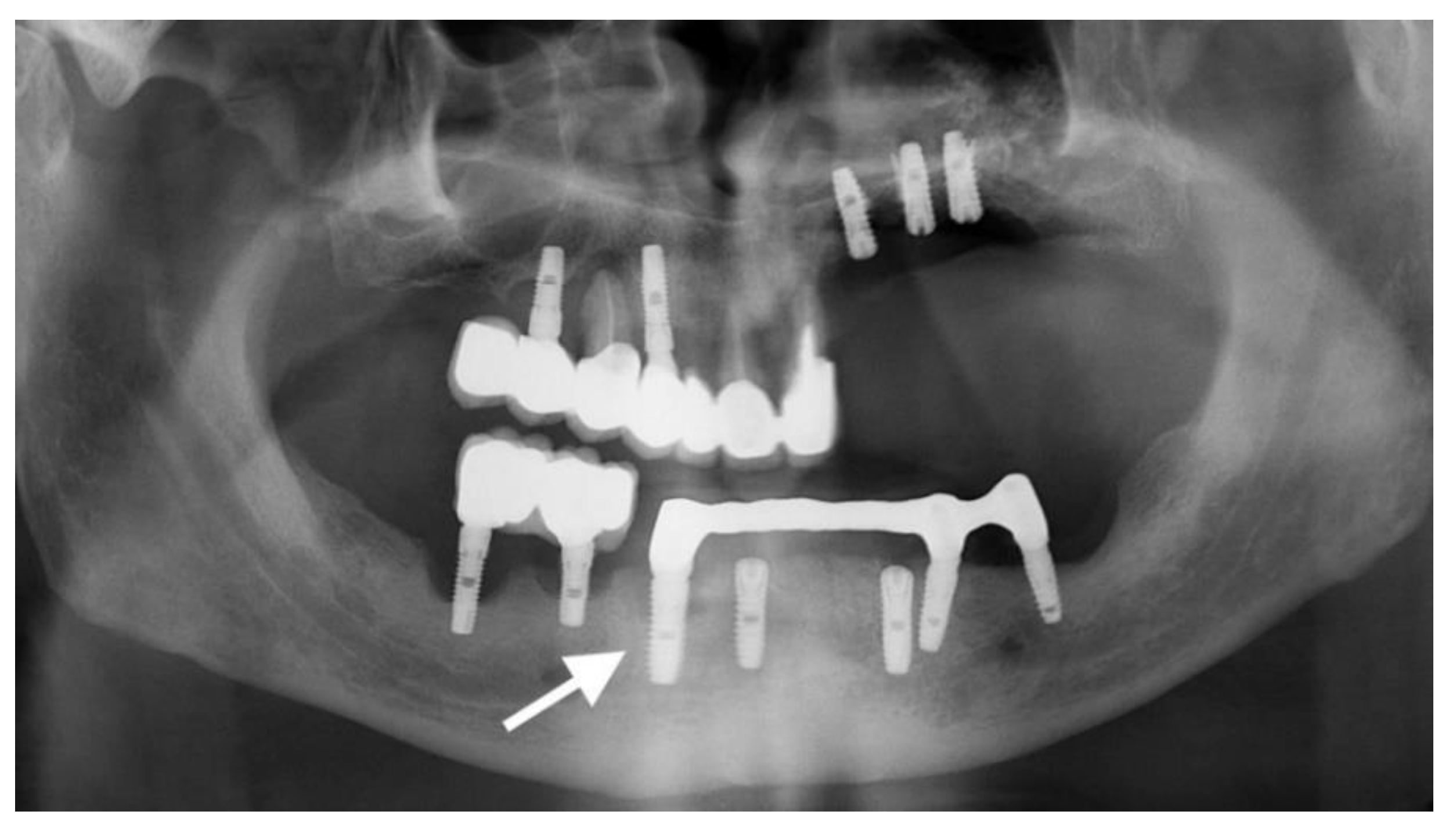
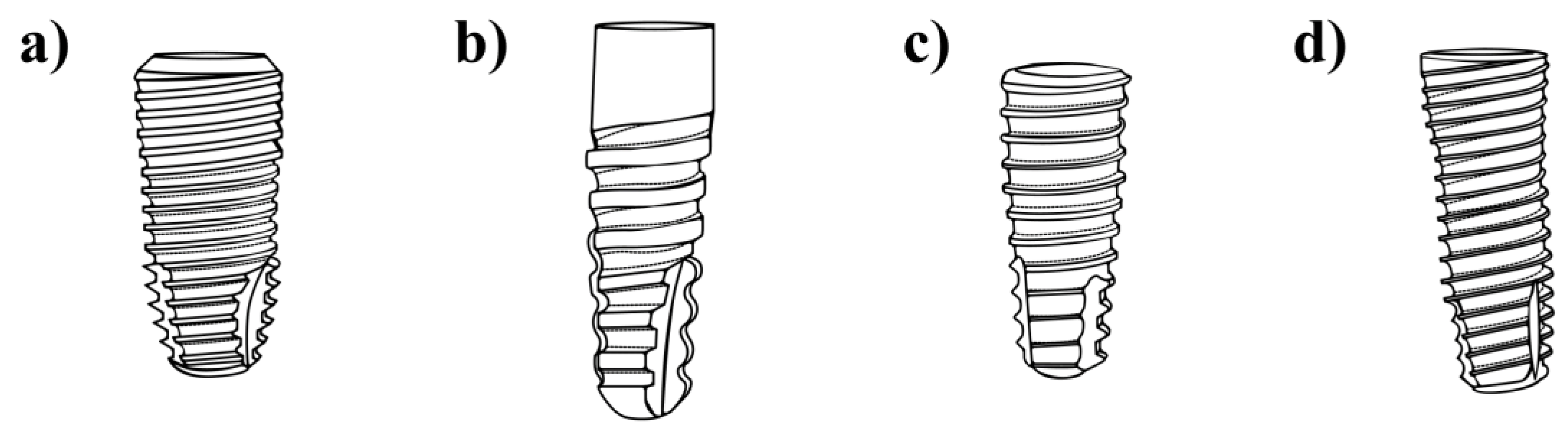
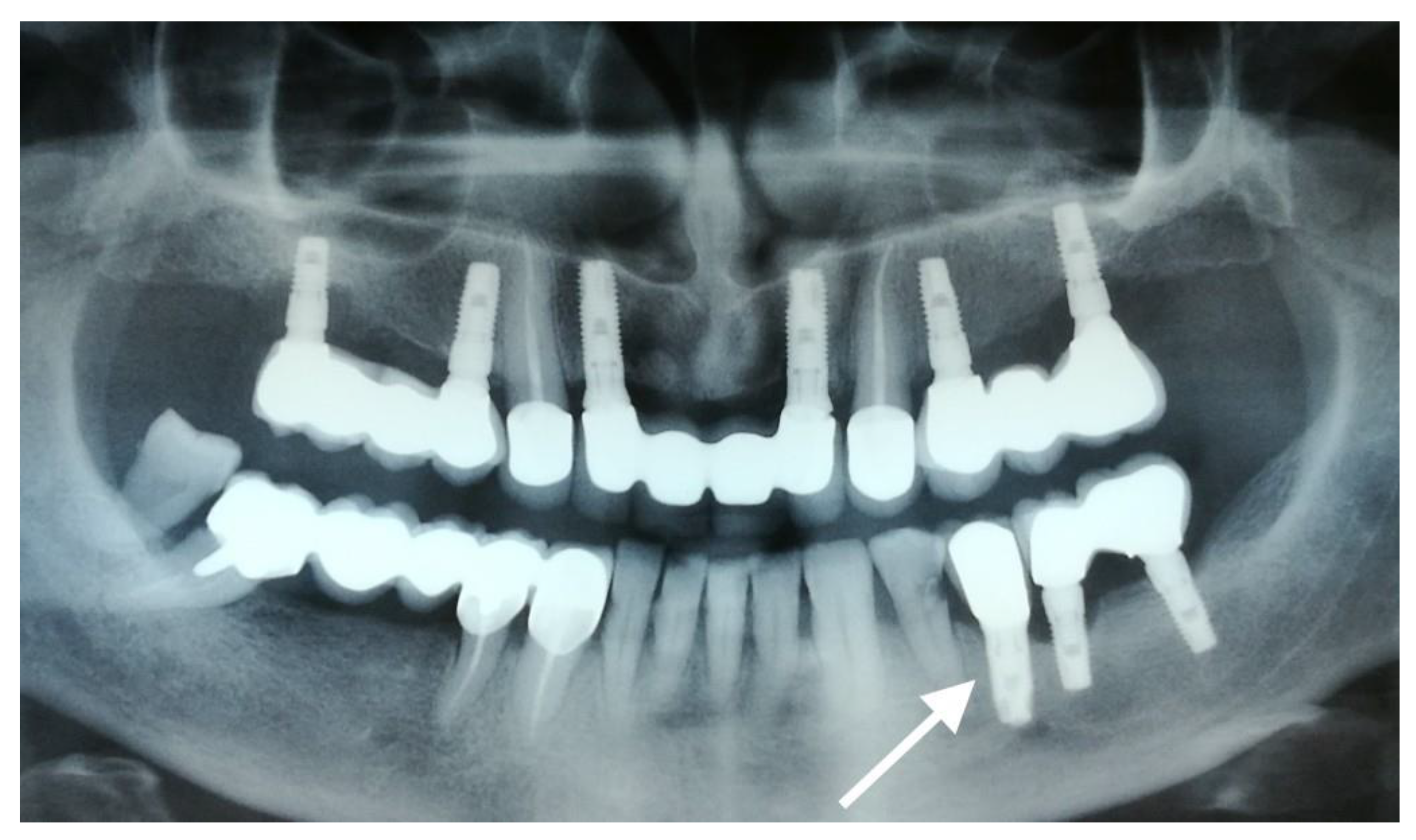
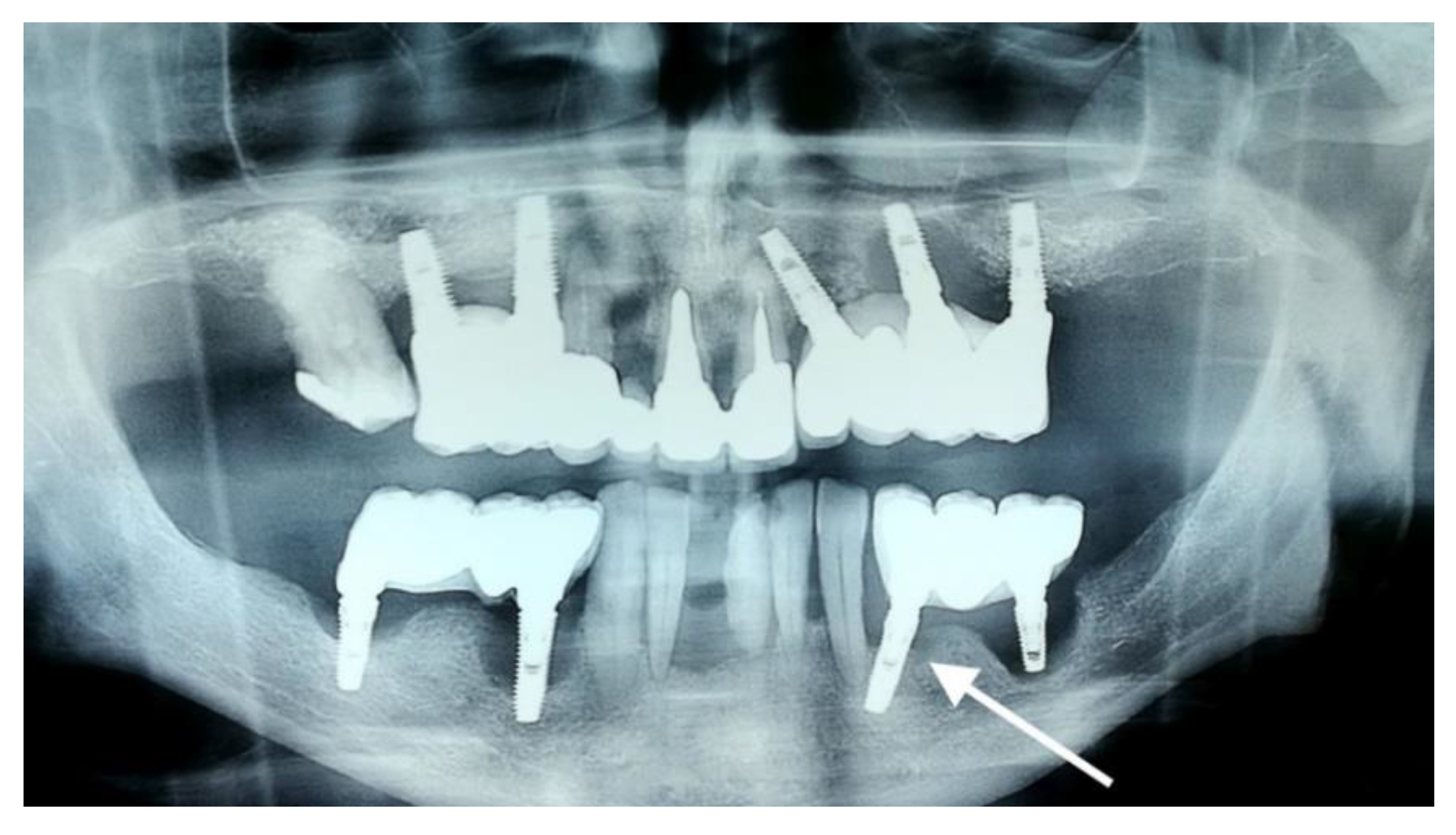
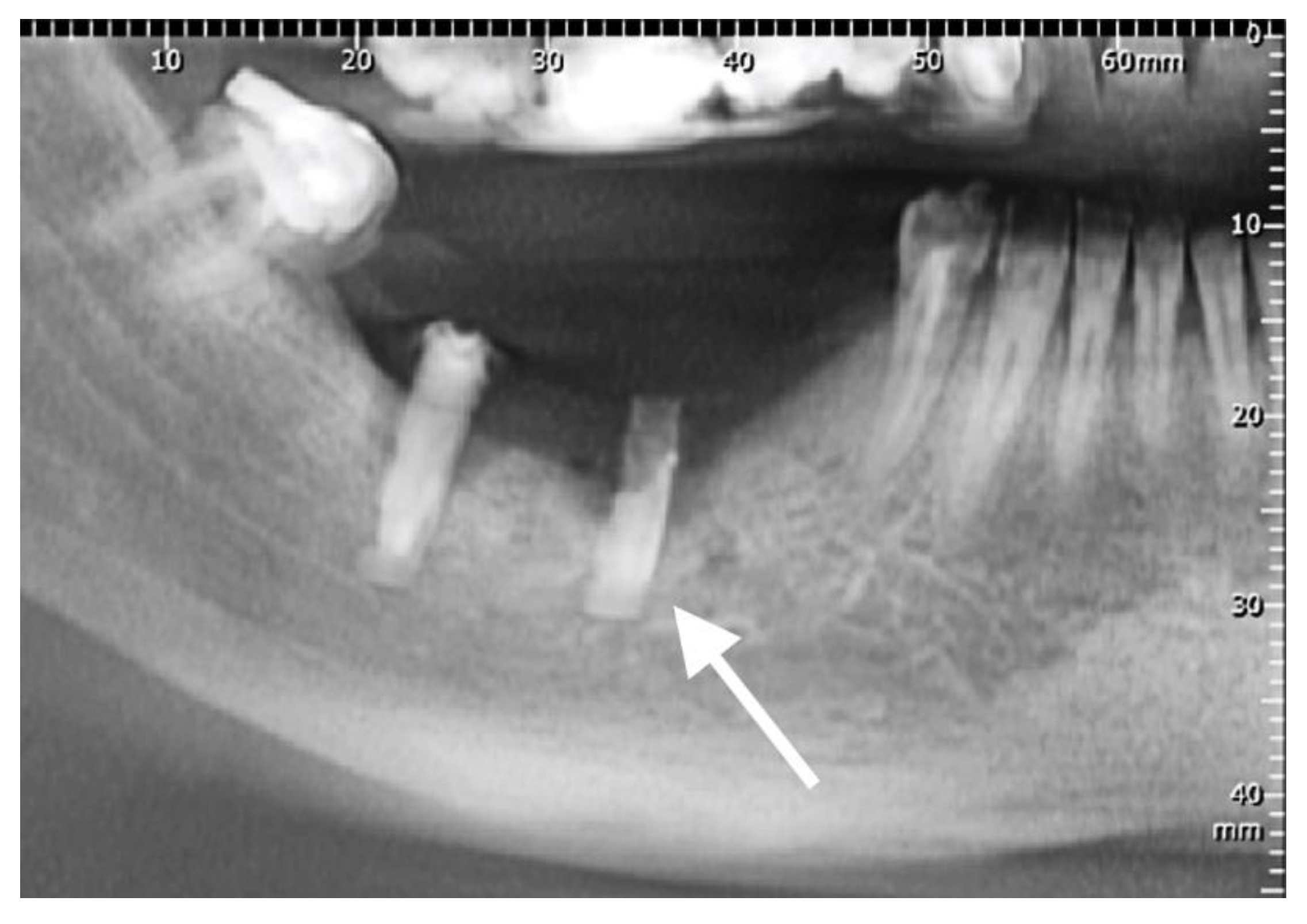
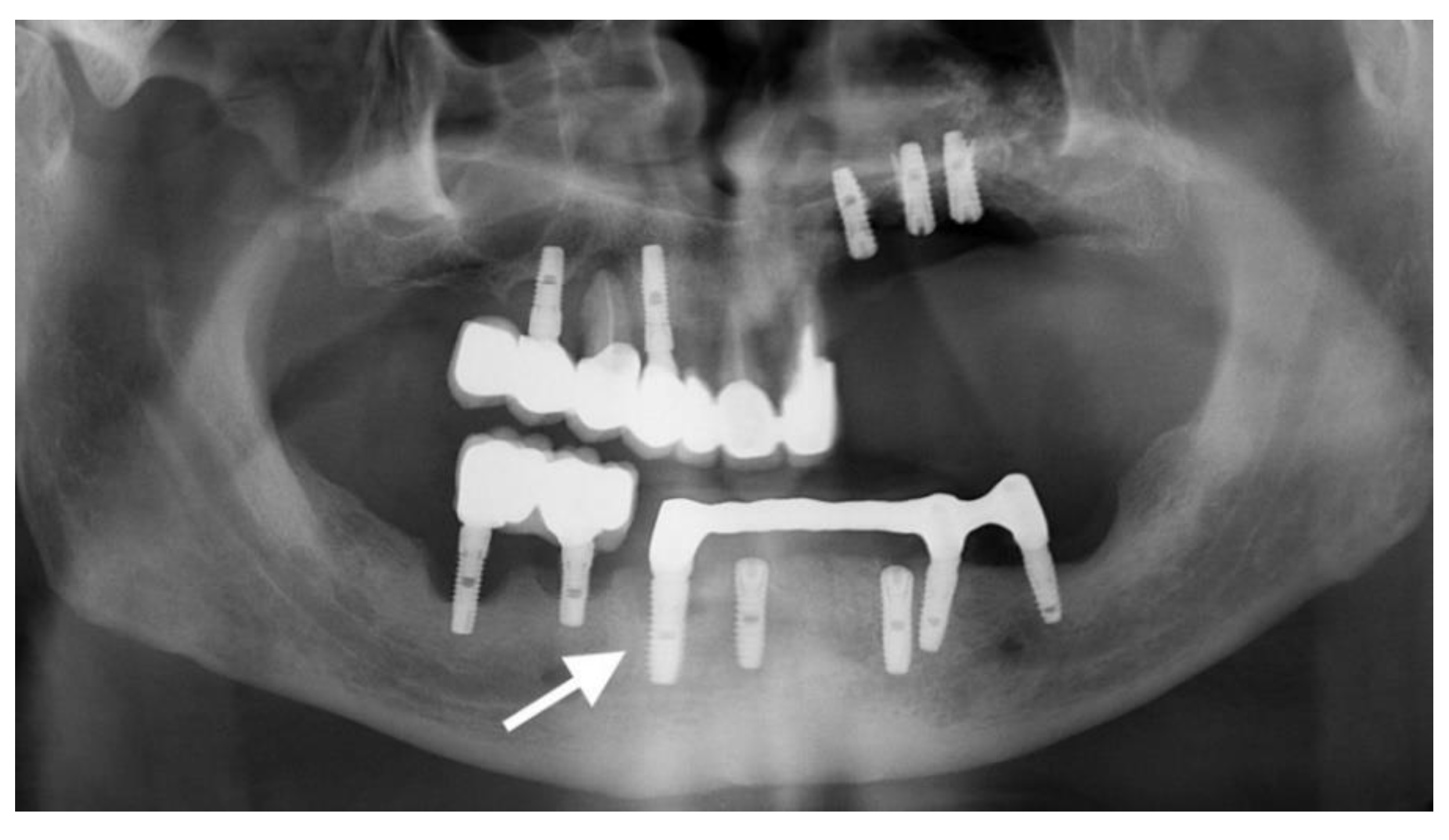
3.1. Dental Implants
3.2. Electrochemical Testing
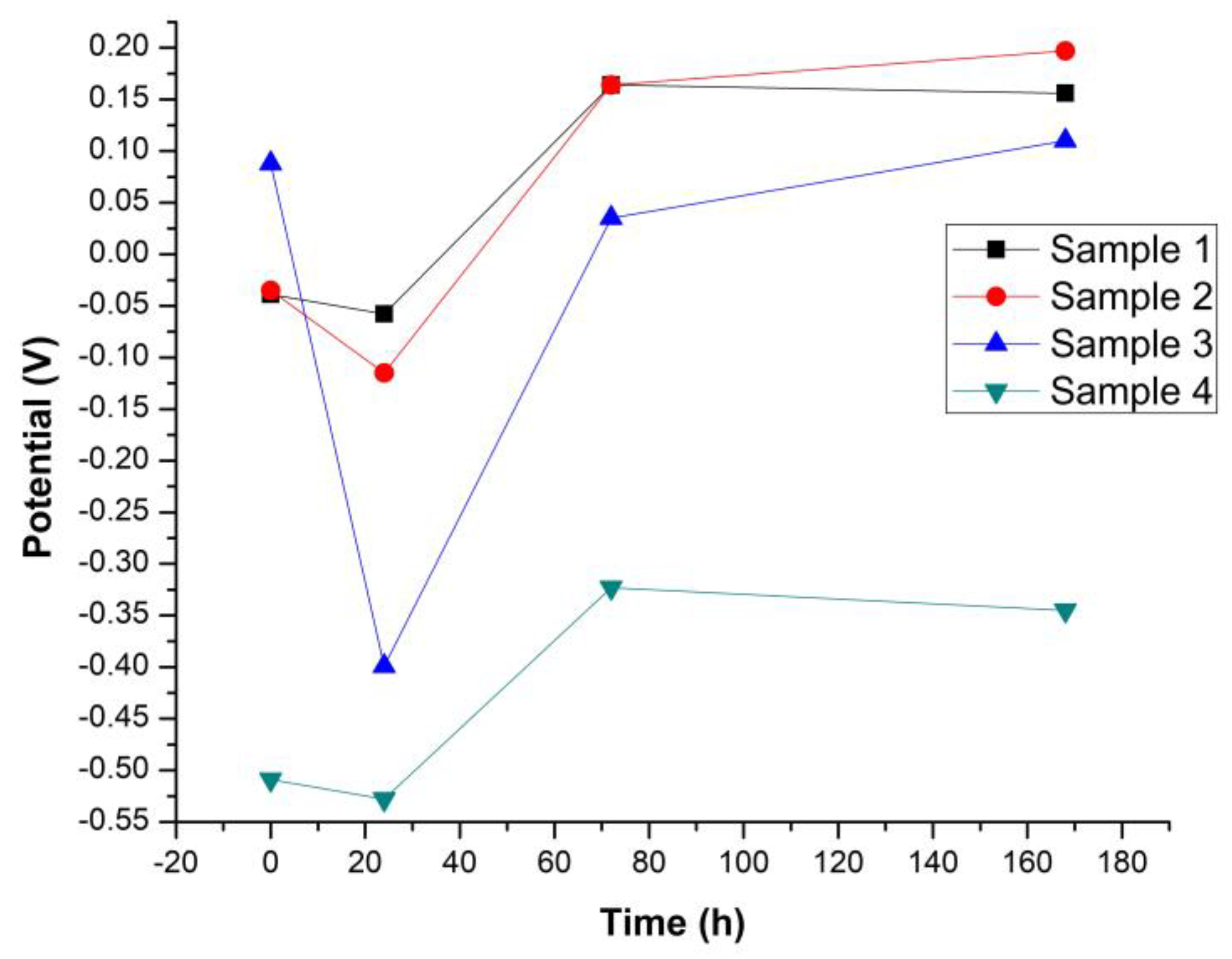
3.2.1. Open Circuit Potential Measurements
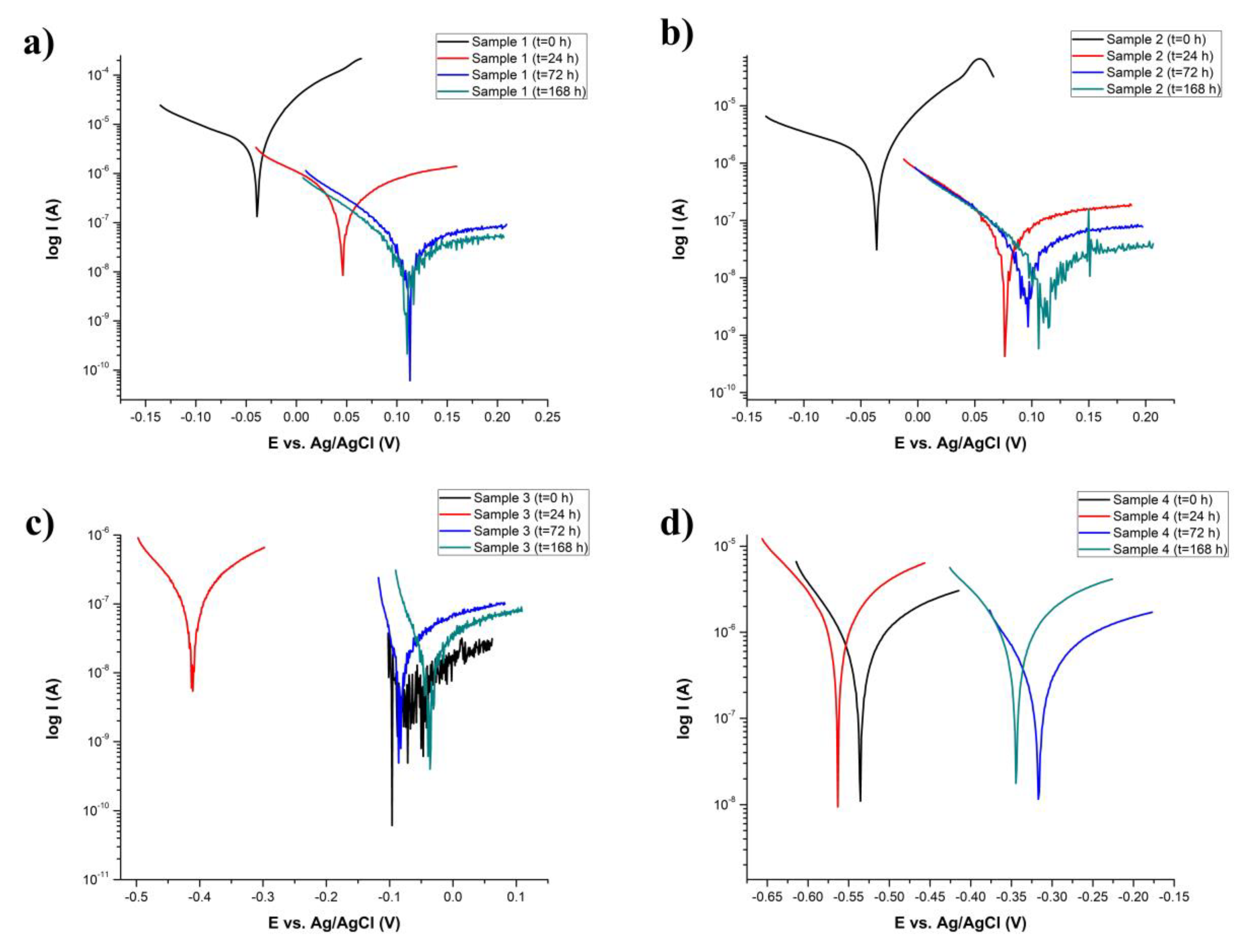
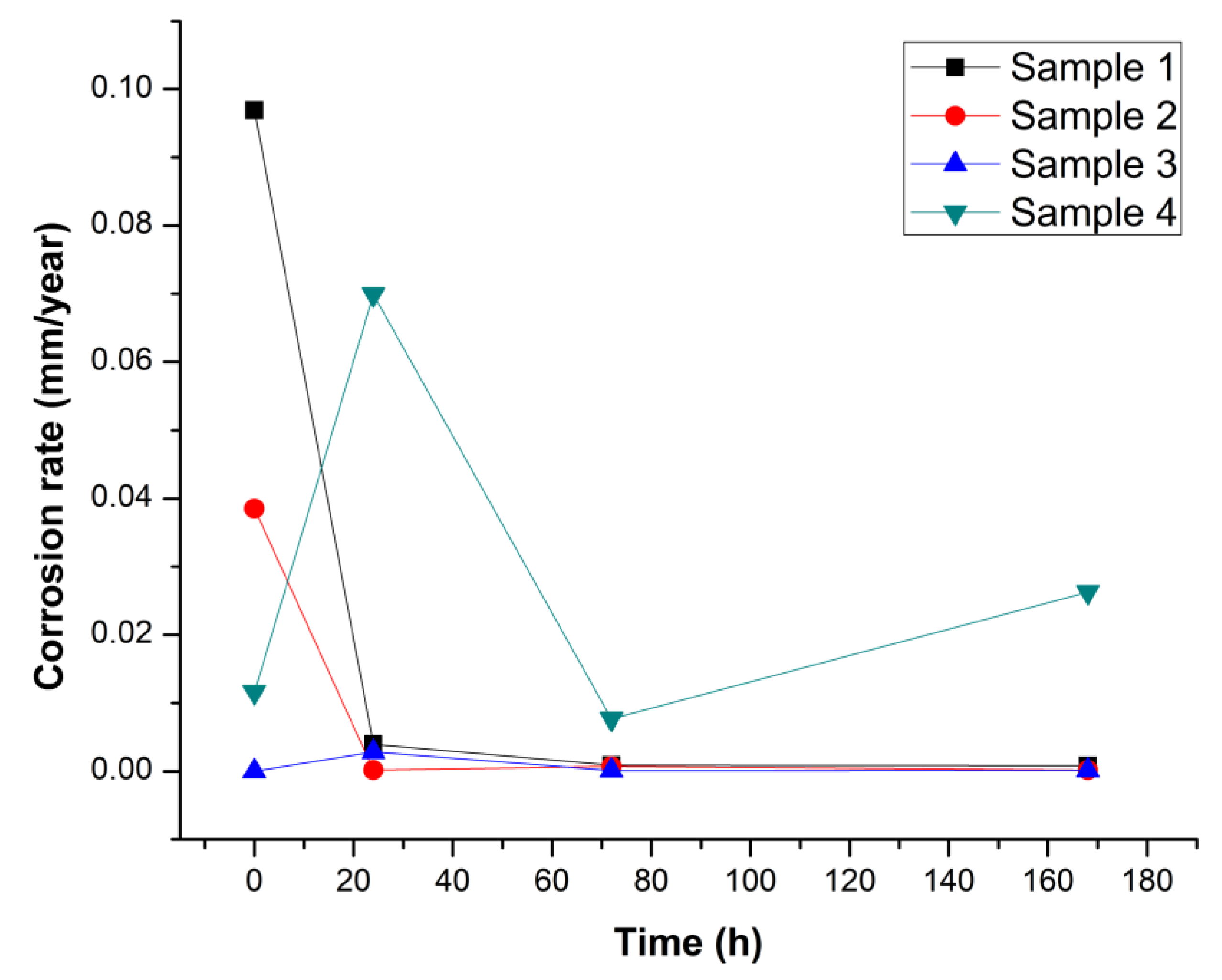
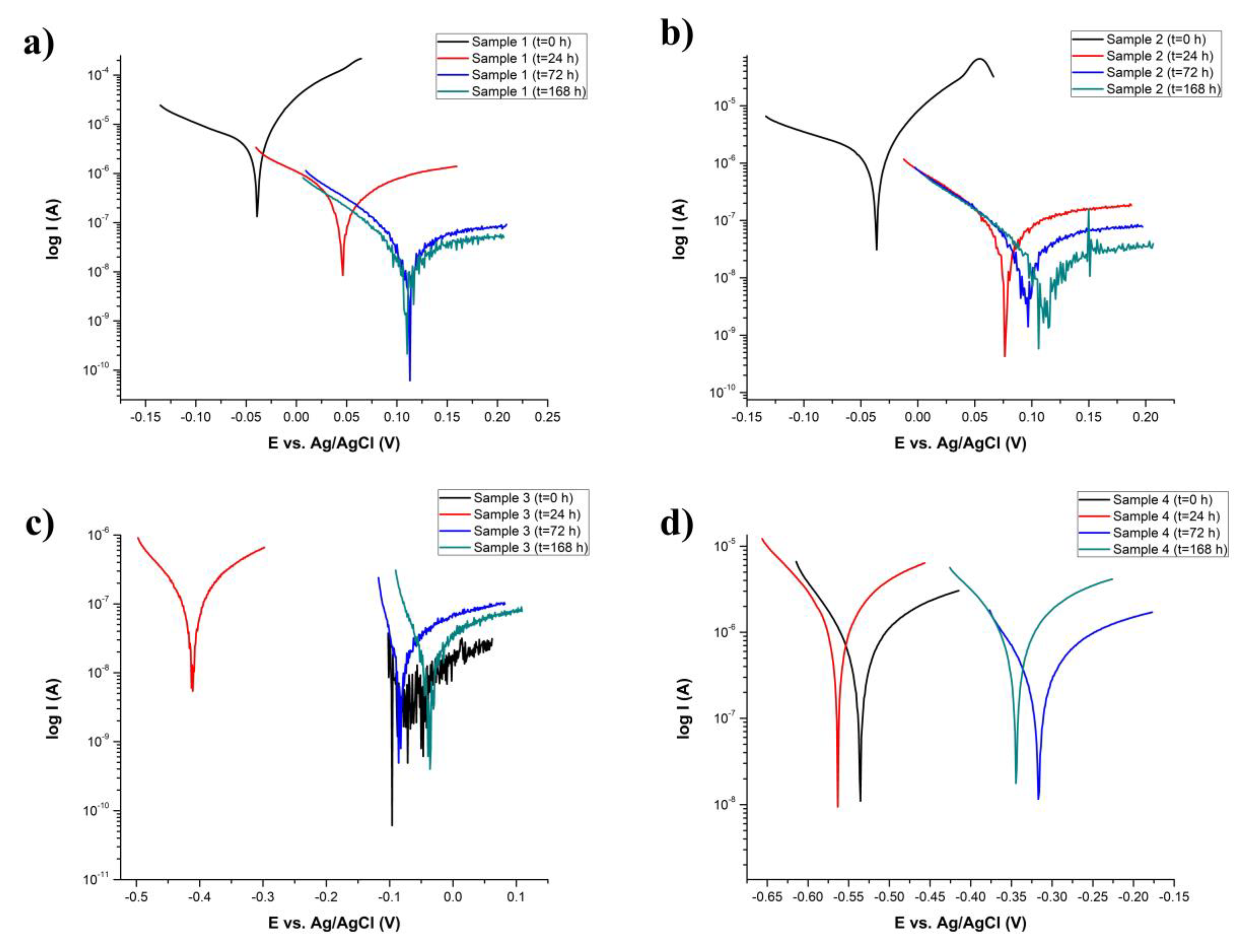
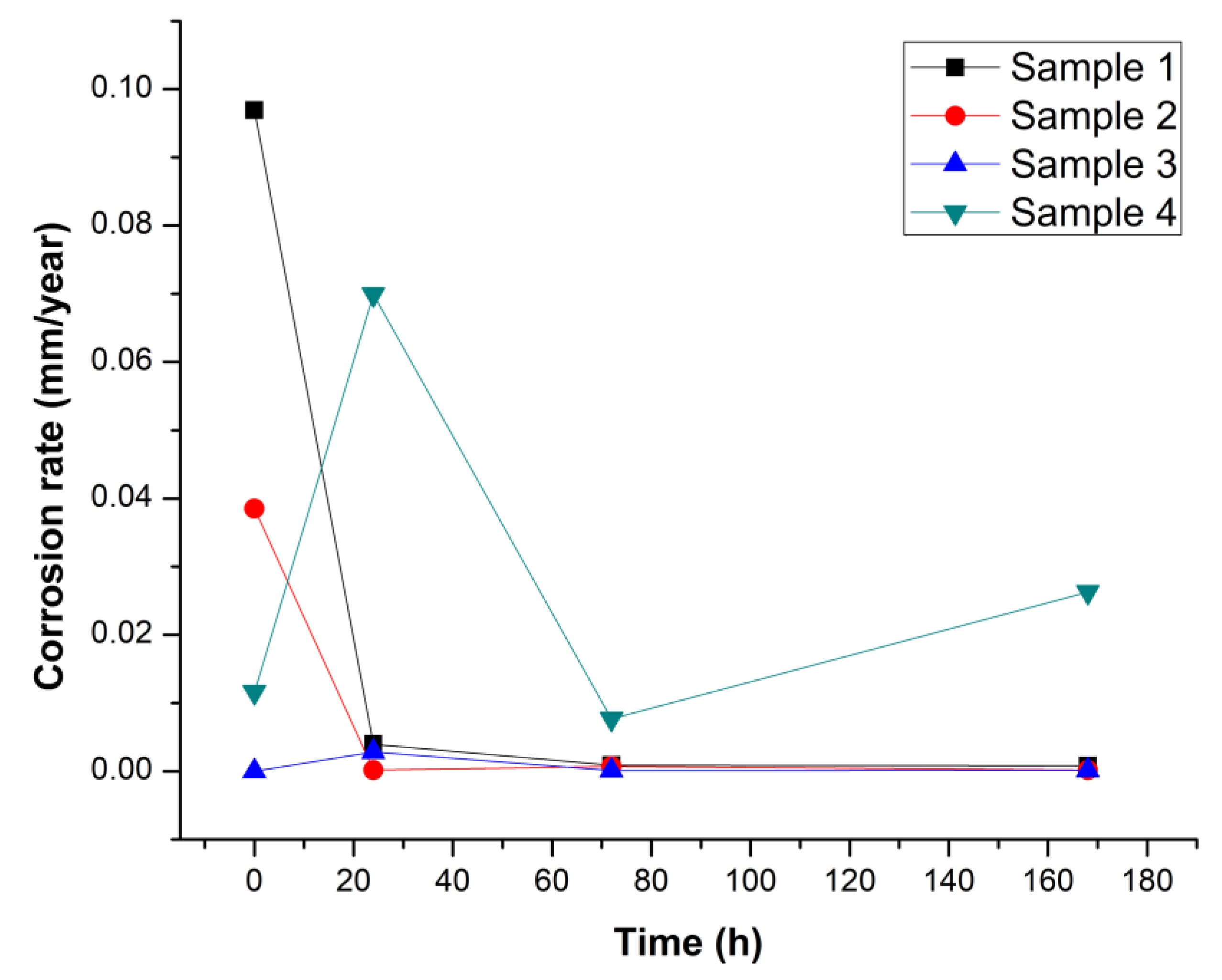
3.2.2. Tafel Analysis
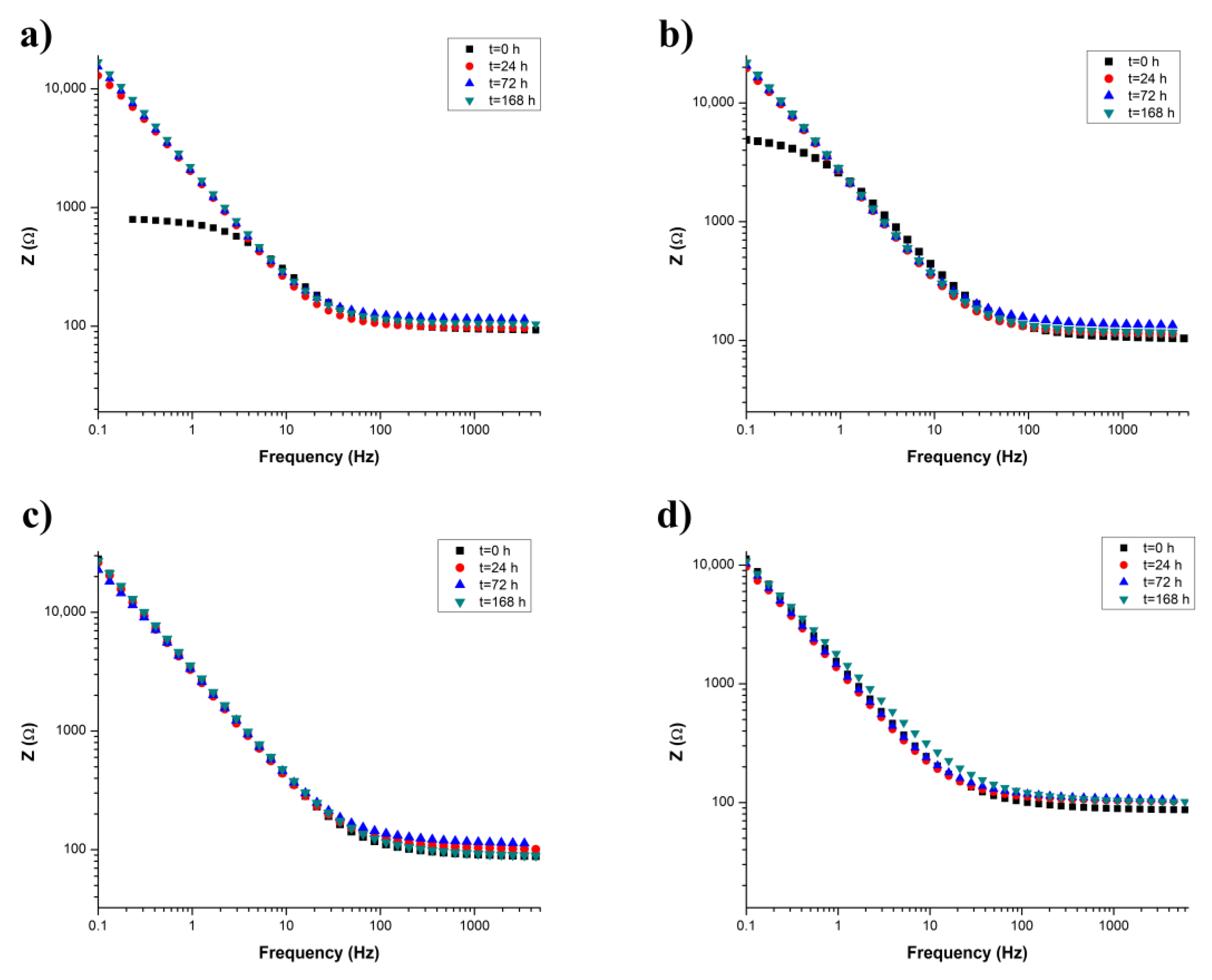
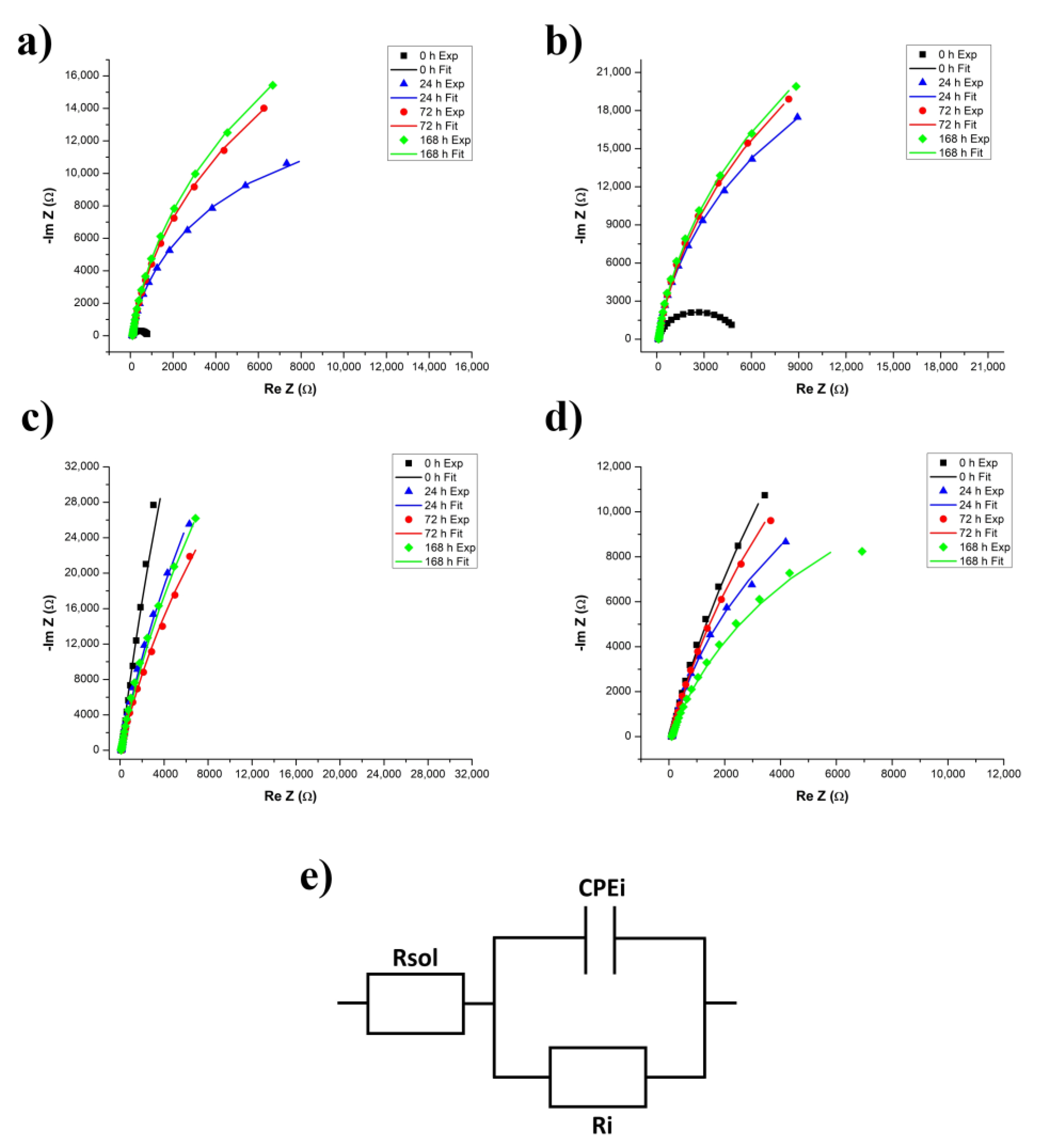
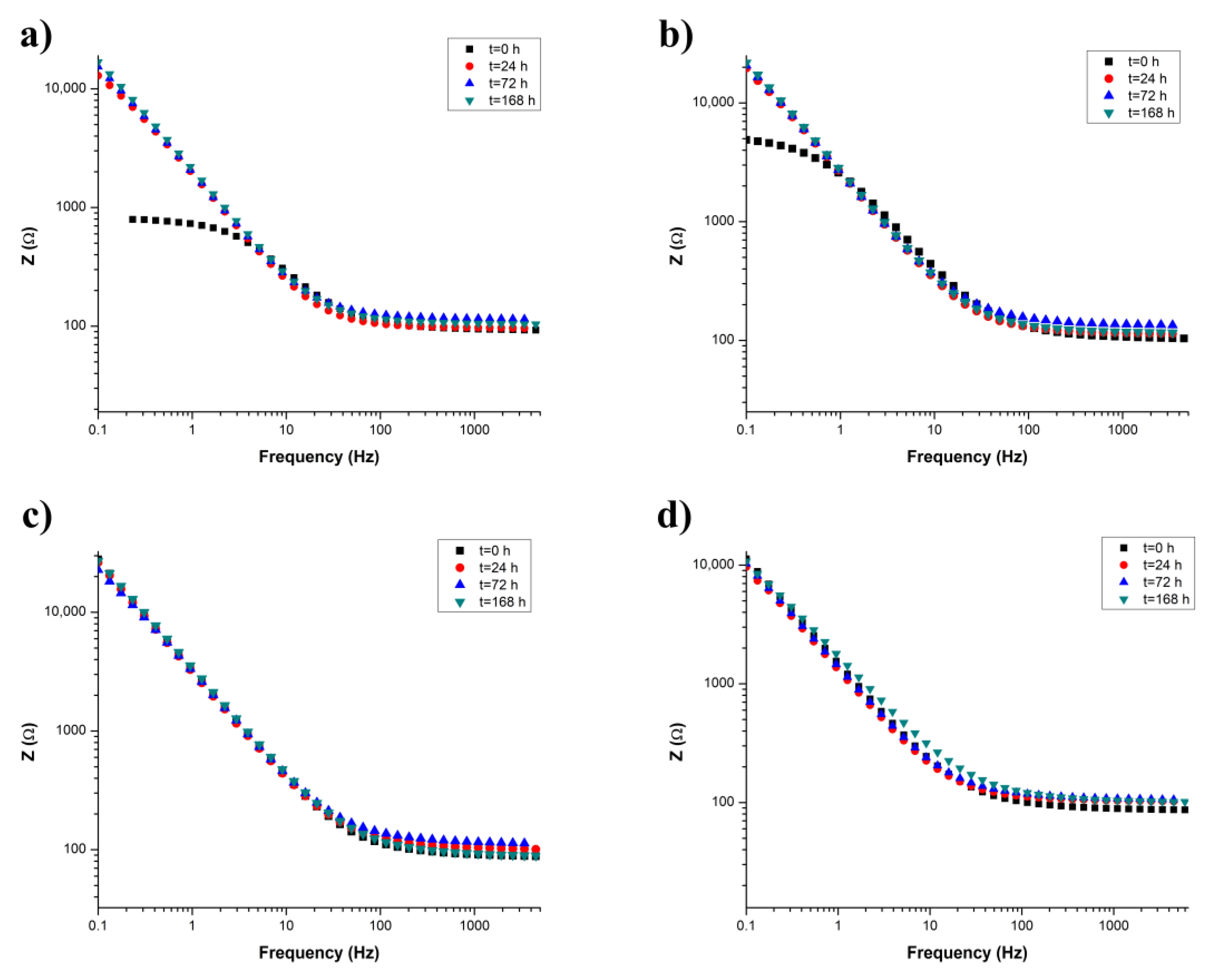
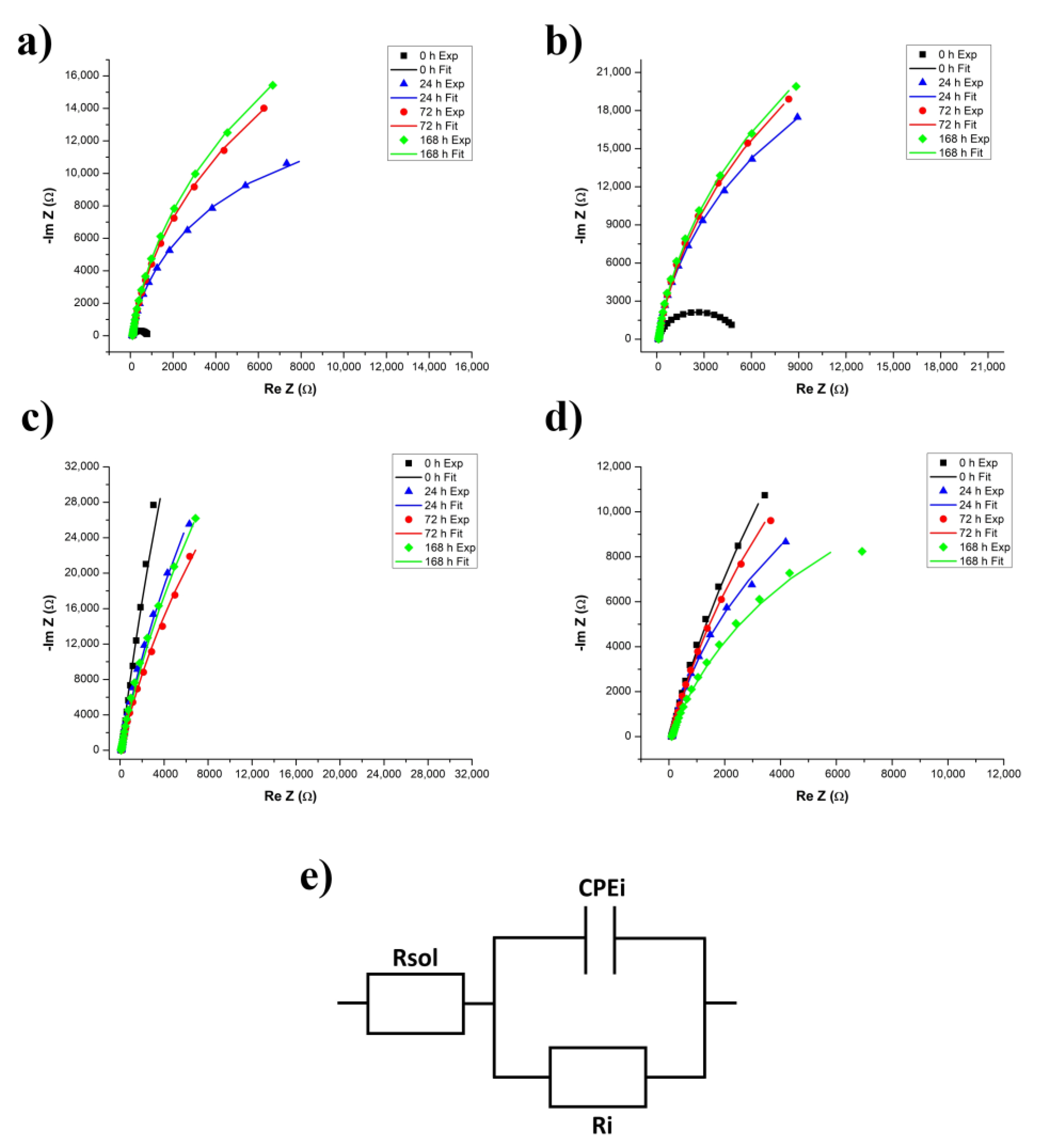
3.2.3. Electrochemical Impedance Spectroscopy
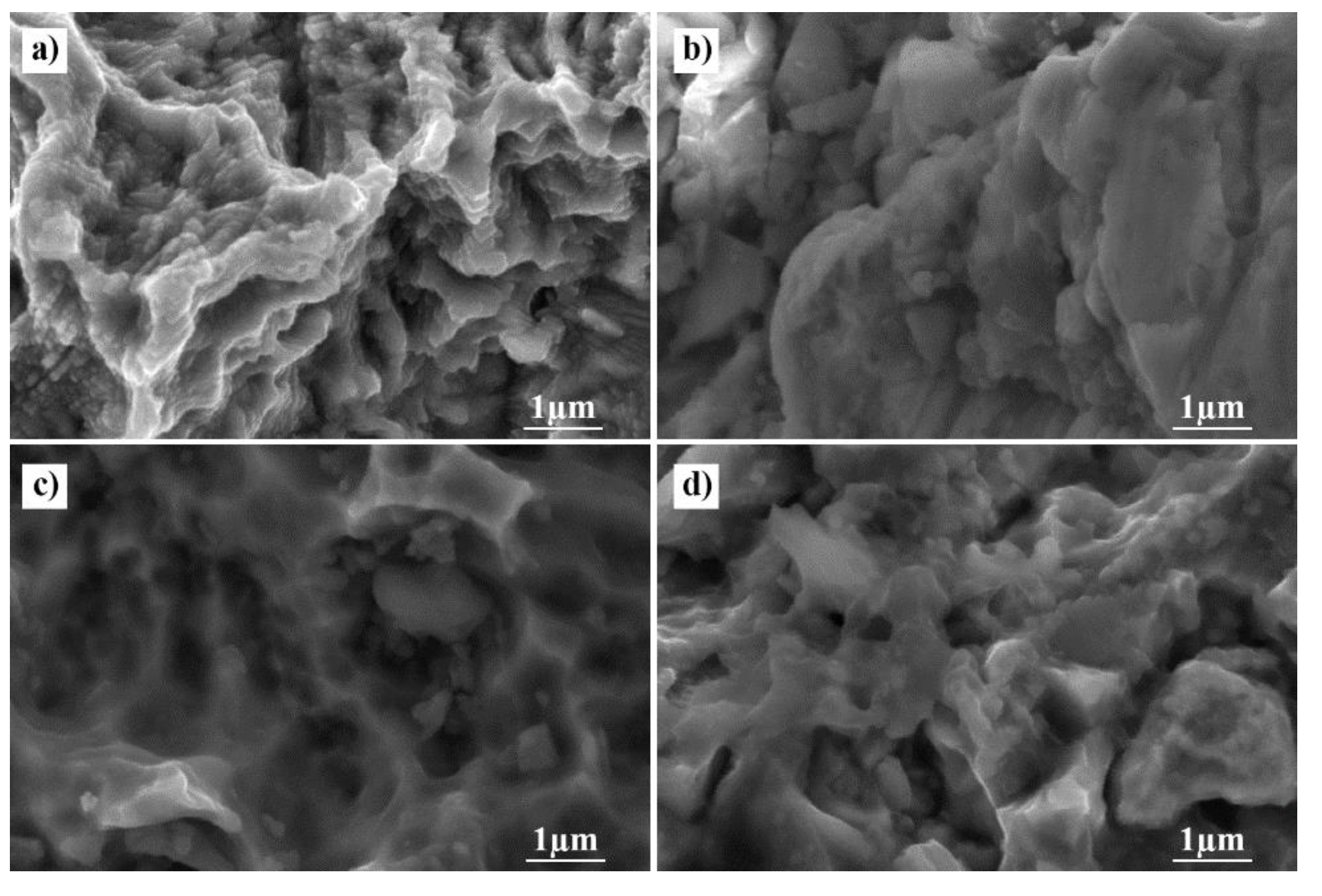
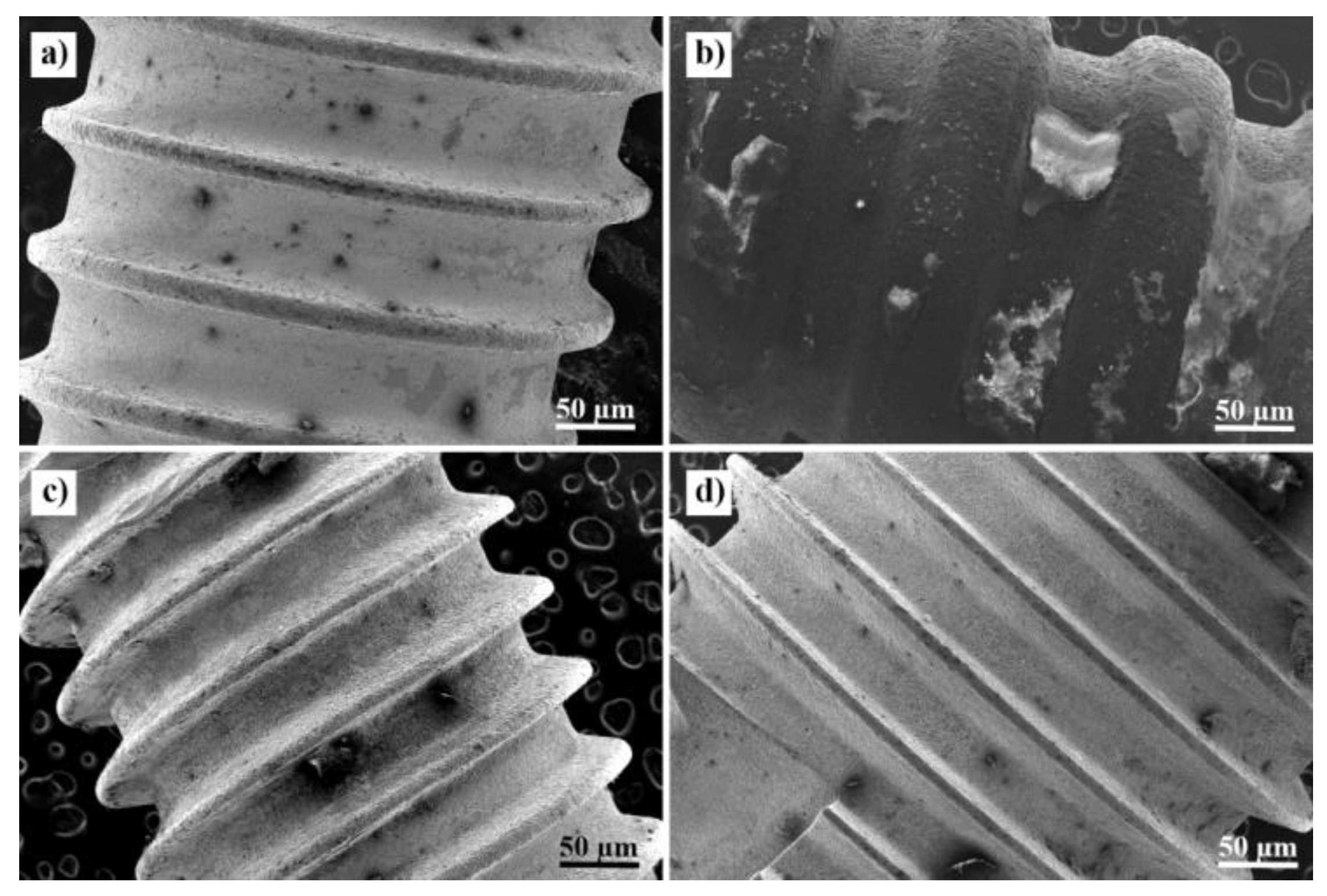
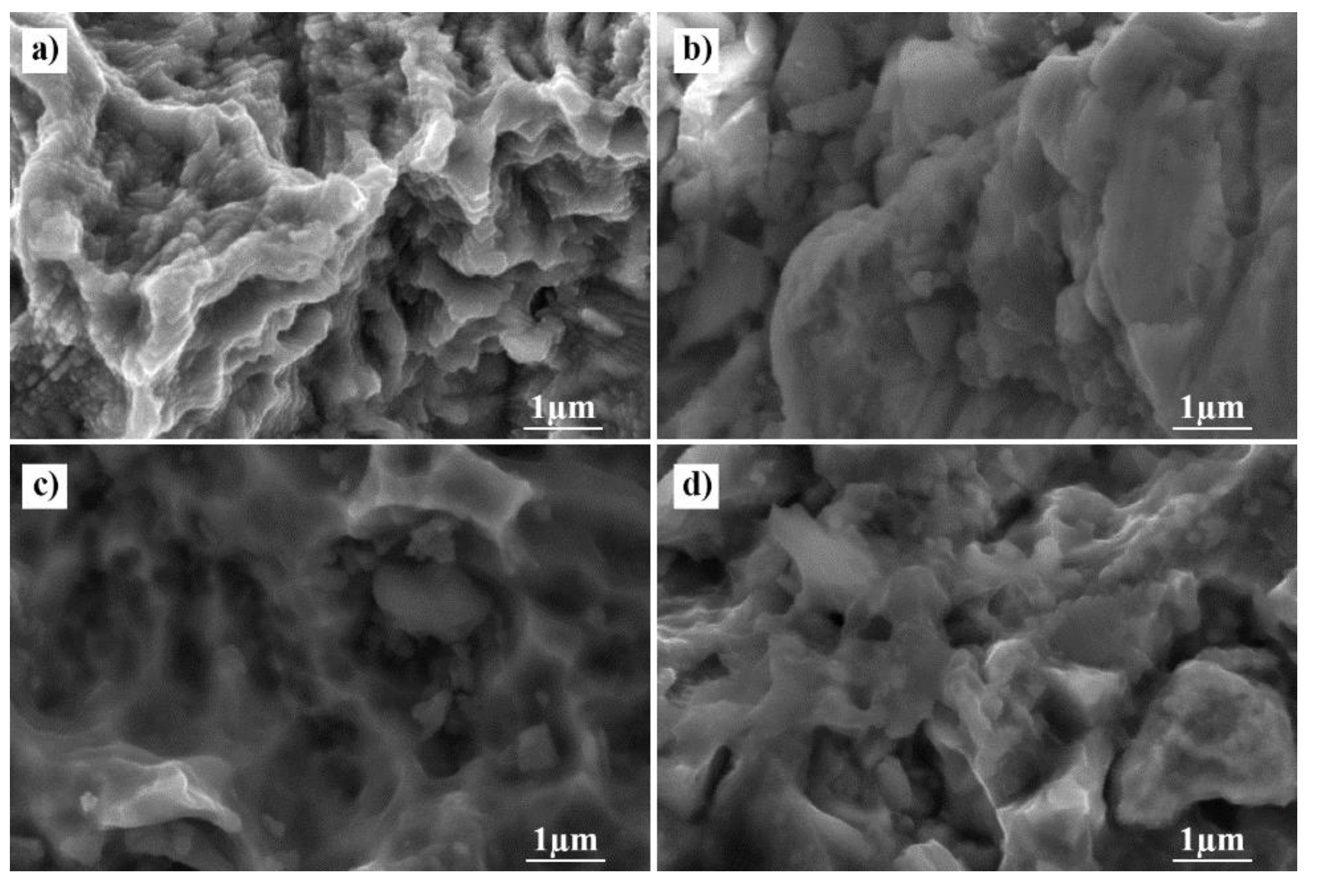
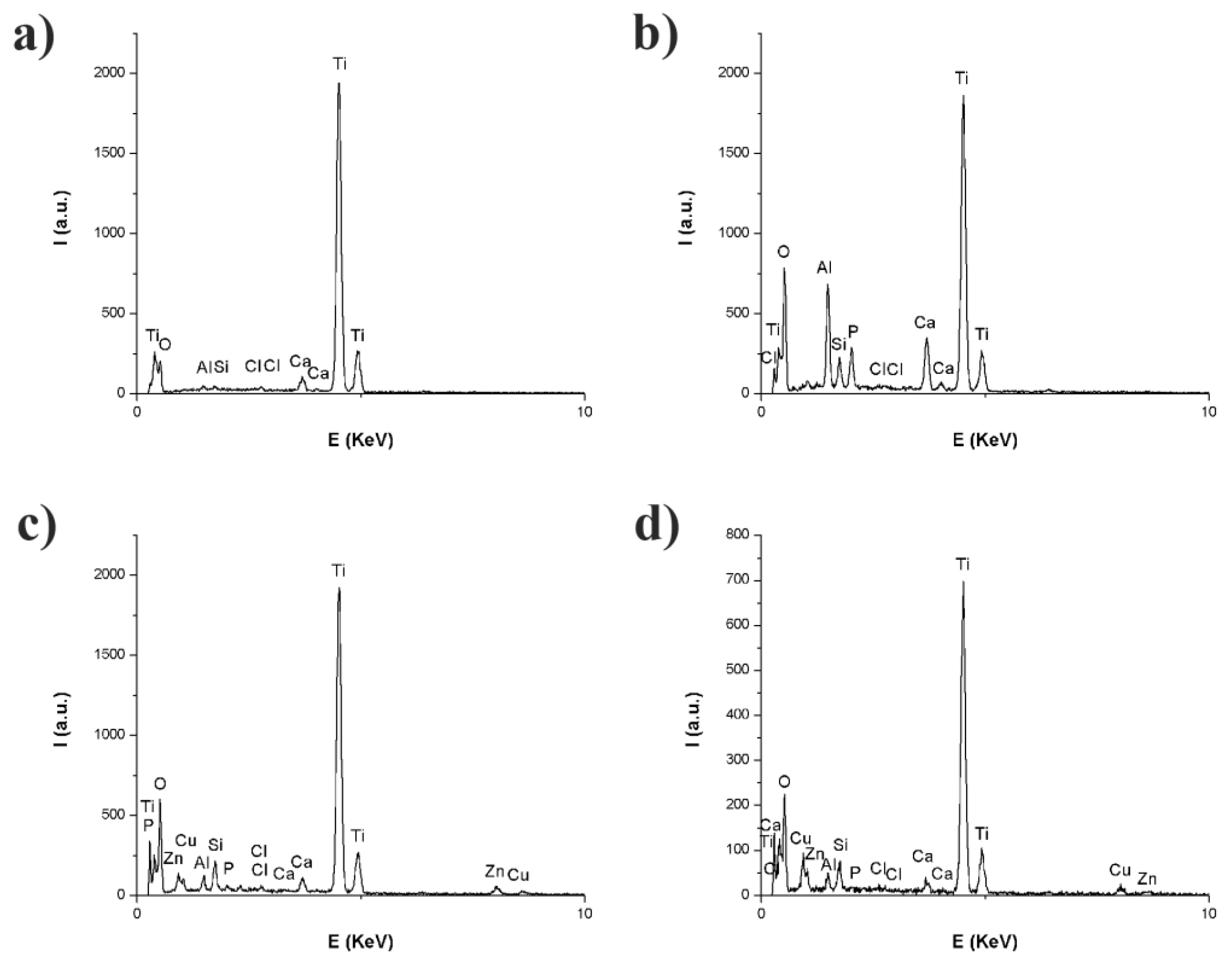
3.3. Scanning Electron Microscopy Coupled with an Energy Dispersive Spectroscopy Probe
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Mombelli, A. Microbiology and antimicrobial therapy of peri-implantitis. Periodontol 2000 2002, 28, 177–189. [Google Scholar] [CrossRef] [PubMed]
- Bunoiu, I.; Mindroiu, M.; Manole, C.C.; Andrei, M.; Nicoara, A.; Vasilescu, E.; Popa, M.; Didilescu, A.C. Electrochemical testing of a novel alloy in natural and artificial body fluids. Ann. Anat.-Anat. Anz. 2018, 217, 54–59. [Google Scholar] [CrossRef] [PubMed]
- Charyeva, O.; Altynbekov, K.; Zhartybaev, R.; Sabdanaliev, A. Long-term dental implant success and survival--a clinical study after an observation period up to 6 years. Swed. Dent. J. 2012, 36, 1–6. [Google Scholar] [PubMed]
- Smeets, R.; Henningsen, A.; Jung, O.; Heiland, M.; Hammacher, C.; Stein, J.M. Definition, etiology, prevention and treatment of peri-implantitis—A review. Head Face Med. 2014, 10, 34. [Google Scholar] [CrossRef] [Green Version]
- Zupnik, J.; Kim, S.W.; Ravens, D.; Karimbux, N.; Guze, K. Factors associated with dental implant survival: A 4-year retrospective analysis. J. Periodontol. 2011, 82, 1390–1395. [Google Scholar] [CrossRef]
