
Distribution and Determinants of Antibiotic Self-Medication: A Cross-Sectional Study in Chinese Residents



Abstract
1. Introduction
2. Results
2.1. Study Participants
2.2. Distribution of ASM
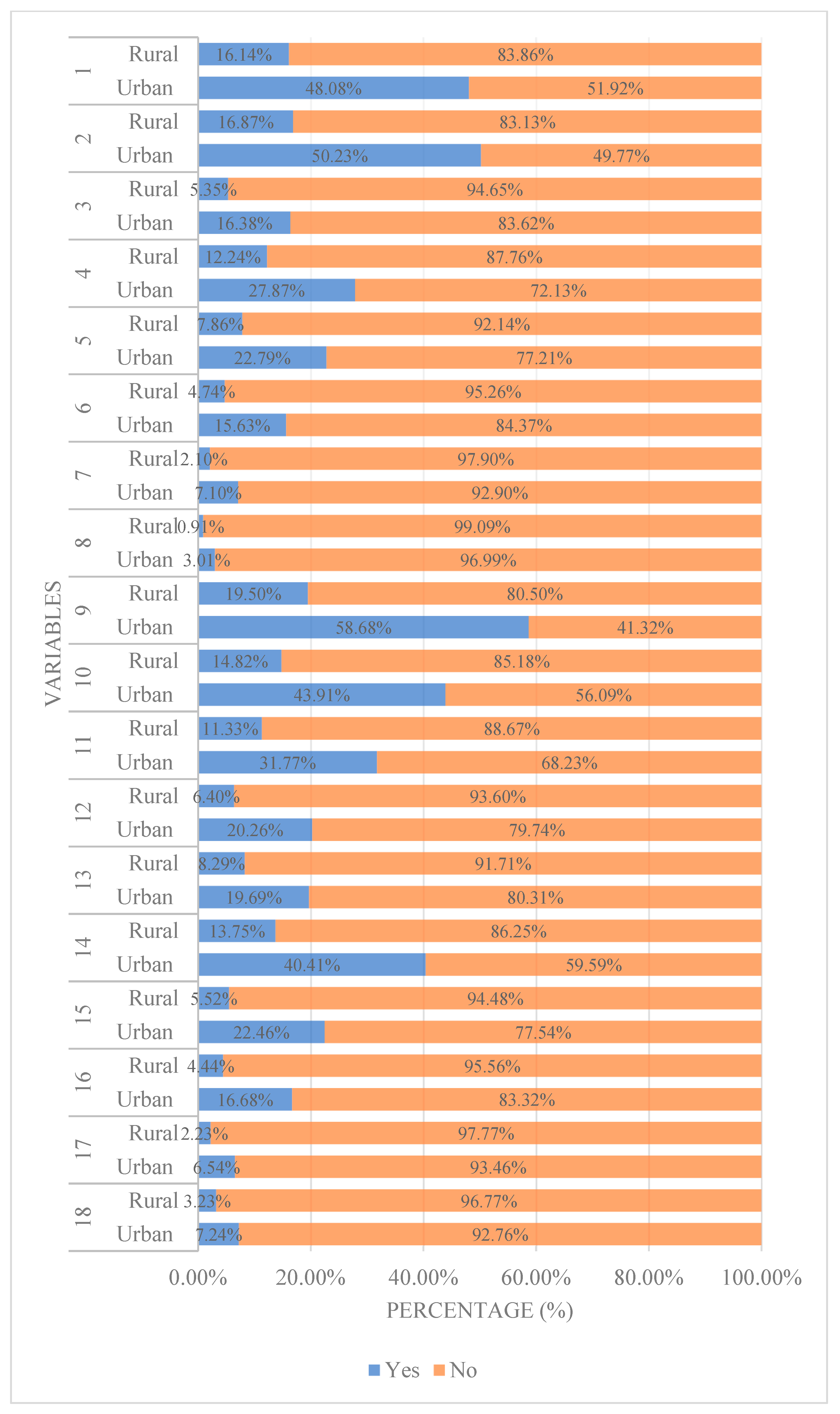
2.3. Considerations of ASM Practitioners
2.4. Determinants of ASM
3. Discussion
4. Materials and Methods
4.1. Study Design and Population
4.2. The Questionnaire and Data Collection
4.3. Statistical Analysis
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: A systematic analysis. Lancet 2022, 399, 629–655. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- O’Neill, J. Antimicrobial Resistance: Tackling a Crisis for the Health and Wealth of Nations. 2014. Available online: https://amr-review.org/ (accessed on 28 April 2025).
