Trends in Antimicrobial Susceptibility of Escherichia coli Isolates in a Taiwanese Child Cohort with Urinary Tract Infections between 2004 and 2018



Abstract
1. Introduction
2. Materials and Methods
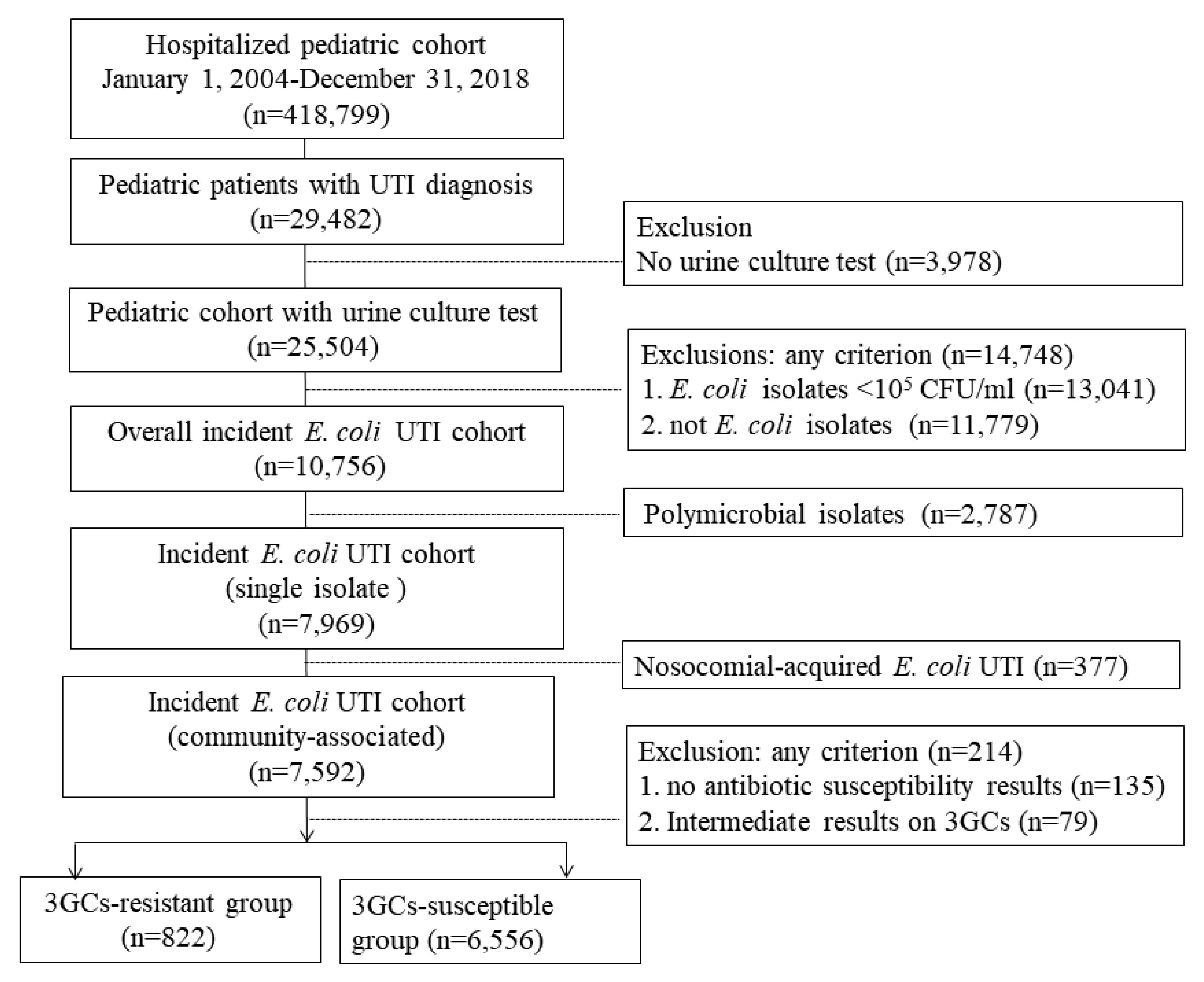
2.1. Study Design and Data Source
2.2. Outcome Measurements
2.3. Statistical Analysis
3. Results
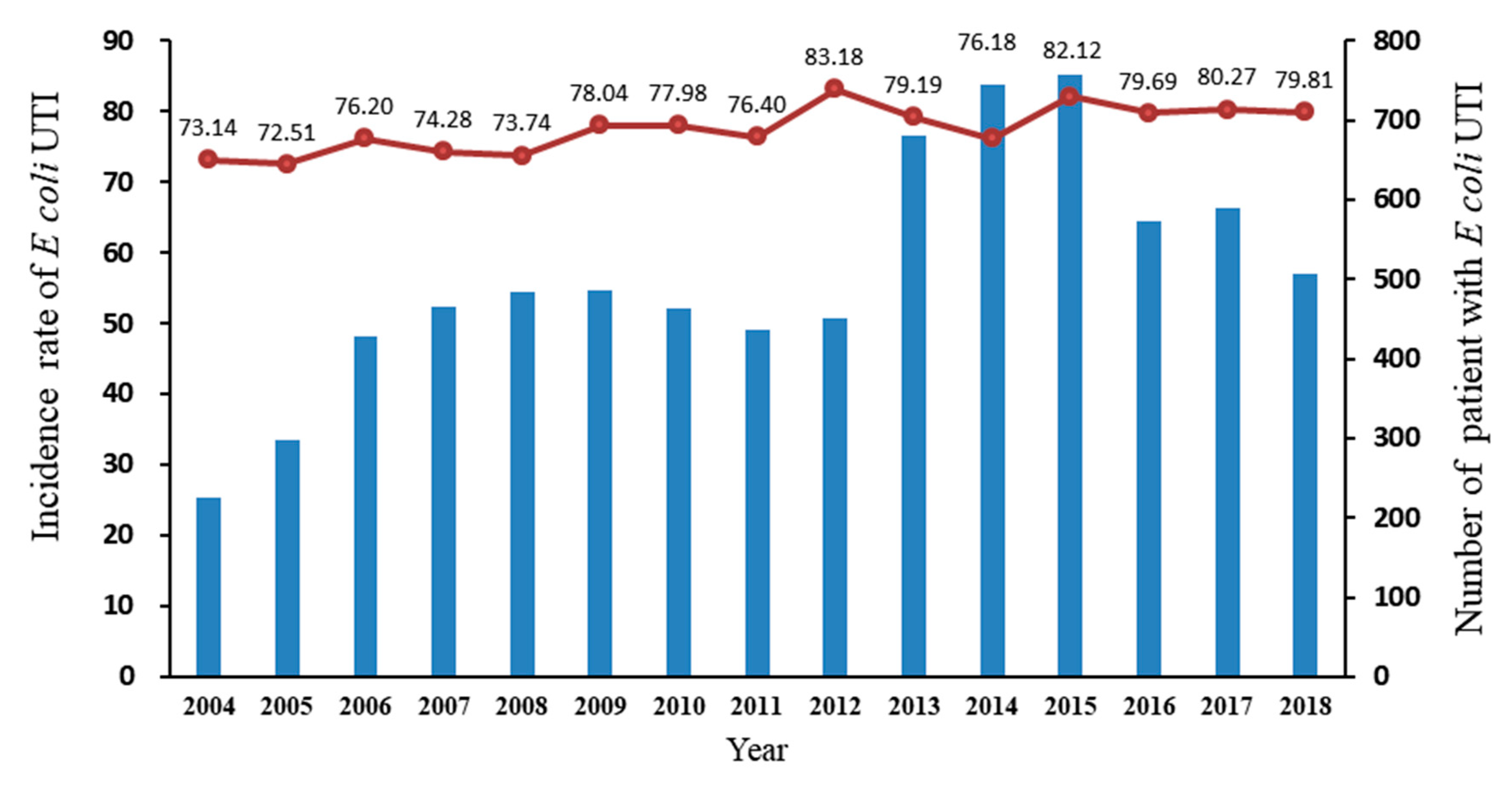
3.1. Incidence of E. coli in Community-Associated UTIs
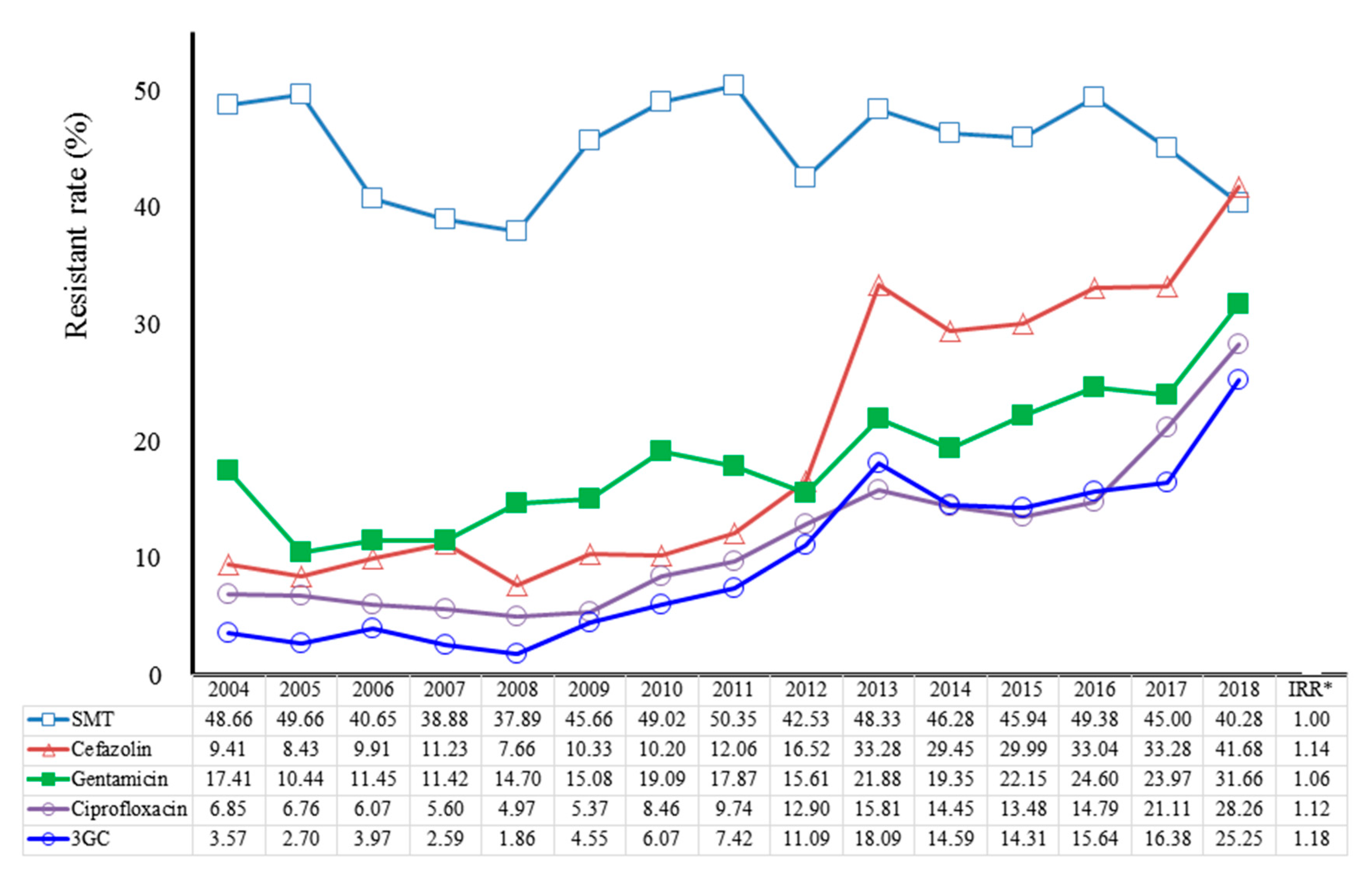
3.2. Trends in Antimicrobial-Drugs-Resistant E. coli Isolates in CA-UTIs
3.3. Outcomes and Factors Associated with E. coli Resistance to Third Generation Cephalosporin
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Shaikh, N.; Ewing, A.L.; Bhatnagar, S.; Hoberman, A. Risk of renal scarring in children with a first urinary tract infection: A systematic review. Pediatrics 2010, 126, 1084–1091. [Google Scholar] [CrossRef]
- Korbel, L.; Howell, M.; Spencer, J.D. The clinical diagnosis and management of urinary tract infections in children and adolescents. Paediatr. Int. Child Health 2017, 37, 273–279. [Google Scholar] [CrossRef]
- Leung, A.K.C.; Wong, A.H.C.; Leung, A.A.M.; Hon, K.L. Urinary Tract Infection in Children. Recent. Pat. Inflamm. Allergy Drug Discov. 2019, 13, 2–18. [Google Scholar] [CrossRef]
- Wang, J.T.; Chang, S.C.; Chang, F.Y.; Fung, C.P.; Chuang, Y.C.; Chen, Y.S.; Shiau, Y.R.; Tan, M.C.; Wang, H.Y.; Lai, J.F.; et al. Antimicrobial Non-Susceptibility of Escherichia coli from Outpatients and Patients Visiting Emergency Rooms in Taiwan. PLoS ONE 2015, 10, e0144103. [Google Scholar] [CrossRef]
- Lin, W.P.; Huang, Y.S.; Wang, J.T.; Chen, Y.C.; Chang, S.C. Prevalence of and risk factor for community-onset third-generation cephalosporin-resistant Escherichia coli bacteremia at a medical center in Taiwan. BMC Infect. Dis. 2019, 19, 245. [Google Scholar] [CrossRef]
- Parajuli, N.P.; Maharjan, P.; Parajuli, H.; Joshi, G.; Paudel, D.; Sayami, S.; Khanal, P.R. High rates of multidrug resistance among uropathogenic Escherichia coli in children and analyses of ESBL producers from Nepal. Antimicrob. Resist. Infect. Control 2017, 6, 9. [Google Scholar] [CrossRef]