- Matys, J.; Swider, K.; Flieger, R.; Dominiak, M. Assessment of the primary stability of root analog zirconia implants designed using cone beam computed tomography software by means of the Periotest(R) device: An ex vivo study. A preliminary report. Adv. Clin. Exp. Med. 2017, 26, 803–809. [Google Scholar] [CrossRef] [Green Version]
- Pi, B.; Bo, H.; Adell, R.; Breine, U.; Lindström, J.; Hallén, O.; Ohman, A. Osseointegrated implants in the treatment of the edentulous jaw. Experience from a 10-year period. Scand. J. Plast. Reconstr. Surg. Suppl. 1977, 16, 1–132. [Google Scholar]
- Smith, D.C. Dental implants: Materials and design considerations. Int. J. Prosthodont. 1993, 6, 106–117. [Google Scholar]
- Popa, M.V.; Demetrescu, I.; Iordachescu, D.; Cimpean, A.; Vasilescu, E.; Drob, P.; Vasilescu, C.; Istratescu, M. The relation between electrochemical tests and in vitro evaluation of titanium alloy biocompatibility. Mater. Corros. 2007, 58, 687–695. [Google Scholar] [CrossRef]
- Popa, M.; Demetrescu, I.; Vasilescu, E.; Drob, P.; Ionita, D.; Vasilescu, C. Stability of some dental implant materials in oral biofluids. Revue Roumaine de Chimie 2005, 50, 399–406. [Google Scholar]
- Matys, J.; Świder, K.; Grzech-Leśniak, K.; Dominiak, M.; Romeo, U. Photobiomodulation by a 635 nm diode laser on peri-implant bone: Primary and secondary stability and bone density analysis-a randomized clinical trial. Biomed. Res. Int. 2019, 2019, 2785302. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Spencer, P.; Misra, A. Material-tissue Interfacial Phenomena: Contributions from Dental and Craniofacial Reconstructions; Woodhead Publishing: Duxford, UK, 2016. [Google Scholar]
- Świder, K.; Dominiak, M.; Grzech-Leśniak, K.; Matys, J. Effect of different laser wavelengths on periodontopathogens in peri-implantitis: A review of in vivo studies. Microorganisms 2019, 7, 189. [Google Scholar] [CrossRef] [Green Version]
