
Early-Outcome Differences between Acute and Chronic Periprosthetic Joint Infections—A Retrospective Single-Center Study
 , ,
, ,
Abstract
1. Introduction
2. Results
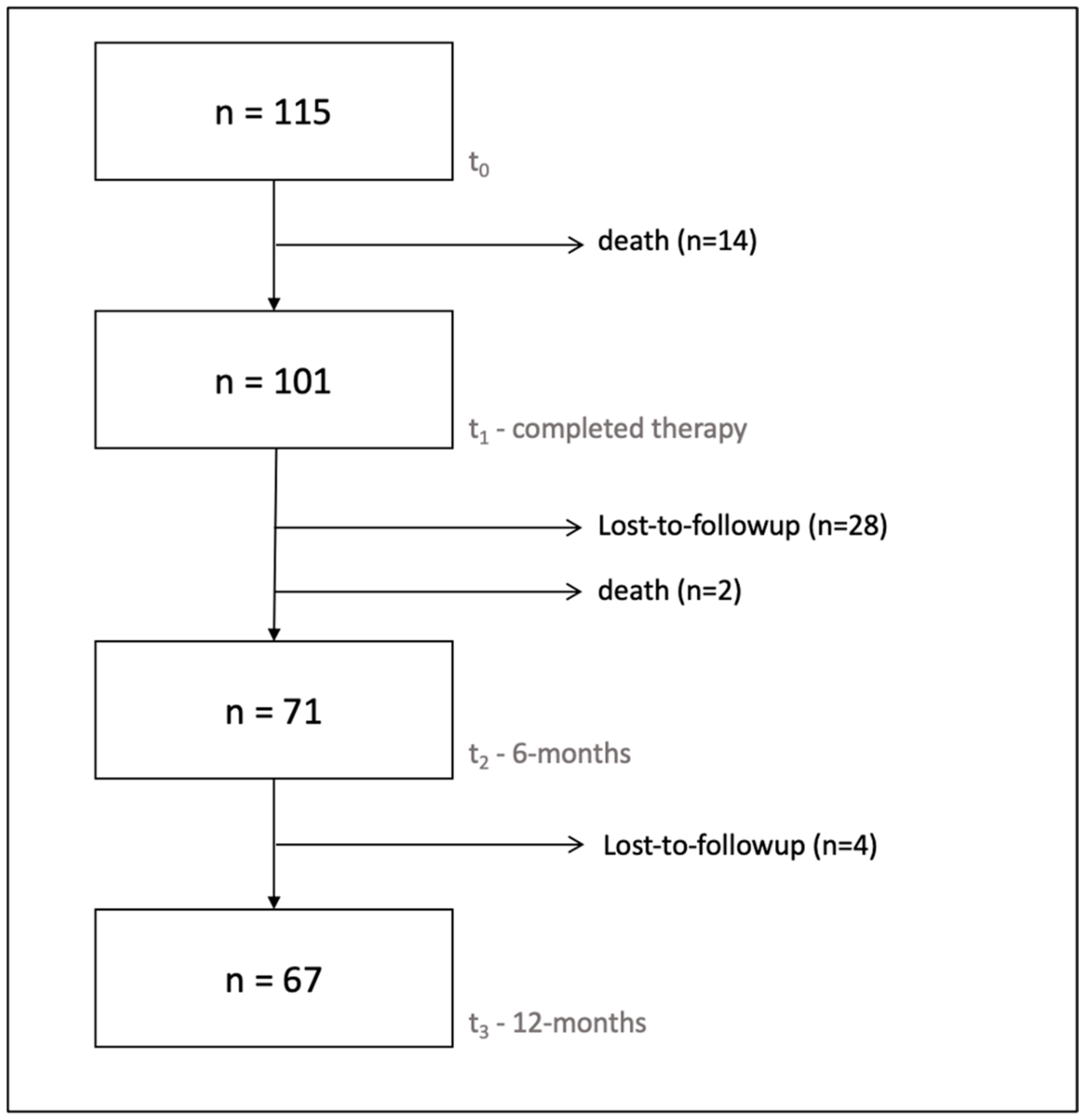
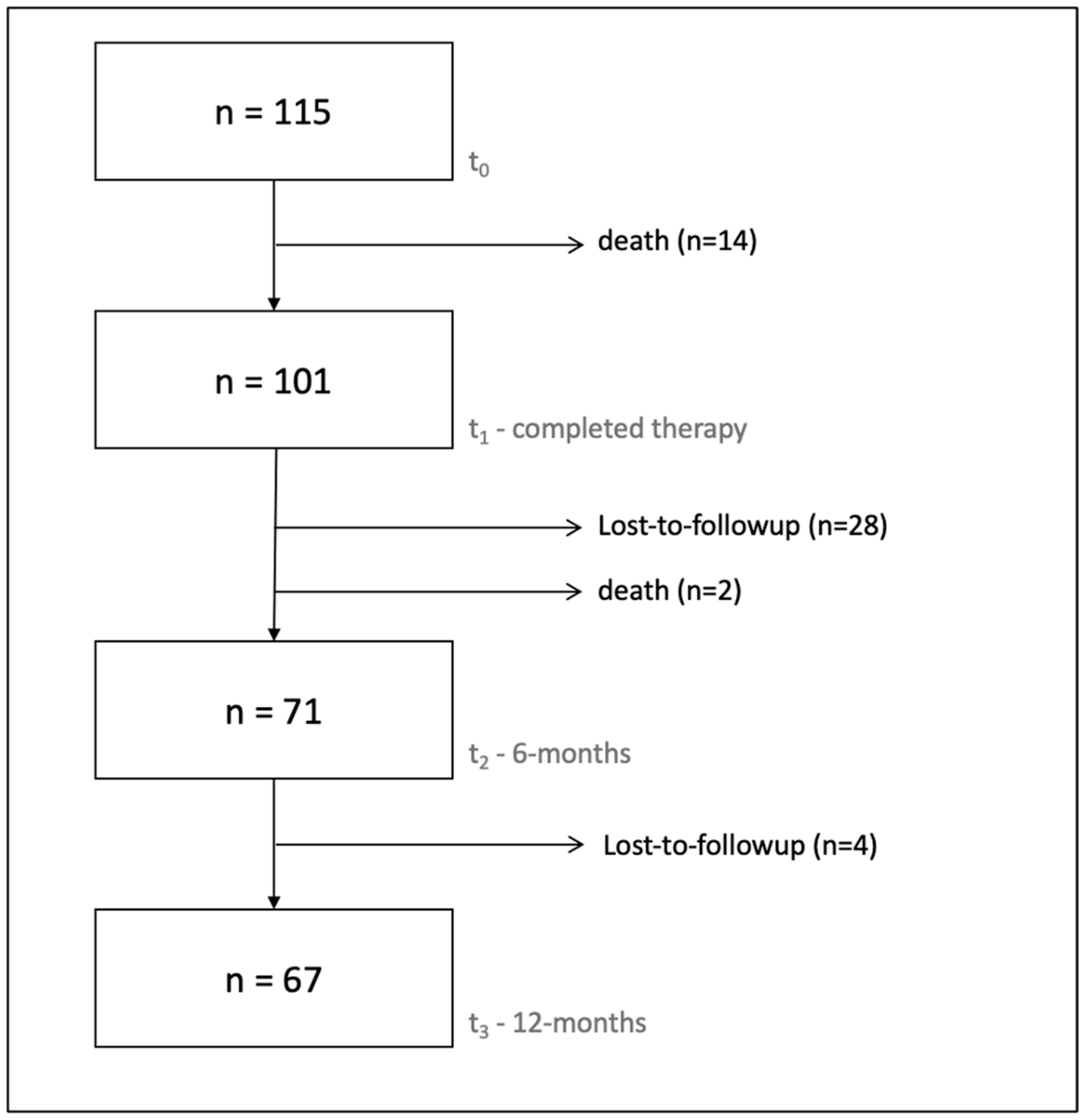
2.1. Sample
2.2. Sociodemographic Characteristics, Secondary Diagnoses, and Inpatient Stay
2.3. Microbiology
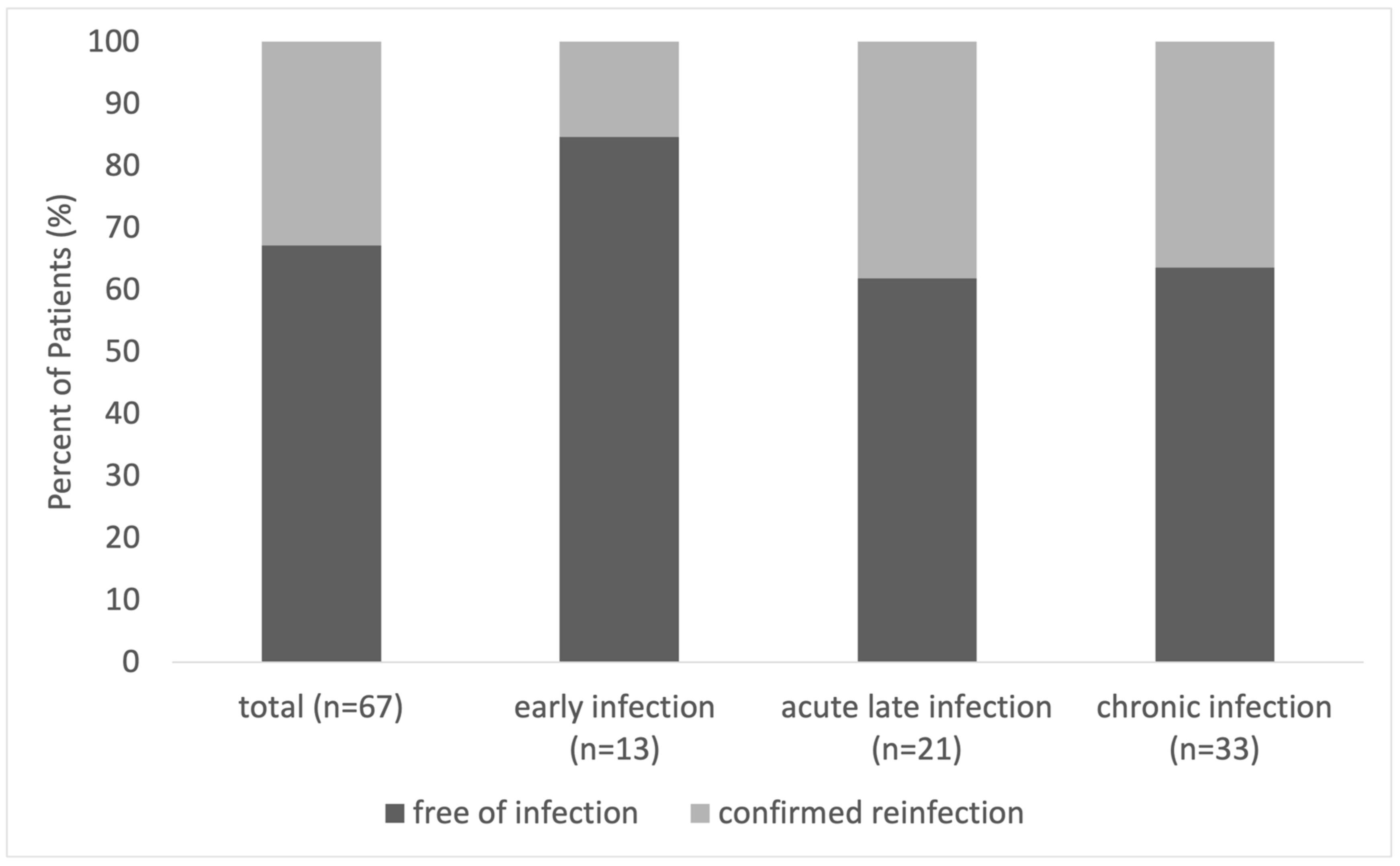
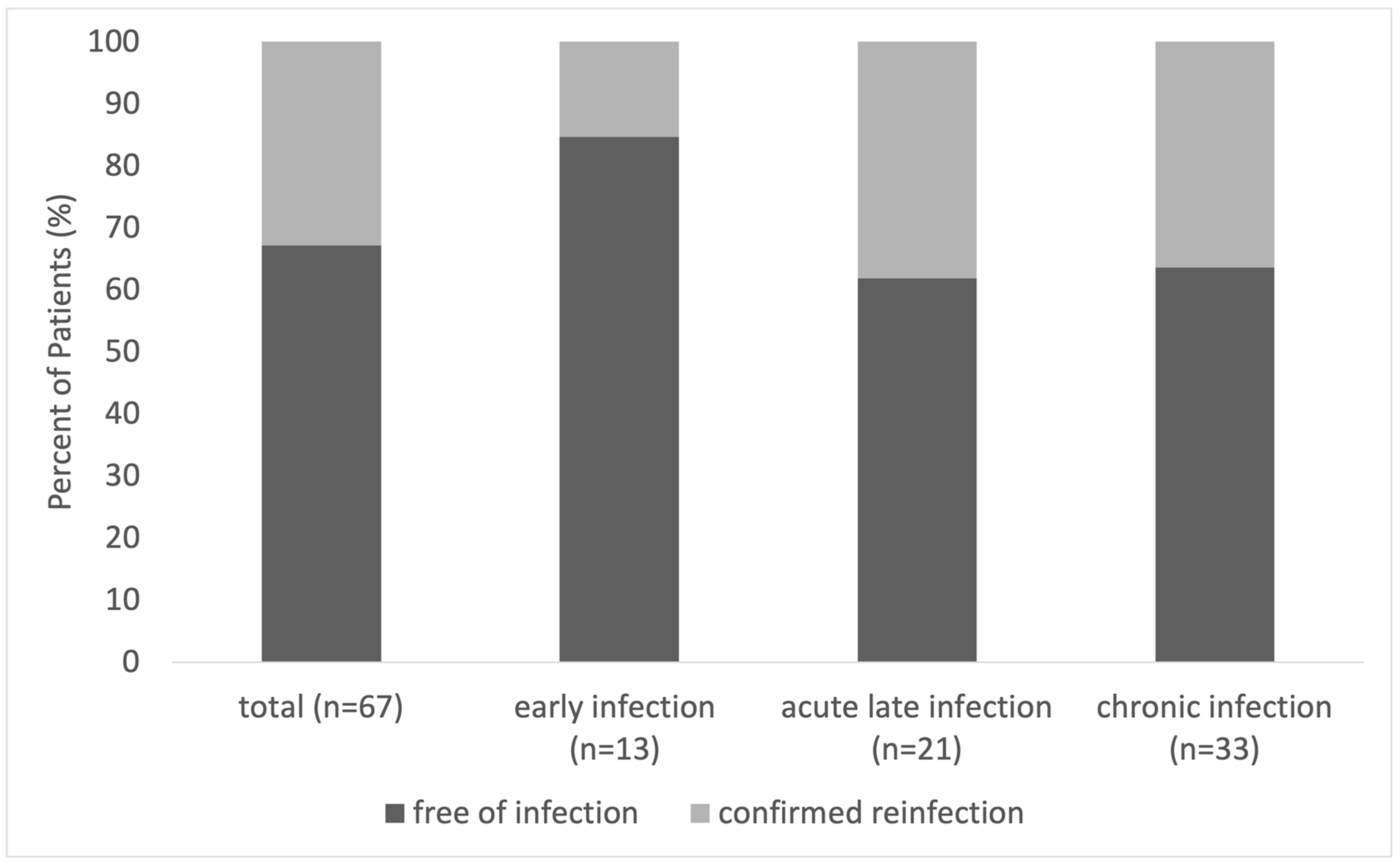
2.4. Relapse-Free Survival (RFS)
2.5. Mortality Analysis
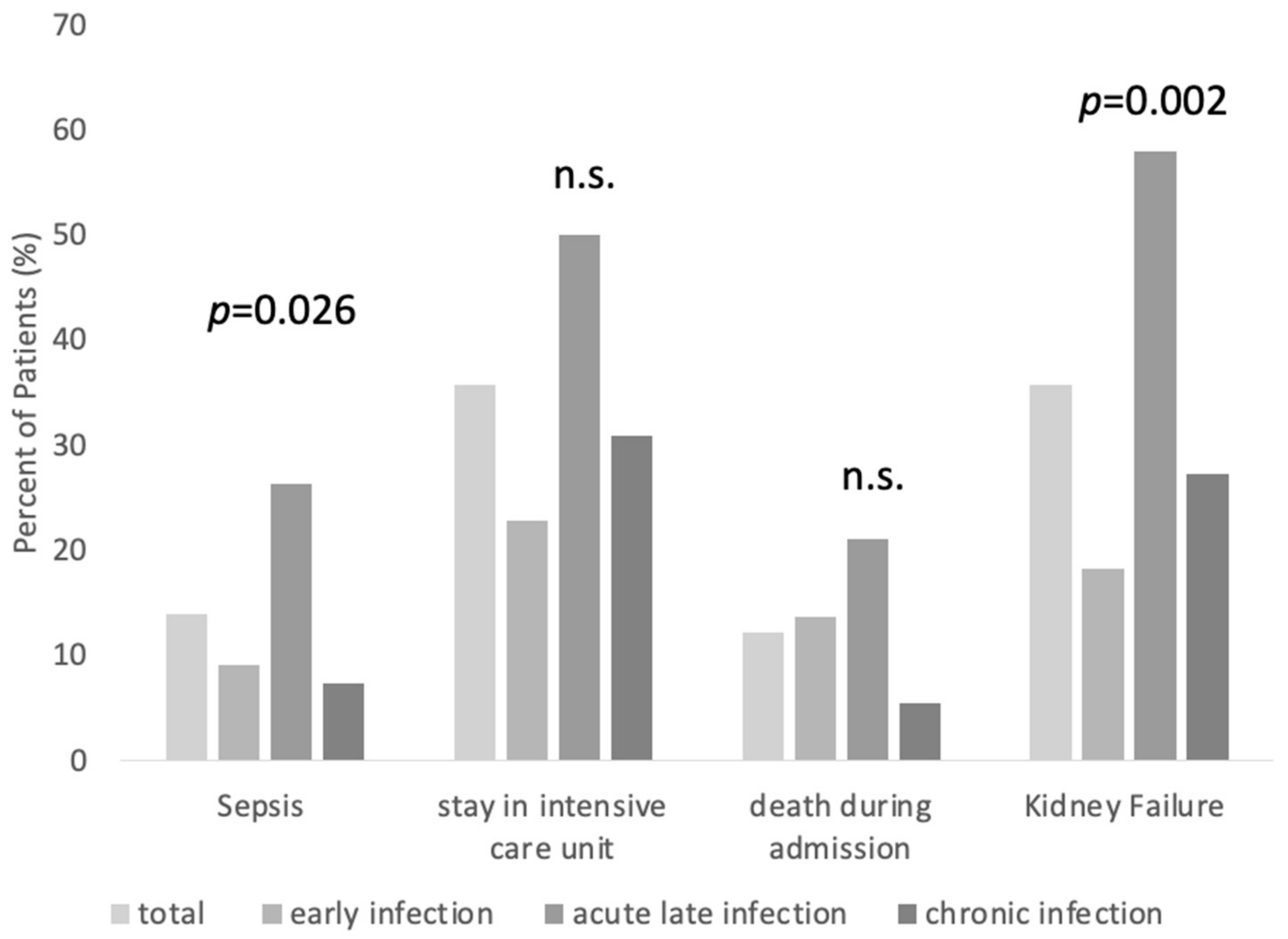
2.6. Complications
3. Materials and Methods
