Cost-Effectiveness Analysis of the Use of Point-of-Care C-Reactive Protein Testing to Reduce Antibiotic Prescribing in Primary Care

 ,
,
Abstract
1. Introduction
2. Results
2.1. Base Case Analysis
2.2. Sensitivity and Scenario Analyes
2.2.1. One-Way Sensitivity and Threshold Analyses
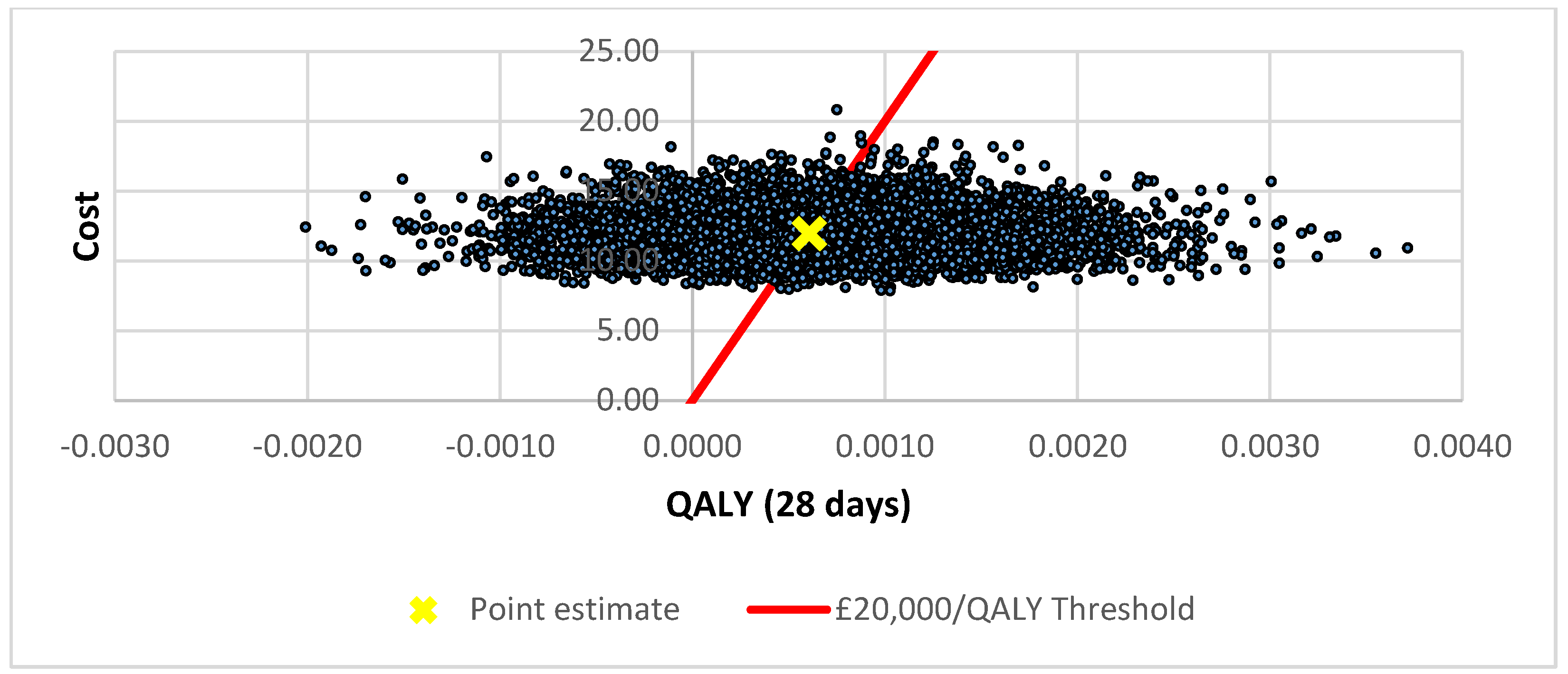
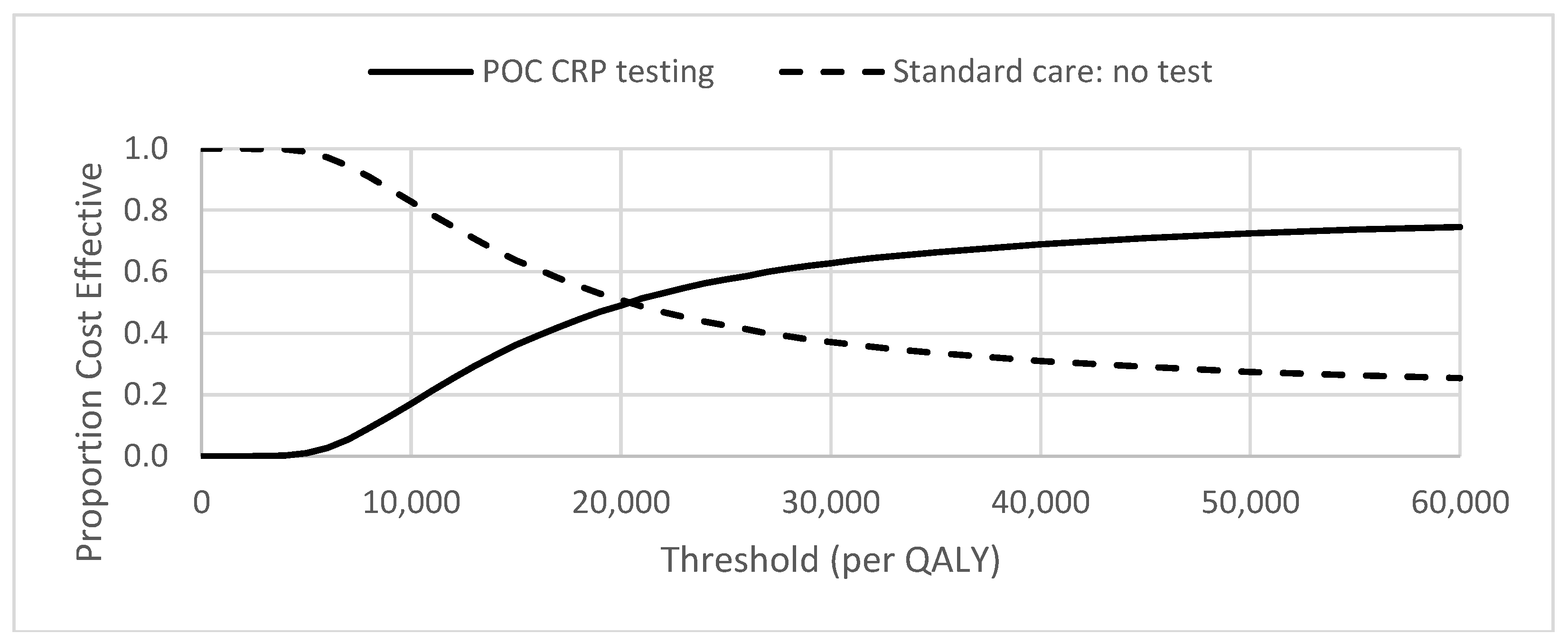
2.2.2. Probabilistic Sensitivity Analysis
2.2.3. Scenario Analyses
3. Discussion
3.1. Key Findings
3.2. Comparisons to Other Studies
3.3. Strengths
3.4. Limitations
3.5. Implications
3.6. Future Research Directions
4. Materials and Methods
4.1. Economic Model
4.1.1. Clinical Parameters
4.1.2. Resource Use and Costs
4.1.3. Health State Utilities
4.2. Analysis
4.2.1. Cost Per QALY
4.2.2. Cost-Effectiveness Analysis
4.2.3. Base-Case Analysis
4.2.4. Sensitivity Analyses
4.2.5. Scenario Analyses
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Section/Item | Item No | Recommendation | Reported on Page No/line No |
|---|---|---|---|
| Title and abstract | |||
| Title | 1 | Identify the study as an economic evaluation or use more specific terms such as “cost-effectiveness analysis”, and describe the interventions compared. | Lines 2–4 |
| Abstract | 2 | Provide a structured summary of objectives, perspective, setting, methods (including study design and inputs), results (including base case and uncertainty analyses), and conclusions. | Lines 18–32 |
| Introduction | |||
| Background and objectives | 3 | Provide an explicit statement of the broader context for the study. | Lines 38–56 |
| Present the study question and its relevance for health policy or practice decisions. | Lines 74–83 | ||
| Methods | |||
| Target population and subgroups | 4 | Describe characteristics of the base case population and subgroups analysed, including why they were chosen. | Lines 273–276 Lines 315–320 |
| Setting and location | 5 | State relevant aspects of the system(s) in which the decision(s) need(s) to be made. | Lines 58–73 Lines 273–275 Lines 302–307 |
| Study perspective | 6 | Describe the perspective of the study and relate this to the costs being evaluated. | Line 275 |
| Comparators | 7 | Describe the interventions or strategies being compared and state why they were chosen. | Lines 282–287 |
| Time horizon | 8 | State the time horizon(s) over which costs and consequences are being evaluated and say why appropriate. | Line 280 |
| Discount rate | 9 | Report the choice of discount rate(s) used for costs and outcomes and say why appropriate. | Line 384 |
| Choice of health outcomes | 10 | Describe what outcomes were used as the measure(s) of benefit in the evaluation and their relevance for the type of analysis performed. | Line 373 |
| Measurement of effectiveness | 11a | Single study-based estimates: Describe fully the design features of the single effectiveness study and why the single study was a sufficient source of clinical effectiveness data. | Prescriptions avoided: Lines 301–313 Utility: Lines 373–382 |
| 11b | Synthesis-based estimates: Describe fully the methods used for identification of included studies and synthesis of clinical effectiveness data. | ||
| Measurement and valuation of preference based outcomes | 12 | If applicable, describe the population and methods used to elicit preferences for outcomes. | Lines 373–382 |