- Mazzariol, A.; Bazaj, A.; Cornaglia, G. Multi-drug-resistant Gram-negative bacteria causing urinary tract infections: A review. J. Chemother. 2017, 29, 2–9. [Google Scholar] [CrossRef]
- Paterson, D.L.; Bonomo, R.A. Extended-spectrum beta-lactamases: A clinical update. Clin. Microbiol. Rev. 2005, 18, 657–686. [Google Scholar] [CrossRef] [PubMed]
- Flokas, M.E.; Detsis, M.; Alevizakos, M.; Mylonakis, E. Prevalence of ESBL-producing Enterobacteriaceae in paediatric urinary tract infections: A systematic review and meta-analysis. J. Infect. 2016, 73, 547–557. [Google Scholar] [CrossRef] [PubMed]
- Sood, A.; Penna, F.J.; Eleswarapu, S.; Pucheril, D.; Weaver, J.; Abd-El-Barr, A.E.; Wagner, J.C.; Lakshmanan, Y.; Menon, M.; Trinh, Q.D.; et al. Incidence, admission rates, and economic burden of pediatric emergency department visits for urinary tract infection: Data from the nationwide emergency department sample, 2006 to 2011. J. Pediatr. Urol. 2015, 11, 246.e1–246.e8. [Google Scholar] [CrossRef] [PubMed]
- Fan, N.C.; Chen, H.H.; Chen, C.L.; Ou, L.S.; Lin, T.Y.; Tsai, M.H.; Chiu, C.H. Rise of community-onset urinary tract infection caused by extended-spectrum beta-lactamase-producing Escherichia coli in children. J. Microbiol. Immunol. Infect. 2014, 47, 399–405. [Google Scholar] [CrossRef] [PubMed]
- Vihta, K.D.; Stoesser, N.; Llewelyn, M.J.; Quan, T.P.; Davies, T.; Fawcett, N.J.; Dunn, L.; Jeffery, K.; Butler, C.C.; Hayward, G.; et al. Trends over time in Escherichia coli bloodstream infections, urinary tract infections, and antibiotic susceptibilities in Oxfordshire, UK, 1998-2016: A study of electronic health records. Lancet Infect. Dis. 2018, 18, 1138–1149. [Google Scholar] [CrossRef]
- McDanel, J.; Schweizer, M.; Crabb, V.; Nelson, R.; Samore, M.; Khader, K.; Blevins, A.E.; Diekema, D.; Chiang, H.Y.; Nair, R.; et al. Incidence of Extended-Spectrum beta-Lactamase (ESBL)-Producing Escherichia coli and Klebsiella Infections in the United States: A Systematic Literature Review. Infect. Control Hosp. Epidemiol. 2017, 38, 1209–1215. [Google Scholar] [CrossRef] [PubMed]
