
Antibiotic Treatment vs. Non-Antibiotic Treatment in Bovine Clinical Mastitis During Lactation with Mild and Moderate Severity
 , , , , ,
, , , , , 
Abstract
1. Introduction
Objective
2. Results
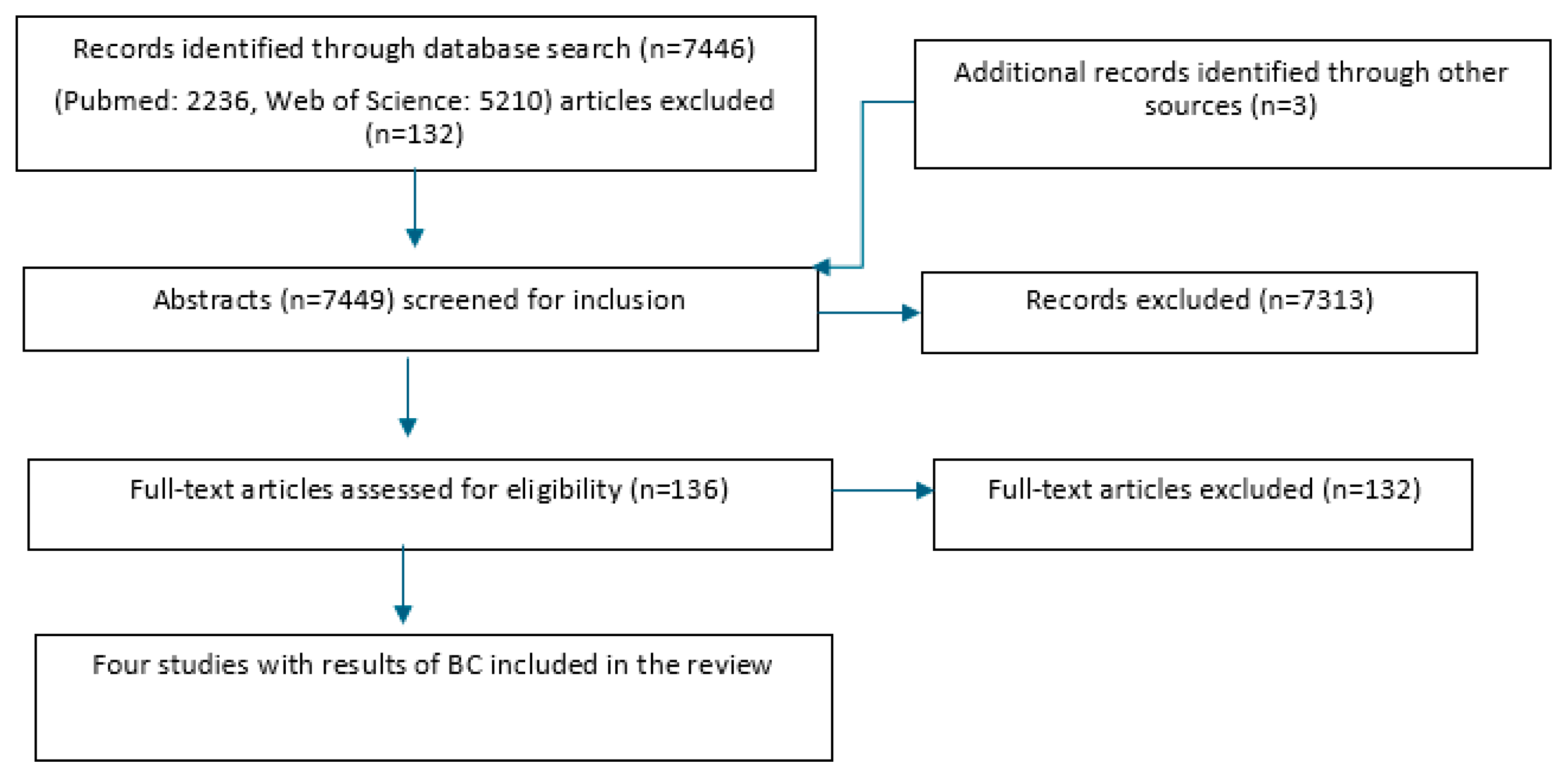
2.1. Study Selection
2.2. Description of the Included Studies
2.3. Risk-of-Bias Assessment
2.4. Descriptive Outcomes of Bacteriological Cure for Specific Pathogens
2.5. Deviation from the PRISMA Path: Exploring Relevant Research Beyond Initial Systematic Review Constraints
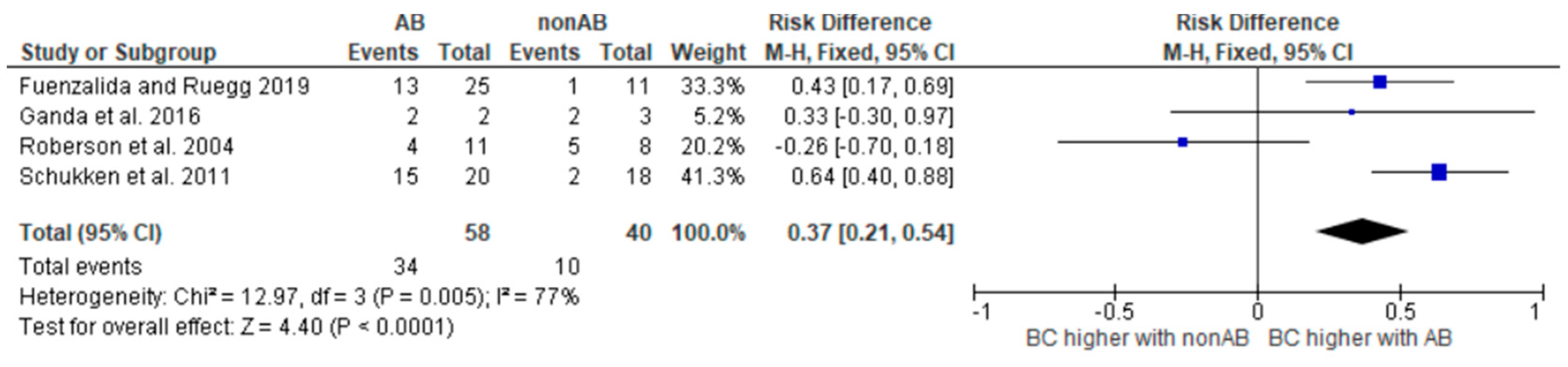
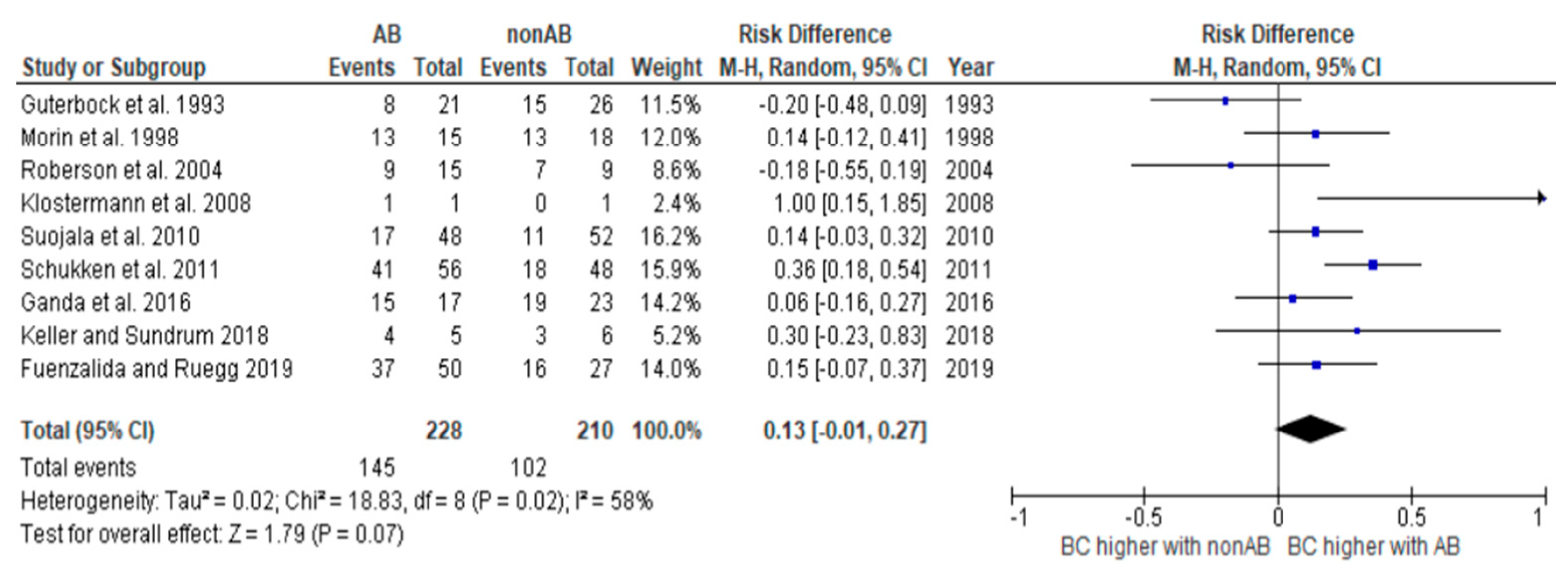
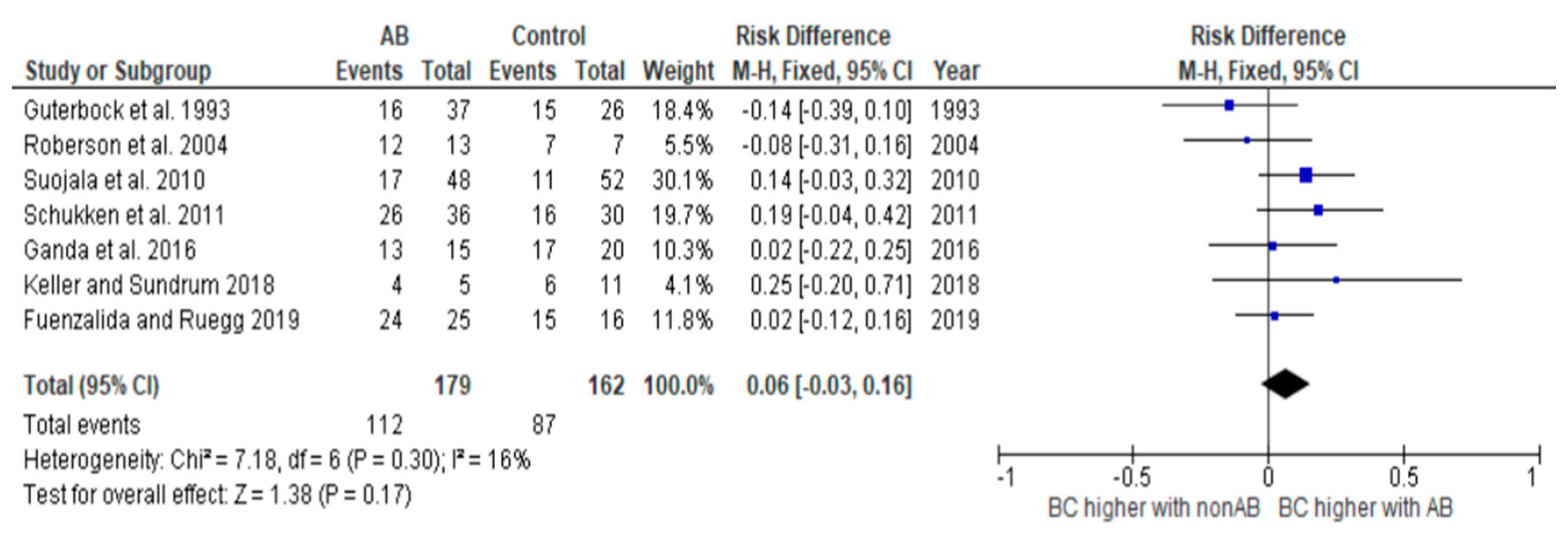
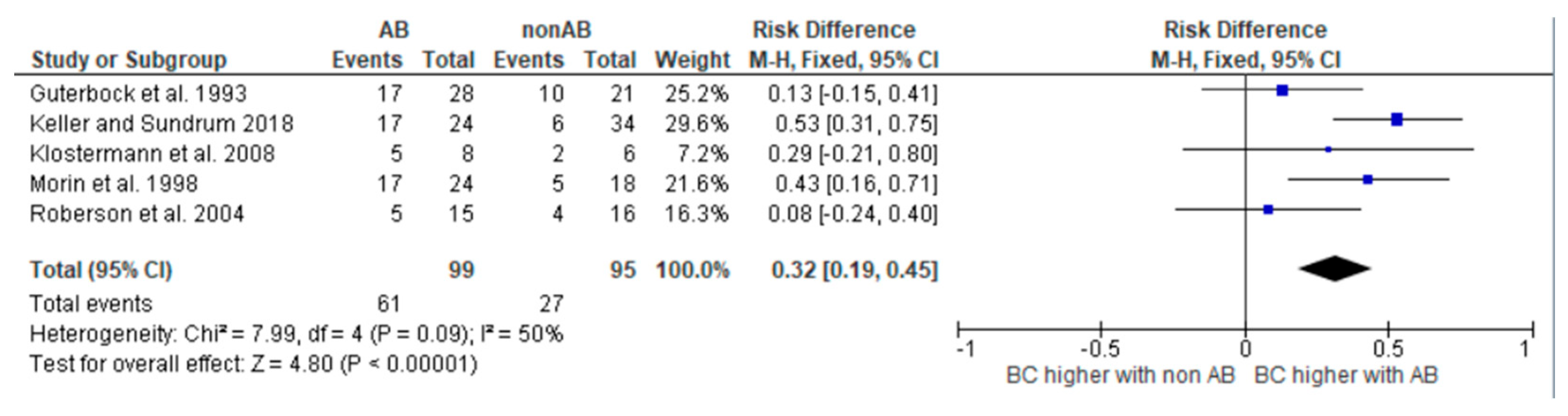
2.6. Risk Difference
3. Discussion
4. Materials and Methods
Search and Study Selection Process
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Van Werven, T. Managing Dairy Cows with Less Antibiotics! WCDS Adv. Dairy Technol. 2018, 30, 37–47. [Google Scholar]
- Krömker, V.; Leimbach, S. Mastitis treatment-Reduction in antibiotic usage in dairy cows. Reprod. Domest. Anim. 2017, 52 (Suppl. 3), 21–29. [Google Scholar] [CrossRef]
- Ruegg, P.L. Making Antibiotic Treatment Decisions for Clinical Mastitis. Vet. Clin. North Am: Food Anim. Pract. 2018, 34, 413–425. [Google Scholar] [CrossRef] [PubMed]
- de Jong, E.; Creytens, L.; De Vliegher, S.; McCubbin, K.D.; Baptiste, M.; Leung, A.A.; Speksnijder, D.; Dufour, S.; Middleton, J.R.; Ruegg, P.L.; et al. Selective treatment of nonsevere clinical mastitis does not adversely affect cure, somatic cell count, milk yield, recurrence, or culling: A systematic review and meta-analysis. J. Dairy Sci. 2023, 106, 1267–1286. [Google Scholar] [CrossRef] [PubMed]
- International Dairy Federation (IDF). Suggested Interpretation of Mastitis Terminology, 2nd ed.; Bulletin of the IDF 448; International Dairy Federation (IDF): Brussels, Belgium, 2011. [Google Scholar]
- Schmenger, A.; Krömker, V. Characterization, Cure Rates and Associated Risks of Clinical Mastitis in Northern Germany. Vet. Sci. 2020, 7, 170. [Google Scholar] [CrossRef]
- Krebs, I.; Zhang, Y.; Wente, N.; Leimbach, S.; Krömker, V. Bacteremia in Severe Mastitis of Dairy Cows. Microorganisms 2023, 11, 1639. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Roberson, J.R. Treatment of clinical mastitis. Vet. Clin. North Am. Food Anim. Pract. 2012, 28, 271–288. [Google Scholar] [CrossRef] [PubMed]
