Meropenem Plasma and Interstitial Soft Tissue Concentrations in Obese and Nonobese Patients—A Controlled Clinical Trial

 ,
,  , ,
, ,  ,
,
Abstract
1. Introduction
2. Results
2.1. Patients
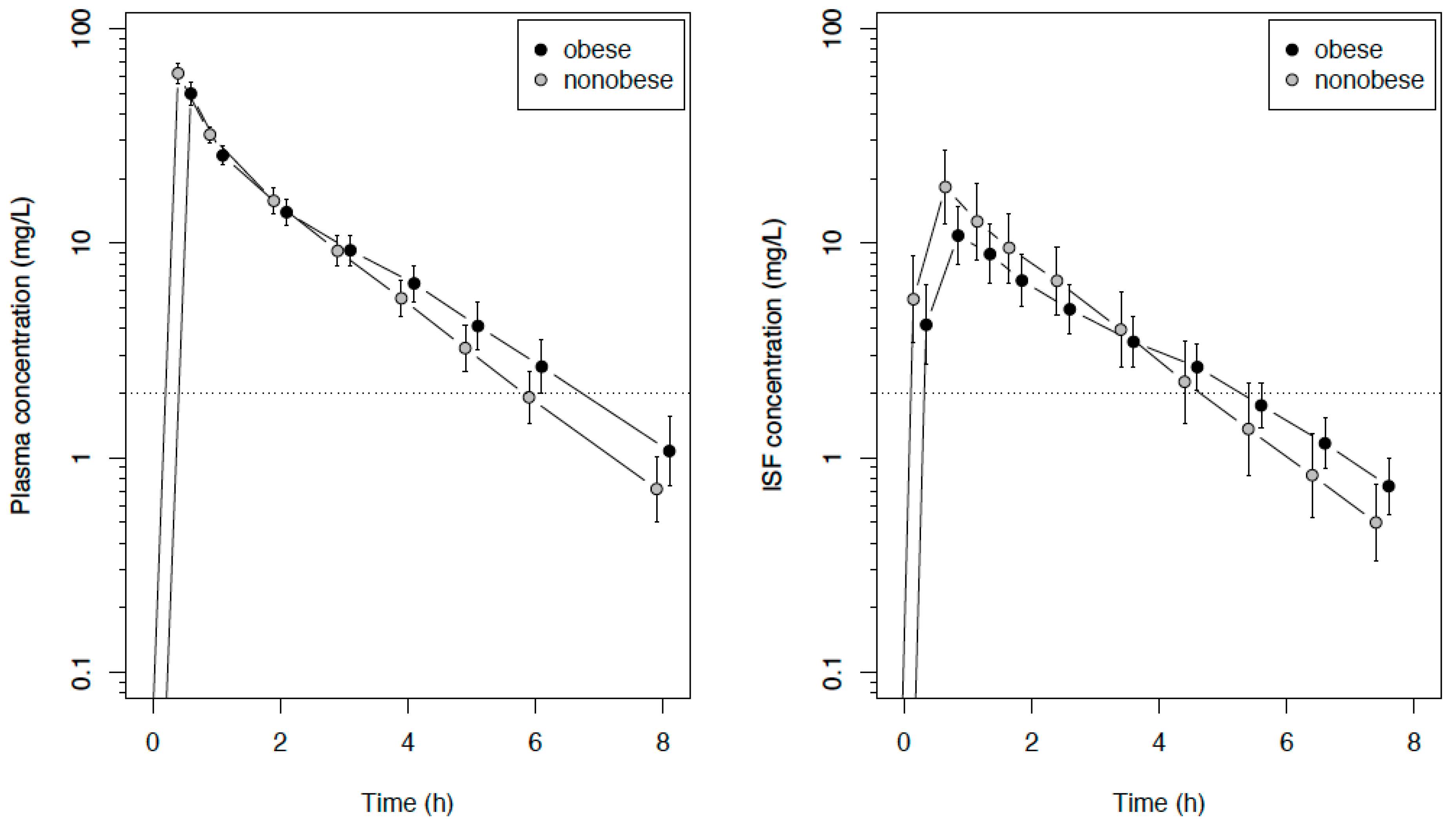
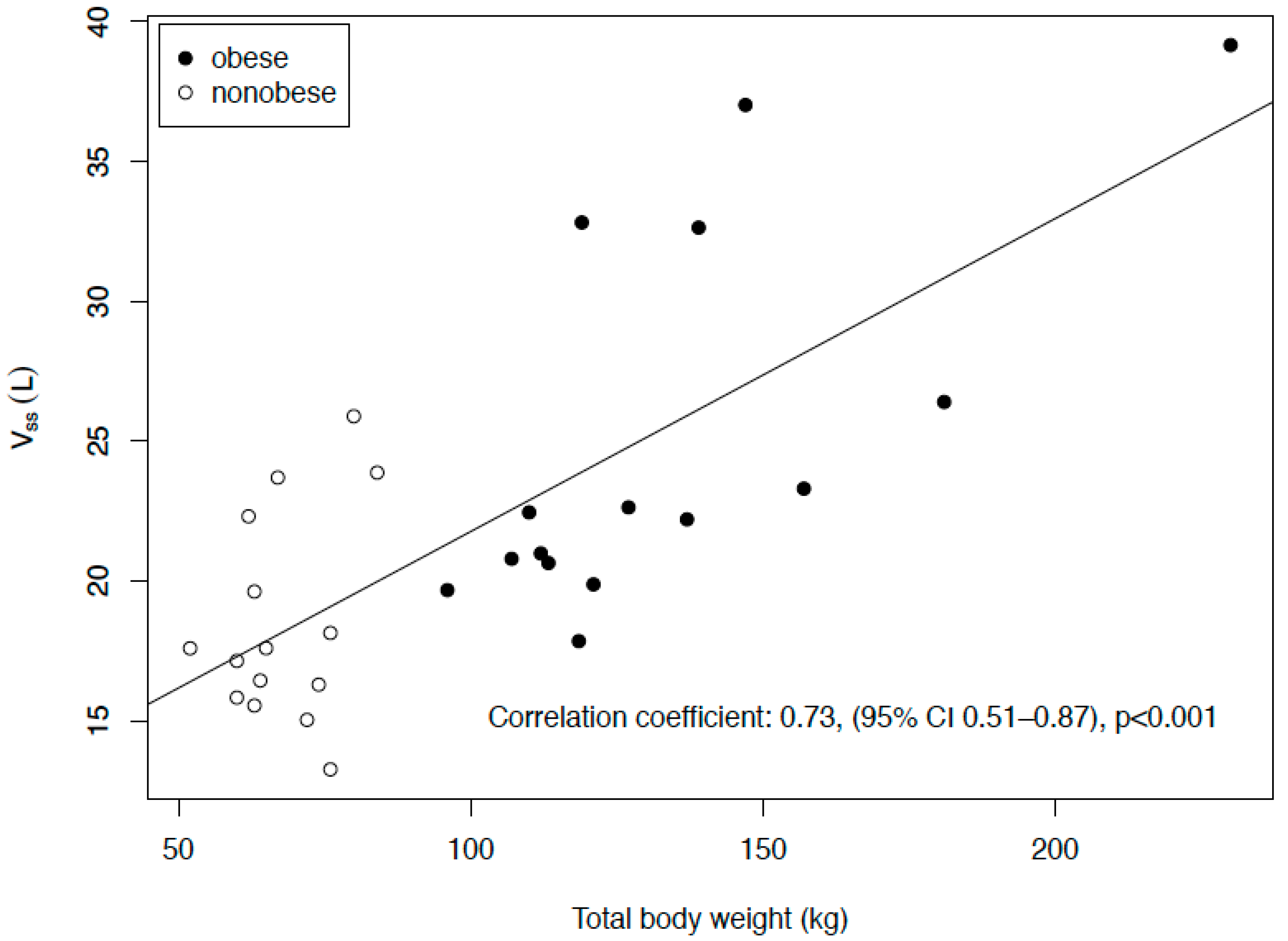
2.2. Pharmacokinetics
3. Discussion
4. Materials and Methods
4.1. Study Design and Patients
4.2. Study Procedure
4.3. Drug Analysis
4.4. Study Endpoints
4.5. Pharmacokinetic and Statistical Analysis
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Rhodes, A.; Evans, L.E.; Alhazzani, W.; Levy, M.M.; Antonelli, M.; Ferrer, R.; Kumar, A.; Sevransky, J.E.; Sprung, C.L.; Nunnally, M.E.; et al. Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016. Intensive Care Med. 2017, 43, 304–377. [Google Scholar] [CrossRef]
- Brinkmann, A.; Röhr, A.C.; Frey, O.R.; Krüger, W.A.; Brenner, T.; Richter, D.C.; Bodmann, K.F.; Kresken, M.; Grabein, B. S2k guidelines of the PEG on calculated parenteral initial treatment of bacterial diseases in adults: Focussed summary and supplementary information on antibiotic treatment of critically ill patients. Anaesthesist 2018, 67, 936–949. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity and Overweight. Available online: http://www.who.int/mediacentre/factsheets/fs311/en/index.html (accessed on 29 September 2009).