- Kizilca, O.; Siraneci, R.; Yilmaz, A.; Hatipoglu, N.; Ozturk, E.; Kiyak, A.; Ozkok, D. Risk factors for community-acquired urinary tract infection caused by ESBL-producing bacteria in children. Pediatr. Int. 2012, 54, 858–862. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.H.; Yang, E.M.; Kim, C.J.; Hernandez Marco, R.; Guillen Olmos, E.; Breton-Martinez, J.R.; Giner Perez, L.; Casado Sanchez, B.; Fujkova, J.; Salamanca Campos, M.; et al. Urinary tract infection caused by community-acquired extended-spectrum beta-lactamase-producing bacteria in infants. J. Pediatr. 2017, 93, 260–266. [Google Scholar] [CrossRef] [PubMed]
- Zhu, F.H.; Rodado, M.P.; Asmar, B.I.; Salimnia, H.; Thomas, R.; Abdel-Haq, N. Risk factors for community acquired urinary tract infections caused by extended spectrum beta-lactamase (ESBL) producing Escherichia coli in children: A case control study. Infect. Dis. 2019, 51, 802–809. [Google Scholar] [CrossRef]
- Roldan-Masedo, E.; Sainz, T.; Gutierrez-Arroyo, A.; Gomez-Gil, R.M.; Ballesteros, E.; Escosa, L.; Baquero-Artigao, F.; Mendez-Echevarria, A. Risk factors for gentamicin-resistant E. coli in children with community-acquired urinary tract infection. Eur. J. Clin. Microbiol. Infect. Dis. 2019, 38, 2097–2102. [Google Scholar] [CrossRef]
- Chen, P.C.; Chang, L.Y.; Lu, C.Y.; Shao, P.L.; Tsai, I.J.; Tsau, Y.K.; Lee, P.I.; Chen, J.M.; Hsueh, P.R.; Huang, L.M. Drug susceptibility and treatment response of common urinary tract infection pathogens in children. J. Microbiol. Immunol. Infect. 2014, 47, 478–483. [Google Scholar] [CrossRef]
- Cheng, M.F.; Chen, W.L.; Hung, W.Y.; Huang, I.F.; Chiou, Y.H.; Chen, Y.S.; Lee, S.S.; Hung, C.H.; Wang, J.L. Emergence of extended spectrum-beta-lactamase-producing Escherichia coli O25b-ST131: A major community-acquired uropathogen in infants. Pediatr. Infect. Dis. J. 2015, 34, 469–475. [Google Scholar] [CrossRef]