3.1. Study Design
3.2. Endpoints
3.3. Inclusion and Exclusion Criteria
- (i)
- Underwent THA or TKA.
- (ii)
- Had PJI according to the definition of the Musculoskeletal Infection Society criteria for periprosthetic joint infections. [14].
- (i)
- Had a prosthesis of a joint other than the hip or the knee or if they had a hemi-prothesis.
- (ii)
- Had a course of treatment that started before 1 January 2018, and after 30 June 2019.
- (iii)
- Had aseptic loosening.
- (iv)
- Had a periprosthetic fracture.
- (v)
- Had a post-traumatic primary endoprosthesis implantation.
3.4. Diagnostic and Treatment Process
3.5. Follow-Up
3.6. Data Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ALI | acute late infection |
| CI | chronic infection |
| EI | early infection |
| RFS | relapse free survival |
| ICU | intensive care unit |
| PJI | periprosthetic joint infection |
| THA | total hip arthroplasty |
| TKA | total knee arthroplasty |
References
- Zardi, E.M.; Franceschi, F. Prosthetic joint infection. A relevant public health issue. J. Infect. Public Health 2020, 13, 1888–1891. [Google Scholar] [CrossRef]
- Li, C.; Renz, N.; Trampuz, A. Management of Periprosthetic Joint Infection. Hip Pelvis 2018, 30, 138. [Google Scholar] [CrossRef] [PubMed]
- Premkumar, A.; Kolin, D.A.; Farley, K.X.; Wilson, J.M.; McLawhorn, A.S.; Cross, M.B.; Sculco, P.K. Projected Economic Burden of Periprosthetic Joint Infection of the Hip and Knee in the United States. J. Arthroplast. 2021, 36, 1484–1489.e3. [Google Scholar] [CrossRef] [PubMed]
- EPRD gGmbH. Jahresbericht 2021—Mit Sicherheit Mehr Qualität. 2021. Available online: https://www.eprd.de/fileadmin/user_upload/Dateien/Publikationen/Berichte/Jahresbericht2021_2021-10-25_F.pdf (accessed on 21 August 2023).