- Alobaid, A.S.; Hites, M.; Lipman, J.; Taccone, F.S.; Roberts, J.A. Effect of obesity on the pharmacokinetics of antimicrobials in critically ill patients: A structured review. Int. J. Antimicrob. Agents 2016, 47, 259–268. [Google Scholar] [CrossRef] [PubMed]
- Hites, M.; Taccone, F.S.; Wolff, F.; Maillart, E.; Beumier, M.; Surin, R.; Cotton, F.; Jacobs, F. Broad-spectrum β-lactams in obese non-critically ill patients. Nutr. Diabetes 2014, 4, e119. [Google Scholar] [CrossRef] [PubMed]
- Chung, E.K.; Cheatham, S.C.; Fleming, M.R.; Healy, D.P.; Kays, M.B. Population Pharmacokinetics and Pharmacodynamics of Meropenem in Nonobese, Obese, and Morbidly Obese Patients. J. Clin. Pharm. 2017, 57, 356–368. [Google Scholar] [CrossRef] [PubMed]
- Alobaid, A.S.; Wallis, S.C.; Jarrett, P.; Starr, T.; Stuart, J.; Lassig-Smith, M.; Mejia, J.L.O.; Roberts, M.S.; Lipman, J.; Roberts, J.A. Effect of Obesity on the Population Pharmacokinetics of Meropenem in Critically Ill Patients. Antimicrob. Agents Chemother. 2016, 60, 4577–4584. [Google Scholar] [CrossRef] [PubMed]
- Alobaid, A.S.; Brinkmann, A.; Frey, O.R.; Roehr, A.C.; Luque, S.; Grau, S.; Wong, G.; Abdul-Aziz, M.; Roberts, M.S.; Lipman, J.; et al. What is the effect of obesity on piperacillin and meropenem trough concentrations in critically ill patients? J. Antimicrob. Chemother. 2016, 71, 696–702. [Google Scholar] [CrossRef]
- Meng, L.; Mui, E.; Holubar, M.K.; Deresinski, S.C. Comprehensive Guidance for Antibiotic Dosing in Obese Adults. Pharmacotherapy 2017, 37, 1415–1431. [Google Scholar] [CrossRef]
- Toma, O.; Suntrup, P.; Stefanescu, A.; London, A.; Mutch, M.; Kharasch, E. Pharmacokinetics and tissue penetration of cefoxitin in obesity: Implications for risk of surgical site infection. Anesth. Analg. 2011, 113, 730–737. [Google Scholar] [CrossRef]
- Hollenstein, U.M.; Brunner, M.; Schmid, R.; Muller, M. Soft tissue concentrations of ciprofloxacin in obese and lean subjects following weight-adjusted dosing. Int. J. Obes. Relat. Metab. Disord. 2001, 25, 354–358. [Google Scholar] [CrossRef]
- Jager, N.G.L.; van Hest, R.M.; Lipman, J.; Roberts, J.A.; Cotta, M.O. Antibiotic exposure at the site of infection: Principles and assessment of tissue penetration. Expert Rev. Clin. Pharm. 2019, 12, 623–634. [Google Scholar] [CrossRef] [PubMed]
- Wittau, M.; Scheele, J.; Kurlbaum, M.; Brockschmidt, C.; Wolf, A.M.; Hemper, E.; Henne-Bruns, D.; Bulitta, J.B. Population Pharmacokinetics and Target Attainment of Meropenem in Plasma and Tissue of Morbidly Obese Patients after Laparoscopic Intraperitoneal Surgery. Antimicrob. Agents Chemother. 2015, 59, 6241–6247. [Google Scholar] [CrossRef]
- Gonçalves-Pereira, J.; Póvoa, P. Antibiotics in critically ill patients: A systematic review of the pharmacokinetics of β-lactams. Crit. Care 2011, 15, R206. [Google Scholar] [CrossRef]
- Craig, W.A. The pharmacology of meropenem, a new carbapenem antibiotic. Clin. Infect. Dis. 1997, 24, 266–275. [Google Scholar] [CrossRef] [PubMed]