- Perez Heras, I.; Sanchez-Gomez, J.C.; Beneyto-Martin, P.; Ruano-de-Pablo, L.; Losada-Pinedo, B. Community-onset extended-spectrum beta-lactamase producing Escherichia coli in urinary tract infections in children from 2015 to 2016: Prevalence, risk factors, and resistances. Medicine 2017, 96, e8571. [Google Scholar] [CrossRef]
- Shao, S.C.; Chan, Y.Y.; Kao Yang, Y.H.; Lin, S.J.; Hung, M.J.; Chien, R.N.; Lai, C.C.; Lai, E.C. The Chang Gung Research Database-A multi-institutional electronic medical records database for real-world epidemiological studies in Taiwan. Pharmacoepidemiol. Drug Saf. 2019, 28, 593–600. [Google Scholar] [CrossRef] [PubMed]
- Stein, R.; Dogan, H.S.; Hoebeke, P.; Kocvara, R.; Nijman, R.J.; Radmayr, C.; Tekgul, S.; European Association of Urology; European Society for Pediatric Urology. Urinary tract infections in children: EAU/ESPU guidelines. Eur. Urol. 2015, 67, 546–558. [Google Scholar] [CrossRef] [PubMed]
- Subcommittee on Urinary Tract Infection; Steering Committee on Quality Improvement and Management; Roberts, K.B. Urinary tract infection: Clinical practice guideline for the diagnosis and management of the initial UTI in febrile infants and children 2 to 24 months. Pediatrics 2011, 128, 595–610. [Google Scholar] [CrossRef] [PubMed]
- Horan, T.C.; Andrus, M.; Dudeck, M.A. CDC/NHSN surveillance definition of health care–associated infection and criteria for specific types of infections in the acute care setting. Am. J. Infect. Control 2008, 36, 309–332. [Google Scholar] [CrossRef] [PubMed]
- Simon, T.D.; Cawthon, M.L.; Popalisky, J.; Mangione-Smith, R. Development and Validation of the Pediatric Medical Complexity Algorithm (PMCA) Version 2.0. Hosp. Pediatr. 2017, 7, 373–377. [Google Scholar] [CrossRef]
- Simon, T.D.; Haaland, W.; Hawley, K.; Lambka, K.; Mangione-Smith, R. Development and Validation of the Pediatric Medical Complexity Algorithm (PMCA) Version 3.0. Acad. Pediatr. 2018, 18, 577–580. [Google Scholar] [CrossRef]
- Morrissey, I.; Hackel, M.; Badal, R.; Bouchillon, S.; Hawser, S.; Biedenbach, D. A Review of Ten Years of the Study for Monitoring Antimicrobial Resistance Trends (SMART) from 2002 to 2011. Pharmaceuticals 2013, 6, 1335–1346. [Google Scholar] [CrossRef]
