The Growing Threat of Gonococcal Blindness

 , , and
, , and 
Abstract
1. Introduction
1.1. Ophthalmia Neonatorum
1.2. Adult Eye Infections
1.3. Treatments for Ophthalmia Neonatorum
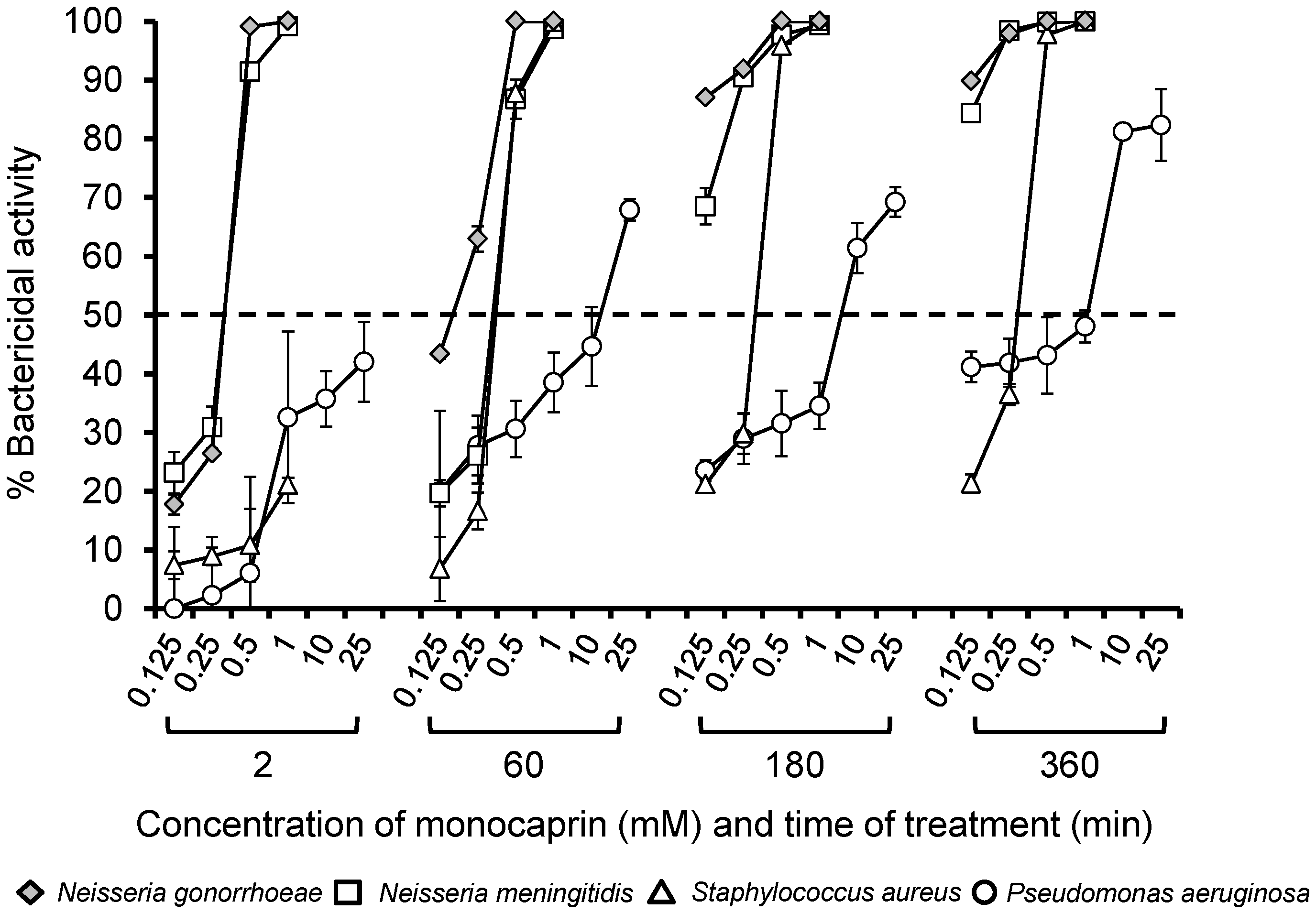
1.4. Anti-Gonococcal Properties of Monocaprin
2. Results and Discussion
3. Materials and Methods
3.1. Bacteria and Growth Conditions
3.2. Bactericidal Assay
4. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Epling, J. Bacterial conjunctivitis. BMJ Clin. Evid. 2012, 2012, 0704. [Google Scholar] [PubMed]
- Laga, M.; Meheus, A.; Piot, P. Epidemiology and control of gonococcal ophthalmia neonatorum. Bull. World Health Organ. 1989, 67, 471–477. [Google Scholar] [PubMed]
- McElnea, E.; Stapleton, P.; Khan, S.; Stokes, J.; Higgins, G. Challenges in the management of Neisseria gonorrhoeae keratitis. Int. Ophthalmol. 2015, 35, 135–140. [Google Scholar] [CrossRef] [PubMed]
- Strand, C.L.; Arango, V.A. Gonococcal ophthalmia neonatorum after delivery by cesarean section: Report of a case. Sex. Transm. Dis. 1979, 6, 77–78. [Google Scholar] [CrossRef] [PubMed]
- Msukwa, G.; Batumba, N.; Drucker, M.; Menezes, L.; Ranjit, R. Maternal and neonatal risk factors associated with vertical transmission of ophthalmia neonatorum in neonates receiving health care in Blantyre, Malawi. Middle East Afr. J. Ophthalmol. 2014, 21, 240–243. [Google Scholar] [CrossRef] [PubMed]
- Delpech, V.; Martin, I.M.C.; Hughes, G.; Nichols, T.; James, L.; Ison, C.A. Epidemiology and clinical presentation of gonorrhoea in England and Wales: Findings from the Gonococcal Resistance to Antimicrobials Surveillance Programme 2001–2006. Sex. Transm. Infect. 2009, 85, 317. [Google Scholar] [CrossRef] [PubMed]
- Lehman, S.S. An uncommon cause of ophthalmia neonatorum: Neisseria meningitidis. J. Am. Assoc. Pediatr. Ophthalmol. Strabismus 1999, 3, 316. [Google Scholar] [CrossRef]
- Mitchell, S.R.; Katz, P. Disseminated neisserial infection in pregnancy: The empress may have a change of clothing. Obstet. Gynecol. Surv. 1989, 44, 780–788. [Google Scholar] [PubMed]
- McAnena, L.; Knowles, S.J.; Curry, A.; Cassidy, L. Prevalence of gonococcal conjunctivitis in adults and neonates. Eye (Lond.) 2015, 29, 875–880. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.J.S.; Ali, B. Gonococcus—The culprit of refractory, severe conjunctivitis in an elderly patient. Contact Lens Anter. Eye 2015, 38, 468–470. [Google Scholar] [CrossRef] [PubMed]
- Matters, R.; Wong, I.; Mak, D. An outbreak of non-sexually transmitted gonococcal conjunctivitis in Central Australia and the Kimberley region. Commun. Dis. Intel. 1998, 22, 57–58. [Google Scholar]