- Long, M.; Rack, H.J. Titanium alloys in total joint replacement—A materials science perspective. Biomaterials 1998, 19, 1621–1639. [Google Scholar] [CrossRef]
- Popa, M.; Vasilescu, E.; Drob, P.; Demetrescu, I.; Popescu, B.; Ionescu, D.; Vasilescu, C. In vitro assessment and monitoring of the implant titanium materials—Physiological environment interactions. Mater. Corros. 2003, 54, 215–221. [Google Scholar] [CrossRef]
- Demetrescu, I. Passive and bioactive films on implant materials and their efficiency in regenerative medicine. Mol. Cryst. Liq. Cryst. 2008, 486, 110–119. [Google Scholar] [CrossRef]
- Bosco, R.; van den Beucken, J.; Leeuwenburgh, S.; Jansen, J. Surface engineering for bone implants: A trend from passive to active surfaces. Coatings 2012, 2, 95–119. [Google Scholar] [CrossRef] [Green Version]
- Kasemo, B.; Lausmaa, J. Surface science aspects on inorganic biomaterials. CRC Crit. Rev. Clin. Neurobiol. 1986, 4, 6940374. [Google Scholar]
- Olmedo, D.G.; Tasat, D.R.; Duffó, G.; Guglielmotti, M.B.; Cabrini, R.L. The issue of corrosion in dental implants: A review. Acta Odontol Latinoam 2009, 22, 3–9. [Google Scholar]
- Zitzmann, N.U.; Berglundh, T. Definition and prevalence of peri-implant diseases. J. Clin. Periodontol. 2008, 35, 286–291. [Google Scholar] [CrossRef]
- Lindhe, J.; Meyle, J. Peri-implant diseases: Consensus report of the sixth european workshop on periodontology. J. Clin. Periodontol. 2008, 35, 282–285. [Google Scholar] [CrossRef] [Green Version]
- Froum, S.J.; Froum, S.H.; Rosen, P.S. Successful management of peri-implantitis with a regenerative approach: A consecutive series of 51 treated implants with 3-to 7.5-year follow-up. Int. J. Periodontics Restorative Dent. 2012, 32, 11. [Google Scholar] [PubMed]
- Salcetti, J.M.; Moriarty, J.D.; Cooper, L.F.; Smith, F.W.; Collins, J.G.; Socransky, S.S.; Offenbacher, S. The clinical, microbial, and host response characteristics of the failing implant. Int. J. Oral Maxillofac. Implant. 1997, 12, 32–42. [Google Scholar]