- Fasugba, O.; Gardner, A.; Mitchell, B.G.; Mnatzaganian, G. Ciprofloxacin resistance in community- and hospital-acquired Escherichia coli urinary tract infections: A systematic review and meta-analysis of observational studies. BMC Infect. Dis. 2015, 15, 545. [Google Scholar] [CrossRef]
- Hernandez Marco, R.; Guillen Olmos, E.; Breton-Martinez, J.R.; Giner Perez, L.; Casado Sanchez, B.; Fujkova, J.; Salamanca Campos, M.; Nogueira Coito, J.M. Community-acquired febrile urinary tract infection caused by extended-spectrum beta-lactamase-producing bacteria in hospitalised infants. Enferm. Infecc. Microbiol. Clin. 2017, 35, 287–292. [Google Scholar] [CrossRef]
- Cohen, E.; Kuo, D.Z.; Agrawal, R.; Berry, J.G.; Bhagat, S.K.; Simon, T.D.; Srivastava, R. Children with medical complexity: An emerging population for clinical and research initiatives. Pediatrics 2011, 127, 529–538. [Google Scholar] [CrossRef]
- Edwards, J.D.; Houtrow, A.J.; Vasilevskis, E.E.; Rehm, R.S.; Markovitz, B.P.; Graham, R.J.; Dudley, R.A. Chronic conditions among children admitted to U.S. pediatric intensive care units: Their prevalence and impact on risk for mortality and prolonged length of stay*. Crit. Care Med. 2012, 40, 2196–2203. [Google Scholar] [CrossRef] [PubMed]
- Topaloglu, R.; Er, I.; Dogan, B.G.; Bilginer, Y.; Ozaltin, F.; Besbas, N.; Ozen, S.; Bakkaloglu, A.; Gur, D. Risk factors in community-acquired urinary tract infections caused by ESBL-producing bacteria in children. Pediatr. Nephrol. 2010, 25, 919–925. [Google Scholar] [CrossRef] [PubMed]
- Zegers, S.H.; Dieleman, J.; van der Bruggen, T.; Kimpen, J.; de Jong-de Vos van Steenwijk, C. The influence of antibiotic prophylaxis on bacterial resistance in urinary tract infections in children with spina bifida. BMC Infect. Dis. 2017, 17, 63. [Google Scholar] [CrossRef]