- Li, J.; Song, X.; Yang, T.; Chen, Y.; Gong, Y.; Yin, X.; Lu, Z. A systematic review of antibiotic prescription associated with upper respiratory tract infections in China. Medicine 2016, 95, e3587. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zhang, Q.Q.; Ying, G.G.; Pan, C.G.; Liu, Y.S.; Zhao, J.L. Comprehensive evaluation of antibiotics emission and fate in the river basins of China: Source analysis, multimedia modeling, and linkage to bacterial resistance. Environ. Sci. Technol. 2015, 49, 6772–6782. [Google Scholar] [CrossRef] [PubMed]
- Ateshim, Y.; Bereket, B.; Major, F.; Emun, Y.; Woldai, B.; Pasha, I.; Habte, E.; Russom, M. Prevalence of self-medication with antibiotics and associated factors in the community of Asmara, Eritrea: A descriptive cross sectional survey. BMC Public Health 2019, 19, 726. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sachdev, C.; Anjankar, A.; Agrawal, J. Self-medication with antibiotics: An element increasing resistance. Cureus 2022, 14, e30844. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Zeb, S.; Mushtaq, M.; Ahmad, M.; Saleem, W.; Rabaan, A.A.; Naqvi, B.S.Z.; Garout, M.; Aljeldah, M.; Al-Shammari, B.R.; Al-Faraj, N.J.; et al. Self-medication as an important risk factor for antibiotic resistance: A multi-institutional survey among students. Antibiotics 2022, 11, 842. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- World Health Organization. Global Action Plan on Antimicrobial Resistance, Geneva, Switzerland. 2015. Available online: https://apps.who.int/iris/bitstream/handle/10665/193736/9789241509763_eng.pdf?sequence=1&isAllowed=y (accessed on 25 May 2025).
- World Health Organization. Antimicrobial Resistance: No Action Today, No Cure Tomorrow, Geneva, Switzerland. 2011. Available online: https://www.who.int/dg/speeches/detail/antimicrobial-resistance-no-action-today-no-cure-tomorrow (accessed on 28 April 2025).
- G20 Summits. Communiqué of the G20 Leaders, Hangzhou, China. 2016. Available online: http://www.g20chn.org/hywj/dncgwj/201609/t20160906_3392.html (accessed on 23 May 2025).
- Li, H.; Yan, S.; Li, D.; Gong, Y.; Lu, Z.; Yin, X. Trends and patterns of outpatient and inpatient antibiotic use in China’s hospitals: Data from the Center for Antibacterial Surveillance, 2012–2016. J. Antimicrob. Chemother. 2019, 74, 1731–1740. [Google Scholar] [CrossRef] [PubMed]
- National Health and Family Planning Commission of the People’s Republic of China. China’s National Action Plan to Contain Antimicrobial Resistance. 2016. Available online: http://www.nhc.gov.cn/yzygj/s3593/201608/f1ed26a0c8774e1c8fc89dd481ec84d7.shtml (accessed on 25 May 2025).
- Fang, Y. China should curb non-prescription use of antibiotics in the community. BMJ 2014, 348, g4233. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Chang, J.; Liu, X.; Zhai, P.; Hu, S.; Li, P.; Hayat, K.; Kabba, J.A.; Feng, Z.; Yang, C.; et al. Dispensing antibiotics without a prescription for acute cough associated with common cold at community pharmacies in shenyang, northeastern china: A cross-sectional study. Antibiotics 2020, 9, 163. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Widowati, I.G.A.R.; Budayanti, N.N.S.; Januraga, P.P.; Duarsa, D.P. Self-medication and self-treatment with short-term antibiotics in Asian countries: A literature review. Pharm. Educ. 2021, 21, 152–162. [Google Scholar] [CrossRef]
- Huh, K.; Chung, D.R.; Kim, S.H.; Cho, S.Y.; Ha, Y.E.; Kang, C.I.; Peck, K.R.; Song, J.H. Factors affecting the public awareness and behavior on antibiotic use. Eur. J. Clin. Microbiol. Infect. Dis. 2018, 37, 1547–1552. [Google Scholar] [CrossRef] [PubMed]
- Demoré, B.; Mangin, L.; Tebano, G.; Pulcini, C.; Thilly, N. Public knowledge and behaviours concerning antibiotic use and resistance in France: A cross-sectional survey. Infection 2017, 45, 513–520. [Google Scholar] [CrossRef] [PubMed]
- Xiao, Y.; Zhang, J.; Zheng, B.; Zhao, L.; Li, S.; Li, L. Changes in Chinese policies to promote the rational use of antibiotics. PLoS Med. 2013, 10, e1001556. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Do, N.T.T.; Vu, H.T.L.; Nguyen, C.T.K.; Punpuing, S.; Khan, W.A.; Gyapong, M.; Asante, K.P.; Munguambe, K.; Gómez-Olivé, F.X.; John-Langba, J.; et al. Community-based antibiotic access and use in six low-income and middle-income countries: A mixed-method approach. Lancet Glob. Health 2021, 9, e610–e619. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- National Bureau of statistics of China. China Statistical Yearbook 2024. Available online: https://www.stats.gov.cn/sj/ndsj/2024/indexeh.htm (accessed on 30 June 2025).