- Suojala, L.; Kaartinen, L.; Pyorala, S. Treatment for bovine Escherichia coli mastitis—an evidence-based approach. J. Vet. Pharmacol. Ther. 2013, 36, 521–531. [Google Scholar] [CrossRef]
- Petersson-Wolfe, C.S.; Leslie, K.E.; Swartz, T.H. An Update on the Effect of Clinical Mastitis on the Welfare of Dairy Cows and Potential Therapies. Vet. Clin. North Am. Food Anim. Pract. 2018, 34, 525–535. [Google Scholar] [CrossRef]
- Francoz, D.; Wellemans, V.; Dupre, J.P.; Roy, J.P.; Labelle, F.; Lacasse, P.; Dufour, S. Invited review: A systematic review and qualitative analysis of treatments other than conventional antimicrobials for clinical mastitis in dairy cows. J. Dairy Sci. 2017, 100, 7751–7770. [Google Scholar] [CrossRef]
- McDougall, S.; Abbeloos, E.; Piepers, S.; Rao, A.; Astiz, S.; van Werven, T.; Statham, J.; Pérez-Villalobos, N. Addition of meloxicam to the treatment of clinical mastitis improves subsequent reproductive performance. J. Dairy Sci. 2016, 99, 2026–2042. [Google Scholar] [CrossRef] [PubMed]
- Smulski, S.; Gehrke, M.; Libera, K.; Cieslak, A.; Huang, H.; Patra, A.K.; Szumacher-Strabel, M. Effects of various mastitis treatments on the reproductive performance of cows. BMC Vet. Res. 2020, 16, 99. [Google Scholar] [CrossRef]
- Ziesch, M.; Wente, N.; Zhang, Y.; Zaremba, W.; Engl, S.; Krömker, V. Noninferiority trial investigating the efficacy of a nonantibiotic intramammary therapy in the treatment of mild-to-moderate clinical mastitis in dairy cows with longer lasting udder diseases. J. Vet. Pharmacol. Ther. 2018, 41, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Krömker, V.; Schmenger, A.; Klocke, D.; Mansion-de Vries, E.M.; Wente, N.; Zhang, Y.; Leimbach, S. Non-inferiority Trial Investigating the Efficacy of Non-steroidal Anti-inflammatory Drugs and Antimicrobial Treatment of Mild to Moderate Clinical Mastitis in Dairy Cows With Long-lasting Udder Diseases. Front. Vet. Sci. 2021, 8, 660804. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Guterbock, W.M.; Van Eenennaam, A.L.; Anderson, R.J.; Gardner, I.A.; Cullor, J.S.; Holmberg, C.A. Efficacy of intramammary antibiotic therapy for treatment of clinical mastitis caused by environmental pathogens. J. Dairy Sci. 1993, 76, 3437–3444. [Google Scholar] [CrossRef]