- Gherlone, E.F.; Cappare, P.; Tecco, S.; Polizzi, E.; Pantaleo, G.; Gastaldi, G.; Grusovin, M.G. A prospective longitudinal study on implant prosthetic rehabilitation in controlled HIV-positive patients with 1-year follow-up: The role of CD4+ level, smoking habits, and oral hygiene. Clin. Implant Dent. Relat. Res. 2016, 18, 955–964. [Google Scholar] [CrossRef] [PubMed]
- Gherlone, E.F.; Cappare, P.; Tecco, S.; Polizzi, E.; Pantaleo, G.; Gastaldi, G.; Grusovin, M.G. Implant prosthetic rehabilitation in controlled HIV-positive patients: A prospective longitudinal study with 1-year follow-up. Clin. Implant Dent. Relat. Res. 2016, 18, 725–734. [Google Scholar] [CrossRef]
- Cappare, P.; Tete, G.; Romanos, G.E.; Nagni, M.; Sannino, G.; Gherlone, E.F. The ‘All-on-four’ protocol in HIV-positive patients: A prospective, longitudinal 7-year clinical study. Int. J. Oral Implantol. (New Malden, London, England) 2019, 12, 501–510. [Google Scholar]
- Tecco, S.; Grusovin, M.G.; Sciara, S.; Bova, F.; Pantaleo, G.; Cappare, P. The association between three attitude-related indexes of oral hygiene and secondary implant failures: A retrospective longitudinal study. Int. J. Dent. Hyg. 2018, 16, 372–379. [Google Scholar] [CrossRef]
- Branemark, P.I. Osseointegration and its experimental background. J. Prosthet. Dent. 1983, 50, 399–410. [Google Scholar] [CrossRef]
- Bruschi, G.B.; Crespi, R.; Cappare, P.; Gherlone, E. Clinical study of flap design to increase the keratinized gingiva around implants: 4-year follow-up. J. Oral Implantol. 2014, 40, 459–464. [Google Scholar] [CrossRef]
- Rodriguez-Hernandez, A.G.; Juarez, A.; Engel, E.; Gil, F.J. Streptococcus sanguinis adhesion on titanium rough surfaces: Effect of shot-blasting particles. J. Mater. Sci. Mater. Med. 2011, 22, 1913–1922. [Google Scholar] [CrossRef]
- Gil, F.J.; Rodriguez, A.; Espinar, E.; Llamas, J.M.; Padulles, E.; Juarez, A. Effect of oral bacteria on the mechanical behavior of titanium dental implants. Int. J. Oral Maxillofac. Implant. 2012, 27, 64–68. [Google Scholar]