- Ehmann, L.; Zoller, M.; Minichmayr, I.K.; Scharf, C.; Huisinga, W.; Zander, J.; Kloft, C. Development of a dosing algorithm for meropenem in critically ill patients based on a population pharmacokinetic/pharmacodynamic analysis. Int. J. Antimicrob. Agents 2019, 54, 309–317. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, J.M.; Riji, A.M. Effects of surgery on the pharmacokinetic parameters of drugs. Clin. Pharm. 1998, 35, 293–312. [Google Scholar] [CrossRef] [PubMed]
- Brill, M.J.E.; Houwink, A.P.I.; Schmidt, S.; Van Dongen, E.P.A.; Hazebroek, E.J.; van Ramshorst, B.; Deneer, V.H.; Mouton, J.W.; Knibbe, C.A.J. Reduced subcutaneous tissue distribution of cefazolin in morbidly obese versus non-obese patients determined using clinical microdialysis. J. Antimicrob. Chemother. 2014, 69, 715–723. [Google Scholar] [CrossRef]
- Mouton, J.W.; Dudley, M.N.; Cars, O.; Derendorf, H.; Drusano, G.L. Standardization of pharmacokinetic/pharmacodynamic (PK/PD) terminology for anti-infective drugs: An update. J. Antimicrob. Chemother. 2005, 55, 601–607. [Google Scholar] [CrossRef]
- Al-Shaer, M.H.; Alghamdi, W.A.; Graham, E.; Peloquin, C.A. Meropenem, Cefepime, and Piperacillin Protein Binding in Patient Samples. Ther. Drug Monit. 2020, 42, 129–132. [Google Scholar] [CrossRef]
- Pinder, N.; Brenner, T.; Swoboda, S.; Weigand, M.A.; Hoppe-Tichy, T. Therapeutic drug monitoring of beta-lactam antibiotics—Influence of sample stability on the analysis of piperacillin, meropenem, ceftazidime and flucloxacillin by HPLC-UV. J. Pharm. Biomed. Anal. 2017, 143, 86–93. [Google Scholar] [CrossRef]
- Liebchen, U.; Dorn, C.; Kees, M.; Schiesser, S.; Hitzenbichler, F.; Kees, F.; Paal, M. Comment on “Meropenem, Cefepime, and Piperacillin Protein Binding in Patient Samples”. Ther. Drug Monit. 2020, 42, 909–910. [Google Scholar] [CrossRef] [PubMed]
- European Committee on Antimicrobial Susceptibility Testing Breakpoint Tables for Interpretation of MICs and Zone Diameters, Version 10.0. Available online: https://www.eucast.org/fileadmin/src/media/PDFs/EUCAST_files/Breakpoint_tables/v_10.0_Breakpoint_Tables.pdf (accessed on 1 January 2020).
- Cheatham, S.C.; Fleming, M.R.; Healy, D.P.; Chung, E.K.; Shea, K.M.; Humphrey, M.L.; Kays, M.B. Steady-state pharmacokinetics and pharmacodynamics of meropenem in morbidly obese patients hospitalized in an intensive care unit. J. Clin. Pharm. 2014, 54, 324–330. [Google Scholar] [CrossRef] [PubMed]
- Simon, P.; Busse, D.; Petroff, D.; Dorn, C.; Ehmann, L.; Hochstädt, S.; Girrbach, F.; Dietrich, A.; Zeitlinger, M.; Kees, F.; et al. Linezolid Concentrations in Plasma and Subcutaneous Tissue are Reduced in Obese Patients, Resulting in a Higher Risk of Underdosing in Critically Ill Patients: A Controlled Clinical Pharmacokinetic Study. J. Clin. Med. 2020, 9, 1067. [Google Scholar] [CrossRef] [PubMed]