| Estimating resources and costs | 13a | Single study-based economic evaluation: Describe approaches used to estimate resource use associated with the alternative interventions. Describe primary or secondary research methods for valuing each resource item in terms of its unit cost. Describe any adjustments made to approximate to opportunity costs. | |
| 13b | Model-based economic evaluation: Describe approaches and data sources used to estimate resource use associated with model health states. Describe primary or secondary research methods for valuing each resource item in terms of its unit cost. Describe any adjustments made to approximate to opportunity costs. | Lines 328–385 3&4 | |
| Currency, price date, and conversion | 14 | Report the dates of the estimated resource quantities and unit costs. Describe methods for adjusting estimated unit costs to the year of reported costs if necessary. Describe methods for converting costs into a common currency base and the exchange rate. | Lines 328–385 |
| Choice of model | 15 | Describe and give reasons for the specific type of decision-analytical model used. Providing a figure to show model structure is strongly recommended. | Lines 280–293 3&4 |
| Assumptions | 16 | Describe all structural or other assumptions underpinning the decision-analytical model. | Lines 280–385 |
| Analytical methods | 17 | Describe all analytical methods supporting the evaluation. This could include methods for dealing with skewed, missing, or censored data; extrapolation methods; methods for pooling data; approaches to validate or make adjustments (such as half cycle corrections) to a model; and methods for handling population heterogeneity and uncertainty. | Lines 413–445 |
| Results | |||
| Study parameters | 18 | Report the values, ranges, references, and, if used, probability distributions for all parameters. Report reasons or sources for distributions used to represent uncertainty where appropriate. Providing a table to show the input values is strongly recommended. | Table 3 |
| Incremental costs and outcomes | 19 | For each intervention, report mean values for the main categories of estimated costs and outcomes of interest, as well as mean differences between the comparator groups. If applicable, report incremental cost-effectiveness ratios. | Table 1 |
| Characterising uncertainty | 20a | Single study-based economic evaluation:Describe the effects of sampling uncertainty for the estimated incremental cost and incremental effectiveness parameters, together with the impact of methodological assumptions (such as discount rate, study perspective). | |
| 20b | Model-based economic evaluation: Describe the effects on the results of uncertainty for all input parameters, and uncertainty related to the structure of the model and assumptions. | Lines 114–128 Lines 138–141 | |
| Characterising heterogeneity | 21 | If applicable, report differences in costs, outcomes, or cost-effectiveness that can be explained by variations between subgroups of patients with different baseline characteristics or other observed variability in effects that are not reducible by more information. | Lines 129-151 Table 1 and Table 2 Figure 1 and Figure 2 |
| Discussion | |||
| Study findings, limitations, generalisability, and current knowledge | 22 | Summarise key study findings and describe how they support the conclusions reached. Discuss limitations and the generalisability of the findings and how the findings fit with current knowledge. | Lines 154–169 |
