
Attitudes, Beliefs, and Behaviors of Topical Antibiotic Prescribing among Primary Care Providers in Saudi Arabia: A Cross-Sectional Study

 , , and
, , and
Abstract
1. Introduction
2. Methods
2.1. Setting, Design, and Population Sampling
2.2. Sample Size
2.3. Questionnaire
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. WHO Report on Surveillance of Antibiotic Consumption: 2016–2018 Early Implementation. World Health Organization. License: CC BY-NC-SA 3.0 IGO. 2018. Available online: https://apps.who.int/iris/handle/10665/277359 (accessed on 2 July 2023).
- Atif, M.; Sarwar, M.R.; Azeem, M.; Naz, M.; Amir, S.; Nazir, K. Assessment of core drug use indicators using WHO/INRUD methodology at primary healthcare centers in Bahawalpur, Pakistan. BMC Health Serv. Res. 2016, 16, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Llor, C.; Bjerrum, L. Antimicrobial resistance: Risk associated with antibiotic overuse and initiatives to reduce the problem. Ther. Adv. Drug Saf. 2014, 5, 229–241. [Google Scholar] [CrossRef] [PubMed]
- Infectious Diseases Society of America (IDSA); Spellberg, B.; Blaser, M.; Guidos, R.J.; Boucher, H.W.; Bradley, J.S.; Eisenstein, B.I.; Gerding, D.; Lynfield, R.; Reller, L.B.; et al. Combating antimicrobial resistance: Policy recommendations to save lives. Clin. Infect. Dis. 2011, 52 (Suppl. S5), S397–S428. [Google Scholar] [CrossRef] [PubMed]
- Del Rosso, J.; Zeichner, J.; Alexis, A.; Cohen, D.; Berson, D. Understanding the Epidermal Barrier in Healthy and Compromised Skin: Clinically Relevant Information for the Dermatology Practitioner: Proceedings of an Expert Panel Roundtable Meeting. J. Clin. Aesthet. Dermatol. 2016, 9, S2–S8. [Google Scholar]
- Bandyopadhyay, D. Topical antibacterials in dermatology. Indian J. Dermatol. 2021, 66, 117–125. [Google Scholar] [CrossRef] [PubMed]
- Aly, R. Microbial Infections of Skin and Nails. In Medical Microbiology, 4th ed; Baron, S., Ed.; University of Texas Medical Branch at Galveston: Galveston, TX, USA, 1996. [Google Scholar]
- Lin, H.-S.; Lin, P.-T.; Tsai, Y.-S.; Wang, S.-H.; Chi, C.-C. Interventions for bacterial folliculitis and boils (furuncles and carbuncles). Emergencias 2018, 2018, CD013099. [Google Scholar] [CrossRef]