- National Medical Products Administration (NMPA) Center for Qualification of Licensed Pharmacists. National Licensed Pharmacist Statistics, May 2025. Available online: http://www.cqlp.org/info/link.aspx?id=7719&page=1 (accessed on 30 June 2025).
- Shi, J.; Jin, H.; Shi, L.; Chen, C.; Ge, X.; Lu, Y.; Zhang, H.; Wang, Z.; Yu, D. The quality of primary care in community health centers: Comparison among urban, suburban and rural users in Shanghai, China. BMC Fam. Pract. 2020, 21, 178. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, X.; Lu, J.; Hu, S.; Cheng, K.K.; De, M.J.; Meng, Q.; Mossialos, E.; Xu, D.R.; Yip, W.; Zhang, H.; et al. The primary health-care system in China. Lancet 2017, 390, 2584–2594. [Google Scholar] [CrossRef] [PubMed]
- Monnet, D.L.; Harbarth, S. Will coronavirus disease (COVID-19) have an impact on antimicrobial resistance? Euro Surveill. 2020, 25, 2001886. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Yang, Y.; Fan, S.; Chen, W.; Wu, Y. Broader open data needed in psychiatry: Practice from the psychology and behavior investigation of chinese residents. Alpha Psychiatry 2024, 25, 564–565. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Ye, D.; Chang, J.; Yang, C.; Yan, K.; Ji, W.; Aziz, M.M.; Gillani, A.H.; Fang, Y. How does the general public view antibiotic use in China? Result from a cross-sectional survey. Int. J. Clin. Pharm. 2017, 39, 927–934. [Google Scholar] [CrossRef] [PubMed]
- Deng, P.; Yu, J.; Zhou, N.; Hu, M. Access to medicines for acute illness and antibiotic use in residents: A medicines household survey in Sichuan Province, western China. PLoS ONE 2018, 13, e0201349. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- McNulty, C.A.; Boyle, P.; Nichols, T.; Clappison, P.; Davey, P. Don’t wear me out--the public’s knowledge of and attitudes to antibiotic use. J. Antimicrob. Chemother. 2007, 59, 727–738. [Google Scholar] [CrossRef] [PubMed]
- Virmani, S.; Nandigam, M.; Kapoor, B.; Makhija, P.; Nair, S. Antibiotic use among health science students in an Indian University: A cross sectional study. Clin. Epidemiol. Glob. Health 2017, 5, 176–179. [Google Scholar] [CrossRef]
- World Health Organization. Using Indicators to Measure Country Pharmaceutical Situations: Fact Book on WHO Level I and Level II Monitoring Indicators. 2006. Available online: https://iris.who.int/bitstream/handle/10665/354554/WHO-TCM-2006.2-eng.pdf (accessed on 23 May 2025).