- Schukken, Y.H.; Bennett, G.J.; Zurakowski, M.J.; Sharkey, H.L.; Rauch, B.J.; Thomas, M.J.; Ceglowski, B.; Saltman, R.L.; Belomestnykh, N.; Zadoks, R.N. Randomized clinical trial to evaluate the efficacy of a 5-day ceftiofur hydrochloride intra-mammary treatment on nonsevere gram-negative clinical mastitis. J. Dairy Sci. 2011, 94, 6203–6215. [Google Scholar] [CrossRef]
- Fuenzalida, M.J.; Ruegg, P.L. Negatively controlled, randomized clinical trial to evaluate intramammary treatment of nonsevere, gram-negative clinical mastitis. J. Dairy Sci. 2019, 102, 5438–5457. [Google Scholar] [CrossRef]
- Roberson, J.; Warnick, L.; Moore, G. Mild to moderate clinical mastitis: Efficacy of intramammary amoxicillin, frequent milk-out, a combined intramammary amoxicillin, and frequent milk-out treatment versus no treatment. J. Dairy Sci. 2004, 87, 583–592. [Google Scholar] [CrossRef]
- Keller, D.; Sundrum, A. Comparative effectiveness of individualised homeopathy and antibiotics in the treatment of bovine clinical mastitis: Randomised controlled trial. Vet. Rec. 2018, 182, 407. [Google Scholar] [CrossRef]
- Suojala, L.; Simojoki, H.; Mustonen, K.; Kaartinen, L.; Pyörälä, S. Efficacy of enrofloxacin in the treatment of naturally occurring acute clinical Escherichia coli mastitis. J. Dairy Sci. 2010, 93, 1960–1969. [Google Scholar] [CrossRef] [PubMed]
- Klostermann, K.; Crispie, F.; Flynn, J.; Ross, R.P.; Hill, C.; Meaney, W. Intramammary infusion of a live culture of Lactococcus lactis for treatment of bovine mastitis: Comparison with antibiotic treatment in field trials. J. Dairy Res. 2008, 75, 365–373. [Google Scholar] [CrossRef] [PubMed]
- Morin, D.E.; Shanks, R.D.; McCoy, G.C. Comparison of antibiotic administration in conjunction with supportive measures versus supportive measures alone for treatment of dairy cows with clinical mastitis. J. Am. Vet. Med Assoc. 1998, 213, 676–684. [Google Scholar] [CrossRef] [PubMed]
- Ganda, E.K.; Bisinotto, R.S.; Lima, S.F.; Kronauer, K.; Decter, D.H.; Oikonomou, G.; Schukken, Y.H.; Bicalho, R.C. Longitudinal metagenomic profiling of bovine milk to assess the impact of intramammary treatment using a third-generation cephalosporin. Sci. Rep. 2016, 6, 37565. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Schulz, K.F.; Chalmers, I.; Hayes, R.J.; Altman, D.G. Empirical evidence of bias. Dimensions of methodological quality associated with estimates of treatment effects in controlled trials. JAMA 1995, 273, 408–412. [Google Scholar] [CrossRef] [PubMed]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.M.