- Shaikh, N.; Craig, J.C.; Rovers, M.M.; Da Dalt, L.; Gardikis, S.; Hoberman, A.; Montini, G.; Rodrigo, C.; Taskinen, S.; Tuerlinckx, D.; et al. Identification of children and adolescents at risk for renal scarring after a first urinary tract infection: A meta-analysis with individual patient data. JAMA Pediatr. 2014, 168, 893–900. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.E.; Lee, V.; Greenhow, T.L.; Beck, J.; Bendel-Stenzel, M.; Hames, N.; McDaniel, C.E.; King, E.E.; Sherry, W.; Parmar, D.; et al. Clinical Response to Discordant Therapy in Third-Generation Cephalosporin-Resistant UTIs. Pediatrics 2020, 145, e20191608. [Google Scholar] [CrossRef] [PubMed]
- Shaikh, N.; Hoberman, A.; Hum, S.W.; Alberty, A.; Muniz, G.; Kurs-Lasky, M.; Landsittel, D.; Shope, T. Development and Validation of a Calculator for Estimating the Probability of Urinary Tract Infection in Young Febrile Children. JAMA Pediatr. 2018, 172, 550–556. [Google Scholar] [CrossRef]
- Zingg, W.; Hopkins, S.; Gayet-Ageron, A.; Holmes, A.; Sharland, M.; Suetens, C.; Almeida, M.; Asembergiene, J.; Borg, M.A.; Budimir, A. Health-care-associated infections in neonates, children, and adolescents: An analysis of paediatric data from the European Centre for Disease Prevention and Control point-prevalence survey. Lancet Infect. Dis. 2017, 17, 381–389. [Google Scholar] [CrossRef]
- Downs, S.M. Technical report: Urinary tract infections in febrile infants and young children. The Urinary Tract Subcommittee of the American Academy of Pediatrics Committee on Quality Improvement. Pediatrics 1999, 103, e54. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Heading | Overall * | 3GCs-Resistant (n = 822) | 3GCs-Susceptible (n = 6556) | p-Value # | ||
|---|---|---|---|---|---|---|
| N | n | (%) | n | (%) | ||
| In-hospital death | 27 | 6 | (0.73) | 21 | (0.32) | 0.1133 |
| Length of stay (day), | <0.0001 | |||||
| Mean (SD) | 7378 | 8.09 | (4.59) | 6.78 | (3.53) | |
| Median (IQR) | 7.00 | (5.00–10.00) | 6.00 | (5.00–8.00) | ||
| Discharge diagnosis with bacteremia | 311 | 45 | (5.47) | 266 | (4.06) | 0.0566 |
| E. coli | 106 | 13 | (1.58) | 93 | (1.42) | 0.7113 |
| Heading | Overall * | 3GCs-Resistant (n = 822) | 3GCs-Susceptible (n = 6556) | p-Value # | ||
|---|---|---|---|---|---|---|
| n | n | (%) | n | (%) | ||
| Age at admission | 0.4516 | |||||