- Harry, T.C.; Black, P.D. Unilateral gonococcal ophthalmia without genital infection: An unusual presentation in an adult. Int. J. STD AIDS 2005, 16, 78–79. [Google Scholar] [CrossRef] [PubMed]
- Mak, D.B.; Smith, D.W.; Harnett, G.B.; Plant, A.J. A large outbreak of conjunctivitis caused by a single genotype of Neisseria gonorrhoeae distinct from those causing genital tract infections. Epidemiol. Infect. 2001, 126, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Mikru, F.S.; Molla, T.; Ersumo, M.; Henriksen, T.H.; Klungseyr, P.; Hudson, P.J.; Kindan, T.T. Community-wide outbreak of Neisseria gonorrhoeae conjunctivitis in Konso district, North Omo administrative region. Ethiop. Med. J. 1991, 29, 27–35. [Google Scholar] [PubMed]
- Di Bartolomeo, S.; Mirta, D.H.; Janer, M.; Rodriguez Fermepin, M.R.; Sauka, D.; Magariños, F.; de Torres, R.A. Incidence of Chlamydia trachomatis and other potential pathogens in neonatal conjunctivitis. Int. J. Infect. Dis. 2001, 5, 139–143. [Google Scholar] [CrossRef]
- Abraha, M.; Egli-Gany, D.; Low, N. Epidemiological, behavioural, and clinical factors associated with antimicrobial-resistant gonorrhoea: A review. F1000Research 2018, 7. [Google Scholar] [CrossRef] [PubMed]
- Nadel, S. Treatment of meningococcal disease. J. Adolesc. Health 2016, 59, S28. [Google Scholar] [CrossRef] [PubMed]
- Moore, D.L.; MacDonald, N.E. Preventing ophthalmia neonatorum. Paediatr. Child Health 2015, 20, 93–96. [Google Scholar] [CrossRef] [PubMed]
- Khauv, P.; Turner, P.; Soeng, C.; Soeng, S.; Moore, C.E.; Bousfield, R.; Stoesser, N.; Emary, K.; Thanh, D.P.; Baker, S.; et al. Ophthalmic infections in children presenting to Angkor Hospital for Children, Siem Reap, Cambodia. BMC Res. Notes 2014, 7. [Google Scholar] [CrossRef] [PubMed]
- Vernel-Pauillac, F.; Ratsima, E.H.; Guillard, B.; Goursaud, R.; Lethezer, C.; Hem, S.; Merien, F.; Goarant, C. Correlation between antibiotic susceptibilities and genotypes in Neisseria gonorrhoeae from different geographical origins: Determinants monitoring by real-time PCR as a complementary tool for surveillance. Sex. Transm. Infect. 2010, 86, 106–111. [Google Scholar] [CrossRef] [PubMed]
- Tang, S.; Li, M.; Chen, H.; Ping, G.; Zhang, C.; Wang, S. A chronological study of the bacterial pathogen changes in acute neonatal bacterial conjunctivitis in southern China. BMC Ophthalmol. 2017, 17. [Google Scholar] [CrossRef] [PubMed]
- Zloto, O.; Gharaibeh, A.; Mezer, E.; Stankovic, B.; Isenberg, S.; Wygnanski-Jaffe, T. Ophthalmia neonatorum treatment and prophylaxis: IPOSC global study. Graefes Arch. Clin. Exp. Ophthalmol. 2016, 254, 577–582. [Google Scholar] [CrossRef] [PubMed]