- Heal, C.F.; Banks, J.L.; Lepper, P.D.; Kontopantelis, E.; van Driel, M.L. Topical antibiotics for preventing surgical site infection in wounds healing by primary intention. Emergencias 2016, 2016, CD011426. [Google Scholar] [CrossRef]
- Sule, O.; Brown, N.M.; Willocks, L.J.; Day, J.; Shankar, S.; Palmer, C.R.; Burrows, N.P. Fusidic acid-resistant Staphylococcus aureus (FRSA) carriage in patients with atopic eczema and pattern of prior topical fusidic acid use. Int. J. Antimicrob. Agents 2007, 30, 78–82. [Google Scholar] [CrossRef] [PubMed]
- Lapolla, W.J.; Levender, M.M.; Davis, S.A.; Yentzer, B.A.; Williford, P.M.; Feldman, S.R. Topical Antibiotic Trends from 1993 to 2007: Use of Topical Antibiotics for Non-Evidence-Based Indications. Dermatol. Surg. 2011, 37, 1427–1433. [Google Scholar] [CrossRef] [PubMed]
- Lyimo, S.R.; Sigalla, G.N.; Emidi, B.; Mgabo, M.R.; Kajeguka, D.C. Cross-sectional Survey on Antibiotic Prescription Practices Among Health Care Providers in Rombo District, Northern Tanzania. East Afr. Health Res. J. 2018, 2, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Nahar, P.; Unicomb, L.; Lucas, P.J.; Uddin, M.R.; Islam, M.A.; Alam Nizame, F.; Khisa, N.; Akter, S.M.S.; Rousham, E.K. What contributes to inappropriate antibiotic dispensing among qualified and unqualified healthcare providers in Bangladesh? A qualitative study. BMC Health Serv. Res. 2020, 20, 656. [Google Scholar] [CrossRef] [PubMed]
- George, S.; Muhaj, F.F.; Nguyen, C.D.; Tyring, S.K. Part I Antimicrobial resistance: Bacterial pathogens of dermatologic significance and implications of rising resistance. J. Am. Acad. Dermatol. 2022, 86, 1189–1204. [Google Scholar] [CrossRef] [PubMed]
- Glasser, J.S.; Guymon, C.H.; Mende, K.; Wolf, S.E.; Hospenthal, D.R.; Murray, C.K. Activity of topical antimicrobial agents against multidrug-resistant bacteria recovered from burn patients. Burns 2010, 36, 1172–1184. [Google Scholar] [CrossRef] [PubMed]
- Cutler, T.S.; Jannat-Khah, D.P.; Kam, B.; Mages, K.C.; Evans, A.T. Prevalence of misdiagnosis of cellulitis: A systematic review and meta-analysis. J. Hosp. Med. 2023, 18, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Onsoi, W.; Chaiyarit, J.; Techasatian, L. Common misdiagnoses and prevalence of dermatological disorders at a pediatric tertiary care center. J. Int. Med. Res. 2020, 48, 0300060519873490. [Google Scholar] [CrossRef] [PubMed]