- Grigoryan, L.; Burgerhof, J.G.; Degener, J.E.; Deschepper, R.; Lundborg, C.S.; Monnet, D.L.; Scicluna, E.A.; Birkin, J.; Haaijer-Ruskamp, F.M.; SAR consortium. Attitudes, beliefs and knowledge concerning antibiotic use and self-medication: A comparative European study. Pharmacoepidemiol. Drug Saf. 2007, 16, 1234–1243. [Google Scholar] [CrossRef] [PubMed]
- Llor, C.; Bjerrum, L. Background for different use of antibiotics in different countries. Clin. Infect. Dis. 2005, 40, 333. [Google Scholar] [CrossRef] [PubMed]
- Frazer, J.S.; Frazer, G.R. Analysis of primary care prescription trends in England during the COVID-19 pandemic compared against a predictive model. Fam. Med. Community Health 2021, 9, e001143. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Mitsi, G.; Jelastopulu, E.; Basiaris, H.; Skoutelis, A.; Gogos, C. Patterns of antibiotic use among adults and parents in the community: A questionnaire-based survey in a Greek urban population. Int. J. Antimicrob. Agents 2005, 25, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Smith, D.R.M.; Dolk, F.C.K.; Smieszek, T.; Robotham, J.V.; Pouwels, K.B. Understanding the gender gap in antibiotic prescribing: A cross-sectional analysis of English primary care. BMJ Open 2018, 8, e020203. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- McNulty, C.A.; Boyle, P.; Nichols, T.; Clappison, P.; Davey, P. The public’s attitudes to and compliance with antibiotics. J. Antimicrob. Chemother. 2007, 60, 63–68. [Google Scholar] [CrossRef] [PubMed]
- Awad, A.; Eltayeb, I.; Matowe, L.; Thalib, L. Self-medication with antibiotics and antimalarials in the community of Khartoum State, Sudan. J. Pharm. Pharm. Sci. 2005, 8, 326–331. [Google Scholar] [PubMed]
- Bogale, A.A.; Amhare, A.F.; Chang, J.; Bogale, H.A.; Betaw, S.T.; Gebrehiwot, N.T.; Fang, Y. Knowledge, attitude, and practice of self-medication with antibiotics among community residents in Addis Ababa, Ethiopia. Expert. Rev. Anti Infect. Ther. 2019, 17, 459–466. [Google Scholar] [CrossRef] [PubMed]
- Vahedi, S.; Jalali, F.S.; Bayati, M.; Delavari, S. Predictors of self-medication in Iran: A notional survey study. Iran. J. Pharm. Res. 2021, 20, 348–358. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Grigoryan, L.; Haaijer-Ruskamp, F.M.; Burgerhof, J.G.; Mechtler, R.; Deschepper, R.; Tambic-Andrasevic, A.; Andrajati, R.; Monnet, D.L.; Cunney, R.; Di-Matteo, A.; et al. Self-medication with antimicrobial drugs in Europe. Emerg. Infect. Dis. 2006, 12, 452–459. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lukovic, J.A.; Miletic, V.; Pekmezovic, T.; Trajkovic, G.; Ratkovic, N.; Aleksic, D.; Grgurevic, A. Self-medication practices and risk factors for self-medication among medical students in Belgrade, Serbia. PLoS ONE 2014, 9, e114644. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Nie, B.; Chapman, S.C.E.; Chen, Z.; Wang, X.; Wei, L. Utilization of the beliefs about medicine questionnaire and prediction of medication adherence in China: A systematic review and meta-analysis. J. Psychosom. Res. 2019, 122, 54–68. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Zhou, M.; Yu, W.; Wang, H. Changes in social support among patients with hematological malignancy undergoing hematopoietic stem cell transplantation in Souzhou, China. Indian J. Cancer 2020, 57, 253–261. [Google Scholar] [CrossRef] [PubMed]
- Awuah, R.B.; Asante, P.Y.; Sakyi, L.; Biney, A.A.E.; Kushitor, M.K.; Agyei, F.; de-Graft Aikins, A. Factors associated with treatment-seeking for malaria in urban poor communities in Accra, Ghana. Malar. J. 2018, 17, 168. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Maibach, E.W.; Leiserowitz, A.; Roser-Renouf, C.; Mertz, C.K. Identifying like-minded audiences for global warming public engagement campaigns: An audience segmentation analysis and tool development. PLoS ONE 2011, 6, e17571. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Chandran, D.S.; Manickavasagam, P.P. Sale of antibiotics without prescription in stand-alone pharmacies in Tamil Nadu. J. Fam. Med. Prim. Care 2022, 11, 5516–5520. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bianco, A.; Licata, F.; Trovato, A.; Napolitano, F.; Pavia, M. Antibiotic-dispensing practice in community pharmacies: Results of a cross-sectional study in Italy. Antimicrob. Agents Chemother. 2021, 65, e02729-20. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Li, Y.; Xu, J.; Wang, F.; Wang, B.; Liu, L.; Hou, W.; Fan, H.; Tong, Y.; Zhang, J.; Lu, Z. Overprescribing in China, driven by financial incentives, results in very high use of antibiotics, injections, and corticosteroids. Health Aff. 2012, 31, 1075–1082. [Google Scholar] [CrossRef] [PubMed]
- Licata, F.; Angelillo, S.; Oliverio, A.; Bianco, A. The Internet: Friend or foe of antibiotic resistance? Results of a cross-sectional study among Italian university students. Antibiotics 2021, 10, 1091. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bianco, A.; Licata, F.; Zucco, R.; Papadopoli, R.; Pavia, M. Knowledge and practices regarding antibiotics use: Findings from a cross-sectional survey among Italian adults. Evol. Med. Public Health 2020, 2020, 129–138. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wang, D.; Ge, P.; Xue, D.M.; Hu, C.; Huang, G.; Qi, J.; Hong, W.Y.; Pan, L.; Han, X.; Zhang, J.; et al. Prevalence and associated factors influencing the use of antibiotics for self-medication among Chinese residents: A cross-sectional study in 2021. Arch. Public Health 2025, 83, 107. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- World Health Organization. Antibiotic Resistance: Multi-Country Public Awareness Survey, Geneva, Switzerland 2015. Available online: http://apps.who.int/iris/bitstream/10665/194460/1/9789241509817_eng.pdf (accessed on 23 April 2025).