- Andrei, M.; Dinischiotu, A.; Didilescu, A.C.; Ionita, D.; Demetrescu, I. Periodontal materials and cell biology for guided tissue and bone regeneration. Ann. Anat.-Anat. Anz. 2018, 216, 164–169. [Google Scholar] [CrossRef] [PubMed]
- Pytko-Polonczyk, J.; Jakubik, A.; Przeklasa-Bierowiec, A.; Muszynska, B. Artificial saliva and its use in biological experiments. J. Physiol. Pharmacol. 2017, 68, 807–813. [Google Scholar]
- Siswanto, B.; Sudjatmoko, L.S.; Wirjoadi, R.M. Effects of nitrogen ion implantation on hardness and wear resistance of the Ti-6Al-4v alloy. Ganendra: Majalah IPTEK Nuklir 2015, 18, 61–68. [Google Scholar] [CrossRef]
- Sanchez-Garces, M.A.; Gay-Escoda, C. Periimplantitis. Med. Oral Patol. Oral Cir. Bucal. 2004, 9, 63–74. [Google Scholar]
- Ebadian, A.R.; Kadkhodazadeh, M.; Zarnegarnia, P.; Dahlen, G. Bacterial analysis of peri-implantitis and chronic periodontitis in Iranian subjects. Acta Med. Iran. 2012, 50, 486–492. [Google Scholar] [PubMed]
- Yeh, H.-C.; Lu, J.-J.; Chang, S.-C.; Ge, M.-C. Identification of microbiota in peri-implantitis pockets by matrix-assisted laser desorption/ionization time-of-flight mass spectrometry. Sci. Rep. 2019, 9, 774. [Google Scholar] [CrossRef]
- Ionita, D.; Mazare, A.; Portan, D.; Demetrescu, I. Aspects relating to stability of modified passive stratum on TiO2 nanostructure. Met. Mater. Int. 2011, 17, 321–327. [Google Scholar] [CrossRef]
- Scully, J. Polarization resistance method for determination of instantaneous corrosion rates. Corrosion 2000, 56, 199–204. [Google Scholar] [CrossRef]
- Liu, S.; Wang, B.; Zhang, P. Effect of glucose concentration on electrochemical corrosion behavior of pure titanium TA2 in Hanks’ simulated body fluid. Materials 2016, 9, 874. [Google Scholar] [CrossRef] [Green Version]
- Naujokat, H.; Kunzendorf, B.; Wiltfang, J. Dental implants and diabetes mellitus—A systematic review. Int. J. Implant Dent. 2017, 2. [Google Scholar] [CrossRef] [Green Version]
- de Almeida, P.D.V.; Grégio, A.M.T.; Machado, M.A.N.; de Lima, A.A.S.; Azevedo, L.R. Saliva composition and functions: A comprehensive review. J. Contemp. Dent. Pract. 2008, 9, 72–80. [Google Scholar]