- Hughey, L.C. The impact dermatologists can have on misdiagnosis of cellulitis and overuse of antibiotics: Closing the gap. JAMA Dermatol. 2014, 150, 1061–1062. [Google Scholar] [CrossRef] [PubMed]
- Pariser, R.J.; Pariser, D.M. Primary care physicians’ errors in handling cutaneous disorders: A prospective survey. J. Am. Acad. Dermatol. 1987, 17, 239–245. [Google Scholar] [CrossRef] [PubMed]
- Hjorth, N.; Schmidt, H.; Thomsen, K. Fusidic acid plus betamethasone in infected or potentially infected eczema. Pharmatherapeutica 1985, 4, 126–131. [Google Scholar] [PubMed]
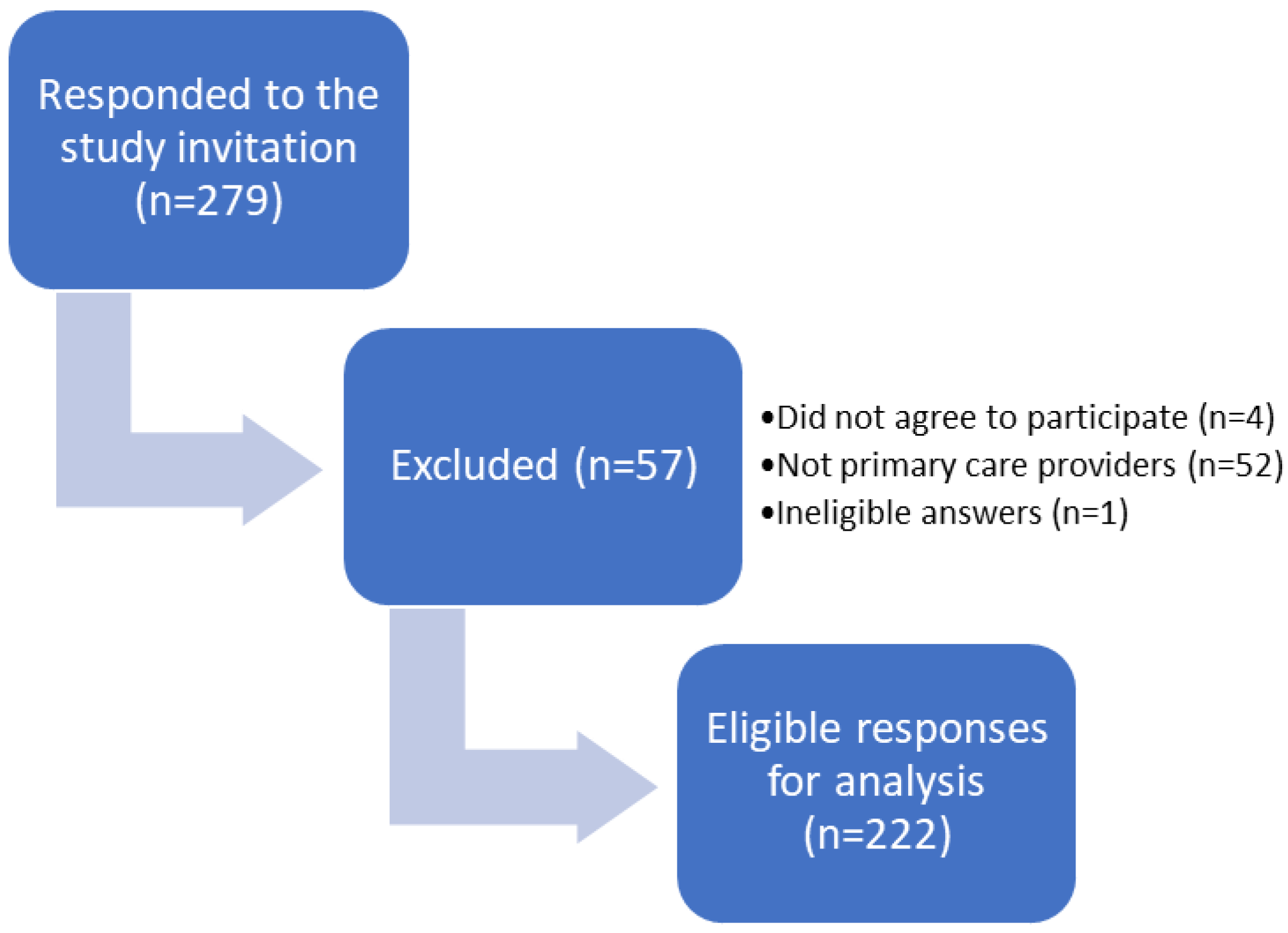

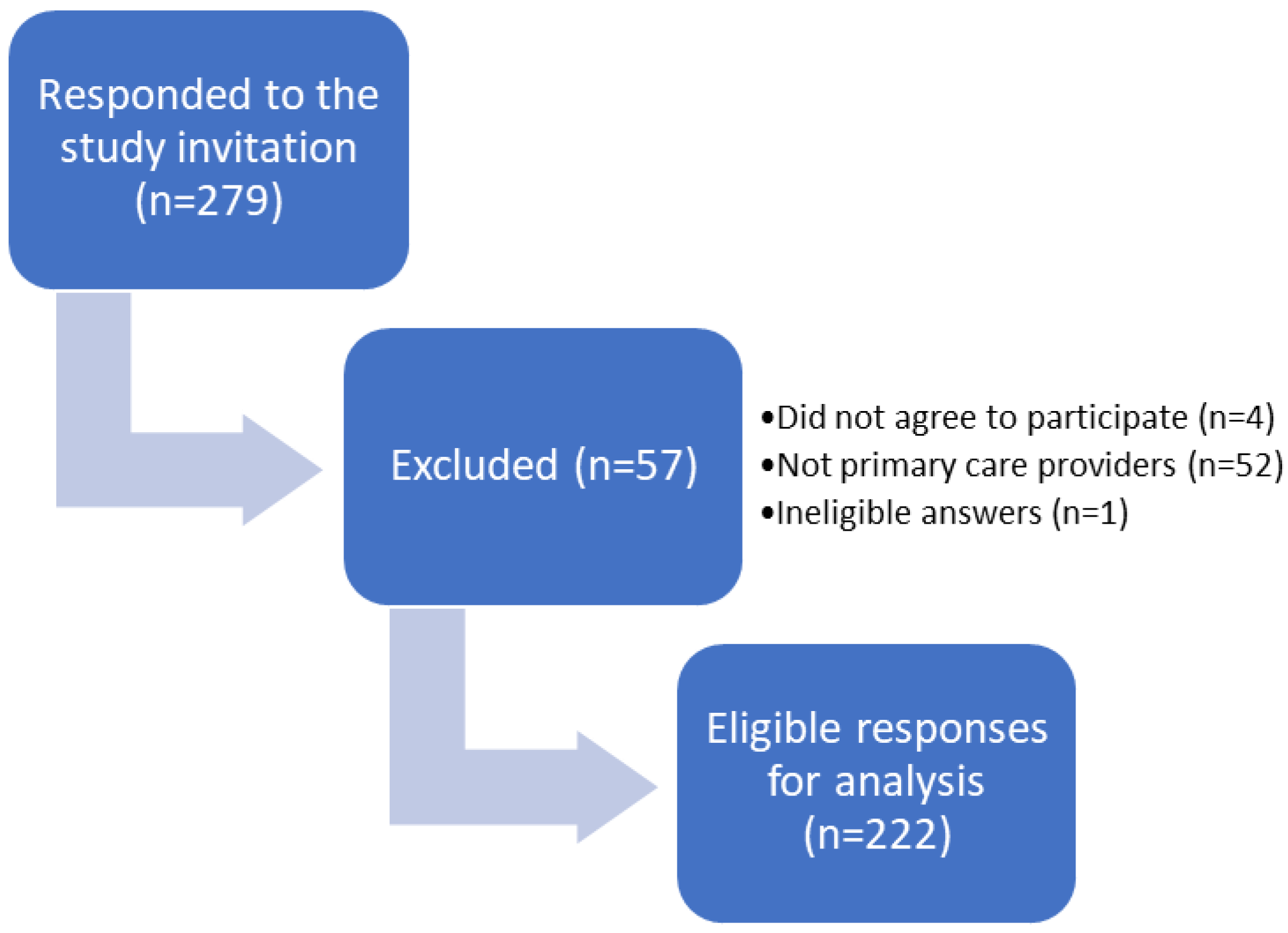{kind=link}
| Value | Variable |
|---|---|
| Gender, n (%) | |
| 89 (41) | Male |
| 130 (59) | Female |
| 36.8 (10.31) | Age, mean (SD) |
| Geographical region, n (%) | |
| 74 (33) | Eastern region |
| 49 (22) | Western region |
| 17 (8) | Central region |
| 37 (17) | Northern region |
| 45 (20) | Southern region |
| Specialty, n (%) | |
| 84 (38) | Non-specialist |
| 107 (48) | Family medicine |
| 31 (14) | Internal medicine |
| Professional title, n (%) | |
| 79 (36) | General practitioner |
| 67 (30) | Resident |
| 60 (27) | Specialist |
| 16 (7) | Consultant |
| Primary care site, n (%) | |
| 160 (68) | Ministry of Health hospitals |
| 14 (6) | National Guard hospitals |
| 17 (7) | Ministry of Defense hospitals |
| 3 (1) | Security Forces hospitals |
| 34 (14) | University hospitals |
| 5 (2) | King Faisal Specialist Hospital and Research Center |
| 4 (2) | Private hospital |
| Years of experience, n (%) | |
| 87 (39) | 0–4 years |
| 52 (23) | 5–9 years |
| 33 (15) | 10–14 years |
| 24 (11) | 15–19 years |
| 26 (12) | >20 years |
| Availability of a local antibiogram, n (%) | |
| 53 (24) | Yes |
| 127 (57) | No |
| 42 (19) | I don’t know |
| MRSA prevalence among antibiogram-available facilities, n (%) | |
| 13 (25) | Less than 10% |
| 16 (30) | Between 10 and 20% |
| 4 (8) | More than 20% |
| 20 (38) | Unavailable in my site |
| Availability of local antibiotic prescribing guidelines, n (%) | |
| 126 (57) | Yes |
| 65 (29) | No |
| 31 (14) | I don’t know |
| Accessibility of guidelines, n (%) | |