| ≤28 days | 379 | 39 | (4.74) | 340 | (5.19) | |
| 29 days to < 1 year | 5534 | 634 | (77.13) | 4900 | (74.74) | |
| 1 to 2 years | 808 | 86 | (10.46) | 722 | (11.01) | |
| 3 to 17 years | 657 | 63 | (7.66) | 594 | (9.06) | |
| Sex | 0.0415 | |||||
| Boys | 4189 | 494 | (60.10) | 3695 | (56.36) | |
| Girls | 3189 | 328 | (39.90) | 2861 | (43.64) | |
| Recent medical visits ≤ 3 months prior, visit | ||||||
| Outpatient | 0.4501 | |||||
| None | 6410 | 721 | (87.71) | 5689 | (86.78) | |
| 1–3 | 722 | 71 | (8.64) | 651 | (9.93) | |
| ≥4 | 246 | 30 | (3.65) | 216 | (3.29) | |
| Emergency department | 0.2825 | |||||
| None | 6911 | 764 | (92.94) | 6147 | (93.76) | |
| 1 | 365 | 49 | (5.96) | 316 | (4.82) | |
| ≥2 | 102 | 9 | (1.09) | 93 | (1.42) | |
| Hospitalization | 0.0834 | |||||
| None | 7070 | 784 | (95.38) | 6286 | (95.88) | |
| 1 | 279 | 31 | (3.77) | 248 | (3.78) | |
| ≥2 | 29 | 7 | (0.85) | 22 | (0.34) | |
| PMCA, CD | <0.0001 | |||||
| Without CD | 6640 | 724 | (88.08) | 5916 | (90.24) | |
| Non-complex CD | 442 | 40 | (4.87) | 402 | (6.13) | |
| Complex CD | 296 | 58 | (7.06) | 238 | (3.63) | |
| Recent antibiotic treatment ≤ 3 months prior | ||||||
| Sum of regimen | <0.0001 | |||||
| None | 6427 | 674 | (82.00) | 5753 | (87.75) | |
| 1 | 515 | 79 | (9.61) | 436 | (6.65) | |
| ≥2 | 436 | 69 | (8.39) | 367 | (5.60) | |
| Amoxicillin/clavulanic acid | 286 | 49 | (5.96) | 237 | (3.62) | 0.0010 |
| Amikacin | 11 | 6 | (0.73) | 5 | (0.08) | <0.0001 |
| Ciprofloxacin | 9 | 5 | (0.61) | 4 | (0.06) | <0.0001 |
| Ceftriaxone | 38 | 9 | (1.09) | 29 | (0.44) | 0.0137 |
| Cefazolin | 37 | 10 | (1.22) | 27 | (0.41) | 0.0021 |
| Ertapenem | 412 | 63 | (7.66) | 349 | (5.32) | 0.0059 |
| Gentamicin | 550 | 75 | (9.12) | 475 | (7.25) | 0.0532 |
| Levofloxacin | 1 | 0 | (0.00) | 1 | (0.02) | -- |
| Sulfamethoxazole–Trimethoprim | 133 | 36 | (4.38) | 97 | (1.48) | <0.0001 |
| Piperacillin/Tazobactam | 2 | 1 | (0.12) | 1 | (0.02) | -- |
| Heading | aOR | 95%CI | p-Value | |
|---|---|---|---|---|
| Age at index hospitalization | ||||
| ≤28 days | 1 | |||