- McCracken, M. Dental implant materials: Commercially pure titanium and titanium alloys. J. Prosthodont. 1999, 8, 40–43. [Google Scholar] [CrossRef] [PubMed]
- Smith, S.A.; Dale, B.A. Immunologic localization of filaggrin in human oral epithelia and correlation with keratinization. J. Invest. Dermatol. 1986, 86, 168–172. [Google Scholar] [CrossRef] [PubMed]
- Ovaere, P.; Lippens, S.; Vandenabeele, P.; Declercq, W. The emerging roles of serine protease cascades in the epidermis. Trends Biochem. Sci. 2009, 34, 453–463. [Google Scholar] [CrossRef]
- Poskevicius, L.; Sidlauskas, A.; Galindo-Moreno, P.; Juodzbalys, G. Dimensional soft tissue changes following soft tissue grafting in conjunction with implant placement or around present dental implants: A systematic review. Clin. Oral Implant. Res. 2017, 28, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Covani, U.; Marconcini, S.; Galassini, G.; Cornelini, R.; Santini, S.; Barone, A. Connective tissue graft used as a biologic barrier to cover an immediate implant. J. Periodontol. 2007, 78, 1644–1649. [Google Scholar] [CrossRef]
- Wennstrom, J.L.; Bengazi, F.; Lekholm, U. The influence of the masticatory mucosa on the peri-implant soft tissue condition. Clin. Oral Implant. Res. 1994, 5, 1–8. [Google Scholar] [CrossRef]
- Greenstein, G.; Cavallaro, J. The clinical significance of keratinized gingiva around dental implants. Compend. Contin. Educ. Dent. 2011, 32, 24–31. [Google Scholar]
- Park, J.B. Increasing the width of keratinized mucosa around endosseous implant using acellular dermal matrix allograft. Implant Dent. 2006, 15, 275–281. [Google Scholar] [CrossRef]
- Bergman, M.; Ginstrup, O.; Nilsson, B. Potentials of and currents between dental metallic restorations. Eur. J. Oral Sci. 1982, 90, 404–408. [Google Scholar] [CrossRef]