- Izakovicova, P.; Borens, O.; Trampuz, A. Periprosthetic joint infection: Current concepts and outlook. EFORT Open Rev. 2019, 4, 482–494. [Google Scholar] [CrossRef] [PubMed]
- Kapadia, B.H.; Berg, R.A.; Daley, J.A.; Fritz, J.; Bhave, A.; Mont, M.A. Periprosthetic joint infection. Lancet 2016, 387, 386–394. [Google Scholar] [CrossRef] [PubMed]
- McNally, M.; Sousa, R.; Wouthuyzen-Bakker, M.; Chen, A.F.; Soriano, A.; Vogely, H.C.; Clauss, M.; Higuera, C.A.; Trebše, R. The EBJIS definition of periprosthetic joint infection: A practical guide for clinicians. Bone Jt. J. 2021, 103-B, 18–25. [Google Scholar] [CrossRef] [PubMed]
- Huotari, K.; Peltola, M.; Jämsen, E. The incidence of late prosthetic joint infections: A registry-based study of 112,708 primary hip and knee replacements. Acta Orthop. 2015, 86, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Mian, H.M.; Lyons, J.G.; Perrin, J.; Froehle, A.W.; Krishnamurthy, A.B. A review of current practices in periprosthetic joint infection debridement and revision arthroplasty. Arthroplasty 2022, 4, 31. [Google Scholar] [CrossRef] [PubMed]
- Le Vavasseur, B.; Zeller, V. Antibiotic Therapy for Prosthetic Joint Infections: An Overview. Antibiotics 2022, 11, 486. [Google Scholar] [CrossRef]
- Rottier, W.; Seidelman, J.; Wouthuyzen-Bakker, M. Antimicrobial treatment of patients with a periprosthetic joint infection: Basic principles. Arthroplasty 2023, 5, 10. [Google Scholar] [CrossRef]
- Sarungi, M.; Wallace, D. Diagnosing prosthetic joint infection: Traditional and contemporary techniques. Ann. Jt. 2021, 6, 46. [Google Scholar] [CrossRef]
- Rimke, C.; Enz, A.; Bail, H.J.; Heppt, P.; Kladny, B.; von Lewinski, G.; Lohmann, C.H.; Osmanski-Zenk, K.; Haas, H.; Mittelmeier, W. Evaluation of the standard procedure for the treatment of periprosthetic joint infections (PJI) in Germany—Results of a survey within the EndoCert initiative. BMC Musculoskelet. Disord. 2020, 21, 694. [Google Scholar] [CrossRef]
- Parvizi, J.; Tan, T.L.; Goswami, K.; Higuera, C.; Della Valle, C.; Chen, A.F.; Shohat, N. The 2018 Definition of Periprosthetic Hip and Knee Infection: An Evidence-Based and Validated Criteria. J. Arthroplast. 2018, 33, 1309–1314.e2. [Google Scholar] [CrossRef]
- Fernando, N.; Yacovelli, S.; Parvizi, J. Periprosthetic Infection in the Setting of Periprosthetic Total Hip Fractures: Evaluation and Management. J. Am. Acad. Orthop. Surg. 2022, 30, 957–964. [Google Scholar] [CrossRef]
- Shah, R.P.; Plummer, D.R.; Moric, M.; Sporer, S.M.; Levine, B.R.; Della Valle, C.J. Diagnosing Infection in the Setting of Periprosthetic Fractures. J. Arthroplast. 2016, 31, 140–143. [Google Scholar] [CrossRef]
- Müller, M.; Winkler, T.; Märdian, S.; Trampuz, A.; Renz, N.; Perka, C.; Karczewski, D. The worst-case scenario: Treatment of periprosthetic femoral fracture with coexistent periprosthetic infection—A prospective and consecutive clinical study. Arch. Orthop. Trauma. Surg. 2019, 139, 1461–1470. [Google Scholar] [CrossRef]
- Sigmund, I.K.; McNally, M.A. Definition of periprosthetic joint infection and fracture-related infection. Orthop. Trauma. 2023, 37, 324–329. [Google Scholar] [CrossRef]
- Schmidutz, F.; Schreiner, A.J.; Ahrend, M.-D.; Stöckle, U.; Maier, S.; Histing, T.; Hemmann, P. Risk of Periprosthetic Joint Infection after Posttraumatic Hip Arthroplasty following Acetabular Fractures. Z. Orthop. Unf. 2023, 161, 671–677. [Google Scholar] [CrossRef] [PubMed]
- O’Driscoll, C.S.; Davey, M.S.; Hughes, A.J.; O’Byrne, J.M.; Leonard, M.; O’Daly, B.J. Total Hip Arthroplasty in the Setting of Post-Traumatic Arthritis Following Acetabular Fracture: A Systematic Review. Arthroplast. Today 2023, 19, 101078. [Google Scholar] [CrossRef] [PubMed]
- Gomes, L.S.M. Diagnóstico precoce da infecção articular periprotética do quadril—situação atual, avanços e perspectivas. Rev. Bras. Ortop. 2019, 54, 368–376. [Google Scholar] [CrossRef] [PubMed]
- Stockley, I.; Mockford, B.J.; Hoad-Reddick, A.; Norman, P. The use of two-stage exchange arthroplasty with depot antibiotics in the absence of long-term antibiotic therapy in infected total hip replacement. J. Bone Jt. Surgery. Br. Vol. 2008, 90-B, 145–148. [Google Scholar] [CrossRef] [PubMed]
- Tornero, E.; Morata, L.; Martínez-Pastor, J.C.; Angulo, S.; Combalia, A.; Bori, G.; García-Ramiro, S.; Bosch, J.; Mensa, J.; Soriano, A. Importance of selection and duration of antibiotic regimen in prosthetic joint infections treated with debridement and implant retention. J. Antimicrob. Chemother. 2016, 71, 1395–1401. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, J.P.; Warren, R.E.; Jones, R.S.; Gregson, P.A. Is prolonged systemic antibiotic treatment essential in two-stage revision hip replacement for chronic Gram-positive infection? J. Bone Jt. Surgery. Br. Vol. 2009, 91-B, 44–51. [Google Scholar] [CrossRef] [PubMed]