| 29 days to < 1 year | 1.08 | (0.77 | 1.52) | 0.6589 |
| 1 to 2 years | 0.98 | (0.65 | 1.47) | 0.9059 |
| 3 to 17 years | 0.80 | (0.51 | 1.24) | 0.3075 |
| Boy (vs. girl) | 1.13 | (0.96 | 1.32) | 0.1337 |
| Healthcare service use ≤3 months prior, visit | ||||
| Outpatient setting | ||||
| None | 1 | |||
| 1–3 | 0.80 | (0.60 | 1.08) | 0.1449 |
| ≥4 | 0.70 | (0.43 | 1.13) | 0.1434 |
| Emergency department | ||||
| None | 1 | |||
| 1 | 1.34 | (0.95 | 1.88) | 0.0910 |
| ≥2 | 0.77 | (0.37 | 1.59) | 0.4785 |
| Hospitalization | ||||
| None | 1 | |||
| 1 | 0.98 | (0.63 | 1.53) | 0.9414 |
| ≥2 | 2.15 | (0.83 | 5.58) | 0.1176 |
| PMCA, CD | ||||
| Non-Chronic | 1 | |||
| Non-complex Chronic | 0.83 | (0.59 | 1.18) | 0.3005 |
| Complex Chronic | 2.04 | (1.47 | 2.83) | <0.0001 |
| Sum of antibiotic regimen use ≤ 3 months prior | ||||
| None | 1 | |||
| 1 | 1.49 | (1.15 | 1.94) | 0.0031 |
| ≥2 | 1.53 | (1.16 | 2.02) | 0.0024 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, H.-E.; Tain, Y.-L.; Kuo, H.-C.; Hsu, C.-N. Trends in Antimicrobial Susceptibility of Escherichia coli Isolates in a Taiwanese Child Cohort with Urinary Tract Infections between 2004 and 2018. Antibiotics 2020, 9, 501. https://doi.org/10.3390/antibiotics9080501
Chen H-E, Tain Y-L, Kuo H-C, Hsu C-N. Trends in Antimicrobial Susceptibility of Escherichia coli Isolates in a Taiwanese Child Cohort with Urinary Tract Infections between 2004 and 2018. Antibiotics. 2020; 9(8):501. https://doi.org/10.3390/antibiotics9080501
Chicago/Turabian StyleChen, Hung-En, You-Lin Tain, Hsiao-Ching Kuo, and Chien-Ning Hsu. 2020. "Trends in Antimicrobial Susceptibility of Escherichia coli Isolates in a Taiwanese Child Cohort with Urinary Tract Infections between 2004 and 2018" Antibiotics 9, no. 8: 501. https://doi.org/10.3390/antibiotics9080501
APA StyleChen, H.-E., Tain, Y.-L., Kuo, H.-C., & Hsu, C.-N. (2020). Trends in Antimicrobial Susceptibility of Escherichia coli Isolates in a Taiwanese Child Cohort with Urinary Tract Infections between 2004 and 2018. Antibiotics, 9(8), 501. https://doi.org/10.3390/antibiotics9080501