| Other | |||
| Source of funding | 23 | Describe how the study was funded and the role of the funder in the identification, design, conduct, and reporting of the analysis. Describe other non-monetary sources of support. | Line 461 |
| Conflicts of interest | 24 | Describe any potential for conflict of interest of study contributors in accordance with journal policy. In the absence of a journal policy, we recommend authors comply with International Committee of Medical Journal Editors recommendations. | Line 467 |
References
- Butler, C.C.; Hood, K.; Verheij, T.; Little, P.; Melbye, H.; Nuttall, J.; Kelly, M.J.; Mölstad, S.; Godycki-Cwirko, M.; Almirall, J.; et al. Variation in antibiotic prescribing and its impact on recovery in patients with acute cough in primary care: Prospective study in 13 countries. BMJ 2009, 338, b2242. [Google Scholar] [CrossRef] [PubMed]
- Currie, C.J.; Berni, E.; Jenkins-Jones, S.; Poole, C.D.; Ouwens, M.; Driessen, S.; de Voogd, H.; Butler, C.C.; Morgan, C.L. Antibiotic treatment failure in four common infections in UK primary care 1991–2012: Longitudinal analysis. BMJ 2014, 349, g5493. [Google Scholar] [CrossRef] [PubMed]
- Llor, C.; Bjerrum, L. Antimicrobial resistance: Risk associated with antibiotic overuse and initiatives to reduce the problem. Ther. Adv. Drug Saf. 2014, 5, 229–241. [Google Scholar] [CrossRef] [PubMed]
- Costelloe, C.; Metcalfe, C.; Lovering, A.; Mant, D.; Hay, A.D. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: Systematic review and meta-analysis. BMJ 2010, 340, c2096. [Google Scholar] [CrossRef] [PubMed]
- Bell, B.G.; Schellevis, F.; Stobberingh, E.; Goossens, H.; Pringle, M. A systematic review and meta-analysis of the effects of antibiotic consumption on antibiotic resistance. BMC Infect. Dis. 2014, 14, 13. [Google Scholar] [CrossRef] [PubMed]
- Owens, R.C., Jr.; Donskey, C.J.; Gaynes, R.P.; Loo, V.G.; Muto, C.A. Antimicrobial-associated risk factors for Clostridium difficile infection. Clin. Infect. Dis. 2008, 46, S19–S31. [Google Scholar] [CrossRef] [PubMed]
- WHO Patient Safety. The Evolving Threat of Antimicrobial Resistance: Options for Action; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- O’Neill, J. Tackling Drug-Resistant Infections Globally: Final report and Recommendations. 2016. Available online: https://amr-review.org/sites/default/files/160525_Final%20paper_with%20cover.pdf (accessed on 26 June 2018).
- National Institute of Health and Care Excellence (NICE) Guidelines on Antimicrobial Stewardship. Quality Standard [QS121]. Published date: April 2016. Available online: https://www.nice.org.uk/guidance/qs121 (accessed on 13 March 2018).
- Welsh Government. Together for Health. Tackling Antimicrobial Resistance and Improving Antibiotic Prescribing; Welsh Government: Cardiff, UK, 2015.
- National Institute for Health and Care Excellence. CG191 Pneumonia in Adults: Diagnosis and Management. 2014. Available online: https://www.nice.org.uk/guidance/cg191 (accessed on 23 September 2017).
- Welsh Scientific Advisory Committee. Policy on the management of Point of Care Testing, what, when and How? May 2017, WG31745. Digital ISBN 978-1-4734-9536-. Available online: https://gov.wales/docs/dhss/publications/170918whc034en.pdf (accessed on 6 December 2018).