- Xiao, Y.; Li, L. Legislation of clinical antibiotic use in China. Lancet Infect. Dis. 2013, 13, 189–191. [Google Scholar] [CrossRef] [PubMed]
- Bartoloni, A.; Cutts, F.; Leoni, S.; Austin, C.C.; Mantella, A.; Guglielmetti, P.; Roselli, M.; Salazar, E.; Paradisi, F. Patterns of antimicrobial use and antimicrobial resistance among healthy children in Bolivia. Trop. Med. Int. Health 1998, 3, 116–123. [Google Scholar] [CrossRef] [PubMed]
- Chang, J.; Xu, S.; Zhu, S.; Li, Z.; Yu, J.; Zhang, Y.; Zu, J.; Fang, Y.; Ross-Degnan, D. Assessment of non-prescription antibiotic dispensing at community pharmacies in China with simulated clients: A mixed cross-sectional and longitudinal study. Lancet Infect. Dis. 2019, 19, 1345–1354. [Google Scholar] [CrossRef] [PubMed]
- Stivers, T. Managing patient pressure to prescribe antibiotics in the clinic. Paediatr. Drugs 2021, 23, 437–443. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Bianco, A.; Licata, F.; Nobile, C.G.; Napolitano, F.; Pavia, M. Pattern and appropriateness of antibiotic prescriptions for upper respiratory tract infections in primary care paediatric patients. Int. J. Antimicrob. Agents 2022, 59, 106469. [Google Scholar] [CrossRef] [PubMed]
- Bianco, A.; Papadopoli, R.; Mascaro, V.; Pileggi, C.; Pavia, M. Antibiotic prescriptions to adults with acute respiratory tract infections by Italian general practitioners. Infect. Drug Resist. 2018, 11, 2199–2205. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- China Family News. CFHI-2021 China Family Health Index Survey General Report. Available online: https://www.cfnews.org.cn/newsinfo/2685237.html (accessed on 21 May 2025).
- Song, Q.; Smith, J.P. Hukou system, mechanisms, and health stratification across the life course in rural and urban China. Health Place 2019, 58, 102150. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]

{kind=link}
| Variables | n (%) | χ2 | p-Value | ||
|---|---|---|---|---|---|
| Urban | Rural | Total | |||
| Total | 8008 (72.60) | 3023 (27.40) | 11,031 (100.00) | ||
| Gender | 0.0831 | 0.7731 | |||
| Male | 3647 (45.54) | 1386 (45.86) | 5033 (45.63) | ||
| Female | 4361 (54.56) | 1637 (54.15) | 5998 (54.37) | ||
| Age (years) | 179.8654 | <0.0001 | |||
| 0–30 | 3377 (42.17) | 1288 (42.61) | 4665 (42.29) | ||
| 31–45 | 2325 (29.03) | 676 (22.36) | 3001 (27.21) | ||
| 46–59 | 1652 (20.63) | 566 (18.72) | 2218 (20.11) | ||
| 60– | 654 (8.17) | 493 (16.31) | 1147 (10.40) | ||
| BMI (kg/m2) | 3.7998 | 0.1496 | |||
| <18.5 | 1103 (13.77) | 459 (15.18) | 1562 (14.16) | ||
| 18.5–24.9 | 5510 (68.81) | 2035 (67.32) | 7545 (68.40) | ||
| 25– | 1395 (17.42) | 529 (17.50) | 1924 (17.44) | ||
| Spouse | 34.7433 | <0.0001 | |||
| Yes | 2243 (60.34) | 3983 (54.56) | 6226 (56.44) | ||
| No | 1474 (39.66) | 3331 (45.54) | 4805 (43.56) | ||
| Education level | 832.9165 | <0.0001 | |||
| Primary or below | 473 (5.91) | 654 (21.63) | 1127 (10.22) | ||
| Secondary | 2272 (28.37) | 1145 (37.88) | 3417 (30.98) | ||
| Higher | 5263 (65.72) | 1224 (40.49) | 6487 (58.81) | ||