- Ehmann, L.; Simon, P.; Busse, D.; Petroff, D.; Dorn, C.; Huisinga, W.; Dietrich, A.; Zeitlinger, M.; Wrigge, H.; Kloft, C. Risk of target non-attainment in obese compared to non-obese patients in calculated linezolid therapy. Clin. Microbiol. Infect. 2020. [Google Scholar] [CrossRef]
- Dorn, C.; Petroff, D.; Neumann, N.; Kratzer, A.; El-Najjar, N.; Dietrich, A.; Kloft, C.; Zeitlinger, M.; Kees, M.G.; Kees, F.; et al. Plasma and tissue pharmacokinetics of fosfomycin in morbidly obese and non-obese surgical patients: A controlled clinical trial. J. Antimicrob. Chemother. 2019, 74, 2335–2340. [Google Scholar] [CrossRef]
- Simon, P.; Petroff, D.; Dorn, C.; Ehmann, L.; Kloft, C.; Prettin, C.; Dietrich, A.; Zeitlinger, M.; Kees, F.; Wrigge, H. Measurement of soft tissue drug concentrations in morbidly obese and non-obese patients—A prospective, parallel group, open-labeled, controlled, phase IV, singlecenter clinical trial. Contemp. Clin. Trials Comm. 2019, 15, 100375. [Google Scholar] [CrossRef]
- Hammarlund-Udenaes, M. Microdialysis as an important technique in systems pharmacology—a historical and methodological review. AAPS J. 2017, 19, 1294–1303. [Google Scholar] [CrossRef]
- McWhinney, B.C.; Wallis, S.C.; Hillister, T.; Roberts, J.A.; Lipman, J.; Ungerer, J.P. Analysis of 12 beta-lactam antibiotics in human plasma by HPLC with ultraviolet detection. J. Chromatogr. B Anal. Technol. Biomed. Life Sci. 2010, 878, 2039–2043. [Google Scholar] [CrossRef]
- Kratzer, A.; Schießer, S.; Matzneller, P.; Wulkersdorfer, B.; Zeitlinger, M.; Schlossmann, J.; Kees, F.; Dorn, C. Determination of total and free ceftolozane and tazobactam in human plasma and interstitial fluid by HPLC-UV. J. Pharm. Biomed. Anal. 2019, 163, 34–38. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Obese (n = 15) | Nonobese (n = 15) | |
|---|---|---|
| Number of females | 13 (87%) | 13 (87%) |
| Age (years) | 50.3 ± 9.5 | 49.5 ± 10.0 |
| Weight (kg) | 134.3 ± 34.3 | 67.9 ± 8.8 |
| BMI (kg/m2) | 48.7 ± 11.2 | 23.9 ± 2.1 |
| Type of surgery | ||
| laparoscopic | 15 (100%) | 3 (20%) |
| open | 0 (0%) | 12 (80%) |
| Length of surgery (h) | 2.9 ± 0.6 | 4.0 ± 1.9 |
| Serum creatinine (µmol/L) | 85.8 ± 26.3 | 75.3 ± 18.8 |
| Measuerments | Plasma | ISF | ||||||
|---|---|---|---|---|---|---|---|---|
| Obese (n = 15) | Nonobese (n = 15) | Change in Location Parameter (95% CI) | p-Value | Obese (n = 15) | Nonobese (n = 15) | Change in Location Parameter (95% CI) | p-Value | |
| maximum concentration (Cmax (mg/L)) | 54.0 (44.8–58.2) | 63.9 (53.6–69.9) | −11.0 (−18.3 to −3.5) | 0.011 | 12.6 (6.5–17.1) | 18.6 (12.4–31.2) | −7.4 (−16.8 to −0.8) | 0.026 |
| Timepoint of maximum (Tmax (h)) | 0.5 (end of infusion) | 0.5 | ― | 1.0 | 0.75/1.25 a (n = 12/3) | 0.75/1.25 a (n = 14/1) | ― | 0.60 |
| Concentration after 8 hours (C8h (mg/L)) | 1.02 (0.74–1.48) | 0.70 (0.48–0.88) | 0.33 (−0.03 to 0.72) | 0.070 | 0.54 (0.45–0.77) b | 0.36 (0.24–0.51) b | 0.21 (0.01–0.38) | 0.041 |
| Half-life (t1/2 (h)) c | 1.52 (1.44–1.67) | 1.31 (1.23–1.43) | 0.22 (0.05 to 0.37) | 0.0066 | 1.55 (1.44–1.66) | 1.32 (1.14–1.49) | 0.24 (−0.02 to 0.42) | 0.061 |