- Valour, F.; Karsenty, J.; Bouaziz, A.; Ader, F.; Tod, M.; Lustig, S.; Laurent, F.; Ecochard, R.; Chidiac, C.; Ferry, T. Antimicrobial-Related Severe Adverse Events during Treatment of Bone and Joint Infection Due to Methicillin-Susceptible Staphylococcus aureus. Antimicrob. Agents Chemother. 2014, 58, 746–755. [Google Scholar] [CrossRef]
- Diaz-Ledezma, C.; Higuera, C.A.; Parvizi, J. Success After Treatment of Periprosthetic Joint Infection: A Delphi-based International Multidisciplinary Consensus. Clin. Orthop. Relat. Res. 2013, 471, 2374–2382. [Google Scholar] [CrossRef] [PubMed]
- Wouthuyzen-Bakker, M.; Sebillotte, M.; Huotari, K.; Escudero Sánchez, R.; Benavent, E.; Parvizi, J.; Fernandez-Sampedro, M.; Barbero, J.M.; Garcia-Cañete, J.; Trebse, R.; et al. Lower Success Rate of Débridement and Implant Retention in Late Acute versus Early Acute Periprosthetic Joint Infection Caused by Staphylococcus spp. Results from a Matched Cohort Study. Clin. Orthop. Relat. Res. 2020, 478, 1348–1355. [Google Scholar] [CrossRef]
- Chang, M.J.; Ro, D.H.; Kim, T.W.; Lee, Y.S.; Han, H.-S.; Chang, C.B.; Kang, S.-B.; Lee, M.C. Worse outcome of debridement, antibiotics, and implant retention in acute hematogenous infections than in postsurgical infections after total knee arthroplasty: A multicenter study. Knee Surg. Relat. Res. 2022, 34, 38. [Google Scholar] [CrossRef]
- Vilchez, F.; Martínez-Pastor, J.C.; García-Ramiro, S.; Bori, G.; Tornero, E.; García, E.; Mensa, J.; Soriano, A. Efficacy of Debridement in Hematogenous and Early Post-Surgical Prosthetic Joint Infections. Int. J. Artif. Organs 2011, 34, 863–869. [Google Scholar] [CrossRef]
- Chen, W.; Klemt, C.; Smith, E.J.; Tirumala, V.; Xiong, L.; Kwon, Y.-M. Outcomes and Risk Factors Associated With Failures of Debridement, Antibiotics, and Implant Retention in Patients With Acute Hematogenous Periprosthetic Joint Infection. J. Am. Acad. Orthop. Surg. 2021, 29, 1024–1030. [Google Scholar] [CrossRef] [PubMed]
- Renz, N.; Trampuz, A.; Perka, C.; Rakow, A. Outcome and Failure Analysis of 132 Episodes of Hematogenous Periprosthetic Joint Infections—A Cohort Study. Open Forum Infect. Dis. 2022, 9, ofac094. [Google Scholar] [CrossRef] [PubMed]
- Pansu, N.; Hamoui, M.; Manna, F.; Makinson, A.; Dufour, S.; Morquin, D.; Canovas, F.; Reynes, J.; Le Moing, V. Implant retention and high rate of treatment failure in hematogenous acute knee and hip prosthetic joint infections. Médecine Mal. Infect. 2020, 50, 702–708. [Google Scholar] [CrossRef]
- Konigsberg, B.S.; Valle, C.J.D.; Ting, N.T.; Qiu, F.; Sporer, S.M. Acute Hematogenous Infection Following Total Hip and Knee Arthroplasty. J. Arthroplast. 2014, 29, 469–472. [Google Scholar] [CrossRef]
- Wouthuyzen-Bakker, M.; Sebillotte, M.; Lomas, J.; Taylor, A.; Palomares, E.B.; Murillo, O.; Parvizi, J.; Shohat, N.; Reinoso, J.C.; Sánchez, R.E.; et al. Clinical outcome and risk factors for failure in late acute prosthetic joint infections treated with debridement and implant retention. J. Infect. 2019, 78, 40–47. [Google Scholar] [CrossRef]
- Löwik, C.A.M.; Jutte, P.C.; Tornero, E.; Ploegmakers, J.J.W.; Knobben, B.A.S.; de Vries, A.J.; Zijlstra, W.P.; Dijkstra, B.; Soriano, A.; Wouthuyzen-Bakker, M. Predicting Failure in Early Acute Prosthetic Joint Infection Treated With Debridement, Antibiotics, and Implant Retention: External Validation of the KLIC Score. J. Arthroplast. 2018, 33, 2582–2587. [Google Scholar] [CrossRef]
- Abrman, K.; Musil, D.; Stehlík, J. Treatment of Acute Periprosthetic Infections with DAIR (Debridement, Antibiotics and Implant Retention)—Success Rate and Risk Factors of Failure. Acta Chir. Orthop. Traumatol. Cech. 2019, 86, 181–187. [Google Scholar] [CrossRef]
- Sigmund, I.K.; Winkler, T.; Önder, N.; Perka, C.; Renz, N.; Trampuz, A. Complications of Resection Arthroplasty in Two-Stage Revision for the Treatment of Periprosthetic Hip Joint Infection. JCM 2019, 8, 2224. [Google Scholar] [CrossRef]
- Drain, N.P.; Bertolini, D.M.; Anthony, A.W.; Feroze, M.W.; Chao, R.; Onyekweli, T.; Longo, S.E.; Hersh, B.L.; Smith, C.N.; Rothenberger, S.D.; et al. High Mortality After Total Knee Arthroplasty Periprosthetic Joint Infection is Related to Preoperative Morbidity and the Disease Process but Not Treatment. J. Arthroplast. 2022, 37, 1383–1389. [Google Scholar] [CrossRef]
- Lum, Z.C.; Natsuhara, K.M.; Shelton, T.J.; Giordani, M.; Pereira, G.C.; Meehan, J.P. Mortality During Total Knee Periprosthetic Joint Infection. J. Arthroplast. 2018, 33, 3783–3788. [Google Scholar] [CrossRef] [PubMed]