| 105 (83) | Easily accessible |
| 21 (17) | Difficult |
| Parameter | Value, n (%) | ||
|---|---|---|---|
| Yes | No | I Don’t Know | |
| Does inappropriate prescribing of topical antibiotics put patients at risk? | 163 (73) | 43 (19) | 16 (7) |
| Is it always better to over-prescribe topical antibiotics than to under-prescribe? | 43 (19) | 155 (70) | 24 (11) |
| Should everyone be able to buy topical antibiotics without a prescription? | 32 (14) | 163 (73) | 27 (12) |
| Is topical antibiotic resistance an issue in your daily practice? | 96 (43) | 84 (38) | 42 (19) |
| Is topical antibiotic resistance a significant issue in your healthcare facility? | 79 (36) | 93 (42) | 50 (23) |
| Parameter | n (%) |
|---|---|
| Which of these factors may influence your decision to start topical antibiotic therapy? * | |
| Patient’s clinical condition | 147 (66.2) |
| Patient’s preference | 44 (19.8) |
| I was trained to prescribe topical antibiotics | 44 (19.8) |
| Positive microbiological results in symptomatic patients | 103 (46.4) |
| Wanting to satisfy the senior treating physician | 21 (9.5) |
| Worry of missing patients with possible infections | 46 (20.7) |
| Do you ever try to ensure that your topical antibiotic prescribing is cost-effective? | |
| Yes | 123 (55) |
| No | 69 (31) |
| I don’t know | 30 (14) |
| Which of these do you think are important causes of prescribers’ inappropriate use of topical antibiotics? * | |
| Un-updated knowledge | 147 (66.2) |
| Unrestricted availability of antibiotics | 72 (32.4) |
| Inadequate supervision | 100 (45) |
| Lack of interest in the subject of antibiotic prescribing and infection management | 68 (30.6) |
| Strained healthcare personnel | 44 (19.8) |
| Which of the following do you think may help minimize topical antibiotic resistance? * | |
| Treating infection, not contamination or colonization | 82 (36.9) |
| Physician education on appropriate antibiotic therapy | 146 (65.8) |
| Consulting with infectious diseases experts | 88 (39.6) |
| Providing local antibiotic guidelines | 128 (57.6) |
| Knowledge of pathogens and antibiotic susceptibility test results | 112 (50.5) |
| Restrict topical antibiotic use | 61 (27.5) |
| Have you received regular training and education in antibiotic prescribing in your workplace? | |