- Lee, A.K.; Newman, D.K. Microbial iron respiration: Impacts on corrosion processes. Appl. Microbiol. Biotechnol. 2003, 62, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Hansen, D.C. Metal corrosion in the human body: The ultimate bio-corrosion scenario. Electrochem. Soc. Interface 2008, 17, 31. [Google Scholar]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sample (Time) | Ecorr (V) | Jcorr (µA/cm2) | Icorr (µA) | Corrosion Rate (mm/year) | Polarization Resistance (kΩ) |
|---|---|---|---|---|---|
| Sample 1 (t = 0 h) | −0.0386 | 11.379 | 12.630 | 0.096932 | 2.614 |
| Sample 1 (t = 24 h) | 0.0461 | 0.462 | 0.513 | 0.003940 | 53.767 |
| Sample 1 (t = 72 h) | 0.1091 | 0.102 | 0.113 | 0.000873 | 437.67 |
| Sample 1 (t = 168 h) | 0.1086 | 0.094 | 0.105 | 0.000808 | 665.98 |
| Sample 2 (t = 0 h) | −0.0361 | 4.520 | 4.703 | 0.038507 | 8.67 |
| Sample 2 (t = 24 h) | 0.0783 | 0.023 | 0.021 | 0.000173 | 316.34 |
| Sample 2 (t = 72 h) | 0.0947 | 0.083 | 0.086 | 0.000709 | 464.66 |
| Sample 2 (t = 168 h) | 0.1053 | 0.019 | 0.019 | 0.000162 | 949.34 |
| Sample 3 (t = 0 h) | −0.0926 | 0.00015 | 0.001 | 0.000013 | 1907.70 |
| Sample 3 (t = 24 h) | −0.4110 | 0.331 | 0.407 | 0.002821 | 168.70 |
| Sample 3 (t = 72 h) | −0.0837 | 0.013 | 0.016 | 0.000115 | 642.49 |
| Sample 3 (t = 168 h) | −0.0392 | 0.017 | 0.021 | 0.000149 | 822.48 |
| Sample 4 (t = 0 h) | −0.5354 | 1.361 | 1.522 | 0.011599 | 27.75 |
| Sample 4 (t = 24 h) | −0.5635 | 8.208 | 9.176 | 0.069919 | 13.96 |
| Sample 4 (t = 72 h) | −0.3166 | 0.902 | 1.008 | 0.007683 | 55.66 |
| Sample 4 (t = 168 h) | −0.3439 | 3.082 | 3.446 | 0.026257 | 21.36 |
| Sample (Time) | Fusayama–Meyer Saliva | Dental Implant | X2 | ||
|---|---|---|---|---|---|
| Rsol (Ω) | Ri (Ω) | CPEi | |||
| n | Y0 (µMho) | ||||
| Sample 1 (t = 0 h) | 94.1 | 719 | 0.881 | 98.7 | 0.0109 |
| Sample 1 (t = 24 h) | 95.7 | 26,300 | 0.934 | 94.5 | 0.0193 |
| Sample 1 (t = 72 h) | 118 | 50,000 | 0.933 | 91.9 | 0.0142 |
| Sample 1 (t = 168 h) | 107 | 56,600 | 0.936 | 85.5 | 0.0147 |
| Sample 2 (t = 0 h) | 104 | 5150 | 0.884 | 66.6 | 0.0375 |
| Sample 2 (t = 24 h) | 114 | 55,900 | 0.927 | 70.9 | 0.0359 |
| Sample 2 (t = 72 h) | 134 | 72,000 | 0.921 | 70.7 | 0.0960 |
| Sample 2 (t = 168 h) | 116 | 75,000 | 0.927 | 67.2 | 0.0554 |