- Huang, Y.; Chen, R.; Wu, T.; Wei, X.; Guo, A. Association between point-of-care CRP testing and antibiotic prescribing in respiratory tract infections: A systematic review and meta-analysis of primary care studies. Br. J. Gen. Pract. 2013, 63, e787–e794. [Google Scholar] [CrossRef]
- Cooke, J.; Butler, C.; Hopstaken, R.; Dryden, M.S.; McNulty, C.; Hurding, S.; Moore, M.; Livermore, D.M. Narrative review of primary care point-of-care testing (POCT) and antibacterial use in respiratory tract infection (RTI). BMJ Open Respir. Res. 2015, 2, e000086. [Google Scholar] [CrossRef]
- Andreeva, E.; Melbye, H. Usefulness of C-reactive protein testing in acute cough/respiratory tract infection: An open cluster-randomized clinical trial with C-reactive protein testing in the intervention group. BMC Fam. Pract. 2014, 15, 80. [Google Scholar] [CrossRef]
- Little, P.; Stuart, B.; Francis, N.; Douglas, E.; Tonkin-Crine, S.; Anthierens, S.; Cals, J.W.; Melbye, H.; Santer, M.; Moore, M.; et al. Effects of internet-based training on antibiotic prescribing rates for acute respiratory-tract infections: A multinational, cluster, randomised, factorial, controlled trial. Lancet 2013, 382, 1175–1182. [Google Scholar] [CrossRef]
- Bjerrum, L.; Gahrn-Hansen, B.; Munck, A.P. General practitioners who use CRP have a lower antibiotic prescribing rate to patients with sinusitis—Secondary publication. Ugeskr. Laeger. 2005, 167, 2775–2777. [Google Scholar]
- Cals, J.W.; Schot, M.J.; de Jong, S.A.; Dinant, G.J.; Hopstaken, R.M. Point-of-care C-reactive protein testing and antibiotic prescribing for respiratory tract infections: A randomized controlled trial. Ann. Fam. Med. 2010, 8, 124–133. [Google Scholar] [CrossRef]
- Diederichsen, H.Z.; Skamling, M.; Diederichsen, A.; Grinsted, P.; Antonsen, S.; Petersen, P.H.; Munck, A.P.; Kragstrup, J. Randomised controlled trial of CRP rapid test as a guide to treatment of respiratory infections in general practice. Scand. J. Prim. Health Care 2000, 18, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Cals, J.W.; Ament, A.J.; Hood, K.; Butler, C.C.; Hopstaken, R.M.; Wassink, G.F.; Dinant, G.J. C-reactive protein point of care testing and physician communication skills training for lower respiratory tract infections in general practice: Economic evaluation of a cluster randomized trial. J. Eval. Clin. Pract. 2011, 17, 1059–1069. [Google Scholar] [CrossRef]
- Dahler-Eriksen, B.S.; Lauritzen, T.; Lassen, J.F.; Lund, E.D.; Brandslund, I. Near patient test for C-reactive protein in general practice: Assessment of clinical, organizational and economic outcomes. Clin. Chem. 1999, 45, 478–485. [Google Scholar] [PubMed]
- Hunter, R. Cost-effectiveness of point-of-care C-reactive protein tests for respiratory tract infection in primary care in England. Adv. Ther. 2015, 32, 69–85. [Google Scholar] [CrossRef]
- Oppong, R.; Jit, M.; Smith, R.D.; Butler, C.C.; Melbye, H.; Mölstad, S.; Coast, J. Cost-effectiveness of point-of-care C-reactive protein testing to inform antibiotic prescribing decisions. Br. J. Gen. Pract. 2013, 63, e465–e471. [Google Scholar] [CrossRef]
- National POCT Standards; ISO22870:2006; Royal College of Pathologists ISO: London, UK, 2006.
- Smith, R.; Coast, J. The true cost of antimicrobial resistance. BMJ 2013, 346, f1493. [Google Scholar] [CrossRef] [PubMed]
- Hughes, A.; Gwyn, L.; Harris, S.; Clark, C. Evaluating point-of-care C-reactive protein testing in a general practice. Clin. Pharm. 2016, 8, 309–318. [Google Scholar]
- Oppong, R.; Smith, R.D.; Little, P.; Verheij, T.; Butler, C.C.; Goossens, H.; Coenen, S.; Moore, M.; Coast, J. Cost-effectiveness of amoxicillin for lower respiratory tract infections in primary care: An economic evaluation accounting for the cost of antimicrobial resistance. Br. J. Gen. Pract. 2016, 21, e633–e639. [Google Scholar] [CrossRef]
- National Institute for Health and Care Excellence. Guide to the Methods of Technology Appraisal 2013. Available online: https://www.nice.org.uk/process/pmg9/chapter/foreword (accessed on 12 March 2018).
- Wilcox, M.H.; Ahir, H.; Coia, J.E.; Dodgson, A.; Hopkins, S.; Llewelyn, M.J.; Settle, C.; Mclain-Smith, S.; Marcella, S.W. Impact of recurrent Clostridium difficile infection: Hospitalization and patient quality of life. J. Antimicrob. Chemother. 2017, 72, 2647–2656. [Google Scholar] [CrossRef] [PubMed]
- Bala, M.V.; Zarkin, G.A. Are QALYs an appropriate measure for valuing morbidity in acute diseases? Health Econ. 2000, 9, 177–180. [Google Scholar] [CrossRef]
- Rothery, C.; Woods, B.; Schmitt, L.; Claxton, K.; Palmer, S.; Sculpher, M. Framework for value assessment of new antimicrobials. Policy Research Unit in Economic Evaluations of Health & Care Interventions, York. September 2018. Available online: http://www.eepru.org.uk/wp-content/uploads/2017/11/eepru-report-amr-oct-2018-059.pdf (accessed on 19 November 2018).
- House of Commons Health and Social Care Committee. Antimicrobial Resistance. Eleventh Report of Session 2017–2019. 22 October 2018 HC962. Available online: https://publications.parliament.uk/pa/cm201719/cmselect/cmhealth/962/962.pdf (accessed on 19 November 2018).