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control. Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Pyörälä, S.; Kaartinen, L.; Käck, H.; Rainio, V. Efficacy of two therapy regimens for treatment of experimentally induced Escherichia coli mastitis in cows. J. Dairy Sci. 1994, 77, 453–461. [Google Scholar] [CrossRef] [PubMed]
- Günther, J.; Petzl, W.; Bauer, I.; Ponsuksili, S.; Zerbe, H.; Schuberth, H.-J.; Brunner, R.M.; Seyfert, H.-M. Differentiating Staphylococcus aureus from Escherichia coli mastitis: S. aureus triggers unbalanced immune-dampening and host cell invasion immediately after udder infection. Sci. Rep. 2017, 7, 4811. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Wenz, J.R.; Barrington, G.M.; Garry, F.B.; McSweeney, K.D.; Dinsmore, R.P.; Goodell, G.; Callan, R.J. Bacteremia associated with naturally occurring acute coliform mastitis in dairy cows. J. Am. Vet. Med Assoc. 2001, 219, 976–981. [Google Scholar] [CrossRef]
- Lago, A.; Godden, S.M.; Bey, R.; Ruegg, P.L.; Leslie, K. The selective treatment of clinical mastitis based on on-farm culture results: I. Effects on antibiotic use, milk withholding time, and short-term clinical and bacteriological outcomes. J. Dairy Sci. 2011, 94, 4441–4456. [Google Scholar] [CrossRef]
- Vasquez, A.K.; Nydam, D.V.; Capel, M.B.; Eicker, S.; Virkler, P.D. Clinical outcome comparison of immediate blanket treatment versus a delayed pathogen-based treatment protocol for clinical mastitis in a New York dairy herd. J. Dairy Sci. 2017, 100, 2992–3003. [Google Scholar] [CrossRef]
- Schmenger, A.; Leimbach, S.; Wente, N.; Zhang, Y.; Biggs, A.M.; Krömker, V. Implementation of a targeted mastitis therapy concept using an on-farm rapid test: Antimicrobial consumption cure rates and compliance. Vet. Rec. 2020, 187, 401. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Sargeant, J.M.; O’COnnor, A.M. Scoping Reviews, Systematic Reviews, and Meta-Analysis: Applications in Veterinary Medi-cine. Front. Vet. Sci. 2020, 7, 11. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (updated February 2021). Cochrane, 2021. Available online: www.training.cochrane.org/handbook (accessed on 1 January 2022).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | Demographics | Method for Identification of Mastitis Agents | BC 1: Time of Measurement | Further Evaluated Outcomes |
|---|---|---|---|---|