| Occupation | 527.0434 | <0.0001 | |||
| Unemployed | 4496 (56.14) | 2379 (78.70) | 6875 (62.32) | ||
| Blue-collar | 992 (12.39) | 295 (9.76) | 1287 (11.67) | ||
| White-collar | 2520 (31.47) | 349 (11.54) | 2869 (26.01) | ||
| Monthly household income per capita | 1020.805 | <0.0001 | |||
| 0–3000 | 1714 (21.40) | 1532 (50.68) | 3246 (29.43) | ||
| 3001–6000 | 3229 (40.32) | 1025 (33.91) | 4254 (38.56) | ||
| 6001– | 3065 (38.27) | 466 (15.42) | 3531 (32.01) | ||
| Medical insurance | 60.1299 | <0.0001 | |||
| Resident/employee | 6083 (75.96) | 2206 (72.97) | 8289 (75.14) | ||
| Commercial | 203 (2.53) | 34 (1.12) | 237 (2.15) | ||
| Government-funded | 168 (2.10) | 38 (1.26) | 206 (1.87) | ||
| Out-of-pocket payment | 1554 (19.41) | 745 (24.64) | 2299 (20.84) | ||
| Number of chronic diseases | 11.7185 | 0.0029 | |||
| none | 6644 (82.97) | 2442 (80.78) | 9086 (82.37) | ||
| Single | 932 (11.64) | 369 (12.21) | 1301 (11.79) | ||
| Multiple | 432 (5.39) | 212 (7.01) | 644 (5.84) | ||
| Smoking history | 15.2551 | <0.0001 | |||
| Yes | 1514 (18.91) | 672 (22.23) | 2186 (19.82) | ||
| No | 6494 (81.09) | 2351 (77.77) | 8845 (80.18) | ||
| Drinking history | 42.7765 | <0.0001 | |||
| Yes | 3383 (42.25) | 1070 (35.40) | 4453 (40.37) | ||
| No | 4652 (57.75) | 1953 (64.60) | 6578 (59.63) | ||
| Variables | ASM [n (%)] | χ2 | p-Value | ||
|---|---|---|---|---|---|
| Yes | No | Total | |||
| Total | 3717 (33.70) | 7314 (66.30) | 11,031 (100.00) | ||
| Gender | 6.6819 | 0.0097 | |||
| Male | 1632 (43.91) | 3401 (46.50) | 5033 (45.63) | ||
| Female | 2085 (56.09) | 3913 (53.50) | 5998 (54.37) | ||
| Age (years) | 55.2949 | <0.0001 | |||
| 0–30 | 1423 (38.28) | 3242 (44.33) | 4665 (42.29) | ||
| 31–45 | 1020 (27.44) | 1981 (27.09) | 3001 (27.21) | ||
| 46–59 | 876 (23.57) | 1342 (18.35) | 2218 (20.11) | ||
| 60– | 398 (10.71) | 749 (10.24) | 1147 (10.40) | ||
| BMI (kg/m2) | 14.5356 | 0.0007 | |||
| <18.5 | 471 (12.67) | 1091 (14.92) | 1562 (14.16) | ||
| 18.5–24.9 | 2548 (68.55) | 4997 (68.32) | 7545 (68.40) | ||
| 25– | 698 (18.78) | 1226 (16.72) | 1924 (17.44) | ||
| Spouse | 34.7433 | <0.0001 | |||
| Yes | 2243 (60.34) | 3983 (54.46) | 6226 (56.44) | ||
| No | 1474 (39.66) | 3331 (45.54) | 4805 (43.56) | ||
| Education level | |||||
| Primary or below | 324 (8.72) | 803 (10.98) | 1127 (10.22) | 14.7739 | 0.0006 |
| Secondary | 1148 (30.89) | 2269 (31.02) | 3417 (30.98) | ||
| Higher | 2245 (60.40) | 4242 (58.00) | 6487 (58.81) | ||
| Occupation | 48.6309 | <0.0001 | |||
| Unemployed | 2156 (58.00) | 4719 (64.52) | 6875 (62.32) | ||
| Blue-collar | 455 (12.24) | 832 (11.38) | 1287 (11.67) | ||
| White-collar | 1106 (29.76) | 1763 (24.10) | 2869 (26.01) | ||
| Monthly household income per capita | 4.7330 | 0.0938 | |||
| 0–3000 | 1045 (28.11) | 2201 (30.09) | 3246 (29.43) | ||
| 3001–6000 | 1454 (39.12) | 2800 (38.28) | 4254 (38.56) | ||
| 6001– | 1218 (32.77) | 2313 (31.62) | 3531 (32.01) | ||
| Medical insurance | 60.5866 | <0.0001 | |||