- Spurling, G.K.; Del Mar, C.B.; Dooley, L.; Foxlee, R.; Farley, R. Delayed Antibiotic Prescriptions for Respiratory Infections; The Cochrane Library: London, UK, 1 January 2017. [Google Scholar]
- Saramago, P.; Manca, A.; Sutton, A.J. Deriving input parameters for cost-effectiveness modelling: Taxonomy of data types and approaches to their statistical synthesis. Value Health 2012, 15, 639–649. [Google Scholar] [CrossRef] [PubMed]
- Adams, H.; Craine, N. Exploring Primary Care Antibiotic Prescribing; Version 1; Betsi Cadwaladr University Health Board (BCUHB): North Wales, UK, February 2017. [Google Scholar]
- NHS Wales Shared Services. ‘Primary Care Prescribing Catalogue’. Available online: http://prescribing.wales.nhs.uk/OnlineCatalogueV2/home/login (accessed on 4 September 2018).
- Summary of Product Characteristics (SPC): Amoxicillin 500 mg Capsules BP [04/08/2017]. Available online: https://www.medicines.org.uk/emc/medicine/25942#UNDESIRABLE_EFFECTS (accessed on 21 September 2017).
- Hobbs, R.; Bankhead, C.; Mukhtar, T.; Stevens, S.; Perera-Salazar, R.; Holt, T.; Salisbury, C. Clinical workload in UK primary care: A retrospective analysis of 100 million consultations in England, 2007–14. Lancet 2016, 387, 2323–2330. [Google Scholar] [CrossRef]
- PSSRU Unit Costs of Health and Social Care 2017. Available online: https://www.pssru.ac.uk/project-pages/unit-costs/unit-costs-2017/ (accessed on 23 June 2018).
- British National Formulary (BNF). September 2017. Available online: https://bnf.nice.org.uk (accessed on 24 September 2017).
- Holt, R. Personal Communication.
- NHS Choices Anaphylaxis. Dated: 2 December 2016. Available online: http://www.nhs.uk/conditions/Anaphylaxis/Pages/Introduction.aspx#treatment (accessed on 24 September 2017).
- Department of Health, NHS England and NHS Improvement. NHS Reference Costs 2016–2017. Department of Health and Social Care. 2017. Available online: https://improvement.nhs.uk/resources/reference-costs/ (accessed on 17 October 2018).
- Janssen, B.; Szende, A. Population Norms for the EQ-5D. In Self-Reported Population Health: An International Perspective Based on EQ-5D; Szende, A., Janssen, B., Cabases, J., Eds.; Springer: Dordrecht, The Netherlands, 2014. [Google Scholar]
- Oppong, R.; Kaambwa, B.; Nuttall, J.; Hood, K.; Smith, R.D.; Coast, J. The impact of using different tariffs to value EQ-5D health state descriptions: An example from a study of acute cough/lower respiratory tract infections in seven countries. Eur. J. Health Econ. 2013, 14, 197–209. [Google Scholar] [CrossRef] [PubMed]
- Neuner, J.M.; Hamel, M.B.; Phillips, R.S.; Bona, K.; Aronson, M.D. Diagnosis and management of adults with pharyngitis: A cost-effectiveness analysis. Ann. Intern. Med. 2003, 139, 113–122. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence. CG69 Respiratory tract infections—Antibiotic prescribing. 2008. Available online: http://www.nice.org.uk/guidance/cg69/ (accessed on 23 September 2017).
- CRP POCT Guidelines for Wales. Using CRP Testing to Support Clinical Decisions in Primary Care. Available online: http://www.gpone.wales.nhs.uk/sitesplus/documents/1000/crp%20poc%20testing%20guidelines%20for%20wales.docx (accessed on 25 September 2017).
- Fenwick, E.; Claxton, K.; Sculpher, M. Representing uncertainty: The role of cost-effectiveness acceptability curves. Health Econ. 2001, 10, 779–787. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Antimicrobial Resistance: No Action Today, no Cure Tomorrow. World Health Day: Media Fact Sheet. 7 April 2011. Available online: http://www.cdc.gov/media/releases/2011/f0407_antimicrobialresistance.pdf (accessed on 19 November 2018).
- European Centre for Disease Prevention and Control, European Medicines Agency. The bacterial challenge: Time to React. Joint Technical Report. Stockholm: ECDPC. 2009. Available online: https://ecdc.europa.eu/sites/portal/files/media/en/publications/Publications/0909_TER_The_Bacterial_Challenge_Time_to_React.pdf (accessed on 19 November 2018).