- Matejcek, A.; Goldman, R.D. Treatment and prevention of ophthalmia neonatorum. Can. Fam. Phys. 2013, 59, 1187–1190. [Google Scholar]
- Darling, E.K.; McDonald, H. A meta-analysis of the efficacy of ocular prophylactic agents used for the prevention of gonococcal and chlamydial ophthalmia neonatorum. J. Midwifery Women’s Health 2010, 55, 319–327. [Google Scholar] [CrossRef] [PubMed]
- Nishida, H.; Risemberg, H.M. Silver nitrate ophthalmic solution and chemical conjunctivities. Pediatrics 1975, 56, 368–373. [Google Scholar] [PubMed]
- Fishman, R. The earliest success of penicillin. Am. J. Ophthalmol. 2016, 163, 204. [Google Scholar] [CrossRef] [PubMed]
- Ali, Z.; Khadije, D.; Elahe, A.; Mohammad, M.; Fateme, Z.; Narges, Z. Prophylaxis of ophthalmia neonatorum comparison of betadine, erythromycin and no prophylaxis. J. Trop. Pediatr. 2007, 53, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Isenberg, S.J.; Apt, L.; Wood, M. A controlled trial of povidone-iodine as prophylaxis against ophthalmia neonatorum. N. Engl. J. Med. 1995, 332, 562–566. [Google Scholar] [CrossRef] [PubMed]
- Butt, U.; ElShaer, A.; Snyder, L.A.S.; Al-Kinani, A.A.; Le Gresley, A.; Alany, R.G. Fatty acid based microemulsions to combat ophthalmia neonatorum caused by Neisseria gonorrhoeae and Staphylococcus aureus. Nanomaterials 2018, 8. [Google Scholar] [CrossRef] [PubMed]
- Churchward, C.P.; Alany, R.G.; Kirk, R.S.; Walker, A.J.; Snyder, L.A.S. Prevention of ophthalmia neonatorum caused by Neisseria gonorrhoeae using a fatty acid-based formulation. mBio 2017, 8, e00534. [Google Scholar] [CrossRef] [PubMed]
- Churchward, C.P.; Calder, A.; Snyder, L.A.S. Mutations in Neisseria gonorrhoeae grown in sub-lethal concentrations of monocaprin do not confer resistance. PLoS ONE 2018, 13, e0195453. [Google Scholar] [CrossRef] [PubMed]
- Thormar, H.; Bergsson, G.; Gunnarsson, E.; Georgsson, G.; Witvrouw, M.; Steingrimsson, O.; De Clercq, E.; Kristmundsdottir, T. Hydrogels containing monocaprin have potent microbicidal activities against sexually transmitted viruses and bacteria in vitro. Sex. Transm. Infect. 1999, 75, 181–185. [Google Scholar] [CrossRef] [PubMed]
- Taube, M.; del Mar Cendra, M.; Elsahn, A.; Christodoulides, M.; Hossain, P. Pattern recognition receptors in microbial keratitis. Eye 2015, 29, 1399–1415. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.S.; Choi, H.Y.; Lee, J.E.; Lee, S.H.; Oum, B.S. Gonococcal keratoconjunctivitis in adults. Eye 2002, 16, 646–649. [Google Scholar] [CrossRef] [PubMed]