- Gundtoft, P.H.; Pedersen, A.B.; Varnum, C.; Overgaard, S. Increased Mortality After Prosthetic Joint Infection in Primary THA. Clin. Orthop. Relat. Res. 2017, 475, 2623–2631. [Google Scholar] [CrossRef] [PubMed]
- Natsuhara, K.M.; Shelton, T.J.; Meehan, J.P.; Lum, Z.C. Mortality During Total Hip Periprosthetic Joint Infection. J. Arthroplast. 2019, 34, S337–S342. [Google Scholar] [CrossRef] [PubMed]
- Leta, T.H.; Lygre, S.H.L.; Schrama, J.C.; Hallan, G.; Gjertsen, J.-E.; Dale, H.; Furnes, O. Outcome of Revision Surgery for Infection After Total Knee Arthroplasty: Results of 3 Surgical Strategies. JBJS Rev. 2019, 7, e4. [Google Scholar] [CrossRef]
- Zmistowski, B.; Karam, J.A.; Durinka, J.B.; Casper, D.S.; Parvizi, J. Periprosthetic Joint Infection Increases the Risk of One-Year Mortality. J. Bone Jt. Surg. 2013, 95, 2177–2184. [Google Scholar] [CrossRef]
- Pöll, A.M.; Baecker, H.; Yilmaz, E.; Jansen, O.; Waydhas, C.; Schildhauer, T.A.; Hamsen, U. Risk factors and outcome of patients with periprosthetic joint infection admitted to intensive care unit. Arch. Orthop. Trauma. Surg. 2020, 140, 1081–1085. [Google Scholar] [CrossRef]
- Maaloum, Y.; Meybeck, A.; Olive, D.; Boussekey, N.; Delannoy, P.-Y.; Chiche, A.; Georges, H.; Beltrand, E.; Senneville, E.; d’Escrivan, T.; et al. Clinical spectrum and outcome of critically ill patients suffering from prosthetic joint infections. Infection 2013, 41, 493–501. [Google Scholar] [CrossRef]
- Balato, G.; Ascione, T.; de Matteo, V.; Lenzi, M.; Amato, M.; de Giovanni, R.; Festa, E.; Mariconda, M. Debridement and implant retention in acute hematogenous periprosthetic joint infection after knee arthroplasty: A systematic review. Orthop. Rev. 2022, 14, 33670. Available online: https://orthopedicreviews.openmedicalpublishing.org/article/33670-debridement-and-implant-retention-in-acute-hematogenous-periprosthetic-joint-infection-after-knee-arthroplasty-a-systematic-review (accessed on 8 May 2023). [CrossRef]
- Kalbian, I.; Park, J.W.; Goswami, K.; Lee, Y.K.; Parvizi, J.; Koo, K.H. Culture-negative periprosthetic joint infection: Prevalence, aetiology, evaluation, recommendations, and treatment. Int. Orthop. 2020, 44, 1255–1261. [Google Scholar] [CrossRef] [PubMed]
- Reisener, M.; Perka, C. Do Culture-Negative Periprosthetic Joint Infections Have a Worse Outcome Than Culture-Positive Periprosthetic Joint Infections? A Systematic Review and Meta-Analysis. BioMed Res. Int. 2018, 2018, 6278012. [Google Scholar] [CrossRef] [PubMed]
- Benito, N.; Mur, I.; Ribera, A.; Soriano, A.; Rodríguez-Pardo, D.; Sorlí, L.; Cobo, J.; Fernández-Sampedro, M.; del Toro, M.D.; Guío, L.; et al. The Different Microbial Etiology of Prosthetic Joint Infections according to Route of Acquisition and Time after Prosthesis Implantation, Including the Role of Multidrug-Resistant Organisms. J. Clin. Med. 2019, 8, 673. [Google Scholar] [CrossRef] [PubMed]
- Yu, Y.; Kong, Y.; Ye, J.; Wang, A.; Si, W. Microbiological pattern of prosthetic hip and knee infections: A high-volume, single-centre experience in China. J. Med. Microbiol. 2021, 70, 001305. [Google Scholar] [CrossRef] [PubMed]
- Bernard, L.; Arvieux, C.; Brunschweiler, B.; Touchais, S.; Ansart, S.; Bru, J.-P.; Oziol, E.; Boeri, C.; Gras, G.; Druon, J.; et al. Antibiotic Therapy for 6 or 12 Weeks for Prosthetic Joint Infection. N. Engl. J. Med. 2021, 384, 1991–2001. [Google Scholar] [CrossRef] [PubMed]
- Olearo, F.; Zanichelli, V.; Exarchakou, A.; Both, A.; Uςkay, I.; Aepfelbacher, M.; Rohde, H. The Impact of Antimicrobial Therapy Duration in the Treatment of Prosthetic Joint Infections Depending on Surgical Strategies: A Systematic Review and Meta-analysis. Open Forum Infect. Dis. 2023, 10, ofad246. [Google Scholar] [CrossRef] [PubMed]
- Reinecke, P.; Morovic, P.; Niemann, M.; Renz, N.; Perka, C.; Trampuz, A.; Meller, S. Adverse Events Associated with Prolonged Antibiotic Therapy for Periprosthetic Joint Infections—A Prospective Study with a Special Focus on Rifampin. Antibiotics 2023, 12, 1560. [Google Scholar] [CrossRef] [PubMed]
- Bouji, N.; Wen, S.; Dietz, M.J. Intravenous antibiotic duration in the treatment of prosthetic joint infection: Systematic review and meta-analysis. J. Bone Jt. Infect. 2022, 7, 191–202. [Google Scholar] [CrossRef] [PubMed]
- Bongers, J.; Jacobs, A.M.E.; Smulders, K.; van, G.G.; Goosen, J.H.M. Reinfection and re-revision rates of 113 two-stage revisions in infected TKA. J. Bone Jt. Infect. 2020, 5, 137–144. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Total (n = 115) | Early Infection (EI) (n = 22) | Acute Late Infection (ALI) (n = 38) | Chronic Infection (CI) (n = 55) | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Absolute | % | Absolute | % | Absolute | % | Absolute | % | ||