- Husereau, D.; Drummond, M.; Petrou, S.; ISPOR Health Economic Evaluation Publication Guidelines-CHEERS Good Reporting Practices Task Force. Consolidated Health Economic Evaluation Reporting Standards (CHEERS)–explanation and elaboration: A report of the ISPOR Health Economic Evaluation Publication Guidelines Good Reporting Practices Task Force. Value Health 2013, 16, 231–250. [Google Scholar]




| Results for 28 Days and 1 Patient | Intervention | Control | Increment | ICER | ||||||
| Pragmatic Use of Testing, Reflective of Practice | Mean | 95% CI | 95% CI | Mean | 95% CI | 95% CI | Mean | 95% CI | 95% CI | |
| Costs (£, over 28 days) | ||||||||||
| Consultation cost | 41.75 | 39.36 | 44.71 | 37.46 | 37.39 | 37.54 | 4.28 | 1.91 | 7.26 | |
| CRP testing | 9.85 | 9.63 | 10.42 | 0.00 | 0.00 | 0.00 | 9.85 | 9.63 | 10.42 | |
| Antibiotic prescription | 0.74 | 0.47 | 1.04 | 2.89 | 2.85 | 2.89 | −2.15 | −2.41 | −1.84 | |
| Adverse drug reaction to antibiotic | 0.02 | 0.01 | 0.02 | 0.06 | 0.05 | 0.07 | −0.04 | −0.06 | −0.03 | |
| Total cost | 52.35 | 49.76 | 55.79 | 40.41 | 40.32 | 40.48 | 11.94 | 9.35 | 15.39 | |
| Effectiveness (over 28 days) | ||||||||||
| Antibiotic prescription avoided (N) | 0.74 | 0.64 | 0.84 | 0.00 | 0.00 | 0.01 | 0.74 | 0.64 | 0.84 | |
| Cost-effectiveness (over 28 days) | ||||||||||
| £/prescription (Rx) avoided | £16.07/Rx avoided | |||||||||
| Utility (for 28 days) | ||||||||||
| Quality-adjusted-life-year (QALY) | 0.0615 | 0.0512 | 0.0706 | 0.0609 | 0.0507 | 0.0700 | 0.0006 | −0.0006 | 0.0019 | |
| Cost–utility | ||||||||||
| £/QALY | £19,705/QALY | |||||||||
| Probabilistic result | % | |||||||||
| Probability cost-effective at £20,000/QALY | 49.06 | |||||||||
| Probability cost-effective at £30,000/QALY | 62.82 | |||||||||
| Results for 28 days and 1 patient | Intervention | Control | Increment | ICER | ||||||
| Adhering to guidelines | Mean | 95% CI | 95% CI | Mean | 95% CI | 95% CI | Mean | 95% CI | 95% CI | |
| Costs (£, over 28 days) | ||||||||||
| Consultation cost | 38.73 | 36.90 | 42.76 | 36.89 | 36.70 | 37.06 | 1.84 | 0.05 | 5.85 | |
| CRP testing | 10.05 | 9.58 | 10.68 | 0.00 | 0.00 | 0.00 | 10.05 | 9.58 | 10.68 | |
| Antibiotic prescription | 0.00 | 0.00 | 0.00 | 2.53 | 2.42 | 2.53 | −2.53 | −2.47 | −1.86 | |
| Adverse drug reaction to antibiotic prescription | 0.00 | 0.00 | 0.00 | 0.06 | 0.05 | 0.07 | −0.06 | −0.07 | −0.04 | |
| Total cost | 48.79 | 46.66 | 53.53 | 39.48 | 39.25 | 39.62 | 9.31 | 7.24 | 14.11 | |
| Effectiveness (over 28 days) | ||||||||||
| Antibiotic prescription avoided (N) | 1.00 | 0.75 | 0.98 | 0.00 | 0.00 | 0.04 | 1.00 | 0.73 | 0.98 | |
| Cost-effectiveness (over 28 days) | ||||||||||
| £/prescription (Rx) avoided | £9.31/Rx avoided | |||||||||
| Utility (for 28 days) | ||||||||||
| Quality-adjusted-life-year (QALY) | 0.0577 | 0.0536 | 0.0612 | 0.0556 | 0.0509 | 0.0594 | 0.0021 | −0.0011 | 0.0058 | |
| Cost–utility | ||||||||||
| £/QALY | £4,390/QALY | |||||||||
| Probabilistic result | % | |||||||||
| Probability cost-effective at £20,000/QALY | 84.10 | |||||||||
| Probability cost-effective at £30,000/QALY | 86.33 | |||||||||
| Analysis | Parameter Description | Pragmatic Analysis Reflective of Practice: Acute Respiratory Tract Infection (ARTI) | Adhering to Protocol: Lower Respiratory Tract Infection (LRTI) only |
|---|---|---|---|
| Incremental Cost-Effectiveness Ration (ICER) | Incremental Cost-Effectiveness Ration (ICER) | ||
| Base case | £19,705 | £4390 | |
| Threshold analysis: cost of test | |||
| Cost of test = £0 | £3449 | DOMINANT | |
| Cost of test = +£0.18 (£9.76) ~2% increase | £20,010 | n/a | |
| Cost of test = +£31.60 (£41.18) ~4-fold increase | n/a | £20,036 | |
| Threshold analysis: Scale of testing: number of tests per year (base case = 376) | |||
| Acute respiratory tract infection (ARTI) only (n = 280 test per practice per annum) | £21,834 | n/a | |
| Lower respiratory tract infection (LRTI) only (n = 80 test per practice per annum) | n/a | £11,094 | |
| 5% decrease (358 tests per practice per year) | £20,017 | n/a | |
| 90% decrease (39 tests per practice per year) | n/a | £20,046 | |
| One-way sensitivity analysis: Healthcare professional at index and re-consultation | |||
| General practitioner (GP): Independent Nurse Prescriber (INP) 50:50 | £18,081 | £4193 | |
| GP | £19,749 | £4410 | |
| Nurse | £16,288 | £3976 | |
| Scenario analyses | |||
| i | Re-consultation rate | ||
| Equal in each arm i.e. standard care = Point-of-care (POC) C-reactive protein (CRP) pilot study | £12,638 | £3520 | |
| ii | Cost of antimicrobial resistance per prescription over 28 days | ||
| (a) European | £19,525 | £4321 | |
| (b) U.S. | £13,854 | £2140 | |
| (c) Global | Dominant | Dominant | |
| iii | Dispensing item fee at local dispensing doctor rate £1.90 | £19,361 | £4258 |