| Guterbock et al., 1993 [16] | 3 California dairy herds Total: n = 254 quarters ABT 2-a 3: n 4 = 74 ABT-b 5: n = 75 NABT 6 n = 105 | Cult 7 | Day 5 (milking 9, ABT a) or day 6 (milking 11, ABT b) and day 21 after initial treatment | CC 8 |
| Roberson et al., 2004 [19] | 1 university dairy herd Total: n = 82 cow mastitis events ABT-a: n = 21 ABT-b: n = 19 NABT (c): n = 20 NC 9 (d): n = 22 | Cult | Days 7 and 36 | CC, milk production, disease progression, CMT 10 scores |
| Schukken et al., 2011 [17] | 5 dairy farms in New York State Total: n = 104 cases ABT: n = 56 NC= n = 48 | Cult & Mol 11 (at enrollment: identification of coliform pathogens mostly via on-farm culture; confirmation in laboratory) | Days 7 ± 2 and 14 ± 2 | Clinical improvement, milk production, linear score, survival probability |
| Fuenzalida and Ruegg, 2019 [18] | 2 commercial Wisconsin dairy herds Total: n = 168 cases ABT-a: n = 56 ABT-b: n = 56 NC: n = 56 | Cult (at enrollment: identification of Gram-negative pathogens via on-farm culture; confirmation in laboratory) | Days 14 and 21 | Quarter-level CM 12 recurrence, cc, culling within 21 days after enrollment, voluntary dry-off of an affected quarter, days until cc, days of milk discard, days to BC, days to culling, voluntary quarter dry-off, daily milk production |
| Study | Intervention | Comparator |
|---|---|---|
| Guterbock et al., 1993 [16] | ABT 1-a 2: IMM 3 amoxicillin (62.5 mg, every 12 h, 3 times ABT-b 6: IMM cephapirin (200 mg, every 12 h, 2 times) | Oxytocin IM 4 (100IU 5, every 12 h, 2 or 3 milkings) (=NABT 7) |
| Roberson et al., 2004 [19] | IMM amoxicillin (62.5 mg, every 12 h, 3 times) | Frequent milk-out (+20IU Oxytocin) (=NABT) No treatment (=NC 8) |
| Schukken et al., 2011 [17] | IMM ceftiofur hydrochloride (125 mg in 10 mL, 5 days, every 24 h) | No treatment (=NC) |
| Fuenzalida and Ruegg, 2019 [18] | ABT-a: IMM ceftiofur hydrochloride (125 mg, 2 days, every 24 h) ABT-b: IMM ceftiofur hydrochloride (125 mg, 8 days, every 24 h) | No treatment (=NC) |
| Study | Domain 1 | Domain 2 | Domain 3 | Domain 4 | Domain 5 | Total |
|---|---|---|---|---|---|---|
| Guterbock et al. (1993) [16] | ! | + | + | ! | + | ! |
| Roberson et al. (2004) [19] | + | + | + | + | + | + |
| Schukken et al. (2011) [17] | + | + | + | + | + | + |
| Fuenzalida and Ruegg (2019) [18] | + | + | + | + | + | + |