| Resident/employee | 2931 (78.85) | 5358 (72.98) | 8289 (75.14) | ||
| Commercial | 95 (2.56) | 142 (1.94) | 237 (2.15) | ||
| Government-funded | 70 (1.88) | 136 (1.86) | 206 (1.87) | ||
| Out-of-pocket payment | 621 (16.71) | 1678 (22.94) | 2299 (20.84) | ||
| Number of chronic diseases | 65.5118 | <0.0001 | |||
| none | 2921 (78.58) | 6165 (84.29) | 9086 (82.37) | ||
| Single | 501 (13.48) | 800 (10.94) | 1301 (11.79) | ||
| Multiple | 295 (7.94) | 349 (4.77) | 644 (5.84) | ||
| Smoking history | 6.7482 | 0.0094 | |||
| Yes | 788 (21.20) | 1398 (18.99) | 2186 (19.82) | ||
| No | 2929 (78.80) | 5916 (80.89) | 8845 (80.18) | ||
| Drinking history | 19.8502 | <0.0001 | |||
| Yes | 1609 (43.29) | 2844 (38.88) | 4453 (40.37) | ||
| No | 2108 (56.71) | 4470 (61.12) | 6578 (59.63) | ||
| Residence | 11.0567 | 0.0009 | |||
| Urban | 2772 (74.58) | 5236 (71.59) | 8008 (72.60) | ||
| Rural | 945 (25.42) | 2078 (28.41) | 3023 (27.40) | ||
| Variables | n (%) | χ2 | p-Value | ||
|---|---|---|---|---|---|
| Urban | Rural | Total | |||
| Total | 2772 (74.58) | 945 (25.42) | 3717 (100.00) | ||
| Clinical factors | |||||
| 1 Drug efficacy | 1787 (64.47) | 600 (63.49) | 2387 (64.22) | 0.2910 | 0.5896 |
| 2 Drug safety | 1867 (67.35) | 627 (66.35) | 2494 (67.10) | 0.3211 | 0.5710 |
| 3 Dosage form (e.g., capsules, patches) | 609 (21.97) | 199 (21.06) | 808 (21.74) | 0.3442 | 0.5574 |
| Economic and accessibility | |||||
| 4 Drug price | 1036 (37.37) | 455 (48.15) | 1491 (40.11) | 34.0566 | <0.0001 |
| 5 Insurance reimbursement eligibility | 847 (30.56) | 292 (30.90) | 1139 (30.64) | 0.0392 | 0.8430 |
| Convenience and experience | |||||
| 6 Ease of administration | 581 (20.96) | 176 (18.62) | 757 (20.37) | 2.3697 | 0.1237 |
| 7 Taste of medication | 264 (9.52) | 78 (8.25) | 342 (9.20) | 1.3602 | 0.2435 |
| 8 Packaging aesthetics | 112 (4.04) | 34 (3.60) | 146 (3.93) | 0.3657 | 0.5453 |
| Social and personal advice | |||||
| 9 Physicians’ advice | 2181 (78.68) | 725 (76.72) | 2906 (78.18) | 1.5873 | 0.2077 |
| 10 Pharmacists’ advice | 1632 (58.87) | 551 (58.31) | 2183 (58.73) | 0.0937 | 0.7596 |
| 11 Family members’ suggestions | 1181 (42.60) | 421 (44.55) | 1602 (43.10) | 1.0879 | 0.2969 |
| 12 Friends’ suggestions | 753 (27.16) | 238 (25.19) | 991 (26.66) | 1.4120 | 0.2347 |
| 13 Recommendations from sales personnel | 732 (26.41) | 308 (32.59) | 1040 (27.98) | 13.3816 | 0.0003 |
| 14 Personal experience | 1502 (54.18) | 511 (54.07) | 2013 (54.16) | 0.0035 | 0.9530 |
| Brand and corporate | |||||
| 15 Brand reputation | 835 (30.12) | 205 (21.69) | 1040 (27.98) | 24.8509 | <0.0001 |
| 16 Corporate credibility | 620 (22.37) | 165 (17.46) | 785 (21.12) | 10.1830 | 0.0014 |
| 17 Advertising influence | 243 (8.77) | 83 (8.78) | 326 (8.77) | 0.0002 | 0.9874 |
| 18 After-sales service | 269 (9.70) | 120 (12.70) | 389 (10.47) | 6.7430 | 0.0094 |
| Variables | β | SE | Wald χ2 | p-Value | OR (95%CI) |
|---|---|---|---|---|---|
| Intercept | −0.2714 | 0.1474 | 3.3924 | 0.0655 | |