| iv | Hospital admission | £26,927 | £ 6454 |
| v | Antibiotic prescribing in standard care 53% | £20,277 | £4533 |
| vi | Amoxicillin prescription | ||
| 500 mg capsules three times daily for 5 days | £20,146 | n/a | |
| 500 mg capsules three times daily for 7 days | n/a | £4220 | |
| vii | CRP analyser machine life 10-years | £19,183 | £4238 |
| Parameter | Point Estimate | Distribution 1 | References |
|---|---|---|---|
| Probabilities | |||
| Antibiotics at index | C-reactive protein (CRP) > 100 mg/L | 1.00 | Fixed | [11] |
| Antibiotics at index consultation | no CRP | 1.00 | Fixed | Assumption 2 |
| Anaphylactic reaction to antibiotic prescription | 0.0001 | Beta (1, 10, 000) | [37] |
| ARTI Observed Data | |||
| CRP < 20 mg/L | 0.77 | Dirichlet (54, 16, 0) | [26] |
| CRP 20–100 mg/L | 0.23 | Dirichlet (16, 54, 0) | [26] |
| No antibiotics at index consultation | CRP < 20 mg/L | 0.93 | Dirichlet (50, 2, 2) | [26] |
| Delayed prescription at index consultation | CRP < 20 mg/L | 0.04 | Dirichlet (2, 50, 2) | [26] |
| Delayed prescription at index consultation not dispensed | CRP < 20 mg/L | 1.00 | Beta (1, 0) | [26] |
| Antibiotics at index consultation | CRP < 20 mg/L | 0.04 | Dirichlet (2, 50, 2) | [26] |
| No antibiotics at index consultation | CRP 20–100 mg/L | 0.38 | Dirichlet (6, 10, 0) | [26] |
| Antibiotics at index consultation | CRP 20–100 mg/L | 0.63 | Dirichlet (10, 6, 0) | [26] |
| No re-consultation within 28 days | CRP < 20 mg/L | 0.86 | Beta (43, 7) | [26] |
| No re-consultation within 28 days | CRP 20–100 mg/L | 0.83 | Beta (5, 1) | [26] |
| No repeat CRP at re-consultation| CRP < 20 mg/L | 0.71 | Beta (5, 2) | [26] |
| No repeat CRP at re-consultation| CRP 20–100 mg/L | 1.00 | Beta (1, 0) | [26] |
| CRP guided no antibiotic decision at re-consultation | CRP <20 mg/L | 1.00 | Beta (2, 0) | [26] |
| Antibiotics at re-consultation | CRP < 20 mg/L at index, CRP not repeated at re-consultation | 1.00 | Beta (5, 0) | [26] |
| Antibiotics at re-consultation | CRP 20–100 mg/L at index, no delayed prescription, CRP not repeated at re-consultation | 1.00 | Beta (1, 0) | [26] |
| Resource Use Proportions | |||
| General Practitioner (GP) face-to-face consultation for lower respiratory tract infection (LRTI) | 0.95 | Beta (20, 1) | Raw data [26] |
| GP face-to-face consultation for acute respiratory tract infection (ARTI) | 0.99 | Beta (77, 1) | Raw data [26] |
| Independent Nurse Prescriber (INP) face-to-face consultations for LRTI | 0.05 | Beta (1, 20) | Raw data [26] |
| GP face-to-face consultation for ARTI | 0.01 | Beta (1, 77) | Raw data [26] |
| Telephone triage 5 | 0.01 | Beta (1, 77) | Raw data [26] |
| Costs (per unit) | |||
| GP consultation (9.22 minutes) | £38.00 | Fixed | [39] |
| INP consultation (15 minutes consultation with band 7) | £13.25 | Fixed | [39] |
| Telephone triage GP led (per telephone call) | £14.60 | Fixed | [39] |
| Telephone triage nurse led (per telephone call) | £6.10 | Fixed | [39] |
| Point-of-care (POC) CRP testing (per test) | £9.58 | Fixed | Table 4 |
| Amoxicillin capsules (500 mg three times daily for 5 days) | £0.91 | Fixed | [40] |
| Amoxicillin capsules (500 mg three times daily for 7 days) | £1.27 | Fixed | [40] |
| Clarithromycin tablets (500 mg twice daily for 7 days) | £2.23 | Fixed | [40] |
| Dispensing rate for community pharmacists (per item) | £1.62 | Fixed | [41] |
| Emergency ambulance 3 (per adverse drug reaction) | £236.00 | Fixed | [43] |
| Emergency medicine 4 (per adverse drug reaction) | £362.00 | Fixed | [43] |
| Utilities | |||
| Utility (EQ-5D-3L score) 6 | |||
| U.K. population norm age 45–54 years | 0.8470 | 1-Gamma (1.0000, 0.0015) | [44] |
| LRTI | 0.6750 | 1-Gamma (1.0000, 0.0033) | [45] |
| Upper respiratory tract infection (URTI). | 0.7970 | 1-Gamma (1.0000, 0.0020) | [44,46,47] |
| Anaphylaxis (adverse drug reaction) weight | 0.5 | Fixed | [47] |
| Symptom Duration (days) | Median | ||
| Patient reported time to full recovery: LRTI CRP | 15.5 | Beta (2.8, 5.5) | [18] |
| Patient reported time to full recovery: LRTI Standard care | 20 | Beta (4.4, 4.5) | [18] |
| Patient reported time to full recovery: URTI CRP | 14 | Beta (2.3, 6.2) | [18] |
| Patient reported time to full recovery: URTI Standard care | 14 | Beta (2.0, 7.0) | [18] |
| Item | Cost (£) | n | £ Per Test | References / Assumptions |
|---|---|---|---|---|
| Resource Use | ||||
| Number of tests per GP practice | - | 376 | - | Projected from Hughes (2016) [26] assuming constant rate of uptake |
| Estimated life of the CRP Analyser (years) | - | 5 | - | Manufacturer quote (Alere) |
| Fixed Costs | ||||
| Afinion CRP analyser | 1500.00 | - | - | Alere Afinion AS100 analyser (Alere; MA, United States) |
| Connectivity | 120.00 | - | - | Betsi Cadwaladr University Health Board (BCUHB) estimate |