| Yes | 106 (47.7) |
| No | 116 (52.3) |
| Do you follow the recommendations of your healthcare facility guidelines on topical antibiotic prescribing? | |
| Yes | 119 (94) |
| No | 7 (6) |
| Indications | Topical Antibiotic (Brand Name) | |
|---|---|---|
| Inappropriate | Appropriate | |
| N (%) | N (%) | |
| 225 (65.4) | 119 (34.5) | Metronidazole (Rozex 0.75% cream) |
| 220 (66) | 114 (34) | Clindamycin (Avocin cream) |
| 215 (68) | 103 (32) | Silver sulfadiazine (Flamazine cream 1%) |
| 282 (84.4) | 52 (15.5) | Neomycin (Betnovate-N 0.1% cream) |
| 180 (56.6) | 138 (43.4) | Mupirocin (Avoban cream) |
| 331 (85) | 58 (15) | Fusidic acid and betamethasone (Fucicort) |
| 118 (44) | 151 (56) | Benzoyl peroxide (Benzac AC gel) |
| 117 (28.3) | 297 (71.7) | Fusidic acid 5% (Fucidin cream or ointment) |
| 283 (78) | 81 (22) | Fusidic acid and hydrocortisone (Fucidin H) |
| 152 (42.8) | 203 (57.1) | Neomycin and bacitracin (Baneocin) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
AlBeladi, B.A.; Alhubail, S.A.; Alsaqer, R.A.; Al-Nasser, A.N.; Radwan, A.S.; Wali, H.A. Attitudes, Beliefs, and Behaviors of Topical Antibiotic Prescribing among Primary Care Providers in Saudi Arabia: A Cross-Sectional Study. Antibiotics 2024, 13, 301. https://doi.org/10.3390/antibiotics13040301
AlBeladi BA, Alhubail SA, Alsaqer RA, Al-Nasser AN, Radwan AS, Wali HA. Attitudes, Beliefs, and Behaviors of Topical Antibiotic Prescribing among Primary Care Providers in Saudi Arabia: A Cross-Sectional Study. Antibiotics. 2024; 13(4):301. https://doi.org/10.3390/antibiotics13040301
Chicago/Turabian StyleAlBeladi, Baneen A., Sara A. Alhubail, Riam A. Alsaqer, Ali N. Al-Nasser, Amira S. Radwan, and Haytham A. Wali. 2024. "Attitudes, Beliefs, and Behaviors of Topical Antibiotic Prescribing among Primary Care Providers in Saudi Arabia: A Cross-Sectional Study" Antibiotics 13, no. 4: 301. https://doi.org/10.3390/antibiotics13040301
APA StyleAlBeladi, B. A., Alhubail, S. A., Alsaqer, R. A., Al-Nasser, A. N., Radwan, A. S., & Wali, H. A. (2024). Attitudes, Beliefs, and Behaviors of Topical Antibiotic Prescribing among Primary Care Providers in Saudi Arabia: A Cross-Sectional Study. Antibiotics, 13(4), 301. https://doi.org/10.3390/antibiotics13040301