| Gender (Ref: Female) | |||||
| Male | −0.2619 | 0.0480 | 29.7837 | <0.0001 | 0.770 (0.700, 0.845) |
| Age (Ref: 60–) | |||||
| 0–30 | −0.0321 | 0.0953 | 0.1133 | 0.7364 | 0.968 (0.803, 1.167) |
| 31–45 | −0.0108 | 0.0857 | 0.0159 | 0.8997 | 0.989 (0.836, 1.170) |
| 46–59 | 0.1848 | 0.0841 | 4.8313 | 0.0279 | 1.203 (1.020, 1.418) |
| BMI (Ref: 25–) | |||||
| <18.5 | −0.1350 | 0.0771 | 3.0688 | 0.0798 | 0.874 (0.751, 1.016) |
| 18.5–24.9 | −0.0362 | 0.0553 | 0.4279 | 0.5130 | 0.964 (0.865, 1.075) |
| Spouse (Ref: No) | |||||
| Yes | 0.0408 | 0.0610 | 0.4482 | 0.5032 | 1.042 (0.924, 1.174) |
| Education level (Ref: Higher) | |||||
| Primary or below | −0.3759 | 0.0863 | 18.9833 | <0.0001 | 0.687 (0.580, 0.813) |
| Secondary | −0.0769 | 0.0509 | 2.2792 | 0.1311 | 0.926 (0.838, 1.023) |
| Occupation (Ref: White-collar) | |||||
| Unemployed | −0.1291 | 0.0559 | 5.3329 | 0.0209 | 0.879 (0.788, 0.981) |
| Blue-collar | −0.0905 | 0.0729 | 1.5406 | 0.2145 | 0.913 (0.792, 1.054) |
| Monthly household income per capita (Ref: 6001–) | |||||
| 0–3000 | 0.0330 | 0.0570 | 0.3365 | 0.5618 | 1.034 (0.924, 1.156) |
| 3001–6000 | 0.0203 | 0.0492 | 0.1707 | 0.6795 | 1.021 (0.927, 1.124) |
| Medical insurance (Ref: Out-of-pocket payment) | |||||
| Resident/employee | 0.2826 | 0.0552 | 26.2324 | <0.0001 | 1.327 (1.191, 1.478) |
| Commercial | 0.4848 | 0.1430 | 11.4930 | 0.0007 | 1.624 (1.227, 2.149) |
| Government-funded | 0.2163 | 0.1572 | 1.8926 | 0.1689 | 1.241 (0.912, 1.690) |
| Number of chronic diseases (Ref: Multiple) | |||||
| None | −0.5776 | 0.0913 | 39.9822 | <0.0001 | 0.561 (0.469, 0.671) |
| Single | −0.3353 | 0.0997 | 11.3167 | 0.0008 | 0.715 (0.588, 0.869) |
| Smoking history (Ref: No) | |||||
| Yes | 0.0849 | 0.0608 | 1.9542 | 0.1621 | 1.089 (0.966, 1.226) |
| Drinking history (Ref: No) | |||||
| Yes | 0.1830 | 0.0461 | 15.7526 | <0.0001 | 1.201 (1.097, 1.314) |
| Residence (Ref: Rural) | |||||
| Urban | 0.0454 | 0.0501 | 0.8211 | 0.3648 | 1.046 (0.949, 1.154) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huang, G.; Ge, P.; Sui, M.; Zhu, H.; Han, S.; Shi, L. Distribution and Determinants of Antibiotic Self-Medication: A Cross-Sectional Study in Chinese Residents. Antibiotics 2025, 14, 701. https://doi.org/10.3390/antibiotics14070701
Huang G, Ge P, Sui M, Zhu H, Han S, Shi L. Distribution and Determinants of Antibiotic Self-Medication: A Cross-Sectional Study in Chinese Residents. Antibiotics. 2025; 14(7):701. https://doi.org/10.3390/antibiotics14070701
Chicago/Turabian StyleHuang, Guo, Pu Ge, Mengyun Sui, He Zhu, Sheng Han, and Luwen Shi. 2025. "Distribution and Determinants of Antibiotic Self-Medication: A Cross-Sectional Study in Chinese Residents" Antibiotics 14, no. 7: 701. https://doi.org/10.3390/antibiotics14070701
APA StyleHuang, G., Ge, P., Sui, M., Zhu, H., Han, S., & Shi, L. (2025). Distribution and Determinants of Antibiotic Self-Medication: A Cross-Sectional Study in Chinese Residents. Antibiotics, 14(7), 701. https://doi.org/10.3390/antibiotics14070701