| Sample 3 (t = 0 h) | 88 | 1,000,000 | 0.913 | 57.3 | 0.1061 |
| Sample 3 (t = 24 h) | 101 | 295,000 | 0.909 | 59.6 | 0.0610 |
| Sample 3 (t = 72 h) | 113 | 200,000 | 0.889 | 62.4 | 0.0500 |
| Sample 3 (t = 168 h) | 89 | 277,000 | 0.9 | 56.1 | 0.0804 |
| Sample 4 (t = 0 h) | 86.7 | 115,000 | 0.873 | 136 | 0.0558 |
| Sample 4 (t = 24 h) | 105 | 36,000 | 0.891 | 148 | 0.0215 |
| Sample 4 (t = 72 h) | 110 | 66,500 | 0.882 | 143 | 0.0270 |
| Sample 4 (t = 168 h) | 101 | 29,000 | 0.829 | 126 | 0.0500 |
| Sample | Element % | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| O | Al | Si | P | S | Cl | Ca | Ti | Cu | Zn | |
| Sample 1 | 4.44 | 0.30 | 0.16 | 0.00 | 0.00 | 0.14 | 2.27 | 54.6 | 0.00 | 0.00 |
| Sample 2 | 58.7 | 6.59 | 1.56 | 2.43 | 0.00 | 0.15 | 4.21 | 26.3 | 0.00 | 0.00 |
| Sample 3 | 57.5 | 1.17 | 1.99 | 0.37 | 0.30 | 0.23 | 1.60 | 33.9 | 1.89 | 0.93 |
| Sample 4 | 58.9 | 1.37 | 1.95 | 0.30 | 0.18 | 0.30 | 1.21 | 33.0 | 1.64 | 1.10 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bunoiu, I.; Andrei, M.; Scheau, C.; Manole, C.C.; Stoian, A.B.; Ibric Cioranu, V.S.; Didilescu, A.C. Electrochemical Behavior of Rejected Dental Implants in Peri-Implantitis. Coatings 2020, 10, 209. https://doi.org/10.3390/coatings10030209
Bunoiu I, Andrei M, Scheau C, Manole CC, Stoian AB, Ibric Cioranu VS, Didilescu AC. Electrochemical Behavior of Rejected Dental Implants in Peri-Implantitis. Coatings. 2020; 10(3):209. https://doi.org/10.3390/coatings10030209
Chicago/Turabian StyleBunoiu, Ioana, Mihai Andrei, Cristian Scheau, Claudiu Constantin Manole, Andrei Bogdan Stoian, Vladimir Sorin Ibric Cioranu, and Andreea Cristiana Didilescu. 2020. "Electrochemical Behavior of Rejected Dental Implants in Peri-Implantitis" Coatings 10, no. 3: 209. https://doi.org/10.3390/coatings10030209
APA StyleBunoiu, I., Andrei, M., Scheau, C., Manole, C. C., Stoian, A. B., Ibric Cioranu, V. S., & Didilescu, A. C. (2020). Electrochemical Behavior of Rejected Dental Implants in Peri-Implantitis. Coatings, 10(3), 209. https://doi.org/10.3390/coatings10030209