| Female | 58 | 50.4 | 12 | 54.5 | 19 | 50.0 | 27 | 49.1 | |
| Male | 57 | 49.6 | 10 | 45.5 | 19 | 50.0 | 28 | 50.9 | |
| Total hip replacement | 67 | 58.3 | 17 | 77.3 | 17 | 44.7 | 33 | 60.0 | |
| Total knee replacement | 48 | 41.7 | 5 | 22.7 | 21 | 55.3 | 22 | 40.0 | |
| Average | SD | Average | SD | Average | SD | Average | SD | p-value | |
| BMI | 30.6 | 7.8 | 30.3 | 9.2 | 31.4 | 7.0 | 30.3 | 7.9 | 0.768 |
| Age at admission | 70.6 | 10.6 | 70.1 | 8.7 | 74.3 | 8.7 | 68.2 | 11.8 | 0.023 * |
| Age at initial implantation | 63.5 | 12.1 | 70.1 | 8.7 | 64.8 | 10.7 | 59.8 | 13.1 | 0.002 * |
| ASA score | 2.7 | 0.6 | 2.5 | 0.5 | 2.9 | 0.6 | 2.6 | 0.6 | 0.031 * |
| CRP | 89.9 | 107.6 | 80.7 | 73.8 | 136.0 | 122.8 | 65.6 | 102.5 | 0.011 * |
| Total (n = 115) | Early Infection (EI) (n = 22) | Acute Late Infection (ALI) (n = 38) | Chronic Infection (CI) (n = 55) | |||||
|---|---|---|---|---|---|---|---|---|
| Absolute | % | Absolute | % | Absolute | % | Absolute | % | |
| Negative microbiological culture | 15 | 13.0 | 2 | 9.1 | 4 | 10.5 | 9 | 16.4 |
| Positive microbiological culture | 100 | 87.0 | 20 | 90.9 | 34 | 89.5 | 46 | 83.6 |
| Multiple pathogens in culture | 14 | 14.0 | 2 | 1.0 | 6 | 17.6 | 7 | 15.2 |
| Staphylococci * | 66 | 57.4 | 7 | 31.8 | 23 | 60.5 | 36 | 65.5 |
| Enterococci | 10 | 8.7 | 2 | 9.1 | 4 | 10.5 | 4 | 7.3 |
| Enterobacterales | 21 | 18.3 | 7 | 31.8 | 8 | 21.1 | 6 | 10.9 |
| Anaerobic bacteria | 10 | 8.7 | 4 | 18.2 | 2 | 5.3 | 4 | 7.3 |
| Corynebacteria | 2 | 1.7 | 1 | 4.5 | 0 | 0.0 | 1 | 1.8 |
| Streptococci | 7 | 6.1 | 1 | 4.5 | 3 | 7.9 | 3 | 5.5 |
| Spore formers | 4 | 3.5 | 0 | 0.0 | 2 | 5.3 | 2 | 3.6 |
| Yeast-like fungi | 1 | 0.9 | 0 | 0.0 | 1 | 2.6 | 0 | 0.0 |
| * S. aureus | 27 | 40.9 | 4 | 57.1 | 11 | 47.8 | 12 | 33.3 |
| Coagulase-negative staphylococci (CNS) | 38 | 57.6 | 3 | 42.9 | 12 | 52.2 | 23 | 63.9 |
| S. aureus and CNS | 1 | 1.5 | 0 | 0.0 | 0 | 0.0 | 1 | 2.8 |
| Total (n = 71) | EI (n = 15) | ALI (n = 21) | CI (n = 35) | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Absolute Number | % | Absolute Number | % | Absolute Number | % | Absolute Number | % | p-Value | ||
| After 6 months | Free of infection | 54 | 76.1 | 14 | 93.3 | 15 | 71.4 | 25 | 71.4 | 0.396 |
| Reinfection | 17 | 23.9 | 1 | 6.7 | 6 | 28.6 | 10 | 28.6 | ||
| Total (n = 67) | EI (n = 13) | ALI (n = 21) | CI (n = 33) | |||||||
| After 12 months | Free of infection | 45 | 67.2 | 11 | 84.6 | 13 | 61.9 | 21 | 63.6 | 0.621 |
| Reinfection | 22 | 32.8 | 2 | 15.4 | 8 | 38.1 | 12 | 36.4 |
| Death before Therapy Completion (n = 14) | Complete Treatment (n = 101) | ||||
|---|---|---|---|---|---|
| Absolute | % | Absolute | % | ||
| Female | 7 | 50.0 | 50 | 49.5 | |
| Male | 7 | 50.0 | 51 | 50.5 | |
| Total hip replacement | 9 | 64.3 | 58 | 57.4 | |
| Total knee replacement | 5 | 35.7 | 43 | 42.6 | |
| Average | SD | Average | SD | p-value | |
| Age at admission | 75.0 | 9.1 | 70.0 | 10.7 | 0.096 |
| BMI | 31.2 | 7.3 | 30.6 | 7.9 | 0.790 |
| ASA score | 3.2 | 0.8 | 2.6 | 0.5 | 0.001 * |
| Stay in intensive care unit | 14 | 100.0 | 27 | 26.7 | 0.000 * |
| Sepsis | 10 | 71.4 | 6 | 5.9 | 0.000 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Youssef, Y.; Roschke, E.; Dietze, N.; Dahse, A.-J.; Chaberny, I.F.; Ranft, D.; Pempe, C.; Goralski, S.; Ghanem, M.; Kluge, R.; et al. Early-Outcome Differences between Acute and Chronic Periprosthetic Joint Infections—A Retrospective Single-Center Study. Antibiotics 2024, 13, 198. https://doi.org/10.3390/antibiotics13030198
Youssef Y, Roschke E, Dietze N, Dahse A-J, Chaberny IF, Ranft D, Pempe C, Goralski S, Ghanem M, Kluge R, et al. Early-Outcome Differences between Acute and Chronic Periprosthetic Joint Infections—A Retrospective Single-Center Study. Antibiotics. 2024; 13(3):198. https://doi.org/10.3390/antibiotics13030198
Chicago/Turabian StyleYoussef, Yasmin, Elisabeth Roschke, Nadine Dietze, Anna-Judith Dahse, Iris F. Chaberny, Donald Ranft, Christina Pempe, Szymon Goralski, Mohamed Ghanem, Regine Kluge, and et al. 2024. "Early-Outcome Differences between Acute and Chronic Periprosthetic Joint Infections—A Retrospective Single-Center Study" Antibiotics 13, no. 3: 198. https://doi.org/10.3390/antibiotics13030198
APA StyleYoussef, Y., Roschke, E., Dietze, N., Dahse, A.-J., Chaberny, I. F., Ranft, D., Pempe, C., Goralski, S., Ghanem, M., Kluge, R., Lübbert, C., Rodloff, A. C., & Roth, A. (2024). Early-Outcome Differences between Acute and Chronic Periprosthetic Joint Infections—A Retrospective Single-Center Study. Antibiotics, 13(3), 198. https://doi.org/10.3390/antibiotics13030198