| Bacterial Group/Species | BC 1 Results ABT 2-a 3 (n 4/n, %) | BC Results ABT-b 5 (n/n, %) | Total Results of ABT | BC Results Comparator NC 6 (n/n, %) | BC Results Comparator NABT 7 (n/n, %) | Total Results of Comparators | Study |
|---|---|---|---|---|---|---|---|
| Streptococci | 6/13 (46.2) | 11/15 (73.3) | 17/28 (60.7) | 10/21 (47.6) | 10/21 (47.6) | Guterbock et al., 1993 [16] | |
| 3/4 (75) | 3/4 (75) | 2/7 (29) | 2/9 (22) | 4/16 (25) | Roberson et al., 2004 [19] | ||
| E. coli | (100.0) | (92.9) | (93.7) | Fuenzalida and Ruegg, 2019 [18] | |||
| (89.0) | (53.0) | Schukken et al., 2011 [17] | |||||
| 8/9 (89) | 8/9 (89) | 4/4 (100) | 3/3 (100) | 7/7 (100) | Roberson et al., 2004 [19] | ||
| Coliforms | 8/21 (38.1) | 8/16 (50.0) | 16/37 (43.2) | 15/26 (57.7) | 15/26 (57.7) | Guterbock et al., 1993 [16] | |
| Klebsiella pneumoniae | (42.9) | (63.6) | (9.1) | Fuenzalida and Ruegg, 2019 [18] | |||
| Klebsiella spp. | (57.0) | (19.0) | Schukken et al., 2011 [17] | ||||
| 2/7 (29) | 2/7 (29) | 3/5 (60) | 2/3 (67) | 5/8 (62.5) | Roberson et al., 2004 [19] |
| Study | Demographics | BC 1: Time of Measurement | Intervention | Comparator | Deviation from the Initial Criteria |
|---|---|---|---|---|---|
| Morin et al., 1998 [23] | 1 university dairy herd in Illinois Total: 172 clinical mastitis cases in 124 cows ABT 2: 90 NC 3: 82 | Day 14 | SevSc 4 1: 200 mg of cephapirin sodium IMM 5 SevSc 2: like SC1, additional oxytetracycline (16.5 mg/kg IV 6, q 24 h) SecSc 3: oxytetracycline (16.5 mg/kg IV 24 h) All SecSc´s: additional supportive treatment as the respective control group | SevSc 1: complete milk out by administering oxytocin (20U, IV or IM 7) (=NABT 8) SevSc 2: like SC 1, with an additional stripping at 12 pm SevSc 3: stripping every 3 h, additional flunixine meglumine (1.1 mg/kg q 8 h) and fluids (in case of dehydration) | Proportion of severe cases: Antibiotic treatment group: 19 (21%) Control group: 20 (24%) |
| Klostermann et al., 2008 [22] | 4 adjacent herds in Ireland Total: n = 50 quarters in 48 cows ABT: 25 quarters NABT: 25 quarters | Day 14 | 150 mg penethamate hydriodide, 150 mg dihydrostreptomycin (as sulphate), 50 mg framycetin sulphate and 5 mg prednisolone; infused at 24-h intervals on days 1, 2 and 3 | lacticin 3147, on days 1, 2 and 3 with 24-h intervals (=NABT) | Proportion of severe cases: Antibiotic treatment group: 10/18 Control group: 10/17 |