| Printer | 250.00 | - | - | Equal life to analyser |
| Scanner | 125.00 | - | - | Equal life to analyser |
| Total analyser set-up cost | 1995.00 | - | 1.06 | Calculated using machine life and number of tests per year |
| Annual Costs | ||||
| Associated connectivity cost | 20.00 | - | 0.05 | BCUHB estimate |
| Internal quality control (IQC) | 136.00 | - | 0.36 | Guidelines for Wales [48] |
| External quality assurance (EQA): Wales External Quality Assessment Service (WEQAS) | 240.00 | - | 0.64 | Guidelines for Wales [48] |
| Laboratory support (including travel, training, competency, clinical interpretation, quality, and troubleshooting support) | 468.92 | - | 1.25 | BCUHB estimate based on mid-point of AFC scale 2017 at each band and 28.1% on costs |
| Maintenance cost (annual after 3-years) | 280 | - | 0.30 | 3-year warrantee |
| Total annual support costs | £976.92 | - | 2.60 | |
| Variable costs | ||||
| Cartridge/reagent (per test) | - | - | 3.50 | |
| Health care assistant (HCA) time | - | - | 2.42 | Band 4 for 5 minutes [39] |
| Total variable costs | - | - | £5.92 | |
| Total cost | ||||
| Total cost per test | - | - | £9.58 | |
| No. | Parameter | Point Estimate | Distribution 1 | Assumptions/References |
|---|---|---|---|---|
| Lower respiratory tract infection (LRTI) per protocol Probabilities | ||||
| C-reactive protein (CRP) < 20 mg/L | 0.70 | Dirichlet (14, 6, 0) | Raw data [26] | |
| CRP 20–100 mg/L | 0.30 | Dirichlet (6, 14, 0) | Raw data [26] | |
| No antibiotics at index consultation | CRP < 20 mg/L | 1.00 | Dirichlet (14, 0, 0) | [11], Raw data [26] | |
| Delayed prescription at index consultation | CRP 20–100 mg/L | 1.00 | Dirichlet (6, 0, 0) | [11], Raw data [26] | |
| Delayed prescription not dispensed| CRP 20–100 mg/L | 1.00 | Beta (1, 0) | [26] | |
| No re-consultation within 28 days | CRP < 20 mg/L | 0.93 | Beta (13, 1) | Raw data [26] LRTI re-consultation with CRP < 20 mg/L | |
| Re-consultation within 28 days | CRP 20–100 mg/L | 0.00 | Beta (0, 1) | Raw data [26] LRTI re-consultation with CRP 20–100 mg/L | |
| Repeat CRP at re-consultation| CRP < 20 mg/L | 1.00 | Beta (1, 0) | Assumption: CRP repeated at re-consultation if used at index consultation. | |
| No antibiotics at re-consultation | CRP < 20 mg/L | 1.00 | Beta (0, 1) | Assumption: antibiotics only indicated at CRP > 100 mg/L; Hughes et al. (2016) [26] reports no evidence of CRP > 100 mg/L | |
| i | Probability acute respiratory tract infection (ARTI) re-consultation standard care = CRP study data | 0.1143 | [26] | |
| LRTI re-consultation standard care = CRP pilot study | 0.0500 | Raw data [26] | ||
| ii | Cost of antimicrobial resistance per prescription over 28 days2 | |||
| a | European | £0.15 | [27] | |
| a | U.S. | £4.77 | [27] | |
| b | Global | £17.83 | [27] | |
| iii | Cost of dispensing Item dispensing fee for dispensing doctor | £1.90 | [41] | |
| iv | Cost and probability of hospital admission Cost of hospital admission for presenting complaint3 | £826.69 | [43] | |
| Probability of hospital admission: Point-of-care (POC) CRP test | 0.0088 | [11] | ||
| Probability of hospital admission: standard care | 0.0035 | [11] | ||
| v | Probability of antibiotic use in standard care | |||
| Antibiotic prescribing: standard care | 0.53 | [11] | ||
| vi | Cost of amoxicillin prescription | |||
| Amoxicillin capsules: 500 mg three times daily for 5 days | £0.91 | [40] | ||
| Amoxicillin capsules: 500 mg three times daily for 7 days | £1.27 | [40] | ||
| vii | CRP analyser machine life 10-years | 10-years | Assumption |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Holmes, E.A.F.; Harris, S.D.; Hughes, A.; Craine, N.; Hughes, D.A. Cost-Effectiveness Analysis of the Use of Point-of-Care C-Reactive Protein Testing to Reduce Antibiotic Prescribing in Primary Care. Antibiotics 2018, 7, 106. https://doi.org/10.3390/antibiotics7040106
Holmes EAF, Harris SD, Hughes A, Craine N, Hughes DA. Cost-Effectiveness Analysis of the Use of Point-of-Care C-Reactive Protein Testing to Reduce Antibiotic Prescribing in Primary Care. Antibiotics. 2018; 7(4):106. https://doi.org/10.3390/antibiotics7040106
Chicago/Turabian StyleHolmes, Emily A. F., Sharman D. Harris, Alison Hughes, Noel Craine, and Dyfrig A. Hughes. 2018. "Cost-Effectiveness Analysis of the Use of Point-of-Care C-Reactive Protein Testing to Reduce Antibiotic Prescribing in Primary Care" Antibiotics 7, no. 4: 106. https://doi.org/10.3390/antibiotics7040106
APA StyleHolmes, E. A. F., Harris, S. D., Hughes, A., Craine, N., & Hughes, D. A. (2018). Cost-Effectiveness Analysis of the Use of Point-of-Care C-Reactive Protein Testing to Reduce Antibiotic Prescribing in Primary Care. Antibiotics, 7(4), 106. https://doi.org/10.3390/antibiotics7040106