| Volume distribution at steady state (Vss (L)) | 22.4 (20.7–29.5) | 17.6 (16.1–21.0) | 5.1 (2.6 to 9.1) | 0.0017 | ― | ― | ― | ― |
| Clearance (CL(L/h)) | 12.5 (9.8–13.9) | 11.1 (9.8–12.6) | 0.8 (−1.4 to 3.1) | 0.46 | ― | ― | ― | ― |
| Area under the curve 0 to 8 hours (AUC8h (mg * h/L)) | 78.7 (69.1, 99.6) | 89.2 (78.1, 100.9) | −7.2 (−21.4 to 8.6) | 0.35 | 28.5 (19.2, 44.4) | 42.0 (29.7, 66.0) | −13.0 (−33.9 to 5.4) | 0.15 |
| Area under the curve extrapolated to infinity (AUC∞ (mg * h/L)) d | 80.3 (71.8–102.0) | 90.3 (79.4–102.3) | −6.5 (−21.1 to 10.4) | 0.46 | 33.7 (23.6–38.7) | 44.6 (29.2–59.1) | −11.4 (−31.9 to 5.5) | 0.22 |
| Penetration ratio (AUC∞, ISF/AUC∞, plasma) | ― | ― | ― | 0.35 (0.27–0.52) | 0.48 (0.33–0.62) | −0.09 (−0.30 to 0.08) | 0.40 | |
| Obese (n = 15) | Nonobese (n = 15) | Difference between Groups | p-Value | ||||
|---|---|---|---|---|---|---|---|
| Estimate | 95% CI | Estimate | 95% CI | Estimate | 95% CI | ||
| MIC in Plasma | |||||||
| 0.25 mg/L | 11.9 | (10.3 to 13.4) | 10.2 | (9.3 to 11.2) | +1.6 | (−0.3 to 3.6) | 0.097 |
| 2 mg/L | 6.9 | (6.0 to 7.8) | 6.1 | (5.5 to 6.8) | +0.8 | (−0.3 to 2.0) | 0.16 |
| 8 mg/L | 3.8 | (3.3 to 4.2) | 3.5 | (3.1 to 3.9) | +0.2 | (−0.4 to 0.9) | 0.42 |
| MIC in ISF | |||||||
| 0.25 mg/L | 11.0 | (10.1 to 11.8) | 9.6 | (8.2 to 10.9) | +1.4 | (−0.3 to 3.0) | 0.10 |
| 2 mg/L | 5.4 | (4.7 to 6.1) | 5.0 | (4.0 to 6.1) | +0.3 | (−1.0 to 1.7) | 0.60 |
| 8 mg/L a | 1.4 | (0.7 to 2.1) | 2.0 | (1.2 to 2.9) | −0.6 | (−1.8 to 0.5) | 0.26 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Simon, P.; Petroff, D.; Busse, D.; Heyne, J.; Girrbach, F.; Dietrich, A.; Kratzer, A.; Zeitlinger, M.; Kloft, C.; Kees, F.; et al. Meropenem Plasma and Interstitial Soft Tissue Concentrations in Obese and Nonobese Patients—A Controlled Clinical Trial. Antibiotics 2020, 9, 931. https://doi.org/10.3390/antibiotics9120931
Simon P, Petroff D, Busse D, Heyne J, Girrbach F, Dietrich A, Kratzer A, Zeitlinger M, Kloft C, Kees F, et al. Meropenem Plasma and Interstitial Soft Tissue Concentrations in Obese and Nonobese Patients—A Controlled Clinical Trial. Antibiotics. 2020; 9(12):931. https://doi.org/10.3390/antibiotics9120931
Chicago/Turabian StyleSimon, Philipp, David Petroff, David Busse, Jana Heyne, Felix Girrbach, Arne Dietrich, Alexander Kratzer, Markus Zeitlinger, Charlotte Kloft, Frieder Kees, and et al. 2020. "Meropenem Plasma and Interstitial Soft Tissue Concentrations in Obese and Nonobese Patients—A Controlled Clinical Trial" Antibiotics 9, no. 12: 931. https://doi.org/10.3390/antibiotics9120931
APA StyleSimon, P., Petroff, D., Busse, D., Heyne, J., Girrbach, F., Dietrich, A., Kratzer, A., Zeitlinger, M., Kloft, C., Kees, F., Wrigge, H., & Dorn, C. (2020). Meropenem Plasma and Interstitial Soft Tissue Concentrations in Obese and Nonobese Patients—A Controlled Clinical Trial. Antibiotics, 9(12), 931. https://doi.org/10.3390/antibiotics9120931