| Suojala et al., 2010 [21] | 61 typical Finnish dairy herds Total: 132 cows ABT: 64 cows NC: 68 cows | Days 2 and 21 | enroflocaxin (5 mg/kg), 2 d, every 24 h, first dose IV, second dose SC 9; additional ketoprofen IV or IM (3 mg/kg) or 4 mg/kg per os daily for 1 to 3 days | Ketoprofen (3 mg/kg IM or 4 mg/kg per os daily for 1 to 3 days) (=NABT) | Proportion of severe cases: 80.1% (n = 105) of the cows had moderate to severe signs 19.9% (n = 26) had mild signs |
| Ganda et al., 2016 [24] | 1 dairy herd in New York Total: 80 cows ABT: 40 cows NC: 40 cows | Days 10 and 14 | ceftiofur (125 mg) IMM, 5 days | No treatment (=NC) | it is not apparent how many cases were mild, moderate, or severe, and this was not included in the statistical analysis |
| Keller and Sundrum, 2017 [20] |
4 German dairy herds (1 organic, 3 conventional) Total: n = 180 dairy cows n = 60 for each treatment group | Days 7, 14 and 28 | Veterinarian’s decision: Synulox LC Plus, Cloxamycin L, Oxacillin-Na 1000 mg-Euter-Injektor, Vetriclox L, Peracef, Ubrolexin, Procain-Penicillin-G Injector or Wedeclox Mastitis | homeopathic treatment (21 remedies, 10 globules per day, 5 days) placebo treatment (Globuli Sacchari HAB Gr. 3, 10 globules per day, 5 days) | Determining BC at day 7 |
| Bacterial Group/Species | BC 1 Results ABT 2-a 3 (n/n, %) | BC Results ABT-b 4 (n/n, %) | Total Results of ABT | BC Results Comparator NC 5 (n/n, %) | BC Results Comparator NABT 6 (n/n, %) | Total Results of Comparators | Study |
|---|---|---|---|---|---|---|---|
| S. uberis | 11/17 (64.7) | 11/17 (64.7) | 3/16 (18.7) | 1/12 (8.3) | 4/28 (14.3) | Keller and Sundrum, 2017 [20] | |
| 3/3 (100.0) | 3/3 (100.0) | 0/1 (0.0) | 0/1 (0.0) | Klostermann et al., 2008 [22] | |||
| S. dysgalactiae | 6/7 (85.7) | 6/7 (85.7) | 2/3 (66.7) | 0/3 (0.0) | 2/6 (33.3) | Keller and Sundrum, 2017 [20] | |
| 2/5 (40.0) | 2/5 (40.0) | 2/5 (40.0) | 2/5 (40.0) | Klostermann et al., 2008 [22] | |||
| Streptococci | 6/13 (46.2) | 11/15 (73.3) | 17/28 (60.7) | 10/21 (47.6) | 10/21 (47.6) | Guterbock et al., 1993 [16] | |
| 3/4 (75) | 3/4 (75) | 2/7 (29) | 2/9 (22) | 4/16 (25) | Roberson et al., 2004 [19] | ||
| 17/24 (71) | 17/24 (71) | 5/18 (28) | 5/18 (28) | Morin et al., 1998 [23] | |||
| E. coli | 4/5 (80.0) | 4/5 (80.0) | 3/5 (60.0) | 3/6 (50.0) | 6/11 (54.5) | Keller and Sundrum, 2017 [20] | |
| (100.0) | (92.9) | (93.7) | Fuenzalida and Ruegg, 2019 [18] | ||||