- Churchward, C.P.; Alany, R.G.; Snyder, L.A.S. Alternative antimicrobials: The properties of fatty acids and monoglycerides. Crit. Rev. Microbiol. 2018, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Hagman, K.E.; Pan, W.; Spratt, B.G.; Balthazar, J.T.; Judd, R.C.; Shafer, W.M. Resistance of Neisseria gonorrhoeae to antimicrobial hydrophobic agents is modulated by the mtrRCDE efflux system. Microbiology 1995, 141, 611–622. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.H.; Shafer, W.M. The farAB-encoded efflux pump mediates resistance of gonococci to long-chained antibacterial fatty acids. Mol. Microbiol. 1999, 33, 839–845. [Google Scholar] [CrossRef] [PubMed]
- Mueller, E.A.; Schlievert, P.M. Non-aqueous glycerol monolaurate gel exhibits antibacterial and anti-biofilm activity against Gram-positive and Gram-negative pathogens. PLoS ONE 2015, 10, e0120280. [Google Scholar] [CrossRef] [PubMed]
- Schlievert, P.M.; Peterson, M.L. Glycerol monolaurate antibacterial activity in broth and biofilm cultures. PLoS ONE 2012, 7, e40350. [Google Scholar] [CrossRef] [PubMed]
- Sun, C.Q.; O’Connor, C.J.; Roberton, A.M. Antibacterial actions of fatty acids and monoglycerides against Helicobacter pylori. FEMS Immunol. Med. Microbiol. 2003, 36, 9–17. [Google Scholar] [CrossRef]
- Vincent, L.R.; Jerse, A.E. Biological feasibility and importance of a gonorrhea vaccine for global public health. Vaccine 2018. [Google Scholar] [CrossRef] [PubMed]
- Hill, S.A.; Masters, T.L.; Wachter, J. Gonorrhea—An evolving disease of the new millennium. Microb. Cell 2016, 3, 371–389. [Google Scholar] [CrossRef] [PubMed]
- Tong, L.; Tan, D.T.H.; Abańo, J.M.; Lim, L. Deep anterior lamellar keratoplasty in a patient with descemetocele following gonococcal keratitis. Am. J. Ophthalmol. 2004, 138, 506–507. [Google Scholar] [CrossRef] [PubMed]
- Samira, N.; Bani, A.P.; Susiyanti, M. Rare case of bilateral perforated corneal ulcer due to gonococcal infection, managed with temporary periosteal graft. BMJ Case Rep. 2016, 2016, bcr2015213547. [Google Scholar] [CrossRef] [PubMed]
- Cendra, M.d.M.; Christodoulides, M.; Hossain, P. Signaling mediated by Toll-Like Receptor 5 sensing of Pseudomonas aeruginosa flagellin influences IL-1β and IL-18 production by primary fibroblasts derived from the human cornea. Front. Cell. Infect. Microbiol. 2017, 7. [Google Scholar] [CrossRef] [PubMed]
- McGuinness, B.T.; Clarke, I.N.; Lambden, P.R.; Barlow, A.K.; Heckels, J.E.; Poolman, J.T.; Jones, D.M. Point mutation in meningococcal porA gene associated with increased endemic disease. Lancet 1991, 337, 514–517. [Google Scholar] [CrossRef]