| (89.0) | (53.0) | Schukken et al., 2011 [17] | |||||
| 8/9 (89) | 8/9 (89) | 4/4 (100) | 3/3 (100) | 7/7 (100) | Roberson et al., 2004 [19] | ||
| 1/1 (100.0) | 1/1 (100.0) | 0/1 (0.0) | 0/1 (0.0) | Klostermann et al., 2008 [22] | |||
| 16/20(80.0) | 16/20 (80.0) | 17/20 (85.0) | 17/20 (85.0) | Ganda et al., 2016 [24] | |||
| 38/42 (90.5) | 38/42 (90.5) | 33/38 (86.8) | 33/38 (86.8) | Suojala et al., 2010 [21] | |||
| Coliforms | 8/21 (38.1) | 8/16 (50.0) | 16/37 (43.2) | 15/26 (57.7) | 15/26 (57.7) | Guterbock et al., 1993 [16] | |
| 13/15 (87) | 13/15 (87) | 13/18 (72) | 13/18 (72) | Morin et al., 1998 [23] | |||
| Klebsiella pneumoniae | (42.9) | (63.6) | (9.1) | Fuenzalida and Ruegg, 2019 [18] | |||
| Klebsiella spp. | (57.0) | (19.0) | Schukken et al., 2011 [17] | ||||
| 2/7 (29) | 2/7 (29) | 3/5 (60) | 2/3 (67) | 5/8 (62.5) | Roberson et al., 2004 [19] | ||
| 2/2 (100.0) | 2/2 (100.0) | 2/3 (66.7) | 2/3 (66.7) | Ganda et al., 2016 [24] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nankemann, F.; Leimbach, S.; Nitz, J.; Tellen, A.; Wente, N.; Zhang, Y.; Klocke, D.; Krebs, I.; Müller, S.; Teich, S.; et al. Antibiotic Treatment vs. Non-Antibiotic Treatment in Bovine Clinical Mastitis During Lactation with Mild and Moderate Severity. Antibiotics 2025, 14, 702. https://doi.org/10.3390/antibiotics14070702
Nankemann F, Leimbach S, Nitz J, Tellen A, Wente N, Zhang Y, Klocke D, Krebs I, Müller S, Teich S, et al. Antibiotic Treatment vs. Non-Antibiotic Treatment in Bovine Clinical Mastitis During Lactation with Mild and Moderate Severity. Antibiotics. 2025; 14(7):702. https://doi.org/10.3390/antibiotics14070702
Chicago/Turabian StyleNankemann, Franziska, Stefanie Leimbach, Julia Nitz, Anne Tellen, Nicole Wente, Yanchao Zhang, Doris Klocke, Isabel Krebs, Stephanie Müller, Sabrina Teich, and et al. 2025. "Antibiotic Treatment vs. Non-Antibiotic Treatment in Bovine Clinical Mastitis During Lactation with Mild and Moderate Severity" Antibiotics 14, no. 7: 702. https://doi.org/10.3390/antibiotics14070702
APA StyleNankemann, F., Leimbach, S., Nitz, J., Tellen, A., Wente, N., Zhang, Y., Klocke, D., Krebs, I., Müller, S., Teich, S., Wilm, J., Katthöfer, P., Kortstegge, J., & Krömker, V. (2025). Antibiotic Treatment vs. Non-Antibiotic Treatment in Bovine Clinical Mastitis During Lactation with Mild and Moderate Severity. Antibiotics, 14(7), 702. https://doi.org/10.3390/antibiotics14070702