- Ward, M.E.; Watt, P.J.; Glynn, A.A. Gonococci in urethral exudates possess a virulence factor lost on subculture. Nature 1970, 227, 382–384. [Google Scholar] [CrossRef] [PubMed]
- Zak, K.; Diaz, J.L.; Jackson, D.; Heckels, J.E. Antigenic variation during infection with Neisseria gonorrhoeae: Detection of antibodies to surface proteins in sera of patients with gonorrhea. J. Infect. Dis. 1984, 149, 166–174. [Google Scholar] [CrossRef] [PubMed]
- Christodoulides, M.; Brooks, J.L.; Rattue, E.; Heckels, J.E. Immunisation with recombinant class 1 outer membrane protein from Neisseria meningitidis: Influence of liposomes and adjuvants on antibody avidity, recognition of native protein and the induction of a bactericidal immune response against meningococci. Microbiology 1990, 144, 3027–3037. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Treatment | Efficacy | Contraindications | Reference |
|---|---|---|---|
| Silver nitrate | Prophylaxis reduced cases of disease. | Chemical conjunctivitis; toxicity; failures. | [25] |
| Penicillin | Treatment cured disease. | Resistance developed. | [26] |
| 1% Tetracycline | Prophylaxis and treatment cured disease. Often used in conjunction with saline washes in low- and middle-income countries (LMICs) where prophylaxis is available. | Resistance developed. | [2,5,20] |
| Erythromycin | Treatment cured disease. | Resistance developed. | [18] |
| Saline washes | May reduce accumulation of purulent discharge. | Unlikely to eliminate infection. | [5,20] |
| Povidone-iodine (betadine, 1.25% or 2.5% (v/v) solutions) | Prophylaxis reduced cases of disease. | 5% rate of chemical conjunctivitis; failure to eradicate infection; not recommended. (https://www.cdc.gov/std/tg2015/gonorrhea.htm) | [25,27,28] |
© 2018 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Dolange, V.; Churchward, C.P.; Christodoulides, M.; Snyder, L.A.S. The Growing Threat of Gonococcal Blindness. Antibiotics 2018, 7, 59. https://doi.org/10.3390/antibiotics7030059
Dolange V, Churchward CP, Christodoulides M, Snyder LAS. The Growing Threat of Gonococcal Blindness. Antibiotics. 2018; 7(3):59. https://doi.org/10.3390/antibiotics7030059
Chicago/Turabian StyleDolange, Victoria, Colin P. Churchward, Myron Christodoulides, and Lori A. S. Snyder. 2018. "The Growing Threat of Gonococcal Blindness" Antibiotics 7, no. 3: 59. https://doi.org/10.3390/antibiotics7030059
APA StyleDolange, V., Churchward, C. P., Christodoulides, M., & Snyder, L. A. S. (2018). The Growing Threat of Gonococcal Blindness. Antibiotics, 7(3), 59. https://doi.org/10.3390/antibiotics7030059